GASTROINTESTINAL Evaluation of the anti-peristaltic effect of glucagon and hyoscine on the small bowel: comparison of intravenous and intramuscular drug administration Andreas Gutzeit & Christoph A. Binkert & Dow-Mu Koh & Klaus Hergan & Constantin von Weymarn & Nicole Graf & Michael A. Patak & Justus E. Roos & Marcus Horstmann & Sebastian Kos & Simone Hungerbühler & Johannes M. Froehlich Received: 25 October 2011 / Revised: 21 November 2011 / Accepted: 5 December 2011 / Published online: 22 January 2012 # European Society of Radiology 2012 Abstract Purpose To evaluate prospectively duration and effectiveness of aperistalsis achieved by glucagon(GLU) or hyoscine N- butylbromide(HBB) following various administration routes. Materials and methods Six volunteers underwent Magnetic Resonance Imaging (MRI) after standardized oral prepara- tion in random order five separate MR examinations with both spasmolytic agents (HBB intravenous(i.v.) or intramus- cular(i.m.), GLU i.v. or i.m., and a combined scheme). The MR protocol included a sagittal 2D cross-section of the small bowel with a temporal resolution of 0.55 s acquired over 60 to 90 min. To quantify bowel motility, small bowel cross-sectional areas were summated over time. Results The anti-peristaltic i.v. effects of HBB and glucagon started on average after 85 s/65 s and ended after 21 min/ 23.3 min, respectively. By comparison, the anti-peristaltic effects of i.m. HBB and glucagon started significantly later 5.1/11.6 min (P 0 0.001; Wilcoxon signed ranks test) and lasted for 17.7/28.2 min with greater inter-individual differences (P 0 0.012; Brown-Forsythe test). The combined scheme resulted in a rapid onset after 65 s with effect duration of 31 min. Conclusion Anti-peristaltic effects on the small bowel are drug dependant, i.e., their onset is faster and more reliable when administering i.v. than i.m.. Combining i.v. GLU with i.m. HBB provides an early onset of effect, sustained spas- molysis and the highest degree of motility impairment. A. Gutzeit (*) : C. A. Binkert : C. von Weymarn : J. E. Roos : J. M. Froehlich Department of Radiology, Cantonal Hospital Winterthur, Brauerstrasse 15, 8401 Winterthur, Switzerland e-mail: [email protected]A. Gutzeit : K. Hergan Department of Radiology, Paracelsus Medical University Salzburg, Salzburg, Austria D.-M. Koh Department of Radiology, Royal Marsden Hospital, Downs Rd, Sutton SM2 5PT, UK N. Graf Clinical Trials Center, Center for Clinical Research, University Hospital Zurich, Zurich, Switzerland M. A. Patak Department of Radiology, University Hospital Zürich, Raemistrasse 100, 8090 Zurich, Switzerland M. Horstmann Department of Urology, Cantonal Hospital Winterthur, Brauerstrasse 15, 8401 Winterthur, Switzerland S. Kos Division of Interventional Radiology, Institute of Radiology and Nuclear Medicine, University Hospital Basel, Petersgraben 4, 4031 Basel, Switzerland S. Hungerbühler Department of Pharmacy, Cantonal Hospital Winterthur, Brauerstrasse 15, 8401 Winterthur, Switzerland Eur Radiol (2012) 22:1186–1194 DOI 10.1007/s00330-011-2366-1
Transcript
GASTROINTESTINAL
Evaluation of the anti-peristaltic effect of glucagonand hyoscine on the small bowel: comparison of intravenousand intramuscular drug administration
Andreas Gutzeit & Christoph A. Binkert &Dow-Mu Koh & Klaus Hergan &
Constantin von Weymarn & Nicole Graf &Michael A. Patak & Justus E. Roos &
Marcus Horstmann & Sebastian Kos &
Simone Hungerbühler & Johannes M. Froehlich
Received: 25 October 2011 /Revised: 21 November 2011 /Accepted: 5 December 2011 /Published online: 22 January 2012# European Society of Radiology 2012
AbstractPurpose To evaluate prospectively duration and effectivenessof aperistalsis achieved by glucagon(GLU) or hyoscine N-butylbromide(HBB) following various administration routes.Materials and methods Six volunteers underwent MagneticResonance Imaging (MRI) after standardized oral prepara-tion in random order five separate MR examinations withboth spasmolytic agents (HBB intravenous(i.v.) or intramus-cular(i.m.), GLU i.v. or i.m., and a combined scheme). TheMR protocol included a sagittal 2D cross-section of thesmall bowel with a temporal resolution of 0.55 s acquiredover 60 to 90 min. To quantify bowel motility, small bowelcross-sectional areas were summated over time.
Results The anti-peristaltic i.v. effects of HBB and glucagonstarted on average after 85 s/65 s and ended after 21 min/23.3 min, respectively. By comparison, the anti-peristalticeffects of i.m. HBB and glucagon started significantly later5.1/11.6 min (P00.001;Wilcoxon signed ranks test) and lastedfor 17.7/28.2 min with greater inter-individual differences (P00.012; Brown-Forsythe test). The combined scheme resulted ina rapid onset after 65 s with effect duration of 31 min.Conclusion Anti-peristaltic effects on the small bowel aredrug dependant, i.e., their onset is faster and more reliablewhen administering i.v. than i.m.. Combining i.v. GLU withi.m. HBB provides an early onset of effect, sustained spas-molysis and the highest degree of motility impairment.
A. Gutzeit (*) : C. A. Binkert :C. von Weymarn : J. E. Roos :J. M. FroehlichDepartment of Radiology, Cantonal Hospital Winterthur,Brauerstrasse 15,8401 Winterthur, Switzerlande-mail: [email protected]
A. Gutzeit :K. HerganDepartment of Radiology,Paracelsus Medical University Salzburg,Salzburg, Austria
D.-M. KohDepartment of Radiology, Royal Marsden Hospital,Downs Rd,Sutton SM2 5PT, UK
N. GrafClinical Trials Center, Center for Clinical Research,University Hospital Zurich,Zurich, Switzerland
M. A. PatakDepartment of Radiology, University Hospital Zürich,Raemistrasse 100,8090 Zurich, Switzerland
M. HorstmannDepartment of Urology, Cantonal Hospital Winterthur,Brauerstrasse 15,8401 Winterthur, Switzerland
S. KosDivision of Interventional Radiology, Institute of Radiologyand Nuclear Medicine, University Hospital Basel,Petersgraben 4,4031 Basel, Switzerland
S. HungerbühlerDepartment of Pharmacy,Cantonal Hospital Winterthur,Brauerstrasse 15,8401 Winterthur, Switzerland
Small bowel motility is essential for transportation of bowelcontents through the gastrointestinal tract to ensure absorp-tion and digestion. Small bowel movement is characterizedby a complex motion pattern of dilatation and contraction,which is influenced by the nervous system, hormones, andhormone-like substances [1].
From the radiological point of view, bowel motility influ-ences the image quality and is often the cause for movementartifacts, especially when using radiological investigationswhich are sensitive to motion such as MRI and angiographyin the abdominal or pelvic region [2–6].
Spasmolytic agents are routinely used in the clinicalsetting to improve the quality of images of the abdomenand pelvis. The most commonly used paralytic agents areglucagon (GlucaGen®, Novo Nordisk, DK-2880 Bagsvaerd)and hyoscine N-butylbromide (HBB; Buscopan®, BoehringerIngelheim, CH-Basel).
Glucagon is a hormone with paralytic effects on thesmooth muscles of the gastrointestinal tract besides antago-nizing insulin and leading to the release of epinephrine. Pa-ralysis of gut motility is achieved via activation of glucagon-like protein −2 receptors (GLP-2) [7, 8]. While Hyoscineexerts an anticholinergic effect, especially on muscarinicreceptors, which are located on visceral smooth muscles.Hyoscine is a frequently used pharmacological agent to re-duce bowel peristalsis and improve image quality [4].Thepharmacological mechanisms of these two substances as spas-molytics are well described [9]. Both drugs are approved inmany countries for the purpose of inducing spasmolysis dur-ing imaging procedures.
Glucagon, as well as hyoscine, can be administered bythe intravenous or intramuscular route. However, little isknown about the efficacy of these two agents administeredvia different routes. Knowledge about the commencement,efficacy and termination of anti-peristaltic effects is essentialfor planning and performing imaging procedures in theabdomen and pelvis.
The physiology of small bowel motility has been scarcelyreported on. Being inaccessible to conventional endoscopicprocedures, bowel motility is difficult to investigate. Capsuleendoscopy in conjunction with cross-sectional imaging tech-niques such as computed tomography (CT) or magnetic reso-nance imaging (MRI) have been used to investigate thesecomplex motion patterns[10]. Assessment of small bowelmotility using MRI is limited by the constraints of the acqui-sition needing both high spatial and temporal resolution.
The aim of our study was to evaluate the anti-peristalticeffect of Glucagon and Hyoscine using different routes ofadministration (i.v., i.m.), and their combination, in order toestablish the optimal regimen for spasmolysis.
Material and methods
Patients
After obtaining institutional review board approval sixhealthy volunteers (one woman, five men; age range 26 to52 years, mean age 30 years) providing informed writtenconsent were included in a prospective clinical study lastingfrom March 2010 to February 2011.
To ensure a standardized small bowel distension thevolunteers fasted for four hours and ingested a preparationconsisting of 1600 mL of water combined with 20 ml gado-terate (0.5 Mol/L; Dotarem®, Guerbet, F-Roissy, France) and23. 2 g Metamucil mite (psyllium husk hydrophilic mucilloid,maltodextrin; Procter & Gamble, Petit-Lancy, France ) beforeeach MR examination. The aqueous preparation was dividedinto four equal portions; each portion was drunk at 15 mininterval over 60 min.
The volunteers underwent the MR examinations withfive different pharmacological regimens (40 mg hyoscineN-butylbromide; Buscopan® i.v. and i.m., 1 mg Glucagon i.v.and i.m., 1 mg Glucagon i.v. plus 40 mg hyoscine i.m.) inrandom order, within a maximum time period of two monthsand with at least a one-week delay between individual meas-urements, thus eliminating any carry-over effect from theprevious assessment.
MR imaging protocol and administration of drugs
The volunteers were imaged using 1.5 Tesla MR (GyroscanIntera, Philips Healthcare, Best, The Netherlands; with a 16-element XL torso coil). The standardized MRI protocol issummarized in Table 1. Clearly visible small bowel loopswere imaged dynamically during breath-holds (about 30s)with a temporal resolution of 0.55 s on a 2D sagittal view(Fig. 1). Before administration of the spasmolytic agentthree separate measurements were performed to establishthe normal basal pattern of small bowel motility.
Eur Radiol (2012) 22:1186–1194 1187
Intravenous administration was achieved rapidly via avenous access on the dorsum of the hand, using a 20-gaugeneedle (BDVenflon, BDMedical systems, New Jersey, USA).For intramuscular injection we employed a 23-gauge needle(Terumo Hospital systems, Eschborn, Germany); the sub-stance was injected in the dorsal aspect of the left lowerextremity, including the gastrocnemius and soleus muscle.For combined intravenous and intramuscular injection oneperson injected Hyoscine in the muscle while another con-comitantly injected Glucagon into the vein. After administra-tion of the spasmolytic agent, we performed sagittal 2Ddynamic T1-weighted imaging repeatedly over the selectedsmall bowel loops with a delay of 15 s and follow-up periodsof 60 min (i.v. administration) or 90 min (i.m. or combinedscheme). The observation periods differed because, in ourexperience, the i.v. anti-peristaltic effect does not last longerthan 60 min, while we suspected that the effects of intramus-cular administration may be prolonged.
Post processing
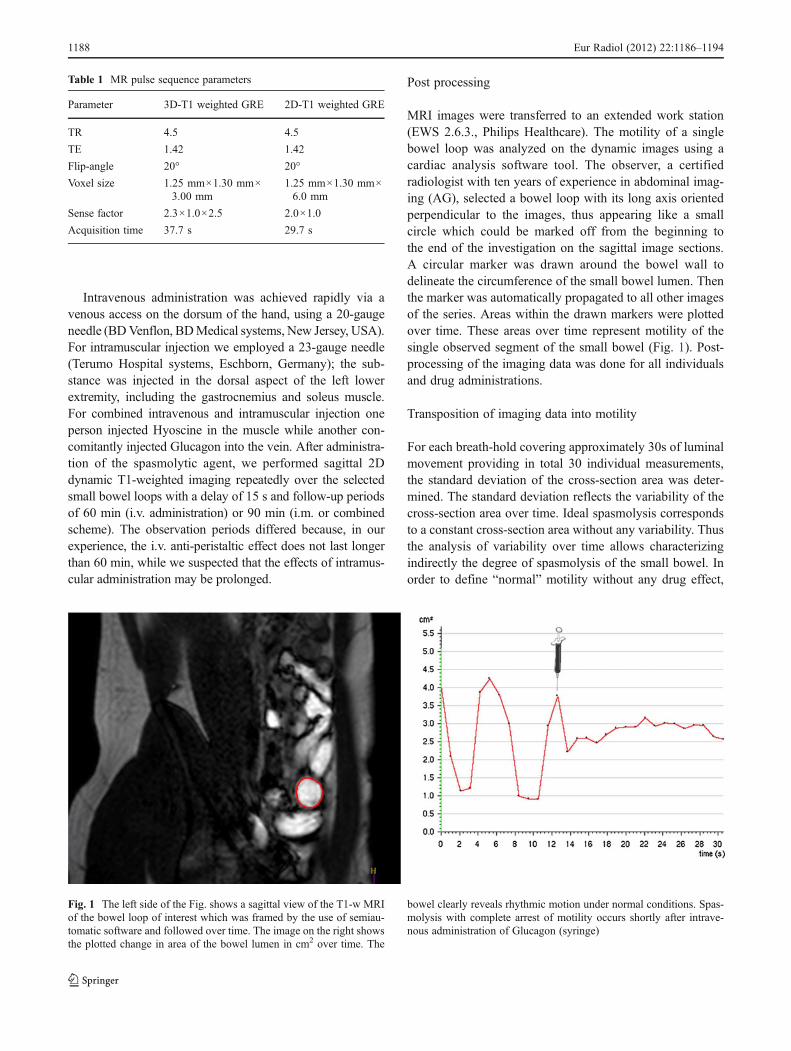
MRI images were transferred to an extended work station(EWS 2.6.3., Philips Healthcare). The motility of a singlebowel loop was analyzed on the dynamic images using acardiac analysis software tool. The observer, a certifiedradiologist with ten years of experience in abdominal imag-ing (AG), selected a bowel loop with its long axis orientedperpendicular to the images, thus appearing like a smallcircle which could be marked off from the beginning tothe end of the investigation on the sagittal image sections.A circular marker was drawn around the bowel wall todelineate the circumference of the small bowel lumen. Thenthe marker was automatically propagated to all other imagesof the series. Areas within the drawn markers were plottedover time. These areas over time represent motility of thesingle observed segment of the small bowel (Fig. 1). Post-processing of the imaging data was done for all individualsand drug administrations.
Transposition of imaging data into motility
For each breath-hold covering approximately 30s of luminalmovement providing in total 30 individual measurements,the standard deviation of the cross-section area was deter-mined. The standard deviation reflects the variability of thecross-section area over time. Ideal spasmolysis correspondsto a constant cross-section area without any variability. Thusthe analysis of variability over time allows characterizingindirectly the degree of spasmolysis of the small bowel. Inorder to define “normal” motility without any drug effect,
Table 1 MR pulse sequence parameters
Parameter 3D-T1 weighted GRE 2D-T1 weighted GRE
TR 4.5 4.5
TE 1.42 1.42
Flip-angle 20° 20°
Voxel size 1.25 mm×1.30 mm×3.00 mm
1.25 mm×1.30 mm×6.0 mm
Sense factor 2.3×1.0×2.5 2.0×1.0
Acquisition time 37.7 s 29.7 s
Fig. 1 The left side of the Fig. shows a sagittal view of the T1-w MRIof the bowel loop of interest which was framed by the use of semiau-tomatic software and followed over time. The image on the right showsthe plotted change in area of the bowel lumen in cm2 over time. The
bowel clearly reveals rhythmic motion under normal conditions. Spas-molysis with complete arrest of motility occurs shortly after intrave-nous administration of Glucagon (syringe)
1188 Eur Radiol (2012) 22:1186–1194
mean variability of three initial measurements were definedas 100%. This allows normalized comparison of the subse-quent drug effects in relation to baseline motility. Therefore,percentage variabilities of all following breathholds afterdrug administration were calculated in relation to the initialvalues. Values below 50% were defined as a relevant anti-peristaltic effect of the drug. Thus the onset of effect, dura-tion of aperistalsis and its efficacy could be determined. Incases of several separate periods of drug effect, only the firstcontinuous period was considered. A maximum of oneoutlier (defined as one measurement above 50%, whichhad to be followed by at least 10 measurements below50%) during drug effect was allowed. The proportionalvalues of each breath-hold interval covering 30 s of imagingwere plotted on graphs for each drug regimen showing theentire follow-up period of 60 to 90 min.
Statistical analysis
Drug effects (effect onset, duration of effect, and drug efficacy)were compared between different drug administration’s using aFriedman or a Wilcoxon signed ranks test. Homogeneity ofvariance was tested with a Brown-Forsythe test. The signifi-cance level was set at P00.05.
Results
All subjects were successfully imaged without complica-tions or drop-outs over the scheduled time period of60 min for intravenous administration and 90 min for intra-muscular and combined administration. Figure 2 illustratesbowel motility by showing the original area data over time.Three phases are typically discernable comprising initialnormal bowel movement, aperistalsis after drug administra-tion and return of bowel movement during recovery. Post-processing and transposition of data into motility was feasiblein all 30 examinations (Fig. 3). Statistical analysis revealedthat both Hyoscine i.v. and Glucagon i.v. arrested bowelmovement early at 85 (+/− 24.5) and 65 (+/−24.5)s after drugadministration, respectively. Intramuscular administration waseffective after a longer delay of 310 (+/− 110.1)s for Hyoscineand 696 (+/− 609.8)s for Glucagon. Thus, the anti-peristalticeffect began much later after intramuscular than after intrave-nous administration (P00.001; Wilcoxon signed ranks test).Moreover, the higher standard deviations for the duration ofdrug effects after intramuscular administration revealed greaterinter-individual differences (P00.012; Brown-Forsythe test).The onset of effect, duration of aperistalsis and efficacy for alldrug administration’s regimes are summarized in Fig. 3.
The individual plots for all volunteers and drug admin-istration’s (Fig. 3) shows interindividual variation, whichdepends to a large extent also on the mode of administration.
Repeated phases of aperistalsis interrupted by phases ofregular or more than 50% normal motility are mainly notedduring intramuscular administration. While the differencesin the onset of effect are statistically significant (P00.001;Friedman test), the differences in the duration of aperistalsisand its intensity are not. Nonetheless, compared to the otherdrug administrations, the combined scheme provides notonly an early onset of effect, but also the longest period ofaperistalsis and the most reduced motion in relation to thebaseline measurement. Thus this scheme provides also ahigh predictability of effect.
Discussion
Spasmolytic drugs are important to ensure high qualityimages with minimal gastrointestinal movement artefactsduring radiological investigations of the abdomen and thepelvis. Bowel paralysis should be sufficiently sustained toallow more prolonged imaging acquisition procedures suchas MRI or angiography (typically about 30 min). Normalbowel peristalsis can impair image quality rendering diagnosismore difficult [2–4, 11–13]. (Figs. 2, 4).
In our study, different degrees of spasmolytic efficacywere observed according to the type of spasmolytic drug(Hyoscine and Glucagon) and the route of administration (i.v.and i.m.). Under normal conditions, gut motility is character-ized by a more or less rhythmic pattern of relaxation andcontraction (Fig. 5). Depending on the route of administration,injection of a spasmolytic agent causes either an immediate(intravenous) or a delayed (intramuscular) effect. Immediatearrest of motility after intravenous administration has recentlybeen reported in another study [14, 15]. However, we foundthat compared to Hyoscine the effect of intravenous Glucagonpersists for a slightly longer period of time (21±12.3 min /23.2±14 min for Hyoscine and Glucagon, respectively) [15].
In the present study the i.m. administration of Hyoscineand Glucagon had a less reliable effect over time with largerinterindividual variation for effect onset and duration. As thedrug substances are released slower into the systemic circu-lation, they might not exceed the threshold concentrationnecessary for inhibiting peristalsis. Other factors such aslocal perfusion, activation of the muscle or general proper-ties of the tissue of interest may also contribute to thisvariability. Thus, clinical use of a single agent administeredvia the i.m. route, although widely practiced, may be sub-optimal because of the unpredictability in the onset andduration of effects. We found that the combination of intra-venous Glucagon with intramuscular Hyoscine resulted inan immediate effect, which persisted for the longest periodof time and with the highest efficacy. Besides the pharma-cological effect over two different receptor systems, theaddition of an i.m. drug seems to act synergistically, leading
Eur Radiol (2012) 22:1186–1194 1189
to a more prolonged and sustained effect of spasmolysiscompared to lone i.v administration of a single drug. Over-all, the predictability appears highest for this mode ofadministration.
Due to the lack of well controlled efficacy studies indiagnostic imaging, little is known about the optimal clinicaluse of spasmolytic drugs, even though these are widely usedin clinical departments. As shown in Figs. 2 and 4, effective
spasmolysis is critical to radiological investigations such asabdominal and pelvic MRI or DSA. Recently, Froehlich etal investigated the effect of Glucagon as opposed to Hyo-scine after intravenous administration [15].Glucagon wasfound to exert a more prolonged effect (mean, 18.3 min)compared to Hyoscine (mean, 6.8 min). This prolongedduration of effect with glucagon was as well confirmed inthe present study. Other endpoints, a differing method of
Fig. 2 This illustration shows the decisive effect of spasmolysis onimage quality in a normal volunteer. In the left column, the 3D seriesshow marked blurring and artifacts during normal motility. On thebottom of the left side, the motility curves show a normal physiologicalrhythmic movement pattern. The middle column shows completelyarrested motility after i.v. administration of Glucagon: note the absenceof rhythmic movement corresponding to a null line of motility on the
plots depicting the cross-section areas over time on the bottom line(comparative to the drug effect as in Fig. 1). Image quality is markedlyimproved on the 3D sequence shown in the upper row. The effect of thespasmolytic agent is reduced 60 min after administration of spasmo-lytic agent as shown in the right column. This, in turn, markedlyimpairs quality of the movement sensible 3D sequences
1190 Eur Radiol (2012) 22:1186–1194
quantitative analysis and study design explain the differingresults of both studies but with similar qualitative information.Some centers use i.m. administration routinely in the hope toachieve prolonged effects compared to i.v. administration.
Due to a lack of guidelines for the usage and administrationof spasmolysis, our results are of high practical relevance asthey demonstrate the great variability of onset and durationwhen the i.m. route is chosen. In individual cases, (Fig 3; for
Fig. 3 Overview of all six volunteers (lines) with their respective drugadministration modes (columns) covering the entire MRI measurementcorresponding to 60 min for i.v. administrations and 90 min for i.m. orcombined schemes. The black bold dots represent the phase wherespasmolysis is rated as sufficient corresponding to a standard deviationof amplitudes beyond 50% compared to mean baseline movement
equal to 100%. Beyond the single schemes of effect the data tableshows mean onset of effect, duration of effect and efficiency (±STD;detailed description of methodology in M&M section). Note the highintraindividual differences regarding the spasmolytic effect which dif-fer between the drug administration modes and for the singlevolunteers
Eur Radiol (2012) 22:1186–1194 1191
example 5th volunteer) i.m. administration may lead to aprolonged cessation of the intestinal motility, while theremay be little effects in other cases (Fig 3; for example 4th
volunteer). From a practical point of view, such a high degreeof variability of drug effects is unreliable for clinical practice.One of the difficulties in our study was to define sufficient
Fig. 4 Example of a typicaldigital subtraction angiographyof a single patient pre- (leftside) and post (right side)administration of i.v. Glucagon(1 mg). One clearly recognizesthe improvement of imagequality and vessel delineationon the right side due to reducedmovement artefacts after drugeffect. Especially the improvedquality of the small vesselscircumscribed with a circlecan be noted
Fig. 5 Plot of the original raw data of a single volunteer (N° 2according to Fig. 3) showing changes of cross-section areas over timefor a single small bowel loop corresponding to motility. Initial baselinemeasurement without any spasmolytic drug was repeated at least threetimes and defined as 100% (left: initial phase of curve). After admin-istration of i.v. Glucagon combined with i.m. Hyoscine the drugs
exerted a rapid spasmolytic effect. In this case, drug effect lasted overa relatively long time period with little rest movement and thus highspasmolytic efficiency. Return to normal motility seems to occur quiterapidly with returning regular oscillating amplitudes as shown furtherto the right
1192 Eur Radiol (2012) 22:1186–1194
spasmolysis for imaging as motility is usually not completelyarrested like an on-off phenomenon (Fig. 5). In an earlierstudy [15] spasmolysis was defined qualitatively on singleplots representing cross-section diameters over time of singlebowel loops, while in the present study a clear quantitativeendpoint (>50% of amplitude variability compared to baselinebefore administration of spasmolytic drugs) was defined.However, this well-defined threshold-value of amplitudevariability does not necessarily correspond to a level of anti-peristaltic effect sufficient for high-quality imaging.
To our knowledge, this is the first prospective studycomparing the small bowel motility effects of intravenousand intramuscular administration of Hyoscine and Glucagon- two of the principal spasmolytic drugs used in clinicalroutine. In addition, our study supports the synergistic useof two spasmolytic agents highly promising in cases withpoor response, which should be addressed in future studies.In clinical practice, cessation of peristalsis is difficult toconfirm as movement artifacts may also result from breathing,heart and blood flow, or even pulse sequence (e.g. from tablevibration incurred during a DW-sequences).
MRI permits non-invasive dynamic imaging of the smallbowel thus allowing assessment of deformations of individualbowel segments over time. Bowel motility has been assessedby various MRI techniques such as two-dimensional turbofast-field echo [16] or a balanced steady-state free precessionsequence [17].In these recent studies, the deformation of theanalyzed bowel loops was recorded by measuring the cross-section diameters of the bowel lumen over time. These one-dimensional values yielded motility patterns with amplitudesand frequencies of wall contractions in single small bowelsegments. In contrast, we did not determine the cross-sectionluminal diameter of the bowel but its luminal cross-sectionalarea. Theoretically, this two-dimensional measurementshould be more precise than a simple one-dimensionalmeasurement.
Our study bears the following limitations. First, we couldonly investigate this study in a small group of volunteersbecause of the high level of compliance needed to fulfill thestudy protocol. Volunteers underwent five separate imagingsessions lasting between 60 and 90 min with the need forrepeated breath-holds. Second, we only analyzed the motil-ity of a single small bowel loop. However, due to the highnumber of data points acquired to each loop, we had a highdegree of confidence in its motility before and after drugadministration. Third, combined injections of Glucagon andHyoscine using the same injection route (i.v. + i.v.; i.m. + i.m.)were not allowed for safety reasons in the present study fromour ethical commission. Last, although our approach allowsquantifying the degree of inhibitory drug effect on smallbowel motility based on bowel cross-section area analysisover time, our threshold value for spasmolysis does not nec-essarily correspond to an optimal degree of spasmolysis
necessary for optimal image quality. Further investigationsare required in this area.
In conclusion, intravenous use of spasmolytic drugsresults in a faster onset and better predictability of effectcompared to the intramuscular administration. Intravenousglucagon guarantees a longer spasmolytic effect comparedto i.v. hyoscine. The combination of intravenous and intra-muscular administration of both spasmolytic agents (glucagoni.v., hyoscine i.m.) has the longest and most reliable spasmo-lytic effect compared with all other schemes.
Acknowledgement We would like to thank Philips Healthcare Swit-zerland for their valuable technical support. We also thank Mr. Hofmannand Mr. Hartmann at our photography department of the Cantonal Hos-pital Winterthur for their well appreciated assistance in the production ofillustrations and photographs. Moreover, we would like to acknowledgethe help provided by Selina Froehlich supporting us in the post-processing of the data. Finally, our special thanks go as well to Dr. EricSchoch, who performed the DSA images.
References
1. Husebye E (1999) The patterns of small bowel motility: physiol-ogy and implications in organic disease and functional disorders.Neurogastroenterol Motil 11:141–161
2. Kozak RI, Bennett JD, Brown TC, Lee TY (1994) Reduction ofbowel motion artifact during digital subtraction angiography: acomparison of hyoscine butylbromide and glucagon. Can AssocRadiol J 45:209–211
3. Laniado M, Grönewäller E, Kopp AF et al (1997) The value ofhyoscine butylbromide in abdominal MR imaging with and withoutoral magnetic particles. Abdom Imaging 22:381–388
4. Johnson W, Taylor MB, Carrington BM, Bonington SC, SwindellR (2007) The value of hyoscine butylbromide in pelvic MRI. ClinRadiol 62:1087–1093
5. Martí-Bonmatí L, Graells M, Ronchera-Oms CL (1996) Reductionof peristaltic artifacts on magnetic resonance imaging of theabdomen: a comparative evaluation of three drugs. Abdom Imaging2:309–313
6. Wagner M, Klessen C, Rief M et al (2008) High-resolution T2-weighted abdominal magnetic resonance imaging using respiratorytriggering: impact of butylscopolamine on image quality. ActaRadiol 49:376–382
7. Mayo KE, Miller LJ, Bataille D et al (2003) International Union ofPharmacology. XXXV. The glucagon receptor family. PharmacolRev 55:167–194
8. Dubé PE, Brubaker PL (2007) Frontiers in glucagon-like peptide-2: multiple actions, multiple mediators. Am J Physiol EndocrinolMetab 293:E460–E465
9. Tytgat GN (2008) Hyoscine butylbromide—a review on its paren-teral use in acute abdominal spasm and as an aid in abdominaldiagnostic and therapeutic procedures. Curr Med Res Opin24:3159–3173
10. Huizinga JD, McKay CM, White EJ (2006) The many facets ofintestinal peristalsis. Am J Physiol Gastrointest Liver Physiol 290:G1347–G1349
11. Stone AJ, Browne JE, Lennon B, Meaney JF, Fagan AJ (2011)Stone Quantification of accuracy of ADC measurements fromWhole-body DWIBS. Proc Intl Soc Mag Reson Med 19:836
12. Rowland-Hill CA, Loveday EJ, Thomas ML (1989) A com-parison of the value of hyoscine butylbromide and glucagon
Eur Radiol (2012) 22:1186–1194 1193
on aorto iliac intravenous digital subtraction. Vasa 18:301–303
13. Rogalla P, Lembcke A, Rückert JC et al (2005) Spasmolysis at CTcolonography: butyl scopolamine versus glucagon. Radiology236:184–188
14. Gutzeit A, Patak MA, von Weymarn C et al (2010) Feasibility ofsmall bowel flow rate measurement with MRI. J Magn ResonImaging 32:345–351
15. Froehlich JM, Daenzer M, von Weymarn C et al (2009) Aperis-taltic effect of hyoscine N-butylbromide versus glucagon on the
small bowel assessed by magnetic resonance imaging. Eur Radiol19:1387–1393
16. Froehlich JM, Patak MA, von Weymarn C, Juli CF, ZollikoferCL, Wentz KU (2005) Small bowel motility assessment withmagnetic resonance imaging. J Magn Reson Imaging 21:370–375
17. Wakamiya M, Furukawa A, Kanasaki S, Murata K (2011) Assess-ment of small bowel motility function with cine-MRI using balancedsteady-state free precession sequence. J Magn Reson Imaging33:1235–1240