Robert O. Bonow, MD, MS No Relationships to Disclose Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology Evidence-Based Management of Mitral Regurgitation?
Transcript
Robert O. Bonow, MD, MS
No Relationships to Disclose
Northwestern University Feinberg School of Medicine
Bluhm Cardiovascular Institute
Northwestern Memorial Hospital
Editor-in-Chief, JAMA Cardiology
Evidence-Based Management
of Mitral Regurgitation?
www.acc.org
www.americanheart.org
Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation
Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation
• Symptomatic patients class I
Mitral regurgitation
Indications for mitral valve surgery
for primary MR?
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
class I
class I
Mitral regurgitation
Indications for mitral valve surgery
for primary MR?
LVEF <60%
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
class I
class I
Mitral regurgitation
Indications for mitral valve surgery
for primary MR?
LVEF <60%
LVSD >40mm
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
class I
class I
class IIa
Mitral regurgitation
Indications for mitral valve surgery
for primary MR?
PASP >50 mmHg at rest
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
class I
class I
class IIa
class IIa
Mitral regurgitation
Indications for mitral valve surgery
for primary MR?
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function,
repair feasible? ?
class I
class I
class IIa
class IIa
Mitral regurgitation
Indications for mitral valve surgery
for primary MR?
Asymptomatic severe primary MR:
• 66% come to surgery in 5 years because
of symptoms, LV dysfunction, pulmonary
hypertension or AF
• Long-term postoperative survival is worse
if surgery is performed after patients
become symptomatic
Indications for mitral valve repair
for asymptomatic primary MR:
Mitral regurgitation
class IIa
• Chronic severe MR
• Preserved LV function
• Experienced surgical center
• Likelihood of durable repairwithout residual MR > 95%
Mitral regurgitation
class IIa
class I
Indications for mitral valve repair
for asymptomatic primary MR:
!• Repair better than mitral valvereplacement
• Patients should be referred tocenters experienced in repair
• Chronic severe MR
• Preserved LV function
• Experienced surgical center
• Likelihood of durable repairwithout residual MR > 95%.
• STS Database 2011-2016
• Isolated primary MV surgery
• 87,214 patients
Annual Case Volume
Degenerative Mitral Disease
Cases Centers
0 106
1-6 763
6-25 213
26-50 28
50-100 11
>100 4
Repair rate 66.7%
Repair rate 90.0%
Mitral regurgitation
class IIb
Indications for transcatheter MV
repair for severe primary MR:
• Chronic severe MR
• Severely symptomatic
• Prohibited surgical risk
• Reasonable life expectancy
Mitral regurgitation
Primary MR: primary valve disease
Secondary MR: primary myocardial disease
Mitral regurgitation
Primary MR: primary valve disease
Secondary MR: primary myocardial disease
• Post MI,
• Heart failure
• Dilated cardiomyopathy
Mitral regurgitation
Primary MR: primary valve disease
Secondary MR: primary myocardial disease
• Diagnostic dilemmas
• Therapeutic dilemmas
Deja et al. Circulation 2012
p<0.001
0
200
400
600
800
1 2 3 4 5 6 7 8
Ischemic Cardiomyopathy80
0
Time (years)
0
60
40
20Mort
alit
y (
perc
ent)
1 2 3 4 5 6
55%
47%
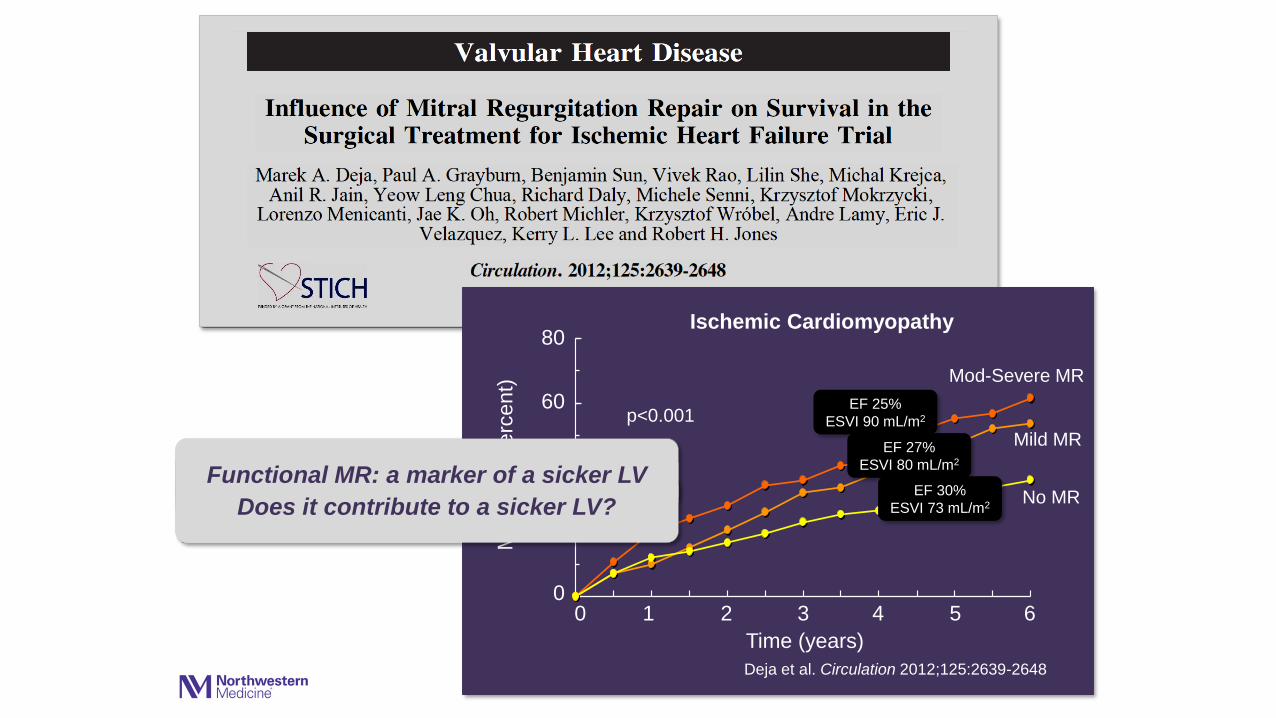
30%
Deja et al. Circulation 2012;125:2639-2648
No MR
Mild MR
Mod-Severe MR
p<0.001
Deja et al. Circulation 2012
p<0.001
0
200
400
600
800
1 2 3 4 5 6 7 8
Ischemic Cardiomyopathy80
0
Time (years)
0
60
40
20Mort
alit
y (
perc
ent)
1 2 3 4 5 6
Deja et al. Circulation 2012;125:2639-2648
No MR
Mild MR
Mod-Severe MR
EF 25%
ESVI 90 mL/m2
EF 27%
ESVI 80 mL/m2
EF 30%
ESVI 73 mL/m2
p<0.001
Functional MR: a marker of a sicker LV
Does it contribute to a sicker LV?
Secondary mitral regurgitation
can be repaired.
But should it be repaired?
Secondary mitral regurgitation
can be repaired.
But should it be repaired?
0
20
40
60
80
100
1 2 3 4 5 6 7 8
100
80
Su
rviv
al (p
erc
en
t)
60
40
20
0
p=NS
n=419
Medical
Surgical
5000 1000 1500 2000
Wu et al. J Am Coll Cardiol 2005;45:381-387
Time (days)
Secondary mitral regurgitation
Guideline-directed medical
therapy for heart failure,
including CRT
class I
Indications for mitral valve surgery:
Secondary mitral regurgitation
Guideline-directed medical
therapy for heart failure,
including CRT
Indications for mitral valve surgery:
• Patients with severe MR undergoing CABG or AVR
class I
class IIa
Secondary mitral regurgitation
Indications for mitral valve surgery:
• Patients with severe MR undergoing CABG or AVR
class IIb• Severe MR, persistent
symptoms despite optimal medical therapy, including CRT
class IGuideline-directed medical
therapy for heart failure,
including CRT
class IIa
Baseline Optimized Medical Therapy
and Biventricular Pacing
Obadia et al. N Engl J Med 2018;379:2297-2306
MITRA-FR Trial
COAPT Trial
Stone et al. N Engl J Med 2018;379:2307-2318
COAPT Trial
Stone et al. N Engl J Med 2018;379:2307-2318
COAPT Trial
67.9%
45.7%
Control group
Device group
Stone et al. N Engl J Med 2018;379:2307-2318
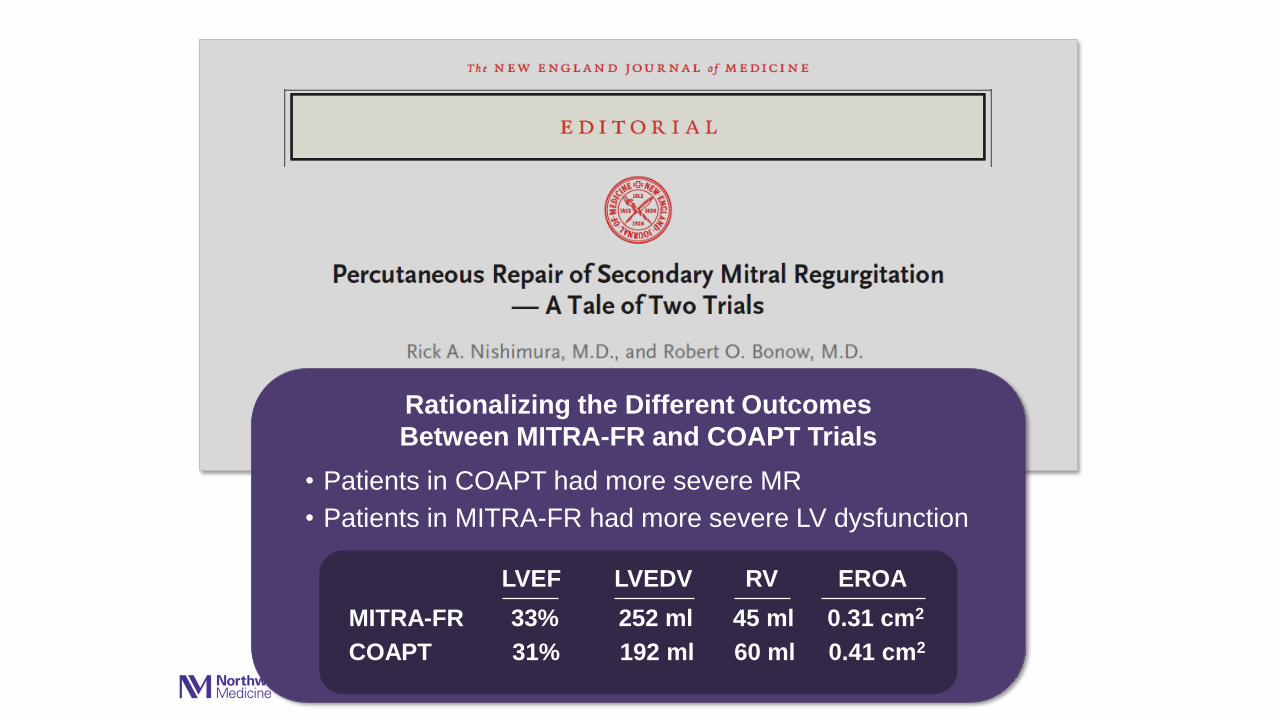
Rationalizing the Different Outcomes
Between MITRA-FR and COAPT Trials
• Patients in COAPT had more severe MR
• Patients in MITRA-FR had more severe LV dysfunction
• Medical therapy was more aggressively optimized
before randomization in COAPT
• COAPT operators more experienced; lower rates of
residual MR at 12 months
Rationalizing the Different Outcomes
Between MITRA-FR and COAPT Trials
• Patients in COAPT had more severe MR
• Patients in MITRA-FR had more severe LV dysfunction
LVEF LVEDV RV EROA
MITRA-FR 33% 252 ml 45 ml 0.31 cm2
COAPT 31% 192 ml 60 ml 0.41 cm2
Grayburn et al. JACC Cardiovasc Imaging 2019;12:353-362