Page 1
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1441
EVALUATION OF ANTI- DIABETIC THERAPY, OUTCOMES AND
IMPACT OF PATIENT COUNSELLING ON QUALITY OF LIFE IN
TYPE-2 DIABETES MELLITUS PATIENT IN A TERTIARY CARE
TEACHING HOSPITAL
*Dr. Jagrit Koirala, Dr. Peter Kandel, Dr. Dipendra Thapa and Dr. R. Parthasaradhi
Reddy
Pharm D Graduate, RRCOP, India.
ABSTRACT
Background: The aim of the study is to evaluate anti- diabetic
therapy, its outcomes and impact of patient counselling on QOL IN
Type- II DM patients. Method: The observational study included 120
diabetics. Patient were interviewed using structural questionnaire
developed by researchers, during the period of 6-months from
December-may (2016-2017). The data was collected using proforma of
patient data collection form and proforma to assess KAP which
contains 25 questionnaire and the data were analysed statistically using
Microsoft excel. Anti-diabetic therapies were evaluated using treatment
chart review, proforma of patient data collection form. Outcome and impact of patient
counselling were measured assessing the response of KAP and RBS. Result: Out of 120
patient 52 were male and 68 were female. The majority of patient, 30% were on the age
group 51-60 years. The patient with age group >50years were more affected. The majority of
patient 52(43.33%) were diseased for a period of 6-10 years 32(26.66%) were diseased for a
period of 1-5 years, 16 (13.33%) were diseased for a period of 11 -15 years, 12 (10%) were
diseased for a period of above 15 years and 8 (6%) below 1 year. Total number of drugs
prescribed were 810 with an average of 6.75 drugs per prescription. The most commonly
prescribed anti-diabetic drugs were biagunides(25%), insulin(20.8%), sulphonylurea(7.5%),
a-glucosidase inhibitor(5.83%). Second commonly prescribed drugs were antibiotics(22.83%)
and cardiovascular drugs(16.66%). Blood glucose values were measured before and after
patient counselling during the time of admission and follow up. After counselling there was
decrease in glucose value which was clinically significant but statistically not significant
World Journal of Pharmaceutical Research SJIF Impact Factor 8.084
Volume 9, Issue 6, 1441-1465. Research Article ISSN 2277– 7105
Article Received on
24 March 2020,
Revised on 14 April 2020,
Accepted on 04 May 2020,
DOI: 10.20959/wjpr20206-17458
*Corresponding Author
Dr. Jagrit Koirala
Pharm D Graduate, RRCOP,
India.
[email protected] ,
Page 2
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1442
(p>0.05). The KAP score of the patient in pre-counselling, knowledge score was 5.13±2.91,
attitude 1.4±0.748 and practice 2.26±0.378 and overall score was 8.81±4.378. In post
counselling the KAP score of patient, knowledge 6.8±3.05, attitude 3.3±1.25, practice
2.63±0.480 and the overall score was 12.63±4.78. Conclusion: Educational intervention is
necessary to improve knowledge, attitude and practices of diabetes patient for health benefits.
As evidenced by study patient who followed pharmacist counselling on medication, diabetic
diet, exercise and practice have achieved better health and quality of life.
KEYWORD: Hyperglycemia, Intervention, Counselling, Quality of life.
INTRODUCTION
The term diabetes mellitus describes a metabolic disorder of multiple aetiology characterized
by chronic hyperglycaemia with disturbances of carbohydrate, fat and protein metabolism
resulting from defects in insulin secretion, insulin action, or both. The effects of diabetes
mellitus include long-term damage, dysfunction and failure of various organs. Diabetes
mellitus may present with characteristic symptoms such as thirst, polyuria, blurring of vision,
and weight loss. In its most severe forms, ketoacidosis or a non-ketotic hyperosmolar state
may develop and leads to stupor, coma, and in absence of effective treatment leads to death.
Often symptoms are not severe, or may be absent, and consequently hyperglycaemia
sufficient to cause pathological and functional changes may be present for a long time before
the diagnosis is made. The long-term effects of diabetes mellitus includes progressive
development of the specific complications of retinopathy with blindness, nephropathy that
may lead to renal failure, and/or neuropathy with risk of foot ulcers, amputation, charcot
joints and features of autonomic dysfunction, including sexual dysfunction. People with
diabetes mellitus are at increased risk of cardiovascular, peripheral vascular and
cerebrovascular disease.
Several pathogenic processes are involved in the development of diabetes. These include
processes which destroy B-cells of the pancreas with consequent insulin deficiency, and
others that results in resistance to insulin actions. The abnormalities of carbohydrate, fat and
protein metabolism are due to deficient action of insulin on target tissues resulting from
insensitivity of lack of insulin.[1]
DIAGNOSIS: Severe hyperglycaemia detected under condition of acute infective, traumatic,
circulatory or other stress may be transitory and should not in itself be regarded as diagnostic
Page 3
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1443
of diabetes. The diagnosis of diabetes in asymptomatic subjects should never be made on the
basis of a single abnormal blood glucose value. For the asymptomatic person, at least one
additional plasma/blood glucose test result with a value in the diabetic range is essential,
either fasting, from a random (casual) sample, or from the oral glucose tolerance test(OGTT)
or HbA1C. If such samples fail to confirm the diagnosis of diabetes mellitus, it will usually
be advisable to maintain surveillance with periodic re-testing until the diagnostic situation
becomes clear. In these circumstances, the clinicians should take into consideration such
additional factors as ethnicity, family history, age, adiposity, and concomitant disorders,
before deciding on a diagnostic or therapeutic course of action. An alternative to blood
glucose estimation or the OGTT has long been sought to simplify the diagnosis of diabetes.
Glycated haemoglobin, reflecting average glycaemia over a period of weeks, was thought to
provide such a test. Although in certain cases it gives equal or almost equal sensitivity and
specificity to glucose measurement, it is not available in many parts of the world and is not
well enough standardised for its use to be recommended at this time.[2]
CLASSIFICATION: The first widely accepted classification of diabetes mellitus was
published by WHO in 1980[3]
and in modified form, in 1985[4]
the 1980 and 1985
classification of diabetes mellitus and allied categories of glucose intolerance included
clinical classes and two statistical risk classes. The 1980 experts committee proposed two
major classes of diabetes mellitus and named them, IDDM or type-1, and NIDDM or type-2.
In the 1985 study group report the terms type-1 and type-2 were omitted, but the classes
IDDM and NIDDM were retained, and a class of malnutrition-released diabetes mellitus
(MRDM) was introduced. In both the 1980 and 1985 reports other classes of diabetes
includes other type and impaired glucose tolerance (IGT) as well as gestational diabetes
mellitus (GDM). These were reflected in the subsequent international nomenclature of
disease (IND) in 1991, and the tenth revision of the international classification of diseases
(ICD-10) in 1992. The 1985 classification was widely accepted and is used internationally.
The recommended classification includes both staging of diabetes mellitus based on clinical
descriptive criteria and a complimentary aetiological classification.
Type-2 is the most common form of diabetes and is characterized by disorders of insulin
actions and insulin secretion, either of which may be the predominant features. Both are
usually present at the time when this form of diabetes clinically manifest. By definition,
specific reason for the development of these abnormalities is not yet known.[5]
Page 4
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1444
India leads the world with largest number of diabetic subjects earning the dubious distinction
of being termed the “diabetes capital of the world”. According to the Diabetes Atlas 2006
published by the International Diabetes Federation, the number of people with diabetes in
India currently around 40.9 million is expected to rise to 69.9 million by 2025 unless urgent
preventive steps are taken.[6]
Diabetes is a chronic condition that can lead to serious and
costly complications. Every 7 seconds a person dies from diabetes. In 2014, diabetes caused
4.9 million deaths globally.[7]
Various factor causes onset of diabetes mellitus e.g. genetic factor, constitutional factor,
environmental factor, insulin resistance, impaired insulin secretion Quality of life may be
thought of as a multidimensional construct incorporating an individual's subjective perception
of physical, emotional, and social well-being, including both a cognitive component
(satisfaction) and an emotional component (happiness).[8]
More than 50 years ago, the World
Health Organization stated that health was defined not only by the absence of disease and
infirmity, but also by the presence of physical, mental, and social well-being.[9]
It appears that
active and effective disease-specific coping can trigger a positive cascade of enhanced well-
being, more active diabetes self-management, better glycemic control, and fewer
complications. This suggests that people with diabetes who are not active or effective copers
may benefit from interventions designed to enhance their coping. Outpatient education
program that incorporated coping skills training interventions designed to improve some
aspects of quality of life. This intervention significantly improved diabetes self-efficacy and
emotional well-being (depression and anxiety) at follow-up, 6 months after the intervention
was completed. Interventions such as this hold promise for improving a broad range of
outcomes for people with diabetes.[10]
Nepal is estimated to reach 6,38,000 of diabetic patient by the year 2025.[11]
Diabetes can
lead to increased morbidity and mortality.[12]
There is improper guidance about the disease
due to lack of understanding of patients characteristics i.e. personality and attitude of the
patient A study from Pakistan highlighted the fact that a proper education and awareness
program can change the attitude of the public regarding diabetes. There is lack of public
awareness regarding DM in Nepal where, medical services are poor.[13]
Several interventions
have been carried out to improve the knowledge level of diabetes patients.[14-16]
Obtaining
information about the level of awareness about diabetes in a population is the first step in
formulating a prevention program for diabetes.[17]
, as a large gap between knowledge and
Page 5
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1445
attitude among the diabetes patients was found[18]
and proper knowledge regarding various
aspects of health education program can improve the knowledge of patients and change their
attitude. Another study showed that intensive diabetes education and care management can
improve the patient outcomes, glycemic control and quality of life in patients with diabetes
mellitus.
In Pakistan 9.5% of the urban and 9.4% of the rural population suffer from type- 2 diabetes.
Overall glucose intolerance (diabetes and impaired glucose tolerance) is 22.04% in urban and
17.15% in rural areas.[19]
According to the WHO estimates, Pakistan ranked seventh in
prevalence of Diabetes. These figures however represent tip of the iceberg with many cases
still undiagnosed.[20-22]
Despite all the research, diabetes remains under diagnosed. This then
ultimately presents with complications, the direct and indirect costs of which are
enormous.[23,24]
Diabetes care aims at improving the quality of life of patients with type 2
diabetes through good glycaemic control[25]
, control of risk factors, lifestyle
modification,[26,27]
prevention of complications and diabetes education. Diabetes education is
the cornerstone of diabetes care.[28,29]
Improved training of the primary health care providers
and patients with diabetes is therefore beneficial.[30]
Several studies of family physicians
identified the need for improvement in their practices for treating and educating
diabetics.[31,32]
In Pakistan, there is paucity of information about knowledge and attitudes
concerning glycaemic control, complications and the health impact of diabetes. There are
some studies from Karachi but data from other regions of the country is sparse especially
from Northern side. This study was designed to explore patients awareness about diabetes,
misconceptions about the disease itself, its treatment especially diet and insulin. The
information gained could subsequently be helpful to design and initiate comprehensive
programmes for detection and control of diabetes and its complications with self-care and
community support as its major components.[33]
The present study was conducted to study
demographic details of patient and to evaluate knowledge, attitude and practice of these
patients.
AIM AND OBJECTIVES OF THE STUDY
AIM: To evaluate anti diabetic therapy, outcome and impact of patient counselling on
quality of life in type-2 diabetes mellitus patient in tertiary care teaching hospital.
Page 6
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1446
Objectives of the Study
To assess the medication regimen, symptoms and complication of diabetes mellitus
patient and to determine the glycemic control by reviewing and assessing the blood
glucose level.
To determine the outcome of patient counselling on quality of life and comprehend
knowledge, attitude and practice of type-2 diabetic patient.
METHODOLOGY
STUDY SITE
This observational study was carried out in In-patient & out-patient in general medicine
Department of Sapthagiri Institute of Medical Science & Research Center.
STUDY DESIGN
This study is a prospective and observational study conducted over six month’s period.
STUDY DURATION
6 months study with data collection for a period of 3 months.
STUDY POPULATION
120 patients with type-2 diabetes mellitus who according to physician needs insulin treatment
and/or oral hypoglycemic drug with or without insulin who were in inpatient and outpatient
department.
STUDY CRITERIA
INCLUSION CRITERIA
The study populations are both men & women having type -2 diabetes mellitus, above age of
18 years.
EXCLUSION CRITERIA
End stage renal failure, cardiac failure, hepatic failure & history of drug abuse, clinically
relevant medical or physiological condition.
SOURCE OF DATA
Patient data collection form.
Prescriptions of patients.
Patient medication chart review.
Page 7
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1447
Lab reports
Verbal communication with patient.
STUDY MATERIAL
Proforma of patient data collection form: A common patient profile form was prepared as
per the need of study, to enter the patient data. (Annexure 1)
Proforma to assess KAP: A Knowledge, attitude and practice (KAP) questionnaire was
prepared and validated, which consists of 25 questions. Among 25 questions 18 were
knowledge related, 4 were attitude and 3 practice related. (Annexure 2)
STUDY PROCEDURE
Patient data was collected in patient data collection proforma which includes
demographic details of patient, lab data, diagnosis, medication.
Response of KAP about the disease by the patient was assessed before and after
counseling of patients using KAP proforma. Each correct answer was given a score of 1
& each wrong was given a score of 0.
STATISTICAL ANALYSIS
Statistical Analysis was done using MS Excel, Student T-test was performed to calculate the
P - value and the results were appropriately interpreted and reported.
RESULTS
The prospective observational study was conducted for 6 months in Sapthagiri Institute of
Medical Science & Research Center. A total of 120 type 2 diabetes mellitus patient were
included in the study.
Patient Distributions Based on Demographic Data
Out of 120 patients 68 (56.66%) were females and 52 (43.33%) were males which is
represented in table-1 and figure-1.
Table 1: Patient Distribution Based on Gender.
Total No. of patients (%) No. of Male patients (%) No. of Female patients (%)
120 (100%) 52 (43.33%) 68 (56.66%)
Page 8
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1448
Fig 1: Pie chart of Patient Distribution Based on Gender.
Patient Distribution with Respect to their Age Groups
Patients were categorized according to their age groups. Out of 120 patients majority 36
(30%) of them were found in the age group between 51-60 years, followed by 28(23.33%) in
the age group between 61-70 years, 24(20%) in the age group between 41-50 years, then
20(16.66%) were found between 30-40 years and 12 (10%) were >70 years which is
represented in table-2 and figure-2.
Table 2: Patient Distribution with Respect to their Age Groups.
Age group of
patients
No. of Male Patients
(%)
No. of Female Patients
(%)
Total No. of
Patients (%)
30-40 16 (80) 4 (20) 20 (16.66)
41-50 12 (50) 12 (50) 24 (20)
51-60 12 (37.5) 24 (66.66) 36 (30)
61-70 8 (25) 20 (71.42) 28 (23.33)
>70 4 (33.33) 8 (66.66) 12 (10)
Page 9
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1449
Fig 2: Graphical Representation of Patient Distribution with Respect to their Age
Groups.
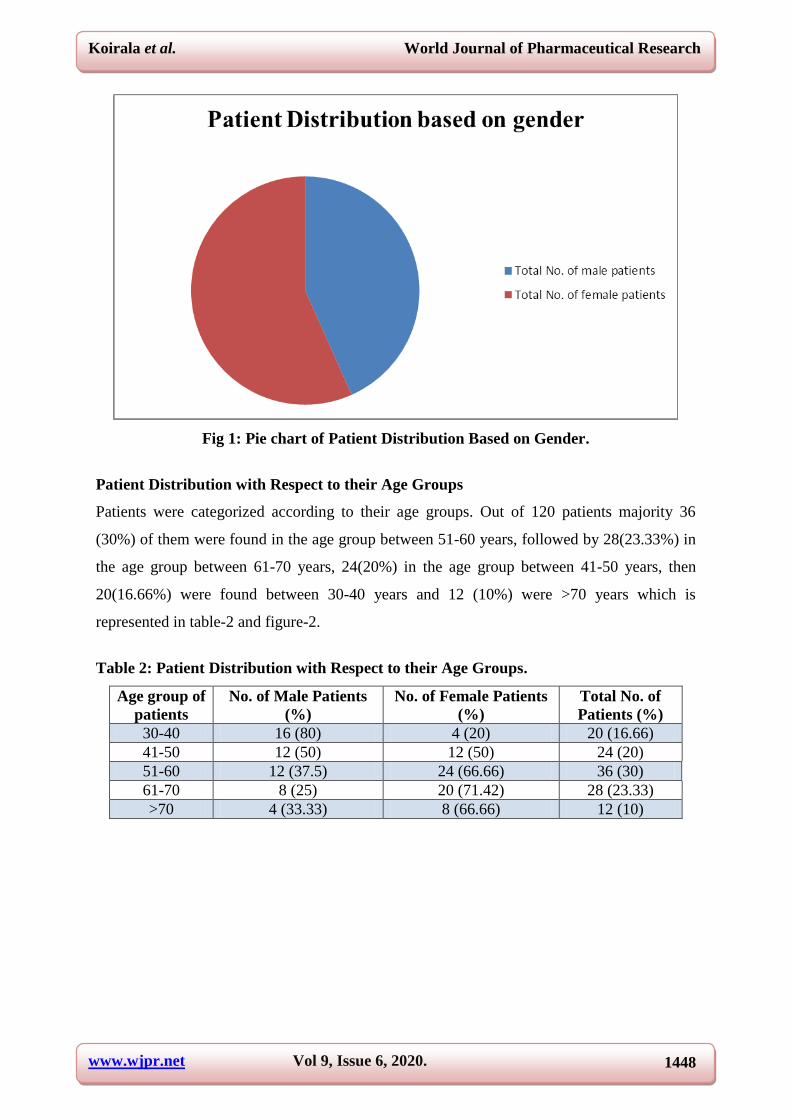
Distribution of Patients Based on Duration of Disease
Out of 120 patients 52 (43.33%) were diseased for a period of 6-10 years, 32(26.66%) were
diseased for a period of 1-5 years, 16 (13.33%) were diseased for a period of 11 -15 years, 12
(10%) were diseased for a period of above 15 years, and 8 (6%) below 1 year. Results are
shown in tables-3 and figure-3.
Table 3: Distributions of Patients Based on Duration of Disease.
Duration of Disease
(Years)
No. of Male
patients (%)
No. of Female
Patient (%)
Total No. of
Patients (%)
<1 4 (50) 4 (50) 8 (6.66)
1-5 16 (50) 16 (50) 32 (26.66)
6-10 20 (38.46) 32 (61.15) 52 (43.33)
11-15 8 (50) 8 (50) 16 (13.33)
>15 4 (33.33) 8 (66.66) 12 (10)
Page 10
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1450
Fig 3: Graphical Representation of Distributions of Patients Based on Duration of
Disease.
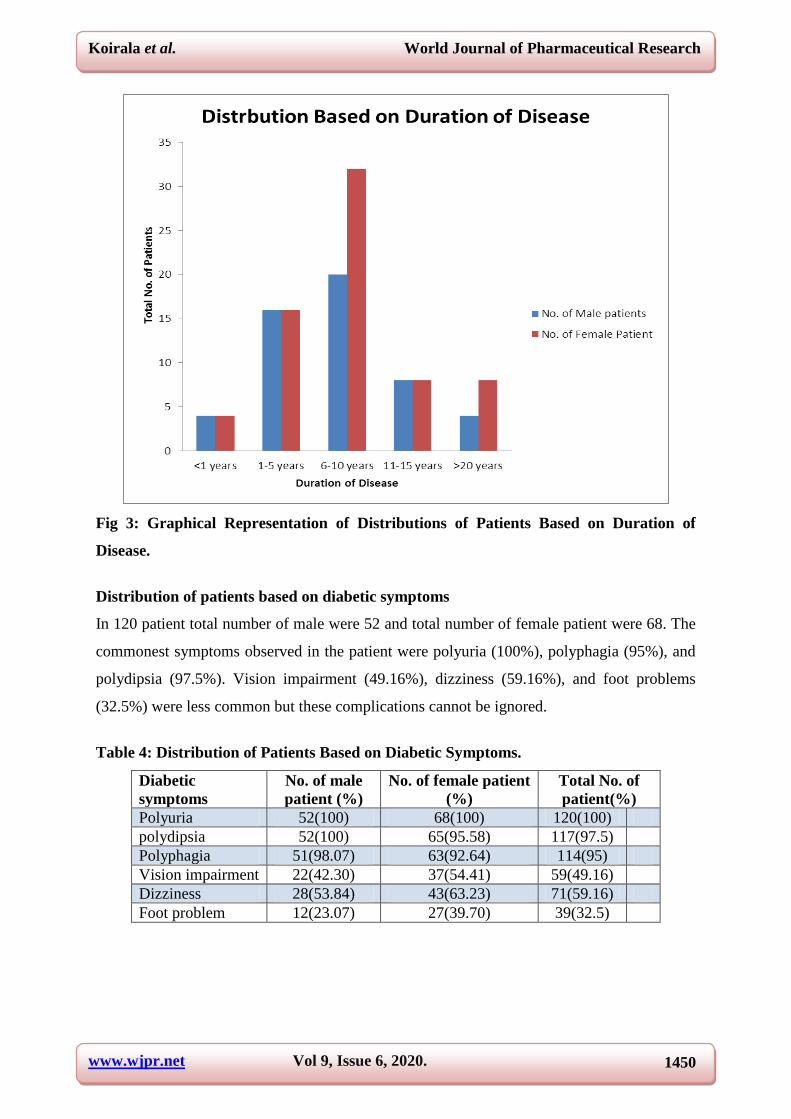
Distribution of patients based on diabetic symptoms
In 120 patient total number of male were 52 and total number of female patient were 68. The
commonest symptoms observed in the patient were polyuria (100%), polyphagia (95%), and
polydipsia (97.5%). Vision impairment (49.16%), dizziness (59.16%), and foot problems
(32.5%) were less common but these complications cannot be ignored.
Table 4: Distribution of Patients Based on Diabetic Symptoms.
Diabetic
symptoms
No. of male
patient (%)
No. of female patient
(%)
Total No. of
patient(%)
Polyuria 52(100) 68(100) 120(100)
polydipsia 52(100) 65(95.58) 117(97.5)
Polyphagia 51(98.07) 63(92.64) 114(95)
Vision impairment 22(42.30) 37(54.41) 59(49.16)
Dizziness 28(53.84) 43(63.23) 71(59.16)
Foot problem 12(23.07) 27(39.70) 39(32.5)
Page 11
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1451
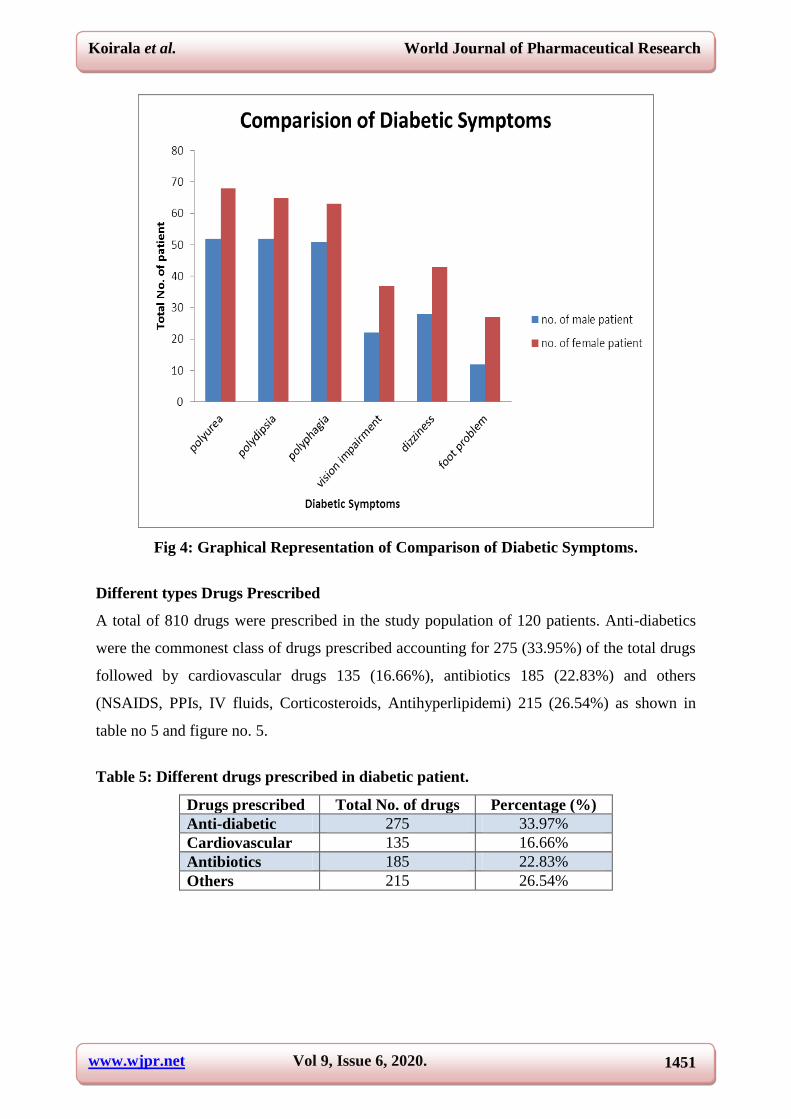
Fig 4: Graphical Representation of Comparison of Diabetic Symptoms.
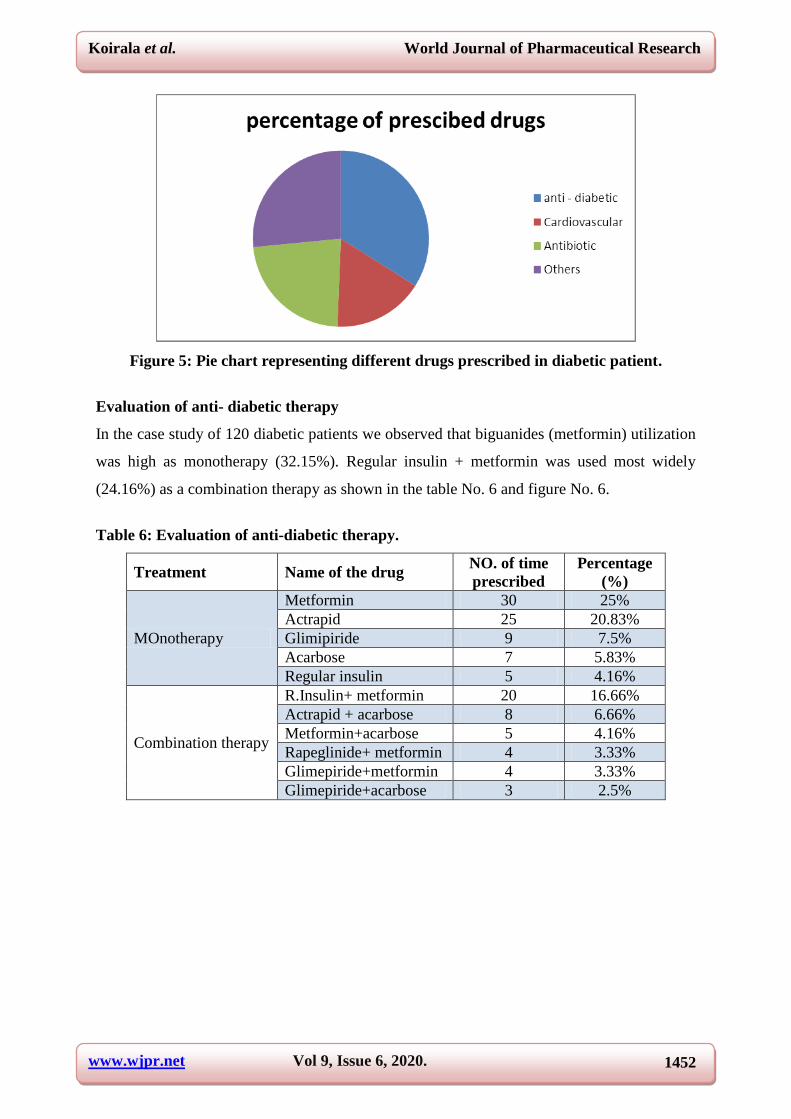
Different types Drugs Prescribed
A total of 810 drugs were prescribed in the study population of 120 patients. Anti-diabetics
were the commonest class of drugs prescribed accounting for 275 (33.95%) of the total drugs
followed by cardiovascular drugs 135 (16.66%), antibiotics 185 (22.83%) and others
(NSAIDS, PPIs, IV fluids, Corticosteroids, Antihyperlipidemi) 215 (26.54%) as shown in
table no 5 and figure no. 5.
Table 5: Different drugs prescribed in diabetic patient.
Drugs prescribed Total No. of drugs Percentage (%)
Anti-diabetic 275 33.97%
Cardiovascular 135 16.66%
Antibiotics 185 22.83%
Others 215 26.54%
Page 12
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1452
Figure 5: Pie chart representing different drugs prescribed in diabetic patient.
Evaluation of anti- diabetic therapy
In the case study of 120 diabetic patients we observed that biguanides (metformin) utilization
was high as monotherapy (32.15%). Regular insulin + metformin was used most widely
(24.16%) as a combination therapy as shown in the table No. 6 and figure No. 6.
Table 6: Evaluation of anti-diabetic therapy.
Treatment Name of the drug NO. of time
prescribed
Percentage
(%)
MOnotherapy
Metformin 30 25%
Actrapid 25 20.83%
Glimipiride 9 7.5%
Acarbose 7 5.83%
Regular insulin 5 4.16%
Combination therapy
R.Insulin+ metformin 20 16.66%
Actrapid + acarbose 8 6.66%
Metformin+acarbose 5 4.16%
Rapeglinide+ metformin 4 3.33%
Glimepiride+metformin 4 3.33%
Glimepiride+acarbose 3 2.5%
Page 13
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1453
Fig 6: pie chart Representing evaluation of anti-diabetic therapy.
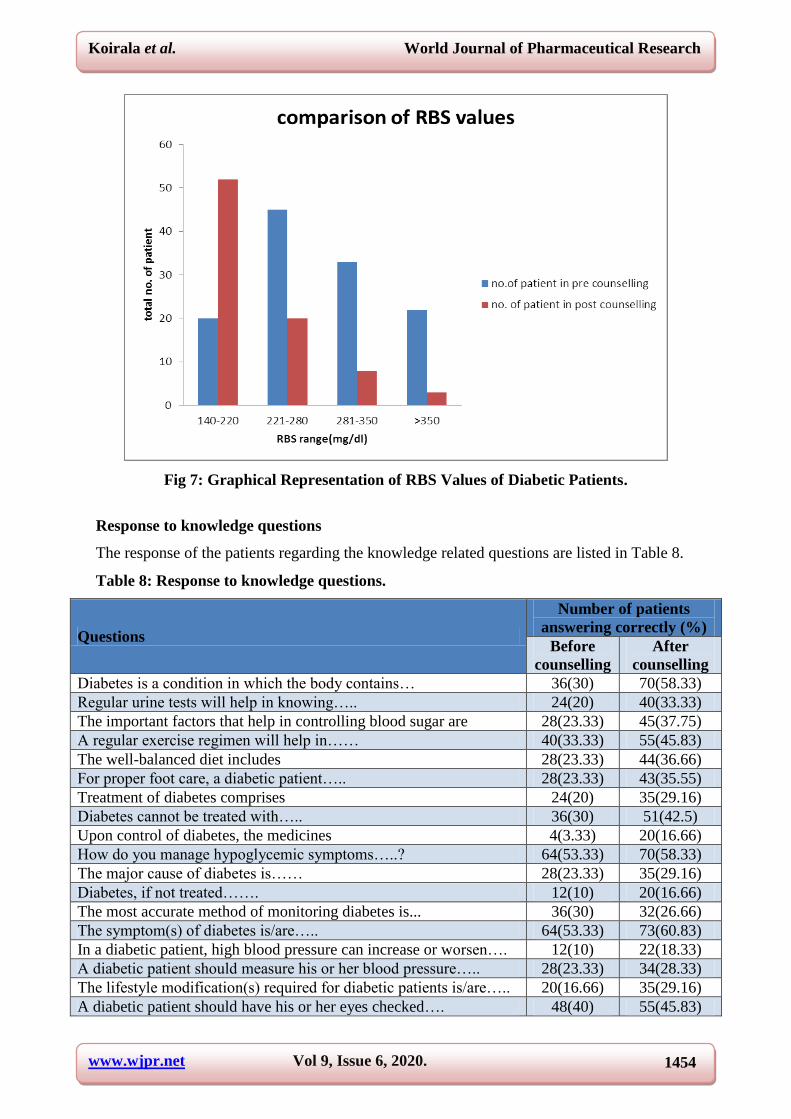
Effects of patient counselling on Blood Glucose levels
On the given scale, before counselling majority of patient 45(69.23%) RBS values lies in
between range of (221-280). After counselling majority of patient 52(72.22%) lies in between
the RBS range of (140-220). The RBS values of the patients are high in pre counselling, after
counselling the patient the RBS values were reduced as shown in table-7 and figure-7.
Table 7: Effect of Patient Counselling on RBS Values of Diabetic Patients.
RBS Range
(mg/dl)
No. of patient
in pre
counselling (%)
No. of patient
in post
counselling (%)
Total number
of patient (%) P value
140-220 20(27.77) 52(72.22) 72(35.46)
0.48474 221-280 45(69.23) 20(30.76) 65(32.01)
281-350 33(80.48) 8(19.51) 41(20,19)
>350 22(88.00) 3(12.00) 25(12.31)
Page 14
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1454
Fig 7: Graphical Representation of RBS Values of Diabetic Patients.
Response to knowledge questions
The response of the patients regarding the knowledge related questions are listed in Table 8.
Table 8: Response to knowledge questions.
Questions
Number of patients
answering correctly (%)
Before
counselling
After
counselling
Diabetes is a condition in which the body contains… 36(30) 70(58.33)
Regular urine tests will help in knowing….. 24(20) 40(33.33)
The important factors that help in controlling blood sugar are 28(23.33) 45(37.75)
A regular exercise regimen will help in…… 40(33.33) 55(45.83)
The well-balanced diet includes 28(23.33) 44(36.66)
For proper foot care, a diabetic patient….. 28(23.33) 43(35.55)
Treatment of diabetes comprises 24(20) 35(29.16)
Diabetes cannot be treated with….. 36(30) 51(42.5)
Upon control of diabetes, the medicines 4(3.33) 20(16.66)
How do you manage hypoglycemic symptoms…..? 64(53.33) 70(58.33)
The major cause of diabetes is…… 28(23.33) 35(29.16)
Diabetes, if not treated……. 12(10) 20(16.66)
The most accurate method of monitoring diabetes is... 36(30) 32(26.66)
The symptom(s) of diabetes is/are….. 64(53.33) 73(60.83)
In a diabetic patient, high blood pressure can increase or worsen…. 12(10) 22(18.33)
A diabetic patient should measure his or her blood pressure….. 28(23.33) 34(28.33)
The lifestyle modification(s) required for diabetic patients is/are….. 20(16.66) 35(29.16)
A diabetic patient should have his or her eyes checked…. 48(40) 55(45.83)
Page 15
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1455
Response to attitude questions
The response of the patients regarding the attitude related questions are listed in Table 9.
Table 9: Response to attitude questions.
Questions
Number of patients
answering correctly (%)
Before
counselling
After
counselling
Do you exercise regularly…………..? 20(16.66) 70(58.33)
Are you following a controlled and planned diet……? 44(36.66) 65(54.16)
Do you miss taking the doses of your diabetic
medication……? 52(43.33) 80(66.66)
Are you aware of blood sugar levels falling below normal
when you are taking drugs…….? 16(13.33) 40(33.33)
Response to practice questions
The response of the patients regarding the practice related questions are listed in Table 10.
Table 10: Response to practice questions.
Questions
Responses
Before counselling After counselling
Yes no Yes no
BP checkup 53 67 97 18
Eye check-up 25 95 43 55
Adherence to therapy 32 88 83 21
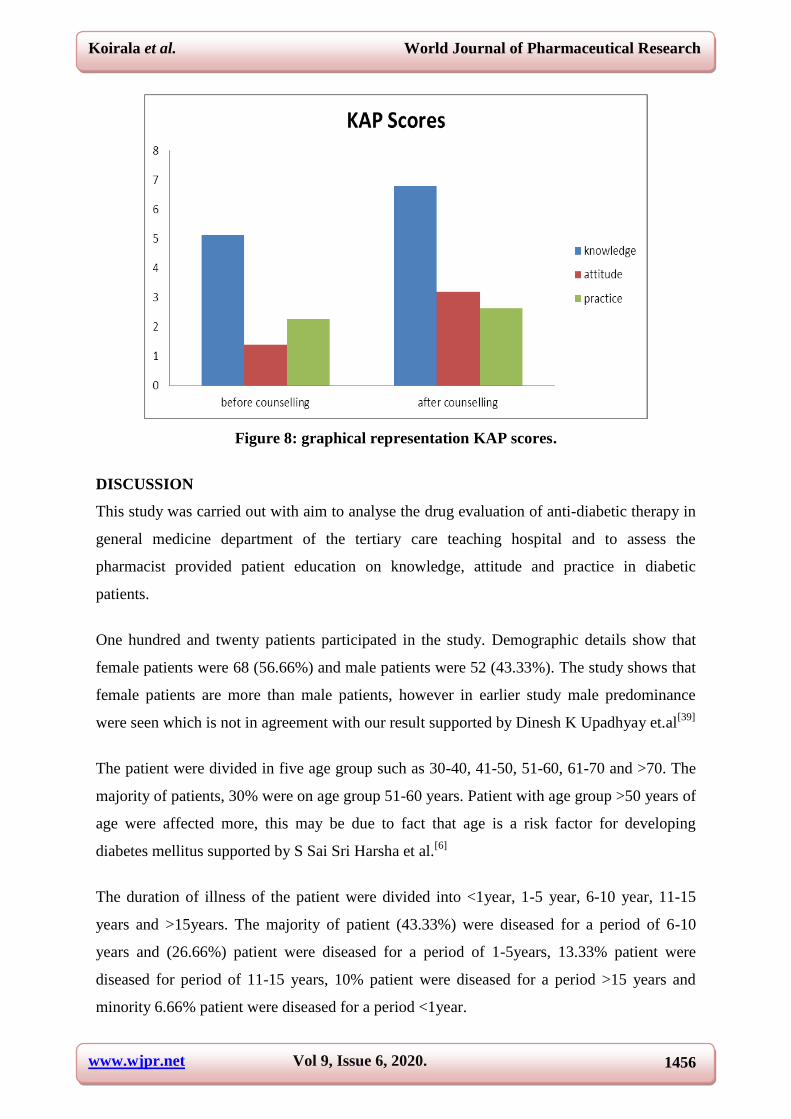
The mean ± SD scores of the study population regarding the knowledge, attitude and
practice outcomes were evaluated and the details are mentioned in Table 11.
Table 11: Mean scores of the patients.
Variables Mean ± SD score before
counselling
Mean±SD score After
counselling p- value
Knowledge 5.13±2.91 6.8±3.05 0.0236s
Attitude 1.4±0.748 3.2±1.25 0.0462s
Practice 2.26±0.378 2.63±0.480 0.1075ns
Overall 8.81±4.036 12.63±4.78
S= Statistically significant, Ns= statistically not significant
Page 16
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1456
Figure 8: graphical representation KAP scores.
DISCUSSION
This study was carried out with aim to analyse the drug evaluation of anti-diabetic therapy in
general medicine department of the tertiary care teaching hospital and to assess the
pharmacist provided patient education on knowledge, attitude and practice in diabetic
patients.
One hundred and twenty patients participated in the study. Demographic details show that
female patients were 68 (56.66%) and male patients were 52 (43.33%). The study shows that
female patients are more than male patients, however in earlier study male predominance
were seen which is not in agreement with our result supported by Dinesh K Upadhyay et.al[39]
The patient were divided in five age group such as 30-40, 41-50, 51-60, 61-70 and >70. The
majority of patients, 30% were on age group 51-60 years. Patient with age group >50 years of
age were affected more, this may be due to fact that age is a risk factor for developing
diabetes mellitus supported by S Sai Sri Harsha et al.[6]
The duration of illness of the patient were divided into <1year, 1-5 year, 6-10 year, 11-15
years and >15years. The majority of patient (43.33%) were diseased for a period of 6-10
years and (26.66%) patient were diseased for a period of 1-5years, 13.33% patient were
diseased for period of 11-15 years, 10% patient were diseased for a period >15 years and
minority 6.66% patient were diseased for a period <1year.
Page 17
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1457
The common symptoms seen in diabetic patients were polyuria, polydipsia, and polyphagia.
Vision impairment, dizziness, foot problems were seen in most of patient this may be due to
poor knowledge attitude and practice towards diabetes.
Total number of drug prescribed were 810 with an average of 6.75 dugs per prescription. The
risk of drug interaction may increase with increase in number of drugs per prescription which
ultimately lead to prescribing errors and in hazardous to the health of patient. Anti-diabetic
drugs were the most common drugs prescribed which accounts for 275 (33.97%) of total
drugs. Anti-diabetic drugs commonly prescribed as monotherapy were metformin(25%),
actrapid(20.8%), glimepiride(7.5%), acarbose(5.83%), regular insulin(4.16%) and as
combination therapy regular insulin+metformin(16.66%), actrapid+ acarbose(6.66%),
rapeglinide+metformin(3.33%), glimepiride+metformin(3.33%), glimepiride+acarbose
(2.5%). Biguanides (metformin) (25%) utilization was high as monotherapy in prescription,
this may be due to its high advantages of no weight gain. In combination therapy regular
insulin + metformin combination was most widely used (16.66%). Antibiotics were the
second commonest drug prescribed which accounts for 185 (22.83%) drugs, cardiovascular
drugs accounts for 135 (16.66%) and others (NSAIDs, PPIs, IV fluids, corticosteroids,
antihyperlipidemic) 215 (26.54%) were prescribed.
In the present study 70% patient reported hypertension along with diabetes mellitus, these
results were supported by Mahesh Gottipati et al.[57]
This study indicates that hypertension is
the commonest co-morbidity seen with diabetes mellitus.
The blood glucose values were measured before and after patient counselling during the time
of admission and follow up, blood glucose values were decreased in number of patient after
counselling. This may be due to awareness about knowledge, attitude, practice and
importance of adherence of medication gained. After counselling there was decrease in
glucose value which was clinically significant but statistically not significant (P>0.05).
The study assessed the level of knowledge, attitude and practice response of patient on
diabetes mellitus. The KAP questionnaire contained 25 questions regarding diabetes, 18
questions for knowledge, 4 questions for attitude and 3 questions for practice. These
questionnaires impart the concept of causes, symptoms, complication, and lifestyle
modification and have given lot of information to the patient on how to control the disease.
KAP score of the patient was found to be low before counselling. Patient counselling on
Page 18
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1458
disease and medication followed by dietician and nutritionist advice is generally not followed
hence, may have contributed to low level of KAP.
The KAP score of the patient in pre-counselling, knowledge score was 5.13±2.91, attitude
1.4±0.748 and practice 2.26±0.378 and overall score was 8.81±4.378. In post counselling the
KAP score of patient, knowledge 6.8±3.05, attitude 3.3±1.25, practice 2.63±0.480 and the
overall score was 12.63±4.78. It is well understood that diabetes management requires patient
involvement for a better disease control.[58]
Patient counselling by pharmacist can play vital
role in imparting education to the diabetics.[59]
CONCLUSION
Education is critical to social and economic development and has profound impact on
population health. We review evidence for the health benefits associated with education,
where we found the leading cause of complications in diabetic was non- adherence to
medication and unplanned diabetic diet and practice towards diabetes. Lack of knowledge
about the adherence, diet and practice leads to rise in blood glucose level and deterioration of
the symptoms. All these upstream factors may contribute to health outcomes and eventually
the quality of life of the patients. Quality of life is the standard of health, comfort, and
happiness experienced by an individual. Patient counselling can create dramatic difference in
morbidity-, mortality and the risk factors which increase quality of life of patient which is
also influenced by education and income of the patient.
Clinical pharmacist imparted patient education through counselling improved quality of life
through knowledge and adherence to therapy.
As he is the first and the last, we thankfully bow with reverence before the almighty who is
the source of all wisdom and knowledge, the creator who by his wishes and blesses made us
to attain successful completion of this dissertation.
With great pleasure and sense of gratitude, we express our most cordial and humble thanks to
our eminent respected HOD DR.GEETHA JAYAPRAKSH, Professor and HOD,
Department of Pharmacy Practice, RRCP, for her valuable guidance, keen interest,
inspiration, unflinching encouragement and moral support throughout our project work. We
express sincere thanks to her for stimulating discussion, meticulous guidance, illimitable
enthusiasm and support since the beginning of our course.
Page 19
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1459
We express our sincere gratitude to our research guide DR. SHAILESH YADAV, assistant
professor, department of pharmacy practice, RRCP with his guidance and support throughout
the work.
We express our deepest sense of gratitude to DR.B GOPALAKRISHNA, Principal of
RRCP, for his sincere guidance and support.
We express our deepest sense of gratitude to our honourable secretory MR. H. R KIRAN,
for providing the facilities and extending his support.
Our sincere thanks to PROF. R RAVINDAR, DR. PETER KANDEL, DR.
PARTHASARATHY, MS. APARNA, MS POORNIMA NB, MR. HEMANTH S.H, MR.
NAGRAJ MR. SUBASH PG, DR. SPANDANA and all other teachers for providing their
support to accomplish this wonderful work.
We would like to express our deep sense of love and affection to our colleagues for their kind
help, co-ordination and support throughout our graduation. You all are the one who made
everything beautiful, funny and happy.
At this moment we would love to express our thanks to our juniors, non-teaching staffs for
supporting us throughout our work in their own way.
We take this opportunity to thank the Liberian for extending library facilities throughout this
study.
We are greatly indebted to our beloved parents PARTHAMANI BHATTARAI, ANJU
DEVI BHATTARAI (GODFATHER), PRITHVINATH KOIRALA, DURGA DEVI
KOIRALA, BAIKUNTHA KOIRALA, SANGITA KOIRALA, SURAKSHYA
KOIRALA. TIRTHA BAHADUR THAPA, KARNAMAYA THAPA, NAGENDRA
THAPA, KABITA THAPA, NABIN THAPA. R LINGA REDDY, K JAYALAKSHMI
for their unending Prayers, Love, Faith, Encouragement and Support throughout this
wonderful journey. We are sure about experiencing such sweetest love and care in our future
ahead too.
We express our deepest and sincere thanks to the general medicine department (Dr.
RAGEVENDRA Dr. TAMIL SELVAN, Dr.SAM AHUJA, and Dr.SOMASEKHAR. C),
Page 20
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1460
other Doctors, Pharmacists, Management, Lab technician, Nurses of Tertiary Care Hospital
for allowing us to collect all the primary information’s required for the study. We are grateful
to you all.
We extend our special thanks to computer operator, printers and binders for their technical
assistance and preparation of this manuscript on time. Last but not the least, we extend our
thanks to all those who have been directly or indirectly associated with our study.
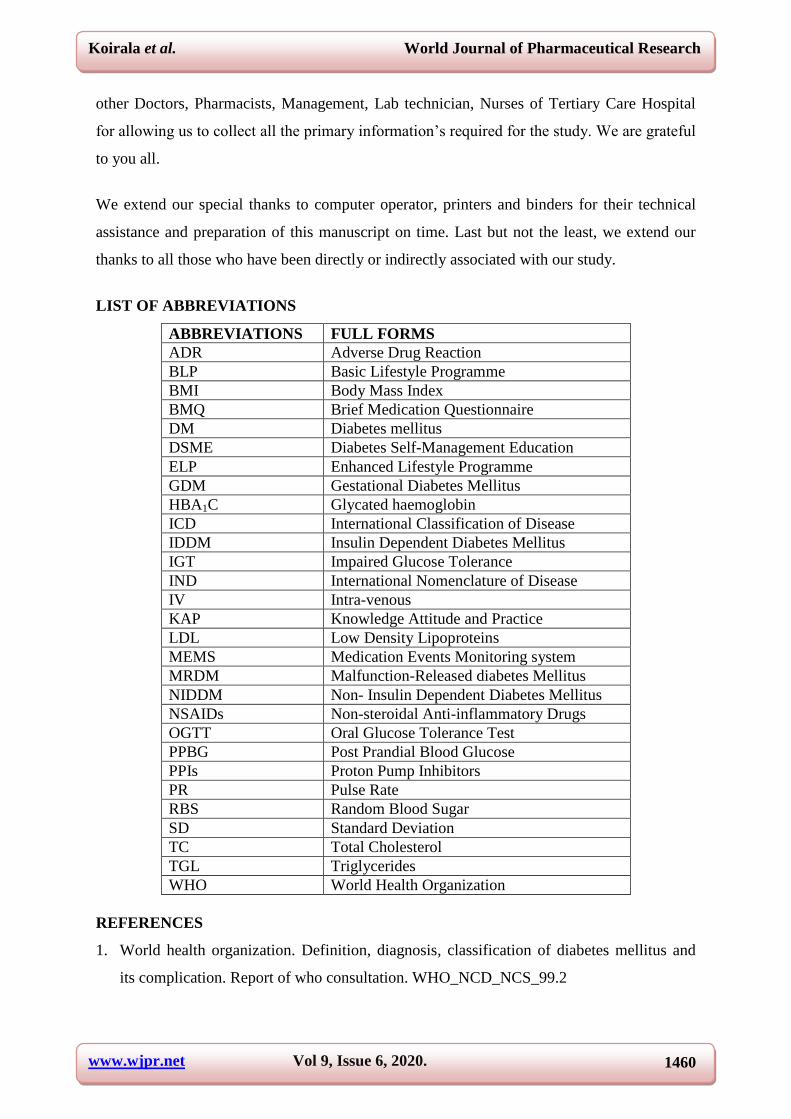
LIST OF ABBREVIATIONS
ABBREVIATIONS FULL FORMS
ADR Adverse Drug Reaction
BLP Basic Lifestyle Programme
BMI Body Mass Index
BMQ Brief Medication Questionnaire
DM Diabetes mellitus
DSME Diabetes Self-Management Education
ELP Enhanced Lifestyle Programme
GDM Gestational Diabetes Mellitus
HBA1C Glycated haemoglobin
ICD International Classification of Disease
IDDM Insulin Dependent Diabetes Mellitus
IGT Impaired Glucose Tolerance
IND International Nomenclature of Disease
IV Intra-venous
KAP Knowledge Attitude and Practice
LDL Low Density Lipoproteins
MEMS Medication Events Monitoring system
MRDM Malfunction-Released diabetes Mellitus
NIDDM Non- Insulin Dependent Diabetes Mellitus
NSAIDs Non-steroidal Anti-inflammatory Drugs
OGTT Oral Glucose Tolerance Test
PPBG Post Prandial Blood Glucose
PPIs Proton Pump Inhibitors
PR Pulse Rate
RBS Random Blood Sugar
SD Standard Deviation
TC Total Cholesterol
TGL Triglycerides
WHO World Health Organization
REFERENCES
1. World health organization. Definition, diagnosis, classification of diabetes mellitus and
its complication. Report of who consultation. WHO_NCD_NCS_99.2
Page 21
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1461
2. McCance DR, Hanson RL, Charles MA, Jacobsson LTH, Pettitt PH et al. Comparision of
tests for glycated haemoglobin and fasting and two hour plasma glucose concentration as
diagnostic method for diabetes. BMJ, 1994; 308: 1323-28.
3. WHO Expert Committee on diabetes mellitus. Second Report. Geneva: WHO, 1980.
Technical Report Series 646.
4. World Health Organization. Diabetes Mellitus: Report of a WHO Study Group. Geneva:
WHO, 1985 Technical Report Series, 727.
5. DeFronzo RA, Bonadonna RC, Ferrannini E. Pathogenesis of NIDDM. In: Alberti
KGMM, Zimmet P, DeFronzo RA, eds. International Textbook of Diabetes Mellitus. 2nd
edn. Chichester: John Wiley, 1997: 635-712.
6. G. Sai Sri Harsha et al. evaluation of antidiabetic therapy, outcomes and impact of patient
counseling on quality of life in type -2 diabetes mellitus in tertiary care hospital indo
American j pharm sci., 2015; 2(4): 870-877.
7. Sriram S., Suresh Damodharan, AkhilaS.Arjun, Latha M. A .and Nandipati
Raghuramcare activities Impact of pharmaceutical on diabetic patients at a private
corporate hospital, 2016; 5: 66-74.
8. Rubin RR, Peyrot M: Quality of life and diabetes. Diabetes Metab Res Rev., 1999; 15:
205-18.
9. Constitution of the World Health Organization. In World Health Organization: Handbook
of Basic Documents. 5th ed. Geneva, Palais des Nations, 1952; 3-20.
10. Rubin RR, Peyrot M, Saudek CS: The effect of a diabetes education program
incorporating coping skills training on emotional well-being and diabetes self-efficacy.
Diabetes Educ., 1993; 19: 210-14.
11. King H, Aubert RE, Herman WH. Global burden of diabetes, 1995-2025: Prevalence,
numerical estimates, and projections. Diabetes care, 1998; 21: 1414- 31.
12. Adibah H, Idris MN Osman ali. Perception and behaviour of diabetic patients on blood
glucose maintenance. Int. J. Diab. Dev. Countries, 1998; 18: 71-74.
13. Karki P, Baral N, Lamsal M et al. Prevalence of NIDDM in urban areas of Eastern Nepal:
A hospital based study. S East Asia J Trop. Med. Public Health, 2000; 31: 163-166.
14. Wee HL, HO HK, Li SC. Public awareness of diabetes mellitus in Singapore. Singapore
Med J., 2002; 43: 128-134.
15. Tan AS, Young LS, Wan S, Wong ML. Patient education in the management of diabetes
mellitus. Singapore Med. J., 1997; 38: 156-60.
Page 22
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1462
16. Baradaran H, Knill-Jones RP, Wallia S, Rodgers A. A controlled trial of the effectiveness
of a diabetes education programme in a multi-ethnic community in Glasgow. BMC Public
Health, 2006; 6: 134.
17. Mohan D, Raj D, Shanthiram CS et al. Awareness and Knowledge of diabetes in
Chennai-The Chennai urban rural epidemiology study [CURES-9]. J Assoc Physicians
India, 2005; 53: 283-285.
18. Sivagnanam G, Namasivayam K, Rajasekaran M, et al. A comparative study of the
knowledge, beliefs and practice of diabetic patients cared for at a teaching hospital (free
service) and those cared for by private practitioners (paid service). Ann NY Acad Sci.,
2002; 958: 416-419.
19. Shera AS, Jawad F, Maqsood A. Prevalence of diabetes in Pakistan. Diabetes Res Clin
Pract, 2007; 76: 219–22.
20. Sheikh MZ. Diabetes Mellitus- The Continuing Challenge. J Coll Physicians Surg Pak,
2004; 14: 63.
21. Zhang X, Geiss LS, Cheng YJ, Beckless GL, Gregg EW, Kahn HS. The missed patients
with diabetes: how access to health care affects the detection of diabetes. Diabetes Care,
2008; 31: 1748–53.
22. Rquibi M, Belasen R. Prevalence and associated risk factors of undiagnosed diabetes
among adult Moroccan Sahraoui women. Public Health Nutr, 2006; 9: 722–7.
23. Brandle M, Zhou H, Smith BRK, Marriot T, Burke R, Jabaei BP, et al. The direct medical
cost of type 2 diabetes. Diabetes care, 2003; 26: 2300–4.
24. Kirigia JM, Sambo HB, Sambo LG, Barry SP. Economic burden of diabetes mellitus in
WHO African region. BMC Int Health Hum Rights, 2009; 9: 6.
25. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HH. 10 year follow up of intensive
glucose control in type 2 diabetes. N Engl J Med, 2008; 359: 1577–89.
26. Johnson ST, Bell GJ, MCcargar LJ, Welsh RS, Bell RC. Improved cardiovascular health
following a progressive walking and dietary intervention for type 2 diabetes. Diabetes
Obes Metab, 2009; 11: 836–43.
27. Gutschall MP, Miller CK, Mitchell DC, Lawrence FR. A randomized behavioral trial
targeting glycemic index improves dietary, weight and metabolic outcomes in patients
with type 2 diabetes. Public Health Nutr, 2009; 23: 1–9.
28. Peyrot M, Rubin RR, Funnell MM, Siminerio LM. Access to diabetes self management
education; Results of national surveys of patients, educators and physicians. Diabetes
Educ, 2009; 35(2): 246–8, 252–6, 258–63.
Page 23
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1463
29. Funnell MM, Brown TL, Childs BP, Haas LB, Hosey GM, Jenson B, et al. National
standards for diabetes self management education. Diabetes Care, 2009; 32(suppl 1):
S87–S94.
30. Van Zyl DG, Rheeder P. Survey on knowledge and attitudes regarding diabetic inpatient
management by medical and nursing staff at kalafong hospital. J Endocrinol Metab
Diabetes South Africa, 2008; 13(3): 90–7.
31. Shera AS, Jawad F, Basit A. Diabetes related knowledge, attitude and practices of family
physicians in Pakistan. J Pak Med Assoc., 2002; 52: 465–70.
32. American diabetes association. Standards of Medical care in Diabetes. Diabetes Care,
2009; 32(suppl 1): S13–S61.
33. Jabbar A, Hameed A, Chawla R, Akhter J. how well do Pakistani patients and physicians
adhere to standards of diabetes care. Int J Diabetes Dev Ctries, 2007; 27: 93–6. [cited
2009 Aug 20]
34. R Malathy, MP Narmadha, S Ramesh, Jose M Alvin, Babu Dinesh Effect of a diabetes
counseling programme on knowledge, attitude and practice among diabetic patients in
Erode district of South India, 2011; 3(1): 65-72.
35. Nally Suman Raj, A.J. Rocky, A. Chandrakanth, C. Praneeth, Dr. B.V.S. Lakshmi, Mr. T.
Praveen Kumar. Evaluation of medication adherence and impact of patient counselling on
quality of life in patients suffering from type 2 diabetes mellitus in a tertiary care teaching
hospital, 2016; 6(8): 6490-6496.
36. Knowledge, Attitude and Practice about Diabetes among Diabetes Patients in Western
Nepal Dinesh K Upadhyay, Subish Palaian, P. Ravi Shankar, Pranaya Mishra, 2008;
23(1): 1-12.
37. King H, Aubert RE, Herman WH. Global burden of diabetes, 1995-2025: Prevalence
numerical estimates, and projections. Diabetes care, 1998; 21: 1414- 31.
38. Badrudin N, Basit A, Hydrie MZI, Hakeem R. Knowledge, Attitude and Practices of
patient visiting a diabetes care unit. Pak J Nutrition, 2002; 1: 99-102.
39. Sivagnanam G, Namasivayam K, Rajasekaran M, et al. A comparative study of the
knowledge, beliefs and practice of diabetic patients cared for at a teaching hospital (free
service) and those cared for by private practitioners (paid service). Ann NY Acad Sci.,
2002; 958: 416-419.
40. B. L. Svarstad, B. A. Chewning, B. L. Sleath, and C. Claesson, “The brief medication
questionnaire: a tool for screening patient adherence and barriers to adherence,” Patient
Education & Counseling, 1999; 37(2): 113–124.
Page 24
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1464
41. McMurray SD, Johnson G, Davis S, Mc-Dougall K. Diabetes education and care
management significantly improve patient outcomes in the dialysis unit. Am J Kidney
Dis., 2002; 40: 566–75.
42. Dr. Sonika Sangra 1, Dr. Nida Nowreen 2, Dr Sunil Sachdev 3. Knowledge, Attitude and
Practice about type 2 Diabetes Mellitus in an adult population attending a Primary Health
Centre in rural Jammu. e-ISSN: 2279-0853, p-ISSN: 2279-0861.
43. Tan AS, Young LS, Wan S, Wong ML. Patient education in the management of diabetes
mellitus. Singapore Med. J., 1997; 38: 156-60.
44. Palaian S, Chhetri AK, Prabhu M, Rajan S, Shankar PR. Role of pharmacist in counseling
diabetes patients. Internet J Pharmacol, 2005; 4: 1-13.
45. Shah VN, Kamdar PK, Shah N. Assessing the knowledge, attitudes and practice of type 2
diabetes among patients of Saurashtra region, Gujarat. Int J Diabetes Dev Ctries., 2009;
29: 118–22.
46. Murata GH, Shaha JH, Adam KD, Wendel CS, Bokhari SU, Solvas PA, et al. Factors
affecting diabetes knowledge in Type 2 diabetic veterans. Diabetologia, 2003; 46:
1170–8.
47. Van der Does FE1, De Neeling JN, Snoek FJ, Kostense PJ, Grootenhuis PA, Bouter LM,
Heine RJ. Symptoms and well-being in relation to glycemic control in type II diabetes,
1996 Mar; 19(3): 204-10.
48. Funnell MM, Brown TL, Childs BP, Haas LB, Hosey GM, Jenson B, et al. National
standards for diabetes self management education. Diabetes Care, 2009; 32(suppl 1):
S87–S94.
49. Tham KY, Ong JJY, Tan DkL, How KY. How much do diabetic patients know about
diabetes mellitus and complications? Ann Acad Med Singapore, 2004; 33(4): 503–9.
50. Murugesan N, Snehalatha C, Shobana R, Roglic G, Ramachandran A. awareness about
diabetes and its complications in the general and diabetic population in a city in southern
India. Diabetes Res Clin Prac., 2007; 77: 433–7.
51. Naheed G.Knowledge, Attitude and practices of type 2 patients. J Auyb Med Coll
Abbotabad, 2010; 22(3).
52. Karam Padma, Samir D Bele, Trupti N Bodhare, Sameer Valsangkar. Evaluation of
knowledge and selfcare practices in diabetic patient and their role in disease management.
pISSN: 0976 3325 eISSN: 2229 6816.
53. Ramachandran A, Snehalatha C, Baskar AD, Mary S, Kumar CK, Selvam S, et al. 3.
Temporal changes in prevalence of diabetes and impaired glucose tolerance associated
Page 25
www.wjpr.net Vol 9, Issue 6, 2020.
Koirala et al. World Journal of Pharmaceutical Research
1465
with lifestyle transition occurring in the rural population in India. Diabetologia, 2004; 47:
860-5.
54. Norris SL, Nichols PJ, Caspersen CJ, Glasgow RE, Engelgau MM, Jack L, et al.
Increasing diabetes self- management education in community settings. A systematic
review. Am J Prev Med, 2002; 22: 39-66.
55. Ciechanowski P, Russo J, Katon W, Von Korff M, Ludman E, Lin E, Simon G, et al.
Influence of patient attachment style on self-care and outcomes in diabetes. Psychosom
Med, 2004; 66: 720-8.
56. Johnson ST, Bell GJ, MCcargar LJ, Welsh RS, Bell RC. Improved cardiovascular health
following a progressive walking and dietary intervention for type 2 diabetes. Diabetes
Obes Metab, 2009; 11: 836–43.
57. Gottipati Mahesh et al. Role of clinical pharmacist in the management of diabetic
patients. International Journal of Comprehensive Pharmacy, 2011; 02.
58. Bakyaraj R, Rajendran NN, Narmadha MP “ Effect of Insulin Therapy in Type-2
Diabetes in Improving Â-Cell Function and Glycemic Control Compared with Oral Anti-
Diabetic Agents with or without Insulin in Routine Clinical Practice” Indian J. Pharm.
Pract., 2010; 3(1): 25-32.
59. Suppapitiporn S, Chindavijak B, Onsanit S. Effect of diabetes drug counseling by
pharmacist, diabetic disease booklet and special medication containers on
glycemiccontrol of type 2 diabetes mellitus: a randomized controlled trial. J Med Assoc
Thai., 2005; 88 Suppl 4: S134-41.