Evidence-based Medicine: Treatment of Crohn’s Disease Raymond Cross, MD, MS, AGAF Professor of Medicine Director, IBD Program University of Maryland School of Medicine Co-Director Digestive Health Center University of Maryland Medical Center Millie Long, MD, MPH Assistant Professor of Medicine University of North Carolina
Transcript
Evidence-based Medicine: Treatment of Crohn’s Disease
Raymond Cross, MD, MS, AGAF Professor of Medicine Director, IBD Program
University of Maryland School of Medicine Co-Director Digestive Health Center
University of Maryland Medical Center Millie Long, MD, MPH
Assistant Professor of Medicine University of North Carolina
Disclosures
• Abbvie: Research grants, participation in advisory boards, and consulting
• Janssen: Participation in advisory boards
• Takeda: Consulting
• UCB: Consulting
Goals of Therapy
• Induce clinical remission (absence of symptoms)
• Avoid short and long term toxicity of therapy
• Maintain steroid-free remission
– Avoid repeated courses of steroids
• Enhance quality of life
• Prevent/treat complications of disease
• Achieve mucosal healing (“deep remission”)
• Decrease unnecessary health care expenditures (ER visits, hospitalizations, etc.)
Pentasa reduces CDAI compared to placebo
Clinical Gastroenterology and Hepatology 2004; 2:379-388
Colombel, J.F., et al. N Engl J Med. 2010;362(15):1383-1395
Pati
en
ts (
%)
P=.02
P<.001
P=.06 P=.006
P=0.02
P<.001
51/170 75/169 96/169 18/109 28/93 47/107 P
ati
en
ts (
%)
30.0%
44.4%
56.8%
16.5%
30.1%
43.9%
100
0 AZA + PBO
IFX + PBO
IFX + AZA
AZA + PBO
IFX + PBO
IFX + AZA
Clinical Remission Mucosal Healing
90
80
70
60
50
40
30
20
10
100
0
90
80
70
60
50
40
30
20
10
PBO = placebo; IFX = infliximab.
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Weeks
MTX Placebo
No Benefit of MTX in Addition to Steroids and IFX for CD
Feagan, B. G., et al. (2014). Gastroenterology
n= 63/group
Pati
en
ts i
n r
em
issio
n [
%]
Prednisone
taper week 0-14
Treatment failure week 14: 24% IFX/MTX, 22% IFX
Treatment failure week 50: 44% IFX/MTX, 43% IFX
Vedolizumab in CD: Second Induction Study
Clinical Remission (CDAI ≤150) at Week 10 (Secondary Endpoint)
Sands, B. E., et al. (2014). Gastroenterology 147(3): 618-627 e613.
.
GEMINI II: Vedolizumab in Crohn’s Disease Through Week 52, Maintenance ITT
Sandborn, W. J., et al. (2013). N Engl J Med 369(8): 711-721.
Ustekinumab Induction Therapy for Anti-TNF Experienced Patients (UNITI-1)
7%
20% 16%
34%
21%
38%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Remission Response
Pe
rce
nt
of
Pat
ien
ts
Placebo 130 mg 6 mg/kg
Feagan, B. G., et al. (2016). N Engl J Med 375(20): 1946-1960.
Ustekinumab Induction Therapy for Treatment Refractory Patients (UNITI-2)
20%
32% 31%
47% 40%
58%
0%
10%
20%
30%
40%
50%
60%
70%
Remission Response
Pe
rce
nt
of
Pat
ien
ts
Placebo 130 mg 6 mg/kg
Feagan, B. G., et al. (2016). N Engl J Med 375(20): 1946-1960.
Clinical Remission at Week 44 after Treatment with Ustekinumab (IM-UNITI)
26%
44% 39%
57%
41%
63%
0%
10%
20%
30%
40%
50%
60%
70%
Remission (UNITI-1) Remission (UNITI-2)
Pe
rce
nt
of
Pat
ien
ts
Placebo 90 q 12 90 q 8
Feagan, B. G., et al. (2016). N Engl J Med 375(20): 1946-1960.
Use of Therapeutic Drug Levels to Guide Changes in Therapy
Response to Test
Clinical Response
P value
Detectable HACA
Increase IFX 17% P<0.004
Change Anti-TNF
92%
Subtherapeutic concentration
Increase IFX 86% P<0.016
Change Anti-TNF
33%
Afif, W., et al. (2010). Am J Gastroenterol 105(5): 1133-1139.
IFX Dosed Based on TDM vs. Clinically Based Dosing of IFX: TAXIT
66 69
0
10
20
30
40
50
60
70
80
90
100
Pe
rce
nt
of
Pat
ien
ts
Clinical and biological remission at one year
CB
LB
N=111/126 N=115/126
Vande Casteele, N., et al. (2015). Gastroenterology 148(7): 1320-1329 e1323.
29% of patients had an IFX level below 3 mcg/ml at baseline; remission rate increased from 65 to 88% (p=0.020) after one time dose optimization
IFX Reduces Post-operative Recurrence after Intestinal Resection
0
10
20
30
40
50
60
70
80
90
100
Placebo IFX
End
osc
op
ic R
ecu
rre
nce
Rat
e
Regueiro, M., et al. (2009) Gastroenterology
Endoscopic Recurrence: endoscopic scores of i2, i3, or i4
The PREVENT Trial: Trends favoring IFX were observed for fewer clinical (wk76, wk104) and endoscopic (wk76) recurrences but the primary endpoint of clinical recurrence
was not met
Prevent: Clinical Outcomes at Week 76
Regueiro, M., et al. (2016). Gastroenterology 150(7): 1568-1578
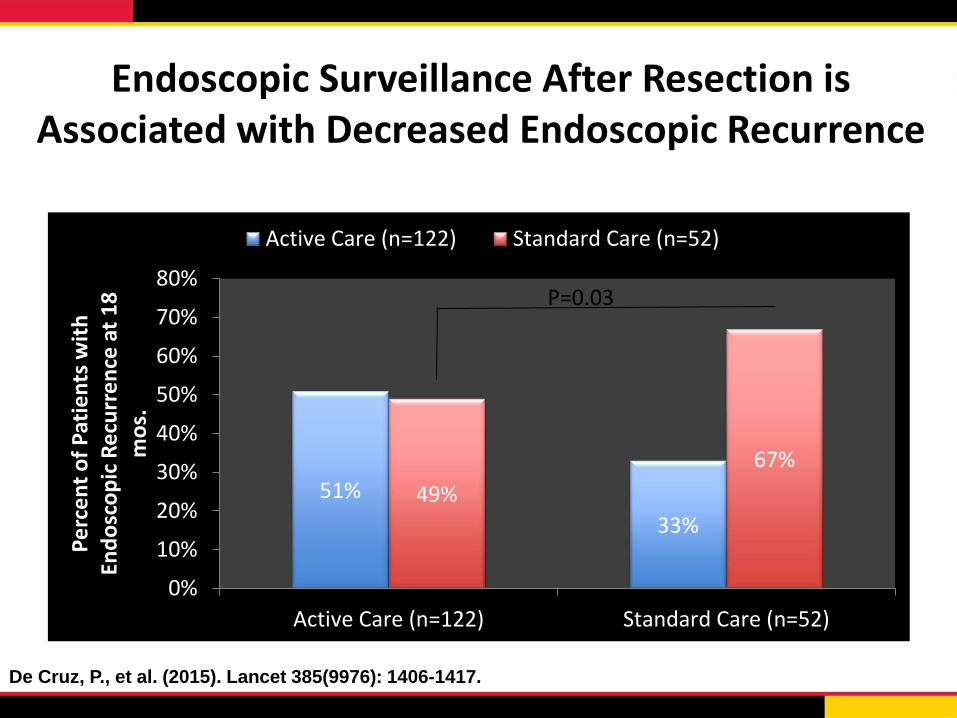
Endoscopic Surveillance After Resection is Associated with Decreased Endoscopic Recurrence
51%
33%
49%
67%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Active Care (n=122) Standard Care (n=52)
Pe
rce
nt
of
Pat
ien
ts w
ith
En
do
sco
pic
Re
curr
en
ce a
t 1
8
mo
s.
Active Care (n=122) Standard Care (n=52)p=0.03
De Cruz, P., et al. (2015). Lancet 385(9976): 1406-1417.
P=0.03
AGA Clinical Pathway for CD:
Stratifying Patients by Risk for Disabling Course
Low risk Limited anatomic involvement
Age at diagnosis >30 years
Superficial ulcerations at
endoscopy
No prior surgery
Non-stricturing, non- penetrating
disease
High risk
AGA = American Gastroenterological Association. Sandborn, W.J., et al. Gastroenterology. 2014;146(1):85-95.
Extensive anatomic involvement
Deep ulcers
Age at diagnosis <30 years
Perianal disease and/or severe rectal
disease
History of prior resection
Complicated disease behavior
AGA Clinical Pathway for CD:
Initial Treatment
Low-risk patient
Ileum and/or proximal colon, none to minimal symptoms Options • Budesonide 9 mg/d with or
without AZA • Tapering course of prednisone
with or without AZA
Diffuse or left colon, none to minimal symptoms Option • Tapering course of prednisone with
or without AZA
Moderate/high-risk patient
Options • Anti-TNF monotherapy over no therapy
or thiopurine monotherapy • Anti-TNF + thiopurine over thiopurine
monotherapy or anti-TNF monotherapy • Methotrexate for patients who do not tolerate
purine analog in combination with anti-TNF
Sandborn, W.J., et al. Gastroenterology. 2014;146(1):85-95
Conclusions
• Limited role for use of antibiotics and aminosalicylates in treatment of CD
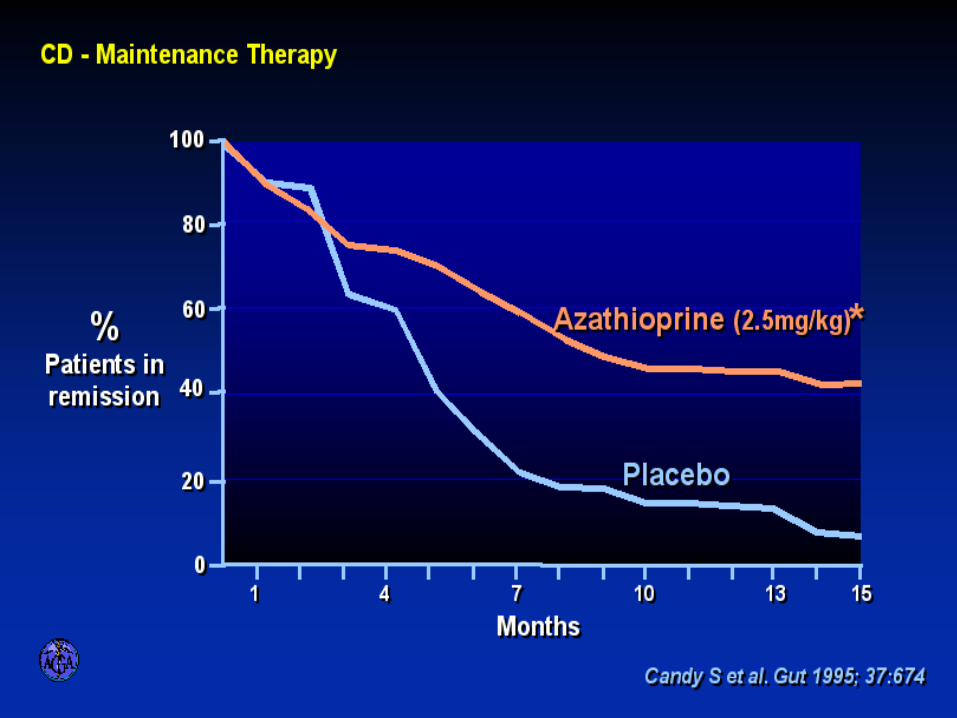
• Steroids are useful for induction of remission in CD
• Immune suppressants, particularly MTX, are effective for maintaining steroid-induced remission in CD – Little to no evidence that earlier use of these agents improves outcomes
• Anti-TNF agents are effective for treatment of luminal and perianal CD – Early combination therapy is most effective
– Outcomes can be improved with TDM
– Prevent post-operative recurrence
• Vedolizumab and ustekinumab also effective for treatment of CD – Not yet clear how to position these agents
• AGA Care Pathways available to guide selection of optimal patient for biologic treatment (not proven to improve clinical outcomes)