ORIGINAL ARTICLE Evaluation of Polo-like kinase 1 as a potential therapeutic target in Merkel cell carcinoma Lorenz Kadletz, MD, 1 Johannes Bigenzahn, MD, 1† Dietmar Thurnher, MD, 1 Isabella Stanisz, MD, 1 Boban M. Erovic, MD, 1 Sven Schneider, MD, 1 Rainer Schmid, MD, 2 Rudolf Seemann, MD, PhD, 3 Peter Birner, MD, PhD, 4 Gregor Heiduschka, MD 1 * 1 Department of Otorhinolaryngology, Head and Neck Surgery, Medical University of Vienna, Vienna, Austria, 2 Department of Radiotherapy, Medical University of Vienna, Vienna, Austria, 3 Department of Craniomaxillofacial and Oral Surgery, Medical University of Vienna, Vienna, Austria, 4 Department of Pathology, Medical University of Vienna, Vienna, Austria. Accepted 17 October 2015 Published online 29 December 2015 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.24349 ABSTRACT: Background. Merkel cell carcinoma (MCC) is a rare and aggressive malignancy of the skin. Treatment options for MCC include surgery, radiotherapy, and chemotherapy. The purpose of this study was to assess the expression of Polo-like kinase 1 (PLK1) in MCC and the role of the inhibitor, BI2536, as a potential therapeutic option in MCC. Methods. PLK1 expression was assessed in tissue samples from 28 patients with MCC and 5 healthy skin samples via immunohistochemis- try and furthermore in the 2 MCC cell lines, MCC13 and MCC26, via immunoblotting. The impact of increasing doses of BI2536 alone and in combination with cisplatin or irradiation on cell viability was measured using the CCK-8 assay. Colony forming assays were performed to evalu- ate long-term effects of combination treatments. Additionally, the induc- tion of apoptotic cell death was measured via flow cytometry. Results. PLK1 is moderately to strongly expressed in 75% of the patients with MCC. The PLK1 inhibitor, BI2536, demonstrated marked inhibition of cell proliferation with IC 50 in the low nM range (from 10.07–12.39 nM). Furthermore, BI2536 induces apoptosis in MCC cell lines and acts synergistically in combination with irradiation and cisplatin. Conclusion. Because of the marked upregulation of PLK1 in MCC tumor samples and potent inhibition of cell proliferation using a specific clini- cally available inhibitor, targeting of PLK1 qualifies as a potential novel therapeutic strategy in MCC. V C 2015 Wiley Periodicals, Inc. Head Neck 38: E1918–E1925, 2016 KEY WORDS: Merkel cell carcinoma, BI2536, Polo-like kinase 1 (PLK1), cancer, chemotherapy INTRODUCTION Merkel cell carcinoma (MCC) is a rare yet highly aggres- sive malignancy of neuroendocrine differentiation 1 with an incidence rate of 0.44 per 100,000. 2 MCC predomi- nantly occurs in sun-exposed areas, especially in the head and neck region. 3 Other known risk factors include immu- nosuppression, 4 age, and sex. 5,6 In 2008, Feng et al 7 delineated the fundamental role of Merkel cell polyoma- virus in carcinogenesis, which is found in up to 80% of specimens. Treatment of MCC includes either surgical resection of the primary tumor alone in early-stage disease, or surgery in combination with radiotherapy. Chemotherapy is reserved for patients with distant metastatic disease. 8 Unfortunately, MCCs have a significant potential to metastasize and the locoregional recurrence rate is high. 9 The 5-year survival rate for MCC varies between 10% and 80% depending on primary tumor size, 10 lymph node, and distant metastasis. 11 Hence, novel therapeutic targets and corresponding agents need to be identified to improve the outcome of patients with MCC. Polo-like kinases (PLKs) are currently in the focus of anticancer research because of their influence on cell cycle progression. 12 Currently, 5 different members have been described, yet only PLK1 to PLK4 exhibit enzy- matic active domains. 13,14 An overexpression of PLK1 is reported in many different types of cancer 15,16 and several studies have established PLK1 as a therapeutic target. 17,18 The potent inhibitor, BI2536, has been described in pre- clinical and clinical studies in squamous cell carcinomas of the head and neck region, anaplastic thyroid carci- noma, and nonsmall cell lung cancer, and it is in late- stage clinical trials for acute myeloid leukemia. 19–21 BI2536 additionally blocks the activities of PLK2 and PLK3 to a slightly lesser extent. The use of this highly selective small molecule inhibitor results in the recruit- ment of g-tubulin and phosphorylation of Apc6 at mitotic *Corresponding author: G. Heiduschka, Department of Otorhinolaryngology, Head and Neck Surgery, Medical University of Vienna, Waehringer Guertel 18-20, A-1090 Vienna. E-mail: [email protected]† Present address: CeMM-Research Center for Molecular Medicine of the Austrian Academy of Sciences, Vienna, Austria. This work was presented at the First International Symposium on Tumor-Host Interaction in Head and Neck Cancer 2015, Essen, Germany, January 22–24, 2015. Contract grant sponsor: This trial obtained funding from the Medical University of Vienna. E1918 HEAD & NECK—DOI 10.1002/HED APRIL 2016
Transcript
ORIGINAL ARTICLE
Evaluation of Polo-like kinase 1 as a potential therapeutic target inMerkel cell carcinoma
Lorenz Kadletz, MD,1 Johannes Bigenzahn, MD,1† Dietmar Thurnher, MD,1 Isabella Stanisz, MD,1 Boban M. Erovic, MD,1 Sven Schneider, MD,1
Rainer Schmid, MD,2 Rudolf Seemann, MD, PhD,3 Peter Birner, MD, PhD,4 Gregor Heiduschka, MD1*
1Department of Otorhinolaryngology, Head and Neck Surgery, Medical University of Vienna, Vienna, Austria, 2Department of Radiotherapy, Medical University of Vienna, Vienna,Austria, 3Department of Craniomaxillofacial and Oral Surgery, Medical University of Vienna, Vienna, Austria, 4Department of Pathology, Medical University of Vienna, Vienna,Austria.
Accepted 17 October 2015
Published online 29 December 2015 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.24349
ABSTRACT: Background. Merkel cell carcinoma (MCC) is a rare andaggressive malignancy of the skin. Treatment options for MCC includesurgery, radiotherapy, and chemotherapy. The purpose of this study wasto assess the expression of Polo-like kinase 1 (PLK1) in MCC and therole of the inhibitor, BI2536, as a potential therapeutic option in MCC.Methods. PLK1 expression was assessed in tissue samples from 28patients with MCC and 5 healthy skin samples via immunohistochemis-try and furthermore in the 2 MCC cell lines, MCC13 and MCC26, viaimmunoblotting. The impact of increasing doses of BI2536 alone and incombination with cisplatin or irradiation on cell viability was measuredusing the CCK-8 assay. Colony forming assays were performed to evalu-ate long-term effects of combination treatments. Additionally, the induc-tion of apoptotic cell death was measured via flow cytometry.
Results. PLK1 is moderately to strongly expressed in 75% of the patientswith MCC. The PLK1 inhibitor, BI2536, demonstrated marked inhibitionof cell proliferation with IC50 in the low nM range (from 10.07–12.39nM). Furthermore, BI2536 induces apoptosis in MCC cell lines and actssynergistically in combination with irradiation and cisplatin.Conclusion. Because of the marked upregulation of PLK1 in MCC tumorsamples and potent inhibition of cell proliferation using a specific clini-cally available inhibitor, targeting of PLK1 qualifies as a potential noveltherapeutic strategy in MCC. VC 2015 Wiley Periodicals, Inc. Head Neck38: E1918–E1925, 2016
INTRODUCTIONMerkel cell carcinoma (MCC) is a rare yet highly aggres-sive malignancy of neuroendocrine differentiation1 withan incidence rate of 0.44 per 100,000.2 MCC predomi-nantly occurs in sun-exposed areas, especially in the headand neck region.3 Other known risk factors include immu-nosuppression,4 age, and sex.5,6 In 2008, Feng et al7
delineated the fundamental role of Merkel cell polyoma-virus in carcinogenesis, which is found in up to 80% ofspecimens.
Treatment of MCC includes either surgical resection ofthe primary tumor alone in early-stage disease, or surgery
in combination with radiotherapy. Chemotherapy isreserved for patients with distant metastatic disease.8
Unfortunately, MCCs have a significant potential tometastasize and the locoregional recurrence rate is high.9
The 5-year survival rate for MCC varies between 10%and 80% depending on primary tumor size,10 lymphnode, and distant metastasis.11 Hence, novel therapeutictargets and corresponding agents need to be identified toimprove the outcome of patients with MCC.
Polo-like kinases (PLKs) are currently in the focus ofanticancer research because of their influence on cellcycle progression.12 Currently, 5 different members havebeen described, yet only PLK1 to PLK4 exhibit enzy-matic active domains.13,14 An overexpression of PLK1 isreported in many different types of cancer15,16 and severalstudies have established PLK1 as a therapeutic target.17,18
The potent inhibitor, BI2536, has been described in pre-clinical and clinical studies in squamous cell carcinomasof the head and neck region, anaplastic thyroid carci-noma, and nonsmall cell lung cancer, and it is in late-stage clinical trials for acute myeloid leukemia.19–21
BI2536 additionally blocks the activities of PLK2 andPLK3 to a slightly lesser extent. The use of this highlyselective small molecule inhibitor results in the recruit-ment of g-tubulin and phosphorylation of Apc6 at mitotic
*Corresponding author: G. Heiduschka, Department of Otorhinolaryngology,Head and Neck Surgery, Medical University of Vienna, Waehringer Guertel18-20, A-1090 Vienna. E-mail: [email protected]
†Present address: CeMM-Research Center for Molecular Medicine of theAustrian Academy of Sciences, Vienna, Austria.
This work was presented at the First International Symposium on Tumor-HostInteraction in Head and Neck Cancer 2015, Essen, Germany, January 22–24,2015.
Contract grant sponsor: This trial obtained funding from the Medical Universityof Vienna.
E1918 HEAD & NECK—DOI 10.1002/HED APRIL 2016
centrosomes, inhibition of cohesin release from chromo-some arms, and induction of monopolar spindles. BI2536treatment leads to an arrest of cells in G2/M and finallyto DNA breakdown and apoptosis.
So far, there are no data available on the potential use-fulness of targeting PLK1 in MCC. Hence, we examinedthe expression pattern of PLK1 in MCC to select poten-tial patients for such a therapeutic approach for the firsttime. Furthermore, we assessed the effect of BI2536 inMCC cell lines and combined it with commonly usedchemotherapeutic agents and irradiation.
MATERIALS AND METHODS
Patients
In this study, 28 archival samples of patients withMCC were included (EK612/2009). All patients weretreated at the Vienna General Hospital. Patients’ clinicaldata are shown in Table 1 and were published previ-ously.22 When the patient was referred with an alreadyresected primary tumor, specimens from metastases wereused. Fifteen samples were obtained from the primarytumor and 13 samples were derived from metastasis. Allpatients were staged as previously described.22,23 As thecontrol group, 5 samples of normal skin were obtainedduring routine breast reduction surgery.
Tissue microarray
Tissue microarrays were assembled from formalin-fixed, paraffin-embedded tissues, as described previ-ously,22 using manual tissue arrayer (MTA-1; BeecherInstruments, Sun Prairie, WI). Three cores with a diame-ter of 0.6 mm were used for each patient, and seriallysectioned slides of 3lm thickness were prepared.
Immunohistochemistry and specimen classification
Ideal antibody dilution and retrieval buffer was deter-mined preceding the analysis. Dewaxed and rehydratedtumor samples were subjected to antigen retrieval in amicrowave oven (600 W) with citrate buffer. Three per-cent H202 was used to block endogenous peroxidaseactivity for 15 minutes. After incubation with Ultra VBlock for 5 minutes, application of the primary antibodydirected against PLK1 (Abcam, Cambridge, UK) at1:1,000 and appropriate negative and positive control wasdone for 1 hour at room temperature. Paraffin-embeddedsamples of gastric cancer and head and neck squamouscell carcinoma served as positive control. Following themanufacturer’s protocol, primary antibody enhancer wasapplied for 10 minutes and afterward horseradish peroxi-dase polymer was applied for 15 minutes. Visualizationwas achieved by UltraVision Plus Detection System DABPlus Substrate System (Thermo Scientific, Fremont, CA).Counterstaining was performed with hematoxylin Gill III
TABLE 1. Clinical data of 28 samples of patients with Merkel cell carcinoma.
Patient # Type Site Stage First treatment Recurrence, mo Status TLF IS
1 Primary Hand I Surgery DOC 7 Yes2 Meta Foot III Surgery 4 DOD 24 Yes3 Primary Thigh I Surgery 4 DOC 36 No4 Meta Cheek I Surgery 6 DOD 18 No5 Meta Cheek II Surgery 6 DOD 24 Yes6 Meta Elbow I Surgery 14 AW 35 Yes7 Meta Chest NA NA8 Primary Face II Surgery 1 RT 2 DOD 6 No9 Primary Cheek I Surgery 1 RT DOC 18 Yes10 Meta Lid I Surgery 1 RT 37 DOD 58 No11 Meta Neck NA NA12 Meta Lid I Surgery 14 AW 44 No13 Meta Thigh I Surgery 3 DOD 50 No14 Meta Leg I Surgery 7 AWD 60 No15 Primary Ear I Surgery 4 AW 41 No16 Primary Nose I Surgery 11 DOD 49 No17 Primary Nose I Surgery 12 AW 68 No18 Meta Arm I Surgery 4 DOD 24 No19 Primary NA I Surgery 2 AW 34 No20 Primary Check I Surgery 12 DOD 94 No21 Meta Chest I Surgery22 Primary Neck I Surgery AW 17 No23 Primary Face II Surgery 5 DOC 87 No24 Meta Leg III Surgery 1 RT 4 DOC 8 No25 Primary Neck I Surgery DOD 17 No26 Meta Face I Surgery 23 DOC 24 No27 Primary Ear I Surgery 6 DOD 6 Yes28 Meta Neck I Surgery 5 DOD 114 No
AW
Abbreviations: Site, site of primary tumor; TLF, time to last follow-up or death; IS, immunosuppression; DOC, died of other cause; DOD, died of disease; AW, alive and well; NA, not available; RT,radiotherapy; AWD, alive with disease.
POLO-LIKE KINASE 1 IN MERKEL CELL CARCINOMA
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1919
(Merck, Darmstadt, Germany). Samples were analyzedusing an Olympus BH-2 microscope. All samples wereassigned to 1 of 4 categories of intensity staining: 0 5
negative; 1 5 weak; 2 5 moderate; and 3 5 strong inten-sity by a pathologist (P.B.). The average of the core stainswas used to determine staining intensity. As healthy skinwas either negative or weakly positive, we counted mod-erate and strong expression as PLK1-positive.
Cell and reagents
The MCC cell lines, MCC13 and MCC26, wereobtained and maintained as described before.24 BI2536was purchased at Selleckchem (Houston, TX), dissolvedat 2 mM stock concentration in dimethyl sulfoxide(DMSO), stored at 2208C at 1:1000, and obtained as aready-to-use infusion and stored at 48C.
Cytotoxicity
Growth inhibition was assessed using the CCK-8 assay(Dojindo Laboratories, Kumamoto, Japan), as describedbefore.25 Briefly, 3 3 103 cells were seeded into 96-wellplates. After 24 hours’ rest, cells were incubated with100% concentration in DMSO, and stored at concentra-tions ranging from 0 to 50 nm, cisplatin doses rangedfrom 0 to 20lM. Next, cells were incubated for 72 hours.DMSO-treated cells served as a control group. Thereafter,cells were counted according to the manufacturer’s
protocol. IC50 values were calculated using Prism 5.0(Graphpad Software). For combination experiments, cellswere either incubated with 2 drugs or exposed to irradia-tion (0, 2, 4, and 8 Gy) simultaneously for 72 hours. Sur-vival data was then analyzed using Calcusyn software 2.0(Biosoft) to calculate a combination index (CI). Accord-ing to Chou and Talalay,26 CI values <1 were consideredsynergistic.
Western blot
Western blots were conducted, as described else-where.27 In brief, MCC13 and MCC26 cell pellets (105
cells in a 6-cm tissue culture dish) were rinsed twice inphosphate-buffered saline and lysed with lysis buffer.Lysates were cleared by centrifugation at 13,000 rpm andthe supernatants were collected. Aliquots of supernatantscontaining 20lg of protein measured by bicinchoninicacid assay were subjected to sodium dodecyl sulfate poly-acrylamide gel electrophoresis and transferred to nitrocel-lulose membranes. After a blocking step, membraneswere incubated with anti-PLK1 (Abcam, Cambridge, UK;dilution 1:3000) and anti-actin (Sigma–Aldrich; 1:2500)as the primary antibody. Membranes were further incu-bated with horseradish peroxidase conjugated species-specific secondary antibodies and visualized with theClarity Western ECL substrate (BIO-RAD, Hercules,CA).
FIGURE 1. Immunohistochemistry ofPolo-like kinase 1 (PLK1) expression inMerkel cell carcinoma (MCC). Samplesof MCC with weak (B), moderate (C),and strong expression (C) PLK1 areshown. Healthy skin served as the con-trol group (A) and showed no expres-sion of PLK1. All photomicrographswere taken at an original magnification3200.
LORENZ ET AL.
E1920 HEAD & NECK—DOI 10.1002/HED APRIL 2016
Colony forming assay
MCC13 and MCC26 cells were seeded at 3 to 15 3102 cells into 6-well plates.28 Cells were allowed to restfor 24 hours and subsequently were treated with IC50 orIC25 and irradiated with a single boost of 2, 4, 6, or 8 Gyusing a conventional radiation source with 250-kV X-rays, as described before.25 Untreated cells served as con-trol. Medium was changed to drug-free medium after 72hours. Cells were rinsed twice with phosphate-bufferedsaline after 10 days, fixed with methanol, and stainedwith methylene blue. Clones with more than 50 cellswere counted and considered as the surviving fraction.
Flow cytometry
MCC13 and MCC26 cells were seeded at 3 3 105 in6-well plates. After 24 hours, cells were treated withBI2536 and 0, 4, or 8 Gy irradiation or in combination.After 48 hours, apoptosis was measured using theAnnexin-V Apoptosis Detection Kit (Bender MedSystems, Vienna, Austria). Annexin/propidium iodide(Ann/PI) 1/2 cells were defined as apoptotic cells,whereas Ann2/PI1 and Ann1/PI1 cells were bothdefined as necrosis, because late apoptosis cannot be dis-tinguished by this assay.
Statistical analysis
For the evaluation of the clonogenic survival, a linearregression model was used, as previously described.28
SPSS software version 21.0 (SPSS, Chicago, IL) wasused to analyze data for the presence of homoscedasticityand either Tukey or Games–Howell post-hoc tests wereperformed after analysis of variance analysis. Error barsrepresent SEM. All experiments were repeated at least 3times. The p values < .05 were considered as statisticallysignificant.
RESULTS
Clinical data
Of the 28 patients, 16 were men and 12 were women.Median age was 63.1 years (range, 41–85 years). In 13patients, the primary tumor was resected not at our insti-tution; hence, no samples of the primary tumor wereavailable. Clinical data are shown in Table 1. Threepatients with samples of the primary tumor developed alocal recurrence, 4 patients developed regional metastasis,and 5 patients showed distant metastasis. Seven of 28patients were under immunosuppression at the time of ini-tial diagnosis.
Expression of Polo-like kinase 1 in Merkel cellcarcinoma
Samples of 28 patients were stained for the expressionPLK1. We observed 1 patient sample with no expression,6 patients’ with samples with weak expression, 15patients’ samples with moderate expression, and 6 withstrong expression of PLK1 (Figure 1). In the control sam-ples, 2 samples showed no expression and 3 samplesshowed weak expression of PLK1. We grouped none andweak expression as well as moderate and strong expres-sion. Comparing both groups, 21 of 28 (75%) showed anupregulated expression of PLK1. There was no differencein the expression pattern between samples derived fromthe primary tumor compared to the sample of metastasis.
Consecutively, we tested 2 MCC cell lines, MCC13and MCC26, for PLK1 protein expression using immuno-blot analysis. Both cell lines showed a general expressionof PLK1 (data not shown).
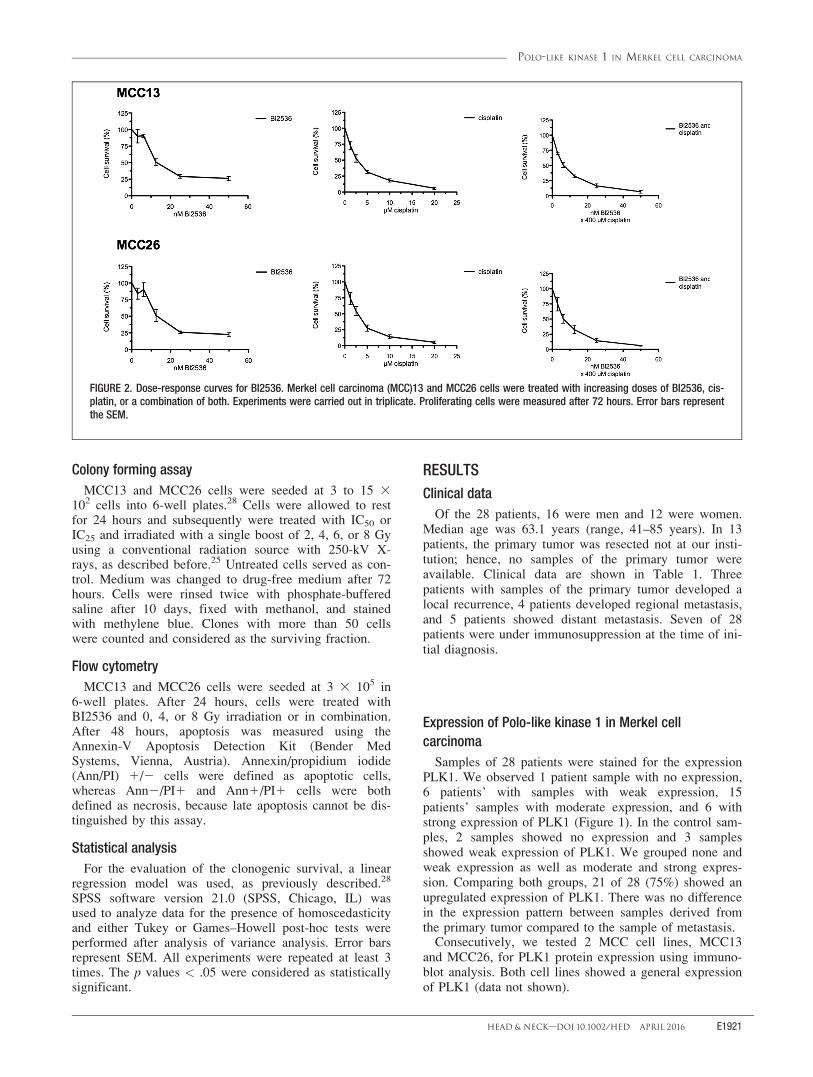
FIGURE 2. Dose-response curves for BI2536. Merkel cell carcinoma (MCC)13 and MCC26 cells were treated with increasing doses of BI2536, cis-platin, or a combination of both. Experiments were carried out in triplicate. Proliferating cells were measured after 72 hours. Error bars representthe SEM.
POLO-LIKE KINASE 1 IN MERKEL CELL CARCINOMA
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1921
Cytotoxicity of BI2536 and cisplatin
Successively, the inhibitory effects of a selective PLK1inhibitor, BI2536, were evaluated in the 2 MCC cell lines,MCC13 and MCC26. At least 3 independent experimentswere conducted in triplicate. After a period of 72 hours ofincubation with BI2536, both cell lines showed a dose-dependent growth inhibition after treatment. A dose of 50 nmled to a growth inhibition of 73.7% in MCC13 and 77.5% inMCC26. The IC50 values were calculated as 10.07 nm(MCC13) and 12.39 nm (MCC26; Figure 2), respectively.
Effects of BI2536 in vitro exposure in combination withcisplatin
In order to assess a potential synergistic effect of com-bination treatment, MCC13 and MCC26 cells wereexposed to BI2536 and cisplatin for 72 hours. The combi-
nation ratio of BI2536:cisplatin was set at 1:400 and theCI was calculated.26 The CI values <1 were consideredas a synergistic effect. In both cell lines, we detected anadditive to mild synergistic effect over the full dose range(Figure 3).
Effects of BI2536 in vitro exposure in combination withirradiation
Additionally, we assessed the effect of BI2536 in com-bination with radiotherapy. Both MCC cell lines wereexposed to increasing doses of BI2536 and irradiation at0, 2, 4, and 8 Gy. Convincingly, we observed a markedsynergistic effect of BI2536 and radiotherapy at higherdoses in MCC13 and MCC26. As shown in the CI blotsin Figure 3 and dose-response graphs in Figure 4,
FIGURE 3. Combination index(CI) for the combination ofBI2536 with cisplatin or irradia-tion in Merkel cell carcinoma(MCC)13 and MCC26. CI 5 1depicts an additive effect, CI<1 an synergism, and CI >1indicates an antagonisticeffect. CI values were calcu-lated using CalcuSyn software.
FIGURE 4. Dose responsecurves for BI2536 and irradia-tion. Merkel cell carcinoma(MCC)13 and MCC26 weretreated with doses rangingfrom 0 to 50 nm BI2536 and 0,2, 4, 6, or 8 Gy for 72 hours.Error bars represent the SEM.
LORENZ ET AL.
E1922 HEAD & NECK—DOI 10.1002/HED APRIL 2016
radiation therapy achieved higher synergy as compared tocisplatin treatment.
BI2536 induces apoptosis in Merkel cell carcinoma
After our proliferation experiments, we performedannexing and PI staining followed by flow cytometry toevaluate the induction of apoptosis. MCC13 and MCC26cell lines were treated with increasing doses of BI2536and combined with irradiation doses of 0 or 4 Gy. Thecombination of BI2536 and irradiation led to increasingfractions of apoptotic and necrotic cells in both cell lines(Figure 5). Exposure to BI2536 and irradiation in MCC13led to apoptotic fractions ranging from 16% to 63% incomparison to 9% apoptotic cells in the control group. InMCC26, apoptotic fractions were measured ranging from17% to 55% in contrast to 15% in the control group.
Effects of combined treatment on colony formation
Finally, to evaluate potential long-term effects ofBI2536 and irradiation, colony-forming assays were per-formed. Therefore, cells were incubated with either noBI2536 or doses of IC50 or IC25 and exposed to irradia-tion at 0, 2, 4, 6, or 8 Gy for 72 hours and switchedthereafter to drug-free medium for an additional 10 days.We observed a significant inhibition of colony formation
after incubation with increasing doses of BI2536 mark-edly enhancing the antiproliferative effect of irradiation(p < .001; Figure 6).
DISCUSSIONBecause MCC is a rare type of cancer, only limited infor-
mation is available about the disease and possible treatmentoptions. Surgical excision with wide margins is currentlydiscussed as the primary treatment option in early-stageMCC.10,11 Radiotherapy serves as a reasonable alternative,because most MCCs are radiosensitive. Furthermore, sev-eral studies indicate an improved locoregional controlwhen irradiation is used in an adjuvant setting.29 In con-trast, systematic therapy is predominantly preserved forpatients with locally advanced, recurrent, or metastatic dis-ease.8,10 Because PLK1 is currently in the focus of cancerdue to its role in cell cycle progression, we set out to inter-rogate the feasibility of targeting PLK1 in MCC.
In our study, we report for the first time that PLK1 isconsistently upregulated in MCC samples, because mosttissue samples showed moderate to strong expression ofPLK1. Furthermore, these findings suggest that PLK1 is apotential molecular target and we were able to describe adirect effect of BI2536, alone and in combination withestablished treatment options, to MCC cell lines.
First, the expression of PLK1 in patients with MCCwas evaluated immunohistochemically to gain knowledgeabout the expression profile. The results showed a moder-ate to strong expression in most of the patients. In linewith this, normal skin tissue showed only weak or no
FIGURE 5. Flow cytometry. Apoptotic and necrotic fraction wasmeasured in Merkel cell carcinoma (MCC)13 and MCC26 viaAnnexin-V Apoptosis Detection Kit (Bender Med Systems). Experi-ments were carried out in triplicate. Cells were treated withBI2536 0, 3, 6, or 12 nm and 0, 4, or 8 Gy.
FIGURE 6. Clonogenic survival. Colony formation in Merkel cellcarcinoma (MCC)13 and MCC26 after treatment with BI2536 andirradiation. Experiments were carried out in triplicate. Error barsrepresent the SEM.
POLO-LIKE KINASE 1 IN MERKEL CELL CARCINOMA
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1923
detectable expression of PLK1. This is in line with sev-eral other cancer entities, such as melanoma,30 cutaneousT-cell lymphoma,31 or basal cell carcinoma.32 On theother hand, normal skin tissue showed no or only weakexpression of PLK1.
Consequently, we assessed whether PLK1 is expressedin MCC cell lines. Using Western analysis, we detectedthe expression of PLK1 in both of our cell lines. In addi-tion, we assessed the potential antiproliferative potentialof targeting PLK1 with the selective inhibitor BI2536.
The substance BI2536 went through multiple phase Istudies warranting its safety profile for clinical use.33 Fur-thermore, BI2536 is tested in several phase II studies inmalignancies of the pancreas,34 head and neck cancer,soft tissue sarcoma, melanoma,35 small lung cell carci-noma,21 and acute myeloid leukemia.36 However, so far,there is no study investigating the effects of BI2536 inMCC. As a single agent, BI2536 is a very potent inhibitorof cellular proliferation with an IC50 located between10.07 nM and 12.39 nM. This dose range is correlatingwith previously published studies in other malignancies,in which IC50 values ranged from 2 to 25 nM.20,37,38
Furthermore, we combined BI2536 with the chemother-apeutic agent cisplatin, because cisplatin serves as a clini-cally applied drug in patients diagnosed with distantdisease of MCC.39 Our results showed an additive to syn-ergistic effect over a wide dose range. In previous studiesin head and neck squamous cell carcinoma, a combinationof BI2536 and cisplatin also showed synergistic antiproli-ferative and proapoptotic effects.19
Because MCC can also be treated with radiotherapy,we conducted combination experiments of BI2536 withirradiation. We therefore conducted both proliferationassays (for the short-term effect) and colony formingassays (for the long-term effect). Our results show thatthe combination of BI2536 with irradiation leads both toa growth inhibition as well as a reduction of formed colo-nies. Lund–Anderson et al40 described that the inhibitionof PLK1 in osteosarcoma and colon cancer cells led to anaccumulation of mitotic cells causing radiosensitization ifradiotherapy is applied.
Finally, we assessed the induction of apoptosis byBI2536 using flow cytometry. When applied as a singleagent, BI2636 induced apoptosis in both of our MCC celllines. This effect was further increased in the combinationexperiments. These results are conclusive with studies inother cancer entities.41
The results of our research have shown, for the firsttime, that PLK1 is highly expressed in MCC and thus mayserve as a potential therapeutic target. Furthermore, weused the PLK1 inhibitor BI2536 in our MCC cell modeland found both a direct as well as a combinatorial effect.The combination of chemotherapy or radiotherapy showedimproved growth inhibitory effects. These data suggestthat BI2536 is a promising candidate in the treatment ofMCC. However, follow-up studies are required to add fur-ther information for a potential clinical application.
3. Lunder EJ, Stern RS. Merkel-cell carcinomas in patients treated withmethoxsalen and ultraviolet A radiation. N Engl J Med 1998;339:1247–1248.
4. Engels EA, Frisch M, Goedert JJ, Biggar RJ, Miller RW. Merkel cell carci-noma and HIV infection. Lancet 2002;359:497–498.
5. Miller RW, Rabkin CS. Merkel cell carcinoma and melanoma: etiologicalsimilarities and differences. Cancer Epidemiol Biomarkers Prev 1999;8:153–158.
6. Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma inthe United States. J Am Acad Dermatol 2003;49:832–841.
7. Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavi-rus in human Merkel cell carcinoma. Science 2008;319:1096–1100.
8. Gessner K, Wichmann G, Boehm A, et al. Therapeutic options for treatmentof Merkel cell carcinoma. Eur Arch Otorhinolaryngol 2011;268:443–448.
9. Hasan S, Liu L, Triplet J, Li Z, Mansur D. The role of postoperative radia-tion and chemoradiation in Merkel cell carcinoma: a systematic review ofthe literature. Front Oncol 2013;3:276.
11. Allen PJ, Bowne WB, Jaques DP, Brennan MF, Busam K, Coit DG. Merkelcell carcinoma: prognosis and treatment of patients from a single institu-tion. J Clin Oncol 2005;23:2300–2309.
12. Luo J, Liu X. Polo-like kinase 1, on the rise from cell cycle regulation toprostate cancer development. Protein Cell 2012;3:182–197.
13. de C�arcer G, Escobar B, Higuero AM, et al. Plk5, a polo box domain-onlyprotein with specific roles in neuron differentiation and glioblastoma sup-pression. Mol Cell Biol 2011;31:1225–1239.
14. McInnes C, Wyatt MD. PLK1 as an oncology target: current status andfuture potential. Drug Discov Today 2011;16:619–625.
15. Zhang Z, Hou X, Shao C, et al. Plk1 inhibition enhances the efficacy ofandrogen signaling blockade in castration-resistant prostate cancer. CancerRes 2014;74:6635–6647.
16. Takahashi T, Sano B, Nagata T, et al. Polo-like kinase 1 (PLK1) is overex-pressed in primary colorectal cancers. Cancer Sci 2003;94:148–152.
17. Triscott J, Lee C, Foster C, et al. Personalizing the treatment of pediatricmedulloblastoma: polo-like kinase 1 as a molecular target in high-risk chil-dren. Cancer Res 2013;73:6734–6744.
18. Lin CC, Su WC, Yen CJ, et al. A phase I study of two dosing schedules ofvolasertib (BI 6727), an intravenous polo-like kinase inhibitor, in patientswith advanced solid malignancies. Br J Cancer 2014;110:2434–2440.
19. Wagenblast J, Hirth D, Eckardt A, et al. Antitumoral effect of PLK-1-inhibitor BI2536 in combination with cisplatin and docetaxel in squamouscell carcinoma cell lines of the head and neck. Mol Clin Oncol 2013;1:286–290.
20. Nappi TC, Salerno P, Zitzelsberger H, Carlomagno F, Salvatore G, SantoroM. Identification of polo-like kinase 1 as a potential therapeutic target inanaplastic thyroid carcinoma. Cancer Res 2009;69:1916–1923.
21. Sebastian M, Reck M, Waller CF, et al. The efficacy and safety of BI 2536,a novel Plk-1 inhibitor, in patients with stage IIIB/IV non-small cell lungcancer who had relapsed after, or failed, chemotherapy: results from anopen-label, randomized phase II clinical trial. J Thorac Oncol 2010;5:1060–1067.
22. Brunner M, Thurnher D, Pammer J, et al. Expression of hedgehog signalingmolecules in Merkel cell carcinoma. Head Neck 2010;32:333–340.
23. Yiengpruksawan A, Coit DG, Thaler HT, Urmacher C, Knapper WK. Mer-kel cell carcinoma. Prognosis and management. Arch Surg 1991;126:1514–1519.
24. Heiduschka G, Lill C, Seemann R, et al. The effect of resveratrol in combi-nation with irradiation and chemotherapy: study using Merkel cell carci-noma cell lines. Strahlenther Onkol 2014;190:75–80.
25. Kotowski U, Heiduschka G, Brunner M, et al. Radiosensitization of headand neck cancer cells by the phytochemical agent sulforaphane. Strah-lenther Onkol 2011;187:575–580.
26. Chou TC, Talalay P. Quantitative analysis of dose-effect relationships: thecombined effects of multiple drugs or enzyme inhibitors. Adv EnzymeRegul 1984;22:27–55.
27. Heiduschka G, Erovic BM, Vormittag L, et al. 7beta-hydroxycholesterolinduces apoptosis and regulates cyclooxygenase 2 in head and neck squa-mous cell carcinoma. Arch Otolaryngol Head Neck Surg 2009;135:261–267.
28. Franken NA, Rodermond HM, Stap J, Haveman J, van Bree C. Clonogenicassay of cells in vitro. Nat Protoc 2006;1:2315–2319.
29. Ghadjar P, Kaanders JH, Poortmans P, et al. The essential role of radiother-apy in the treatment of Merkel cell carcinoma: a study from the Rare Can-cer Network. Int J Radiat Oncol Biol Phys 2011;81:e583–e591.
30. de Oliveira JC, Brassesco MS, Pezuk JA, et al. In vitro PLK1 inhibition byBI 2536 decreases proliferation and induces cell-cycle arrest in melanomacells. J Drugs Dermatol 2012;11:587–592.
31. Stutz N, Nihal M, Wood GS. Polo-like kinase 1 (Plk1) in cutaneous T-celllymphoma. Br J Dermatol 2011;164:814–821.
32. Schmit TL, Zhong W, Nihal M, Ahmad N. Polo-like kinase 1 (Plk1) innon-melanoma skin cancers. Cell Cycle 2009;8:2697–2702.
33. Mross K, Frost A, Steinbild S, et al. Phase I dose escalation and pharmaco-kinetic study of BI 2536, a novel polo-like kinase 1 inhibitor, in patientswith advanced solid tumors. J Clin Oncol 2008;26:5511–5517.
LORENZ ET AL.
E1924 HEAD & NECK—DOI 10.1002/HED APRIL 2016
34. Mross K, Dittrich C, Aulitzky WE, et al. A randomised phase II trial of thepolo-like kinase inhibitor BI 2536 in chemo-na€ıve patients with unresect-able exocrine adenocarcinoma of the pancreas – a study within the CentralEuropean Society Anticancer Drug Research (CESAR) collaborative net-work. Br J Cancer 2012;107:280–286.
35. Sch€offski P, Blay JY, De Greve J, et al. Multicentric parallel phase II trialof the polo-like kinase 1 inhibitor BI 2536 in patients with advanced headand neck cancer, breast cancer, ovarian cancer, soft tissue sarcoma andmelanoma. The first protocol of the European Organization for Researchand Treatment of Cancer (EORTC) Network of Core Institutes (NOCI).Eur J Cancer 2010;46:2206–2215.
36. M€uller–Tidow C, Bug G, L€ubbert M, et al. A randomized, open-label,phase I/II trial to investigate the maximum tolerated dose of the polo-likekinase inhibitor BI 2536 in elderly patients with refractory/relapsed acutemyeloid leukaemia. Br J Haematol 2013;163:214–222.
37. Deeraksa A, Pan J, Sha Y, et al. Plk1 is upregulated in androgen-insensitiveprostate cancer cells and its inhibition leads to necroptosis. Oncogene2013;32:2973–2983.
38. Wagenblast J, Hirth D, Thron L, et al. Effects of the polo-like-kinase-1-inhibitor BI2536 in squamous cell carcinoma cell lines of the head andneck. Oncol Lett 2012;4:175–177.
39. Fields RC, Busam KJ, Chou JF, et al. Five hundred patients with Merkel cellcarcinoma evaluated at a single institution. Ann Surg 2011;254:465–475.
40. Lund–Andersen C, Patzke S, N€ahse–Kumpf V, Syljuasen RG. PLK1-inhi-bition can cause radiosensitization or radioresistance dependent on thetreatment schedule. Radiother Oncol 2014;110:355–361.
41. Chopra AS, Kuratnik A, Scocchera EW, Wright DL, Giardina C.Identification of novel compounds that enhance colon cancer cell sensitiv-ity to inflammatory apoptotic ligands. Cancer Biol Ther 2013;14:436–449.














![Mutations in Drosophila Greatwall/Scant Reveal Its Roles ... · Polo, originally discovered in Drosophila [2,3], exemplifies an evolutionarily conserved mitotic protein kinase. Polo,](https://static.documents.pub/doc/80x56/60869d314968237b9d3377d8/mutations-in-drosophila-greatwallscant-reveal-its-roles-polo-originally-discovered.jpg)









