See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/342572286 Evaluating the Implementation of an Intervention to Improve Postpartum Contraception in Tanzania: A Qualitative Study of Provider and Client Perspectives Article in Global Health: Science and Practice · June 2020 DOI: 10.9745/GHSP-D-19-00365 CITATIONS 0 READS 4 8 authors, including: Some of the authors of this publication are also working on these related projects: Willows Reproductive Health Impact Evaluation View project PPIUD Project View project Kristy M Hackett Harvard University 25 PUBLICATIONS 66 CITATIONS SEE PROFILE Sarah Huber-Krum Centers for Disease Control and Prevention 18 PUBLICATIONS 27 CITATIONS SEE PROFILE Leigh Senderowicz Harvard University 15 PUBLICATIONS 62 CITATIONS SEE PROFILE Hellen Siril Muhimbili University of Health and Allied Sciences 36 PUBLICATIONS 132 CITATIONS SEE PROFILE All content following this page was uploaded by Kristy M Hackett on 30 June 2020. The user has requested enhancement of the downloaded file.
Transcript
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/342572286
Evaluating the Implementation of an Intervention to Improve Postpartum
Contraception in Tanzania: A Qualitative Study of Provider and Client
Perspectives
Article in Global Health: Science and Practice · June 2020
DOI: 10.9745/GHSP-D-19-00365
CITATIONS
0READS
4
8 authors, including:
Some of the authors of this publication are also working on these related projects:
Willows Reproductive Health Impact Evaluation View project
PPIUD Project View project
Kristy M Hackett
Harvard University
25 PUBLICATIONS 66 CITATIONS
SEE PROFILE
Sarah Huber-Krum
Centers for Disease Control and Prevention
18 PUBLICATIONS 27 CITATIONS
SEE PROFILE
Leigh Senderowicz
Harvard University
15 PUBLICATIONS 62 CITATIONS
SEE PROFILE
Hellen Siril
Muhimbili University of Health and Allied Sciences
36 PUBLICATIONS 132 CITATIONS
SEE PROFILE
All content following this page was uploaded by Kristy M Hackett on 30 June 2020.
The user has requested enhancement of the downloaded file.
Evaluating the Implementation of an Intervention to ImprovePostpartum Contraception in Tanzania: A Qualitative Studyof Provider and Client PerspectivesKristy Hackett,a Sarah Huber-Krum,a Joel M. Francis,b,c Leigh Senderowicz,a Erin Pearson,d Hellen Siril,b
Nzovu Ulenga,b Iqbal Shaha
Key Findings
n Constraints on staff, time, and supplies andchallenges with referrals influencedimplementation outcomes and threatenedsustainability.
n Women reported that interpersonal aspects ofcare varied.
n Providers reported that additional trainingopportunities, improved staffing, and increasedavailability of PPIUD supplies would strengthenfuture initiatives.
Key Implications
We recommend that PPFP program imple-menters consider:
n Assessing the feasibility of integrating PPFPcounseling into existing antenatal care servicesbefore program implementation
n Ensuring that future initiatives emphasize patient-centered PPFP counseling, informed choice, andrespectful and nondiscriminatory service delivery
n Implementing a stronger interfacility performanceand quality improvement system to strengthencoordination
n Using different models of PPFP counseling tohelp alleviate provider workload
ABSTRACTBackground: This qualitative study assessed implementation ofthe Postpartum Intrauterine Device (PPIUD) Initiative in Tanzania,a country with high rates of unintended pregnancy and low con-traceptive prevalence. The PPIUD Initiative was implemented toreduce unmet need for contraception among new mothersthrough postpartum family planning counseling delivered duringantenatal care and offering PPIUD insertion immediately follow-ing birth.Methods: We used the implementation outcomes framework andan ecological framework to analyze in-depth interviews with pro-viders (N=15) and women (N=47) participating in the initiative.We applied a multistage coding protocol and used thematic con-tent analysis to identify the factors influencing implementation.Results: Both women and providers were enthusiastic and recep-tive to the PPIUD Initiative. Health system and resource constraintsmade adoption and fidelity to the intended intervention challeng-ing. Many providers questioned the sustainability of the initiative,and most agreed that changes to the initiative’s design (e.g., ad-ditional training opportunities, improved staffing, and availabilityof PPIUD supplies) would strengthen future iterations of the initia-tive. According to women, interpersonal aspects of care varied,with some women reporting rushed or incomplete counseling oran emphasis on the PPIUD over other methods. The perceptionthat some providers treat older married women more favorablysuggests that fidelity to the intended PPIUD Initiative was not uni-formly achieved.Conclusions: Study findings inform initiatives seeking to developand adopt postpartum family planning programs and enhanceprogram implementation. A comprehensive needs assessment toevaluate feasibility and identify potential adaptations for the localcontext is recommended. Training and supervision to improveinterpersonal aspects of care, including an emphasis on patient-centered counseling, informed choice, and respectful andnondiscriminatory service delivery should be integrated into fu-ture postpartum family planning initiatives.
INTRODUCTION
Unintended and mistimed pregnancies are pressingglobal public health concerns due to their associa-
tions with increased maternal, newborn, and childmorbidity and mortality.1–4 The postpartum periodrepresents a critical window of opportunity to ensurehealthy timing and spacing of subsequent pregnanciesand to address unmet need for family planning.5
a Department of Global Health and Population, Harvard T.H. Chan School ofPublic Health, Boston, MA, USA.b Management and Development for Health, Dar es Salaam, Tanzania.c Department of Family Medicine and Primary Care, School of Clinical Medicine,Faculty of Health Sciences, University of theWitwatersrand, Johannesburg, SouthAfrica.d Technical Innovation and Evidence, Ipas, Chapel Hill, NC, USA.Correspondence to Kristy Hackett ([email protected]).
Global Health: Science and Practice 2020 | Volume 8 | Number 2 270
Despite increased attention to the postpartumperiod as an opportunity for family planning inter-ventions, recent estimates from 57 countries showthat 62% of women have an unmet need forcontraception immediately after delivery, and40% have an unmet need within the first year af-ter birth.6 Postpartum family planning (PPFP)initiatives that respect women’s right to make fulland informed choices have the potential to helpmeet these needs.
Where available, PPFP counseling is part ofpostnatal care (PNC) services.7 However, PPFPcounseling is not consistently provided, and PNCoften disproportionally focuses on the well-beingof the newborn rather than the mother. Addi-tionally, in many low-income settings, a host ofsocioeconomic obstacles prevent mothers fromreturning to facilities for postnatal check-ups;therefore, opportunities for PPFP are oftenmissed.8 One strategy to overcome this challengeis to provide PPFP counseling during antenatalcare (ANC), which is more widely used than PNC,followed by immediate insertion of the intrauter-ine device (IUD) after delivery (within 10 minutesfollowing delivery of the placenta or within48 hours) to women who opt for this method.The copper IUD is widely accepted as an effective,long-acting (up to 12 years), reversible methodof contraception and is particularly convenientwhen inserted immediately after birth.9 Otherbenefits of the postpartum IUD (PPIUD) are thatit can be inserted after either vaginal or cesareandelivery, does not interfere with breastfeeding,and can be used by women who have HIV.9
Several systematic reviews have established thesafety and effectiveness of PPIUD insertion.10,11
Immediate PPIUD insertion is a specializedtechnique that differs from interval IUD insertion,and thus requires additional hands-on didactictraining and specialized equipment.12 Due to theearly postpartum timing of the procedure and therapid change in the uterus during this time, expul-sion rates for immediate PPIUD insertions arehigher than for interval insertions.12 According toa recent review, expulsion rates vary by timing ofIUD placement, ranging from 1.9% with intervalplacements (greater than 4 weeks postpartum),10.0% for immediate placements within 10 min-utes following placental delivery, and 29.7% forplacements between 10 minutes to 4 weeks post-partum.13 For these reasons, it is recommendedthat women who opt for PPIUD insertion arecounseled regarding the increased expulsion risk,as well as signs and symptoms of expulsion.12
Recent improvements in institutional deliveryrates across sub-Saharan Africa14 make prenatalcontraceptive counseling and PPIUD a promisingPPFP option among populations likely to receiveANC and/or deliver in facilities but unlikely toreturn for care in the postpartum period. InTanzania, institutional delivery rates have in-creased substantially in recent decades (44% to63% between 1999 and 2016) and uptake ofANC from a skilled provider is almost universal(98% in 2016), yet PNC coverage has been slowto improve.15 Only 37%ofmothers receive a post-natal checkup after their most recent live birth15
and the quality of postnatal services is often low.16
Therefore, providing prenatal contraceptivecounseling and offering PPIUD insertion is adesirable intervention in Tanzania, where thegovernment recently committed to increasing theavailability ofmodern contraception at all levels ofthe health system from 40% in 2012 to 70% by2020.17 Tanzania’s modern contraceptive preva-lence rate (mCPR) is 31%, and more than a quar-ter of reproductive-age women have an unmetneed for modern contraception.17 Despite theknown benefits of PPIUD, uptake of the IUD, re-gardless of insertion timing, is low in Tanzania(less than 1%among reproductive-agewomen).15
Programs providing PPIUD services are just begin-ning to emerge in low- and middle-income coun-tries (LMICs); consequently, there is a gap in theliterature on PPIUD programs, with few publishedevaluations and limited research on implementa-tion processes.18 This study helps to fill this gapby assessing the factors influencing implementa-tion of a novel PPIUD Initiative in Tanzania.
PPIUD INITIATIVE DESCRIPTION ANDACHIEVEMENTS
In 2013, the International Federation of Gyne-cology and Obstetrics (FIGO) launched an initia-tive to institutionalize PPIUD services in SriLanka, followed by Tanzania, Nepal, India,Kenya, and Bangladesh in 2015.19 Through thisinitiative, clinic and hospital staff in select facilitiesreceived training on the provision of PPFPcounseling and PPIUD insertion techniques asnovel services. To promote sustainability, the proj-ect was designed for implementation within exist-ing maternity services, and current staff wereintended to deliver PPFP counseling and PPIUDinsertion rather than recruiting new health work-ers. Facilities were selected on the basis of having alarge annual obstetric caseload (>5000 deliveries),a large number of providers and medical trainees,
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 271
and no PPIUD services already provided.19 In eachcountry, the project was implemented throughnational pro-fessional societies or colleges to en-courage ownership by in-country obstetriciansand gynecologists. Although the project designand budget allowed for country-specific tailoring,the same general model was implemented in eachcountry. This model included a dedicated projectmanagement team, a coordinator at each partici-pating facility, a Data Safety MonitoringCommittee, and national steering groups whoprovided clinical and technical guidance.19
Further details on the PPIUD Initiative design andcomponents are published elsewhere.19 We pre-sent key elements and inputs of the PPIUDInitiative in Table 1 and summarize interventioncomponents at the provider and client levels inFigure 1.
Tanzania PPIUD InitiativeIn Tanzania, the PPIUD Initiative was first imple-mented in 6 hospitals. However, 1 facility wasdropped because it had an ongoing PPIUD inter-vention. Therefore, the study was conducted in5 hospitals. FIGO and their local affiliate, theAssociation of Gynecologists and Obstetricians ofTanzania (AGOTA): (1) trained maternity careproviders at tertiary/teaching hospitals on PPFPcounseling, PPIUD insertion techniques, and com-plications management; (2) hosted informationalworkshops for nurses and midwives at satelliteclinics on PPFP counseling techniques; (3) provid-ed PPFP leaflets to be distributed during counsel-ing; (4) provided a video to be played in hospitalwaiting areas; (5) supplied Kelly forceps for vagi-nal PPIUD insertion; and (6) conducted regularmonitoring and support.
Provider TrainingThe PPIUD Initiative applied a “train-the-trainer”approach whereby a group of master trainerswere identified in each country, trained providerson PPFP counseling and PPIUD insertion, andthen those providers were expected to cascadetraining to other staff after returning to their hos-pital. Master trainers were accredited by theTanzania Ministry of Health and Social Welfare.All providers eligible to insert IUDswere to receivetraining, and refresher trainings were to be con-ducted as needed. Three days of training werededicated to counseling, and 3 days to insertion.During the 6-day training period, providers re-ceived a daily allowance of the equivalent toUS$55 to cover the cost of lodging and meals.
During counseling training, trainers presenteddetailed information on all available methods in-cluding PPIUD. Providers were encouraged toshare their opinions on PPIUD so that underlyingprejudices could be addressed.19 Training sessionswere interactive and included role-play with casescenarios of women with different family plan-ning needs. Staff were encouraged to use learningaids (leaflets, posters, flipcharts, and videos) to en-hance PPFP counseling sessions.
Providers at satellite clinics were trained onPPFP counseling only, but had the opportunity toobserve and perform practice insertions onMama-U models during their training. Those workingin selected tertiary/teaching hospitals receivedadditional off-site training on PPIUD insertion.Providers were trained to counsel women duringroutine ANC and at labor and delivery. Trainingcovered the benefits and side effects of PPIUD andall other methods, as outlined in Tanzania’s na-tional PPFP guidelines.20 Trainers also emphasizedthe voluntary nature of the program—that wom-en have the option to opt in or out of PPIUD inser-tion both pre- and postpartum.
PPIUD insertion and removal training includ-ed both classroom-based theoretical training andpractical sessions using the Mama-U postpartumuterus, an anatomical model intended for clinicaltraining purposes. The technique taught used thelong-handled 33 cm curved Kelly forceps to en-sure that the IUD was placed at the top of thefunduswhile the uterus is still enlarged as opposedto 24 cm tissue or sponge forceps, which do notreach the fundus and may lead to higher expul-sion rates.19 Assessment of trainee competencyfollowing PPIUD insertion training was standard-ized across countries. To achieve competency,trainees had to successfully complete a minimumof 3 peer-assessed Mama-U insertions, 2 super-vised live insertions, and 3 unsupervised liveinsertions.19
Program ImplementationWomen attending ANC at satellite clinics wereintended to receive one-on-one PPFP counseling.In accordance with national PPFP guidelinesaround informed choice,20 counselors wereexpected to deliver information about all avail-able family planning methods, including howthey work, duration of use, effectiveness, andpossible side effects. Women had the choice ofmethod, and all methods were available free ofcost. Available methods included condoms, oralcontraceptive pills, emergency contraceptives,
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 272
natural family planning methods, injectables,implants, IUDs, and voluntary surgical steriliza-tion.20 Within the range of methods described,providers emphasized the advantages of PPIUDas a safe, effective, and long-acting method.19
They were also expected to demonstrate howthe PPIUD is inserted using visual aids, bro-chures, and anatomical models. Pregnant women
who received counseling during ANC visits hadthe option to provide advance consent to PPIUDinsertion after delivery, and their medical chartswere marked with their stated decision. Thosewho opted for PPIUD in advance were referredto a tertiary/teaching facility for delivery, wheretrained providers would insert the PPIUD.Women who consented during pregnancy were
TABLE 1. Key Elements and Inputs Intended for Implementation of the PPIUD Initiative in 6 Countries
Elements and Inputs Description
Training: “Train-the-trainer” model: Training cascaded frommaster trainers to existing eligible providers at selectedhealth facilities
Counseling:� Prenatal counseling on available family planning methods with an emphasis
on PPFP using standard training methods (e.g., GATHER model)� Included information on the advantages of PPIUD� Open discussion about providers’ views of PPIUD to address any prejudices� Role play, case scenarios� Providers encouraged to use counseling aids (e.g., leaflets, posters, flipcharts,
and videos)PPIUD insertion and removal:� Theoretical (classroom-based) training and practical sessions using Mama-U
postpartum uterus models� Refresher trainings offered as needed� Regular training of new staff rotating in
Equipment and supplies � Mama-U models� Copper T IUDs� Long-handled 33 cm curved Kelly forceps
National coordination � Implementation was coordinated through national professional societies orcolleges to encourage local ownership
� National societies set up steering groups for clinical and technical guidance
Structures established to facilitate implementation � Dedicated project management team� Facility-level project coordinators� Data Safety Monitoring Committees
PPIUD counseling and insertion services delivered by trainedproviders
� Integrated within existing maternity services� Prenatal counseling on all available contraception methods with an emphasis
on PPFP, and the advantages of PPIUD as a safe, effective, and reversiblelong-acting method
� Consent forms provided during prenatal visits� Stickers placed on women’s case files to identify consenting women at
delivery� Women who did not receive prenatal counseling could be counseled during
early labor or the postnatal period to ensure insertion within 48 hours ifPPIUD was desired
Monitoring and evaluation � Data collection officers collected information on counseling, consent, PPIUD,and follow-up for women delivering in participating facilities
Abbreviations: GATHER, greet, ask, tell, help, explain, and return; IUD, intrauterine device; PPFP, postpartum family planning; PPIUD, postpartum intrauterinedevice.
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 273
asked again at the time of delivery to confirmtheir choice of PPIUD insertion, at which pointthey could refuse PPIUD without consequence.Additional counseling on other family planningmethods was available to all women. Womenwho received a PPIUD were advised to return fora follow-up visit at 6 weeks postpartum to ensureproper placement of the IUD. In some cases, IUDthreads were trimmed at follow-up if womencomplained of feeling them or reported discom-fort during intercourse.
Four levels of supervision and quality assur-ance were put into place. First, facility-level coor-dinators provided weekly supervision. Second,the AGOTAmonitoring and evaluation team con-ducted quarterly supervision visits. As part of
AGOTA’s routine monitoring, trained data collec-tion officers conducted exit interviews with allconsenting women after delivery and before dis-charge. These interviews captured data on wheth-er women received PPFP counseling, and whetherthey consented to having PPIUD inserted. Third,the Tanzania Data and Safety Monitoring Boardreviewed progress semiannually. Fourth, a steer-ing committee comprised of experienced gynecol-ogists and the national coordinators providedhigh-level oversight. Providers who had difficul-ties with their insertion technique received quar-terly refresher trainings throughout the initiative.
Key achievements of the PPIUD Initiative inTanzania are summarized in Table 2. A prospec-tive cohort study nested within Tanzania’s PPIUD
TABLE 2. PPIUD Initiative Achievements in Tanzania
Achievements
Participating hospitals, n 6
Providers trained under the PPIUD Initiative, n 827
Women counseled on family planning and PPIUD, n 21,479
Counseled during antenatal care, % 57.0
Counseled only after admission for delivery, % 43.0
Deliveries during the PPIUD Initiative period, n 91,387
Women followed up for postpartum interview, n 80,194
FIGURE 1. Provider- and Client-Level Interventions for the PPIUD Initiative
Abbreviations: AGOTA, Association of Gynecologists and Obstetricians of Tanzania; FP, family planning; IUD, intrauterine device;ob/gyn, obstetrics/gynecology; PPFP, postpartum family planning; PPIUD, postpartum intrauterine device.
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 274
Initiative reported that 5.8% of women who de-livered at project hospitals during the study periodhad a PPIUD inserted.21 Forty-three percent ofwomen with a PPIUD returned to a project-affiliated clinic for follow-up visit 4–6 weeks afterdelivery. Among them, midwives performed59% of PPIUD insertions, and clinicians per-formed 41%. PPIUD expulsion and removal rateswere 1.2% and 8.3%, respectively.21
Parent PPIUD StudyThis qualitative investigation was nested withinthe Tanzania PPIUD parent study, which evaluat-ed the causal effect of the initiative on the uptakeand subsequent continued use of PPIUD in3 countries: Nepal, Sri Lanka, and Tanzania. Thestudy in Tanzania was conducted in tertiary/teaching hospitals in 5 cities: Arusha, Dodoma,Dar es Salaam, Mbeya, and Pwani. A hospitaland 3–4 of its satellite clinics were selected ineach location (see research protocol for detailedprocedures).9
In the parent study, the PPIUD initiative hadonly a modest impact on women’s choice ofPPIUD (an increase of 6.3 percentage points) dueto low coverage of PPIUD counseling among wom-en delivering in study facilities.22 Adherence-adjusted estimates suggest that if all women hadbeen counseled as intended, we could expect a31.6 percentage point increase in choice ofPPIUD. Qualitative findings from the presentstudy are intended to contextualize these resultsby highlighting strengths and weaknesses in pro-gram implementation and potential opportuni-ties to improve future implementation of similarinterventions.
Identifying factors that influence program im-plementation is essential for assessing the fidelityof interventions and understanding why theywere or were not effective. For example, negativeresults can occur when interventions are not imple-mented sufficiently, and similarly, positive resultscan be achieved by an intervention that wasdelivered differently than intended.23 Therefore,understanding what contributes to implementationsuccess or failure is critical to program improvement,replication, and scale-up across settings.
METHODSStudy Design and Data Collection ProceduresOne objective of the evaluation was to understandhow the initiative was implemented, the perspec-tives of providers on implementation, and recep-tiveness of women toward PPIUD services. In the
present study, we conducted qualitative in-depthinterviews (IDIs) with providers and women whoparticipated in the initiative to assess the imple-mentation barriers and facilitators.
The consolidated criteria for reporting quali-tative research (COREQ) was used to ensurecomplete reporting of qualitative procedures(Supplement 1). Sample sizes for IDIs were esti-mated based on what would be sufficient toachieve saturation in themes and study aims.24
Authors recruited and trained 2 female Tanzanianinterviewers, who were hired as independent con-sultants. The interviewers each had bachelor’sdegrees in sociology andmore than 10 years’ expe-rience conducting qualitative interviews. Authorsoriented the interviewers on study proceduresincluding the ethical considerations, informedconsent process, and interview guides, as well asoversaw piloting and data collection. The inter-viewers had no prior relationship to study partici-pants, and participants had no prior knowledge ofany research teammembers.
We conducted IDIs with 15 providers betweenJune 2016 and February 2017, approximately3 months after they received PPIUD training, tounderstand their experiences with the trainingand perceived facilitators and barriers to imple-mentation. We purposively selected 2–4 providersfrom each hospital who had participated in thetraining and were actively delivering the initia-tive. Researchers contacted providers by phoneto inform them about the interviews, briefly ex-plain the purpose of the interviews, and requestparticipation.
We conducted IDIs with 47 women exposed tothe initiative to understand their experiences withPPFP counseling, and their decision making re-garding postpartum contraceptive use. BetweenJune 2016 and February 2017, we conducted IDIswith 20 pregnant women who had at least 2 ANCvisits in a study facility, received PPFP counseling,and were offered PPIUD insertion. From each site,we purposively sampled 4 pregnant women to in-clude a mix of women from higher- and lower-income levels and range of ages. Eligible womenwere initially approached by providers at the endof their ANC appointment to inform them aboutthe study. Women who were interested to learnmore were referred to the research team. Inter-viewers assessed women’s eligibility independentof providers, explained the purpose of the study,administered informed consent, and conductedprivate one-on-one interviews after an ANC visit.
Between April 2018 and August 2018, weinterviewed a separate sample of 27 postpartum
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 275
women who had received a PPIUD. The parentstudy collected data on whether women contin-ued using the PPIUD, discontinued due toexpulsion, or intentionally discontinued beforethe qualitative interviews. We aimed to recruit10 women from each of these groups; however,the number of women who experienced expul-sion was small (1.2% in the parent study), thuswe were only able to recruit 7 women. Thesewomen were randomly selected for interviewsfrom the parent study database, which includeddetailed contact information for enrolled women.Researchers contacted women by phone to informthem about the qualitative interviews, briefly ex-plain the purpose of the interviews, and requestparticipation.
We developed semistructured interview guideswith open-ended questions in English and translat-ed them into Swahili. The interview guide forproviders covered the following topics: knowledge,experiences, and preferences for contraceptivemethods; PPIUD training experience; and imple-mentation, scale-up, and diffusion of PPIUDservices. Interview guides for women includedquestions to assess contraceptive knowledge andprior use, as well as their experiences and percep-tions of PPFP counseling and postpartum contra-ceptive decision making. For postpartum womenwho received a PPIUD, the guide included ques-tions regarding their experience with the PPIUDInitiative, including content and perceived qualityof PPFP counseling. We also asked questions abouttheir experiences using the PPIUD, including rea-sons for continuation or discontinuation. Tanzanianresearchers verified translations and back-translatedthe guides to ensure content and semantic equiva-lence of each question.25 We pretested interviewguides to assess question phrasing, sequencing, andoverall comprehension and modified the guides asappropriate.
Before each interview, participants were askedto providewritten consent to take part in the study.Women who were unable to sign their names pro-vided a thumbprint alongwith awitness’ signature.All providers gave a signature. One-on-one inter-views were conducted in Swahili, and in a privatespace at the facilities or another private location ifparticipants preferred. Interviewers made fieldnotes during interviews that were used duringtranscription/translation to add contextual details.Interviews were audiorecorded with participants’permission and subsequently transcribed and tran-slated to English for analysis. Interviews lastedbetween 60 to 90 minutes. No one refused to par-ticipate in the study.
Ethics Approval and Consent to ParticipateEthical approval as exempt was granted by theInstitutional Review Board at Harvard University.The study received ethical approval from theNational Health Research Ethics Review Com-mittee of the National Institute of MedicalResearch in Tanzania. The consent statement in-cluded the purpose of the study, confidentiality ofpersonal information, and the use of informationfor publication. Only those who consented wereinterviewed.
Analytical StrategyWe used ATLAS.ti (Version 8.0) to manage, code,and interpret transcripts using thematic contentanalysis. We applied a multistage analytical strate-gy to identify key themes, codes, and subcodes.26
In the first stage, we prepared an initial list of par-ent codes and definitions based on study aims, in-terview guides, and existing literature on PPFP.Examples of parent codes include: counseling im-plementation, IUD, other family planning meth-ods, decision making, and quality of services. Weapplied these high-level codes to group the datain our first pass through the transcripts.26 Duringthis process, we identified relevant subcodes un-der each parent code. For example, under the“counseling implementation” code, we added thefollowing subcodes: client receptiveness, counsel-ing frequency, counseling content, counselingprovider, and counseling timing. Under “decisionmaking” we identified the following subcodes:support, trust, method choice influence, discon-tinuation, fertility limit, fertility space, fertilitycontinue, coercion, and trade-offs. We developeda preliminary codebook, which included both pre-determined and emergent codes. Next, we dividedthe transcripts between researchers and indepen-dently coded line-by-line using the codebook. Wewrote analyticalmemos to summarize case details,highlighting particularly rich narratives and emer-gent themes. We reviewed each other’s codingand came to agreement on categories and themesto ensure analytical rigor and consistency acrosstranscripts.26
In the final stage, we analyzed the codedtranscripts using 2 theoretical frameworks (de-scribed later) to answer the following questions:(1) What were the barriers to, and facilitators of,PPIUD implementation? and (2) At what level dideach of these barriers and facilitators operate? Todo this, we sorted coded sections of the transcriptsinto “bins” that correspond to elements of eachframework. This process was done manually in
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 276
Microsoft Excel to enable visualization of thesorted data in a matrix. We then analyzed all thequotes within each element/level of the frame-works to further categorize them into barriers orfacilitators.
Theoretical FrameworksTo gain insight into the successes and challenges ofthe PPIUD Initiative’s implementation, we appliedthe implementation outcomes framework devel-oped by Proctor and colleagues.27 The frameworkdifferentiates between 3 “distinct but interrelated”sets of outcomes: implementation, service, and cli-ent outcomes. Implementation outcomes are de-fined as27:
the effects of deliberate and purposive actions to implementnew treatments, practices, and services, . . .which . . . serveas necessary preconditions for attaining subsequentdesired changes in clinical or service outcomesdownstream.
Figure 2 shows a visual representation of theframework developed by Proctor et al. Applica-tion of this framework helps advance our theoret-ical understanding of the implementation processof the PPIUD Initiative in Tanzania and evaluatethe drivers of successful implementation usingcommon nomenclature and a systematic analyti-cal approach.
In conjunction with the implementation out-comes framework, we used an ecological frame-work adapted by the United States Agency forInternational Development’s Maternal and ChildHealth Integrated Program for PPFP,28 to catego-rize factors influencing implementation into 5 dif-ferent levels: individual (woman), partner/family,
health system, community, and policy. Imple-mentation of novel interventions is intrinsicallymultifaceted, thus it is important to measure out-comes at different levels to understand areas ofsuccess and failure and potential opportunities forimprovement. Yet, few studies specify the leveland rarely address how different levels relate toone another.27 Thus, the ecological framework isa useful tool to guide our assessment of this PPFPinitiative by highlighting the contextual, healthsystem, and policy-level factors that influencedimplementation.
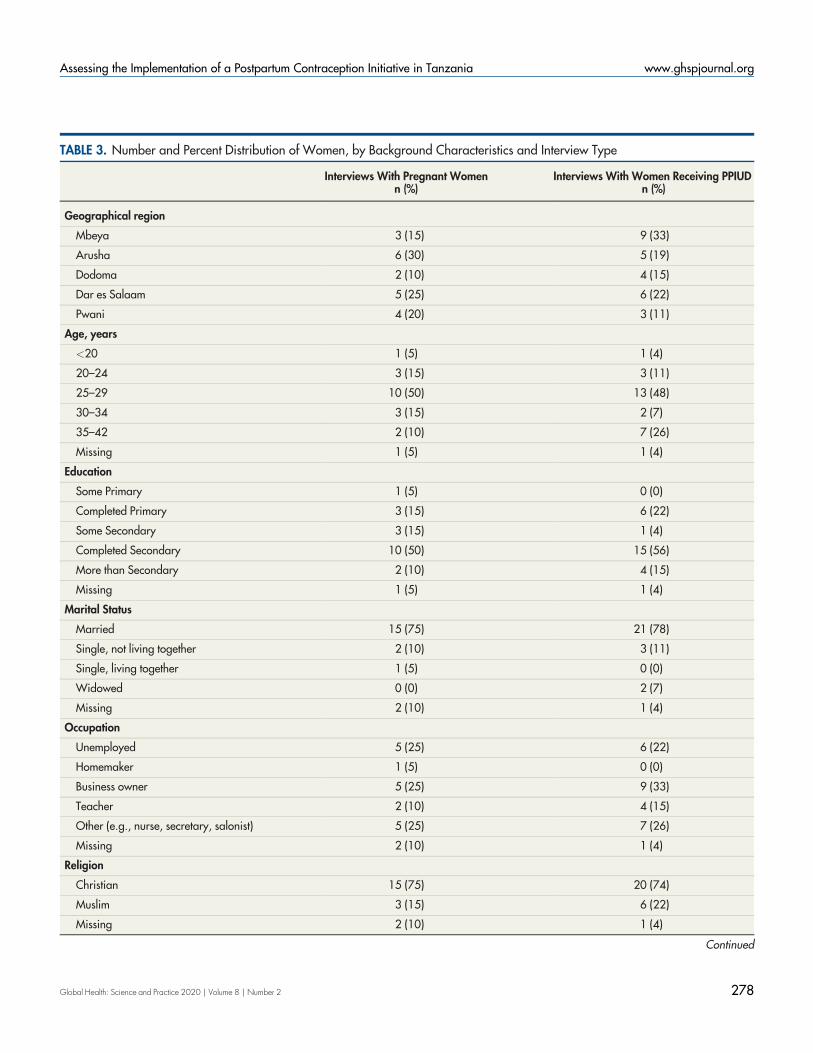
RESULTSDemographic characteristics of women and provi-ders are summarized in Tables 3 and 4. Analyzingtranscripts using the 2 frameworks describedrevealed a number of factors that influencedPPIUD implementation. In Figure 3, we summa-rize findings by level in the ecological frameworkand include these summaries in the descriptorboxes for each level. In the text that follows, weapply the Proctor framework to categorize thesefactors as barriers and facilitators under imple-mentation outcomes, service outcomes, and clientoutcomes (Table 5).27 Illustrative quotes are in-cluded in the text, and additional quotes are inSupplement 2. We did not find any meaningfuldifferences in women’s perceptions of how the in-tervention was implemented by age, sociodemo-graphic status, or location.
Implementation OutcomesAcceptabilityAcceptability refers to the perception among im-plementation stakeholders that an intervention is
FIGURE 2. Visual Representation of the Implementation Outcomes Framework27
aInstitute of Medicine standards of care.
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 277
“agreeable, palatable, or satisfactory” and can beassessed qualitatively based on individuals’ opin-ions of the intervention’s content, complexity, orcomfort.27 We identified a majority of these fac-tors at the health system level.
Facilitators. The most important facilitator ofintervention acceptability at the health systemlevel was high satisfactionwith the PPIUD trainingamong providers. Providers were highly contentwith the training in terms of the content covered,complexity of information provided, and comfortin implementing the skills they learned. One par-ticipant articulated this particularly clearly, andmost providers shared these views:
Implementation was good . . . I can say motivation washigh because of the way training was conducted. Itequipped people with knowledge and each personcame out feeling that she is capable of doing PPIUDinsertion.—Provider
Barriers.Bothwomen and providers reportedthat too few staff were trained specifically on IUDinsertion. The limited number of trained inserterswas perceived as a missed opportunity, creatingadditional barriers for women seeking PPFP ser-vices. For example, some women consented toPPIUD insertion during ANC but failed to havethe method inserted due to lack of availabletrained providers:
More providers should be trained on PPIUDinsertion . . . a woman that I advised to get the PPIUD -when she went to the hospital, the health provider whocould provide the service was not around that day.Manywomen may be discouraged if they experience this. For abetter service, we need providers that can give the ser-vices whenever needed.—Woman, postpartum
One provider who was trained only on PPFPcounseling expressed a desire for additional train-ing on insertion.
A policy-level barrier to implementation was alack of support from local health authorities.According to a provider, the district reproductiveand child health coordinator imposed administra-tive hurdles to timely implementation, noting thatit was difficult to convince the coordinator of theintervention’s value, which, in turn, delayed theprocess of obtaining the necessary equipment intime. This suggests that while acceptability washigh among training recipients, it was loweramong administrative authorities who played akey role in implementation.
AdoptionAdoption is defined as a provider’s “intention,initial decision, or action to try or employ” anintervention.27
Facilitators. Increased confidence amongproviders following the PPIUD training was a keyfacilitator of adoption. Although some providersfelt the training could be longer, almost all claimedthat they left the training with new knowledge.Many reported increased confidence in their abili-ty to offer family planning counseling and educa-tion because of the training received:
I was not competent with family planning [prior to thetraining], but I was able to learn about the other meth-ods too because we were taught briefly [about all meth-ods] during the training. I came out feeling that I amcapable of caring for a woman and all challenges thatmay come up, and all the misconceptions related toIUD.—Provider
Barriers. A commonly cited barrier to PPIUDcounseling adoption was time constraints amongalready overburdened staff. Despite their satisfac-tion with training content, some counselors hadinsufficient time to implement what they hadlearned.
TABLE 3. Continued
Interviews With Pregnant Women Interviews With Women Receiving PPIUDn (%) n (%)
Time constraints were compounded by short-ages in facility staff, and as a result, PPFP counsel-ing was often deprioritized or adaptions weremade to ease provider workload. Time constraintswere particularly problematic when women re-ceived PPFP counseling at the time of hospital ad-mission before delivery, which may have led torushed and/or incomplete counseling. To copewith time constraints at the time of delivery, a pro-vider described a process of triaging patients forPPFP counseling based on previous exposure toinformation. If a woman received PPFP counselingduring pregnancy, then providers streamlined thetopics discussed:
Due to time limitations, you ask a woman if she has everreceived any counseling previously. If yes, then you onlyfocus on the key points because we know she has receivedinformation from the antenatal clinic. So we emphasizethe advantages of birth control, minor side effects andtheir symptoms.—Provider
Providers also described gaps in the referralsystem between satellite clinics and larger referralhospitals. Within this system, PPIUD insertionproviders relied on satellite clinic nurses to pro-vide high quality PPFP counseling, make appro-priate referrals, and provide timely follow-upcare, which was not always implemented asintended:
We often say tragedies that occur in the referral hospitalsare caused by facilities at the lower level. . . . This isdue to the nurse’s carelessness, perhaps not doingtheir job well. If people don’t get proper counselingat the clinic, we will end up having problems here (atthe hospital).—Provider
Although the PPIUD referral system wasintended to streamline project implementation,several hospital-based providers felt there was lim-ited oversight of providers in smaller clinics. Oneprovider was particularly concerned about 6-weekfollow-up procedures, in which women were ad-vised to return to the hospital to have the IUDplacement checked and threads shortened if neces-sary. According to a provider, if a client returned toa facility that was unable to provide quality follow-up care, then she may have had a negative experi-ence and discouraged others from adopting PPIUD.
FidelityFidelity is the degree to which an interventionwas implemented as initially intended by design.Providers described several adaptations to theintended PPIUD intervention, primarily in re-sponse to barriers related to adoption.
Barriers. To cope with time and staff short-ages, providers invited pregnant women to attendscheduled group PPFP counseling sessions ratherthan the intended one-on-one counseling duringANC visits. Shifting to group counseling helped toreduce the burden on busy providers, but socialdynamics between older and younger womenmay have influenced some women’s willingnessto fully participate:
Although counseling women as a group is good, I thinkthere is also a need to have individual sessions where awoman can ask [her own] questions. Some women, es-pecially those who are old like me, may fail to ask
TABLE 4. Number and Percent Distribution ofProviders by Background Characteristics
Characteristic n (%)
Geographical Region
Mbeya 4 (27)
Arusha 4 (27)
Dodoma 2 (13)
Dar es Salaam 2 (13)
Pwani 3 (20)
Gender
Male 2 (13)
Female 13 (87)
Age
29–39 7 (47)
40–50 4 (27)
>50 2 (13)
Missing 2 (13)
Profession
Physician 3 (20)
Nurse 12 (80)
Length working in profession, years
≥5 5 (33)
6–15 4 (27)
≥16 3 (20)
Missing 3 (20)
Length providing family planning services, years
≥5 5 (33)
6–10 7 (47)
≥11 1 (7)
Missing 2 (13)
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 280
questions when they are in a group of young women,some of whom are teenagers.—Woman, postpartum
Although providers considered group familyplanning counseling to be an effective time man-agement strategy, they also acknowledged that itwas difficult for some women to attend at thespecified times due to competing householddemands. Since it was not feasible for providers todeliver comprehensive one-on-one counselingthroughout the day, women who were unable toattend group sessions or who arrived late wouldmiss counseling completely; a deviation from theintended intervention. This challenge was linkedto diminished motivation, rushed counseling,and/or missed counseling opportunities:
The nurses are overwhelmed and tired. There are daysthat you go to the clinic to get services, but you leavewithout getting educated or counseled on anything. Yet,when women gather at the clinic that is the bestplatform to explain about the methods for familyplanning . . . When the woman goes back home, shewill appreciate that she has learned something andwhen she delivers, she will have already decided onwhich family planning method to use.—Woman,postpartum
Lastly, counselors were trained to counsel onall available methods to enable informed choiceand ensure that women understand the full range
of PPFP options, including their benefits and po-tential side effects. However, women’s narrativesdemonstrated that PPFP counseling was highlyskewed toward PPIUD, and some may have re-ceived incomplete information (or could only re-call partial information) on the possible physicalside effects of the PPIUD. This suggests a lack of fi-delity to the training delivered.
[The nurses] told us it works for 10 to 12 years’ time andcan be inserted just after delivery . . . and you may re-move it at any time. And this method has no side effectsunlike implants, which may cause long term bleeding orlack of menstruation at all. But these new methods, youwill still have yourmenstrual cycle as usual and have noside effects. Unpleasant effects can occur for the first3 months but not longer. –Woman, prenatal
PenetrationProctor et al. define penetration as the “integra-tion of a practice within a service setting and itssubsystems.”27 Penetration is closely related tothe concept of “diffusion” and is typically mea-sured quantitatively; however, qualitative analy-sis revealed important insights into how theinitiative could be better integrated into existingservice delivery environments. Here, we considerpenetration to include diffusion of the initiativeboth within participating intervention facilities
FIGURE 3. Ecological Framework Illustrating Factors That Influenced Implementation of the PPIUD Initiative in Tanzania
Abbreviations: PPFP, postpartum family planning; PPIUD, postpartum intrauterine device.
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 281
TABLE 5. Application of the Implementation Outcomes Framework to Assess Facilitators and Barriers to PPIUD InitiativeImplementation in Tanzania
Outcome and Definition Facilitator Barrier
Implementation Outcomes
Acceptability: Perception among stake-holders that intervention is acceptable (e.g.,satisfaction with PPIUD training content,complexity, comfort)
� High satisfaction with PPIUD training � Lack of providers trained on PPIUD insertion� Lack of support from local health authorities
Adoption: Initial implementation of PPFPcounseling and PPIUD insertion; Intention totry
� Increased confidence following PPIUDtraining
� Time constraints and inadequate staffing� Gaps in referral system between satellite clinics
and hospitals
Fidelity: Delivered counseling as intended(e.g., reach, content, and targetpopulation)
� Individual counseling replaced by groupcounseling
� Diminished provider motivation� Counseling rushed or skipped� Skewed or incomplete counseling
Penetration: Diffusion of PPIUD Initiativewithin intervention facilities and to othernon-intervention sites
� Emphasis on PPIUD’s mechanism ofpregnancy prevention during training
� Objections from faith-based facilities� Expectation for remuneration among staff who
did not receive initial training
Sustainability: Long-term maintenance andinstitutionalization of the PPIUD Initiative
� Support for population policies andfamily planning programs to achievefertility reduction goals
� Breakdown of supply chain and stock-outs
Service Outcomes
Equity: Extent to which the PPIUDimplementation is equally available/accessible to all intended beneficiaries
� Differential treatment by health care providers� Financial barriers to accessing hospitals� Lack of community-based PPFP counseling and
services
Client Outcomes
Client receptiveness/demand for services:Client receptiveness to being counseled onPPFP and/or demand for receiving thePPIUD
� Level of support from husband/partner� Shared intention among couples to
space pregnancy for financial reasons� Community and gender norms related to
birth spacing� Community diffusion of preference for
PPIUD and peer recommendation� Women's trust in provider advice� Cost-free counseling and insertion
services
� Fear of insertion, concerns related to sexualexperiences postinsertion, unexpectedexpulsion and experience of unanticipatedside effects (results published elsewhere26).
Satisfaction with PPIUD services:Client receptiveness to being counseled onPPFP and/or receiving PPIUD; Satisfactionwith counseling and services
� Delivery of counseling and services byfemale provider
� Interpersonal aspects of care
� Perceived provider incompetence
Abbreviations: PPIUD, postpartum intrauterine device; PPFP, postpartum family planning.
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 282
and to other local facilities not selected for thePPIUD Initiative.
Facilitators. When service providers reflectedon the potential for diffusion of the initiative toother facilities, they identified a number of factorsoperating at the health system level. One providerexplained that receiving focused training on thePPIUD’s mechanism of action clarified theirmisconceptions about how PPIUD functions andrelieved moral concerns about providing themethod:
I heard from Catholics that using loops is killing chil-dren and you are killing every month, so that thinkingaffected me . . . Well according to the training it is nottrue . . . [Prior to PPIUD training] when I was advisingthe woman about the methods, afterwards I regrettedthat, thinking, “my God, I might have killed” . . . I per-sonally don’t have any obstacles now, even if I go back tothe Roman Catholic [facility] where I studied, I will ed-ucate them about the [PPIUD].––Provider
Barriers. The most common potential barrierto diffusion was that faith-based facilities wouldobject to implementing PPIUD services. Conse-quently, both women and providers believed thata PPIUD intervention would only be effective andsustainable in government facilities. Anotherhealth system-level barrier was the expectationfor remuneration among other staff who did notattend the off-site training. Providers explainedthat diffusion of information and learnings toother colleagues could be a challenge becausePPIUD training participants received an allow-ance. Consequently, other staff may perceive thisarrangement to be unfair. Despite this challenge,some staff were reportedly open to learning, with-out expectations of rewards. This was dependenton the workplace culture of specific facilities:
There are some who received it well. At this facility, wehave a norm that if you go to a training, when you comeback you have to provide feedback. So when you’re onshift and you have some time, you can instruct and teachothers what you learned [. . .] but not all staff do this be-cause some may complain, saying, “You got the moneyand now you come back with just words.” ––Provider
SustainabilityIntervention sustainability is the extent to which anewly implemented intervention is “maintainedor institutionalizedwithin a service setting’s ongo-ing, stable operations.”27 Penetration and sustain-ability are conceptually similar, but temporallydistinct, as higher penetration typically contri-butes to long-term sustainability.
Facilitators. Most health care providers be-lieved there was strong political will among gov-ernment officials to invest in strategies that wouldachieve fertility reduction goals. This was viewedas a policy-level facilitator of PPIUD sustainabilitybeyond the life of the project:
I don’t see any reasonwhy it would fail because we havea problem of high population, and we have an interven-tion that can reduce this population growth rate, so whycan’t the government support this? . . . If they are able tosupply other services then why not this as well . . . it’s anational priority, and it is in the sustainable develop-ment goals! ––Provider
Barriers. A key driver of successful institu-tionalization at the health system level was havingthe necessary instruments and equipment readilystocked and available, which requires supportfrom and coordinationwithMinistry of Health au-thorities. At the time of the study, AGOTA sup-plied PPIUD equipment at no charge. Manyrespondents expressed frustration with the short-age of PPIUD equipment and supplies, and, asmore women learned about the PPIUD Initiative,equipment shortages became increasingly prob-lematic. Despite an increased influx of patients,there was no equivalent increase in equipmentand supplies to meet the heightened demand.Providers felt strongly that even if other govern-ment facilities agreed to provide PPIUD services,the inconsistent provision of supplies would beproblematic. This raised questions about the long-term sustainability of the intervention withoutAGOTA support:
To be honest, it will be difficult to supply the instrumentsto other facilities. . . that is not easy, and it may take along time because for now, our facility is supplied bydonors. That’s why it’s possible. But with the govern-ment, you may write a request for the material until allthe ink in that pen is gone, and still not get what youasked for! ––Provider
Service OutcomesEquity
Barriers. Equity was themain service outcomeconstruct to emerge from IDIs. At the health sys-tem level, a key barrier to equitable PPFP counsel-ing was differential treatment by health careproviders. One woman suggested that adolescentsare reluctant to seek family planning counselingout of fear of judgment by health care providers.In addition, some providers reportedly prioritizedwomen who attended antenatal clinics with their
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 283
husbands, whereas those who attended alonewaited longer for services:
They would prioritize women who came with theirhusbands. It did not matter whether you were therefirst, they would ask those who came with theirhusbands to go in for the services first [. . .] In mostcases, my husband is always with me because he knowswhen you go to the clinic with a man, you will be givenpriority. ––Woman, postpartum
These reports indicate a lack of fidelity to theintervention, as providers were trained to counselall ANC clients and to tailor contraceptive methodrecommendations according to women’s individ-ual needs regardless of age or marital status.
Another barrier to equitable service deliverywas the cost of accessing large hospitals. One pro-vider stated that lower incomewomen have a ten-dency to deliver at peripheral facilities becausethey are less busy, closer to home, and less costlyto access. Transportation to large hospitals for de-livery or PPIUD services may not be feasible forwomen with fewer resources:
Another challenge is women’s economic status. Somegive birth here (at the health center) for free, but whenyou ask her to take a [USD$0.86] bajaji (motorized rick-shaw) to [the hospital], she can’t manage it, so we feelthat we are going to lose them . . . and the providers there(at the hospital) are overloaded, so women are scared.They prefer to get the delivery services here . . . the hospi-tal is very busy. ––Provider
Lastly, although the PPIUD Initiative wasdesigned for implementation only at the facilitylevel, both women and providers viewed the lackof community-based PPFP counseling as a missedopportunity for equitable service delivery:
We should also get out of this hospital and educatepeople in the village because problems are not only intown. Amajority who face challenges are in the villages,in our districts . . . we have to go there and trainpeople. ––Provider
Client OutcomesClient Receptiveness and Demand for ServicesAlthough women’s receptiveness was not includ-ed in the original implementation outcomesframework, we consider it an important addition,as factors motivating or discouraging engagementwith the intervention may directly influence bothimplementation and PPIUD uptake.
Facilitators. Women identified several facili-tators of PPIUD uptake at the partner/family level.
In addition to feeling supported by health careproviders, several women highlighted the impor-tant role of their husbands in supporting their de-cision to use PPIUD. Another motivator to usePPIUD was a shared intention among couples tospace pregnancy for financial reasons:
Depending on my business and the way I planned withmy husband, I know that if I use the loop, there are somethings we will be able to accomplish before getting preg-nant again. ––Woman
At the community level, 2 important factorsfacilitated women’s receptiveness to PPFP coun-seling and PPIUD services. The first was communi-ty norms around preference for long birth spacing.When asked to explain why she felt it was impor-tant to prevent pregnancy soon after birth, awom-an described the shame and stigma associatedwithshort birth spacing:
First, it’s because the baby will still be very young, [and]second, I feel shame when I am in the community,getting pregnant when the baby is only about 4 or5 months old; it’s a shameful thing! [. . .] If you happento get pregnant [again], they tend to put all the weighton women, like, “how did you let yourself get preg-nant?” He won’t abandon you, but he will put all theblame on you, saying that you did it on purpose. ––Woman, prenatal
Second, the presence of women who hadpositive experiences using PPIUD was a criticalcommunity-level facilitator of PPIUD counselingand service uptake. Participants described a com-munity diffusion effect in which nonusers wereencouraged by “positive deviants”––peers whohad opted for the PPIUD and could speak fromfirsthand experience:
At some point I was acting like an ambassador for theIUD because many women would come to me; they feltthat I understood more. Even the health service provi-ders would tell women to [talk to me] and I would sharewith them what the IUD was all about. Many womenquestioned how the PPIUD could be inserted immediate-ly after delivery. They thought it was impossible. ––Woman, postpartum
Despite the strong influence of their peers andneighbors, women were generally receptive tobiomedical information and the advice providedby medical professionals, and most were likely toshow interest in the PPIUD if providers demon-strated their own approval of the method.
At the policy level, the most important facilita-tor of PPIUD uptake was the availability of cost-
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 284
free insertion services. Despite Tanzania’s policy toprovide free health services for pregnant womenand users of family planning services, some wom-en were not aware that PPIUD and other contra-ceptive methods were available free of cost. As aprovider noted, informing women of this policyinfluenced their decision to choose the method.
Barriers. We identified several important bar-riers to PPIUD demand at multiple levels. Manyindividual-level factors influenced women’s deci-sions to use PPIUD, which we have reported else-where in depth.29 These included fear of insertion,concerns related to sexual experiences postinser-tion, unexpected expulsion, and experience of un-anticipated side effects.
SatisfactionFacilitators. At the health system level,
women’s PPFP counseling experience influencedtheir overall satisfaction with PPFP services.These included the use of counseling aids duringprenatal counseling (leaflets, waiting roomvideos,and brochures), and most importantly, having ac-cess to female family planning service providers.Women were generally more satisfied with careand more motivated to use PPIUD when coun-seled by female nurses who could speak to theirpersonal experience using family planning.Women also appreciated providers who were re-spectful, compassionate, and patient, indicatingthat interpersonal aspects of care are a valuedcomponent of PPFP services:
I am very grateful to them [providers] because they gaveme all the support I needed. They were ready to answermy questions even before I started using the PPIUD,when I had it and when I went to remove it . . . Theyhave really been supportive, even after removingthe PPIUD . . . calling to ask if I was doing fine andif I needed any assistance with family planningmethods. ––Woman, postpartum
Barriers. Although most providers reportedhigh confidence in their technical skills after train-ing, some women reported contrasting percep-tions of providers’ clinical skills. Several womenperceived technical incompetence as a primarycontributor to adverse PPIUD outcomes, inclu-ding expulsion and/or improper placement, andwarned that such negative experiences might de-ter future patients from using PPIUD:
The person that inserted the PPIUD for me did not insertit well. She struggled very much, and it was like a trialand error thing . . . It was very painful because I had justgiven birth. When I got home, the PPIUD was expelled
. . . The providers giving PPIUD services should betrained [on insertion] and should only be allowed toprovide that service when they are competent; otherwise,many women run away from using the IUD. ––
Woman, postpartum
DISCUSSIONThis study applied 2 theory-based frameworks toassess the implementation of a postpartum contra-ception intervention in 5 Tanzanian hospitals.Applying a PPFP ecological framework to analyzequalitative IDIs demonstrated that successful im-plementation and uptake of PPIUD counselingand services depends on a complex interplay offactors operating at multiple levels, spanningfrom the individual (woman) level to the policylevel. In addition, using the implementationoutcomes framework informs our theoretical un-derstanding of the implementation process, illu-minating the “black box” of implementationdynamics, and highlights potential entry pointsfor improvement in program delivery.27
Overall, acceptability of the PPIUD Initiativewas high. However, providers perceived the selec-tive training of some staff only on PPFP counsel-ing, and others on both PPFP counseling andPPIUD insertion to be inequitable, which mayhave led to demotivation. The extent to whichclinic staff are both “intrinsically” and “externally”motivated, valued, and supported in their profes-sional roles directly influences program imple-mentation.30,31 Previous research on promotionof IUD uptake in LMICs found that provider en-thusiasm is a critical driver of implementation suc-cess.18 As such, providing remuneration only toproviders participating in the off-site AGOTA-hosted trainings may have weakened possibleopportunities of diffusion to other facility staff.AGOTA and FIGO believed the payments werejustified given that some providers worked addi-tional hours to support the initiative; however,this may have disincentivized employees whoroutinely work additional hours for other tasks.19
Further, ongoing payment is not sustainable,19 es-pecially given that this intervention was imple-mented in a low-resource context.
There were many health system-level barriersto optimal implementation, including supplychain issues, gaps in referral between satelliteclinics and tertiary/teaching hospitals, inadequatestaffing and supplies, and overworked providers.A common narrative to emerge from both provi-ders and women is that the existing health system
infrastructure is fragile and any additional demandsplace further burden on providers. Consequently,the potential of any facility-based PPFP interven-tion is limited if existing health systems shortfallsare not addressed first. These findings are consistentwith previous studies in Tanzania, which report ir-regularities in staffing, supplies and equipment,work overload, and communication challenges be-tween facilities as barriers to implementation ofmaternal and newborn care.16,30,32–34
Further, although there was high acceptanceof the initiative, and providers repeatedly echoedthe importance of PPFP on women’s health andwell-being, they also perceived contraceptivecounseling as a time-intensive endeavor, particu-larly when added onto routine ANC protocols.The perceived characteristics of an interventioncan drive the adoption process, mediating the in-fluence of intention to implement the programand actual behaviors to do so.35 A comprehensiveneeds assessment to evaluate feasibility and iden-tify potential adaptations for the local context isrecommended. For example, an audit of satelliteclinics to assess providers’ current duties, work-load, and willingness to take on additional tasksmay have helped to identify clinics with more ca-pacity to implement new initiatives.
Paradoxically, if an intervention leads to in-creased demand for services (as providers reportedfor PPIUD), this may diminish the quality of careprovided in the long run if strategies to facilitatethe increased workload are not in place. Anotherstudy in Tanzania found that unpredictable fluxesin uptake of maternal and newborn care createdchallenges for service delivery and directly influ-enced the quality of care provided.16 Althoughstreamlining health care provision by integratingservices (ANC and PPFP counseling, for example)is often promoted to improve health system effi-ciencies,36,37 such integration must be matchedwith proportional increases in staffing, training,and supplies. A scoping review of integration ofHIV and sexual and reproductive health servicessimilarly cautions that integration of maternaland reproductive health services must be judi-ciously planned in relation to current health sys-tems functions.38
Providers reportedly adapted to health systemconstraints by implementing scheduled group-based PPIUD counseling sessions for womenattending ANC clinics. Their intention was to im-prove efficiency and reduce the burden of addi-tional one-on-one counseling (as intended by thePPIUD Initiative). Although group-based PPFPcounseling was a deviation from the intervention
design, this modality has been successfully imple-mented in LMICs for other reproductive healthissues,39–42 and may be warranted, particularly inresource-constrained settings. However, severalproviders indicated that in practice, some womenwere unable to attend the early morning groupsessions and missed the opportunity for prenatalPPFP counseling. Additionally, some women hadreservations about discussing PPFP in a group set-ting due to age-related social dynamics. Given thatwomen seeking ANC are not a homogenousgroup, implementation of the PPIUD Initiativemay have been strengthened if group sessionswere stratified by age, parity, marital status, oreducation.
Group- versus individual-based PPFP counsel-ingmay produce different results, and themode ofcounseling delivery likely influences the effective-ness of PPFP programs. Research from NorthernTanzania found that while PPFP counseling deliv-ered alongside routine prenatal HIV-testing hadan effect on postpartum contraceptive intentions,intentions were poor predictors of postpartum re-productive behavior.43 Taken together, results callfor additional investigation of various integrationmodels to determine the optimal timing and modeof PPFP counseling. Implementers might considersupplementing one-on-one PPFP counseling withgroup education opportunities to ease the burdenon providers. However, these groups should bedesigned with social dynamics in mind to ensurethat women feel comfortable to speak freely.
The PPIUD Initiative intended to serve womenof all ages and socioeconomic status, and providerswere expected to deliver comprehensive PPFPcounseling covering all available methods. How-ever, findings suggest that interpersonal aspectsof care varied, with somewomen reporting rushedor incomplete counseling or an emphasis on thePPIUD over other methods. Further, the percep-tion that some providers treated older womenand/or those accompanied by their husbandsmore favorably during ANC suggests that fidelityto the intended PPIUD Initiative was not uniform-ly achieved. This finding aligns with a previousstudy in Tanzania in which adolescent mothersfelt stigmatized by health care providers duringANC due to early pregnancy and childbearing.44
Such practices may reflect widely held sociocul-tural norms, and/or broader efforts to encouragemale involvement in reproductive health,45 butmay lead to unintended consequences in the longrun. If unmarried and adolescent women (whoaremore likely to have unmet need for contracep-tion) perceive differential treatment by health
care providers, they may be discouraged fromseeking future care. Women are also likely to dis-cuss these experiences with peers, and a generalmistrust of providers and/or reluctance to seekcare may diffuse among communities. Unless eq-uitable, high-quality care is delivered, these socialdiffusion dynamics will ultimately threaten thelong-term sustainability of PPFP interventions.
Narratives suggest that women in our studywere strongly influenced by their peers. Onewoman viewed herself as an “ambassador for theIUD” and took great pride in sharing her experi-ence with others. Future initiatives could considerengaging women with positive experiences tohelp facilitate diffusion of information to theirpeers, both within the community and at facilities.This may be particularly useful in facilities whereproviders are overburdened.
Although women’s receptiveness to PPIUDservices was strongly influenced by the experienceof their peers, the perspectives of female providerswere highly valued, primarily due to their abilityto empathize with clients. This represents an im-portant opportunity for intervention. However,women’s perceptions regarding differential treat-ment have concerning implications for long-termsustainability. Additional training and supervisionto improve interpersonal aspects of care, includingan emphasis on patient-centered counseling, in-formed choice, and respectful and nondiscrimina-tory service delivery should be integrated intofuture PPFP initiatives.
Narratives suggest that it is less feasible forwomen of lower socioeconomic status to deliverin tertiary teaching hospitals, despite referral tothese facilities for PPIUD. Both delivery andPPIUD services were free of cost, but somewomenexpressed concerns about distance, cost of trans-port, unfamiliarity with staff, and overcrowdingin hospitals. This suggests that the PPIUDInitiative may unintentionally give privilege towomen with greater financial means and thosewho may be more motivated to complete thePPIUD referral and deliver at tertiary hospitals.Although the initiative’s referral system wasintended to streamline service delivery, the inter-vention does not address the barriers women en-counter when attempting to complete referrals.
Additionally, the designated trainer at eachteaching hospital was expected to provide cascadetraining and ongoing support to other staff; how-ever, we do not have evidence to suggest that su-pervision strategies were implemented in theinitial months to ease adoption or facilitate sus-tainability. Improved supervision strategies such
as regular evaluation and feedback, strengthenedorganizational culture, and an emphasis on collab-oration and partnership between facilitiesmay im-prove implementation outcomes.46 To strengthencoordination between satellite facilities and hos-pitals, we recommend a stronger interfacilityperformance and quality improvement system beimplemented from the outset of future initiatives.
Strengths and LimitationsThis was a qualitative study with purposively se-lected participants; therefore our results are nottransferrable beyond the study sample. Interview-ing both women and providers captured a range ofperspectives on implementation, service, and clientoutcomes. However, interviews were often held atthe participating facility, increasing the risk of socialdesirability bias. To minimize this risk, interviewswere held in rooms with both audio and visual pri-vacy. Given that many participants’ spoke candidlyabout their experiences and concerns, we believesocial desirability bias was minimal. A further limi-tation is that we interviewed providers at only asingle time point. Implementation outcomes aredynamic, and provider perspectives may changethroughout the course of the initiative.27 How-ever, implementation tends to be most difficultduring its early stages, and by capturing providers’immediate reactions and perceptions during theinitial phase, we were able to highlight key oppor-tunities for improved implementation of futurePPFP initiatives.
CONCLUSIONSRenewed interest in postpartum family planninghas ushered in a wave of interventions aimed toincrease contraceptive use immediately followingbirth, including a focus on long-acting reversiblemethods. However, in LMICs such as Tanzania,health systems are overburdened, and providersoften have limited resources to implement newinitiatives with high fidelity. Constraints that im-pede implementation of novel PPFP programs inresource-poor contexts are often overlooked46;yet, given rapid development and eagerness toadopt effective programs, implementation strate-gies in these settings require attention.
Meeting women’s contraceptive needs is cru-cial to reduce adverse maternal and infant healthoutcomes in LMICs, yet there is limited researchon the implementation of postpartum family plan-ning programs in these contexts. Continuedefforts to integrate contraceptive counseling intoANC as a part of national guidelines, and offering
PPIUD insertion as part of a country’s method mixmake implementation studies of such initiativesincreasingly important.
Acknowledgments: We are grateful to the women and health careproviders who shared their experiences with the research team.Weacknowledge the PPIUD Tanzania research team, including GoodluckMbando, Angelica Rugarabamu, Caritas Pesha, and JosephTumushabe, for their contributions to this research study. The authorswould also like to thank the regional service providers and medicaldoctors who supported the study, including Bernad Mgeta, WilliamMwebeya, John Francis Rwegoshorwa, Caroline Damian, and JohnMwakipesile.
Funding: This study was funded by an anonymous donor.
Competing interests:None declared.
REFERENCES1. Stover J, Ross J. How increased contraceptive use has reduced ma-
ternal mortality.Matern Child Health J. 2010;14(5):687–695.CrossRef. Medline
2. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Effects ofbirth spacing on maternal health: a systematic review. Am J ObstetGynecol. 2007;196(4):297–308. CrossRef. Medline
3. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birthspacing and risk of adverse perinatal outcomes: a meta-analysis.JAMA. 2006;295(15):1809–1823. CrossRef. Medline
4. Kozuki N, Walker N. Exploring the association between short/longpreceding birth intervals and child mortality: using reference birthinterval children of the same mother as comparison. BMC PublicHealth. 2013;13(3):S6. CrossRef. Medline
5. Gaffield ME, Egan S, Temmerman M. It’s about time: WHO andpartners release programming strategies for postpartum familyplanning.Glob Health Sci Pract. 2014;2(1):4–9. CrossRef. Medline
6. Rossier C, Bradley SEK, Ross J, Winfrey W. Reassessing unmet needfor family planning in the postpartum period. Stud Fam Plann.2015;46(4):355–367. CrossRef. Medline
7. Makins A, Taghinejadi N, Sethi M, et al. Factors influencing the like-lihood of acceptance of postpartum intrauterine devices across fourcountries: India, Nepal, Sri Lanka, and Tanzania. Int J GynaecolObstet. 2018;143 Suppl 1:13–19. CrossRef. Medline
8. McNamee P, Ternent L, Hussein J. Barriers in accessing maternalhealthcare: evidence from low-and middle-income countries. ExpertRev Pharmacoecon Outcomes Res. 2009;9(1):41–48. CrossRef.Medline
9. Canning D, Shah IH, Pearson E, et al. Institutionalizing postpartumintrauterine device (IUD) services in Sri Lanka, Tanzania, and Nepal:study protocol for a cluster-randomized stepped-wedge trial. BMCPregnancy Childbirth. 2016;16(1):362. CrossRef. Medline
10. Grimes D, Schulz K, Van Vliet H, Stanwood N. Immediate post-partum insertion of intrauterine devices. Cochrane Database SystRev. 2003;(1):CD003036. CrossRef. Medline
11. Kapp N, Curtis KM. Intrauterine device insertion during the postpar-tum period: a systematic review. Contraception. 2009;80(4):327–336. CrossRef. Medline
12. American College of Obstetricians and Gynecologists. ImmediatePostpartum Long-Acting Reversible Contraception. CommitteeOpinionNo. 670. Published August 2016. AccessedMay 15, 2020.https://www.acog.org/en/Clinical/Clinical%20Guidance/Committee%20Opinion/Articles/2016/08/Immediate%20Postpartum%20Long-Acting%20Reversible%20Contraception
13. Jatlaoui TC,Whiteman MK, Jeng G, et al. Intrauterine device expul-sion after postpartum placement: a systematic review and meta-
14. Doctor HV, Nkhana-Salimu S, Abdulsalam-Anibilowo M. Health fa-cility delivery in sub-Saharan Africa: successes, challenges, andimplications for the 2030 development agenda. BMC Public Health.2018;18(1):765. CrossRef. Medline
15. Ministry of Health, Community Development, Gender, Elderly andChildren (MOHCDGEC) Tanzania Mainland, Ministry of HealthZanzibar (MOH), National Bureau of Statistics (NBS), Office of theChief Government Statistician (OCGS), and ICF. TanzaniaDemographic and Health Survey and Malaria Indicator Survey2015–2016: Final Report. MOHCDGEC, MOH, NBS, OCGS, ICF;2016. Accessed June 8, 2020. https://dhsprogram.com/pubs/pdf/FR321/FR321.pdf
16. Pallangyo EN, Mbekenga C, Källestål C, Rubertsson C, Olsson P. “Ifreally we are committed things can change, starting from us”:healthcare providers’ perceptions of postpartum care and its poten-tial for improvement in low-income suburbs in Dar es Salaam,Tanzania. Sex Reprod Healthc. 2017;11:7–12. CrossRef. Medline
17. Tanzania: commitment maker since 2012. FP2020 website.Accessed June 8, 2020. https://www.familyplanning2020.org/tanzania
18. Cleland J, Ali M, Benova L, Daniele M. The promotion of intrauterinecontraception in low- and middle-income countries: a narrative re-view. Contraception. 2017;95(6):519–528. CrossRef. Medline
19. de Caestecker L, Banks L, Bell E, Sethi M, Arulkumaran S. Planningand implementation of a FIGO postpartum intrauterine device initia-tive in six countries. Int J Gynaecol Obstet. 2018;143 Suppl 1:4–12.CrossRef. Medline
20. United Republic of Tanzania Ministry of Health and Social Welfare(MOHSW).National Family Planning Guidelines and Standards.MOHSW; 2013. Accessed June 10, 2020. https://www.prb.org/wp-content/uploads/2018/05/National-Family-Planning-Guidelines-and-Standards-2013.Tanzania.pdf
21. Muganyizi PS, Kimario G, Ponsian P, Howard K, Sethi M, Makins A.Clinical outcomes of postpartum intrauterine devices inserted bymidwives in Tanzania. Int J GynaecolObstet. 2018;143 Suppl 1:38–42. CrossRef. Medline
22. Pearson E, Senderowicz L, Pradhan E, et al. Effect of a postpartumfamily planning intervention on postpartum intrauterine devicecounseling and choice: evidence from a cluster-randomized trial inTanzania. BMCWomens Health. 2020;20(1):102. CrossRef.Medline
23. Gearing RE, El-Bassel N, Ghesquiere A, Baldwin S, Gillies J, NgeowE. Major ingredients of fidelity: a review and scientific guide to im-proving quality of intervention research implementation.Clin PsycholRev. 2011;31(1):79–88. CrossRef. Medline
24. Corbin J, Strauss A. Basics of Qualitative Research: Techniques andProcedures for Developing Grounded Theory. 3rd ed. SagePublications; 2008.
26. Saldaña J. The Coding Manual for Qualitative Researchers. 3rd ed.Sage Publications; 2009.
27. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementa-tion research: conceptual distinctions, measurement challenges, andresearch agenda. Adm Policy Ment Health. 2011;38(2):65–76.CrossRef. Medline
28. Maternal and Child Health Integrated Program (MCHIP).AGuide forPlanning and Implementing Social and Behavior ChangeCommunication Activities for Postpartum Family Planning. MCHIP;2014. Accessed June 10, 2020. https://toolkits.knowledgesuccess.org/sites/default/files/sbcc_ppfp_guide_12.11.14.pdf
Assessing the Implementation of a Postpartum Contraception Initiative in Tanzania www.ghspjournal.org
Global Health: Science and Practice 2020 | Volume 8 | Number 2 288
29. Huber-Krum S, Hackett K, Senderowicz L, et al. Women’s perspec-tives on postpartum intrauterine devices in Tanzania. Stud FamPlann. 2019;50(4):317–336. CrossRef. Medline
30. Manongi RN, Marchant TC, Bygbjerg IC. Improving motivationamong primary health care workers in Tanzania: a health workerperspective. Hum Resour Health. 2006;4(1):6. CrossRef. Medline
31. Stokes T, Shaw EJ, Camosso-Stefinovic J, Imamura M, Kanguru L,Hussein J. Barriers and enablers to guideline implementation strate-gies to improve obstetric care practice in low- and middle-incomecountries: a systematic review of qualitative evidence. Implement Sci.2016;11(1):144. CrossRef. Medline
32. Baker U, Hassan F, Hanson C, et al. Unpredictability dictates qualityof maternal and newborn care provision in rural Tanzania- a quali-tative study of health workers’ perspectives. BMC PregnancyChildbirth. 2017;17(1):55. CrossRef. Medline
33. Kwesigabo G, Mwangu MA, Kakoko DC, et al. Tanzania’s healthsystem andworkforce crisis. J Public Health Policy. 2012;33 Suppl 1:S35–S44. CrossRef. Medline
34. Immediate postpartum family planning: A key component ofchildbirth care. High Impact Practices in Family Planning website.Published October 2017. Accessed June 10, 2019. https://www.fphighimpactpractices.org/briefs/immediate-postpartum-family-planning/
35. Frambach RT, Schillewaert N. Organizational innovation adoption:a multi-level framework of determinants and opportunities for futureresearch. J Business Res. 2002;55(2):163–176. CrossRef
36. Firoz T, McCaw-Binns A, Filippi V, et al. A framework for healthcareinterventions to address maternal morbidity. Int J Gynaecol Obstet.2018;141(Suppl 1):61–68. CrossRef. Medline
37. Kerber KJ, de Graft-Johnson JE, Bhutta ZA, Okong P, Starrs A, LawnJE. Continuum of care for maternal, newborn, and child health: fromslogan to service delivery. Lancet. 2007;370(9595):1358–1369.CrossRef. Medline
38. Hope R, Kendall T, Langer A, Bärnighausen T. Health systems inte-gration of sexual and reproductive health and HIV services in sub-Saharan Africa: a scoping study. J Acquir Immune Defic Syndr.2014;67 (Suppl 4):S259–S270. CrossRef. Medline
39. Lori JR, Ofosu-Darkwah H, Boyd CJ, Banerjee T, Adanu RMK.Improving health literacy through group antenatal care: a prospec-tive cohort study. BMC Pregnancy Childbirth. 2017;17(1):228.CrossRef. Medline
40. Sharma J,O’ConnorM, Rima Jolivet R. Group antenatal care modelsin low- and middle-income countries: a systematic evidence synthe-sis. Reprod Health. 2018;15(1):38. CrossRef. Medline
41. Boyee D, Peacock E, Plotkin M, et al. What messages are adolescentvoluntary medical male circumcision (VMMC) clients getting andhow? Findings from an observational study in Tanzania. AIDSBehav. 2017;21(5):1383–1393. CrossRef. Medline
42. Campbell C. Creating environments that support peer education:experiences from HIV/AIDS-prevention in South Africa. HealthEducation. 2004;104(4):197–200. CrossRef
43. Keogh SC, Urassa M, Kumogola Y, Kalongoji S, Kimaro D, Zaba B.Postpartum contraception in Northern Tanzania: Patterns of use, re-lationship to antenatal intentions, and impact of antenatal counsel-ing. Stud Fam Plann. 2015;46(4):405–422. CrossRef. Medline
44. Hackett K, Lenters L, Vandermorris A, et al. How can engagement ofadolescents in antenatal care be enhanced? Learning from the per-spectives of youngmothers in Ghana and Tanzania. BMC PregnancyChildbirth. 2019;19(1):184. CrossRef. Medline
45. Peneza AK, Maluka SO. ‘Unless you come with your partner you willbe sent back home’: strategies used to promote male involvement inantenatal care in Southern Tanzania.Glob Health Action. 2018;11(1):1449724. CrossRef. Medline
46. Yapa HM, Bärnighausen T. Implementation science in resource-poorcountries and communities. Implement Sci. 2018;13(1):154.CrossRef. Medline
Peer Reviewed
Received: October 20, 2019; Accepted: June 2, 2020
Cite this article as: Hackett K, Huber-Krum S, Francis JM, et al. Evaluating the implementation of an intervention to improve postpartum contraception inTanzania: a qualitative study of provider and client perspectives. Glob Health Sci Pract. 2020;8(2):270-289. https://doi.org/10.9745/GHSP-D-19-00365