8/14/2012 1 Every patient is an athlete: Hot Topics in Sports Medicine 2012 Carlin Senter M.D. Primary Care Sports Medicine UCSF Internal Medicine and Orthopaedics UCSF Essentials of Primary Care August 14, 2012 In 50 minutes you will know 1. The return to play/work progression for concussion treatment. 2. 2 unique causes of fatigue in an athlete. 3. 5 questions to ask every athlete with hip pain. 4. How to write an exercise prescription. Case #1 • 40 y/o woman presents to your office for ER follow-up one week after bike accident. • Went over handle bars traveling on city streets. • No loss of consciousness. • Taken by ambulance to ER. • Had trauma work-up including head CT (-). • Diagnosed with clavicle fracture, nonoperativetxby orthopaedic surgeon, discharged home. • Has headache, fatigue, dizziness, light sensitivity. Trouble staying focused at work, sleeping more than usual. • Normal neurologic exam. Diagnosis: Concussion • H/o trauma • Headache • Fatigue • Dizziness • Light sensitivity • Trouble staying focused at work • Sleeping more than usual.
Transcript
8/14/2012
1
Every patient is an athlete: Hot Topics in Sports Medicine 2012
Carlin Senter M.D.Primary Care Sports Medicine
UCSF Internal Medicine and Orthopaedics
UCSF Essentials of Primary Care August 14, 2012
In 50 minutes you will know1. The return to play/work progression for
concussion treatment.2. 2 unique causes of fatigue in an athlete.3. 5 questions to ask every athlete with hip pain.4. How to write an exercise prescription.
Case #1• 40 y/o woman presents to your office for ER follow-up one
week after bike accident.• Went over handle bars traveling on city streets. • No loss of consciousness.• Taken by ambulance to ER.• Had trauma work-up including head CT (-).• Diagnosed with clavicle fracture, nonoperative tx by
Does iron deficiency without anemia impair performance?
Does treating this improve performance?
Controversial
Normal Iron deficient Anemic
FerritinHemoglobin
Does iron deficiency without anemia impair performance?
• 48 non-anemic collegiate rowers at beginning of season– 24 normal, 24 “depleted” (Ferritin < 20 µg/L.)– Compared to normals, depleted group demonstrated
• 10min less training/day• 0.3L/min lower VO2 peak• Higher lactate during 4K time trial
Does treating iron deficiency without anemia improve performance?
• Garza Clin J Sports Med,1997 meta analysis– Increasing ferritin levels does not lead to improvements in endurance
performance– In athlete with low ferritin and low-normal hemoglobin, “relative anemia”
may be present and iron supplementation may help improve performance by increasing hemoglobin
• Hinton et al. J Appl Physiol, 2000.– RCT with 42 untrained women with avg ferritin 9 and Hgb 13– Iron supplementation x 6wks– Iron group: ferritin incr 10 to 14.5, no change Hgb, decreased time to
complete time trial, increased O2 consumption, no change VO2max• Friedmann et al. Med Sci Sports Exerc, 2001
– RCT 40 elite athletes with ferritin < 20 and avg Hgb 13.6– Iron supplement x 12 wks– Iron group: ferritin incr 16 to 40, no change Hgb, increased VO2max, oxygen
consumption, time to exhaustion
8/14/2012
8
Effects of iron deficiency without anemia: controversial
• Low ferritin indicates relative anemia in some athletes. Improved performance is based on improved hemoglobin with supplementation leading to increased oxygen carrying capacity leading to increased VO2.
OR• Low ferritin indicates decreased store of iron in tissue
leading to decreased function of mitochondrial iron complexes which may or may not affect VO2max but compromises endurance capacity in athletes.
Iron supplementation for elite athletes• Iron deficiency with anemia
– Treat with iron supplementation as you would with non-athlete
– Goal = normal hemoglobin (> 12g/dL for women)– Improves athletic performance, increases VO2max
• Iron deficiency without anemia– No defined protocol– Studies use different cut-offs to define low ferritin in
athletes• Australian Institute of Sport
– Ferritin ≤ 20 µg/L = iron deficiency without anemia– Goal Ferritin 30 µg/L
Case #3• 18 y/o freshman cross-
country runner• “heart beat stays fast”• “hard to stop sweating”• “tired all the time”• Times worse than when in
• If symptoms continue – More rest– Track symptoms– Track mood scores– Sports psychology– Nutrition http://www.genucare.com/archives/496.html
Case #4• 20 y/o collegiate cross
country athlete• Presents to clinic with right
groin pain• Started a few weeks ago,
getting worse gradually• Still able to run but pain
gets worse the more she runs, hard to lift her leg due to pain
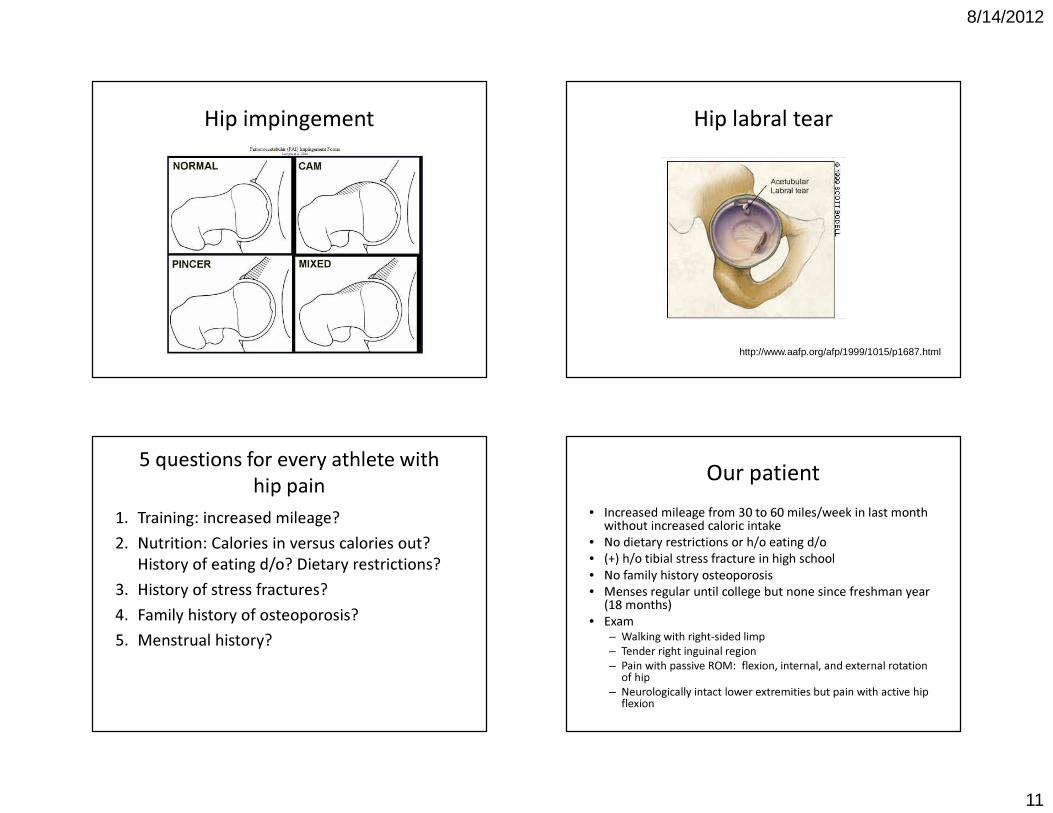
Differential diagnosisgroin pain in runner
• Intraarticular hip problem– Impingement– Labral tear– Femoral neck stress
fracture • Extraarticular hip
problem– Hip flexor strain– Sports hernia
• GI/gyn problemsFalvey EC et al, BJSM. 2007.
8/14/2012
11
Hip impingement Hip labral tear
http://www.aafp.org/afp/1999/1015/p1687.html
5 questions for every athlete with hip pain
1. Training: increased mileage?2. Nutrition: Calories in versus calories out?
History of eating d/o? Dietary restrictions?3. History of stress fractures?4. Family history of osteoporosis?5. Menstrual history?
Our patient• Increased mileage from 30 to 60 miles/week in last month
without increased caloric intake• No dietary restrictions or h/o eating d/o• (+) h/o tibial stress fracture in high school• No family history osteoporosis• Menses regular until college but none since freshman year
(18 months) • Exam
– Walking with right-sided limp– Tender right inguinal region– Pain with passive ROM: flexion, internal, and external rotation
of hip– Neurologically intact lower extremities but pain with active hip
flexion
8/14/2012
12
Hip passive range of motion
Flexionnormal 120°
External rotationnormal 40-60°
Internal rotationnormal 30-40°
http://www.youtube.com/watch?v=5LNYdJIrWYo
What’s your leading diagnosis?
H i p f l e x
o r st r . . .
H i p i m p
i n g em e
n . . . G I /
g y n p r o
b l em . . .
S p or t s
h e rn i a
F e mo r a
l n ec k s
. . .
20%
54%
18%
6%2%
1. Hip flexor strain2. Hip impingement or hip labral tear3. GI/gyn problems4. Sports hernia5. Femoral neck stress fracture
High index of suspicion to prevent bad outcome Female athlete triad
Healthy energy status
Healthy menstrual
cycles
Healthy bones
Low energy availability with or without eating d/o
Osteoporosis Amenorrhea
Low bone density
Suboptimal energy availability
Irregular menses
OPTIMAL HEALTH
PATHOLOGY
Nattiv A et al, ACSM Position Stand, 2007.
8/14/2012
13
Female athlete triad treatment• Best treatment = prevention
– Screen for risk factors– Finding 1 risk factor should prompt eval for others
• Increase energy availability – Increase dietary intake– Decrease exercise– Has been shown to restore menses– Has been shown to increase bone density
• Estrogen: does not improve BMD as much as if menses are restored with increased energy availability
What treatment would most benefit this patient now and in the long run? Strong evidence that physical activity
associated with lower risk of• Coronary artery
disease• Stroke• High blood pressure• High cholesterol
• Type 2 diabetes• Colon cancer• Breast cancer• Falls
US Dept Health and Human Services. Physical Activity Guidelines Advisory Committee Report, 2008: http://www.health.gov/paguidelines/guidelines/chapter2.aspx. Accessed 11/6/2011.
8/14/2012
14
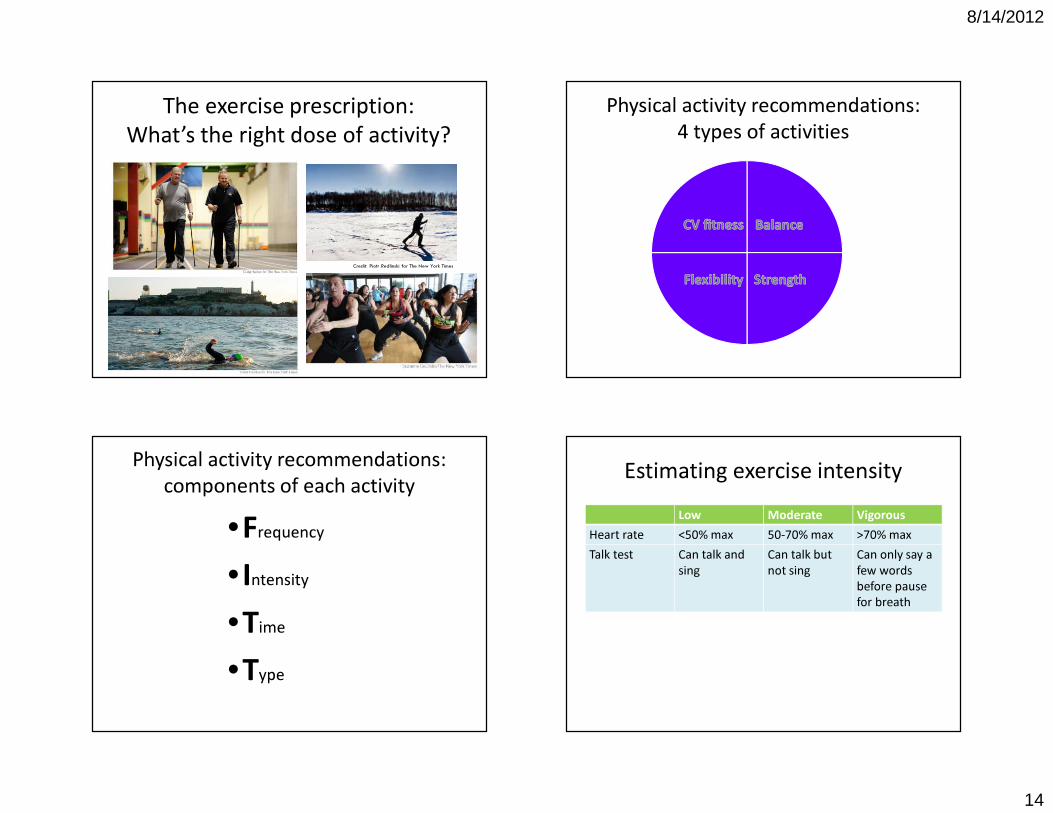
The exercise prescription: What’s the right dose of activity?
Credit: Piotr Redlinski for The New York Times
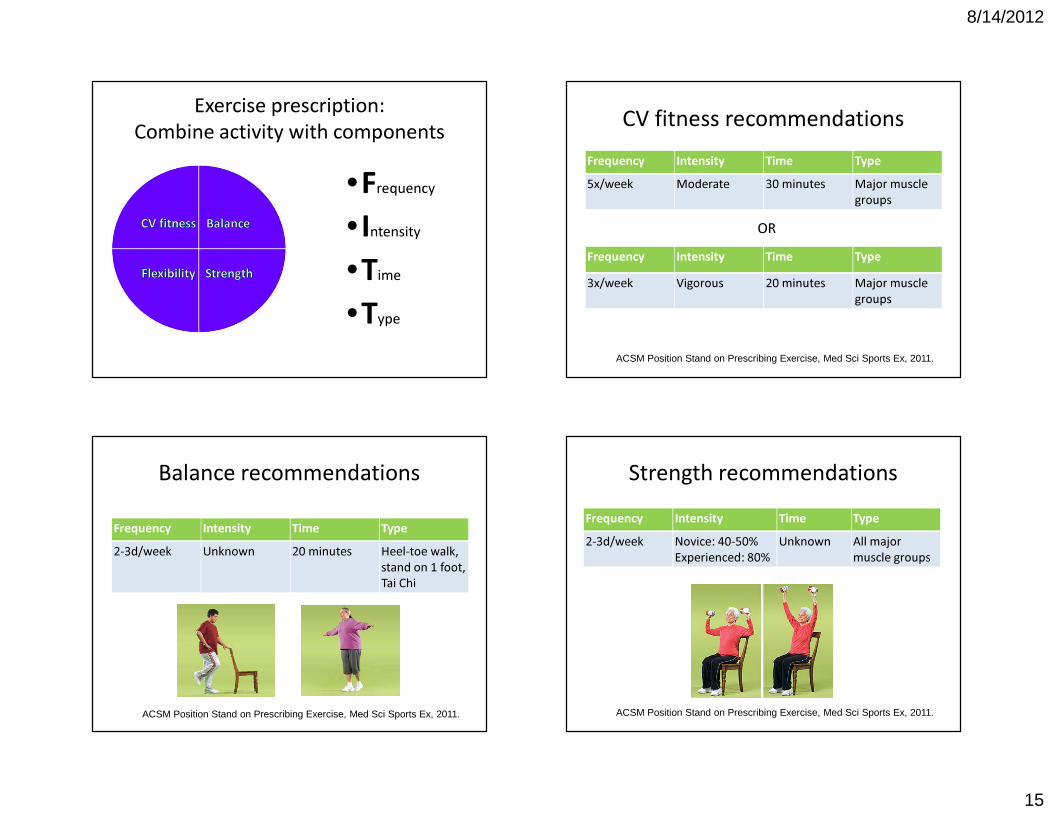
Physical activity recommendations: 4 types of activities
Physical activity recommendations: components of each activity
“All parts of the body if used in moderation and exercised in labors to which each is
accustomed, become thereby healthy and well developed, and age slowly; but if
unused and left idle, they become liable to disease, defective in growth, and age
quickly.”Hippocrates
Thank you!
Carlin Senter, M.D.Primary Care Sports Medicine
UCSF Internal Medicine and Orthopaedics http://www.cdc.gov/physicalactivity/everyone/guidelines/index.html Accessed October 23, 2011.
8/14/2012
19
http://go4life.niapublications.org/ Accessed October 23, 2011.http://go4life.niapublications.org/try-these-exercises#strength-exercises Accessed October 23, 2011.
http://win.niddk.nih.gov/publications/walking.htm Accessed October 23, 2011.