This article was downloaded by: [Memorial University of Newfoundland] On: 18 July 2014, At: 10:47 Publisher: Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Immunoassay and Immunochemistry Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/ljii20 EVALUATION OF DIAGNOSTIC POTENTIAL OF Rv3803c AND Rv2626c RECOMBINANT ANTIGENS IN TB ENDEMIC COUNTRY PAKISTAN Sajjad Ashraf a , Muhammad Arif Nadeem Saqib b , Mirza Zahid Sharif c , Aamer Ali Khatak d , Sadiq Noor Khan e , Salman Akbar Malik d , Sabira Tahseen f & Azra Khanum e a Pakistan Medical Research Council , Faisalabad , Pakistan b Pakistan Medical Research Council , Islamabad , Pakistan c Department of Zoology , PMAS-Arid Agriculture University Rawalpindi , Pakistan d Department of Biochemistry and Molecular Biology , Quaid-i-Azan University , Islamabad , Pakistan e Department of Biochemistry , PMAS-Arid Agriculture University Rawalpindi , Pakistan f National TB Control Program , Islamabad , Pakistan Accepted author version posted online: 08 Aug 2013.Published online: 02 Dec 2013. To cite this article: Sajjad Ashraf , Muhammad Arif Nadeem Saqib , Mirza Zahid Sharif , Aamer Ali Khatak , Sadiq Noor Khan , Salman Akbar Malik , Sabira Tahseen & Azra Khanum (2014) EVALUATION OF DIAGNOSTIC POTENTIAL OF Rv3803c AND Rv2626c RECOMBINANT ANTIGENS IN TB ENDEMIC COUNTRY PAKISTAN, Journal of Immunoassay and Immunochemistry, 35:2, 120-129, DOI: 10.1080/15321819.2013.824897 To link to this article: http://dx.doi.org/10.1080/15321819.2013.824897 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content
Transcript
This article was downloaded by: [Memorial University of Newfoundland]On: 18 July 2014, At: 10:47Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Immunoassay andImmunochemistryPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/ljii20
EVALUATION OF DIAGNOSTIC POTENTIALOF Rv3803c AND Rv2626c RECOMBINANTANTIGENS IN TB ENDEMIC COUNTRYPAKISTANSajjad Ashraf a , Muhammad Arif Nadeem Saqib b , Mirza Zahid Sharifc , Aamer Ali Khatak d , Sadiq Noor Khan e , Salman Akbar Malik d ,Sabira Tahseen f & Azra Khanum ea Pakistan Medical Research Council , Faisalabad , Pakistanb Pakistan Medical Research Council , Islamabad , Pakistanc Department of Zoology , PMAS-Arid Agriculture UniversityRawalpindi , Pakistand Department of Biochemistry and Molecular Biology , Quaid-i-AzanUniversity , Islamabad , Pakistane Department of Biochemistry , PMAS-Arid Agriculture UniversityRawalpindi , Pakistanf National TB Control Program , Islamabad , PakistanAccepted author version posted online: 08 Aug 2013.Publishedonline: 02 Dec 2013.
To cite this article: Sajjad Ashraf , Muhammad Arif Nadeem Saqib , Mirza Zahid Sharif , AamerAli Khatak , Sadiq Noor Khan , Salman Akbar Malik , Sabira Tahseen & Azra Khanum (2014)EVALUATION OF DIAGNOSTIC POTENTIAL OF Rv3803c AND Rv2626c RECOMBINANT ANTIGENS IN TBENDEMIC COUNTRY PAKISTAN, Journal of Immunoassay and Immunochemistry, 35:2, 120-129, DOI:10.1080/15321819.2013.824897
To link to this article: http://dx.doi.org/10.1080/15321819.2013.824897
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content
should not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
EVALUATION OF DIAGNOSTIC POTENTIAL OF Rv3803c ANDRv2626c RECOMBINANT ANTIGENS IN TB ENDEMIC COUNTRYPAKISTAN
Sajjad Ashraf,1 Muhammad Arif Nadeem Saqib,2 Mirza Zahid Sharif,3
Aamer Ali Khatak,4 Sadiq Noor Khan,5 Salman Akbar Malik,4
Sabira Tahseen,6 and Azra Khanum5
1Pakistan Medical Research Council, Faisalabad, Pakistan2Pakistan Medical Research Council, Islamabad, Pakistan3Department of Zoology, PMAS-Arid Agriculture University Rawalpindi, Pakistan4Department of Biochemistry and Molecular Biology, Quaid-i-Azan University,Islamabad, Pakistan5Department of Biochemistry, PMAS-Arid Agriculture University Rawalpindi, Pakistan6National TB Control Program, Islamabad, Pakistan
& To overcome and eliminate tuberculosis (TB), definitive, reliable, and rapid diagnosis is manda-tory. Presently, the diagnostic potential of acute and latent stage TB specific antigens i.e., Rv3803cand Rv2626c was determined. Immunogenic recombinant genes of Rv3803c and Rv2626c antigenswere cloned in bacterial expression vector pET23b and expressed product was purified. The homogen-eity and structural integrity was confirmed by Western blot analysis. Diagnostic potential of Rv3803cand Rv2626c antigens was analyzed using the sera of 140 active TB patients (AFB smear positive)by indirect ELISA. Ten patients of leprosy and 94 healthy individuals were taken as disease and nor-mal control respectively. The data was analyzed using R statistical package. The sensitivity and speci-ficity of Rv3803c in active TB patients was of 69.3% and 76.4% respectively with an area underROC curve of 0.77, whereas sensitivity and specificity of Rv2626c 77.1% and 85.1%, respectively.The area under ROC curve of Rv2626c was 0.89 which was significantly higher than Rv3803c(p< 0.0001). Recombinant antigens Rv3803c and Rv2626c have potential to be used as diagnosticmarkers for TB and need to evaluate with other antigens for differential diagnosis of TB.
Keywords ELISA, Rv3803c, Rv2626c
INTRODUCTION
Tuberculosis (TB) is caused by Mycobacterium tuberculosis (M. tb) which isa growing health problem in the developing countries. It usually affects the
Address correspondence to Azra Khanum, Department of Biochemistry, PMAS-Arid AgricultureUniversity Rawalpindi, Pakistan. E-mail: [email protected]
Journal of Immunoassay and Immunochemistry, 35:120–129, 2014Copyright # Taylor & Francis Group, LLCISSN: 1532-1819 print/1532-4230 onlineDOI: 10.1080/15321819.2013.824897
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
lungs causing pulmonary TB but can also affect other sites, resulting inextra pulmonary TB. TB is also more common among men and affectsmostly adults in the economically productive age groups; around two-thirdof cases are estimated to occur among people aged 15–59 years. About 8.8million incident cases of TB were reported, among which 1.1 million TBpatients were died. An additional 0.35 million deaths occurred inHIV-associated TB patients.[1] TB cases have increased in both industria-lized and developing countries.[2]
Early and reliable diagnostic tests are required for the proper treatmentand to reduce the risk of transmission to community. Patients are usuallydiagnosed at a great cost after weeks to months of waiting and majorityremained undiagnosed. Sputum microscopy for AFB by Ziehl-Neelsen(ZN) staining is being used since the 1880s and has an important role inearly diagnosis. However, this test has low sensitivity and can only detectsroughly half of all active cases of TB.[3] Mantoux tuberculin skin test(TST) is another routine method for detecting M. tb infection which isnon specific.[4] The sputum culture technique has much higher sensitivityand specificity but it requires 3–4 weeks for results which is estimated to beresponsible for transmission of TB in 20% of cases.[5] The sensitivity andspecificity of chest X-Ray (CXR) depends on the intensity and the presen-tation of the disease, immune status of the patient, gender, quality of thefilm, and more importantly, on experience and the interpretation skill ofthe reader. These factors make CXR unable to distinguish smear-positiveTB from smear negative TB.[6] Polymerase chain reaction (PCR), BACTEC,QuantiFERON-TB Gold, and T-SPOT.TB are advanced techniques whichare rapid, sensitive, and specific. However, these tests need extra expertise.Similarly the cost and non availability of all these tests have limited theiruses.[7,8] Therefore, serological methods represent a good alternative toolto diagnose TB in a simple, fast, and cheaper way.[9]
Antigens detection provides direct evidence of the presence of diseaseand is important to diagnose TB at its exact stage.[10] Different myco-bacterial antigens have been used for diagnosis of TB. Rv3803c antigenis secreted by M. tb in acute stage and is highly immunodominant.Ramlingam et al.[11] reported the sensitivity of 71% and specificity of95% of this antigen in ELISA against TB. Similarly this antigen was recog-nized by serum antibodies in 80% of TB patients.[12] Antigen Rv2626c isa latent stage antigen and is immunogenic as it has strong humoral andcellular Th1-type response.[13] Goletti et al.[14] used Rv2626c in the IGRAsfor the diagnosis of recent infection and found no significant resultsbecause it is a latent stage antigen and cannot be used for the diagnosisof recent infection.
Pakistan is among the world’s highest TB burden countries and isranked fifth. The province Punjab alone bears the burden of about 60%
Diagnostic Potential of TB Specific Antigens 121
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
of TB cases.[16] Incidence and prevalence of the disease in Pakistan is 181and 329=100,000 habitants per year, respectively.[17]
The objective of this article was to see antigenic response of Rv3803cand Rv2626c antigens in newly diagnosed TB patients and patients whowere under treatment, which may be helpful in developing some techniquefor early diagnosis of the disease.
MATERIALS AND METHODS
Study Subjects
A total of 140 active TB patients who were first time diagnosed for TB bysputum AFB smear test and had never taken TB treatment were enrolled atNational TB Center (NTC) Rawalpindi. Ten patients of leprosy and 94healthy individuals were taken as disease and normal control respectively.After taking informed consent, 5mL of blood sample was drawn as per stan-dard protocol. Further out of 140 patients, 16 were followed for 6 monthsand blood was taken on each visit=month. The blood was centrifuged forplasma which was then stored at �80�C until used for ELISA. This studywas approved by Ethics Committee of Pir Mehr Ali Shah Arid AgricultureUniversity Rawalpindi.
Antigens
Antigenic genes of M. tb already cloned in bacterial expression vectorpET23b were obtained from TB Resource Centre, Colorado State Univer-sity (Boulder, CO, USA). Two immunogenic recombinant genes (Rv3803cand Rv2626c) were selected for this study which were expressed andpurified as described by Awan et al.[18] The homogeneity and structuralintegrity of both recombinant proteins were checked by Western blot analy-sis. The concentration of both antigens were measured by BCA proteinassay (Novagen, San Diego, CA, USA).
ELISA
The protocol of indirect ELISA was adopted from Goldsby et al.[19] withslight modifications. One hundred micro liter of antigens Rv2626c andRv3803c having the concentration of 2mg=mL in PBS (pH 7.4) was coatedon 96 wells ELISA plates separately (Corning Incorporate, New York, NY,USA). The contents of both plates were discarded after overnight incubationat 4�C and wells were washed three times with washing buffer. The blockingbuffer i.e., 3% BSA was added in each well, incubated at 37�C for 2hr and
122 S. Ashraf et al.
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
washed. Plasma samples diluted 1:100 were added and after incubation at37�C for 1hr, wells were washed. The secondary antibodies, i.e., antihumanimmunoglobulin M (IgM) (Calbiochem-Merck, Billerica, MA, USA) wasadded in plate coated with Rv3803c antigen while antihuman immunoglob-ulin G (IgG) (Invitrogen, Billerica, MA, USA) was added in plates coated withRv2626c antigen. Both secondary antibodies were conjugated with alkalinephosphatase enzyme (1:3000 in phosophate buffer saline Tween 20). Theplates were again incubated at 37�C for 1hr. The wells were washed thriceand freshly prepared substrate (175mg tablet containing 5mg of para nitrophenyl phosphate (p-NPP) in 10mL of 0.1M diethanolamine buffer) wasadded. The plates were kept at 37�C for 30min in the dark. The reactionwas stopped by adding 100uL of stop solution (0.75M NaOH) and absor-bance was measured at 405nm using ELISA reader (GDV Roma, Itlay).
Statistical Analysis
The data was analyzed using R statistical package (R foundation forstatistical computing, Vienna, Austria). Receiver operating curves were con-structed by R statistical package to find out cutoff value, sensitivity, speci-ficity, positive predictive value (PPV), and negative predictive value(NPV). Sample which had optical density (OD) more than cutoff valuewere considered positive. Statistical comparison between the areas coveredby two ROC curves was analyzed by statistical software Med. Calc, version12.1.4 (Mariakerke, Belgium).
RESULTS
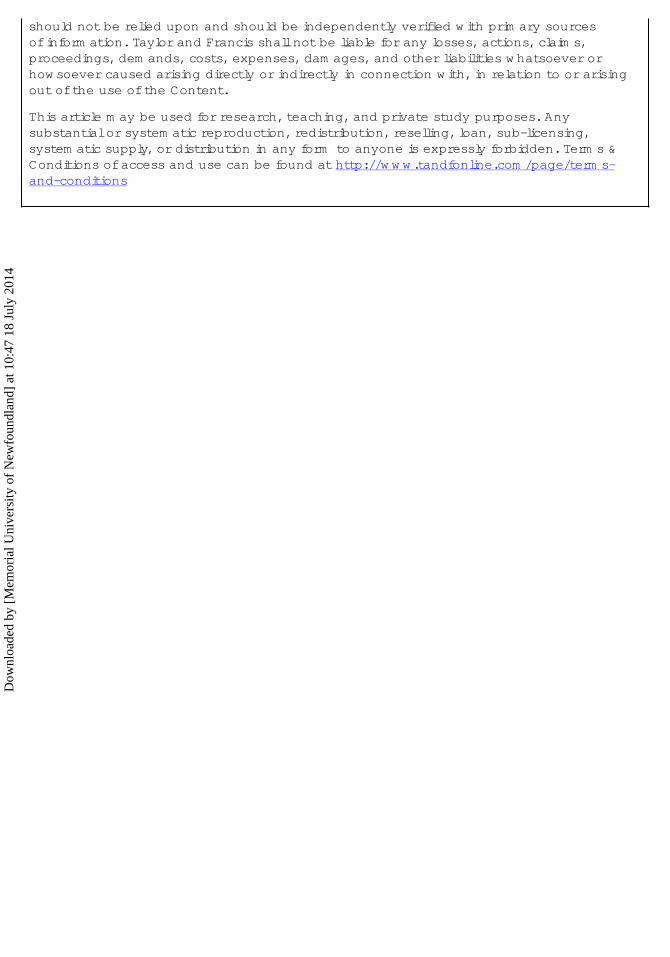
The purified products of both immunogenic recombinant genes(Rv3803c and Rv2626c) were analyzed by Western blot showing completehomogeneity and structural integrity (Figure 1). The concentrations ofpurified products of Rv3803c and Rv2626c antigens were 990 mg=mL and1035 mg=mL, respectively. Both antigens (Rv3803c and Rv2626c) were eval-uated for their serological response in active TB patients (n¼ 140), leprosypatients (n¼ 10), and healthy control (n¼ 90).
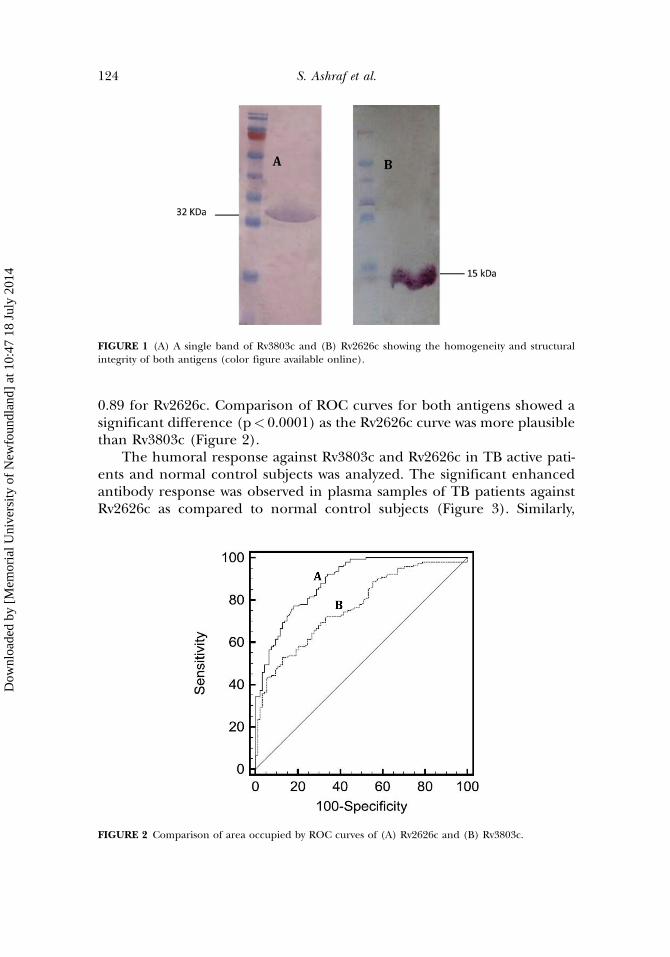
A cutoff value of 0.46 was determined for Rv3803c by ROC analysis. Thesensitivity and specificity of Rv3803c in active TB patients was 69.3% and76.4%, respectively, with a PPV of 76.9% and 68.6% NPV. Out of 10 leprosypatients only 1 was positive for Rv3803c. In case of Rv262c, the cutoff valuewas 0.61. The sensitivity and specificity of Rv2626c in active Tb patients was77.1% and 85.1%, respectively with 86.4% PPV and 75.2% NPV. None of theleprosy patient was positive for this antigen showing no cross reactivity ofRv2626c. The area under ROC curve of Rv3803c was 0.77 while it was
Diagnostic Potential of TB Specific Antigens 123
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
0.89 for Rv2626c. Comparison of ROC curves for both antigens showed asignificant difference (p< 0.0001) as the Rv2626c curve was more plausiblethan Rv3803c (Figure 2).
The humoral response against Rv3803c and Rv2626c in TB active pati-ents and normal control subjects was analyzed. The significant enhancedantibody response was observed in plasma samples of TB patients againstRv2626c as compared to normal control subjects (Figure 3). Similarly,
FIGURE 2 Comparison of area occupied by ROC curves of (A) Rv2626c and (B) Rv3803c.
FIGURE 1 (A) A single band of Rv3803c and (B) Rv2626c showing the homogeneity and structuralintegrity of both antigens (color figure available online).
124 S. Ashraf et al.
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
FIGURE 3 Scatter plot of humoral responses against (A) Rv3803c and (B) Rv2626c in plasma of TBpatients and normal individuals. Each dot represents the 4O.D where blue representing TB patientswhile red normal healthly individuals (color figure available online).
FIGURE 4 A graphical representation of antibody response against Rv2626c of TB patients who wereon anti-tuberculosis therapy under DOTs program (color figure available online).
Diagnostic Potential of TB Specific Antigens 125
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
the humoral response against Rv3803c and Rv2626c in 16 TB patients whowere on anti-tuberculosis therapy under DOT program was assessed for 6months. No significant variation was seen in antibody titer againstRv3803c (data not shown). However, in the case of Rv2626c a sharpincrease in antibody titer was observed at second month of therapy. There-after, a constant decrease was found until the fifth month which remainedsame at the sixth month (Figure 4).
DISCUSSION
Despite much advancement in diagnosis, rapid TB detection is stillproblematic in TB endemic countries. Antibodies detection against M. tbantigens in sero-assays is promising in this regard. It has been reported thatTB specific antigens are good candidate for the rapid and early detection.Diagnostic potential of M. tb specific purified recombinant antigens hasbeen evaluated in number of studies depending either on nature of anti-gens i.e., secretory antigens, lipid containing antigens or depending onTB stage, i.e., acute stage antigens, latent stage antigens, and inactive (past)TB.[20] Performance of serological assays based on these antigens variedsignificantly with test sensitivities ranging from 10–90% and specificitiesranging from 47–100%.[21] Despite this, interest in developing serodiagnos-tic methods is increasing because detection of antibody is rapid, simple,and relatively inexpensive.[22]
In this study, we have analyzed the diagnostic potentials of Rv3803c andRv2626c antigens using indirect ELISA. The immunogenic characteristic ofboth antigens were already reported.[13,23] The data of this study demon-strated that sensitivity of Rv3803c in active TB patient was 69.3% for detec-tion of IgM antibodies which was consistent to previous reports of Almeidaet al.[22] and Ramalingam et al.[21] However, these values are higher as com-pared to sensitivity of 13% and 63% reported by Bethunaickan et al.[23] andSteingart et al.,[24] respectively.
It was observed that in 43 active TB patients, antibody response againstRv3803c was below the cutoff value. As IgM is acute stage antibody whichdiminished with prolonged onset of disease and IgG started developing.[25]
This might be possible reason as there is an average delay of 8 weeks indiagnosis of TB in Pakistan.[26] A significant difference in serologicalresponse against Rv3803c was observed in active TB patients and healthyindividuals indicating its potential as serological marker.
No significant difference was observed in antibody titer against Rv3803cfor 06 month in patients who were on anti-tuberculosis treatment. Similarfinding was also reported by Khan et al.[27] Ten control plasma from lep-rosy patients was also included to analyze the cross reactivity and only
126 S. Ashraf et al.
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
one patient was found positive. Rv3803c is a precursor of Ag85 complex,and this antigen also find in other environmental bacteria as well as inM. Leprae.[5] Therefore, this cross reactivity in leprosy patient might bedue to antigen of Ag85 complex.
The sensitivity of Rv2626c antigen in active TB patients was 77.1%.Although Rv2626c antigen is encoded by gene which is a member of dor-mancy regulon but it has been reported that this antigen was associatedwith active TB and elicited a strong antibody response,[28] which is consist-ent to our findings. Bashir et al.[29] revealed that Rv2626c antigen modu-lates macrophages effecter functions elicits strong humoral immuneresponse against TB in mice. Similarly scatter chart showed that Rv2626 eli-cited high humoral response in active TB patients as compared to normalindividuals. Further no antibody cross reactivity was observed in leprosypatients against Rv2626c. This indicates that Rv2626c has strong potentialto be used for the detection of TB. The six-month antibody responseagainst Rv2626c showed maximum peak in the second month whichdecreased gradually and became constant at the fifth month of therapy.Similar findings were also reported by Azzurri[30] in which antibody levelagainst Rv2626c decreased during therapy. However, individually in fewpatients IgG antibodies level did not increase in the second month andremained constant throughout the treatment. The reason for such kindof pattern observed is unclear. According to Abebe et al.,[31] antibodiesresponse to antigen varied greatly from patient to patient and variationof antibody level among different individuals might be due different stagesof disease and their body immune response to treatment.
It is concluded that Rv3803c and Rv2626c antigens have strong humoralresponse in active TB patients however this was prominent for Rv2626c.Furthermore, Rv2626c may be used as a prognostic marker for treatmentoutcome as it showed decreasing trend in antibody response in patientswho were on anti-tuberculosis therapy.
REFERENCES
1. World Health Organization (WHO). WHO Report. Global Tuberculosis Control 2011. Available athttp://www.who.int/tb/publications/global_report/en/ (accessed on January 2012).
2. Zaman, K. Tuberculosis: A Global Health Problem. J. Health. Popul. Nutr. 2010, 28(2), 111–113.3. Perkins, M. D.; Roscigno, G.; Zumla, A. Progress towards Improved Tuberculosis Diagnostics for
Developing Countries. Lancet 2006, 18, 367(9514), 942–943.4. Donald, P. R. Childhood Tuberculosis: Out of Control? Curr. Opin. Pulm. Med. 2002, 8(3),
178–182.5. Kumar, G.; Dagur, P. K.; Singh, P. K.; Shankar, H.; Yadav, V. S.; Katoch, V. M.; Bajaj, B.; Gupta, R.;
Sengupta, U.; Joshi, B. Serodiagnostic Efficacy of Mycobacterium Tuberculosis 30=32-kDa MycolylTransferase Complex, ESAT-6, and CFP-10 in Patients with Active Tuberculosis. Arch. Immunol. Ther.Exp. 2010, 58(1), 57–65.
Diagnostic Potential of TB Specific Antigens 127
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
6. van Cleeff, M. R. A.; Kivihya-Ndugga, L. E.; Meme, H.; Odhiambo, J. A.; Klatser, P. R. The Roleand Performance of Chest X-ray for the Diagnosis of Tuberculosis: A Cost-effectiveness Analysisin Nairobi, Kenya. BMC. Infect. Dis. 2005, 12(5), 111.
7. Tortoli, E.; Palomino, J. C. New Diagnostic Methods. In Tuberculosis 2007: From Basic Science to PatientCare, 1st Ed.; Palomino, J.C., Leao, S.C., Ritacco, V., Eds.; Texbook.com: Belgium, 2007.
8. Bienek, D. R.; Chang, C. K. Evaluation of an Interferon-Gamma Release Assay, T-SPOT.TB, in aPopulation with a Low Prevalence of Tuberculosis. Int. J. Tuberc. Lung. Dis. 2009, 13(11), 1416–1421.
9. Hernandez-Pando, R.; Castanon, M.; Espitia, C.; Lopez-Vidal, Y. Recombinant BCG VaccineCandidates. Curr. Mol. Med. 2007, 7(4), 365–372.
10. Khomenko, A. G.; Bayensky, A. V.; Chernousova, L. N.; Kulikovskaya, N. V.; Demianenko, N. V.;Litvinov, V. I. Serodiagnosis of Tuberculosis: Detection of Mycobacterial Antibodies and Antigens.Int. J. Tuberc. Lung. Dis. 1996, 77(6), 510–515.
11. Ramalingam, B.; Baulard, A. R.; Locht, C.; Narayanan, P. R.; Raja, A. Cloning, Expression, andPurification of the 27 kDa (MPT51, Rv3803c) Protein of Mycobacterium Tuberculosis. Protein. Expr.Purif. 2004, 36(1), 53–60.
12. Achkar, J. M.; Dong, Y.; Holzman, R. S.; Belisle, J.; Kourbeti, I. S.; Sherpa, T.; Condos, R.;Rom, W. N.; Laal, S. Mycobacterium Tuberculosis Malate Synthase and MPT51 basedSerodiagnostic Assay as an Adjunct to Rapid Identification of Pulmonary Tuberculosis. Clin.Vaccine. Immunol. 2006, 13(11), 1291–1293.
13. Roupie, V.; Romano, M.; Zhang, L.; Korf, H.; Lin, M. Y.; Franken, K. L.; Ottenhoff, T. H.; Klein, M. R.;Huygen, K. Immunogenicity of Eight Dormancy Regulon-Encoded Proteins of MycobacteriumTuberculosis in DNA-Vaccinated and Tuberculosis-Infected Mice. Infect. Immun. 2007, 75(2), 941–949.
14. Goletti, D.; Butera, O.; Vanini, V.; Lauria, F. N.; Lange, C.; Franken, K. L.; Angeletti, C.; Ottenhoff,T. H. M.; Girardi, E. Response to Rv2628 Latency Antigen Associates with Cured Tuberculosis andRemote Infection. Eur. Respir. J. 2010, 36(1), 135–142.
15. WHO. Tuberculosis program, Pakistan. Author: Geneva. Available at http://www.emro.who.int/pak/programmes/stop-tuberculosis.html (accessed April 2013).
16. Mushtaq, M. U.; Majrooh, M. A.; Ahmad, W.; Rizwan, M.; Luqman, M. Q.; Aslam, M. J.; Siddiqui,A. M.; Akram, J.; Shad, M. A. Knowledge, Attitudes and Practices Regarding Tuberculosis in TwoDistricts of Punjab, Pakistan. Int. J. Tuberc. Lung. Dis. 2010, 14(3), 303–310(8).
17. Afzal, M. S.; Anjum, S.; Salman, A.; Ashraf, S.; Farooqi, Z. U. R.; Ahmed, T.; Waheed, Y.; Qadri, I.Interleukin-10 Gene Promoter Polymorphism as a Potential Host Susceptibility Factor in PakistaniPatients with Pulmonary Tuberculosis. Afr. J. Biotechnol. 2011, 10(66), 14706–14710.
18. Awan, I. N.; Rizvi, S. K. I.; Saqib, M. A. N.; Shahzad, M. I.; Khattak, A. A.; Tahseen, S.; Khan, I. H.;Ravindran, R.; Luciw, P. A.; Khanum, A. Expression and Purification of Mycobacterium TuberculosisAntigens for Use in Immunoassays for Serodetection of M. Tuberculosis Infection in TB patients.Pakistan. J. Zool. 2012, 44(1), 217–226.
19. Goldsby, R. A.; Kindt, T. J.; Osborne, B. A.; Kuby, J. Enzyme-Linked Immunosorbent Assay.Immunol. 2003, 5, 148–150.
20. Kashyap, R. S.; Rajan, A. N.; Ramteke, S. S.; Agrawal, V. S.; Kelkar, S. S.; Purohit, H. J.; Taori, G. M.;Daginawala, H. F. Diagnosis of Tuberculosis in an Indian Population by an Indirect ELISAProtocol based on Detection of Antigen 85 Complex: A Prospective Cohort Study. BMC Infect.Dis. 2007, 774.
21. Ramalingam, B.; Baulard, A. R.; Locht, C.; Narayanan, P. R.; Raja, A. Cloning, Expression, andPurification of the 27 kDa (MPT51, Rv3803c) Protein of Mycobacterium Tuberculosis. Protein. Expr.Purif. 2004, 36(1), 53–60.
22. Almeida, C. M. C.; Vasconcelos, Jr., A. C.; Kipnis, A.; Andrade, A. L.; Junqueira-Kipnis, A. P. HumoralImmune Responses of Tuberculosis Patients in Brazil Indicate Recognition of Mycobacteriumtuberculosis MPT-51 and GlcB. Clin. Vaccine. Immunol. 2008, 15(03), 579–581
23. Bethunaickan, R.; Baulard, A. R.; Locht, C.; Raja, A. Antibody Response in Pulmonary Tuberculosisagainst Recombinant 27 kDa (MPT51, Rv3803c) Protein of Mycobacterium Tuberculosis. Scand. J.Infect. Dis. 2007, 39(10), 867–874.
24. Steingart, K. R.; Henry, M.; Laal, S.; Hopewell, P. C.; Ramsay, A.; Menzies, D.; Cunningham, J.;Weldingh, K.; Pai, M. Commercial Serological Antibody Detection Tests for the Diagnosis ofPulmonary Tuberculosis: A Systematic Review. PLoS. Med. 2007, 4(6), 202.
128 S. Ashraf et al.
Dow
nloa
ded
by [
Mem
oria
l Uni
vers
ity o
f N
ewfo
undl
and]
at 1
0:47
18
July
201
4
25. Steingart, K. R.; Dendukuri, N.; Henry, M.; Schiller, I.; Nahid, P.; Hopewell, P. C.; Ramsay, A.; Pai, M.;Laal, S. Performance of Purified Antigens for Serodiagnosis of Pulmonary Tuberculosis: AMeta-Analysis. Clin. Vaccine. Immunol. 2009, 16(2), 260–276.
26. Saqib, M. A.; Awan, I. N.; Rizvi, S. K.; Shahzad, M. I.; Mirza, Z. S.; Tahseen, S.; Khan, I. H.; Khanum,A. Delay in Diagnosis of Tuberculosis in Rawalpindi, Pakistan. BMC Res. Notes 2011, 4(1), 165.
27. Khan, I. H.; Ravindran, R.; Krishnan, V. V.; Awan, I. N.; Rizvi, S. K.; Saqib, M. A.; Shahzad, M. I.;Tahseen, S.; Ireton, G.; Goulding, C. W.; Felgner, P.; DeRiemer, K.; Khanum, A.; Luciw, P. A. PlasmaAntibody Profiles as Diagnostic Biomarkers for Tuberculosis. Clin. Vaccine Immunol. 2011, 10(1128),05304–11.
29. Bashir, N.; Kounsar, F.; Mukhoeadhyay, S.; Hasnain, S. E. Mycobacterium Tuberculosis ConservedHypothetical Protein rRv2626c Modulates Macrophage Effector Functions. Immunol. Lett. 2010,130(1), 34–45.
30. Azzurri, A.; Kanaujia, G. V.; Sow, O. Y.; Bah, B.; Diallo, A.; Del Prete, G.; Gennaro, M. L. SerologicalMarkers of Pulmonary Tuberculosis and of Response to Anti-tuberculosis Treatment in a PatientPopulation in Guinea. Int. J. Immunopathol. Pharmacol. 2006, 19(1), 199–208.
31. Abebe, F.; Holm-Hansen, C.; Wiker, H. G.; Bjune, G. Progress in Serodiagnosis of MycobacteriumTuberculosis Infection. Scan. J. Immunol. 2007, 66(2–3), 176–191.