Correspondence: Dr. Ola Landgren, Multiple Myeloma Section, Metabolism Branch, National Cancer Institute, National Institutes of Health, 9000 Rockville
tent melphalan plus alternate-day prednisone, or melphalan
plus prednisone given together at 4 – 6-week intervals. MP
prolonged median survival from initiation of therapy by 33%
versus the groups receiving melphalan alone. Most patients
receiving alternate-day prednisone developed Cushingoid
symptoms that were eff ectively managed with dose reduc-
tion, and other toxicities in the MP groups were comparable
to the melphalan-only groups. Subsequent studies confi rmed
the survival benefi t for MP versus melphalan alone [17], and
extended dosing with MP became the standard strategy to
induce remission in patients with MM.
A shift from extended dosing to maintenance
Despite the survival benefi t achieved with extended MP, 25%
of patients failed to respond to this therapy and all inevitably
Figure 1. Osteolysis of vertebral body recovered from the necropolis of Th ebes-West. Th e lesion revealed almost no osseous reaction, suggestive of plasmacytoma (multiple myeloma). Reprinted from Nerlich et al . [1], with permission.
Figure 2. Timeline of therapeutic advances in MM. MM, multiple myeloma; RRMM, relapse and/or refractory multiple myeloma.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
Evolving myeloma treatment paradigms 453
relapsed [16]. Th ere was a distinct need for further therapy to
prolong treatment response. Unlike salvage therapies given
at relapse, maintenance therapies are administered during
periods of remission or stable disease to prolong survival
through continuous disease suppression. Early maintenance
eff orts with conventional chemotherapeutics yielded signifi -
cant toxicity and no survival benefi t. Th e Southwest Oncology
Group (SWOG) randomized 96 patients who had responded
to 12 months of MP induction therapy to continued treat-
ment with MP, combination prednisone and carmustine, or
no treatment, but found no diff erences between duration of
remission or overall survival [18].
Interferon Th e interferon (IFN) cytokines were among the fi rst drugs
to show promise for MM maintenance therapy. Th ese mol-
ecules are soluble glycoproteins produced by human cells
that act by binding to receptors on target cells to induce
gene transcription, resulting in varied downstream eff ects
[19,20]. Th ey have been shown in vitro to aff ect tumor cell
survival and immune response through the Janus kinase-
signal transducer and activator of transcription (JAK-STAT)
and nuclear factor- κ B (NF- κ B) signaling pathways [21,22],
and act as potent inhibitors of the cell cycle, leading to an
accumulation of cells in the G0 phase [23].
IFNs have been used to treat both hematologic and non-
hematologic malignancies [24], and have been studied as
therapy for MM since 1979, when Mellstedt and colleagues
demonstrated a partial response to single agent IFN- α in four
chemotherapy resistant MM patients [25]. Th e fi rst random-
ized, controlled trial using high-dose IFN for single agent
induction therapy showed it to be inferior to melphalan/
prednisone and revealed signifi cant central nervous system
and gastrointestinal toxicities [26]. Subsequent studies of
IFN as a co-induction agent have yielded confl icting results
[27], and these agents are not routinely included in current
induction strategies.
In 1985, Mandelli et al . initiated a randomized trial of IFN
as maintenance therapy in MM and found that in patients
who had responded to conventional chemotherapy, IFN
alone and found a PFS benefi t in the IFN plus prednisone
arm, 19 months vs. 9 months ( p � 0.008) [44]. No OS benefi t
was observed. In a subsequent study comparing single-agent
maintenance with dexamethasone versus IFN, Alexanian
et al . showed a similar duration of remission between the two
arms, but demonstrated that patients in the dexamethasone
maintenance arm were half as likely to respond to a steroid-
containing regimen at relapse versus patients in the IFN arm
[45]. Th e National Cancer Institute of Canada (NCIC) CTG
MY.7 study compared dexamethasone to observation and
found an increase in PFS of 2.8 years vs. 2.1 years ( p � 0.0002),
but again showed no OS benefi t.
Published in 2002, SWOG 9210 is the only random-
ized trial to demonstrate an OS benefi t with glucocorticoid
maintenance therapy for MM [46]. Th is trial randomized 125
patients who had responded to induction with vincristine,
doxorubicin, dexamethasone and prednisone (VAD-P) or
VAD-P plus quinine (VAD-P/Q) to receive either predni-
sone 50 mg or prednisone 10 mg on an alternate-day dosing
schedule until disease progression. At a median follow-up
of 53 months, both PFS and OS were found to be prolonged
in the 50 mg arm versus the 10 mg arm: 14 months vs.
5 months ( p � 0.003) and 37 months vs. 26 months ( p � 0.05),
respectively. Th e authors noted that while prednisone main-
tenance was generally well-tolerated, 23% of patients in the
study experienced grade 3 adverse events or higher, includ-
ing infection, edema, weight gain, change in mood, muscle
weakness and myalgia, and Cushingoid appearance. No
subsequent randomized study has been conducted to
confi rm the survival benefi t of single-agent glucocorticoid
maintenance reported in SWOG 9210.
A paradigm shift: the age of intensive therapy
With the above-mentioned maintenance therapies show-
ing only marginal improvements on conventional therapies,
clinicians sought treatment options that could produce
radical tumor debulking with the hope that this outcome
would lead to longer remissions or cure. High-dose therapy
(HDT) for MM was fi rst explored in 1981, when physicians
at Royal Marsden Hospital in the United Kingdom used high
doses (100 – 140 mg/m 2 ) of intravenous melphalan in eight
patients with MM, half of whom had received previous che-
motherapy [47]. Four of these patients, including one who
function tests [35]. Hematologic side eff ects of anemia, leu-
kopenia and thrombocytopenia appear to be dose-related
and are most common in patients receiving � 10 MU per
day [36], but treatment cessation rates of 20% due to IFN-
associated toxicity have been reported even at doses as low
as 3 MU, three times per week [37]. Th e severity of toxic side
eff ects is linked in part to patient age [24], and studies of older
patients with MM have reported toxicity-related cessation of
treatment in as many as 37% of patients receiving IFN [38].
Glucocorticoids Glucocorticoids were discovered to inhibit cells of lympho-
cytic origin in the 1940s [39], and have since become crucial
agents for the treatment of hematological malignancies,
including leukemias, lymphomas and MM [39 – 41]. Given
prednisone ’ s success in extending survival when used as part
of initial therapy, this class was among the fi rst to be explored
for maintenance therapy in MM, along with IFNs. As mainte-
nance agents, they represented an appealing alternative to
IFN therapy due to their more favorable toxicity profi le.
Th ese adrenocortical steroid hormones modulate
immune processes, metabolism, cell growth and prolifera-
tion, development and reproduction; they have been used
for therapeutic immunosuppression, to treat infl ammation
and to induce cytotoxicity [42]. Th e exact mechanism by
which these agents exert their anti-MM eff ect is unknown,
but in vitro studies have shown that the cytolytic eff ects of
glucocorticoids are mediated via the glucocorticoid receptor,
a ligand-dependent transcription factor that is ubiquitously
expressed in human cells [43]. Th e glucocorticoid receptor
resides in the cytoplasm as part of an oligomeric complex,
and upon ligand binding translocates to the nucleus where it
aff ects gene transcription through interaction with the basal
transcription machinery and other transcription factors
including activator protein 1 (AP-1) and NF- κ B [43].
Although glucocorticoids are an integral component of
induction regimens for MM, results from studies evaluat-
ing their use as maintenance agents have been generally
disappointing (Table II). Th eir long-term use is limited by
the development of adrenal suppression that may cause
secondary adrenal insuffi ciency; abrupt withdrawal in this
context leads to acute adrenal crisis. Th e earliest published
randomized trial of glucocorticoid maintenance therapy for
MM, SWOG 9028, compared IFN plus prednisone to IFN
Table II. Trials evaluating glucocorticoids as maintenance therapy for multiple myeloma.
Author, study Year n Comparison Impact on progression-free survival Impact on overall survival
Salmon et al ., SWOG 9028
1998 89 IFN � prednisone, IFN IFN � prednisone superior to IFN alone, 19 months vs. 9 months ( p � 0.008)
No statistically signifi cant diff erence in OS
Alexanian et al . 2000 84 Dexamesthasone, IFN Similar duration to fi rst remission between study arms; dexamethasone inferior to IFN in duration to melphalan-resistant relapse, 19 months vs. 32 months ( p � 0.01)
No statistically signifi cant diff erence in OS
Berenson et al ., SWOG 9210
2001 125 Prednisone 50 mg, prednisone 10 mg
Prednisone 50 mg superior to prednisone 10 mg, 14 months vs. 5 months ( p � 0.003)
Prednisone 50 mg superior to prednisone 10 mg, 37 months vs. 26 months, p � 0.05
Shustik et al ., NCIC CTG MY.7
2006 292 Dexamethasone, observation
Dexamethasone superior to observation, 2.8 years vs. 2.1 years ( p � 0.0002)
and Durie – Salmon stage, although patients with deletion of
chromosome 13 did not benefi t. Another important fi nding
of this study was the consolidation role of thalidomide to
improve depth of response: 16 of the 200 patients random-
ized to receive thalidomide – pamidronate maintenance who
had achieved a partial response (PR) or less with induction
therapy improved to CR or VGPR following randomization.
Subsequent trials of thalidomide maintenance following
HDT-ASCT confi rmed the consolidation role of thalidomide
in this setting [68 – 70]. A trend toward improved OS across tri-
als was also seen, and although this trend reached statistical
signifi cance in only three [61,70,71], a recent meta-analysis
of fi ve of the six studies confi rmed a signifi cant improve-
ment in both PFS (hazard ratio [HR] 0.64, 95% confi dence
interval [CI] 0.56 – 0.73, p � 0.001) and in OS (HR 0.70, 95% CI
0.55 – 0.89, p � 0.004) [72].
Th e role of thalidomide maintenance for patients con-
sidered ineligible for HDT-ASCT is less clear. Five random-
ized trials have evaluated thalidomide maintenance after
induction with standard therapies [73 – 76]. Four of these
assigned patients to MP induction followed by observation
or MP plus thalidomide induction followed by thalidomide
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
456 B. M. Cherry et al.
Total Th erapy 2 study at 30 months [71], increasing to nearly
80% at 80 months [80].
To further evaluate these toxicities, Stewart and col-
leagues studied maintenance therapy with thalidomide
(either 200 mg or 400 mg per day) plus prednisone (50 mg
on alternate days) following HDT-ASCT, with a primary
outcome measure of discontinuation or dose reduction due
to toxicity within 6 months of beginning maintenance [81].
Th e investigators defi ned “ a tolerable maintenance therapy ”
as no dose reduction or discontinuation due to toxicity in at
least 65% of patients; the 200 mg arm met and the 400 mg
arm failed to meet this defi nition, with overall rates of dose
reduction or discontinuation of 31% and 64%, respectively. In
2010, this group included specifi c quality of life endpoints in
their evaluation of thalidomide and prednisone (TP) main-
tenance following HDT-ASCT [82]. Th ey reported a non-
signifi cant increase in survival for TP maintenance compared
to observation alone (not reached [NR] vs. 5 years, p � 0.18).
Although the TP group experienced superior PFS versus
observation (28 months vs. 17 months, p � 0.0001), there was
also a signifi cantly higher incidence of serious (grade 3 and 4)
toxicities (grade 3: 92% vs. 49%; grade 4: 16% vs. 7%), as well
maintenance (MPT-T), and showed that MPT-T was associ-
ated with signifi cant improvement in overall response rates.
Th e Dutch – Belgian Hemato-Oncology Cooperative Group
(HOVON) study reported a statistically signifi cant survival
benefi t for MPT-T versus MP, 40 months vs. 31 months
( p � 0.05) [76]. Although encouraging, these results are at
odds with similar studies, which found no survival benefi t to
MPT-T versus MP [73,75,77]. Furthermore, the inclusion of
thalidomide in induction makes it impossible to evaluate the
role of thalidomide maintenance in the HOVON observed
survival increase.
Th e benefi t of thalidomide also comes at the cost of
signifi cant toxicities, which manifest in both a dose- and
time-dependent manner [78]. Important side eff ects of
thalidomide therapy include somnolence, constipation,
peripheral neuropathy and venous thromboembolism [79].
Th e incidence of these toxicities varies between studies,
but leads to treatment discontinuation in an unaccept-
ably large number of patients. A 30% discontinuation rate
was observed in the Australian transplant study [70], 58%
discontinuation or dose reduction in the HOVON-50 trans-
plant study [69] and 43% discontinuation in the Arkansas
Table IV. Trials evaluating thalidomide as maintenance therapy following conventional chemotherapy induction for MM.
Author, study Year n Induction and maintenance
regimensImpact on progression-free
survival Impact on overall survival
Beksac, Turkish myeloma study group
2011 115 MPT (100/day), MP MPT vs. MP, 21 vs. 14 months ( p � 0.342)
MPT vs. MP, 26 vs. 28 months ( p � 0.655)
Palumbo, GIMEMA 2006 331 MPT (100/day), MP MPT superior to MP, 21.8 vs. 14.5 months ( p � 0.001)
No diff erence in MPT vs. MP, 45.0 vs. 47.6 months ( p � 0.79)
Waage, Nordic myeloma study group
2010 357 MPT (200/400/200), MP No diff erence in MPT vs. MP, 15 vs. 14 months ( p � 0.84)
No diff erence in MPT vs. MP, 29 vs. 32 months ( p � 0.16)
Wijermans, HOVON 49 2008 333 MPT (200/day), MP MPT superior to MP, 13 vs. 9 months ( p � 0 .001)
MPT superior to MP, 40 vs. 31 months ( p � 0.05)
Ludwig, CEMSG 2010 128 TD or MP induction, then either: IFN 3 MU TIW � thal 200 mg/day, IFN 3 MU TIW
Superiority of IFN � thal vs. IFN alone, 27.7 vs. 13.2 months ( p � 0.0068)
No diff erence in IFN � thal vs. IFN alone, 52.6 vs. 51.4 months ( p � 0.81)
MM, multiple myeloma; IFN, interferon; PFS, progression-free survival; OS, overall survival; MPT, melphalan, prednisone and thalidomide; MP, melphalan and prednisone; TD, thalidomide and dexamethasone; thal, thalidomide.
Table III. Trials evaluating thalidomide as maintenance therapy following HDT-ASCT for MM.
Author, study Year n Maintenance regimen Impact on progression-free survival Impact on overall survival
Attal, IFM-99 2006 597 Pamidronate � thalidomide, pamidronate, no maintenance
Pamidronate � thalidomide superior to pamidronate alone and no maintenance for 3-year EFS, 52% vs. 37% and 36%, respectively ( p � 0.009)
Pamidronate � thalidomide superior to pamidronate alone and no maintenance for 4-year OS, 87% vs. 74% and 77%, respectively ( p � 0.04)
Morgan, MRC IX
2011 818 Th alidomide, observation alone Th alidomide superior to observation for PFS among all patients, 23 vs. 15 months ( p � 0.001); no PFS diff erence for patients with adverse cytogenetics
Th alidomide associated with a worse outcome for patients with adverse cytogenetic profi les ( p � 0.009)
Spencer, ALLG MM6
2009 243 Th alidomide � prednisone, prednisone
Superiority of thalidomide vs. prednisone for 3-year PFS, 42% vs. 23% ( p � 0.001)
Superiority of thalidomide vs. prednisone for 3-year OS, 86% vs. 75% ( p � 0.004)
Barlogie, Total Th erapy 2
2006 668 All received induction, tandem ASCT, chemo consolidation and IFN maintenance; comparison of thalidomide in all phases of treatment vs. no thalidomide
Superiority of thalidomide vs. no-thalidomide for 5-year PFS, 57% vs. 44% ( p � 0.0005)
Superiority of thalidomide vs. no-thalidomide for 5-year OS, 68% vs. 65% ( p � 0.04)
Lokhorst, HOVON 50
2010 536 IFN (after VAD � ASCT), thalidomide (after TAD � ASCT)
Superiority of thalidomide vs. IFN, 34 vs. 25 months ( p � 0.001)
No diff erence in thalidomide vs. IFN, 73 vs. 60 months ( p � 0.77)
[95,96], but the relationship between these observations and
a clinical benefi t is still under investigation.
Recently, three large phase III trials comparing lenali-
domide maintenance to placebo found PFS benefi ts for
both ASCT-eligible [97,98] and -ineligible [99] patients
(Table V). Palumbo and colleagues studied 459 newly diag-
nosed patients with MM aged 65 years or older and not eli-
gible for ASCT [99]. Th e patients were randomized into three
groups that received MP and lenalidomide induction followed
by lenalidomide maintenance (MPR-R), MPR induction
as more venous thromboembolic events in the absence of
prophylaxis (7% vs. 0%). Patients receiving TP showed clear
trends toward worse quality of life (QoL) on various mea-
sures including physical ( p � 0.07), role ( p � 0.08), cognitive
( p � 0.01) and global ( p � 0.06) domains. Patients receiving
TP also experienced signifi cantly worse symptoms includ-
ing dyspnea ( p � 0.0007), constipation ( p � 0.0001), thirst
( p � 0.003), leg swelling ( p � 0.03), numbness ( p � 0.02), dry
mouth ( p � 0.0001) and balance problems ( p � 0.0001). All
QoL measures were worse in the TP group with the exception
of appetite and sleep. Th is decreased quality of life without a
clear survival benefi t should give clinicians cause to consider
the true cost of PFS.
Th e signifi cant side eff ects of prolonged thalidomide
administration may be attenuated by dose reduction and
time-limited therapeutic regimens [70,83], but the largest trial
of thalidomide maintenance therapy has not shown a survival
benefi t with low-dose (100 mg/day) therapy after a median
follow-up of 38 months from randomization [84]. Moreover,
there are data to suggest that thalidomide maintenance is
ineff ective and potentially harmful in patients with higher-
risk disease associated with cytogenetic abnormalities (CA).
Th e British Medical Reesearch Council (MRC) IX study eval-
uated 818 patients randomized to thalidomide maintenance
or observation after an intensive or non-intensive induction
regimen [84]. Th is study found no signifi cant PFS benefi t in
patients with CA detected by interphase fl uorescence in situ
hybridization (FISH); in fact these patients had worse OS
relative to standard-risk patients when receiving thalido-
mide maintenance therapy ( p � 0.009). Similar results were
reported by Stewart et al . in a study including 332 patients
[82]. In a study of elderly patients randomized to thalidomide – -
interferon maintenance or interferon maintenance alone fol-
lowing MP or thalidomide – dexamethasone (TD) induction,
patients with CA by FISH had a median overall survival of
39.6 months vs. 72.3 months for patients with standard-risk
disease (HR 1.94, CI 0.91 – 4.13, p � 0.082) [85]. In patients
with CA detected by gene expression profi ling, however, the
Arkansas study showed thalidomide maintenance to be an
independent favorable prognostic variable versus control
[71], and long-term follow-up showed increased survival in
the thalidomide arm among all patients [86]. Finally, survival
after relapse tends to be shorter in patients receiving tha-
lidomide maintenance when those patients have previously
received thalidomide induction. Palumbo et al . found that
Table V. Trials evaluating lenalidomide as maintenance therapy for multiple myeloma.
Author, study Year n Comparison Impact on TTP/PFS Impact on overall survival
Attal et al ., IFM 2005-02
2012 614 Lenalidomide, placebo
Lenalidomide showed longer PFS vs. placebo, 41 months vs. 23 months, HR 0.5 ( p � 0.001)
No statistically signifi cant diff erence in OS
McCarthy et al ., CALGB 100104
2012 460 Lenalidomide, placebo
Lenalidomide showed TTP benefi t vs. placebo, 46 months vs. 27 months ( p � 0.001)
Lenalidomide showed OS benefi t vs. placebo, at 34 months of follow-up, 85% vs. 77% ( p � 0.03)
Palumbo et al ., MM-015
2012 459 MPR-R, MPR-placebo, MP-placebo
MPR-R superior to MPR-p and MP-p for PFS, 31 months vs. 14 months vs. 13 months, HR 0.398 ( p � 0.0000001 for MPR-R vs. MP-p)
No statistically signifi cant diff erence in OS
TTP, time to progression; PFS, progression-free survival; OS, overall survival; MP, melphalan and prednisone; MPR-R, MP and lenalidomide induction followed by lenalidomide maintenance; HR, hazard ratio; MP-p, MP induction with placebo maintenance; MPR-p, MPR induction with placebo maintenance.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
458 B. M. Cherry et al.
activity. In 1999, Adams and colleagues reported that bort-
ezomib (then known as PS-341) was an eff ective inhibitor
of the proteasome, a novel biochemical target [102]. Pro-
teasomes are enzyme complexes responsible for the degra-
dation and clearance of misfolded, unfolded and cytotoxic
intracellular proteins, including mediators of cell-cycle pro-
gression and apoptosis [103]. Bortezomib blocks the tumor
ing in decreased binding of MM cells to bone marrow stem
cells (BMSCs) [104], and reversibly inhibits the chymotryptic
activity of the proteasome 20S subunit, leading to MM cell
apoptosis [105]. Th is activity is observed even in cell lines
resistant to conventional anti-MM therapies [106].
Bortezomib received FDA approval in 2003 [107], after
showing signifi cant activity in relapsed and refractory MM
[108]. Studies of bortezomib maintenance have shown it
to improve response rate and prolong survival (Table VI).
Mateos and colleagues compared MP to bortezomib in com-
bination with MP (VMP) for primary induction in elderly
patients with myeloma [109]. VMP demonstrated an 89%
induction response, including 32% immunofi xation-negative
CRs, in contrast to a historical response to MP induction of
42% [110]. At 16 months of follow-up, patients in the VMP
arm experienced superior PFS versus MP alone (91% vs.
66%, p � 0.002), as well as increased survival (90% vs. 62%,
p � 0.001). Subsequent studies confi rmed this survival ben-
efi t [111], and showed increased activity of bortezomib com-
pared to dexamethasone when used as a single agent [112].
Th e Spanish PETHEMA (Programa de Estudio y
Tratamiento de las Hemopat í as Malignas) trial randomized
260 patients to bortezomib maintenance in combination
with prednisone (VP) or thalidomide (VT) after randomiza-
tion to induction with VTP or VMP [113]. Th e trial found
similar proportions of patients achieving CR after induction
with VTP or VMP (28% vs. 20%, p � 0.2), and showed that
maintenance therapy with bortezomib increased the overall
CR rate to 42%. A subset of patients developed signifi cant
peripheral neuropathy following induction (7% VTP; 9%
VMP) and maintenance (2% VP; 7% VT).
with placebo maintenance, or MP induction with placebo
maintenance. Patients who received MPR-R experienced a
longer median PFS than patients in the MPR and MP arms,
and this benefi t persisted when the arms were compared
across patient characteristics including age, International
Staging System (ISS) disease stage, renal function, level of β 2 -
microglobulin and Karnofsky performance score. Th is study
is still in follow-up. At the American Society of Hematology
meeting in December 2011, the group reported a trend toward
a survival benefi t in the lenalidomide maintenance arm for
patients aged 65 – 75 years, with a 4-year OS of 69% vs. 58% for
the non-lenalidomide arm (HR 0.71, p � 0.133). In the most
recent analysis including all patients (February 2012), no OS
benefi t was observed for lenalidomide maintenance [99].
Attal et al . enrolled 614 patients with non-progressive MM
within 6 months of fi rst-line HDT-ASCT [98]. All patients were
given lenalidomide consolidation therapy following ASCT,
and then randomized to lenalidomide or placebo mainte-
nance. Th is study found that patients randomized to lenali-
domide maintenance experienced signifi cantly longer PFS of
41 months vs. 21 months with placebo (HR 0.5, p � 0.001), but
did not detect any statistically signifi cant survival benefi t after
45 months from randomization. McCarthy et al . randomized
patients with stable disease or better following HDT-ASCT
to maintenance therapy with lenalidomide or placebo [97].
Patients receiving lenalidomide experienced a signifi cant
decrease in the risk of disease progression with an extended
time to progression (TTP) when compared to placebo, 46
months vs. 27 months ( p � 0.001). Th e authors reported that
at 34 months of follow-up, 85% of patients in the lenalidomide
arm were alive versus 77% in the placebo arm ( p � 0.03). Th is
is the fi rst randomized, controlled trial for lenalidomide
maintenance to show a signifi cant survival benefi t.
Notably, all three of these studies reported more frequent
hematologic and non-hematologic malignancies in the groups
receiving lenalidomide at a rate of 7 – 8% [97,99]. Th e excess
of myeloid tumors and myelodysplastic diseases seems most
pronounced. Given that the Cancer and Leukemia Group B
(CALGB) study has reported a survival benefi t with lenalido-
mide maintenance, the signifi cance of these fi ndings is not
entirely clear. Th e FDA has encouraged physicians to weigh
the benefi ts of lenalidomide therapy against the risk of second
primary malignancies, and to continue to monitor patients for
this risk [73]. At present, it seems that the benefi ts do outweigh
the risks: the increased risk of death without treatment is sub-
stantially higher than the risk of death from a second malig-
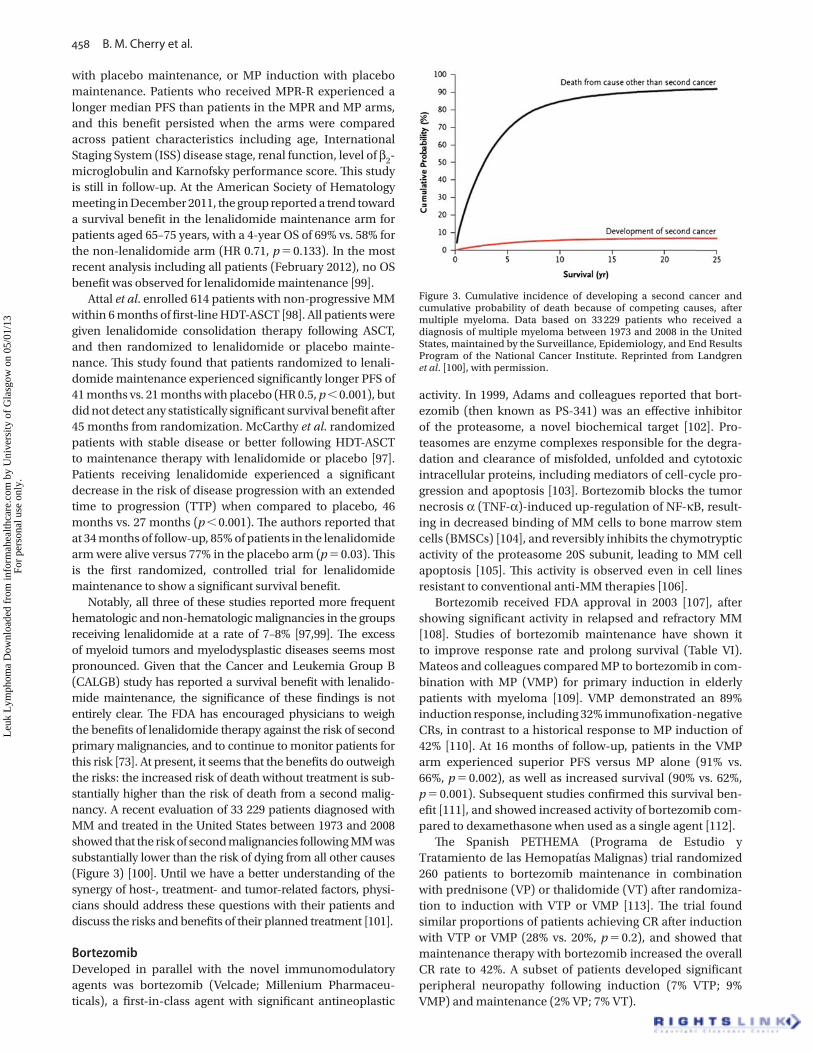
nancy. A recent evaluation of 33 229 patients diagnosed with
MM and treated in the United States between 1973 and 2008
showed that the risk of second malignancies following MM was
substantially lower than the risk of dying from all other causes
(Figure 3) [100]. Until we have a better understanding of the
synergy of host-, treatment- and tumor-related factors, physi-
cians should address these questions with their patients and
discuss the risks and benefi ts of their planned treatment [101].
Bortezomib Developed in parallel with the novel immunomodulatory
agents was bortezomib (Velcade; Millenium Pharmaceu-
ticals), a fi rst-in-class agent with signifi cant antineoplastic
Figure 3. Cumulative incidence of developing a second cancer and cumulative probability of death because of competing causes, after multiple myeloma. Data based on 33 229 patients who received a diagnosis of multiple myeloma between 1973 and 2008 in the United States, maintained by the Surveillance, Epidemiology, and End Results Program of the National Cancer Institute. Reprinted from Landgren et al . [100], with permission.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
Evolving myeloma treatment paradigms 459
Th ough a cure remains elusive, our success in achieving
long-term disease suppression through continuous therapy
is transforming MM into a chronic disease. As we seek to
develop optimal strategies for the management of this dis-
ease, we must consider multiple complicated questions.
One prominent uncertainty is what role aggressive treat-
ment should play in the initial therapy of MM. While upfront
HDT-ASCT has led to signifi cant improvements in disease
response and PFS, it has shown no impact on OS when com-
pared to a stepwise treatment approach [116]. Th e results of
recent trials indicate that even by combining most available
chemotherapies in combination with novel drugs, only a
small number of patients with MM experience remissions
consistent with a cure [117].
An appealing alternative to using most drugs in most
patients is to develop agents that target the specifi c biology of
MM. At this time, several rationally designed small molecules
and antibodies against defi ned targets are being evaluated in
clinical trials for MM. Given current therapies, however, the
question remains: would patients who respond well to HDT-
ASCT as upfront therapy achieve similar survival if given
substantially less intensive and less toxic initial therapy with
newer agents alone? No randomized scientifi c data are yet
available to answer this critical question; however, newer
agents are demonstrating considerable effi cacy (responses
and PFS) when used upfront in the absence of HDT-ASCT
[74,111,118,119]. Proponents of both intensive and conserva-
tive approaches agree that there is a pressing need for better
risk-adapted treatment algorithms [120], which could guide
the choice of initial therapy based on individual patient char-
acteristics and minimize avoidable toxicities.
Th e question of toxicity in MM therapy is not a trivial one,
as both historical and recent experiences have shown. As
MM evolves to a chronic disease model, we should be par-
ticularly attentive to the recognized side eff ects of extended
therapy (Table VII) and to those that may emerge upon fur-
ther investigation. Relatively few studies of MM therapy have
included specifi c quality of life endpoints, and we believe
that future studies need to include such measures in parallel
with measures of clinical eff ect and survival outcomes. Cost
of therapy, too, will be an important issue in the future as we
consider indefi nite administration of maintenance agents.
For example, the estimated cost for 1 year of lenalidomide
therapy is approximately $ 160 000, and this number does not
include the cost of laboratory monitoring, physician visits or
management of treatment side eff ects [121].
Palumbo et al . randomized 511 patients to receive either
VMPT induction followed by continuous VT maintenance
(VMPT-VT) or VMP induction with no maintenance [114].
Th is study reported greater PFS at 3 years for VMPT-VT versus
VMP (56% vs. 41%, p � 0.008), even though a greater propor-
tion of patients receiving VMPT-VT had discontinued therapy
(72% vs. 60%, p � 0.007). Th e CR rate was signifi cantly higher
in the VMPT-VT arm (38% vs. 24%, p � 0.001), but survival at
3 years did not diff er signifi cantly between the study groups
(89% vs. 87%, p � 0.77).
Th e joint HOVON-65/German Speaking Myeloma Multi-
center Group (GMMG)-HD4 trial compared bortezomib to
conventional chemotherapy for induction in newly diagnosed
patients with MM [115]. Patients then underwent single or
double ASCT and were randomized to maintenance with
bortezomib or thalidomide. After a median follow-up of 40
months, the bortezomib arm showed a superior rate of VGPR
or better (75% vs. 61%), PFS (HR 0.81, p � 0.047 and p � 0.056
when adjusted for ISS stage) and OS (HR 0.74, p � 0.048).
tenance versus thalidomide due to toxicity (9% vs. 31%),
although rates of progression were similar (29% vs. 31%).
Summary and future directions
Strategies to achieve and maintain remission in MM have
continually evolved since the disease was described in the
mid-19th century. Th e last 50 years have witnessed substan-
tial advances in MM therapy as well as distinct changes in the
prevailing treatment paradigms for this currently incurable
disease. Early strategies sought to prolong survival through
control of post-response residual disease with extended
dosing of standard chemotherapeutics and with steroid
and interferon maintenance therapies. Th ese approaches
showed little to no benefi t in the face of undeniable side
eff ects and were not widely adopted. Th e introduction of
HDT-ASCT represented an aggressive shift in the intensity of
treatment for MM toward a curative approach, but this strat-
egy failed to induce durable remissions in the overwhelming
majority of patients. More recently introduced drugs such as
thalidomide, lenalidomide and bortezomib have revived the
prospect of eff ective long-term maintenance when given in
an extended dosing fashion alongside conventional chemo-
therapeutics and HDT-ASCT. Th is union of the “ cure ” and
“ control ” approaches represents our current best off ering for
patients with MM.
Table VI. Trials evaluating bortezomib as maintenance therapy for multiple myeloma.
Author, study Year n Maintenance regimen Findings
Mateos, PETHEMA
2010 260 VP (after VMP or VTP), VT (after VMP or VTP)
Consolidation role of bortezomib seen in both VP and VT maintenance, 39% and 44% achieved CR, respectively
Palumbo, GIMEMA
2010 511 VMPT induction, VT, observation alone
Superiority of VMPT-VT vs. VMPT-observation for CR rate, 38% vs. 24% ( p � 0.001), superiority of VMPT-VT vs. VMPT-observation for 3-year PFS, 56% vs. 41% ( p � 0.008), no diff erence in 3-year OS for VMPT-VT vs. VMPT-observation, 89% vs. 87% ( p � 0.77)
Sonneveld, HOVON-65/GMMG-HD4
2010 827 Induction � single or double ASCT, thalidomide 50 mg/day, bortezomib 1.3 mg/m 2 2 � /week
Superiority of bortezomib vs. thalidomide for 3-year PFS, 46% vs. 42% ( p � 0.047), superiority of bortezomib vs. thalidomide for 3-year OS, HR 0.74 (p � 0.048)
VP, bortezomib and prednisone; VT, bortezomib and thalidomide; VMP, bortezomib, melphalan and prednisone; VTP, bortezomib, thalidomide and prednisone; ASCT, autologous stem cell transplant; CR, complete remission; PFS, progression-free survival; OS, overall survival; HR, hazard ratio.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
460 B. M. Cherry et al.
A further important need is for better measures to monitor
treatment response and disease status. Rather than treating
all patients with a fi xed number of chemotherapy cycles and
relying on endpoints such as CR defi ned by elimination of
the M-spike, we anticipate that emerging tests will combine
both high sensitivity and specifi city (through molecular and
functional imaging-based methods) to rule out evidence of
minimal residual disease (MRD). If used in combination with
highly eff ective and less toxic drugs, these MRD tests may
help to determine the need for therapy and type of therapy
on an individual basis to maximize treatment effi cacy and
minimize toxicity.
In closing, the treatment paradigm for MM has shifted
back toward maintenance but continues to evolve. An
emerging and important area of exploration is the develop-
ment of treatment strategies for patients with lower disease
burden ( “ early myeloma ” ). Currently, a few clinical trials
are evaluating treatment for high-risk smoldering MM and
are showing signs of success in delaying progression to MM.
Defi nitive data are not yet available, and no drugs have been
approved for the treatment of smoldering MM. At present, all
treatment studies for high-risk smoldering MM have been
built on the platform of “ chronic disease control, ” e.g. lenali-
domide and dexamethasone for a fi xed number of cycles, fol-
lowed by a lower dose of lenalidomide maintenance therapy
[122]. With increased access to eff ective but less toxic drugs
and full integration of careful monitoring (including molec-
ular and imaging-based MRD tests), it is likely that we will
see the development of more targeted and less toxic treat-
ment studies for high-risk smoldering MM. Such studies will
revisit similar goals to those established at the conception of
HDT-ASCT, testing the hypothesis that it is possible to cure
or achieve long-term remissions in MM by approaching the
disease more eff ectively in an earlier time window. Th ese
and other important questions face MM investigators as we
look to the future.
Potential confl ict of interest: Disclosure forms provided by the authors are available with the full text of this article at www.informahealthcare.com/lal.
References
Nerlich AG , Rohrbach H , Bachmeier B , et al . Malignant tumors in [1] two ancient populations: an approach to historical tumor epidemiology . Oncol Rep 2006 ; 16 : 197 – 202 .
Raab MS , Podar K , Breitkreutz I , et al . Multiple myeloma . Lancet [2] 2009 ; 374 : 324 – 339 .
Perez-Persona E , Vidriales MB , Mateo G , et al . New criteria [3] to identify risk of progression in monoclonal gammopathy of uncertain signifi cance and smoldering multiple myeloma based on multiparameter fl ow cytometry analysis of bone marrow plasma cells . Blood 2007 ; 110 : 2586 – 2592 .
Landgren O , Kyle RA , Pfeiff er RM , et al . Monoclonal gammopathy [4] of undetermined signifi cance (MGUS) consistently precedes multiple myeloma: a prospective study . Blood 2009 ; 113 : 5412 – 5417 .
Kyle RA , Durie BG , Rajkumar SV , et al . Monoclonal gammopathy of [5] undetermined signifi cance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWG consensus perspectives risk factors for progression and guidelines for monitoring and management . Leukemia 2010 ; 24 : 1121 – 1127 .
Kyle RA , Steensma DP . History of multiple myeloma . Recent Results [6] Cancer Res 2011 ; 183 : 3 – 23 . T
ab
le V
II.
Ma
jor
toxi
citi
es
of
ma
inte
na
nce
th
era
pie
s fo
r m
ult
iple
mye
lom
a.
Ma
inte
na
nce
d
rug
Re
pre
sen
tati
ve
do
se a
nd
tr
ea
tme
nt
du
rati
on
Th
era
pe
uti
c b
en
efi
tC
om
mo
n a
dv
ers
e e
ff e
cts
G3
/G4
he
ma
tolo
gic
AE
s,
cess
ati
on
ra
tes
du
e t
o A
Es
(da
ta f
or
sin
gle
-ag
en
t T
x)C
om
me
nts
IFN
3 M
U/m
2 ,
3 t
ime
s p
er
we
ek
Incr
ea
ses
PF
S,
ma
y in
cre
ase
OS
(i)
Ma
lais
e,
fev
er,
he
ad
ach
e,
mya
lgia
, co
gn
itiv
e a
nd
mo
od
ch
an
ge
s,
card
iac
arr
hyt
hm
ias
22
% G
3 �
G4
(S
we
dis
h – I
tali
an
),
15
– 37
% c
ess
ati
on
Sid
e e
ff e
cts
ap
pe
ar
to b
e d
ose
-re
late
d,
sev
eri
ty
of
toxi
city
in
cre
ase
s w
ith
pa
tie
nt
ag
e,
(i)
OS
b
en
efi
t se
en
in
tw
o m
eta
-an
aly
ses
on
ly
Ste
roid
sP
red
nis
on
e 5
0 m
g e
ve
ry o
the
r d
ay,
de
xam
eth
aso
ne
40
mg
, 4
da
ys e
ve
ry 2
8 d
ays
Imp
rov
es
resp
on
se q
ua
lity
, in
cre
ase
s P
FS
, m
ay
incr
ea
se O
S (
ii)
Irri
tab
ilit
y, i
nso
mn
ia,
Cu
shin
go
id
cha
ng
es,
in
fect
ion
, m
usc
le
we
ak
ne
ss,
mya
lgia
� G
3 2
1 – 2
5%
(S
WO
G 9
21
0),
�
5%
ce
ssa
tio
nA
dre
na
l su
pp
ress
ion
wit
h e
xte
nd
ed
use
, (i
i) O
S
be
ne
fi t
see
n i
n a
sin
gle
RC
T o
nly
Th
ali
do
mid
e1
00
– 20
0 m
g/d
ay,
co
nti
nu
ed
up
to
1 y
ea
rIm
pro
ve
s re
spo
nse
qu
ali
ty,
incr
ea
ses
PF
S,
incr
ea
ses
OS
Pe
rip
he
ral
ne
uro
pa
thy,
so
mn
ole
nce
, co
nst
ipa
tio
n,
ve
no
us
thro
mb
oe
mb
oli
sm
G3
: 9
2%
, G
4:
16
% (
wit
h
pre
dn
iso
ne
, S
tew
art
),
up
to
80
% c
ess
ati
on
Sid
e e
ff e
cts
incr
ea
se w
ith
do
se a
nd
le
ng
th o
f tr
ea
tme
nt,
co
ntr
ain
dic
ate
d i
n p
ati
en
ts w
ith
F
ISH
-de
fi n
ed
hig
h-r
isk
ge
ne
tics
Le
na
lid
om
ide
5 – 1
5 m
g/d
ay,
da
ys 1
– 21
of
28
-da
y c
ycle
, co
nti
nu
ed
to
p
rog
ress
ion
Imp
rov
es
resp
on
se q
ua
lity
, in
cre
ase
s P
FS
, m
ay
incr
ea
se
OS
(ii
i)
Mye
losu
pp
ress
ion
, so
mn
ole
nce
, co
nst
ipa
tio
n,
pe
rip
he
ral
ne
uro
pa
thy
G3
: 5
8 – 7
4%
; G
4:
16
– 23
%,
8 – 2
7%
ce
ssa
tio
nIn
cre
ase
d r
isk
fo
r se
con
d p
rim
ary
m
ali
gn
an
cie
s, (
iii)
OS
be
ne
fi t
pre
sen
tly
sho
wn
in
1/3
stu
die
sB
ort
ezo
mib
1.3
mg
, tw
ice
pe
r w
ee
k,
con
tin
ue
d u
p t
o 2
ye
ars
Imp
rov
es
resp
on
se q
ua
lity
, in
cre
ase
s P
FS
, in
cre
ase
s O
SP
eri
ph
era
l n
eu
rop
ath
y9
% c
ess
ati
on
(H
OV
ON
-65
)S
ub
cuta
ne
ou
s a
dm
inis
tra
tio
n d
ecr
ea
ses
pe
rip
he
ral
ne
uro
pa
thy
AE
, a
dv
ers
e e
ve
nt;
Tx
, th
era
py;
IF
N,
inte
rfe
ron
; P
FS
, p
rog
ress
ion
-fre
e s
urv
iva
l; O
S,
ov
era
ll s
urv
iva
l; R
CT
, ra
nd
om
ize
d c
on
tro
lle
d t
ria
l; F
ISH
, fl
uo
resc
en
ce i
n s
itu
hyb
rid
iza
tio
n.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
Evolving myeloma treatment paradigms 461
utilizing an escalating induction phase . Cancer Treat Rep 1986 ; 70 : 1251 – 1254 .
Blade J , San Miguel JF , Escudero ML , et al . Maintenance [37] treatment with interferon alpha-2b in multiple myeloma: a prospective randomized study from PETHEMA (Program for the Study and Treatment of Hematological Malignancies, Spanish Society of Hematology) . Leukemia 1998 ; 12 : 1144 – 1148 .
Schaar CG , Kluin-Nelemans HC , Te Marvelde C , et al . Interferon-[38] alpha as maintenance therapy in patients with multiple myeloma . Ann Oncol 2005 ; 16 : 634 – 639 .
Moalli PA , Rosen ST . Glucocorticoid receptors and resistance [39] to glucocorticoids in hematologic malignancies . Leuk Lymphoma 1994 ; 15 : 363 – 374 .
Gaynon PS , Carrel AL . Glucocorticosteroid therapy in childhood [40] acute lymphoblastic leukemia . Adv Exp Med Biol 1999 ; 457 : 593 – 605 .
Alexanian R , Dimopoulos M . Th e treatment of multiple myeloma . [41] N Engl J Med 1994 ; 330 : 484 – 489 .
Greenstein S , Ghias K , Krett NL , et al . Mechanisms of [42] glucocorticoid-mediated apoptosis in hematological malignancies . Clin Cancer Res 2002 ; 8 : 1681 – 1694 .
Frankfurt O , Rosen ST . Mechanisms of glucocorticoid-induced [43] apoptosis in hematologic malignancies: updates . Curr Opin Oncol 2004 ; 16 : 553 – 563 .
Salmon SE , Crowley JJ , Balcerzak SP , et al . Interferon versus [44] interferon plus prednisone remission maintenance therapy for multiple myeloma: a Southwest Oncology Group Study . J Clin Oncol 1998 ; 16 : 890 – 896 .
Alexanian R , Weber D , Dimopoulos M , et al . Randomized trial [45] of alpha-interferon or dexamethasone as maintenance treatment for multiple myeloma . Am J Hematol 2000 ; 65 : 204 – 209 .
Berenson JR , Crowley JJ , Grogan TM , et al . Maintenance therapy [46] with alternate-day prednisone improves survival in multiple myeloma patients . Blood 2002 ; 99 : 3163 – 3168 .
Selby P , Zulian G , Forgeson G , et al . Th e development of high [48] dose melphalan and of autologous bone marrow transplantation in the treatment of multiple myeloma: Royal Marsden and St Bartholomew ’ s Hospital studies . Hematol Oncol 1988 ; 6 : 173 – 179 .
Westbury G , Humble JG , Newton KA , et al . Disseminated [49] malignant melanoma: response to treatment by massive dosage of a cytotoxic agent combined with autogenous marrow replacement . Lancet 1959 ; 1 : 968 – 969 .
Ariel IM , Pack GT . Treatment of disseminated melanoma with [50] phenylalanine mustard (melphelan) and autogenous bone marrow transplants . Surgery 1962 ; 51 : 583 – 591 .
Barlogie B , Alexanian R , Dicke KA , et al . High-dose [51] chemoradiotherapy and autologous bone marrow transplantation for resistant multiple myeloma . Blood 1987 ; 70 : 869 – 872 .
Barlogie B , Hall R , Zander A , et al . High-dose melphalan with [52] autologous bone marrow transplantation for multiple myeloma . Blood 1986 ; 67 : 1298 – 1301 .
Barlogie B , Jagannath S , Naucke S , et al . Long-term follow-up [53] after high-dose therapy for high-risk multiple myeloma . Bone Marrow Transplant 1998 ; 21 : 1101 – 1107 .
Attal M , Harousseau JL , Stoppa AM , et al . A prospective, [54] randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Francais du Myelome . N Engl J Med 1996 ; 335 : 91 – 97 .
Child JA , Morgan GJ , Davies FE , et al . High-dose chemotherapy [55] with hematopoietic stem-cell rescue for multiple myeloma . N Engl J Med 2003 ; 348 : 1875 – 1883 .
Barlogie B , Tricot GJ , van Rhee F , et al . Long-term outcome results [56] of the fi rst tandem autotransplant trial for multiple myeloma . Br J Haematol 2006 ; 135 : 158 – 164 .
Cavo M , Tosi P , Zamagni E , et al . Prospective, randomized study [57] of single compared with double autologous stem-cell transplantation for multiple myeloma: Bologna 96 clinical study . J Clin Oncol 2007 ; 25 : 2434 – 2441 .
Gahrton G , Svensson H , Cavo M , et al . Progress in allogenic bone [58] marrow and peripheral blood stem cell transplantation for multiple myeloma: a comparison between transplants performed 1983--93 and 1994–8 at European Group for Blood and Marrow Transplantation centres . Br J Haematol 2001 ; 113 : 209 – 216 .
Bjorkstrand B , Iacobelli S , Hegenbart U , et al . Tandem autologous/[59] reduced-intensity conditioning allogeneic stem-cell transplantation versus autologous transplantation in myeloma: long-term follow-up . J Clin Oncol 2011 ; 29 : 3016 – 3022 .
McArthur JR , Athens JW , Wintrobe MM , et al . Melphalan and [7] myeloma . Experience with a low-dose continuous regimen. Ann Intern Med 1970 ; 72 : 665 – 670 .
Harrington WJ , Moloney WC . Th e treatment of multiple myeloma [8] with urethane . Cancer 1950 ; 3 : 253 – 271 .
Speed DE , Galton DA , Swan A . Melphalan in the treatment of [9] myelomatosis . Br Med J 1964 ; 1 : 1664 – 1669 .
Snapper I . On the infl uence of stilbamidine upon multiple [10] myeloma . J Mt Sinai Hosp NY 1946 ; 13 : 119 – 127 .
Scott RB . Cancer chemotherapy--the fi rst twenty-fi ve years . Br [11] Med J 1970 ; 4 : 259 – 265 .
Blokhin N , Larionov L , Perevodchikova N , et al. [Clinical [12] experiences with sarcolysin in neoplastic diseases] . Ann NY Acad Sci 1958 ; 68 : 1128 – 1132 .
Myelomatosis: comparison of melphalan and cyclophosphamide [13] therapy . Br Med J 1971 ; 1 : 640 – 641 .
Alexanian R , Bergsagel DE , Migliore PJ , et al . Melphalan therapy [14] for plasma cell myeloma . Blood 1968 ; 31 : 1 – 10 .
Bergsagel DE , Griffi th KM , Haut A , et al . Th e treatment of plasma [15] cell myeloma . Adv Cancer Res 1967 ; 10 : 311 – 359 .
Alexanian R , Haut A , Khan AU , et al . Treatment for multiple [16] myeloma . Combination chemotherapy with diff erent melphalan dose regimens. JAMA 1969 ; 208 : 1680 – 1685 .
Costa G , Engle RL , Schilling A , et al . Melphalan and prednisone: [17] an eff ective combination for the treatment of multiple myeloma . Am J Med 1973 ; 54 : 589 – 599 .
Remission maintenance therapy for multiple myeloma . Southwest [18] Oncology Group Study . Arch Intern Med 1975 ; 135 : 147 – 152 .
Edwards BS , Hawkins MJ , Borden EC . Comparative in vivo and [20] in vitro activation of human natural killer cells by two recombinant alpha-interferons diff ering in antiviral activity . Cancer Res 1984 ; 44 : 3135 – 3139 .
Darnell J E Jr, Kerr IM , Stark GR . Jak-STAT pathways and [21] transcriptional activation in response to IFNs and other extracellular signaling proteins . Science 1994 ; 264 : 1415 – 1421 .
Du Z , Wei L , Murti A , et al . Non-conventional signal transduction [22] by type 1 interferons: the NF-kappaB pathway . J Cell Biochem 2007 ; 102 : 1087 – 1094 .
Creasey AA , Bartholomew JC , Merigan TC . Role of G0-G1 arrest [23] in the inhibition of tumor cell growth by interferon . Proc Natl Acad Sci USA 1980 ; 77 : 1471 – 1475 .
Gutterman JU . Cytokine therapeutics: lessons from interferon [24] alpha . Proc Natl Acad Sci USA 1994 ; 91 : 1198 – 1205 .
Mellstedt H , Aahre A , Bjorkholm M , et al . Interferon therapy in [25] myelomatosis . Lancet 1979 ; 2 : 697 .
Ahre A , Bjorkholm M , Mellstedt H , et al . Human leukocyte [26] interferon and intermittent high-dose melphalan-prednisone administration in the treatment of multiple myeloma: a randomized clinical trial from the Myeloma Group of Central Sweden . Cancer Treat Rep 1984 ; 68 : 1331 – 1338 .
Khoo TL , Vangsted AJ , Joshua D , et al . Interferon-alpha in the [27] treatment of multiple myeloma . Curr Drug Targets 2011 ; 12 : 437 – 446 .
Mandelli F , Avvisati G , Amadori S , et al . Maintenance treatment [28] with recombinant interferon alfa-2b in patients with multiple myeloma responding to conventional induction chemotherapy . N Engl J Med 1990 ; 322 : 1430 – 1434 .
Corso A , Nozza A , Lazzarino M , et al . Plateau phase in multiple [29] myeloma: an end-point of conventional-dose chemotherapy . Haematologica 1999 ; 84 : 336 – 341 .
Fritz E , Ludwig H . Interferon-alpha treatment in multiple [30] myeloma: meta-analysis of 30 randomised trials among 3948 patients . Ann Oncol 2000 ; 11 : 1427 – 1436 .
Myeloma Trialists ’ Collaborative Group . Interferon as therapy [31] for multiple myeloma: an individual patient data overview of 24 randomized trials and 4012 patients . Br J Haematol 2001 ; 113 : 1020 – 1034 .
Quesada JR , Talpaz M , Rios A , et al . Clinical toxicity of interferons [32] in cancer patients: a review . J Clin Oncol 1986 ; 4 : 234 – 243 .
Valentine AD , Meyers CA , Kling MA , et al . Mood and cognitive [33] side eff ects of interferon-alpha therapy . Semin Oncol 1998 ; 25 : 39 – 47 .
Floyd JD , Nguyen DT , Lobins RL , et al . Cardiotoxicity of cancer [34] therapy . J Clin Oncol 2005 ; 23 : 7685 – 7696 .
Weiss K . Safety profi le of interferon-alpha therapy . Semin Oncol [35] 1998 ; 25 : 9 – 13 .
Case D C Jr, Sonneborn HL , Paul SD , et al . Phase II study of rDNA [36] alpha-2 interferon (INTRON A) in patients with multiple myeloma
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
462 B. M. Cherry et al.
Stewart AK , Trudel S , Bahlis N , et al . A randomized phase III trial [82] of thalidomide and prednisone as maintenance therapy following autologous stem cell transplantation (ASCT) in patients with multiple myeloma (MM): the NCIC CTG MY.10 trial . Blood 2010 ; 116(Suppl. 1) : Abstract 2039.
Abdelkefi A , Ladeb S , Torjman L , et al . Single autologous stem-cell [83] transplantation followed by maintenance therapy with thalidomide is superior to double autologous transplantation in multiple myeloma: results of a multicenter randomized clinical trial . Blood 2008 ; 111 : 1805 – 1810 . Retraction in Blood 2009;113:6265.
Morgan GJ , Gregory WM , Davies FE , et al . Th e role of maintenance [84] thalidomide therapy in multiple myeloma: MRC Myeloma IX results and meta-analysis . Blood 2012 ; 119 : 7 – 15 .
Ludwig H , Adam Z , Tothova E , et al . Th alidomide maintenance [85] treatment increases progression-free but not overall survival in elderly patients with myeloma . Haematologica 2010 ; 95 : 1548 – 1554 .
Barlogie B , Anaissie E , van Rhee F , et al . Reiterative survival [86] analyses of total therapy 2 for multiple myeloma elucidate follow-up time dependency of prognostic variables and treatment arms . J Clin Oncol 2010 ; 28 : 3023 – 3027 .
Lokhorst HM , van der Holt B , Zweegman S , et al . A randomized [87] phase 3 study on the eff ect of thalidomide combined with adriamycin, dexamethasone, and high-dose melphalan, followed by thalidomide maintenance in patients with multiple myeloma . Blood 2010 ; 115 : 1113 – 1120 .
Kumar SK , Rajkumar SV , Dispenzieri A , et al . Improved survival [88] in multiple myeloma and the impact of novel therapies . Blood 2008 ; 111 : 2516 – 2520 .
Dimopoulos MA , Chen C , Spencer A , et al . Long-term follow-[89] up on overall survival from the MM-009 and MM-010 phase III trials of lenalidomide plus dexamethasone in patients with relapsed or refractory multiple myeloma . Leukemia 2009 ; 23 : 2147 – 2152 .
Palumbo A , Delforge M , Catalano J , et al . A phase 3 study evaluating [90] the effi cacy and safety of lenalidomide combined with melphalan and prednisone in patients � 65 years with newly diagnosed multiple myeloma (NDMM): continuous use of lenalidomide vs fi xed-duration regimens . Blood 2010 ; 116(Suppl. 1) : Abstract 2310.
Palumbo A , Gay F , Falco P , et al . Bortezomib as induction before [91] autologous transplantation, followed by lenalidomide as consolidation-maintenance in untreated multiple myeloma patients . J Clin Oncol 2010 ; 28 : 800 – 807 .
Davies F , Baz R . Lenalidomide mode of action: linking bench and [92] clinical fi ndings . Blood Rev 2010 ; 24(Suppl. 1) : S13 – S19 .
Lopez-Girona A , Heintel D , Zhang LH , et al . Lenalidomide [93] downregulates the cell survival factor, interferon regulatory factor-4, providing a potential mechanistic link for predicting response . Br J Haematol 2011 ; 154 : 325 – 336 .
Heintel D , Zojer N , Schreder M , et al . Expression of MUM1/IRF4 [94] mRNA as a prognostic marker in patients with multiple myeloma . Leukemia 2008 ; 22 : 441 – 445 .
Lioznov M , El-Cheikh J Jr, Hoff mann F , et al . Lenalidomide as [95] salvage therapy after allo-SCT for multiple myeloma is eff ective and leads to an increase of activated NK (NKp44( � )) and T (HLA-DR( � )) cells . Bone Marrow Transplant 2010 ; 45 : 349 – 353 .
van Heteren P , Renz O , Hahn-Ast C , et al . Activation of innate [96] immunity in patients receiving combination therapy with lenalidomide (Revlimid), cyclophosphamide and low-dose dexamethasone (RCd) for newly diagnosed or relapsed/refractory myeloma . Haematologica 2010 ; 95(Suppl. 2) :Abstract 0352.
McCarthy PL , Owzar K , Hofmeister CC , et al . Lenalidomide [97] after stem-cell transplantation for multiple myeloma . N Engl J Med 2012 ; 366 : 1770 – 1781 .
Attal M , Lauwers-Cances V , Marit G , et al . Lenalidomide [98] maintenance after stem-cell transplantation for multiple myeloma . N Engl J Med 2012 ; 366 : 1782 – 1791 .
Palumbo A , Hajek R , Delforge M , et al . Continuous lenalidomide [99] treatment for newly diagnosed multiple myeloma . N Engl J Med 2012 ; 366 : 1759 – 1769 .
Landgren O , Th omas A , Mailankody S . Myeloma and second [100] primary cancers . N Engl J Med 2011 ; 365 : 2241 – 2242 .
Th omas A , Mailankody S , Korde N , et al . Second malignan-[101] cies after multiple myeloma: from 1960s to 2010s. Blood 2012; 119 : 2731 – 2737 .
Adams J , Palombella VJ , Sausville EA , et al . Proteasome [102] inhibitors: a novel class of potent and eff ective antitumor agents . Cancer Res 1999 ; 59 : 2615 – 2622 .
Adams J . Th e proteasome: a suitable antineoplastic target . [103] Nat Rev Cancer 2004 ; 4 : 349 – 360 .
Krishnan A , Pasquini MC , Logan B , et al . Autologous [60] haemopoietic stem-cell transplantation followed by allogeneic or autologous haemopoietic stem-cell transplantation in patients with multiple myeloma (BMT CTN 0102): a phase 3 biological assignment trial . Lancet Oncol 2011 ; 12 : 1195 – 1203 .
Attal M , Harousseau JL , Leyvraz S , et al . Maintenance therapy [61] with thalidomide improves survival in patients with multiple myeloma . Blood 2006 ; 108 : 3289 – 3294 .
Kotla V , Goel S , Nischal S , et al . Mechanism of action of [62] lenalidomide in hematological malignancies . J Hematol Oncol 2009 ; 2 : 36 .
D ’ Amato RJ , Loughnan MS , Flynn E , et al . Th alidomide is an [63] inhibitor of angiogenesis . Proc Natl Acad Sci USA 1994 ; 91 : 4082 – 4085 .
Kenyon BM , Browne F , D ’ Amato RJ . Eff ects of thalidomide and [64] related metabolites in a mouse corneal model of neovascularization . Exp Eye Res 1997 ; 64 : 971 – 978 .
Singhal S , Mehta J , Desikan R , et al . Antitumor activity [65] of thalidomide in refractory multiple myeloma . N Engl J Med 1999 ; 341 : 1565 – 1571 .
Rajkumar SV , Hayman S , Gertz MA , et al . Combination therapy [66] with thalidomide plus dexamethasone for newly diagnosed myeloma . J Clin Oncol 2002 ; 20 : 4319 – 4323 .
List AF . Lenalidomide--the phoenix rises . N Engl J Med [67] 2007 ; 357 : 2183 – 2186 .
Barlogie B , Tricot G , Anaissie E , et al . Th alidomide and [68] hematopoietic-cell transplantation for multiple myeloma . N Engl J Med 2006 ; 354 : 1021 – 1030 .
Lokhorst HM , Schmidt-Wolf I , Sonneveld P , et al . Th alidomide [69] in induction treatment increases the very good partial response rate before and after high-dose therapy in previously untreated multiple myeloma . Haematologica 2008 ; 93 : 124 – 127 .
Spencer A , Prince HM , Roberts AW , et al . Consolidation therapy [70] with low-dose thalidomide and prednisolone prolongs the survival of multiple myeloma patients undergoing a single autologous stem-cell transplantation procedure . J Clin Oncol 2009 ; 27 : 1788 – 1793 .
Barlogie B , Pineda-Roman M , van Rhee F , et al . Th alidomide arm [71] of Total Th erapy 2 improves complete remission duration and survival in myeloma patients with metaphase cytogenetic abnormalities . Blood 2008 ; 112 : 3115 – 3121 .
Hahn-Ast C , von Lilienfeld-Toal M , van Heteren P , et al . Improved [72] progression-free survival and overall survival with thalidomide maintenance therapy in multiple myeloma: a meta-analysis of randomized trials in 2274 patients . Haematologica 2010 ; 95(Suppl. 2) : Abstract 0942.
Beksac M , Haznedar R , Firatli-Tuglular T , et al . Addition of [73] thalidomide to oral melphalan/prednisone in patients with multiple myeloma not eligible for transplantation: results of a randomized trial from the Turkish Myeloma Study Group . Eur J Haematol 2011 ; 86 : 16 – 22 .
Palumbo A , Bringhen S , Caravita T , et al . Oral melphalan and [74] prednisone chemotherapy plus thalidomide compared with melphalan and prednisone alone in elderly patients with multiple myeloma: randomised controlled trial . Lancet 2006 ; 367 : 825 – 831 .
Waage A , Gimsing P , Fayers P , et al . Melphalan and prednisone [75] plus thalidomide or placebo in elderly patients with multiple myeloma . Blood 2010 ; 116 : 1405 – 1412 .
Wijermans P , Schaafsma M , Termorshuizen F , et al . Phase III study [76] of the value of thalidomide added to melphalan plus prednisone in elderly patients with newly diagnosed multiple myeloma: the HOVON 49 Study . J Clin Oncol 2010 ; 28 : 3160 – 3166 .
Palumbo A , Bringhen S , Liberati AM , et al . Oral melphalan, [77] prednisone, and thalidomide in elderly patients with multiple myeloma: updated results of a randomized controlled trial . Blood 2008 ; 112 : 3107 – 3114 .
Lonial S , Mitsiades CS , Richardson PG . Treatment options [78] for relapsed and refractory multiple myeloma . Clin Cancer Res 2011 ; 17 : 1264 – 1277 .
Laubach J , Richardson P , Anderson K . Multiple myeloma . Annu [79] Rev Med 2011 ; 62 : 249 – 264 .
Barlogie B , Attal M , Crowley J , et al . Long-term follow-up of [80] autotransplantation trials for multiple myeloma: update of protocols conducted by the intergroupe francophone du myelome, southwest oncology group, and university of arkansas for medical sciences . J Clin Oncol 2010 ; 28 : 1209 – 1214 .
Stewart AK , Chen CI , Howson-Jan K , et al . Results of a multicenter [81] randomized phase II trial of thalidomide and prednisone maintenance therapy for multiple myeloma after autologous stem cell transplant . Clin Cancer Res 2004 ; 10 : 8170 – 8176 .
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f G
lasg
ow o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.
Evolving myeloma treatment paradigms 463
Palumbo A , Bringhen S , Rossi D , et al . Bortezomib-melphalan-[114] prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial . J Clin Oncol 2010 ; 28 : 5101 – 5109 .
Sonneveld P , Schmidt-Wolf I , van der Holt B , et al . HOVON-[115] 65/GMMG-HD4 randomized phase III trial comparing bortezomib, doxorubicin, dexamethasone (PAD) vs VAD followed by high-dose melphalan (HDM) and maintenance with bortezomib or thalidomide in patients with newly diagnosed multiple myeloma (MM) . Blood 2010 ; 116(Suppl. 1) :Abstract 2040.
Rajkumar SV , Gahrton G , Bergsagel PL . Approach to the [116] treatment of multiple myeloma: a clash of philosophies . Blood 2011 ; 118 : 3205 – 3211 .
van Rhee F , Szymonifka J , Anaissie E , et al . Total Th erapy 3 for [117] multiple myeloma: prognostic implications of cumulative dosing and premature discontinuation of VTD maintenance components, bortezomib, thalidomide, and dexamethasone, relevant to all phases of therapy . Blood 2010 ; 116 : 1220 – 1227 .
Rajkumar SV , Jacobus S , Callander NS , et al . Lenalidomide [118] plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trial . Lancet Oncol 2010 ; 11 : 29 – 37 .
Tan D , Ong KH , Koh LP , et al . Th e impact of frontline risk-adapted [119] strategy on the overall survival of patients with newly diagnosed multiple myeloma: an analysis of the Singapore multiple myeloma study group . Eur J Haematol 2012 ; 89 : 136 – 144 .
Moreau P , Rajkumar SV . “ Should all eligible patients with [120] multiple myeloma receive autologous stem-cell transplant as part of initial treatment? ” . Leuk Res 2012 ; 36 : 677 – 681 .
Badros AZ . Lenalidomide in myeloma--a high-maintenance [121] friend . N Engl J Med 2012 ; 366 : 1836 – 1838 .
Waxman AJ , Kuehl WM , Balakumaran A , et al . Smoldering [122] (asymptomatic) multiple myeloma: revisiting the clinical dilemma and looking into the future . Clin Lymphoma Myeloma Leuk 2010 ; 10 : 248 – 257 .
Hideshima T , Chauhan D , Schlossman R , et al . Th e role of [104] tumor necrosis factor alpha in the pathophysiology of human multiple myeloma: therapeutic applications . Oncogene 2001 ; 20 : 4519 – 4527 .
LeBlanc R , Catley LP , Hideshima T , et al . Proteasome inhibitor [105] PS-341 inhibits human myeloma cell growth in vivo and prolongs survival in a murine model . Cancer Res 2002 ; 62 : 4996 – 5000 .
Hideshima T , Richardson P , Chauhan D , et al . Th e proteasome [106] inhibitor PS-341 inhibits growth, induces apoptosis, and overcomes drug resistance in human multiple myeloma cells . Cancer Res 2001 ; 61 : 3071 – 3076 .
Hideshima T , Richardson PG , Anderson KC . Mechanism of [107] action of proteasome inhibitors and deacetylase inhibitors and the biological basis of synergy in multiple myeloma . Mol Cancer Th er 2011 ; 10 : 2034 – 2042 .
Richardson PG , Barlogie B , Berenson J , et al . A phase 2 [108] study of bortezomib in relapsed, refractory myeloma . N Engl J Med 2003 ; 348 : 2609 – 2617 .
Mateos MV , Hernandez JM , Hernandez MT , et al . Bortezomib [109] plus melphalan and prednisone in elderly untreated patients with multiple myeloma: results of a multicenter phase 1/2 study . Blood 2006 ; 108 : 2165 – 2172 .
Hernandez JM , Garcia-Sanz R , Golvano E , et al . Randomized [110] comparison of dexamethasone combined with melphalan versus melphalan with prednisone in the treatment of elderly patients with multiple myeloma . Br J Haematol 2004 ; 127 : 159 – 164 .
San Miguel JF , Schlag R , Khuageva NK , et al . Bortezomib plus [111] melphalan and prednisone for initial treatment of multiple myeloma . N Engl J Med 2008 ; 359 : 906 – 917 .
Richardson PG , Sonneveld P , Schuster MW , et al . Bortezomib [112] or high-dose dexamethasone for relapsed multiple myeloma . N Engl J Med 2005 ; 352 : 2487 – 2498 .
Mateos MV , Oriol A , Martinez-Lopez J , et al . Bortezomib, [113] melphalan, and prednisone versus bortezomib, thalidomide, and prednisone as induction therapy followed by maintenance treatment with bortezomib and thalidomide versus bortezomib and prednisone in elderly patients with untreated multiple myeloma: a randomised trial . Lancet Oncol 2010 ; 11 : 934 – 941 .