4/11/2016 1 Controversies in Coronary Revascularization Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization Laboratory, Emory University Hospital Atlanta CCU April 15, 2016 • Medtronic, PI SHEAR STENT Trial • Abbott Vascular , PI Restoration Study (Subanalysis of ABSORB III Img.) • Gilead, PI MARINA Trial Giliead • Volcano Therapeutics, Research Grants and Steering Comm ADVISE II • St. Jude Medical, Research Grants and Steering Comm ILUMIEN III • American Heart Association, Mentor Fellowship Awards • National Institute of Health, Co-I NIH ROI/PPG • American College of Cardiology , Deputy Editor, JACC Interventions Grant Support Disclosures
Transcript
4/11/2016
1
Controversies in Coronary
Revascularization
Habib Samady MD FACC FSCAI Professor of Medicine
Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization Laboratory, Emory University Hospital
Atlanta CCU
April 15, 2016
• Medtronic, PI SHEAR STENT Trial
• Abbott Vascular, PI Restoration Study (Subanalysis of ABSORB III Img.)
• Gilead, PI MARINA Trial Giliead
• Volcano Therapeutics, Research Grants and Steering Comm ADVISE II
• St. Jude Medical, Research Grants and Steering Comm ILUMIEN III
• American Heart Association, Mentor Fellowship Awards
• National Institute of Health, Co-I NIH ROI/PPG
• American College of Cardiology, Deputy Editor, JACC Interventions
Grant Support
Disclosures
4/11/2016
2
• SIHD
- Accepted Indications for revascularization
- Controversies in revascularization - How much Ischemia to Revascularize
- How to revascularize 3 VD: CABG vs PCI vs HCR
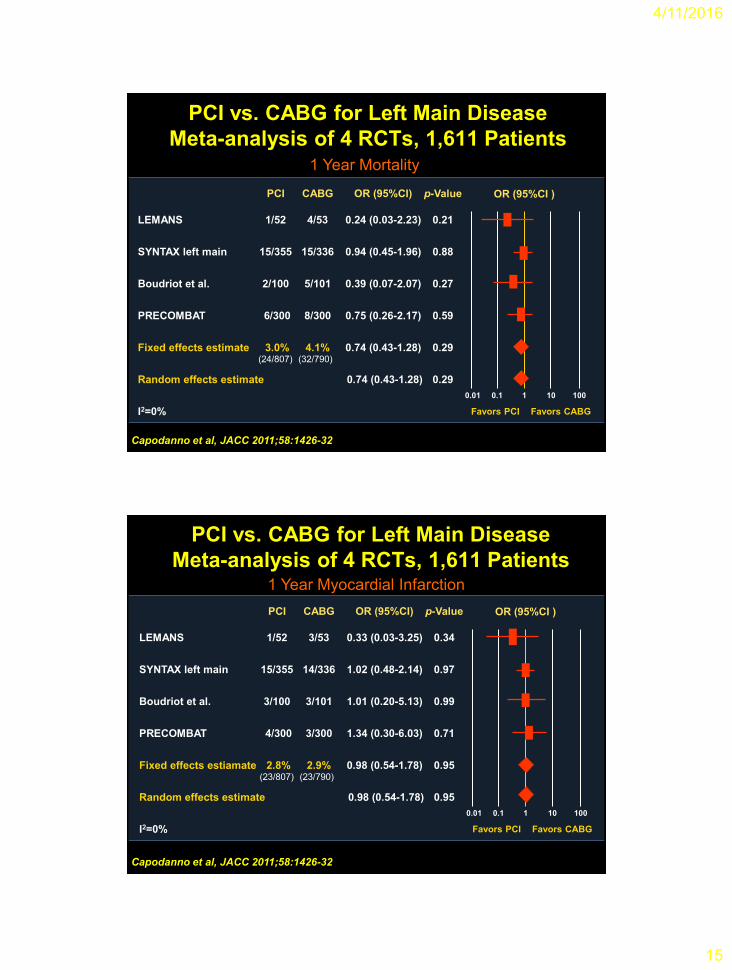
- How to revascularize LMCA: CABG vs PCI
• ACS - Accepted Indications for revascularization
- Controversies in revascularization - Non culprit vessel in STEMI: PCI vs Med tx.
- Culprit vessel in STEMI: Angio vs OCT guided
Controversies in Coronary
Revascularization
• SIHD
- Accepted Indications for revascularization
- Controversies in revascularization - How much Ischemia to Revascularize
- How to revascularize 3 VD: CABG vs PCI vs HCR
- How to revascularize LMCA: CABG vs PCI
• ACS - Accepted Indications for revascularization
- Controversies in revascularization - Non culprit vessel in STEMI: PCI vs Med tx.
- Culprit vessel in STEMI: Angio vs OCT guided
Controversies in Coronary
Revascularization
4/11/2016
3
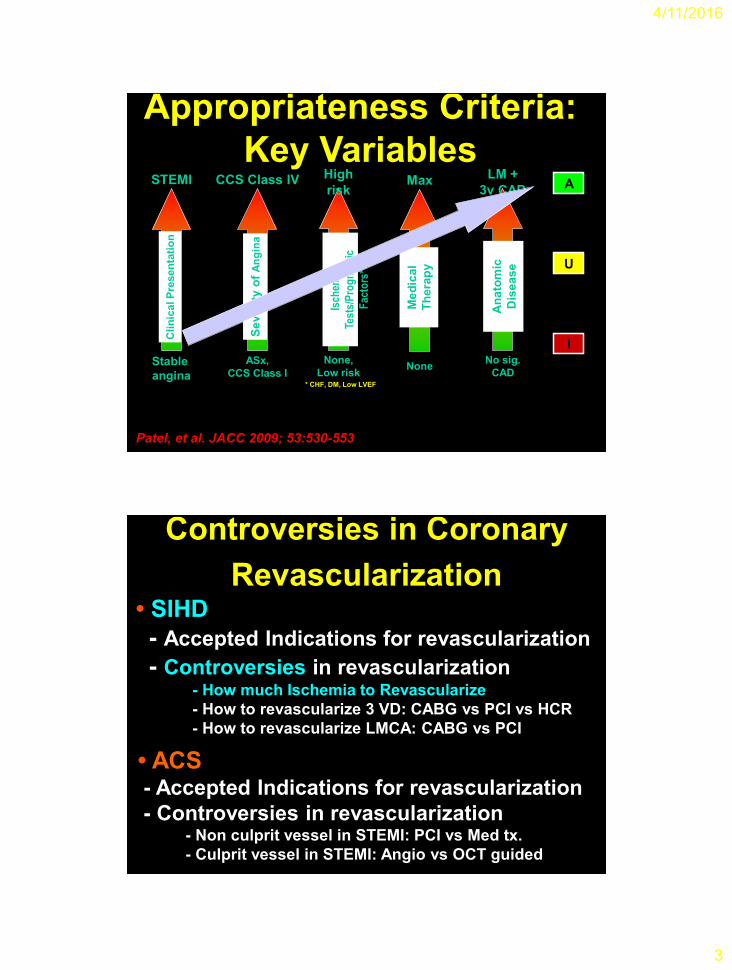
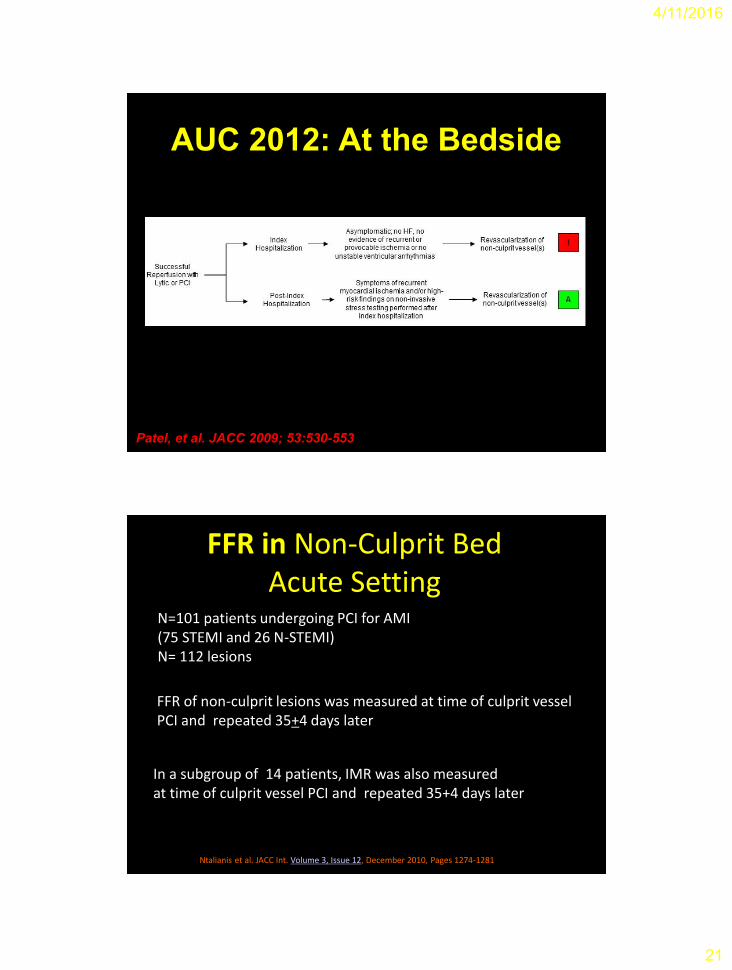
Patel, et al. JACC 2009; 53:530-553
Cli
nic
al P
resen
tati
on
Stable
angina
STEMI
Se
ve
rity
of
An
gin
a
ASx,
CCS Class I
CCS Class IV
Isch
emia
Test
s/P
rog
no
stic
Fac
tors
* None,
Low risk
High
risk
None
Max
Me
dic
al
Th
era
py
No sig.
CAD
LM +
3v CAD
An
ato
mic
D
ise
as
e
* CHF, DM, Low LVEF
A
U
I
Appropriateness Criteria:
Key Variables
• SIHD
- Accepted Indications for revascularization
- Controversies in revascularization - How much Ischemia to Revascularize
- How to revascularize 3 VD: CABG vs PCI vs HCR
- How to revascularize LMCA: CABG vs PCI
• ACS - Accepted Indications for revascularization
- Controversies in revascularization - Non culprit vessel in STEMI: PCI vs Med tx.
- Culprit vessel in STEMI: Angio vs OCT guided
Controversies in Coronary
Revascularization
4/11/2016
4
Courage Trial
Boden et al. NEJM. 2007; Volume 356:1503-1516
N-2287 pt
Stable angina
6.7%
3.7%3.3%
1.0%
2.9%
4.8%
1.8% 2.0%
0%
2%
4%
6%
8%
10% Medical Rx Revasc
Survival Benefit with Revascularization
Stratified by Ischemic Risk
% Total Myocardium Ischemic
1- 5% 5-10% 11-20% >20%
Card
iac D
eath
Rate
1331 56 718 109 545 243 252 267
P <.0001
Hachamovitch et al Circulation. 2003; 107:2900-2907
N=10 627 undergoing MPI with 1.9±0.6 year f/u propensity matched.
4/11/2016
5
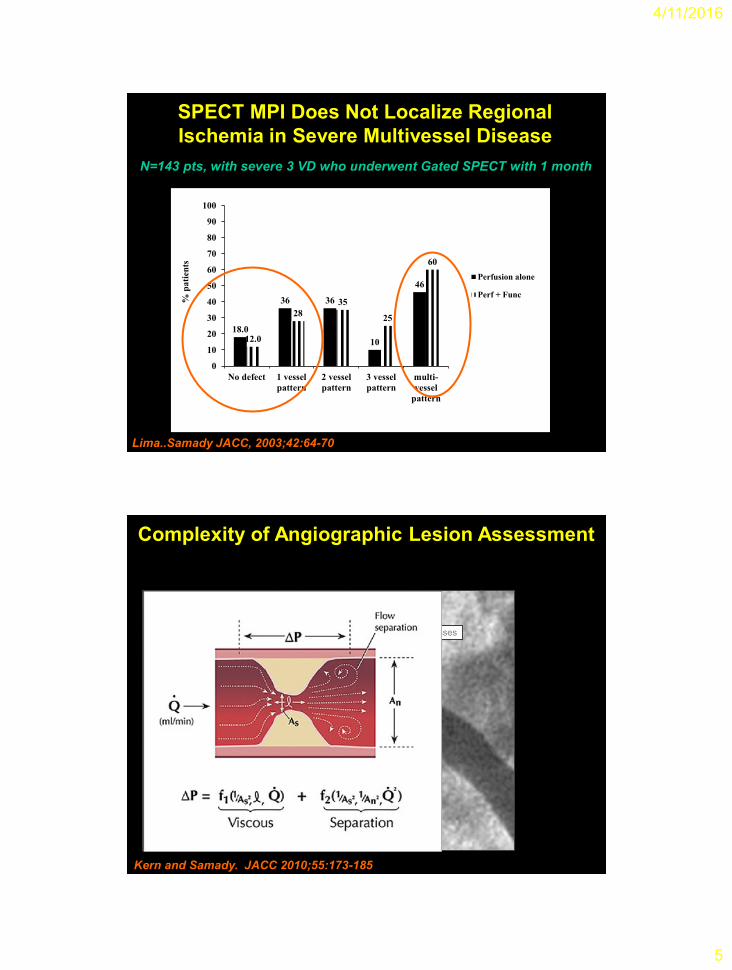
18.0
36 36
10
46
12.0
28
35
25
60
0
10
20
30
40
50
60
70
80
90
100
No defect 1 vessel
pattern
2 vessel
pattern
3 vessel
pattern
multi-
vessel
pattern
% p
ati
ents
Perfusion alone
Perf + Func
Lima..Samady JACC, 2003;42:64-70
N=143 pts, with severe 3 VD who underwent Gated SPECT with 1 month
SPECT MPI Does Not Localize Regional
Ischemia in Severe Multivessel Disease
Entrance effects Separation losses
Friction loss
Kern and Samady. JACC 2010;55:173-185
Complexity of Angiographic Lesion Assessment
4/11/2016
6
Pa Pd
NHJ Pijls et al. Circulation 1993
Fractional Flow Reserve
Validation of FFR For Intermediate
Lesion Assessment
Kern and Samady. JACC 2010;55:173-185
4/11/2016
7
Flow Chart
Stable CAD patients scheduled for 1, 2 or 3 vessel DES-PCI
N = 1220
FFR in all target lesions
When all FFR > 0.80 (n=332)
MT
At least 1 stenosis with FFR ≤ 0.80 (n=888)
Randomization 1:1
PCI + MT MT
Follow-up after 1, 6 months, 1, 2, 3, 4, and 5 years