112
A PATIENT, PROFESSIONAL, PROVIDER AND PAYER PERSPECTIVE R f d C WOUND CARE – SHAPING THE FUTURE Volume 14 Number 2 October 2014 Published by European Wound Management Association
| Date post: | 05-Apr-2016 |
| Category: |
Documents |
| Upload: | ewma-european-wound-management-association |
| View: | 282 times |
| Download: | 8 times |

A PATIENT, PROFESSIONAL, PROVIDER AND PAYER PERSPECTIVE
R f
d C
1234567890+´
qwertyuiopå¨
asdfghjklæø’
<zxcvbnm,.-
§!”#€%&/()=?`
QWERTYUIOPÅ^
ASDFGHJKLÆØ*
>ZXCVBNM;:_
WOUND CARE – SHAPING THE FUTURE
Volume 14Number 2October 2014
Published byEuropeanWound ManagementAssociation

EWMA Council
The EWMA JournalISSN number: 1609-2759
Volume 14, No 2, October, 2014
The Journal of the EuropeanWound Management Association
Published twice a year
Editorial BoardSue Bale, UK, Editor
Salla Seppänen, Finland Georgina Gethin, Ireland
Martin Koschnick, GermanyRytis Rimdeika, Lithuania
José Verdú Soriano, SpainRita Gaspar Videira, Portugal
EWMA web sitewww.ewma.org
Editorial Officeplease contact:
EWMA SecretariatNordre Fasanvej 113
2000 Frederiksberg, DenmarkTel: (+45) 7020 0305Fax: (+45) 7020 0315
Layout:Birgitte Clematide
Cover:Nils Hartmann, Open design/advertising
Printed by:CS Grafisk A/S, Denmark
Copies printed: 11.000
Prices:The EWMA Journal is distributed
in hard copies to members as part of their EWMA membership.
EWMA also shares the vision of an “open access” philosophy,
which means that the journal is freely available online.
Individual subscription per issue: 7.50€
Libraries and institutions per issue: 25€
The next issue will be published in April 2015. Prospective material for
publication must be with the EWMA Secretariat as soon as possible and no later than January 15th 2015.
The contents of articles and letters inEWMA Journal do not necessarily reflect
the opinions of the Editors or the European Wound Management Association.
All scientific articles are peer reviewed by EWMA Scientific Review Panel.
Copyright of published materialand illustrations is the property of
the European Wound ManagementAssociation. However, provided prior
written consent for their reproduction, including parallel publishing
(e.g. via repository), obtained from EWMA via the Editorial Board of the Journal,
and proper acknowledgement, such permission will normally
be readily granted. Requests to reproduce material should state
where material is to be published, and, if it is abstracted, summarised,
or abbreviated, then the proposed new text should be sent to the
EWMA Journal Editor for final approval.
All issues of EWMA Journal are CINAHL listed.
COOPERATING ORGANISATIONS’ BOARD
Esther Armans Moreno, AEEVHChristian Thyse, AFISCeP.beMassimo Rivolo, AISLeCRoberto Cassino, AIUCAna-Maria Iuonut, AMP RomaniaAníbal Justiniano, APTFeridasGilbert Hämmerle, AWAKirsty Mahoney, AWTVNFJan Vandeputte, BEFEWOVladislav Hristov, BWAEls Jonckheere, CNCLenka Veverková, CSLRIvana Vranjkovic, CWAArne Buss, DGfWBo Jørgensen, DSFSHeidi Castrén, FWCS
Rosa Nascimento, GAIFJ. Javier Soldevilla, GNEAUPPGeorgios Vasilopoulos, HSWHChristian Münter, ICWAleksandra Kuspelo, LBAASusan Knight, LUFLoreta Pilipaityte, LWMACorinne Ward, MASCHunyadi János, MSKTSuzana Nikolovska, MWMALinda Primmer, NATVNSØystein Karlsen, NIFSLouk van Doorn, NOVWArkadiusz Jawien, PWMASeverin Läuchli, SAfW (DE)
Hubert Vuagnat, SAfW (FR)
Goran D. Lazovic, SAWMA
Mária Hok, SEBINKOF. Xavier Santos Heredero, SEHERSylvie Meaume, SFFPCSusanne Dufva, SSISJozefa Košková, SSOORLeonid Rubanov, STW (Belarus)Guðbjörg Pálsdóttir, SUMSCedomir Vucetic, SWHS SerbiaMagnus Löndahl, SWHS SwedenTina Chambers, TVSJasmina Begic-Rahic, URuBiHZoya Ishkova, UWTOBarbara E. den Boogert-Ruimschotel, V&VNCaroline McIntosh, WMAISkender Zatriqi, WMAKNada Kecelj Leskovec, WMASMustafa Deveci, WMAT
Paulo Jorge Pereira Alves, PortugalCaroline Amery, UKJan Apelqvist, SwedenSue Bale, UKMichelle Briggs, UKStephen Britland, UKMark Collier, UKRose Cooper, UKJavorka Delic, SerbiaCorrado Durante, ItalyBulent Erdogan, TurkeyAnn-Mari Fagerdahl, SwedenMadeleine Flanagan, UK Milada Francu, Czech RepublicPeter Franks, UKFrancisco P. García-Fernández, SpainMagdalena Annersten Gershater, Sweden
Georgina Gethin, IrelandLuc Gryson, BelgiumMarcus Gürgen, NorwayEskild W. Henneberg, DenmarkAlison Hopkins, UKGabriela Hösl, AustriaDubravko Huljev, CroatiaArkadiusz Jawien, PolandGerrolt Jukema, NetherlandsNada Kecelj, SloveniaKlaus Kirketerp-Møller, DenmarkZoltán Kökény, HungaryMartin Koschnick, Germany Knut Kröger, GermanySeverin Läuchli, SchwitzerlandMaarten J. Lubbers, NetherlandsSylvie Meaume, France
EWMA JOURNAL SCIENTIFIC REVIEW PANEL
Zena Moore, Ireland Christian Münter, GermanyAndrea Nelson, UKPedro L. Pancorbo-Hidalgo, Spain Hugo Partsch, AustriaPatricia Price, UKSebastian Probst, SchwitzerlandElia Ricci, ItalyRytis Rimdeika, LithuaniaZbigniew Rybak, PolandSalla Seppänen, FinlandJosé Verdú Soriano, Spain Robert Strohal, AustriaRichard White, UKCarolyn Wyndham-White, SwitzerlandGerald Zöch, Austria
Salla SeppänenPresident
Jan ApelqvistImmediate Past President
Severin LäuchliPresident Elect
Hubert VuagnatRobert StrohalRytis Rimdeika Jan StryjaAlberto Piaggesi Andrea Pokorná
Edward JudeArkadiusz Jawien Knut KrögerMartin KoschnickGerrolt Jukema
Ann-Mari Fagerdahl Magdalena Anner-sten Gershater
Mark Collier Georgina GethinSue BaleEWMA Journal Editor
Luc GrysonTreasurer
Dubravko HuljevSecretary
José Verdú SorianoScientific Recorder
2
Science, Practice and Education
Organisations
Cochrane Reviews
Scientific Communication
EWMA
5 Editorial
7 Economic outcomes of a new chronic wound treatment system in Poland. K. Grzegorz, W. Robert, O. N. Małgorzata 15 Dressings for split thickness skin graft donor sites
D. P. Barrit, H. Birke-Sorensen 21 The utility of pulse volume waveforms in the identification of lower limb arterial insufficiency. J. H. Davies, J. E. A. Lewis, E. M. Williams 27 The importance of using a nutritional risk analysis scale in patients admitted to continued care
J. M. Corrales, N. P. Gayo, M. C. P. Águila, A. M. Martín, A. Ribeiro 33 Neonatal facial pressure ulcers related to non-invasive ventilation L Bonell-Pons, P. García-Molina, E. Balaguer-López, M. Á. M., M. C. Rodríguez
35 Healthcare-associated infections (HCAIs). M. Kiernan, D. Leaper 39 The value of veterinary wound management for human wounds and wound care. J. M. Wilmink 43 Telemedical wound assessment on the way to large scale deployment in Denmark. E. W. Henneberg 48 Reflections on the use of telemedicine in wound Care. R. Jelnes 52 R.I.S.E for the prevention of pressure ulcers. G. Gethin, C. McIntosh 56 Setting a course on chronic wounds in Cameroon
A. Same-Ekobo, G. Ehounou, E. Comte, H. Vuagnat
61 Abstracts of recent cochrane reviews. S. Bell-Syer
68 EWMA Journal previous issues and other journals 70 EWMA-GNEAUPP 2014 in Madrid, Spain. G. Jukema 74 Cooperating Organisations activities during the EWMA - GNEAUPP Conference. J. Apelqvist 76 TVS 2014 activities. H. Sandoz 78 The organisation of wound care in England. A. Hopkins 80 Visit EWMA 2015 in London, United Kingdom 82 A report from the EWMA Teacher Network
S. Holloway, D. Hopkins, D. Huljev 84 Home Care – Wound Care. G. Gethin, S. Probst 88 Nordic Diabetic Foot Task Force: status and activities
K. Kirketerp-Møller 90 EWMA study recommendations for clinical investigations in leg ulcers and wound care. P. Price 92 EWMA in collaboration with the EU Joint Action on Chronic Diseases
S. Seppänen 94 Report from the 2nd Charcot Foot Course. A. Koller, M. Spraul 95 EWMA news 96 EWMA’s participation in EU-funded projects – Update 98 EWMA appreciations and new EWMA council members
S. Seppänen100 Book Review: Acute and Chronic Wounds: Current Management Concepts. G. Gethin101 Former EMWA President gives the honorary State of the Art Jörg Auer Lecture at the ECVS annual meeting 102 EWMA Corporate Sponsors
103 Conference calendar104 AAWC news. V. R. Driver105 WAWLC annual symposium 2014 with focus on wound care kit107 Report from the 10th national conferenceof AWMA in Gold Coast A. Fagerdahl108 All Wales Tissue Viability Nurse Forum T. Young110 Cooperating Organisations
LONDON · UKEWMA 2015
13-15 MAY 2015
25th Conference of the European Wound Management Association
WOUND CARE – SHAPING THE FUTURE
A PATIENT, PROFESSIONAL, PROVIDER AND PAYER PERSPECTIVE
WWW.EWMA2015.ORGWWW.EWMA.ORG WWW.TVS.ORG.UK
Abstract submission
deadline: 1 December 2014
EWMA Journal 2014 vol 14 no 2

Suprasorb® P silicone NEW
The wound dressing for the sensitive skin around the wound.
Please find more about Suprasorb P silicone here:
■■ easy to apply■■ virtually painless to remove ■■ promotes a moist wound healing environment
With an adhesive silicone layer – especially gentle on the wound bed and the sensitive skin around the wound.
For an improved life quality and a high patient satisfaction.
www.Lohmann-Rauscher.com
L-R_AZ_Suprasorb_P_silicone_210x297_EWMA Journal_E_DU20140825.indd 1 25.08.14 14:15

This issue of EWMA Journal reflects our Confer-ence theme for 2015. This event will be held in London 13-15 May and we are very pleased
to announce that it is being organised in collaboration with The Tissue Viability Society (TVS). The conference theme “WOUND CARE SHAPING THE FUTURE – a patient, professional, provider and payer perspective” underlines the importance of the challenges posed by the demographic development in the European Union, which has caused healthcare costs across Europe to grow exponentially over the past decades, as demonstrated by the OECD report Health at a glance Europe from 2012.
Governments across Europe are actively exploring work-able solutions to save costs in order to control health care expenditures, whilst at the same time seeking to provide excellent quality of care. These challenges are driving the re-organisation of health care systems, which among other aspects include speeding up the discharge home of hos-pitalised patients. To help ensure patient safety and cost-effective care, such developments provide opportunities to utilise new and existing technological solutions. These solutions include telemedicine and other technologies that may provide cost effective ways of monitoring and treating patients in their own home.
The EWMA 2015 conference will explore issues that in-clude: n Who will benefit from this development? Are we always placing the patient’s best interest in the centre or has the focus shifted towards the “payer”?n Is today’s healthcare structure prepared for the current and future development and if not, which organisational changes are needed to ensure optimal benefit from the available technologies? n What training and education is needed for patients and health care professionals to improve cross sectorial communication.The EWMA 2015 conference in London will seek to provide answers to some of those controversies and give some direction for innovative and effective solutions in wound care. Some articles in this issue of the EWMA Journal focus on economical and technology-related aspects of treat-ment. On page 7, Grzegorz Krasowski et al. show how organisation of the treatment of chronic wounds in Poland
has shown promising results on outcomes such as savings on economy as well as the extent of hospitalisation of pa-tients. On page 15, Dorte P Barrit evaluates new, cheaper dressings for split skin donor sites, as alternatives to more costly products. Using cost-effectiveness arguments, that author demonstrates that the cheapest option based on product costs; turn out to be more expensive when tak-ing into account other factors such as number of dressing changes required.
On page 21, Jane Davies investigates how combining and automating two tools for the assessment of lower limb arterial status may provide more precise diagnostics and lower the barriers to performing an accurate analysis of the results. This is an example of how technology may lead to better wound care, better distribution of work load, and possibly a smaller economic footprint per patient. Telemedicine and digital health are important develop-ments in health care, and on page 43 Eskild W. Hen-neberg from the Danish Society for Wound Healing re-ports progress made in Denmark in recent years. Building on this Rolf Jelnes, page 48, further explores the use of telemedical wound assessment in Southern Jutland. De-veloping telemedicine in this region has formed the basis for the large scale deployment of telemedical wound as-sessment in Denmark based on the positive feedback from patients as well as health care staff.
EWMA follows closely innovation and initiates projects that aim to optimise the organisation of wound care, devel-oping new technology and gathering evidence for the effect of digital medicine. One obvious example is the United 4 Health project (www.united4health.eu) of which EWMA has been an active partner since its start in January 2013.EWMA and TVS will put the future of wound care in the spotlight at the conference in London on 13-15 May 2015 (EWMA2015.org). We invite you to take part in these developments and make your own contribution, not only to the aspects mentioned here but to all aspects of wound care, either as a participant or as a contributor, by sending in your abstract before 1 December 2014 (ewma2015.org/scientific/abstracts).
We look forward to seeing you in London.
Salla Seppänen, EWMA PresidentSue Bale, Editor of EWMA Journal
Wound care shaping the future– a patient, professional, provider and payer perspective
Editorial
EWMA Journal 2014 vol 14 no 2 5
To learn more, please visit acelity.com
VeraFlo™ Therapyusing V.A.C.Ulta™ Negative Pressure
Wound Therapy System
CelluTome™
Epidermal HarvestingSystem
Prevena™
Incision ManagementSystemSystem
SILVERCEL®NON-ADHERENT
AntimicrobialDressing
ADAPTICTOUCH®
Non-Adhering SiliconeDressing
TIELLE®FAMILY
HydropolymerDressing
PROMOGRAN®
Collagen/ORC Dressing
PROMOGRAN PRISMA®
Collagen/ORC/Silver Dressing
Note: Specifi c indications, contraindications, warnings, precautions and safety information exist for KCI and Systagenix’ products and therapies. Please consult a physician and product instructions for use prior to application. Please refer to the full instructions for use.
©2014 KCI Licensing, Inc. All rights reserved. All trademarks designated herein are proprietary to KCI Licensing, Inc. and/or Systagenix, their affi liates and/or licensors. DSL#14-0435 (7/14).
You already know our products. Now meet Acelity.
We offer a portfolio of advanced wound healing products and support to better meet your needs.
Our commitment is to deliver proven solutions and specialisedknowledge to help people heal and be whole again.
4291
/ACE
/GLO
/08
14/P
RB34
70

Science, Practice and Education
Krasowski Grzegorz1,2
Wajda Robert1
Olejniczak-Nowakowska Małgorzata3
1Krapkowice Health Center, Krapkowice, Osiedle, Poland
2Opole University of Technology, Opole, Poland
3Public Health Department Public Health FacultyMedical University of Silesia, Bytom, Poland
Correspondence: [email protected]
Conflicts of interest: None
Health Fund (NHF) centres, from two visits per week to one visit per 2 weeks. Concurrently, the ratio of patients treated in a home-based setting increased from 15.7% to 68.8%. The average ulcer treatment duration decreased from 10 months to 5 months. The number of dressing changes also decreased from 7.5 dressing changes to 2.7 dressing changes per week. The number of patients in home based setting with nurse’s assistance per year increased from 18,8% to 41,8%. However, the cost of one dressing change increased from 5 euros to 10 euros. Overall, the cost to treat a single ulcer was 1,500 euros before and 540 euros after the introduction of the new system. Under the previous system, the combined cost incurred by the NHF was 1,822 euros per week. This cost declined to 1,564 euros per week after the introduction of the new system. The number of leg amputations due to a non-healing diabetic foot ulcer, and ischemic and mixed ulcers also declined from 7.8% to 2.9%.Conclusions: A change in the system and mode of treatment of chronic leg ulcers resulted in a significant decrease in expenditures incurred by the NHF.
Economic outcomes of a new chronic wound treatment system in PolandA comparison of the costs and expenses incurred by the National Health Fund before and after the introduction of a new system of leg ulcer treatment
ABSTRACTAim: The purpose of this study was to compare costs before and after the implementation of a new system of leg ulcer treatment.Methods: The study included four types of chro nic leg and foot ulcers (venous, ischemic, mixed, and dia-betic foot ulcers). The costs associated with leg and foot ulcers were compared between the years 2010 and 2012, which was before and after the implemen-tation of a new leg ulcer treatment system in the Krapkowice District, southwestern Poland. The key features of the new treatment system included a change in the primary treatment location from the hospital to the patient’s residence, and the introduc-tion of a modern therapy that consisted of causal and local wound treatment. The costs associated with the treatment were calculated from information about the ulcer duration, the number of dressings used, the number of patient visits, and the average cost of one dressing change. Results: Implementation of the new leg ulcer treat-ment system led to a decrease in visits to National
wounds and the disproportionate ratio between funding and treatment costs.
Prior to the introduction of a new system of treatment in the Krapkowice District of south-western Poland, patients suffering from chronic wounds were treated at hospitals and surgical out-patient clinics, and by primary healthcare physi-cians, using methods that were below the current standards of care. The basic procedures included once per day or more frequent dressing changes with gauze and peroxide or ethacridine solutions and application of antibiotic steroid ointments. Causal treatments were rarely applied, and pain
INTRODUCTIONAll healthcare systems aim to establish a model of chronic wound treatment that meets medical, so-cial, and economic requirements. Contemporary healthcare systems are based on social economy principles, which assume that the best overall treatment results should be obtained with limited financial resources. In practice, new procedures are financed by public funds when financial ben-efits exceed costs1. Unfortunately, as a result of this system, many specialist centres are reluctant to treat patients with chronic wounds. This reluc-tance arises from the chronic nature of chronic
EWMA Journal 2014 vol 14 no 2 7

Fig. 4. Chronic wound treatment in the Krapkowice Health Centre, Poland: Day 2
Figure 5. Chronic wound treatment in the Krapkowice Health Centre, Poland: Day 3
Patient identification
Initial assessment and treatment qualification
Home-based treatment
Specialized interventions
Training and assessment of
results
Figure 1. Organization of chronic wound treatment: Part 1
Lower leg ulceration treatment: How the program works
Specialised centres in cooperation with EWMA PTF PTLR
and sponsors
Specialized centres and short-term hospitalisations
PHC physicians and
community nurses
Specialised centres for chronic wound
treatment
Nursing home care
Figure 2. Organization of chronic wound treatment: Part 2
Venous leg ulceration treatment:Who conducts the treatment
Day 1: First stage of ambulatory care
n Anamnesis, physical examination, pulse measurement, ABI, weight and height measurements, photographic documentation of the wound, nutritional assessment, numerical pain intensity assessment
n Complementary tests: CBC, electrolytes, urea, creatinine, serum glucose, general urinalysis, ECG, and wound cultures
n Plans for further management (TIME), assignment of a supervising physician, the use of lavaseptic dressings and/or other antiseptics from the same line in infected wounds
n Pain treatment, anti-thrombotic prophylaxis, nutritional treatment initiation (if necessary)
n Complementary tests: vascular system UDP and possible obliteration
Day 2: Second stage of ambulatory careHospital-based procedures in italic.
n Surgical procedures: sections for histopathological examinations, surgical demarcations, amputations, cutaneous transplantations, transverse skin flaps, expander implantations, vascular procedures, establishment of nutritional access, etc.
n Additional consultations, e.g., diabetic, vascular, cardiology, etc.
n Specialised dressing implementationsn Patient educationn Motor rehabilitation
Day 3: Third stage of ambulatory careHospital-based procedures in italic.
n Preparation of information for home-based nursing care; orders for nursing care
n Dressing correction, follow-up planningn Prescriptions for dressings, analgesics, and nutritional
treatmentn Patients with severe complications such as inflammation,
recommended amputation, diabetic foot, or additional complications that require further hospital-based treatment are admitted
n Referral of patients to other centres, e.g., vascular surgery
Figure 3. Chronic wound treatment in the Krapkowice Health Centre, Poland: Day 1
treatments and nutritional support were never prescribed. In addition, most of the patients were subjected to am-bulatory or hospital treatment. Only 15.7% of patients received home-based treatment without the assistance of a nurse (Table 1). The authors developed a new chronic wound treatment model that aimed to satisfy contempo-rary pharmacoeconomics requirements. This new model
was implemented and assessed within the context of treat-ment efficacy and incurred expenses. This paper presents a detailed comparative analysis of conditions before and after the introduction of the new system of chronic wound treatment. Four types of chronic leg and foot ulcers were included in the study (i.e., venous, ischemic, mixed, and diabetic foot, ulcers).
MATERIALS AND METHODSThe new chronic wound treatment model included or-ganisational changes that allowed patients to receive home-based treatment, with simultaneous access to specialised medical supervision. The development and implementa-tion of the model was inspired by participation in the European Wound Management Association (EWMA)2. The model was first implemented in the Opole and Strzelce Opolskie districts of southwestern Poland between 2008 and 2010. It was implemented in the Krapkowice District, which includes approximately 70,000 inhabitants, after 2010. This paper presents a comparison of results from the Krapkowice District before (2010) and after (2012) the introduction of the new chronic wound treatment model.
Model introduction required many changes to the ex-isting system (e.g., Fig. 1, Fig. 2). The essential pillars of the implemented model included:
EWMA Journal 2014 vol 14 no 2 8

Science, Practice and Education
Recommendations for further management
n Please kindly change the dressing every day or when soaked according to the following schedule:
Performed by the patient:n 1. Remove old dressing; wash and iron the compres-
sion bandages*n 2. Wash lower legs and wounds with Octenisan liquid
and sponge (disposable)n 3. Dry lower legsn 4. Lubricate healthy-looking skin (Vaselini***)n 5. Swab the wound with an octenidine liquid for
approximately 15 minutes
Performed by a nurse:n 6. Sprinkle the wound with an octenidine liquid*****;
dry the skin around the woundn 7. Apply an octenidine gel****** to the woundn 8. Apply the absorbent hydrofibre dressing*******to
the wound; place non-adhesive foam on the dressingn 9. Fix dressings with an elastic bandage (new)n 10. Apply the compression dressings* (2 dressings on
each lower leg)
Orally: 2x1 pain-relieving tablets (active ingredient keto-profen)********Pain-relieving plaster (active ingredient fentanyl 25 µg) (change every 3 days)*********Injectable low molecular weight heparin solution 0.3 ml ********** 1 × 1 SC
Thanks in advance for your cooperationKind regards
Recommendations for further management
n Please kindly change the dressing every 3 days or when soaked according to the following schedule:
Performed by the patient:n 1. Take off the knee-length socks, remove the old dressing,
and wash the knee-length socksn 2. Wash lower legs and wounds with Octenisan liquid* and
sponge (disposable)n 3. Dry lower legsn 4. Lubricate healthy-looking skin (Vaselini**, linseed oil)n 5. Lubricate reddened and flaky skin (skin cream, active ingre-
dient Clobetasol Propionate)***n 6. Apply an octenidine liquid**** to the wound for approxi-
mately 15 minutes
Performed by a nurse:n 7. Sprinkle the wound with an octenidine liquid* and dry the
skin around the woundn 8. Apply a hydrofibre dressing with silver****** to the woundn 9. Apply an absorbent pad******* to the wound (change earlier
in the case of a soaked dressing)n 10. Fix gauze with an elastic bandage (new)n 11. Apply the thin knee-length sock first, then the rubber sock
Orally: 1x1 pain-relieving tablet (active ingredient tramadolhydro-chlorid 150 mg)******** – 1 × 1 pain-relieving tablet (active in-gredient ketoprofen 100mg) *********, 2 × 1 sachet, acid neu-tralising product (active ingredient someprazole 20 mg) **********
Injectable low molecular weight heparin solution (active ingredient enoxaparin sodium 20 mg)*********** 1 × 1 SC
Remember to remove the rubber knee-length sock before sleep
Thank you in advance for your cooperation,Kind regards
Figure 7. Examples of medical recommendations for a venous leg ulcer patient upon discharge from the surgical unit of the Krapkowice Health Centre, Poland
Figure 6. Examples of medical recommendations for a venous leg ulcer patient upon discharge from the Krapkowice Health Centre, Poland
1. Rapid identification of chronic wound patients. Chronic wounds are often hidden conditions that cause long-term suffering, and can be a sensitive is-sue for the patient. Home-care nurses and primary healthcare (PHC) physicians have a fundamental role in this system as a result of their frequent con-tact with patients from many risk groups.
2. Cooperation with centres specialised in the causal diagnosis of chronic wounds and in the performance of interventions that cannot be conducted at the patient’s home (e.g., surgical procedures, complex diagnostic management, modifications of previously ineffective treatments, establishment of nutritional access). At the Krapkowice Health Centre, chronic wound patients were admitted by appointment or
emergency care for both in- and outpatient treat-ment. The average length of the hospital stay was 3 days. During this period, causal diagnostics, causal, local, and pain treatment, and nutritional, bariatric, and antibiotic treatments were performed as needed (Fig. 3, Fig. 4, Fig. 5) On the day of discharge, each patient received detailed recommendations for fur-ther management (Fig. 6, Fig. 7). Hospitalisation was indicated for each patient whose medical condi-tion warranted further treatment (e.g., systemic in-fection, necrosis that requires surgical debridement, vascular procedures, skin grafts). In the remaining cases, preliminary diagnostics were performed on an
Figure 6. : * Putterbinde®, HARTMANN, ** Octenisan®, Schülke , *** Linomag®, Ziołolek Sp. z o.o., **** Octenilin® or Octenisept®, Schülke, ***** Octenisept®, Schülke, ****** Octenilin gel®, Schülke, ******* Hydrofiber®, ConvaTec, ******** Refastin®, Medana, ********* Matrifen®, NYCOMED, ********** Fraxiparin®, GlaxoSmithKline
Figure 7. : *Octenisan®, Schülke, **Linomag®, Ziołolek Sp. z o.o.,*** Novate®, BLAU FARMA, **** Octenilin® or Octenisept®, Schülke, ***** Octenisept®, Schülke, ****** Aquacel Ag®, ConvaTec, ******* Zetuvit®, Hartmann,********Tramal retard® 150, Grünenthal, ********* Refastin®, Medana, ********** Polprazol® 20, Polpharma, *********** Clexane® 20, Sanofi
EWMA Journal 2014 vol 14 no 2 9

Table 2. Costs of materials under the previous treatment system
Product Cost (Euro)
ethacridine €0.1 per 100ml
local antibiotic €0.4 per amp
hydrogen peroxide €0.05 per 100ml
silver sulfadiazine €0.74 per 100g
compress 5×5cm: €0.017×7cm: €0.015
chlorhexidine €1.13 per 100ml
elastic bandage €1 per bandage
Table 1. Comparison of monthly costs for venous leg ulcer treatment incurred by the NHF, for the previous and the new treatment systems
Costs given in this table are amounts reimbursed by NHF and described in Tables 2, 5 -7
Old system(2010)
New system(2012)
Number of patients with chronic wound 111 69
Number of patients per 1,000 inhabitants 1.59 0.99
Number of patients treated in a home-based setting
17/108=15.7% (n = 108) 44/64=68.8% (n = 64)
(Missing data: 3) (Missing data: 5)
Number of patients in home based setting with nurse’s assistance/year
18,8% (n = 17) 41.8% (n=44)
(4 patients × 9,6 months/ 12 months = 3,2)
(40 patients × 5,52 months/12 months = 18,4)
Amputation rate 7.8% (n = 103) 2.9% (n = 69)
(Missing data: 8)(diabetic foot-4, ischemic-3, mixed-1)
(diabetic foot-1, ischemic-1)
Number of visits to NHF units per month 8 2
Costs of ambulatory visits (according to the NHF prices in Table 7) €8 €8
Total monthly cost of ambulatory visits to NHF units (Euro) €7104 €1104
Monthly NHF reimbursement for dressings (euro)
€0
€1490.4(€2 per dressing change
× 2.7 dressing changes per week × 4 weeks × 69 patients)
NHF reimbursement for additional diagnostics (e.g., USG Doppler examination, microbiological cultures, histological assessment) per month (Euro)
0
€276 per monthOne Doppler examination (€26),
two microbiological cultures (2 × €7 = €14), one histological assessment (€8) per year
× 69 patients = 3312 per year
NHF reimbursement for home-based long-term nursing care per month €0
€3312 per month(26.67% of patients with nursing care coverage
× 69 patients × €180)
Hospital stays per month €184 per month(2.87 hospital stays per year × €768
= €2208 per year)
€73.6 per month(1.15 hospital stays per year × €768
= €883.2 per year)
Total cost (€ per month) €7288 €6256
NHF savings per year in the Krapkowice district under the new treatment system (Euro) €12,384
Expected NHF savings per year across Poland under the new treatment system (Euro) €6,811,200
outpatient basis in accordance with the procedures listed in Figures 3, 4, and 5. Wounds that did not re-quire surgical cleansing were debrided by staff at an outpatient clinic. More complex procedures (italics, Fig. 4 and Fig. 5) were performed during hospitalisa-tion.
3. Activation and appropriate education of nursing staff responsible for dressing changes, which included the development of long-term nursing care at the pa-tient’s residence.
4. Involvement of patients and relatives in the thera-peutic process. Patients who are included in the ther-apeutic process become co-responsible for the effects that are achieved. Patient involvement is important, especially during motor activity implementation.
5. Application of modern chronic wound treatment methods according to EWMA guidelines. Applica-tion of modern chronic wound treatment methodsaccording to EWMA and Polish Wound Treatment
Association guidelines (PTLR) 3, 4, 5, 6.
EWMA Journal 2014 vol 14 no 2 10
Science, Practice and Education
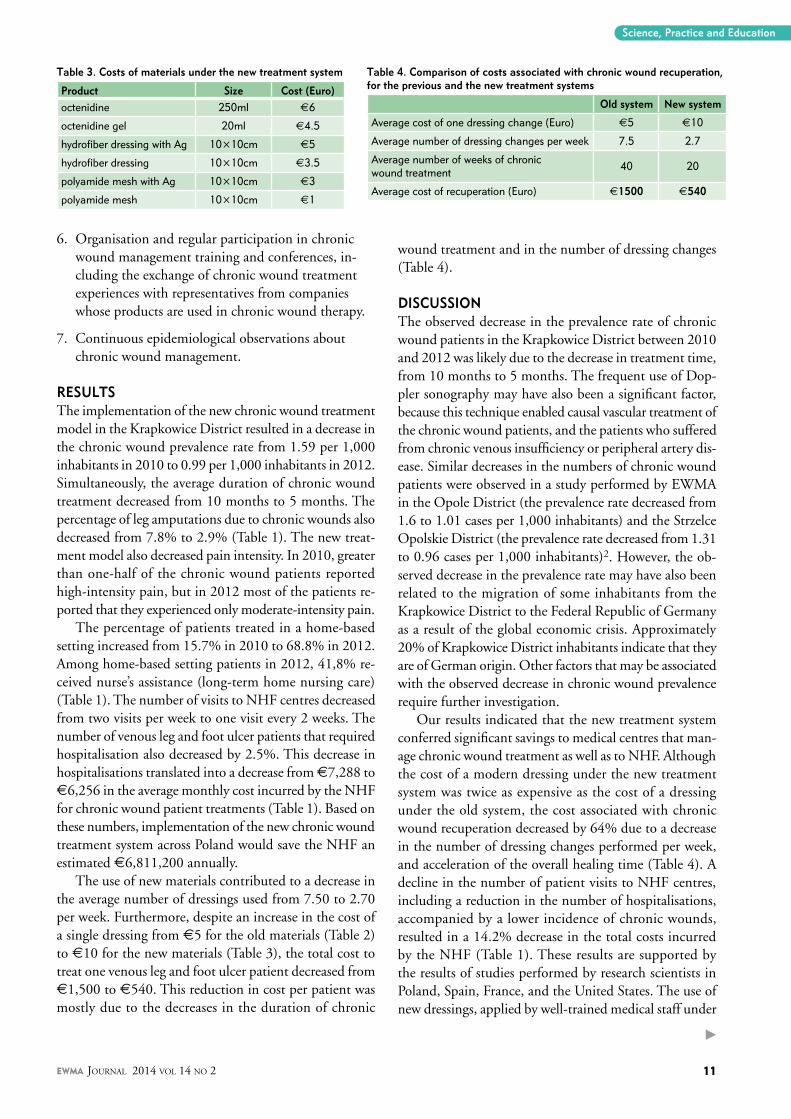
Table 3. Costs of materials under the new treatment system
Product Size Cost (Euro) octenidine 250ml €6
octenidine gel 20ml €4.5
hydrofiber dressing with Ag 10×10cm €5
hydrofiber dressing 10×10cm €3.5
polyamide mesh with Ag 10×10cm €3
polyamide mesh 10×10cm €1
Table 4. Comparison of costs associated with chronic wound recuperation, for the previous and the new treatment systems
Old system New system
Average cost of one dressing change (Euro) €5 €10
Average number of dressing changes per week 7.5 2.7
Average number of weeks of chronic wound treatment 40 20
Average cost of recuperation (Euro) €1500 €540
6. Organisation and regular participation in chronic wound management training and conferences, in-cluding the exchange of chronic wound treatment experiences with representatives from companies whose products are used in chronic wound therapy.
7. Continuous epidemiological observations about chronic wound management.
RESULTS The implementation of the new chronic wound treatment model in the Krapkowice District resulted in a decrease in the chronic wound prevalence rate from 1.59 per 1,000 inhabitants in 2010 to 0.99 per 1,000 inhabitants in 2012. Simultaneously, the average duration of chronic wound treatment decreased from 10 months to 5 months. The percentage of leg amputations due to chronic wounds also decreased from 7.8% to 2.9% (Table 1). The new treat-ment model also decreased pain intensity. In 2010, greater than one-half of the chronic wound patients reported high-intensity pain, but in 2012 most of the patients re-ported that they experienced only moderate-intensity pain.
The percentage of patients treated in a home-based setting increased from 15.7% in 2010 to 68.8% in 2012. Among home-based setting patients in 2012, 41,8% re-ceived nurse’s assistance (long-term home nursing care) (Table 1). The number of visits to NHF centres decreased from two visits per week to one visit every 2 weeks. The number of venous leg and foot ulcer patients that required hospitalisation also decreased by 2.5%. This decrease in hospitalisations translated into a decrease from €7,288 to €6,256 in the average monthly cost incurred by the NHF for chronic wound patient treatments (Table 1). Based on these numbers, implementation of the new chronic wound treatment system across Poland would save the NHF an estimated €6,811,200 annually.
The use of new materials contributed to a decrease in the average number of dressings used from 7.50 to 2.70 per week. Furthermore, despite an increase in the cost of a single dressing from €5 for the old materials (Table 2) to €10 for the new materials (Table 3), the total cost to treat one venous leg and foot ulcer patient decreased from €1,500 to €540. This reduction in cost per patient was mostly due to the decreases in the duration of chronic
wound treatment and in the number of dressing changes (Table 4).
DISCUSSIONThe observed decrease in the prevalence rate of chronic wound patients in the Krapkowice District between 2010 and 2012 was likely due to the decrease in treatment time, from 10 months to 5 months. The frequent use of Dop-pler sonography may have also been a significant factor, because this technique enabled causal vascular treatment of the chronic wound patients, and the patients who suffered from chronic venous insufficiency or peripheral artery dis-ease. Similar decreases in the numbers of chronic wound patients were observed in a study performed by EWMA in the Opole District (the prevalence rate decreased from 1.6 to 1.01 cases per 1,000 inhabitants) and the Strzelce Opolskie District (the prevalence rate decreased from 1.31 to 0.96 cases per 1,000 inhabitants)2. However, the ob-served decrease in the prevalence rate may have also been related to the migration of some inhabitants from the Krapkowice District to the Federal Republic of Germany as a result of the global economic crisis. Approximately 20% of Krapkowice District inhabitants indicate that they are of German origin. Other factors that may be associated with the observed decrease in chronic wound prevalence require further investigation.
Our results indicated that the new treatment system conferred significant savings to medical centres that man-age chronic wound treatment as well as to NHF. Although the cost of a modern dressing under the new treatment system was twice as expensive as the cost of a dressing under the old system, the cost associated with chronic wound recuperation decreased by 64% due to a decrease in the number of dressing changes performed per week, and acceleration of the overall healing time (Table 4). A decline in the number of patient visits to NHF centres, including a reduction in the number of hospitalisations, accompanied by a lower incidence of chronic wounds, resulted in a 14.2% decrease in the total costs incurred by the NHF (Table 1). These results are supported by the results of studies performed by research scientists in Poland, Spain, France, and the United States. The use of new dressings, applied by well-trained medical staff under
EWMA Journal 2014 vol 14 no 2 11
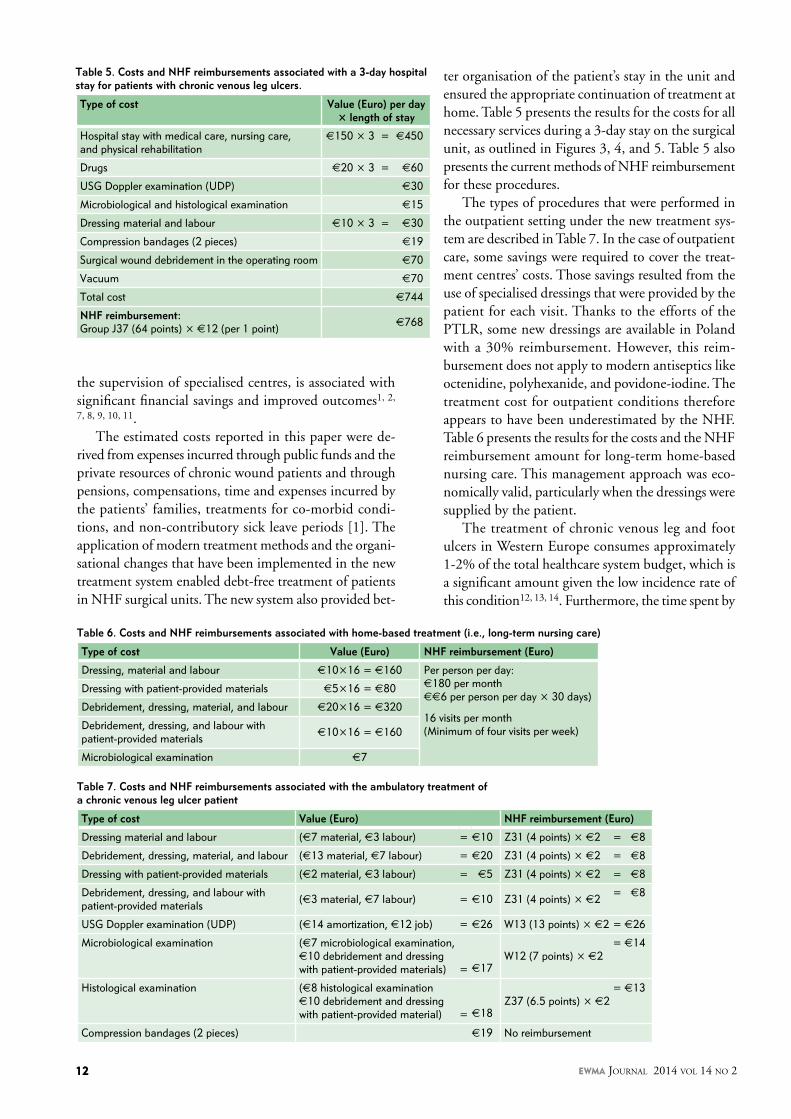
Table 5. Costs and NHF reimbursements associated with a 3-day hospital stay for patients with chronic venous leg ulcers.
Type of cost Value (Euro) per day × length of stay
Hospital stay with medical care, nursing care, and physical rehabilitation
€150 × 3 = €450
Drugs €20 × 3 = €60
USG Doppler examination (UDP) €30
Microbiological and histological examination €15
Dressing material and labour €10 × 3 = €30
Compression bandages (2 pieces) €19
Surgical wound debridement in the operating room €70
Vacuum €70
Total cost €744
NHF reimbursement: Group J37 (64 points) × €12 (per 1 point) €768
Table 7. Costs and NHF reimbursements associated with the ambulatory treatment of a chronic venous leg ulcer patient
Type of cost Value (Euro) NHF reimbursement (Euro)
Dressing material and labour (€7 material, €3 labour) = €10 Z31 (4 points) × €2 = €8
Debridement, dressing, material, and labour (€13 material, €7 labour) = €20 Z31 (4 points) × €2 = €8
Dressing with patient-provided materials (€2 material, €3 labour) = €5 Z31 (4 points) × €2 = €8
Debridement, dressing, and labour with patient-provided materials (€3 material, €7 labour) = €10 Z31 (4 points) × €2 = €8
USG Doppler examination (UDP) (€14 amortization, €12 job) = €26 W13 (13 points) × €2 = €26
Microbiological examination (€7 microbiological examination, €10 debridement and dressing with patient-provided materials) = €17
W12 (7 points) × €2 = €14
Histological examination (€8 histological examination €10 debridement and dressing with patient-provided material) = €18
Z37 (6.5 points) × €2 = €13
Compression bandages (2 pieces) €19 No reimbursement
Table 6. Costs and NHF reimbursements associated with home-based treatment (i.e., long-term nursing care)
Type of cost Value (Euro) NHF reimbursement (Euro)
Dressing, material and labour €10×16 = €160 Per person per day: €180 per month(€6 per person per day × 30 days)
16 visits per month(Minimum of four visits per week)
Dressing with patient-provided materials €5×16 = €80
Debridement, dressing, material, and labour €20×16 = €320
Debridement, dressing, and labour with patient-provided materials €10×16 = €160
Microbiological examination €7
the supervision of specialised centres, is associated with significant financial savings and improved outcomes1, 2,
7, 8, 9, 10, 11. The estimated costs reported in this paper were de-
rived from expenses incurred through public funds and the private resources of chronic wound patients and through pensions, compensations, time and expenses incurred by the patients’ families, treatments for co-morbid condi-tions, and non-contributory sick leave periods [1]. The application of modern treatment methods and the organi-sational changes that have been implemented in the new treatment system enabled debt-free treatment of patients in NHF surgical units. The new system also provided bet-
ter organisation of the patient’s stay in the unit and ensured the appropriate continuation of treatment at home. Table 5 presents the results for the costs for all necessary services during a 3-day stay on the surgical unit, as outlined in Figures 3, 4, and 5. Table 5 also presents the current methods of NHF reimbursement for these procedures.
The types of procedures that were performed in the outpatient setting under the new treatment sys-tem are described in Table 7. In the case of outpatient care, some savings were required to cover the treat-ment centres’ costs. Those savings resulted from the use of specialised dressings that were provided by the patient for each visit. Thanks to the efforts of the PTLR, some new dressings are available in Poland with a 30% reimbursement. However, this reim-bursement does not apply to modern antiseptics like octenidine, polyhexanide, and povidone-iodine. The treatment cost for outpatient conditions therefore appears to have been underestimated by the NHF. Table 6 presents the results for the costs and the NHF reimbursement amount for long-term home-based nursing care. This management approach was eco-nomically valid, particularly when the dressings were supplied by the patient.
The treatment of chronic venous leg and foot ulcers in Western Europe consumes approximately 1-2% of the total healthcare system budget, which is a significant amount given the low incidence rate of this condition12, 13, 14. Furthermore, the time spent by
EWMA Journal 2014 vol 14 no 2 12
Science, Practice and Education
3. Jawienń A.,Szewczyk M.T.,Kaszuba A. i inni. Wytyczne ekspertów w sprawie gojenia owrzodzeń ńylnych goleni Leczenie Ran 2011;8(3):59-80
4. European Wound Management Association (EWMA) Position Document: Pain at wound dressing changes. London: MEP Ltd, 2002. Available from http://www.ewma.org
5. European Wound Management Association (EWMA). Position Document: Identifying criteria for wound infection . London: MEP Ltd, 2005.
6. European Wound Management Association (EWMA). Position Document: Understanding compression therapy. London: MEP Ltd, 2003:1–17.
7. Ghauri AS, Taylor MC, Deacon JE, Whyman MR, Earnshaw JJ, Heather BP, Poskitt KR. Influence of specialized leg ulcer service on management and outcome. Br J Surg 2000;87:1048-56.
8. Rybak, G.Krasowski, P.Stepinski, A.Tukiendorf, M.Niewada. Hydrocolloid dressings in management of chronic venous leg ulcers – clinical efficacy and cost effectiveness assessment. Przeglad Flebologiczny 2003;11(1):7-11.
9. Capillas Perez R, Cabre Aguilar V, Gil Colome AM, Gaitano Garcia A, Torra I, Bou JE (2000) Comparacion de la efectividad y coste de la cura en ambiente humedo frente a la cura tradicional. Ensayo clinico en pacientes de atencion primaria con ulceras vasculares y por presion. Rev Enferm 2000;23(1):17-24.
10. Meaume S, Gemmen E. Cost-effectiveness of wound management in France: pressure ulcers and venous leg ulcers. J Wound Care 2002;11(6):219-24.
11. Kerstein MD. Unexpected economics of ulcer care protocols. South Med J 2004;97(2):135-6.
12. Allegra C. Chronic venous insufficiency: the effect of health-care reforms on the cost of treatment and hospitalisation – an Italian perspective. Curr Med Res Opin 2003;19(8):761-69.
13. De Castro Silva M. Chronic venous insufficiency of the lower limbs and its socioeconomic significance. Int Angiol 1991;10:152-7.
14. Simka M, Majewski E. The social and economic burden of venous leg ulcers. Focus on the role of micronized purified flavonoid fraction adjuvant therapy. Am J Clin Dermatol 2003;4(8):573-81.
15. Hampton S. Jobst UlcerCARE compression hosiery for venous leg ulcers. Br J Community Nurs 2004;8:279-83.
16. Oien RF, Hakansson A, Ovhed I, Hansen BU. Wound management for 287 patients with chronic leg ulcers demands 12 full-time nurses. Leg ulcer epidemiology and care in a well-defined population in southern Sweden. Scand J Prim Health Care 2000;18(4):220-5.
16TH EFORT CongressPrague, Czech Republic: 27-29 May 2015
Main Theme: InfectionHighlights in Orthopaedics & Traumatology
www.efort.org/prague2015
Abstract submission
15 Sept. - 15 Nov. 2014
Key dates Abstract submission & registration open: 15 September 2014 Abstract submission closes: 15 November 2014 Early registration deadline: 16 February 2015
#EFORT2015
EFORT_Prague_210x142_EWMA_Abstracts.indd 1 21/08/2014 17:38:59
medical staff caring for chronic wound patients is directly proportional to the chronic nature of the condition. In the United Kingdom, community nurses spend 22% of their time caring for patients with chronic lower leg wounds; in Sweden, these patients require 7% of a nurse’s time15, 16. The results of this study indicated that the new treatment system that was introduced into the Krapkowice District has resulted in chronic wound treatment cost reductions in the total healthcare system budget.
CONCLUSIONSThe implementation of a new chronic wound treatment system for chronic leg and foot ulcers (venous, ischemic, mixed, and diabetic foot) resulted in a reduction in medi-cal costs incurred by the NHF, a reduction in medical costs for the treatment of one patient, reduced hospital unit debt, and new knowledge regarding the relevance and effectiveness of home-based nursing care. However, outpatient surgical care for ulcer treatments remains un-derfunded by the NHF. m
References
1. Simka M: A comparison of the treatment costs of leg ulcers in the primary versus specialized care. Leczenie ran 2005;2(1):3-6.
2. Rybak Z., Franks P. J., Krasowski G., Kalemba J., Glinka M. Strategy for the treatment of chronic leg wounds: a new model in Poland. Int Angiol 2012;31(6):550-6.

Flexibility for body contours The unique design of Mepilex Border Flex delivers benefits to both clinicians and patients:
Optimised and less stressful healing promotes a faster recovery1,2
Unique and efficient absorption structure delivers optimal healing conditions3
Retention of exudate avoids leakage and allows less frequent changes4
Unique flex technology in the pad to enhance natural movement5
Easy and safe to wear, for the patient to feel safe and secure
References: 1. Upton D. et al. The Impact of Atraumatic Vs Conventional Dressings on Pain and Stress in Patients with Chronic Wounds. Journal of Wound Care, 2012. 4. Feili F et al. Retention capacity. Poster presentation at the EWMA conference, Lisbon, Portugal 2008. 5. Tensile force. Mölnlycke Health Care lab. report 20130301-002. 2. Upton D. et al. Pain and stress as contributors to delayed wound healing. Wound Practice and Research, 2010. 3. Fluid handling capacity. SMTL lab. report SMTL 13/4161/1.
CONTOURSCARE FOR
www.molnlycke.com Mölnlycke Health Care AB, Box 13080, SE-40252 Göteborg, Sweden. Phone +46317223000 The Mölnlycke Health Care, Mepilex® Border Flex, Safetac® names and logos are registered globally to one or more of the Mölnlycke Health Care Group of Companies. © 2014 Mölnlycke Health Care AB. All rights reserved.
Dorte P. Barrit1, Specialist nurse, Diploma of health
Hanne Birke-Sorensen1,2 MD, Ph.D., Plastic and reconstructive surgeon
1Department of Plastic Surgery, Aarhus University Hospital, Aarhus, Denmark
2Institute of Clinical Medicine, Aarhus University, Aarhus, Denmark
Correspondence: [email protected]
Conflicts of interest: None
Science, Practice and Education
INTRODUCTIONSplit thickness skin grafts (STSGs) are used to repair acute and chronic skin defects when direct closure cannot be accomplished, and a STSG is considered preferable to a surgical flap or closure by secondary intention. The wound created by harvesting the STSG – the STSG donor site – is a flat wound. A STSG donor site reepithelialises through the in-growth of keratinocytes originating from the apocrine glands and pilosebaceous units left intact in the preserved deep layer of the der-mis. A donor site can be expected to heal within 2 weeks, if complications are avoided1, 2.
A recent systematic review regarding donor site dressing found no clear evidence to support the choice of any particular dressing3. A STSG donor site is painful, so it is important to the patient that the dressing, placed over the site, reduces pain3, 4 Furthermore, it is preferable that the dressing is relatively inexpensive and easy to handle, apply, and remove5,6. It is also essential that the dress-ing is comfortable and does not hinder physical activities4,7,8. In addition to the abovementioned requirements, it is crucial that the dressing im-proves, or at least does not impair, healing at the donor site8-10. The combination of providing protection and maintaining a moist surface are the main factors that minimise wound-related discomfort3.
In 2010, it was decided that all hospitals in Re-gion Midt in Denmark should shift from one product to another for STSG dressings. In our department, we used the shift as an opportunity to conduct this clinical trial, to compare three dif-ferent donor site dressings. The original dressing was a calcium sodium alginate dressing covered with a transparent semi-occlusive polyurethane film*. The new product chosen for all hospitals in the region was also calcium sodium alginate dressing covered with transparent semi-occlusive
*Group 1: Kaltostat®, ConvaTec, covered with Stabilon®, Coloplast
**Group 2: Tegaderm alginat®, 3M, covered with Mepore film®,
Mölnlycke Health Care
*** Group 3: Aquacel®, ConvaTec, covered with Mepilex Border®,
Mölnlycke Health Care
Dressings for split thickness skin graft donor sites: A comparison of three optionsABSTRACTBackground: The management of donor sites after harvesting of split thickness skin grafts is a challenge.Aim: The aim of this study was to compare three dif-ferent dressings for split thickness skin donor sites.Methods: This study was designed as a prospective comparative study of 60 patients allocated to one of three donor site dressings groups, following harvesting of split skin. The first and second groups (n=20 for each) were treated with calcium sodium alginate dressings covered with transparent semi-occlusive films*, **, and the third group (n=20) with a hydrofi-bre dressing covered with a soft silicone foam dress-ing***. Endpoints were healing, pain, costs, and number of dressing changes. Results: No difference was found among the three groups with respect to healing and pain. Significantly more unplanned dressing changes were required in the second group (28) compared with the first and third groups (4 for each). Significantly lower total direct dressing costs were found in the first and third groups compared with the second group. The median ratios of total dressing costs were 1.13, 2.15, and 1.00 for the first through third groups, respectively. Conclusions: This study shows that two dressings, almost identically described by manufacturers, per-formed significantly differently when used clinically. The dressing with the lower per-dressing cost was the most expensive choice because of its high frequency of dressing changes.
EWMA Journal 2014 vol 14 no 2 15

polyurethane film**. A hydrofibre dressing covered with soft silicone foam dressing was chosen as a third option for evaluation in this trial***. Therefore, the aim of this study was to compare these three different dressings used on donor sites after STSG harvesting.
METHODSThe study protocol was approved by the Central Region Denmark and by the Danish Data Protection Agency, and the study was conducted in accordance with good clinical practice and ethical principles consistent with the Declara-tion of Helsinki. This was a prospective comparative study with historic allocation to three groups, based on different products used as dressings for donor sites after harvesting STSGs. Group allocation to the three groups is shown in Figure 1. The first 20 patients were included in Group 1; they were treated with calcium sodium alginate dressings covered with transparent semi-occlusive film. The next 20 patients were included in Group 2; they were also treat-ed with calcium sodium alginate dressings covered with transparent semi-occlusive film. The last 20 patients were included in Group 3; they were treated with a hydrofibre dressing covered with a soft silicone foam dressing.
All adult (>18 years old) patients hospitalised or seen in the Department of Plastic Surgery’s outpatient clinic at the Aarhus University Hospital, Aarhus C, Denmark, be-tween September 2010 and October 2011 were offered inclusion in the study if they required surgery to obtain an STSG from the anterior thigh. Only patients expected to have a donor site with an area <300 cm2 were included, to obtain donor sites suitable for comparison. All patients were informed about the study both orally and in writing by the coordinating investigator during a clinical consul-tation. Patients were excluded if they were not physically
or mentally able to cooperate, had a history of allergy to dressings, or refused to provide consent.
In the operating theatre, the STSG was harvested from the anterior aspect of the thigh of the patient using a der-matome or knife, according to standards for best practice. Immediately after split skin harvesting, the donor site was covered with adrenaline-soaked gauze (at a concentration of 1 mg adrenaline in 500 mL saline). After 10 minutes, the donor site was covered with a dressing according to the protocol and group allocation. The patients and staff could not be blinded to the chosen dressing because of the nature of the intervention and allocation in this study.
According to the protocol, the donor site dressing was left unchanged until the first clinic visit, which was planned at 8 to 10 days postoperatively unless leakage occurred (see an example of a dressing without leakage in Figure 2A). The nurses were instructed to act in accordance with the standards of the department and good clinical practice in all instances, and to report all occurrences and actions taken. The entire dressing was removed and replaced with a new dressing identical to the initial dressing (according to the treatment group), if the maximum capacity of the dressing was exceeded, leading to leakage or a high risk of leakage (see an example of a dressing with leakage in Figure 2B). The dressing was left in place and simply reinforced along the edges if there was loosening of the top layer. If infection was suspected, the dressing was changed, and if signs of infection were confirmed, the site was treated with a silver dressing, according to our standard treatment for infected STSG donor sites. At the first planned clinic visit, the percentage of healing at the donor site, as well as patient-reported pain and discomfort, were recorded. All contacts with the patient and abnormalities at the donor
Consort diagram
Figure 1: Patients included and evaluated in the three groups. Figure 2A: Group 3 dressing on the ninth day, immediately prior to its removal.
EWMA Journal 2014 vol 14 no 2 16
Science, Practice and Education
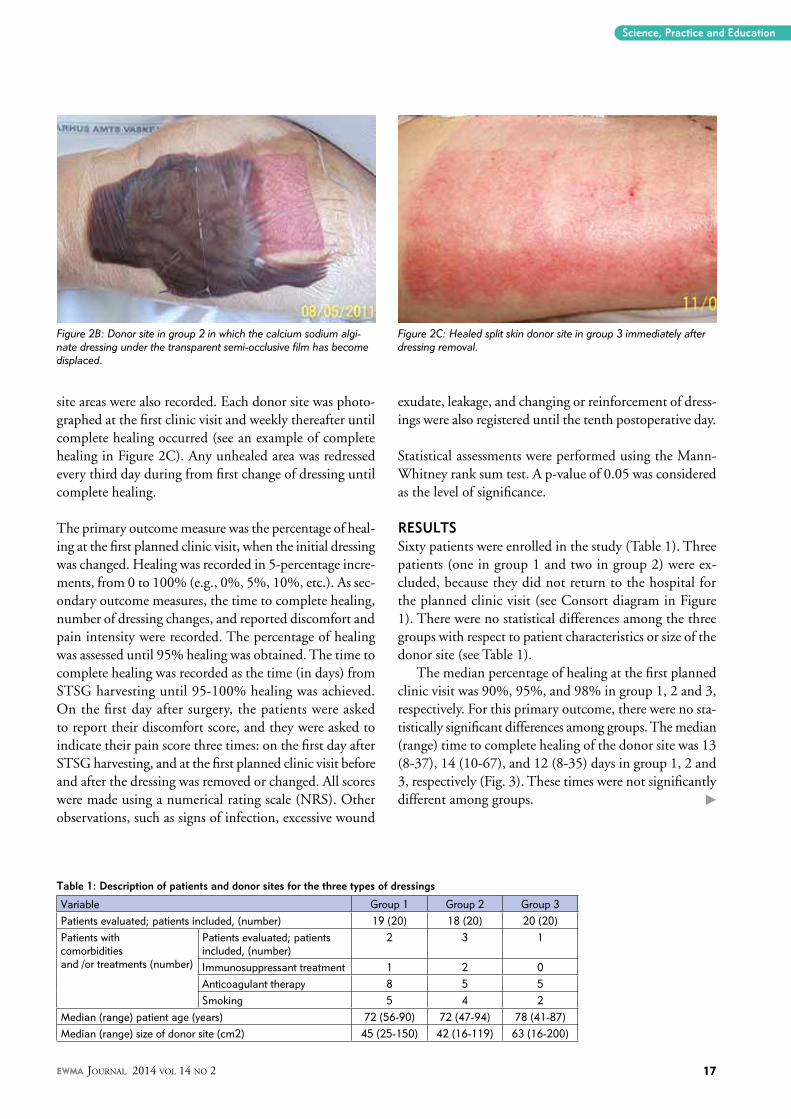
site areas were also recorded. Each donor site was photo-graphed at the first clinic visit and weekly thereafter until complete healing occurred (see an example of complete healing in Figure 2C). Any unhealed area was redressed every third day during from first change of dressing until complete healing.
The primary outcome measure was the percentage of heal-ing at the first planned clinic visit, when the initial dressing was changed. Healing was recorded in 5-percentage incre-ments, from 0 to 100% (e.g., 0%, 5%, 10%, etc.). As sec-ondary outcome measures, the time to complete healing, number of dressing changes, and reported discomfort and pain intensity were recorded. The percentage of healing was assessed until 95% healing was obtained. The time to complete healing was recorded as the time (in days) from STSG harvesting until 95-100% healing was achieved. On the first day after surgery, the patients were asked to report their discomfort score, and they were asked to indicate their pain score three times: on the first day after STSG harvesting, and at the first planned clinic visit before and after the dressing was removed or changed. All scores were made using a numerical rating scale (NRS). Other observations, such as signs of infection, excessive wound
exudate, leakage, and changing or reinforcement of dress-ings were also registered until the tenth postoperative day.
Statistical assessments were performed using the Mann-Whitney rank sum test. A p-value of 0.05 was considered as the level of significance.
RESULTSSixty patients were enrolled in the study (Table 1). Three patients (one in group 1 and two in group 2) were ex-cluded, because they did not return to the hospital for the planned clinic visit (see Consort diagram in Figure 1). There were no statistical differences among the three groups with respect to patient characteristics or size of the donor site (see Table 1).
The median percentage of healing at the first planned clinic visit was 90%, 95%, and 98% in group 1, 2 and 3, respectively. For this primary outcome, there were no sta-tistically significant differences among groups. The median (range) time to complete healing of the donor site was 13 (8-37), 14 (10-67), and 12 (8-35) days in group 1, 2 and 3, respectively (Fig. 3). These times were not significantly different among groups.
Figure 2B: Donor site in group 2 in which the calcium sodium algi-nate dressing under the transparent semi-occlusive film has become displaced.
Figure 2C: Healed split skin donor site in group 3 immediately after dressing removal.
Table 1: Description of patients and donor sites for the three types of dressings
Variable Group 1 Group 2 Group 3Patients evaluated; patients included, (number) 19 (20) 18 (20) 20 (20)Patients withcomorbiditiesand /or treatments (number)
Patients evaluated; patients included, (number)
2 3 1
Immunosuppressant treatment 1 2 0Anticoagulant therapy 8 5 5Smoking 5 4 2
Median (range) patient age (years) 72 (56-90) 72 (47-94) 78 (41-87)Median (range) size of donor site (cm2) 45 (25-150) 42 (16-119) 63 (16-200)
EWMA Journal 2014 vol 14 no 2 17

In all three groups, at least 70% of patients reported 0 or 1 out of 10 on the NRS scale regarding pain or dis-comfort at any time, and at no time was the mean score above 1.2 for any group (data not shown). There were no statistically significant differences in pain or discomfort scores among the three groups.
The number of additional, unplanned dressing changes within the first 8 to 10 days after harvesting was higher in group 2 compared with group 1 and 3 (p<0.001 for both comparisons) (Fig. 4). The number of reinforcements performed was similar in the three groups (six, five, and four reinforcements in group 1, 2 and 3 respectively). After the first 10 days, only the number of dressing changes was recorded. The total number of dressing changes was 36, 47, and 24 in group 1, 2 and 3 respectively; these numbers were not statistically different between groups.
Significantly more silver dressings were used for clini-cally identified infection at the STSG donor site in group 2 compared to group 1 and 3 (seven dressings compared to two [p<0.03] and zero [p<0.001] dressings, respectively) (Fig. 5). No systemic antibiotics were administered for donor site infection. Two patients received systemic an-tibiotic treatment for other reasons: one in group 1 and one group 2.
The direct cost of dressings used in the first 10 days af-ter STSG harvesting was significantly lower in group 1 and group 3 compared with group 2 (p<0.004 and p<0.003, respectively). The ratios of the median total dressing costs for the three groups were 1.13, 2.15, and 1.00 for group 1, 2 and 3, respectively. The ratios of the costs per dress-ing for the same three groups were 1.13, 1.00, and 1.28, respectively.
DISCUSSIONIn our study, we found no statistically significant differ-ences among the three groups with respect to the per-centage of healing at the first planned visit, total healing time, or patient-reported pain or discomfort. Yet, signifi-cant differences among the three groups were observed in
the number of dressing changes required before the first planned dressing change, number of silver dressings used, and direct costs of the dressing used (Table 2).
In a randomised controlled trial, Vaingankar et al. dem-onstrated that moist wound healing protects the wound from dehydration and contamination, promotes wound healing, and is associated with decreased levels of wound pain7. Only dressings designed to provide moist wound healing were used in this trial. Because the raw surface of the donor site produces a considerable amount of exu-date, the ideal donor site dressing must be able to deal with a large volume of exudate initially, yet still provide moist wound healing when the quantity of exudate later decreases7, 10, 11.
Many products are available that potentially or theo-retically fulfil the requirements for an optimal donor site dressing. However, none has been definitively shown to be superior to the others, and the choice of dressing currently depends on the clinician’s preferences2, 3.The healing effect of the dressing is of primary importance, but discomfort and pain caused by the donor site and dressings are also important. The choice of dressing for the donor site can have a major impact on a patient’s satisfaction and recov-ery12. Other significant considerations when choosing a STSG donor site dressing are the risk of complications, costs related to the dressing products, ease with which the dressing products can be applied and removed, and contentment of the caretakers.
The calcium alginates used in our study seem to be suitable for STSG donor sites according to the information provided by the manufacturers. Calcium sodium alginate interacts with the wound exudate, forming a gel that pro-motes a moist environment and provides a haemostatic effect. To cover the calcium sodium alginate dressing, we used a semi-occlusive transparent film. These transparent semi-occlusive polyurethane films are appropriate for this purpose, as they allow inspection without being removed and they allow exudate to evaporate through the film. A review concluded that as a primary dressing on small
Time until at least 95% healing was obtained
Figure 3: Number of days before obtaining minimum 95% healing of the donor site in the three groups.
EWMA Journal 2014 vol 14 no 2 18

donor sites, these dressings are the most comfortable for patients and allow reepithelialisation in approximately 10 days10. They have also been demonstrated to be useful when applied on top of calcium sodium alginate dress-ings13, 14. Transparent semi-occlusive polyurethane films are recommended primarily for small donor sites when used without fillers, because they have difficulty handling excessive exudate10, 15.
Another sort of filler and cover was used in group 3. The hydrofibre dressing is made of sodium carboxymeth-ylcellulose. It absorbs and interacts with wound exudate to form a hydrophilic, gas-permeable gel that traps bacteria. To cover the filler, we chose a soft silicone foam dressing. The silicone foam dressing allows evaporation like the transparent semi-occlusive polyurethane films used for the first two groups. It is not as transparent as the aforemen-tioned two films, but as it is a foam cover, it has its own absorbing and retaining capacity, which can supplement the capacity of the filler.
In our study, we found that significantly more dressing changes were performed in group 2 than in group 1, despite the calcium sodium alginate dressing being covered with transparent semi-occlusive film in both groups. According to the information regarding the absorption and evapora-
tion capacity supplied by the manufacturers, the descrip-tions of the products are almost identical, so no differences were expected. A clinical comparison between these two dressings has not been heretofore performed. There is no obvious explanation why the dressings in group 2 required more changes than those in the other groups. Suggestions might be the lower absorption capacity of the filler, inferior or lesser evaporation or adherence capacity of the dressings in group 2, or a combination of these reasons. The final test of a product is how it performs clinically, regardless of the capacity described by the manufacturers. Higgins et al. have shown in a randomised controlled trial that the time until the first unplanned dressing change was earlier, and the total number of dressing changes was greater in the group randomised to a hydrocellular foam dressing compared with a calcium sodium alginate dressing5.
Infection is the most important complication in the heal-ing of donor sites, and the ideal dressing to a donor site will reduce the risk of wound infection2, 6. As early detection of complications is essential for adequate intervention, it is likewise of importance to caretakers that the dressing does not interfere with inspection of the wound. When choosing a donor site dressing, it is also important to re-member that the donor site is caused not by a disease of
Additional dressing changes
Figure 4: Additional dressing changes performed in the three groups before the first planned dressing change.
Antibacterial silver dressings
Figure 5: Total number of antibacterial silver dressings used in the three groups before the first planned dressing change.
Table 2: Results for the three types of dressings
Variable Group 1 Group 2 Group 3Patients evaluated; patients included, (number) 19 (20) 18 (20) 20 (20)Median percentage healing at first planned dressing change (%) 90 95 98Median (range) healing time (days) 13 (8-37) 14 (10-67) 12 (8-35)Total non-planned dressing changes before first planned dressing change (number) 4 28 4Total unplanned interventions before first planned change (number)a 10 33 8Total leaks before first planned change of dressing (number) 5 18 0Relative cost per dressingb 1.13 1.00 1.28Relative total dressing costsb,c 1.13 2.15 1.00
a interventions include dressing changes and reinforcementsb dressing with the lowest cost is set at 1.00c total cost accounts for the cost per dressing and number of dressing changes
Science, Practice and Education
EWMA Journal 2014 vol 14 no 2 19

Science, Practice and Education
the patient but by a treatment of the patient, which may impact how the patient reacts to pain and discomfort at the donor site.
All donor sites clinically diagnosed as infected were covered with silver dressings according to our standard for treatment of infected donor sites. In our trial, we found a significantly larger use of silver dressing in group 2 compared to the two other groups. This means that a significantly larger number of donor sites in group 2 were assessed as being infected. As a consequence it would be less appealing in this group to let less experienced staff perform the changes of dressings, as any shift in treatment has to be based on qualified evaluation. As silver dressings are more expensive than standard dressings the change to silver dressing will on its own increase the cost of the treatment. No patients required systemic antibiotics for infection at the donor site.
In our study, the dressing was left intact for 8-10 days un-less unexpected events occurred. We found, in accordance with other studies, that it was possible to leave more than 80% of the dressings in group 1 and group 3 unchanged for 8 to 10 days without problems. In other studies of STSG donor sites, dressing protocols have involved earlier planned dressing changes3, 11. Such earlier planned changes may be beneficial, especially in group 2, as some instances of leakage might be avoided. However, a lower percentage healing would be expected at an earlier planned change, which may increase patient pain and discomfort, as well as the time and costs required for the dressing change procedure.
For the first 10 days, the ratios of the median direct total dressing costs were 1.13, 2.15, and 1.00 for group 1, 2 and 3, respectively. However, the ratios among the same groups for the per-dressing costs were 1.13, 1.00, and 1.28, respectively. The exact costs are not stated, as they will vary according to the number of appointments between the
user and provider. It is important that the cost per dress-ing, as well as the frequency of dressing changes, is low to reduce the total direct costs. In our study, group 2 had the highest total direct costs, despite the lowest cost per dressing, because of the high number of dressing changes it required. The total number of unplanned changes in group 2 was 28, whereas it was only 4 in the two other groups. In our study, we have not included indirect costs, such as nursing hours, transportation of patients, time during which patients were unfit for work, or additional outpatient visits. However, there is no indication that the indirect costs in group 2 would be smaller than in the other groups; indeed, extra dressing changes will likely increase indirect costs.
In our study, we noted the number of dressing changes after the tenth day until the total healing of the donor site, but we have not been able to obtain information regarding the exact type of dressings used after 10 days. However, the number of changes performed after the tenth day in group 1, 2 and 3 – 36, 47, and 24, respectively – provides some indications about the costs. These findings again suggest that group 2 was more expensive.
CONCLUSIONThis study shows that two dressings that appeared to be almost identical according to the manufacturers’ descrip-tions performed significantly differently in the clinical situation when used to cover a STSG donor site. The least expensive dressing on a per-dressing basis was found to be the most expensive choice because it was associated with a high frequency of dressing changes. m
Acknowledgements: The authors wish to thank the patients who volunteered in this study and colleagues who helped in completing it.
References
1. Eskes AM, Brolmann FE, Gerbens LA, Ubbink DT, Vermeulen H. Which dressing do donor site wounds need?: study protocol for a randomized controlled trial. Trial 2011;12:229.
2. Geary PM, Tiernan E. Management of split skin graft donor sites-results of a national survey. Clin Plast Surg 2012; 39(1):77-84.
3. Voineskos SH, Ayeni OA, McKnight L, Thoma A. Systematic review of skin graft donor-site dressings. Plast Reconstr Surg 2009;124(1):298-306.
4. Terrill PJ, Goh RC, Bailey MJ. Split-thickness skin graft donor sites: a comparative study of two absorbent dressings. J Wound Care 2007;16(10):433-8.
5. Higgins L, Wasiak J, Spinks A, Cleland H. Split-thickness skin graft donor site management: a randomized controlled trial comparing polyurethane with calcium alginate dressings. Int Wound J 2012;9(2):126-131.
6. Demirtas Y, Yagmur C, Soylemez F, Ozturk N, Demir A. Management of split-thickness skin graft donor site: a prospective clinical trial for comparison of five different dressing materials. Burns 2010;36(7): 999-1005.
7. Vaingankar NV, Sylaidis P, Eagling V, King C, Elender F. Comparison of hydrocellular foam and calcium alginate in the healing and comfort of split-thickness skin-graft donor sites. J Wound Care 2001;10(7):289-91.
8. Dornseifer U, Lonic D, Gerstung TI, Herter F, Fichter AM, Holm C, et al. The ideal split-thickness skin graft donor-site dressing: a clinical comparative trial of a modified polyurethane dressing and aquacel. Plast Reconstr Surg 2011;128(4):918-24.
9. Muangman P, Nitimonton S, Aramwit P. Compara-tive Clinical Study of Bactigras and Telfa AMD for Skin Graft Donor-Site Dressing. Int J Mol Sci 2011;12(8):5031-38.
10. Feldman DL, Rogers A, Karpinski RH. A prospective trial comparing Biobrane, Duoderm and xeroform for skin graft donor sites. Surg Gynecol Obstet 1991;173(1):1-5.
11. Wiechula R. The use of moist wound-healing dressings in the management of split-thickness skin graft donor sites: a systematic review. Int J Nurs Pract 2003;9(2):9-17.
12. Kaartinen IS, Kuokkanen HO. Suprathel((R)) causes less bleeding and scarring than Mepilex((R)) Transfer in the treatment of donor sites of split-thickness skin grafts. J Plast Surg Hand Surg 2011; 45(4-5):200-3.
13. Young T, Fowler A. Nursing management of skin grafts and donor sites. Br J Nurs 1998; 7(6): 324-6, 328, 330 passim.
14. Fernandes de Carvalho V, Paggiaro AO, Isaac C, Gringlas J, Ferreira MC. Clinical trial comparing 3 different wound dressings for the management of partial-thickness skin graft donor sites J Wound Ostomy Continence Nurs. 2011;38(6):643-7
15. Blome-Eberwein S, Johnson RM, Miller SF, Caruso DM, Jordan MH, Milner S, et al. Hydrofiber dressing with silver for the management of split-thickness donor sites: a randomized evaluation of two protocols of care. Burns 2010;36(5):665-72.
EWMA Journal 2014 vol 14 no 2 20

Science, Practice and Education
Jane H Davies1, BN
Jane E A Lewis2, PhD
E Mark Williams1, PhD
1Faculty of Life Sciences and Education, University of South Wales, Pontypridd, UK.
2Cardiff and Vale Universi-ty Health Board, St David’s Hospital, Cardiff, UK, Metropolitan University, Cardiff, UK.
Correspondence:[email protected]
Declared Conflict of Inter-est: JD’s PhD is part spon-sored by Huntleigh Health-care. However, the compa-ny had no part in the re-search reported, nor in the paper presented.
INTRODUCTIONThe use of the ankle brachial index (ABI) dates back to the 1950’s when Windsor was the first to compare peripheral systolic pressure with central systolic pres-sure for the purpose of identifying peripheral arterial disease (PAD)1. More than six decades later, the ABI remains the gold standard for non-invasive assessment of the arterial status of the lower limb. However, ABI has limitations, the most prominent of which relates to the artefactual elevation of arterial occlusion pressures in the lower limb, which can result in inaccurate and uninformative ABIs. This elevation can be attributed to factors such as peripheral oedema, lipodermatoscle-rosis associated with venous insufficiency, and circular arteriosclerotic lesions2. However, the most common aetiology relates to the accumulation of calcium and phosphate in the medial layer of the arterial wall, mak-ing compression of the vessel difficult. This phenom-enon is known as Monckeberg’s medial sclerosis or medial artery calcification (MAC)3. MAC is associated with advancing age and hypertension4 as well as dia-betes mellitus5 and chronic kidney disease6,7.
Experienced practitioners are usually alerted to the possibility of a falsely elevated or inaccurate ABI when the clinical presentation of the assessed limb does not correspond with the ABI result or when the audible signal emitted from a Doppler ultrasound device dur-ing the ABI measurement procedure does not cor-respond with the ABI result. A Doppler ultrasound signal indicating healthy or normal lower limb arterial flow has three distinct phases. On the other hand, a low pitched, monophasic sound indicates reduced blood flow and usually represents vessel disease. Some Doppler ultrasound devices also provide visualisation of the Doppler ultrasound waveform, which can also be analysed to determine if the waveform is triphasic, biphasic, or monophasic.
The utility of pulse volume waveforms in the identification of lower limb arterial insufficiencyABSTRACTBackground: The ankle brachial index is widely used for non-invasive assessment of lower limb arterial status, but has recognised limitations. The most significant limitation involves arterial calcification, which results in artefactually raised occlusion pressures and uninformative ankle brachial indices.Hypothesis: Analysis of the pulse volume wave-form is useful for identification of lower limb arterial insufficiency in the presence of arterial calcification.Method: Individuals (n = 1101) registered at a Welsh general practice were invited to undergo cardiovascular risk assessment. The ankle bra-chial index was measured using an automated device utilising volume plethysmography and the traditional Doppler ultrasound method.Results: Eight percent of participants (30/368) had an ankle brachial index ≥1.3, suggesting possible arterial calcification; consideration of the pulse volume waveform in these cases iden-tified possible mild peripheral arterial disease in three cases (10%). Furthermore, in one case, the ankle brachial indices were within the normal range, but the pulse volume waveforms sug-gested a moderate degree of arterial insuffi-ciency; this participant was subsequently diag-nosed with bilateral superficial femoral artery stenoses and treated accordingly.Conclusion: Pulse volume waveforms can be easily utilised as an adjunct to ankle brachial index measurement to identify patients who may benefit from further vascular assessment and intervention.
EWMA Journal 2014 vol 14 no 2 21

Pulse Volume Waveform (PVW) RecordingPVW recording constitutes a further non-invasive, diagnostic procedure that can be uti-lised to evaluate blood flow in the extremities. PVW corresponds to the phases of the cardiac cycle, with a brisk upstroke and sharp peak that occur during systole, followed by a gradual downslope that occurs in diastole (Figure 1). A reflective wave, or dicrotic notch, represents reflected blood flow.
According to Raines and Almeida8, two as-pects of the PVW require consideration for its qualitative interpretation: the contour and the amplitude of the waveforms. If, at rest, the reflected wave (dicrotic notch) is absent, this implies that the peripheral resistance distal to the point at which the recording is taken has
METHODSAs PAD is a marker of systemic atherosclerosis,10 the pri-mary aim of the PIPETTE (Peripheral Arterial Disease in Primary Care: Targeted screening and subsequent manage-ment) study was to assess cardiovascular risk by measuring the ABI. This prospective observational study was based in a South Wales (UK) General Practice. We invited 1101 individuals with at least two pre-identified cardiovascu-lar risk factors without known cardiovascular disease or diabetes mellitus to participate. Ethical approval for this study was granted by the South East Wales Research Ethics Committee (REC No: 12/WA/0075), and all participants (n = 368) provided written consent.
First, while supine, participants underwent ABI meas-urement using an automated device utilising volume plethysmography*. The device utilises dual chamber cuffs.
Figure 1: Normal PV waveform: 1) Brisk systolic upstroke, 2) Sharp systolic peak, 3) Gradual downslope, 4) Dicrotic notch.
Figure 2: PVW grading system9.
been reduced. Reduction in peripheral resistance is most often caused by proximal arterial obstruction. Waveform amplitude is a function of local pulse pressure and is re-duced with arterial occlusion proximal to the point at which the recording is taken. Therefore, the more reduced the amplitude, the greater the proximal obstruction and the poorer the local perfusion. Interpretation of PVWs can be undertaken by visually comparing them to a four-level grading system9 (Figure 2).
Until recently, PVW recording was confined to the vas-cular laboratory; however, the development of portable equipment with PVW recording capabilities has made this diagnostic technique much more amenable for use in other, non-specialist settings, such as primary care.
The aim of this study was to assess the utility of PVW recordings undertaken in a primary care setting by com-paring simultaneously recorded ABI and PVW data taken during a cardiovascular screening study.
* dopplex® ABIlity, DA100PB, Huntleigh Healthcare.
** Doppler MD2, 8 MHz, Huntleigh Healthcare.
*** Aneroid sphygmomanometer, Welch Allyn Inc.
1
2
3
4
Dicrotic Notch: NormalGood Amplitude
Absent Dicrotic Notch:Minimal-Mild PAD
1
2
3
4
Dicrotic Notch: NormalGood Amplitude
Absent Dicrotic Notch:Minimal-Mild PAD
Amplitude ReductionAbsent Dicrotic Notch:
Mild-Moderate PAD
Poor AmplitudePulse Elongation:
Moderate-Severe PAD
Severe AmplitudeReduction & Elongation:
Severe-Critical PAD
Pulse FlatlineCritical PAD
Amplitude ReductionAbsent Dicrotic Notch:
Mild-Moderate PAD
Poor AmplitudePulse Elongation:
Moderate-Severe PAD
Severe AmplitudeReduction & Elongation:
Severe-Critical PAD
Pulse FlatlineCritical PAD
Grade A: NormalSharp systolic peak with prominent dicrotic notch.
Grade B: Mildly AbnormalSharp peak, absent dicrotic notch;downslope is bowed away from baseline.
Grade C: Moderately AbnormalFlattened systolic peak, upslope and downslope time decreased and nearly equal, absent dicrotic notch.
Grade D: Severely AbnormalLow amplitude or absent pulse wawe with eqal upslope and downslope time.
EWMA Journal 2014 vol 14 no 2 22

Science, Practice and Education
For each limb, an upper chamber occludes arterial blood flow, and the lower chamber utilises pneumoplethysmog-raphy to detect returning pulsations as the pressure in the upper chamber is gradually reduced (Figure 3). This tech-nology is used to measure and calculate ABIs for both legs simultaneously. The device also records a 5-second strip of PVWs for each foot (via the lower detection chamber) that are printed out along with ABI results for analysis. Following a 5-minute rest period, the ABI was measured again, this time utilising the traditional manual method of Doppler ultrasound** and sphygmomanometry***. The Doppler ultrasound ABI measurement was performed in accordance with the evidence-based procedure recom-mended by Aboyans et al.11 All ABI measurements were performed by a qualified nurse with extensive experience in the procedures (JD). JD subsequently graded the obtained PVW record-ings according to Rumwell and McPharlin’s grading sys-tem9 (Figure 2). The PVW recordings of all PIPETTE participants were also graded by JL (Clinical Specialist Podiatrist and Therapies, Cardiff and Vale NHS trust), an experienced researcher and practitioner in this field12. The review was single-blinded as JL did not have access to participants’ clinical data or knowledge of JD’s gradings. The subsequent gradings were first reviewed to determine agreement between reviewers, and second to identify cases in which the ABI may have been artefactually raised and potentially uninformative; namely cases with an ABI ≥1.3 and cases in which the ABI and PVW did not correspond.
Figure 3: Automated ABI device dual chamber leg cuff
Figure 4: Example of a printout from an automatic ABI device showing an elevated ABI with an abnormal pulse volume waveform. A: rounded systolic peaks, B: absence of defined dicrotic notch.
Figure 5: Example showing a normal ABI but abnormal PVW suggesting that this individual may have peripheral arterial disease and that calcification may have artefactually raised the ABI to within the normal range. The PVW shows flattened systolic peaks, and the upstroke and downstroke times are decreased and nearly equal.
(n = 18). For example, participants who had undergone a previous mastectomy could not undergo bilateral brachial blood pressure measurements. Both reviewers reported the same grading for 99% of the PVW recordings (n = 673). For the 1% (n = 7) of recordings for which the reviewers did not agree, the disagreement always involved one re-viewer allocating grade A and the other grade B. Because this difference in grading also equated to disagreement regarding the PAD status of the participants, these cases were excluded from the subsequent results analysis.
An ABI of 1.3 is frequently used as a cut-off point to sig-nify when results may be artefactually high; 8% (n = 30) of the ABIs in the PIPETTE study exceeded this value. Analysis of the corresponding PVW recordings suggest-ed that 10% of these participants (n = 3) had abnormal waveforms, which were all graded B by both reviewers, suggesting the presence of mild PAD. Figure 4 shows an example of a participant with ABIs ≥1.3. However, in-spection of the corresponding PVW revealed abnormal waveforms with the absence of the dicrotic notch and rounded systolic peaks.
Both reviewers also identified a case in which although both the automatic and manual methods returned ABI results within the normal range (0.91-1.29), inspection of the PVW recordings revealed abnormal waveforms (Figure 5). Based on the abnormal PVWs, this participant was subsequently referred to a vascular surgeon for further
RESULTSThe variability between the automatic* and manual** methods of deriving the ABI was 10.1% as defined by the standard deviation of the difference in the results divided by the mean13. From 736 PVW recordings (n = 368 × 2 legs), 680 were suitable for grading. Fifty-eight recordings could not be graded because of poor quality PVW recordings (n = 28), failed measurements (n = 10), and problems associated with the automated device for various reasons
EWMA Journal 2014 vol 14 no 2 23

investigation and was found to have bilateral superficial femoral artery stenoses and subsequently underwent suc-cessful angioplasty.
DISCUSSIONThe 10.1% variability between the ABI measurements in this study matches the inter-observer variability observed between two experts (vascular laboratory technicians) who measured the ABI of 40 participants using Doppler ultra-sound (inter-observer variability = 10.1%)13. According to Nicolaï et al.,14 variability of ≤10-15% is regarded as acceptable for clinical tests.
An ABI ≥1.3 is considered to be artefactually high, and MAC is likely to be a contributing factor. MAC is frequently associated with diabetes. Thus, although diabet-ics were excluded from the PIPETTE study, the percentage of participants with elevated ABIs was surprisingly high at 8%.
When an ABI exceeds the cut-off point of 1.3, this measurement cannot be relied upon to provide an accurate indication of the arterial status of the limb. Suominen et al.15 found that a large proportion of individuals with high ABIs actually had PAD. They conducted a retrospective clinical study in which 1762 patients, who were referred to a vascular laboratory with suspicion of PAD, had their ABI and toe pressures measured via photoplethysmography. An ABI ≥1.3 was considered abnormally elevated, and a toe brachial index <0.6 was considered diagnostic of PAD. The prevalence of an elevated ABI was 8.4%, and of those, 62% had PAD according to toe pressures and digital subtrac-tion angiography. In comparison, only 10% of PIPETTE participants with an ABI ≥1.3 were likely to have had PAD as indicated by their corresponding PVW recordings. This lower rate can likely be attributed to the differing study populations. Lilly et al.16 offer an explanation for this by proposing that some individuals have elevated ABIs due to an increased pulse pressure amplitude rather than MAC; this constitutes a benign form of elevated ABI.
Hence, when the ABI is elevated, practitioners must be able to utilise alternative strategies to determine if the arterial status of the limb is compromised. Experienced practitioners are likely able to make this judgement based on the nature of the audible Doppler signal and the clini-cal presentation of the patient. However, whether less experienced, non-specialist practitioners, such as novice community nurses, would have the knowledge, skills, and confidence to make such a judgement, is less clear. A study by Davies et al.17 highlighted that practitioners based in general practices in Wales experience issues with several practical and theoretical aspects of the ABI measurement procedure.
The PIPETTE study also highlighted that MAC can some-times falsely elevate the ABIs of PAD patients to within the accepted normal range (0.9-1.29). Such patients must be identified promptly to ensure timely referral for further investigation and intervention. Subsequent optimisation of the arterial status of the limb will of course have ben-eficial effects for wound healing. An inexperienced nurse may have used the normal ABI results in the described case as an indication to apply compression and may have then failed to identify that the patient required further investigation. Inspection of the PVW provides a simple method of identifying such patients. Use of the PVW recording is recommended by both the European Society of Cardiology10 and the American College of Cardiology/American Heart Association18 as a second-level assessment tool for patients with suspected PAD. Thus, the PVW can be utilised to establish an initial diagnosis of lower extremity PAD.
Advantages of PVW recordingsAn added advantage of PVW recordings that is particu-larly pertinent to wound care relates to the fact that these recordings represent the sum of all blood flow through the examined area. Hence, a patient with a significant obstruction to blood flow in one or more arteries, but good collateral blood flow may have a normal waveform. This could be useful in assessing whether a lower extrem-ity wound has sufficient arterial blood supply to facilitate healing. Furthermore, the process of obtaining a PVW does not require operator skill and merely involves the application of a cuff to the foot or ankle; the device then automatically inflates, obtains, and displays the PVW. In contrast, the process of obtaining a Doppler waveform is operator dependent because a Doppler probe must be carefully positioned over an artery at a specific angle and pressure. Results can vary according to the Doppler angle used19.
Limitations of PVW recordingsPVW recording has recognised physiological limitations. First, the PVW depends on peripheral blood flow and thus, may be influenced by factors other than vessel pat-ency such as sympathetic nerve input20. Second, severe congestive heart failure may also slow blood flow and mimic inflow disease8. Third, the PVW represents the total blood flow through the area being assessed, and therefore, cannot provide accurate diagnostic informa-tion regarding where and to what extent a specific artery is diseased. A further limitation of PVW recordings involves susceptibility to interference from factors such as patient movement, which can result in artefact in the detection signal and subsequent poor quality PVW recordings. This can sometimes be addressed with repeated measurements
EWMA Journal 2014 vol 14 no 2 24

after repositioning the patient and reminding him or her of the importance of remaining still during the procedure.
Study LimitationsAlthough this study demonstrated that reviewers with considerable experience in interpreting PVW recordings agreed on the identification of apparently abnormal PVW recordings, this may not necessarily apply to practitioners less experienced at the task. Furthermore, the majority of obtained PVW gradings were not verified by comparison with a superior diagnostic modality such as Duplex ultra-sound scanning.
CONCLUSIONSThis study highlighted the shortcomings of the ABI as a single diagnostic tool and demonstrated the need for a secondary mode of lower limb arterial assessment that is also easy for non-specialist practitioners to use. PVW recordings may be acceptable for fulfilling this role and may, thus, be particularly useful in the field of wound management. m
References
1. Windsor, T. Influence of arterial disease on the systolic blood pressure gradients of the extremity. Am J Med Sci 1950;220:117-126.
2. Kröger, K., Stang, A., Kondratieva, J., Moebus, S., Beck, E. et al. Prevalence of peripheral arterial disease - results of the Heinz Nixdorf recall study. Eur J Epidemiol 2006;21:279-85.
3. Rocha-Singh, K. J., Zeller, T. & Jaff, M. R. Peripheral arterial calcification: Prevalence, mechanism, detection and clinical implications. Catheter Cardiovasc Interv 2014;83(6):e212-20.
4. Hirsch, A. T., Haskal, Z. J., Hertzer, N. R., Bakal, C. W., Creager, M. et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circ 2006;113: e463-e654.
5. Formosa, C., Cassar, K., Gatt, A., Mizzi, A., Mizzi, S. et al. Hidden dangers revealed by misdiagnosed peripheral arterial disease using ABPI measurement. Diabetes Res Clin Pract 2013;102:112-16.
6. Nitta, K. Vascular calcification in patients with chronic kidney disease. Ther Apher Dial 2011;15:513-21.
Implications for Clinical PracticeThis study highlighted that:n The prevalence of an elevated ABI (≥1.3) is
relatively high even in a population in which diabetics were excluded.
n The ABIs of patients with PAD can some-times be artefactually raised to within normal limits.
n In such cases, simple analysis of PVW record-ings is a useful adjunct for the identification of patients who require further vascular inves-tigation.
Further ResearchFurther research should investigate the utility of PVW recordings by examining the associated sen-sitivity for detecting PAD or specificity for ruling out PAD. Further investigation is also required to determine the ease of use and the cost and training required to achieve reliable results.
Acknowledgements This study was undertaken as part of JD’s PhD, which is funded by a Knowledge Economy Skills Scholarship (KESS). This is a major European Convergence programme led by Bangor University on behalf of the HE sector in Wales. Benefiting from European Social Funds (ESF), KESS supports collaborative research projects (in this case, University of South Wales and Huntleigh Healthcare).
7. Mizobuchi, M., Towler, D. & Slatopolsky, E. Vascular calcification: the killer of patients with chronic kidney disease. J Am Soc Of Nephrol 2009;20:1453-64.
8. Raines, J. K., Almeida, J. I. Pulse volume recording in the diagnosis of peripheral vascular disease. In: Aburahma, A. F. & Bergan, J. J. (eds.). Noninvasive peripheral arterial diagnosis. 3rd Ed. London: Springer-Verlag Limited; 2010:39-46.
9. Rumwell, C., Mcpharlin, M. 1998. Arterial evalua-tion. In: Vascular Technology. California: Davies publishing Inc.; 1998:60-9.
10. Tendera, M., Aboyans, V., Bartelink, M. L., Baumgartner, I., Clement, D. et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries * The Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur Heart J 2011;32(22):2851-906.
11. Aboyans, V., Criqui, M. H., Abraham, P., Allison, M. A., Creager, M. A. et al. Measurement and interpre-tation of the ankle-brachial index: a scientific statement from the american heart association. Circ 2012;126:2890-2909.
12. Lewis, J. E. A. & Owens, D. R. The pulse volume recorder as a measure of peripheral vascular status in people with diabetes mellitus. Diabetes Technol & Ther 2010;12:75-80.
13. Van Langen, H., Van Gurp, J. & Rubbens, L. Interobserver variability of ankle-brachial index measurements at rest and post exercise in patients with intermittent claudication. Vasc Med 2009;14:221-26.
14. Nicolaï, S. P., Kruidenier, L. M., Rouwet, E. V., Bartelink, M. L., Prins, M. H. et al. Ankle brachial index measurement in primary care: are we doing it right? Br J of Gen Pract 2009;59:422-27.
15. Suominen, V., Rantanen, T., Venermo, M., Saarinen, J. & Salenius, J. Prevalence and risk factors of PAD among patients with elevated ABI. Eur J Vasc Endovasc Surg 2008;35:709-14.
16. Lilly, S. M., Jacobs, D. R., Jr., Kronmal, R., Bluemke, D. A., CRIQUI, M. et al. Arterial compliance across the spectrum of ankle-brachial index: the multiethnic study of atherosclerosis. Atherosclerosis 2014;233:691-6.
17. Davies, J. H., Kenkre, J. & Williams, E. M. Current utility of the ankle-brachial index (ABI) in general practice: implications for its use in cardiovascular disease screening. BMC Fam Pract 2014;15:69.
18. Anderson, J. L., Halperin, J. L., Albert, N. M., Bozkurt, B., Brindis, R. G. et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommenda-tions): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013;127:1425-43.
19. Aburahma, A. F., Jarrett, K. S. Segmental Doppler pressures and Doppler waveform analysis in peripheral vascular disease of the lower extremities. In: Aburahma, A. F. & Bergan, J. J. (eds.). Noninva-sive peripheral arterial diagnosis. 3rd Ed. London: Springer-Verlag Limited; 2010:25-38.
20. Weinburg, I. 2010. Vascular Medicine. Available at: http://www.angiologist.com/vascular-laboratory/pulse-volume-recording/ [Accessed 27/03/14].
The research team also acknowledges the support of the National Institute for Health Research through the comprehensive clinical research network.
The authors thank Cwm Taf University Health Board for their support and Professor Jonathan Richards for hosting the study at Morlais Medical Practice, Merthyr Tydfil.
Science, Practice and Education
EWMA Journal 2014 vol 14 no 2 25

New and improved
The Coloplast logo is a registered trademark of Coloplast A/S. © [YYYY-MM.] All rights reserved Coloplast A/S, 3050 Humlebæk, Denmark.
Enjoy the freedom of superior absorption
The new Biatain Silicone and Biatain Silicone Lite combine superior absorption and a secure fit
· With the new design we introduce a perforated, soft silicone adhesive wound contact layer, which delivers a secure fit without compromising superior absorption.
· The unique Biatain foam still conforms closely to wound bed ensuring superior absorption and an optimal moist wound healing environment.
· Safe and easy application due to 3-piece non-touch opening.
· Biatain Silicone and Biatain Silicone Lite are foam dressings that can be used on a wide range of exuding wounds.
BiatainSilicone Lite– superior absorption with soft adhesion for increased mobility
Biatain Silicone – superior absorption with soft adhesion for general purposes

Jose M Corrales, MSN
Nuria P Gayo, BSN
Mª del Carmen P Águila, MSN
Almudena M Martín, BSN
Ana Ribeiro, SF, PhD
Fundación Instituto San José – Orden Hospitalaria de los Hermanos de San Juan de Dios. Department of Nursing, Madrid, Spain
Correspondence:[email protected]
Conflicts of interest: None
Science, Practice and Education
INTRODUCTIONUndernutrition or malnutrition is a serious problem that leads to important economic and social health issues1, and is one of the most frequent causes of mor-tality and one of the main health problems worldwide. Very often, malnutrition affects patients admitted to the hospital, where disability and disease are frequent, and in this case it is known as hospital malnutrition2. The most widely accepted definition of malnutrition was proposed by Elia et al in 2005: “A state of nutri-tion in which a deficiency or excess (or imbalance) of energy, protein and other nutrients causes measurable adverse effects on tissue/body structure and function and on clinical outcome”3.
Patients admitted to the hospital can have a deterio-rated nutritional status due to multiple factors: their acute illness, fasting required for multiple diagnostic and therapeutic procedures they need to undergo, the change from their usual diet to hospital food, and the temperature and presentation of institutional food4.
Malnutrition can be classified as: caloric malnutrition, protein malnutrition or mainly protein malnutrition, mixed malnutrition, and deficiency states. Caloric malnutrition is a type of chronic malnutrition caused by the lack or prolonged loss of energy and nutrients. Significant weight loss occurs, characterised by loss of adipose tissue, loss of muscle mass to a lesser extent, and no significant abnormality in visceral protein or oedema status. Anthropometric parameters show ab-normalities, and the albumin and plasmatic protein values are usually normal or very close to normal rang-es. Protein malnutrition or mainly protein malnutri-tion is a type of acute malnutrition due to stress that occurs when there is a decreased protein intake and an increased protein requirement in serious infections, multiple trauma, and major surgery. The adipose tis-sue is preserved, and the main problem is protein loss, specifically visceral protein loss. Anthropometric pa-rameters can be within normal limits with low visceral
ABSTRACTIntroduction: Malnutrition is a frequent compli-cation in institutionalised patients. Malnutrition consequences that contribute to poor outcome include the emergence or worsening of chronic wounds and increased functional dependence.Objectives: To describe the nutritional status of hospitalised patients and assess the evolution of their nutritional status during their hospital stay until discharge. Methods: Prospective observational study of patients admitted to a medium/long term care unit for 6 months. Clinical socio-demographic variables and instrument data were collected to perform the Mini Nutritional Assessment (MNA). Results: Seventy-six patients (mean age 78.13±11.31 years-old) were enrolled. Of these, 63.2% of patients were admitted to hos-pital for continued care and 36.8% were admit-ted for rehabilitation, with the most common diagnoses being: immobility syndrome (21.1%), respiratory conditions (17.1%), hip fracture (15.8%), and pressure ulcers (15.8%).Of the total cohort, 80.3% had multiple chronic condi-tions, total functional dependence, and moder-ate-to-high risk of developing pressure ulcers. By assessing nutritional status, 77.6% of the sample was malnourished and 22.4% were at risk of malnutrition at admission. Finally, 52.7% were discharged home at the end-of-care period. Of those, 17.1% had a normal nutri-tional status, 14.5% had risk of malnutrition, and 21.1% were malnourished. Conclusions: This study demonstrated that there is a high prevalence of malnutrition in elderly patients hospitalised for medium/long-term care for >6 months. We justify the need to adopt measures against malnutrition to improve the general health of our patients.
The importance of using a nutritional risk analysis scale in patients admitted to continued care
adrid · Spain
EWMA n GNEAUPP 2014
Submitted to the EWMA Journal, based on a pres-entation given a free paper session (Free paper session: Miscellaneous I) at the EWMA - GNEAUPP 2014, Madrid.
EWMA Journal 2014 vol 14 no 2 27

proteins. Mixed malnutrition is a type of protein-calorie malnutrition that mixes the characteristics of the two pre-vious conditions, and decreases lean mass, fat, and visceral proteins. Mixed malnutrition affects patients with previous chronic malnutrition that undergo some kind of acute process causing stress (e.g., surgery or infections). This kind of malnutrition is the most common type observed in the hospital setting. Deficiency states are an isolated nutritional deficiency (trace elements or vitamins), and they are due to a decreased intake or increased loss, and is usually associated with some of the malnutrition types described above2.
Malnutrition affects 30-50% of hospitalised patients of all ages, and its prevalence increases as the hospital stay is extended2. On its own, malnutrition is considered a geriatric syndrome with variable incidence depending on the diagnostic method and the research setting. This prevalence varies between 3.7-17% in non-institution-alised persons5,6, 7.7-26.8% in patients living in nurs-ing homes7, 22-57.1% in hospitalised patients4,8,9, and 14.7-23% in patients included in Home-Based Primary Care programmes10. Despite its high prevalence, this pa-thology often goes unnoticed by healthcare professional due to the lack in training or motivation with regards to nutritionally assessing patients, or because it is considered a minor issue1.
Malnutrition is considered one or the internal factors that promote pressure ulcers PU development, one of the most frequent complications of immobilised patients with a prevalence of 74%11,12. Several studies confirmed that malnutrition is directly linked to the incidence and seriousness of Pus13-15. Reduced calorie intake, dehydra-tion, and reduced serum albumin can impair the skin and its underlying tissue tolerance to pressure, friction, and shearing forces. This leads to an increased risk of skin breakdown and reduced tissue regeneration capacity12.
Given the above considerations, it is important to assess the nutritional status and identify possible risk factors for malnutrition in hospitalised patients. It is crucial to make an early malnutrition diagnosis to implement preventive and therapeutic measures that improve patient quality-of-life, while reducing both the occurrence of associated conditions and of hospital admissions. The aims of this study were to: 1) describe the nutritional status of patients admitted
to the special care unit; 2) assess whether there are associations between the
nutritional status at admission and the type of admission programme, reason for admission, and dependence level in daily life activities; and
3) study the evolution of patient nutritional status during their hospital stay until discharge.
METHODSA prospective observational study was performed in a spe-cial care unit of a medium- to long-stay social health centre that provides long-term care and functional rehabilitation programmes. Patients admitted between June-November 2013 were included in the study.
The following variables were collected within the first 24 hours of admission: age, sex, type of admission programme, reason for admission, multiple conditions, medical history, and the type and origin of any chronic wound(s). Barthel index (BI) and Braden scale were meas-ured at admission and at discharge. The BI, which assesses disability in patients, is an ordinal scale comprised of 10 daily living activities (bathing, grooming, ascending and descending stairs, bladder and bowel management, dress-ing, feeding, toilet use, transfers, and walking)16. With the exception of bladder and bowel management, a maxi-mum score means that the patient is fully independent in performing that activity. The scores of the 10 items are summed to a maximum possible score of 100 (inde-pendent) and minimum of 0 (totally dependent)16. The Braden scale, which assesses a patient’s risk of developing a pressure ulcer, is based on a summated rating scale of the following six indicators, each scored on a scale of 1-3 or 1-4, for a total score that ranges from 6-23: sensory percep-tion, moisture, activity, mobility, nutrition, and friction or shear17. A lower Braden scale score indicates a lower level of functioning and therefore a higher risk of developing a pressure ulcer. Conversely, a score of 19 or higher indicates that the patient is at low risk of developing a pressure ulcer and does not require treatment17.
To assess malnutrition risk, anthropometric data such as weight, height, and body mass index (BMI, mass in kg/height in m2) were gathered. All patients were assessed using the Mini Nutritional Assessment (MNA), a nutri-tional screening and assessment tool used to identify pa-tients at risk of malnutrition18.The MNA was divided into screening and assessment parts. If the respondent scored 11 or less on the screening part, the assessment questions were asked. If the respondent scored 12 or more on the screening portion, he/she was considered to be in normal nutritional state and the assessment part was omitted. The screening and assessment scores were added to obtain the total malnutrition indicator score (maximum 30 points). A final score of greater than 23.5 points indicated a nor-mal nutritional state, a score ranging from 17 to 23.5 points indicated a possible malnutrition, and a score below 17 points indicated the patient was malnourished.18 The MNA detects risk of malnutrition more specifically and accurately (sensitivity 90%, specificity 88%)19 than other nutritional assessment instruments18,20,21.
EWMA Journal 2014 vol 14 no 2 28

Science, Practice and Education
To ensure voluntary participation, patients were asked to provide written informed consent form after admission (as part of the centre’s protocol), which authorised use of their clinical data. All admitted patients agreed to participate in the study and complete the examination. The study was approved by the Ethics Research Committee of the health centre and conformed to the tenets of the Declaration of Helsinki.
Data was collected from medical history records using IBM Cognos Connection 10.1.1. software (IBM Corp., Armonk, NY). Statistical analyses were performed using
SPSS® v.19 statistical software (IBM/SPSS Inc., Chicago, IL). Descriptive analyses were presented as the mean ± standard deviation. Absolute and relative frequencies were presented for quantitative variables. Comparison of patient classification according to nutritional status was performed using chi-squared tests for qualitative and independent variables. Statistical significance was set at p<0.05.
RESULTSIn the time period of this study, 76 patients were enrolled with an average age of 78.13±11.3 years (39 men/37 wom-en). Of these, 48 patients were admitted for continued/extended care and 28 were admitted for a functional re-habilitation programme. The most common reasons for admission were: immobility syndrome (21.1%), respira-tory conditions (17.1%), hip fracture (15.8%), pressure ulcer (15.8%), and tumors (13.2%) (Table 1). At baseline, 80% of patients had multiple chronic conditions. The most common medical history components were hyper-tension, cardiovascular conditions, respiratory conditions, and diabetes (Table 1).
Regarding patient dependence levels, 51.3% were fully dependent, 30.3% were severely dependent, and 18.54% were moderately to slightly dependent. Risk of PU devel-opment measured by the Braden scale revealed that 39.5% had a high risk of developing a PU, 22.4% of patients had a moderate risk, and 38.2% of patients had a slight risk. Data scrutiny indicated that 56.6% of patients had a least one chronic ulcer, of which 44.7% were PUs, 9.2% were vascular ulcers, and 2.6% were moisture-related injuries. Of the patients with PU, 79.4% showed malnutrition and 20.6% showed risk of malnutrition.
According to the baseline MNA results, 22.4% of the sam-ple showed risk of malnutrition and 77.6% showed overt malnutrition. Of the total cohort, 36 patients (47.3%) died or were referred to a different hospital before study completion, and40 patients (52.7%) were discharged to home. Of the 40 home-discharged patients, 13 had normal nutritional status, 11 had risk of malnutrition, and 16 had malnutrition (Fig. 1). There was a statistically significant difference in the nutritional state at the time of admission versus the time of discharge (p=0.007).
We did not find statistically significant differences with other variables, such as the reason for admission (p=0.291) or the admission programme type (p=0.102). However, there was a statistically significant relationship between malnutrition and dependence in daily life activi-ties (p=0.004).
Table 1.Patient demographic and clinical data
Variable Patients, N=76
Sex1 Male 39 (51.3%)
Female 37 (48.7%)
Age, years2 78.13±11.31
Reason for admission1
Immobility syndrome 16 (21.1%)
Pressure ulcer 12 (15.8%)
Hip fracture 12 (15.8%)
Tumors 10 (13.2%)
Respiratory conditions 13 (17.1%)
Acute cerebrovascular accident 5 (6.6%)
Sepsis 7 (9.2%)
Severe cerebral damage 1 (1.3%)
Multiple chronic condi-tions1
Diabetes 24 (31.6%)
Hypertension 55 (72.4%)
Cardiovascular conditions 56 (73.7%)
Respiratory conditions 26 (34.2%)
Dementia 13 (17.1%)1 Scores: Absolute and relative (%) frequencies.2 Scores: mean±SD.
Figure 1: Classification of the nutritional status of the patients includ-ed in this study as a result of the Mini Nutritional Assessment (MNA) at admission and discharge.
0
17
59
13 11 16
0
10
20
30
40
50
60
70
Normal nutritional state
Risk of malnutrition
Malnutrition
MNA at admission
MNA at discharge
Patie
nts,
n
Figure 1- Classification of the nutritional status of the patients included in this study as a result of the Mini Nutritional Assessment (MNA) at admission and discharge.
EWMA Journal 2014 vol 14 no 2 29
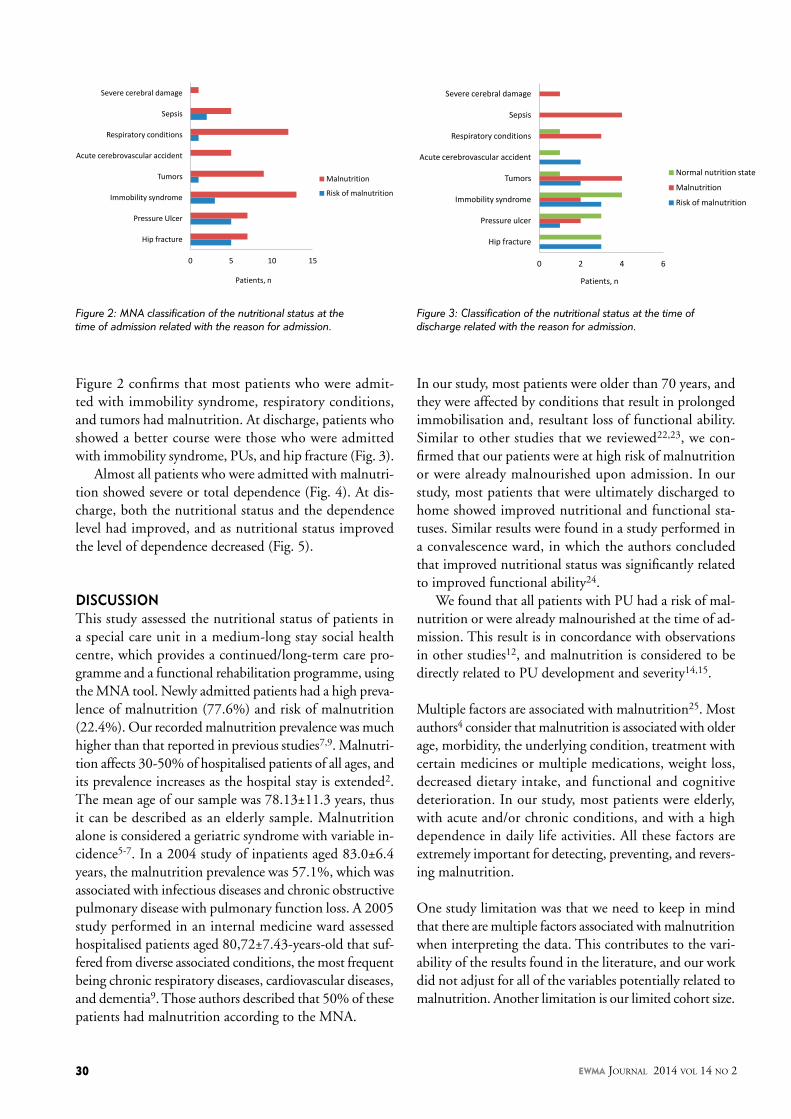
Figure 2 confirms that most patients who were admit-ted with immobility syndrome, respiratory conditions, and tumors had malnutrition. At discharge, patients who showed a better course were those who were admitted with immobility syndrome, PUs, and hip fracture (Fig. 3).
Almost all patients who were admitted with malnutri-tion showed severe or total dependence (Fig. 4). At dis-charge, both the nutritional status and the dependence level had improved, and as nutritional status improved the level of dependence decreased (Fig. 5).
DISCUSSIONThis study assessed the nutritional status of patients in a special care unit in a medium-long stay social health centre, which provides a continued/long-term care pro-gramme and a functional rehabilitation programme, using the MNA tool. Newly admitted patients had a high preva-lence of malnutrition (77.6%) and risk of malnutrition (22.4%). Our recorded malnutrition prevalence was much higher than that reported in previous studies7,9. Malnutri-tion affects 30-50% of hospitalised patients of all ages, and its prevalence increases as the hospital stay is extended2. The mean age of our sample was 78.13±11.3 years, thus it can be described as an elderly sample. Malnutrition alone is considered a geriatric syndrome with variable in-cidence5-7. In a 2004 study of inpatients aged 83.0±6.4 years, the malnutrition prevalence was 57.1%, which was associated with infectious diseases and chronic obstructive pulmonary disease with pulmonary function loss. A 2005 study performed in an internal medicine ward assessed hospitalised patients aged 80,72±7.43-years-old that suf-fered from diverse associated conditions, the most frequent being chronic respiratory diseases, cardiovascular diseases, and dementia9. Those authors described that 50% of these patients had malnutrition according to the MNA.
In our study, most patients were older than 70 years, and they were affected by conditions that result in prolonged immobilisation and, resultant loss of functional ability. Similar to other studies that we reviewed22,23, we con-firmed that our patients were at high risk of malnutrition or were already malnourished upon admission. In our study, most patients that were ultimately discharged to home showed improved nutritional and functional sta-tuses. Similar results were found in a study performed in a convalescence ward, in which the authors concluded that improved nutritional status was significantly related to improved functional ability24.
We found that all patients with PU had a risk of mal-nutrition or were already malnourished at the time of ad-mission. This result is in concordance with observations in other studies12, and malnutrition is considered to be directly related to PU development and severity14,15.
Multiple factors are associated with malnutrition25. Most authors4 consider that malnutrition is associated with older age, morbidity, the underlying condition, treatment with certain medicines or multiple medications, weight loss, decreased dietary intake, and functional and cognitive deterioration. In our study, most patients were elderly, with acute and/or chronic conditions, and with a high dependence in daily life activities. All these factors are extremely important for detecting, preventing, and revers-ing malnutrition.
One study limitation was that we need to keep in mind that there are multiple factors associated with malnutrition when interpreting the data. This contributes to the vari-ability of the results found in the literature, and our work did not adjust for all of the variables potentially related to malnutrition. Another limitation is our limited cohort size.
Figure 3: Classification of the nutritional status at the time of discharge related with the reason for admission.
0 2 4 6
Hip fracture
Pressure ulcer
Immobility syndrome
Tumors
Acute cerebrovascular accident
Respiratory conditions
Sepsis
Severe cerebral damage
Normal nutrition state
Malnutrition
Risk of malnutrition
Patients, n
Figure 3- Classification of the nutritional status at the time of discharge related with the reason for admission.
Figure 2: MNA classification of the nutritional status at the time of admission related with the reason for admission.
0 5 10 15
Hip fracture
Pressure Ulcer
Immobility syndrome
Tumors
Acute cerebrovascular accident
Respiratory conditions
Sepsis
Severe cerebral damage
Malnutrition
Risk of malnutrition
Patients, n
Figure 2- MNA classification of the nutritional status at the time of admission related with the reason for admission.
EWMA Journal 2014 vol 14 no 2 30

Science, Practice and Education
Implications for clinical practiceThis study demonstrated a high prevalence of malnutrition in elderly patients admitted to a long-term care unit, and its asso-ciation with pressure ulcer incidence and level of patient de-pendence. These data justify the need to adopt measures that assess and address malnutrition to improve the general health of our patients. Nutritional status should be routinely assessed upon admission. It would be convenient to standardise using
Figure 4: Classification of the nutritional status at the time of admission as assessed with the Barthel Index.
Figure 5: Classification of the nutritional status at discharge as assessed with the Barthel Index.
0
5
10
15
20
25
30
35
40
Completely dependent
Severely dependent
Moderately dependent
Slightly dependent
Risk of malnutrition
Malnutrition
Patie
nts,
n
Figure 4-Classification of the nutritional status at the time of admission as assessed with the Barthel Index. Figure 5-Classification of the nutritional status at discharge as assessed with the Barthel Index.
0 1 2 3 4 5 6 7 8
Completely dependent
Severely dependent
Moderately dependent
Slightly dependent
Independent
Normal nutrition state Risk of malnutrition
Malnutrition
Patie
nts,
n
References
1. Perdomo Pérez E, Navarro Vázquez FJ, González de la Torre H, Mosquera Fernández A. Cribado nutricional en pacientes inmovilizados del Servicio de Atención Domiciliaria de una zona básica de salud del área de Salud de Gran Canaria. Gerokomos. 2012;23(3):118-22.
2. Álvarez J, Río JD, Planas M, García Peris P, García de Lorenzo A, Calvo V, et al. Documento SENPE-SEDOM sobre la codificación de la desnutrición hospitalaria. Nutr Hosp. 2008;23(6):536-40.
3. Elia M, Zellipour L, Stratton RJ. To screen or not to screen for adult malnutrition? Clin Nutr. 2005;24(6):867-84.
4. García Duque S, Pérez Segura G, Sanavia Morán E, Juanes Pardo JRd, Arrazola Martínez MP, Resines Erasun C. Control nutricional en pacientes de traumatología. Nutr Hosp. 2008;23(5):493-9.
5. Morillas J, García-Talavera N, Martín-Pozuelo G, Reina AB, Zafrilla P. Detección del riesgo de desnutrición en ancianos no institucionalizados. Nutr Hosp. 2006;21(6):650-6.
6. De la Montaña Miguélez J, Areal Salve C, Míguez Bernárdez M. Evaluación del riesgo nutricional mediante el MNA en una población anciana no institucionalizada. Arch Lat Nutr. 2009;59(4):390-5.
7. Hernández Mijares A, Royo Taberner R, Martínez Triguero ML, Graña Fandos J, López García A, Morales Suárez-Varela MM. Prevalencia de malnutrición entre ancianos institucionalizados en la Comunidad Valenciana. Med Cli. 2014;117(8):289-94.
8. Ramos Martínez A, Asensio Vegas A, Núñez Palomo S, Millán Santos I. Prevalencia y factores asociados a malnutrición en ancianos hospitalizados. An Med Interna. 2004;21(6):9-18.
simple and validated nutritional screening tools, such as the Mini Nutritional Assessment, to systematically detect malnutrition or risk of malnutrition in hospitalised patients. This approach would enable health care professionals to introduce early-stage nutri-tional support for malnourished patients. This would ensure proper nutrition and reduce associated complications such as pressure ulcers.
9. Gómez Ramos MJ, González Valverde FM, Sánchez Álvarez C. Estudio del estado nutricional en la población anciana hospitalizada. Nutr Hosp. 2005;20(4):286-92.
10. Rodríguez-Martín A, Novalbos-Ruiz JP, Jiménez-Rodríguez A, Baglietto Ramos M, Romero Sánchez JM, . Implicaciones de la desnutrición en atención primaria. Nutr Hosp. 2010;25:67-79.
11. Ramos A, Ribeiro ASF, Martín A, Vázquez M, Blanco B, Corrales JM, et al. Prevalencia de úlceras por presión en un centro sociosanitario de media-larga estancia. Gerokomos. 2013;24(1):36-40.
12. Breslow R. Nutritional status and dietary intake of patients with pressure ulcers: review of research literature 1943 to 1989. Decubitus. 1991;4(1):16-21.
13. Berlowitz DR, Wilking SV. Risk factors for pressure sores. A comparison of cross-sectional and cohort-derived data. J Am Geriatr Soc. 1989;37(11):1043-50.
14. Bergstrom N, Braden B. A prospective study of pressure sore risk among institutionalized elderly. J Am Geriatr Soc. 1992;40(8):747-58.
15. Thomas DR. The role of nutrition in prevention and healing of pressure ulcers. Clin Geriatr Med. 1997;13(3):497-511.
16. Sainsbury A, Seebass G, Bansal A, Young JB. Reliability of the Barthel Index when used with older people. Age Ageing. 2005;34(3):228-32.
17. Bergstrom N, Braden BJ, Laguzza A, Holman V. The Braden Scale for Predicting Pressure Sore Risk. Nurs Res. 1987;36(4):205-10.
18. Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, et al. The Mini Nutritional
Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. 1999;15(2):116-22.
19. Young AM, Kidston S, Banks MD, Mudge AM, Isenring EA. Malnutrition screening tools: comparison against two validated nutrition assessment methods in older medical inpatients. Nutrition. 2013;29(1):101-6.
20. Ocón Bretón MJ, Altemir Trallero J, Mañas Martínez AB, Sallán Díaz L, Aguillo Gutiérrez E, Gimeno Orna JA. Comparación de dos herramientas de cribado nutricional para predecir la aparición de complica-ciones en pacientes hospitalizados. Nutr Hosp. 2012;27(3):701-6.
21. Cereda E. Mini nutritional assessment. Curr Opin Clin Nutr Metab Care. 2012;15(1):29-41.
22. Jiménez Sanz M, Sola Villafranca JM, Pérez Ruiz C, Turienzo Llata MJ, Larrañaga Lavin G, Mancebo Santamaría MA, et al. Estudio del estado nutricional de los ancianos de Cantabria. Nutr Hosp. 2011;26(2):345-54.
23. Sandoval L, Heredia UPC, Varela L, Heredia UPC. Evaluación del estado nutricional de pacientes adultos mayores ambulatorios. Rev Med Hered. 1998;9(3):104-8.
24. Arellano Pérez M, Miralles Basseda R, Cervera Alemany AM, García Caselles MP, Márquez Lorente MÁ, Vázquez Ibar O. Valoración del estado nutricional en una unidad de convalecencia: evaluación inicial y seguimiento. Rev mult ger. 2004;14(5):258-261.
25. Micklewright A. Nutritional status at submission for dietetic services and screening for malnutrition at admission to hospital. Clin Nutr. 1999;18(1):3-4.
AcknowledgementsWe express our sincerest appreciation to the Institution for the support we received to complete this study, as well as to all the profes-sionals who work there and strive every day to provide patients and families with the best care possible.
EWMA Journal 2014 vol 14 no 2 31

www.flenpharma.com I [email protected]
a total ap-
proach for every wound
and a
convenient solution for you and your patient.
for any type of wound
Flaminal ®, a total approach for every wound and a convenient solution for you and your patient.
Your peace of mindFlaminal ®
A new class in wound healing Enzyme Alginogels®
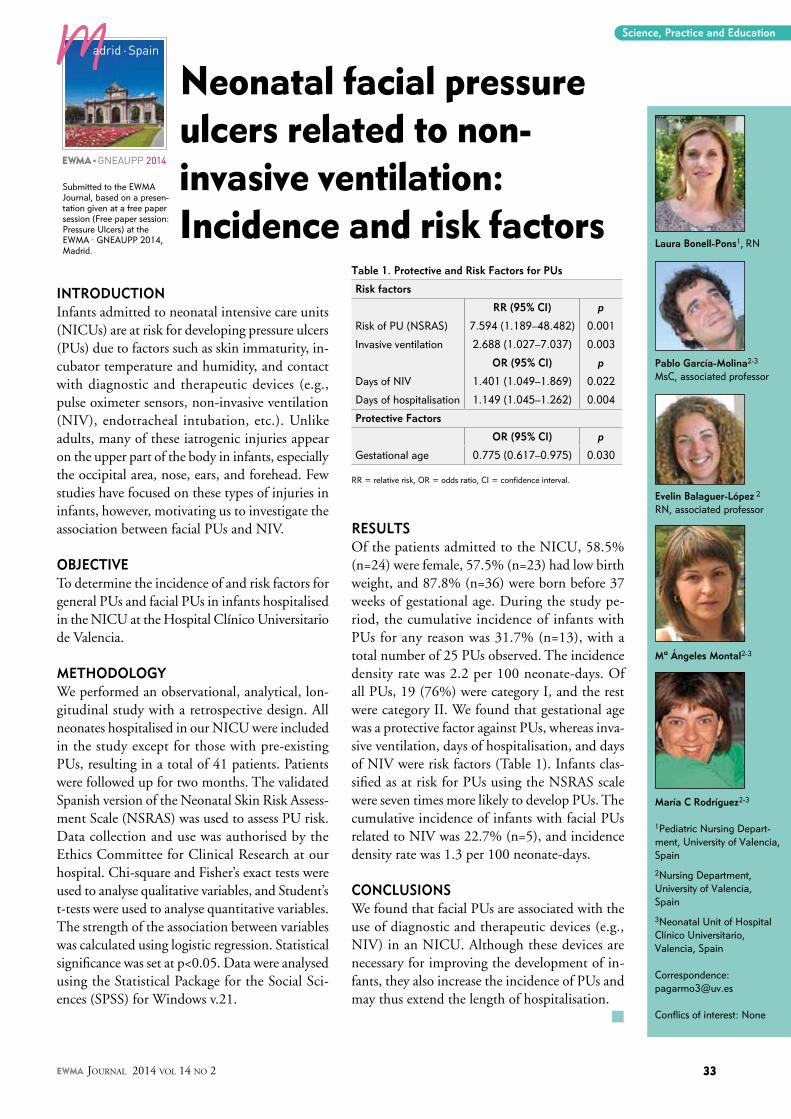
Laura Bonell-Pons1, RN
Pablo García-Molina2-3
MsC, associated professor
Evelin Balaguer-López 2
RN, associated professor
Mª Ángeles Montal2-3
María C Rodríguez2-3
1Pediatric Nursing Depart-ment, University of Valencia, Spain
2Nursing Department, University of Valencia, Spain
3Neonatal Unit of Hospital Clínico Universitario, Valencia, Spain
Correspondence:[email protected]
Conflics of interest: None
Science, Practice and Education
INTRODUCTION Infants admitted to neonatal intensive care units (NICUs) are at risk for developing pressure ulcers (PUs) due to factors such as skin immaturity, in-cubator temperature and humidity, and contact with diagnostic and therapeutic devices (e.g., pulse oximeter sensors, non-invasive ventilation (NIV), endotracheal intubation, etc.). Unlike adults, many of these iatrogenic injuries appear on the upper part of the body in infants, especially the occipital area, nose, ears, and forehead. Few studies have focused on these types of injuries in infants, however, motivating us to investigate the association between facial PUs and NIV.
OBJECTIVE To determine the incidence of and risk factors for general PUs and facial PUs in infants hospitalised in the NICU at the Hospital Clínico Universitario de Valencia.
METHODOLOGy We performed an observational, analytical, lon-gitudinal study with a retrospective design. All neonates hospitalised in our NICU were included in the study except for those with pre-existing PUs, resulting in a total of 41 patients. Patients were followed up for two months. The validated Spanish version of the Neonatal Skin Risk Assess-ment Scale (NSRAS) was used to assess PU risk. Data collection and use was authorised by the Ethics Committee for Clinical Research at our hospital. Chi-square and Fisher’s exact tests were used to analyse qualitative variables, and Student’s t-tests were used to analyse quantitative variables. The strength of the association between variables was calculated using logistic regression. Statistical significance was set at p<0.05. Data were analysed using the Statistical Package for the Social Sci-ences (SPSS) for Windows v.21.
RESULTS Of the patients admitted to the NICU, 58.5% (n=24) were female, 57.5% (n=23) had low birth weight, and 87.8% (n=36) were born before 37 weeks of gestational age. During the study pe-riod, the cumulative incidence of infants with PUs for any reason was 31.7% (n=13), with a total number of 25 PUs observed. The incidence density rate was 2.2 per 100 neonate-days. Of all PUs, 19 (76%) were category I, and the rest were category II. We found that gestational age was a protective factor against PUs, whereas inva-sive ventilation, days of hospitalisation, and days of NIV were risk factors (Table 1). Infants clas-sified as at risk for PUs using the NSRAS scale were seven times more likely to develop PUs. The cumulative incidence of infants with facial PUs related to NIV was 22.7% (n=5), and incidence density rate was 1.3 per 100 neonate-days.
CONCLUSIONS We found that facial PUs are associated with the use of diagnostic and therapeutic devices (e.g., NIV) in an NICU. Although these devices are necessary for improving the development of in-fants, they also increase the incidence of PUs and may thus extend the length of hospitalisation. m
Neonatal facial pressure ulcers related to non-invasive ventilation: Incidence and risk factors
Table 1. Protective and Risk Factors for PUs
Risk factors
RR (95% CI) p
Risk of PU (NSRAS) 7.594 (1.189–48.482) 0.001
Invasive ventilation 2.688 (1.027–7.037) 0.003
OR (95% CI) p
Days of NIV 1.401 (1.049–1.869) 0.022
Days of hospitalisation 1.149 (1.045–1.262) 0.004
Protective Factors
OR (95% CI) p
Gestational age 0.775 (0.617–0.975) 0.030
RR = relative risk, OR = odds ratio, CI = confidence interval.
adrid · Spain
EWMA n GNEAUPP 2014
Submitted to the EWMA Journal, based on a presen-tation given at a free paper session (Free paper session: Pressure Ulcers) at the EWMA · GNEAUPP 2014, Madrid.
EWMA Journal 2014 vol 14 no 2 33
sorbion silver fl exTargeting bacteria
www.sorbion.com
✓ Effective against bacteria and fungi
✓ No discoloration of the wound
✓ Wear time up to 7 days
NEW
Pro
du
ct a
vaila
bili
ty m
ay d
iffe
r fr
om
co
un
try
to c
ou
ntr
y.
AZ_silverflex_A4_EN.indd 1 22.08.14 12:41

Martin KiernanNurse Consultant Prevention and Control of InfectionSouthport and Ormskirk Hospitals NHS Trust
David Leaper Professor of Clinical SciencesUniversity of Huddersfield, UK
Conflicts of interest: None
Scientific Communication
ABSTRACTHealthcare-associated infections (HCAIs) are an important and costly complication of health-care throughout both primary and secondary sectors. In the European Union alone, the financial burden associated with HCAIs is up to €10b annually. HCAIs add unacceptable costs to healthcare economies – a 2- to 3-fold overall increase in the cost of the affected patient’s care in terms of extended hospital stay and associated costs. Increasing resistance following the use, mis-use, and over-use of antibiotics poses a world-wide problem that is compounded by the fact that no new antibiot-ics are in the pipeline. The recent and expand-ing appearance of carbapenemase resistance is of particular concern, as some strains of Klebsiella pneumoniae that produce carbap-enemase are almost pan-resistant, meaning that antimicrobial therapy is virtually impossi-ble. There is, however, good evidence that control measures can be effective. In the UK, the overall numbers of methicillin-resistant Staphylococcus aureus (MRSA) and Clostridium difficile infections have fallen due to increased compliance with infection prevention/control procedures. In particular, the delivery of care bundles containing evidence-based interven-tions has proved highly effective in preventing MRSA bacteraemias along with the “clean-your-hands” campaign and other measures such as universal admission screening. Surgical site infection (SSI) is probably the most prevent-able HCAI, yet due to the inconsistent imple-mentation of level 1A evidence-based interven-tions, the UK and US have shown disappoint-ing failures to reduce SSI. The reason for this lack of progress in SSI likely reflects poor com-pliance with guidelines and checklists.
BACKGROUND OF ANTIBIOTIC RESISTANCE AND HEALTHCARE-ASSOCIATED INFECTIONSAfter noting in 1928 that Penicillium notatum inhibited Staphylococcus aureus in a Petri dish, Alexander Fleming and his colleagues went on to successfully treat Police Constable Alexander for staphylococcal bacteraemia, although the patient relapsed and died when the antibiotic ran out. Nevertheless, a new class of antimicrobial drugs had been born, and although we have ever since relied on antibiotics to prevent and control infec-tion, we did not heed Fleming’s prophetic warning that inappropriate use might lead to resistance. We now know that resistance inevitably follows the introduction of new antibiotics within 15-20 years or even as little as 2-3 years1. Until recently, however, there has always been an alternative an-tibiotic when resistance was encountered. Now, times have changed; no new class of antibiotic has been introduced for well over a decade, and there are no new antibiotic classes in the pipe-line, rather just combinations of existing agents. Although there are many reasons for this lack of progress, it is mostly related to economic factors bound to research and development, regulatory procedures, and financial returns on investment for pharmaceutical companies.
With increasing antibiotic resistance, healthcare-associated infections (HCAIs) have become a more challenging problem. These iatrogenic com-plications, which are acquired through contact with healthcare services and institutions and are associated with considerable morbidity and mor-tality, are to a significant extent avoidable. Their costs to healthcare are enormous - up to €10b an-nually in Europe due to added costs of treatment and extended hospital stays. Additionally, some individuals become reservoirs of resistant organ-
Healthcare-associated infections (HCAIs): The magnitude of the problem
adrid · Spain
EWMA n GNEAUPP 2014
Submitted to the EWMA Journal based on a presen-tation given at a key session (A broad perspective in infection: The magnitude of today’s problem) at the EWMA · GNEAUPP 2014, Madrid.
EWMA Journal 2014 vol 14 no 2 35

isms (i.e., carriers) for whom suppression is expensive and complex, resulting in national screening programmes or “search and destroy” strategies. Today, the leading HCAIs are hospital-acquired pneumonia (not ventilator-associat-ed); urinary tract infection (UTI), including those associ-ated with catheters2; ventilator-associated pneumonia3; prosthetic and surgical site infection (SSI)4 caused by Sta-phylococci, including methicillin-resistant and -sensitive Staphylococcus aureus (MRSA and MSSA, respectively) and multiply resistant coagulase negative staphylococci, which are often associated with joint replacement or intravascular catheters; secondary bacteraemias; and complicated skin and soft tissue infections. Clostridium difficile infection (CDI)5, occurs as a secondary infection due to gut flora disturbances resulting from treatment with other HCAIs.
REDUCING THE RISE OF ANTIMICROBIAL RESISTANCEThe media has a huge impact on the HCAI political agen-da6 by driving public awareness and fostering the need for politicians to “do something” about “superbugs”, “killer microbes”, and outbreaks of “flesh-eating viruses”7. For instance, the media portrayed England as one of the “dirti-est” countries because of the rise of MRSA bacteraemia be-tween 1991 and 2003. While the actions of politicians may have been driven by media influence, infection prevention and control teams have turned the tide through hand hy-giene campaigns, improved clinical practice with respect to invasive devices, undertaking root cause analysis when infections occur, and implementing search and destroy campaigns (historically effective in the Low Countries and Scandinavia). The contribution of individual interventions is difficult to assess, but together with care bundles for central venous and peripheral intravenous catheter use and improvements in antibiotic stewardship, rates of MRSA bacteraemia continue to decline in the UK with impres-sive zero tolerance in NHS Trusts. It has been claimed by one UK “red top” daily newspaper, however, that MRSA has been minimised through a “plea to medics” to wash their hands.
Unfortunately, infection prevention and control issues are not at the top of busy clinicians’ agendas. Despite that mandatory infection control lectures are considered thera-peutic for sleep-deprived staff members, infection/preven-tion team-led training, surveillance, and feedback on local infection data have significantly reduced rates of MRSA and CDI. Interestingly, this does not seem to have been the case with Escherichia coli bacteraemia, the majority of which occur in community settings. Root cause analysis of increasing rates of infection in community settings sug-gests a relationship among use of urinary catheters, UTI,
and the lack of effective antibiotics available to general practitioners. The evidence base for long-term urinary catheter use and related complications is poor, but we know that catheterisation is not an intervention without complication. Urinary catheters are foreign bodies, and colonisation with Proteus mirabilis and Providentia rettgeri can cause biofilm formation, encrustation, and blockage8.
A FURTHER LOOK AT ExTENDED SPECTRUM b-LACTAMASES b-lactamases are enzymes that destroy the b-lactam ring of penicillins and cephalosporins. Common coliforms producing these enzymes are becoming resistant to most b-lactam antibiotics, and simple E. coli UTIs may be im-possible to treat in primary care due to a lack of effective oral therapies. Controlling the spread of resistance in com-munity settings is a huge challenge9, as plasmid-mediated resistance facilitates spread and makes resistance difficult for microbiology laboratories to detect10. This in turn leads to challenges in antibiotic formulary construction and a lack of information for clinical decision-making. Again, the media has drawn attention to extended spectrum b-lactamase-related deaths and has demanded tougher action, despite these deaths not being related to spread in hospitals. Carbapenem antibiotics are the current last resort in this battlefield, but already there are increasing numbers of carbapenemase-producing Enterobacteriaceae, such as New Delhi metallo-b-lactamase producers and carbapenemase-resistant Klebsiella pneumonia, which have implications for global travel, health-care tourism, overseas military action, and inter-hospital transfers.
CONCERTED ACTION IS NEEDEDResistance to antibiotics is an issue for all, not just clini-cians and specialists but also health-care and procurement managers, politicians, and, of course, patients and carers. It is time to move on from MRSA and CDI, which are coming closer to being under control. Multi-drug resistant Gram negatives, such as carbapenemase-resistant Kleb-siella, should in principle present no differences in terms of control. Reduction of HCAIs can be achieved through the use of care bundles (provided that compliance is meas-ured and reported) together with strict hand hygiene and environmental cleaning. Care bundles addressing intra-vascular care have proved effective in preventing MRSA bacteraemia, but similar success has not been found in reducing SSIs on either side of the Atlantic, despite that such bundles may contain several elements with a level I evidence base. The problem is related to poor compli-ance. We all need to understand that the real problem posed by antibiotic resistance is not just the over-use or
EWMA Journal 2014 vol 14 no 2 36

Scientific Communication
mis-use of antibiotics; it is any antibiotic use that risks the development of resistance. We need to preserve the gift of antibiotics.
A world without antibiotics is almost unimaginable in the modern era. Formerly fatal infections such as meningitis, bacteraemia, and pneumonia would become killers again; postoperative SSIs would increase to 30% or more after “at risk” contaminated/dirty surgery due to the lack of effective agents for prophylaxis; transplantation of tissue and organs might need to cease; cancer chemotherapy with the attendant risk of infection would be too risky; joint replacement and implants, such as vascular grafts, would become very high risk procedures; and post-partum and neonatal infections would return. Although there are options for action that involve the development of new antibiotics and vaccines, the motivation for such actions remains poor. Certainly we can sustain the effectiveness of existing antibiotics with close antibiotic stewardship. Per-haps better communication and precision concerning the choice and duration of antibiotic use could occur between microbiological laboratories and clinicians at the front line.
References
1. Krummenauer EC, Carneiro M, Alves Machado JA, de Mello Rauber J, Adam MS, Muller LB, et al. The impact of antimicrobial resistance and the challenge for professionals. Am J Infect Control. 2013;41(4):386-7.
2. Lo E, Nicolle LE, Coffin SE, Gould C, Maragakis LL, Meddings J, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(5):464-79.
3. Tedja R, Nowacki A, Fraser T, Fatica C, Griffiths L, Gordon S, et al. The impact of multidrug resistance on outcomes in ventilator-associated pneumonia. Am J Infect Control. 2014;42(5):542-5.
4. Anderson DJ, Podgorny K, Berrios-Torres SI, Bratzler DW, Dellinger EP, Greene L, et al. Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(6):605-27.
5. Dubberke ER, Carling P, Carrico R, Donskey CJ, Loo VG, McDonald LC, et al. Strate-gies to Prevent Clostridium difficile Infections in Acute Care Hospitals: 2014 Update. Infect Control Hosp Epidemiol. 2014;35(6):628-45.
6. Kiernan MA. Public reporting of healthcare-associated infection: professional reticence versus public interest. J Hosp Infect. 2013;83(2):92-3.
7. Chan P, Dipper A, Kelsey P, Harrison J. Newspaper reporting of meticillin-resistant Staphylococcus aureus and ‘the dirty hospital’. J Hosp Infect. 2010;75(4):318-22.
8. Wyndaele JJ. The encrustation and blockage of longterm indwelling catheters. Spinal Cord. 2010;48(11):783.
9. Cochard H, Aubier B, Quentin R, van der Mee-Marquet N, Reseau des Hygienistes du C. Extended-spectrum beta-lactamase-producing Enterobacteriaceae in French nursing homes: an association between high carriage rate among residents, environmental contamination, poor conformity with good hygiene practice, and putative resident-to-resident transmission. Infect Control Hosp Epidemiol. 2014;35(4):384-9.
10. Munoz-Price LS, Quinn JP. The spread of Klebsiella pneumoniae carbapenemases: a tale of strains, plasmids, and transposons. Clin Infect Dis. 2009;1;49(11):1739-41.
The burden of infection can be reduced by monitoring and enforcing hygiene and other public health measures, the adoption of novel immunisation strategies (which have been so effective for polio and smallpox), and continuous improvement in the design of healthcare environments.
Antibiotics will always have a role in treating cellulitis and lymphangitis before they progress to systemic inflamma-tory response syndrome, sepsis, or multiple organ dys-function syndrome. In situations in which host defences are poor, such as immunosuppression or diabetes, and in which the bioburden in chronic wounds is out of con-trol and leads to critical colonisation and local spreading infection, there will always be a need to consider anti-biotic therapy, although early intervention with topical antiseptics should also be considered. HCAIs are not an inevitable part of the provision of healthcare. Effective infection control measures help us protect patients from themselves and each other when in their most vulnerable states. Staff delivering healthcare should continually reflect on their practice. We owe this level of care to the memory of Alexander Fleming and his legacy. m
Become a Member of EWMAMake a difference in clinical practice
Benefits of your EWMA Membership:n You make a difference in clinical practice within wound management in Europen Right to vote and stand for EWMA Counciln EWMA Journal sent directly to you two times a yearn EWMA news and statements sent directly to youn A discount on your registration fee for EWMA Conferencesn Right to apply for EWMA travel grantsn Yearly membership fee € 25n Yearly membership fee for members of cooperating organisations € 10
Please register as a EWMA member at WWW.EWMA.ORG
EWMA Journal 2014 vol 14 no 2 37

Vivano®
Safety. And Simplicity.
The VivanoTec negative pressure unit by HARTMANN is the central component of the Vivano system for successful negative pressure treatment of wounds. Its low weight means it can be used either on the move or in hospitals. Thanks to its intuitive menu navigation, the VivanoTec negative pressure unit combines easy usage with highly precise treatment settings and the necessary reliability, thus guaranteeing a high level of safety and user-friendly handling.
050-3-013_AZ-Vivano_EWMA_210x297#.indd 1 05.08.13 09:17

Species Common name Skin type 2nd closure
Wound reduc6on by contrac6on
Homo sapiens humans (ght epithelialisa(on 20-‐40 %
Roden6a rats, mice loose contrac(on 90%
Porcine pigs (ght epithelialisa(on 20% in 11 days
Carnivora dogs
Trunk loose
Legs (ght
Trunk contrac(on
Limbs epithelialisa(on
Legs: unknown
Carnivora cats Legs: unknown
Equus ferus caballus
horses Trunk 59% Legs 20 %
Equus ferus caballus
ponies Trunk 76 % Legs 49 %
Scientific Communication
Wound healing and management is a challenge not only in human medicine but also in veteri-nary medicine. The struggles to heal complicated wounds in companion animal species are strik-ingly similar to those in human patients despite major differences between species. A comparison of the similarities in healing between species may identify new mammalian wound models with a much higher concordance rate, and a critical analysis of the differences may contribute to the common good. Sharing clinical problems, treat-ments, research, models, and ideas between hu-man and veterinary experts can therefore benefit both human and veterinary wound healing and management, which speaks for an intensified col-laboration between human and veterinary wound healing associations.
the contribution of wound contraction and epithelialisation to second intention healing of cutaneous wounds varies significantly across spe-cies due to differences in the gross and histologic structure of the skin. Rapid contraction is a com-mon feature of loose skin, which is present in the body/trunk of most companion animals, includ-ing horses, dogs, and cats. In contrast, extremity wounds in these animals heal in a manner more similar to wounds in tight-skinned species (e.g., humans and porcines), primarily as the result of re-epithelialisation2. Limb wounds in horses and human leg wounds heal in a similar way: healing in both species occurs mainly through epitheli-alisation with only limited wound contraction (Table 1, Fig. 1).
Jacintha M. Wilmink DVM, PhD, Diplomate RNVA
Veterinary Wound Healing Association (VWHA) Past President and Council Member
Correspondence:[email protected]
Conflicts of interest: None.
The value of veterinary wound management for human wounds and wound care
Animal wound modelsAlthough the majority of animal models in wound healing resear ch are based on rodents, the concord-ance rate between rodents and hu-mans is only 53%, which suggests that results from rodent models are not likely to translate into im-proved clinical outcomes. A lack of concordance is not surprising given the anatomical, physiological, and immunological differences between rodents and humans1. For example;
Table 1: Comparative cutaneous wound healing across species.
adrid · Spain
EWMA n GNEAUPP 2014
Submitted to the EWMA Journal, based on a pres-entation given a EWMA symposium (VWHA/EWMA Symposium on Veterinary Wound Management and Antimicrobial Resistance: Animal Wound Care - Best practice and new knowl-edge) at the EWMA · GNEAUPP 2014, Madrid.
THE FIRST IN A SERIES: There remains much to learn about the science of wound healing in humans. It may be possible to improve our understanding of wound healing by looking to other disciplines. Veterinary wound healing research has something to offer and this article
appears in the EWMA Journal as the first in a series of articles that looks outside of the traditional topics covered. We hope that you enjoy learning about wound healing in another species and will gain a better under-standing of the similarities that exist.
EWMA Journal 2014 vol 14 no 2 39

EqUINE WOUNDS AS A MODEL FOR HUMAN WOUNDS AND WOUND CARE:DIFFERENCES AND SIMILARITIES
Differences between human and equine patients and woundsAt first glance, human and equine patients do not seem to have much in common, and their wounds seem very different. Human patients are often elderly and sometimes obese or with nutritional deficiencies. Many human pa-tients suffer from systemic diseases that lead to vascular, diabetic, or pressure ulcers. These ulcers occur gradually with the progression of the disease, must heal by second intention, and often develop into chronic, difficult to heal wounds. In contrast, equine patients are usually less than 3 years of age and in normal nutritional condition. Their wounds are the result of sudden trauma, and the aim of treatment is primary intention healing. Not all wounds can be sutured, however, and wound dehiscence occurs frequently, which means that many wounds must heal by second intention and can develop into chronic, difficult to heal wounds.
Similarities between human and equine woundsAlthough human and equine patients and wounds are
initially very different, both species can suffer strikingly similar problems with second intention healing. It is close to normal for the limb wounds of horses to form unhealthy granulation tissue that is covered in biofilm and subject to chronic inflammation (Fig. 2). In contrast to human wounds, that often have a lack of granulation tissue, exu-berant granulation tissue (EGT) is a regular complication in horse wounds (Fig. 3). The clinical presentation of EGT is similar to that of human keloids, except that equine EGT is not epithelialised. Horse limb wounds sometimes develop scars that look like keloids, but histology shows that these are hypertrophic scars rather than true keloids. Horses, but not ponies, have a genetic predisposition for developing EGT and hypertrophic scars. Likewise, a ge-netic susceptibility to keloid formation has been observed in humans. Similarities in the histological appearance and dysregulated cytokine profiles of these fibroproliferative disorders in horses and humans have been shown3.
Another similarity between humans and equines is the hypoxia of wounds. In horses, wound hypoxia is caused by the anatomy of the limbs, which have only 2 main arteries running to the distal limb and limited collateral alternatives. When a horse limb is injured, the perfusion of the wound and the distal part of the limb can be dam-
Figure 3: Fibroproliferative disorders in the horse. This horse exhibits EGT in the central part of the wound, hypertrophic scarring along the wound margins, congestion, edema, and fi-brosis in the tissues around the wound and distal limb.
Figure 2: An example of a horse limb wound with unhealthy granulation tissue, necrotic parts, and biofilm formation, which most likely is subject to chronic inflammation. Some excess granulation tissue has already formed.
Scientific Communication
Figure 1: An example of a horse limb wound that has healed almost completely by epithe-lialisation.
EWMA Journal 2014 vol 14 no 2 40

aged, both by vessels that are cut and/or obstructed by clots or by the swelling of the tissues as a reaction to the traumatic incident. Equine wounds can therefore suffer from impaired oxygenation as well as problems with the venous return, which can lead to congestion, oedema, and finally to fibrosis (Fig. 3).
The final similarity between human and equine wounds is the susceptibility of limb wounds to the development of pressure sores. Equine pressure sores occur due to treat-ment with bandages or casts. The causes are the same as those that are known in humans: the amount of pressure, the duration of time in which the pressure is present, and shearing forces. A similar division in the severity and depth of pressure sores or ulcers can be made in equine and humans.
Comparative physiologyIt has been shown that within the equine species horses heal much slower and with more complications than po-nies. By comparing many aspects of the physiology of wound healing between these sub-species, it has been determined that most of the differences in clinical heal-ing can be explained by the course of the inflammatory response and the capacity of leucocytes to produce in-flammatory mediators. This knowledge has resulted in enormous improvement in clinical treatment strategies.
Comparing the (patho)physiology of human and equine wounds may also reveal new elements of wound heal-ing and wound management. The similarities in the epithelialisation/contraction ratio, the development of fibroproliferative disorders, biofilm formation, chronic inflammation, dysregulated cytokine profiles, hypoxia, and problems with pressure may introduce some promising modeling alternatives to consider. In addition, naturally occurring horse wounds may be useful for clinical trials because neither equine nor human wounds can be easily mimicked in experimental set-ups. The correlation be-tween human and equine wounds may lead to the devel-opment of new insights and treatments for both species. We conclude that further collaborations between human and veterinary experts in wound healing and management will be of benefit to both fields. m
References
1. Special Section Wound Repair and Regeneration: Wound healing in Veterinary Medicine; Asking the right questions to find the keys to wound healing. WRR 2013;21:363.
2. Volk SW and Bohling MW. Comparative wound healing- Are the small animal veterinarian’s clinical patients an improved translational model for human wound healing research? WRR. 2013;21:372-81
3. Theoret CL and Wilmink JM. Aberrant wound healing in the horse: naturally occurring conditions reminiscent of those observed in man. WRR. 2013;21:365-71.
The EWMA UCM programme offers students of wound management from institutes of higher education across Europe the opportunity to take part of their academic studies whilst participating in the EWMA Conference.
The opportunity of participating in the EWMA UCM is available to all teaching institutions with wound management courses for health professionals.
The UCM programme at the EWMA 2015 Conference in London will offer networking opportunities between the students from various UCM groups, UCM Lectures as well as assignments and workshops arranged specifically for the UCM students.
EWMA strongly encourages teaching institutions and students from all countries to benefit from the possibilities of interna-tional networking and access to lectures by many of the most experienced wound management experts in the world.
Yours sincerely
Dubravko Huljev
Chair of the Education Committee
THE EWMA UNIVERSITY CONFERENCE MODEL (UCM)
in London
Participating institutions:
Lithuanian University of Health SciencesLithuania
Haute École de Santé Geneva, Switzerland
HUB BrusselsBelgium
University of Hertfordshire United Kingdom
Universidade Católica Portuguesa Porto, Portugal
Donau Universität KremsAustria
For further information about the EWMA UCM, please visit the Education section of the EWMA website www.ewma.org or contact the EWMA Secretariat at [email protected]
LONDON · UK13-15 MAY 2015
EWMA 2015
EWMA Journal 2014 vol 14 no 2 41

4326
/ACE
/GLO
/091
4/PR
B36
13
* Results have not yet been confi rmed in humans. Lessing MC, et al. Negative Pressure Wound Therapy With Controlled Saline Instillation (NPWTi): Dressing Properties and Granulation Response In Vivo. Wounds 2011; 23:309-319.
NOTE: Specifi c indications, contraindications, warnings, precautions and safety information exist for KCI and Systagenix products and therapies. Please consult a physician and product instructions for use prior to application. This material is intended for healthcare professionals.
© 2014 KCI Licensing, Inc. All rights reserved. All trademarks designated herein are proprietary to KCI Licensing, Inc., its affi liates and/or licensors. DSL#14-0456.SYX4326.EWMA (9/14)
www.systagenix.comwww.kci-medical.com
VeraFlo™ Therapy can help Cleanse, Treat and Heal by combining the benefi ts of V.A.C.® Therapy with automated solution distribution, dwell and removal.
V.A.C.Ulta™ Negative Pressure Wound Therapy System:
TWO THERAPIES, ONE SYSTEM.
VeraFlo™ Therapy
It is also suitable for use, under medical supervision, with NEGATIVE PRESSURE WOUND THERAPY (NPWT).
NON-ADHERING SILICONE DRESSING
ALL YOU COULD WISH FORIN A WOUND CONTACT LAYER
ADAPTIC TOUCH®Cellulose acetate
mesh, coated with soft tack silicone
x20magnifi cation
NO ONE IMAGINED WOUND THERAPY COULD GET ANY BETTER… WE DID
more granulation
INNOVATIVE SOLUTIONS
In a porcine study comparing V.A.C.® Therapy to VeraFlo™ Therapy
with saline, there was 43%* more granulation after 7 days
of therapy.
4326 Joint Veraflo and ADAPTIC TOUCH ad (GLO)_AW2.indd 1 14/08/2014 09:24

Eskild W. Henneberg
President of the Danish Wound Healing Society
Correspondence:[email protected]
Conflits of interest: None
Telemedical wound assessment on the way to large scale deployment in Denmark
A status on the large-scale deployment of telemedicine as a tool for the rapid diagno-sis and enhanced treatment of wounds in Denmark
Resource savings and patient satisfaction stand to improve if we are successful in the large-scale deployment of telemedicine for the treatment of wounds in hospitals, municipalities, and medical practices throughout Denmark. This is supported by the successful implementation in Southern Jut-land, where Sygehus Sønderjylland (Hospital of Southern Jutland) and affiliated municipalities have been using telemedical wound assessment for a number of years with great success.
TELEMEDICINE – A NECESSARy TOOL IN A CROSS-SECTORAL HEALTH SERVICE The opportunities related to the large-scale de-ployment of telemedicine have generated a sig-nificant interest from decision makers. In profes-sional circles and the Danish Society for Wound Healing (DSFS)1, we wish to exploit this interest to facilitate the use of telemedicine in Denmark. We are delighted that the field of wound care has been chosen as a test bed for telemedicine, as we believe that it highlights the possibilities that tele-medicine offers within a cross-sectoral and multi-professional field. We see the telemedicine project as an opportunity to show decision makers what we can achieve by increased interdisciplinary col-laboration and wish to ensure that telemedicine becomes a platform for inter-disciplinary and inter-sectoral collaboration in future healthcare systems.
DSFS has therefore decided to engage in and support discussion and communication about the benefits and challenges related to the large-scale deployment of telemedical wound assessment.
Telemedical wound assessment should be ex-tended to the whole country The Danish Public Welfare Technology Founda-
tion has granted 4 mill EUR (30 million DKK) specifically for the dissemination of telemedical wound assessment. The focus is on venous leg ulcers and diabetic foot ulcers, and the project runs from September 2012 to September 2015.
The dissemination is controlled by MedCom2, a publicly funded organisation with responsibility for developing, testing, and assuring the quality of electronic communication in the healthcare sector. MedCom establishes the overall manage-ment of the processes that will lead to the use of telemedicine. The expected gains are: n Shorter healing time n Increased skills of the local nurses n Less time spent in hospitals, less travel time n Increased patient satisfaction
However, there are still a number of obstacles toovercome before these benefits can be achieved. Among these are disparate referral procedures,
TELEMEDICINE IN DENMARKAs in other European countries, the Danish healthcare system is facing major economic challenges in the years to come. Telemedicine solu-tions are seen as one of the primary opportunities to achieve increased quality of care and improved patient satisfaction, while simultaneously supporting efficient and coherent healthcare organisation and savings in healthcare budgets. Telemedicine should be an integral part of the healthcare services of the future. The national government, the regions and the municipalities are all in agreement about this.
In 2012, the national government, the regions and the municipalities initiated targeted telemedicine trials to learn more about telemedical solutions in practice. A sum of 12 mill EUR (90 mill DKK) was allo-cated for this purpose, and five areas (primarily cross-sectoral) were chosen for the studies:
1. Clinically integrated home monitoring 2. Home monitoring for chronic obstructive pulmonary disease
(COPD) patients 3. Telepsychiatry4. Internet psychiatry 5. National dissemination of telemedical wound assessment
EWMA Journal 2014 vol 14 no 2 43

No patient information added within the previous 30 days
Information added concerning up to 1 ptt/10.000 inhabitants within the previous 30 days
Information added concerning more than 1 ptt/10.000 inhabit-ants within the previous 30 days
Figure 1: Deployment status, telemed-ical wound assessment in Denmark
lack of coordination between sectors, lack of specifica-tion of the requirements for service redesign, and necessary changes in the roles of the involved groups of healthcare staff. Other challenges include full integration of the general practitioners and ensuring full support from the managements of the involved organisations. Finally, a few technology-related obstacles remain, such as the need to improve image quality to optimise the possibility of con-ducting proper wound assessments via the system.
The telemedical wound assessment project will run until September 2015, and the goal is that at least 80% of the municipalities will offer telemedical wound assessments to at least 40% of all relevant patients by the end of the project3.
Figure 1 illustrates the current status on the deploy-ment of telemedical wound assessment in the municipali-ties of Denmark (September 2014).
In the sections below we have elaborated some of the pri-mary challenges and opportunities related to the large-scale deployment of telemedical wound assessment.
TELEMEDICINE AND DOCUMENTATION – THE NATIONAL OVERVIEWA second and important perspective of telemedicine is the possibility to increase the amount of documentation via the registration of data on wound patients in Denmark in the national telemedicine system.
Previously, the epidemiological data of wound patients in existing systems has been incomplete. It has been dif-ficult to identify wound patients in the patient adminis-tration systems (PAS) (via ICD-10-CM4 diagnosis codes), as there are countless diagnoses of the different types of wounds, and the wound care units in the hospitals often do not have independent registration numbers. Therefore, patients’ data are often mixed up with the data of other patients admitted to the same department.
Through the gathering of patient data via a national telemedicine system, we will build an independent data-base with information about the patients’ demographics, diagnoses, and healing rates. On the national level, the ambition is that specific basic data from the telemedicine platform will be reported to a national wound database, allowing us to create a national overview of the wound patients.
A national expert group including clinicians with wound care expertise was established in connection with the large-scale deployment of telemedical wound assessment. This group suggests that the following clinical quality param-eters are used: Age, sex, wound, when did the wound oc-cur (note if the date is estimated), when was the wound discovered, first contact with the wound centre (time), healing time, use of telemedicine (start date and end date), wound area, wound treatment responsibility, re-sponsibility for the patient pathway, diagnosis, palliative treatment, intended cure, has the telemedicine consul-tation replaced a physical visit/resulted in an additional visit/no change, number of dressing changes since pre-vious evaluation, number of visits to the wound centre, number of hospital admissions, amputations, and death.
However, there are still a number of challenges that need to be dealt with before the system can provide the data col-lection needed to ensure continued evaluation and wound care improvement in Denmark. One of the primary ob-stacles is dealing with the variable ways data are registered in the different regions using the system, which means that comparable national-level data extracts are not yet available. These are some of the issues that must be solved to ensure maximum benefits of the system with regard to data collection.
THE NEED FOR ORGANISATIONAL CHANGES IN ALL SECTORSThere is no doubt that implementation of telemedical wound assessment will change our organisation and prac-tice in this field – in the municipalities, for the general practitioners, and in the wound clinics/departments.
The challenge for many municipalities will be to ensure that the nurses who have to deal with wounds and com-
EWMA Journal 2014 vol 14 no 2 44

Scientific Communication
Two large EU supported projects are currently working on the collection and analysis of data on telehealth and telemedicine:
RENEWING HEALTH aims at implementing real-life test beds for the evaluation of innovative telemedicine services. The project was started in 2010 and included a study of telemedical wound assessment of the diabetic foot. Data analysis is still ongoing, but the final report of the project is available at www.renewinghealth.eu
UNITED4HEALTH aims to test scaled up telehealth solutions. The project focuses on the disease areas COPD*, CHF* and diabetes. The data collection is on going. The core ambition of UNITED4HEALTH is to share the understanding that in order for telehealth solutions to work, it is essential that healthcare providers adopt innovative health and care service models. EWMA is a partner in the project, and is responsible for developing a dissemination model for information about telemedicine within the wound care community. More information about the project can be found at www.united4health.eu
*COPD = Chronic Obstructive Pulmonary Disease, CHF = Chronic Heart Failure
municate with the hospital departments are given neces-sary wound training. One major achievement related to the implementation of telemedical wound assessment is that it has supported the systematic implementation of wound-care training courses for all primary healthcare nurses dealing with wound care.
With regard to the medical practices involved in the cross-sectoral teamwork supported by the telemedicine system, they also need to adjust their daily practice to fit with this new type of collaboration.
A thorough examination of working practices in hos-pital departments will be required to varying extents to ensure that they are ready to meet the needs with regard to servicing telemedical communications on a daily ba-sis. The hospitals are also struggling with the challenges related to the adaption of the accounting system. This is something we hope will be resolved soon.
The national expert group provided the following advice5 for an educational programme. This advice aims to sup-port the organisational changes and new roles of the in-volved healthcare staff:
n E-learning is offered to all involved parties.n Medical doctors working in the wound care units of
the hospitals must have wound treatment experience, and collaboration among dermatology, endocrinol-ogy, vascular surgery, orthopaedic surgery, and foot therapy must be present.
n Wound care nurses in the hospitals must have com-pleted a diploma programme or post-graduate course in wound care. They must also possess specialised knowledge about the use of the telemedicine system and be responsible for establishing good collabora-tions with the community care units in the region.
n Wound care nurses in the municipalities must have completed a diploma programme or post-graduate course in wound care, in addition to a minimum of 2 years experience (minimum one wound care nurse in each area/per 15.000 citizens). Generalist regis-tered nurses in the municipalities should participate in a 5-day basic wound care course. This could be extended with a study visit to the wound care centre in the hospital.
n Social/healthcare workers in the municipalities should not be given responsibility for wound care (in the case of complex wounds) but should be offered education in prevention via the e-learning system.
n Registered nurses working in a medical practice, if responsible for wound care, should have completed a diploma programme or post-graduate course in wound care.
Finally, we see the drafting of precise cooperation agree-ments between municipalities and wound departments as a necessary basis for a successful collaboration. Ideally this agreement should also include education and train-ing obligations. A clear matching of expectations and a specification of the obligations of the involved parties is necessary. The involved parties (on national, regional, and local levels) should meet in connection with educational activities to support good collaboration. The training may be provided locally by the hospital department and/or al-located to national providers in this field. In the Danish case, MedCom has been involved in the development of a programme for education and training.
BUSINESS CASE INDICATIONS FOR HEALTH CARE BUDGET SAVINGS OPPORTUNITIESBehind the Danish Public Welfare Technology Founda-tion’s support for the dissemination of telemedicine is a business case commissioned by the Danish Ministry of Health. This was written in 20096 and revised in 20137 based on an evaluation of the use of telemedical wound assessment in the included areas throughout the country.
EWMA Journal 2014 vol 14 no 2 45

1/20
11
3/20
11
5/20
11
7/20
11
9/20
11
11/2
011
1/20
12
3/20
12
5/20
12
7/20
12
9/20
12
11/2
012
1/20
13
3/20
13
5/20
13
7/20
13
9/20
13
11/2
013
1/20
14
3/20
14
5/20
14
7/20
14
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0
Wounds
Patients
Pictures
Users
New patients
Cross sector patients
ACTIVITY PER MONTHN
UM
BER
MONTH/YEAR
Figure 2: Monthly activity in the Danish telemedicine system for wound assessment
Scientific Communication
The revised business case is based on the analysis of data related to 448 wounds, including venous leg ulcers (182), diabetic foot ulcers (114), and “mixed” wounds (venous and arterial) (152). A group of specialists has evaluated the expected savings based on an assessment of the costs related to necessary ambulatory visits, wound assessments, home visits, and visits by community nurses in connection with the treatment of a diabetic foot ulcer. Factors such as travel time and dressing materials and changes have been taken into account.
The revised business case shows that a realistic estima-tion of the potential savings from using telemedicine (on venous leg ulcers and diabetic foot ulcers) in municipalities and hospitals in Denmark is 2 mill EUR in 2014 with a continued increase in the annual saving potential of ap-proximately 5,5 mill EUR in 2020 (Total saving 2013-2020 estimated to approx. 30 mill EUR).
The expectations from the first version of the business case (based on historical data and assumptions) were sig-nificantly higher, but the prospectively collected data used in the revised version of the business case shows a lower number of cases, which is a primary reason for the reduc-tions in the expected financial outcome.
Fig. 2 illustrates the monthly activity in the telemedi-cine system during the period 2011-2014, following ex-tended use of the system throughout the country.
The revised business case shows average healing times of 24 and 29 weeks for diabetic foot ulcers and venous leg ulcers, respectively. However, as there are no relevant Dan-ish data for comparison, only time and more data will show if this is to be considered the baseline or particularly good or bad results.
Despite the reduction of the potential savings derived from the revised business case, there are indications that
resource savings will increase when the system has been integrated into the daily clinical practice and some of the listed obstacles have been dealt with. A more exact over-view of the economical outcome and consequences for the implementation will be provided when the results of the final data collection are available in 2015.
CONCLUSIONIn DSFS, we anticipate that the use of telemedicine will contribute to an improved use of the available resources of the healthcare staff, promote care givers’ knowledge about correct wound care, and ensure proper care for the patients throughout the country. But we also realise that large-scale deployment of the system demands organisational changes on many levels and will take time. However, we believe that with joint efforts, the barriers will be overcome, and telemedicine offers a possibility to ensure best-practice wound care throughout the country in the years to come.
Even though the economical outcome will not be sig-nificant for the involved organisations, these new commu-nication tools and organisational changes will result in an increased focus on the wound patients and improved pro-fessional skills and organisation of wound care in general.
m
References
1. www.saar.dk
2. http://www.medcom.dk/wm109991 (Accessed 22 September 2014) [In Danish only]
3. http://www.medcom.dk/wm112455 (Accessed 22 September 2014) [In Danish only]
4. International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM)
5. National implementering af telemedicinsk sårvurdering - Kliniske anbefalinger, MedCom, September 2013, Available at http://www.medcom.dk/dwn6328.pdf (Accessed 22 September 2014) [In Danish only]
6. MedCom: Business case for hjemmemonitorering, Maj 2009, Ref 70202521, Version 1.0 Dato 2009-05-01, Udarbejdet af PBL, PETH, Godkendt af Rambøll Management [In Danish only]
7. Epikon: Sårinitiativet – Business case baselining (Endelig udgave),
http://www.medcom.dk/dwn6588 (Accessed 22 September 2014) [In Danish only]
EWMA Journal 2014 vol 14 no 2 46
Helping you manage a widerange of surgical incisions
* TIELLE® Lite is indicated for use on low to non-exuding and bleeding wounds. ** At the discretion of the clinician.
References: 1. Boothman S. et al. Testing of the Bacterial Barrier Properties of TIELLE Dressings Using a Modifi ed Version of the Draft CEN Test Method (prEN 13726-5). Poster 2001. 2. Tournay, J. TIELLE® Lite on Lipoma. Case study. J&J Medical 2002. 3. Ballard, K. and Baxter, H. TIELLE® Lite on breast lump requiring an excisional biopsy. Case study. J&J Medical 2002. 4. Schulze, H.J . et al. Evaluating a superabsorbent hydropolymer dressing for exudating venous leg ulcers.. J Wound Care 2001, 10(1):511-518. 5. Data on fi le at Systagenix. 6. Data on fi le at Systagenix. 7. Taylor, A., et al. A non-comparative multicentre clinical evaluation of a new hydropolymer adhesive dressing. J Wound Care 1999, 8(10):489-492. 8. Wilkes et al., Surg Innov 2012 Mar;19(1):67-75.
TIELLE® LITE Prevena™
TIELLE® Lite offers safety and comfort
on sutures*1-7
• Physical bacterial barrier1
• Allows showering**2-4
• Minimises adherence to the wound bed5
To learn more, visit www.systagenix.com
Prevena™ Therapyactively manages and
protects surgical incisions
• Holds the edges of the incision together, reducing the risk of dehiscence
• Decreases lateral tension8 and edema
• Protects the operative site from external infectious materials
To learn more, visit www.kci-medical.com
For otherwise healthy patients For high risk patients with one or multiple comorbidities
4344
/ACE
/GLO
/08
14/P
RB36
09
NOTE: Specifi c indications, warnings, precautions and safety information exist for the Prevena™ Incision Management System. Please consult the Clinician Guide and Instructions for Use prior to application.
© 2014 KCI Licensing, Inc. All rights reserved. All trademarks designated herein are proprietary to KCI Licensing, Inc. and/or Systagenix, their affi liates and/or licensors. DSL#14-0468.SYX4344.EWMA (8/14).
4344 Incision management ad for EWMA Journal (GLO)_AW.indd 1 14/08/2014 16:26
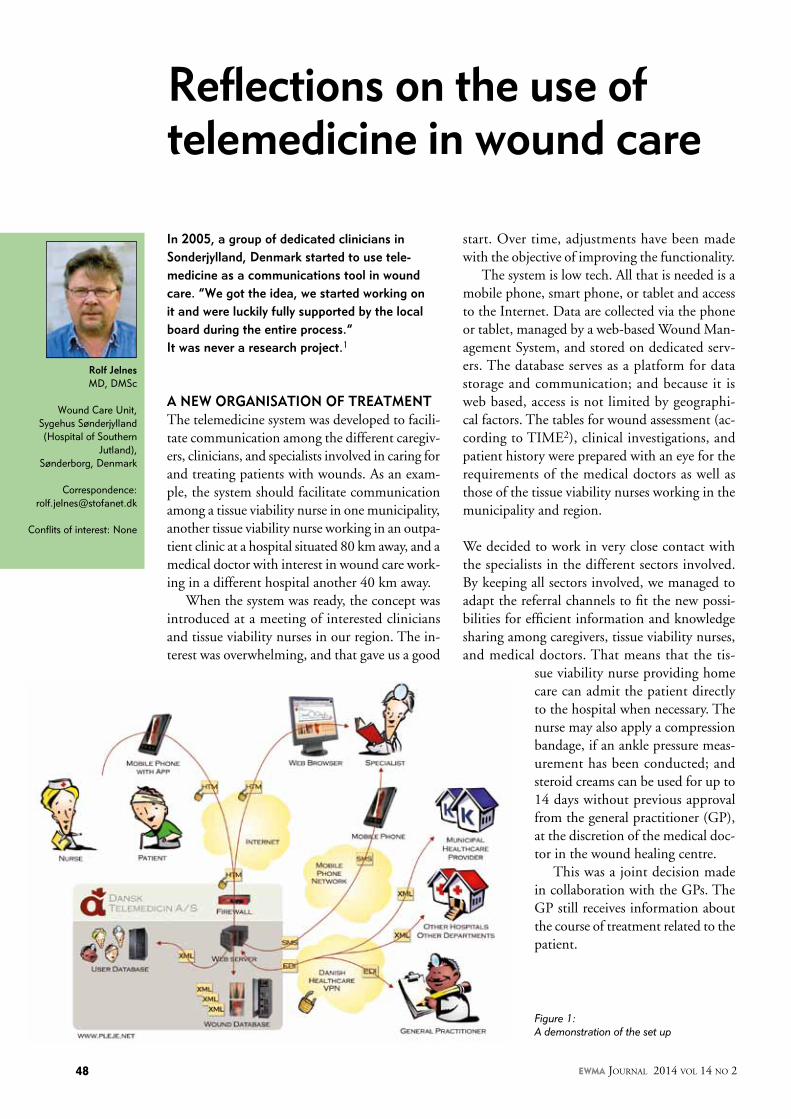
Rolf JelnesMD, DMSc
Wound Care Unit, Sygehus Sønderjylland (Hospital of Southern
Jutland), Sønderborg, Denmark
Correspondence:[email protected]
Conflits of interest: None
In 2005, a group of dedicated clinicians in Sonderjylland, Denmark started to use tele-medicine as a communications tool in wound care. “We got the idea, we started working on it and were luckily fully supported by the local board during the entire process.” It was never a research project.1
A NEW ORGANISATION OF TREATMENTThe telemedicine system was developed to facili-tate communication among the different caregiv-ers, clinicians, and specialists involved in caring for and treating patients with wounds. As an exam-ple, the system should facilitate communication among a tissue viability nurse in one municipality, another tissue viability nurse working in an outpa-tient clinic at a hospital situated 80 km away, and a medical doctor with interest in wound care work-ing in a different hospital another 40 km away.
When the system was ready, the concept was introduced at a meeting of interested clinicians and tissue viability nurses in our region. The in-terest was overwhelming, and that gave us a good
Reflections on the use of telemedicine in wound care
Figure 1: A demonstration of the set up
start. Over time, adjustments have been made with the objective of improving the functionality.
The system is low tech. All that is needed is a mobile phone, smart phone, or tablet and access to the Internet. Data are collected via the phone or tablet, managed by a web-based Wound Man-agement System, and stored on dedicated serv-ers. The database serves as a platform for data storage and communication; and because it is web based, access is not limited by geographi-cal factors. The tables for wound assessment (ac-cording to TIME2), clinical investigations, and patient history were prepared with an eye for the requirements of the medical doctors as well as those of the tissue viability nurses working in the municipality and region.
We decided to work in very close contact with the specialists in the different sectors involved. By keeping all sectors involved, we managed to adapt the referral channels to fit the new possi-bilities for efficient information and knowledge sharing among caregivers, tissue viability nurses, and medical doctors. That means that the tis-
sue viability nurse providing home care can admit the patient directly to the hospital when necessary. The nurse may also apply a compression bandage, if an ankle pressure meas-urement has been conducted; and steroid creams can be used for up to 14 days without previous approval from the general practitioner (GP), at the discretion of the medical doc-tor in the wound healing centre.
This was a joint decision made in collaboration with the GPs. The GP still receives information about the course of treatment related to the patient.
EWMA Journal 2014 vol 14 no 2 48

The illustration provided in Figure 1 shows the data flow and communication among the involved parties. A tissue viability nurse is visiting a patient in the patient’s home. A photo of the wound is taken using the camera in a mobile phone, and the photo is transmitted to the patient “wound database” on the web server by the use of an identification programme on the phone. If an immediate specialist evalu-ation is needed, a text message and e-mail can be sent to the medical doctor in the outpatient wound clinic (upper right quadrant) with a notification that an emergency call is wanted. The medical doctor evaluates the photo in the database and calls the tissue viability nurse while she or he is still in the home of the patient. Via that direct contact, a plan for treatment can be agreed upon.
In most cases, the nurse enters relevant data when he or she has returned to the office after a visit to a patient’s home. The data may include, for example, the results of ankle pressure measurement, pulse palpation, investigation for neuropathy, as well as wound assessment according to TIME2 and a short description highlighting the possible problems to be addressed. The medical doctor responsible for the wound treatment reviews the patient information on a daily basis. Based on those assessments, the patient may be signed up for one of the following options: n a first appointment for a visit to the outpatient clinic
(in case the patient is new);n a new appointment in case of deterioration (in case
the patient has been examined previously for the same wound).
If there is no need for a specialist examination in the out-patient clinic, the medical specialist informs the tissue vi-ability nurse that the planned treatment can be continued according to the relevant data that have been entered into the database.
During the first visit to the outpatient clinic, the results of the tests undertaken, for example, toe pressure meas-urement and X-ray and duplex scans, are entered into the relevant boxes, and a diagnosis is made. As the patient leaves the clinic, a message is sent directly to the electronic records of the primary healthcare provider organisations in the municipality, including those of the GP (direct trans-mission of data or information about new data in the database). This ensures that everyone involved in caring for the patient stays informed about the latest developments.
A network/task force is created for the particular patient. Typically, this will include the following profiles/individu-als.
n A tissue viability nurse in the municipalityn A tissue viability nurse in the outpatient clinicn The secretary in the outpatient clinicn The medical doctor responsible for the treatmentn The general practitionern The caseworker in the municipalityn The podiatrist and orthopaedic shoemaker, in case
the patient has a diabetic foot ulcern The patient
Thus, the implementation of a telemedicine system for the provision of wound care in the catchment area (250.000 inhabitants) of Sygehus Sønderjylland (Hospital of South-ern Jutland) represents a good example of the integrated care and the facilitation of the interdisciplinary teamwork that are crucial for providing good wound care3.
DATA SECURITyTo ensure that no ethical standards for data storage are violated, informed consent must be given by the patient before the patient records are established in the system. The system complies with Danish law and EU regula-tions concerning the protection of personal data4. Data are stored on dedicated servers located at two secure data facilities in Copenhagen, Denmark (the system is NOT a so-called “cloud-based” solution). Data are transmitted using point-to-point encryption, ensuring that the loca-tion of sensitive data is known and controlled at all times. All data access is managed and logged in accordance with Title 21 CFR Part 11 of the FDA guidelines on electronic records5, ensuring a detailed audit trail of user access to sensitive data. Clinical data are owned by the patient and are never accessed, handled, or otherwise used by non-clinical personnel. Likewise, clinical data are never shared with a third party (anyone not part of the team responsible for the treatment of the patient).
qUALITy OF THE TREATMENTWith regards to measuring the impact of the system lo-cally, the web-based clinical database, which is a part of the telemedicine system, has shown to be of great value for collecting data on wounds and the effects of wound care. Thus, the system provides researchers interested in wound care with a substantial amount of data, which may be used to evaluate and eventually adjust current treatment methods to ensure that the optimal treatment solutions are used.
When handling patients with venous leg ulcers, post-thrombotic syndrome, and traumatic ulcers, we include information on the size of the wound. This provides
Scientific Communication
EWMA Journal 2014 vol 14 no 2 49
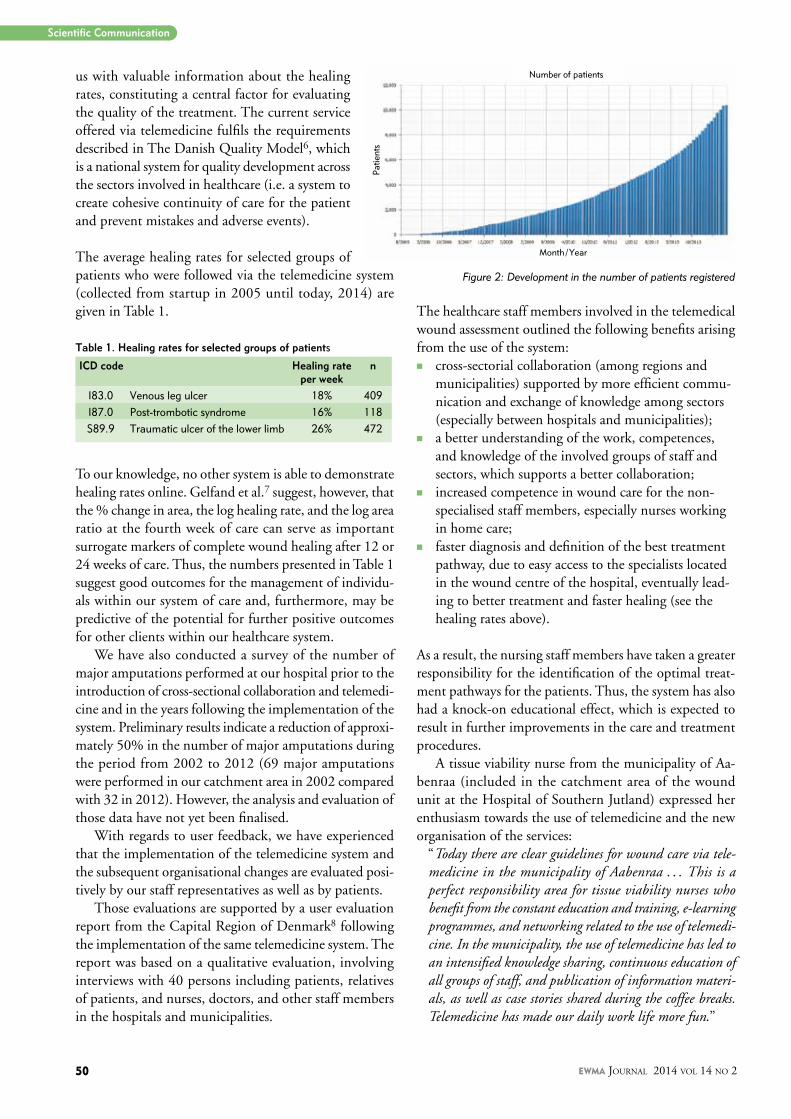
us with valuable information about the healing rates, constituting a central factor for evaluating the quality of the treatment. The current service offered via telemedicine fulfils the requirements described in The Danish Quality Model6, which is a national system for quality development across the sectors involved in healthcare (i.e. a system to create cohesive continuity of care for the patient and prevent mistakes and adverse events).
The average healing rates for selected groups of patients who were followed via the telemedicine system (collected from startup in 2005 until today, 2014) are given in Table 1.
Table 1. Healing rates for selected groups of patients
ICD code Healing rate per week
n
I83.0 Venous leg ulcer 18% 409I87.0 Post-trombotic syndrome 16% 118S89.9 Traumatic ulcer of the lower limb 26% 472
To our knowledge, no other system is able to demonstrate healing rates online. Gelfand et al.7 suggest, however, that the % change in area, the log healing rate, and the log area ratio at the fourth week of care can serve as important surrogate markers of complete wound healing after 12 or 24 weeks of care. Thus, the numbers presented in Table 1 suggest good outcomes for the management of individu-als within our system of care and, furthermore, may be predictive of the potential for further positive outcomes for other clients within our healthcare system.
We have also conducted a survey of the number of major amputations performed at our hospital prior to the introduction of cross-sectional collaboration and telemedi-cine and in the years following the implementation of the system. Preliminary results indicate a reduction of approxi-mately 50% in the number of major amputations during the period from 2002 to 2012 (69 major amputations were performed in our catchment area in 2002 compared with 32 in 2012). However, the analysis and evaluation of those data have not yet been finalised.
With regards to user feedback, we have experienced that the implementation of the telemedicine system and the subsequent organisational changes are evaluated posi-tively by our staff representatives as well as by patients.
Those evaluations are supported by a user evaluation report from the Capital Region of Denmark8 following the implementation of the same telemedicine system. The report was based on a qualitative evaluation, involving interviews with 40 persons including patients, relatives of patients, and nurses, doctors, and other staff members in the hospitals and municipalities.
The healthcare staff members involved in the telemedical wound assessment outlined the following benefits arising from the use of the system:n cross-sectorial collaboration (among regions and
municipalities) supported by more efficient commu-nication and exchange of knowledge among sectors (especially between hospitals and municipalities);
n a better understanding of the work, competences, and knowledge of the involved groups of staff and sectors, which supports a better collaboration;
n increased competence in wound care for the non-specialised staff members, especially nurses working in home care;
n faster diagnosis and definition of the best treatment pathway, due to easy access to the specialists located in the wound centre of the hospital, eventually lead-ing to better treatment and faster healing (see the healing rates above).
As a result, the nursing staff members have taken a greater responsibility for the identification of the optimal treat-ment pathways for the patients. Thus, the system has also had a knock-on educational effect, which is expected to result in further improvements in the care and treatment procedures.
A tissue viability nurse from the municipality of Aa-benraa (included in the catchment area of the wound unit at the Hospital of Southern Jutland) expressed her enthusiasm towards the use of telemedicine and the new organisation of the services:
“Today there are clear guidelines for wound care via tele-medicine in the municipality of Aabenraa . . . This is a perfect responsibility area for tissue viability nurses who benefit from the constant education and training, e-learning programmes, and networking related to the use of telemedi-cine. In the municipality, the use of telemedicine has led to an intensified knowledge sharing, continuous education of all groups of staff, and publication of information materi-als, as well as case stories shared during the coffee breaks. Telemedicine has made our daily work life more fun.”
Figure 2: Development in the number of patients registered
Number of patients
Patie
nts
Month / Year
Scientific Communication
EWMA Journal 2014 vol 14 no 2 50

From the perspective of the patient, the use of telemedicine has led to increased interconnection in the continuity of care, leading to an increased sense of security. Over time, we have also observed that patients have become more actively involved in their own care. Some have sent pho-tos asking if a visit to the outpatient clinic was needed, and others have asked to be seen as an emergency due to unexpected deterioration noticed by the patient. Thus, our experience shows a tendency for the implementation of telemedicine to lead to increased quality of care via patient empowerment.
As of 2014, Sygehus Sonderjylland (Hospital of Southern Jutland) has included 2293 patients in the database, with 20-25 new patients being added monthly. A national strat-egy for the large-scale deployment of the system has been developed, and the process is ongoing. Figure 2 illustrates the growth in the amount of patient information held on the database at a national level.
CONCLUSIONIntroducing this new, low-tech tool has changed our daily activities dramatically, to the ultimate benefit of the pa-tients. Many routine outpatient visits have been replaced by a standard visit by the responsible nurse working in the community and a professional evaluation of the patient’s condition via a wound description and photograph, all of which are entered into the database. This leaves the outpatient clinic more time to focus on performing the examinations needed to ensure that the correct diagnosis is given, defining a treatment pathway, and promptly treat-ing the most problematic wounds and emergency cases. In the primary healthcare setting, the use of the system has resulted in increased knowledge about wound care and faster healing of leg ulcers is indicated. m
References
1 Jelnes R: Telemedicine in the management of chronic wounds. Jour Wound Care. 2011;20(4):187-91.
2 Dowsett C, Ayello E, TIME principles of chronic wound bed preparation and treatment, British Journal of Nursing. 2004;13(15); ProQuest Nursing & Allied Health Source.
3 Moore Z, Butcher G, Corbett L, McGuiness W, van Acker K, AAWC, AWMA, EWMA Position paper: Managing wounds as a team, J Wound Care 2014;23 (5 Suppl):1-38.
4 Directive 95/46/Ec Of The European Parliament And Of The Council of 24 October 1995 on the protection of individuals with regard to the processing of personal data and on the free movement of such data
5 Food and drugs, chapter I, Food and drug administration, Department of health and human services subchapter A, General, Part 11: Electronic records; Electronic signatures www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?CFRPart=11 (Accessed 12 Sept 2014)
6 http://www.ikas.dk/DDKM.aspx (accessed 25.08.2014)
7 Gelfand JM, Hoff stad O, Margolis DJ. Surrogate endpoints for the treatment of venous leg ulcers, J Invest Dermatol. 2002;119(6):1420-5.
8 Telemedicinsk sårvurdering - En kvalitativ brugerevaluering blandt patienter og sundhedsfagligt personale i Region Hovedstaden. Brugerevaluering af telemedicinsk sårvurdering i Region H Brugerevaluering af telemedicinsk sårvurdering i Region H Februar 2013, Enheden for Brugerundersøgelser, Region Hovedstaden [in Danish]
PUBLICATIONS 2014
Document by AAWC, AWMA & EWMA: Managing Wounds as a TeamThe document provides a universal model for the adoption of a team approach to wound care.Publication: April 2014
Document by ICW, TVS & EWMA:Home Care-Wound CareThe document uncovers the preconditions that are necessary to provide safe, high-quality care for wound patients in a home care setting. Publication: May 2014
EWMA Study RecommendationsStudy recommendations for clinical investigations in leg ulcers and wound care. An easy-to-use guidance document for the novice researcher in wound care.Publication: May 2014
All the EWMA documents are published by the Journal of Wound Care, and can be downloaded free of charge at www.ewma.org
EWMA Journal 2014 vol 14 no 2

Georgina Gethin, Member of the EWMA Council
PhD, RGN, PG Dip Wound Healing, FFNM
RCSI, Dip Anatomy, Dip Applied Physiology, MSc
(c) Clinical Research. Senior Lecturer, School of
Nursing and Midwifery, National University of
Ireland, Galway, Ireland
Professor Caroline McIn-tosh, PhD, BSc (Hons),
MSc, MChS. Head of po-diatry, School of Health
Sciences, National Univer-sity of Ireland, Galway,
Ireland
Correspondence: georgina.gethin@
nuigalway.ie
AcknowledgementsWe are grateful for
the funding from the EXPLORE team at NUI
Galway (Wound Manage-ment Association of
Ireland [Western branch]) and the valuable feedback
and contributions from many colleagues.
Conflits of interest: None
INTRODUCTIONPressure ulcers are a significant health care issue that affect up to 18% of hospitalised patients and 3-10% in the home care setting. They also rep-resent 4% of the caseload of community nurses1,
2. These ulcers are a major source of morbidity, and they cause pain, depression, and the reduced quality of life in the individual. In some cases, death may occur. In addition, they constitute a significant cost to the health service, the patients, and their families3.
Pressure ulcers are defined as a localized injury to the skin and/or underlying tissue. They usually develop over a bony prominence as a result of pressure itself or in combination with shear and/or friction4. Attempts to prevent pressure ulcers are varied and include approaches, such as risk assessment, pressure re-distributing devices, and local and regional health care initiatives, includ-ing education programmes for staff and patients and the introduction of clinical care pathways. Although all health care professionals have a role and responsibility in pressure ulcer prevention, the current situation of more people receiving health care in the home care setting means that informal carers are increasingly in the front line for preven-tion strategies.
HOME CARE SETTINGThe shift in health care provisions from a hospital-based system to the home care setting throughout Europe has been reported in the European Wound Management Association (EWMA) document en-titled “Home Care Wound Care” (Probst et al. 2014) . The aim of this shift in care has been to promote community and health care delivery in the home care setting while simultaneously de-livering better services, improving productivity, increasing patient safety, and improving the qual-ity of care5. A key challenge is that there is an in-creasing trend for patients in the home care setting
to be older with multiple co-morbidities, more disabilities, and more complex health needs6, 7. Such individuals rely not only on resources of the healthcare system but also on informal carers to help meet their needs.
Informal carers may include spouses, children, neighbours, or friends. There is a large range of possible relationships. For example, a young in-formal carer could provide support to a parent or sibling, or younger parents could care for children. Informal carers often gain satisfaction from their caring role, as they are willing to take over the responsibility of caring for a family member at home8, 9. This underscores the need for the infor-mal carer to receive appropriate support to be able to undertake practical health care tasks, such as the application of a wound dressing. Furthermore, the onus is on health care providers to ensure that appropriate information is available for informal carers and that they can access support for their decision-making role9.
The aims of education for patients and carers are to optimize their input in the decision-making process, improve understanding, recall, and compliance, and reduce stress and anxiety. Effec-tive education strategies for lay persons require an understanding of factors that influence them in decision making: knowledge, attitudes, skills, and understanding. These strategies should also consider literacy and language barriers and how people may access information. The latter ele-ments of language and literacy should be a major consideration in designing information strategies, due to the multicultural societies we now live in and the low levels of literacy that are seen in some countries.
Using data from Ireland as an example, the 2011 census figures showed that over half a million (514,068) Irish residents spoke a foreign language
R.I.S.E for the prevention of pressure ulcersReposition, Inspection, Skin care, Eat well (R.I.S.E.)
– Information leaflet for carers for pressure ulcer prevention
EWMA Journal 2014 vol 14 no 2 52

Repositon
Try to help the person you
are caring for tomove
every 2 hours or more oft
en. This could involve
standing with help for a f
ewminutes,a short walk
or changingposition in th
e chair or bed. Always
try to keep the heels free o
f pressure asthey are
soft and canbecome dam
aged very easily.
Inspect
Inspect the skin at least d
aily for any signs of
redness particularly at th
e pressure points shown
in the pictureoverleaf. If yo
u notice redness that
does not go away, keep pr
essure off the area and
inform your local health p
rofessional such as your
GP or publichealth nurse
whowill be able to
advise you.
Some peoplehave very po
or feeling in their skin
and will not be able to tell
you if an area is
hurting, so always inspec
t carefully.
Care Giver Tip
Choose socks that do not
have a tightelastic
band at the top as this can
impede circulation in
the legs.
Skin Care
Whenwashing the perso
n you are caring for use a
mild soap and water and
pat the skin dry but do
not rub! If the person is in
continent make sure to
wash the skin in that area
regularly anddry well
Eat well
We need good food to kee
p our bodieshealthy
and to help healing. It is im
portant to offer the
person fluidsand foods th
at are high innutrition.
Sometimes small meals o
fferedmore frequently
are easier than largemea
ls. If the skinis very dry it
may be a sign the person
is not gettingenough
fluids. If in doubt contact y
our health
professionals.
Care Giver Tip
Remember red is a warnin
g sign! If concerned talk
to a health care professio
nal.
What is a Pressure Ulcer?
A pressure ulcer (sometim
es called a pressure sore
or bed sore)is an area of
damage to the skin
usually overa bony area s
uch as the hip, bottom,
heels or elbows. The skin
needs a goodblood
supply to stay healthy. To
omuch pressure on the
skin, for instance from sitt
ing or lying inone
position for along time, ca
n disrupt blood flow
and cause the skin to beco
me red. If pressure
continues the skin can be
come damaged; this is
called a pressure ulcer.
Who can get a Pressure Ulcer
Pressure ulcer can affect a
nyone. Thosemost at
risk are people who canno
t move very well, for
example people who are c
onfined to bed for long
periods of time or those in
wheelchairs.The
elderly and people with ill
health are particularly
at risk.
How To Prevent Pressure Ulcers
RISEReposition • Inspect • Skin
Care • EatWell
Scientific Communication
at home. Of these languages, Polish was by far the most common, followed by French, Lithuanian, and German10. Foreign languages are not the only consideration in the provision of information. The International Survey of Adult Literacy has shown that one in four Irish adults have literacy difficulties11. Another 30% of Irish adults were demonstrated to be at level 2, which signifies that they can only cope with very simple materials. Individuals with literacy difficulties struggle to understand discharge instructions, consent forms, handouts, and labels on pre-scriptions and over-the-counter medications. Many of them cannot understand important health-related letters or medical forms.
PROJECT AIMS This project was established, due to (1) the important role of the informal carer in health care provisions and the promotion of health and wellbeing, (2) increases in the number of people who are receiving health care in the home care setting, and (3) challenges that are involved in increasing the awareness of pres-sure ulcers and their prevention. Funding was
successfully obtained from EXPLORE at the National University of Ireland, Galway (NUI Galway). This scheme was intended to support initiatives in which students and staff collaborate as equal partners in projects. Therefore, this project aimed not only to promote the awareness of pressure ulcer prevention among informal carers but also to engage undergraduate nursing and podiatry students in wound care innovations and to foster a lifelong interest in the subject area. Further collaboration was gained from the Carers Association of Ireland and the Irish Practice Nurses Association (IPNA).
Samples of the leaflet were distributed by team members at the EWMA conference in Madrid in May 2014.
Informationfor Carers
Further Information:
To download this leaflet or for furtherinformation on pressure ulcers please visit :
• www.wmai.ie• www.carersassociation.ie• www.irishpracticenurses.ie
Funded by:
Endorsed by:
Contact Details:
PreventingPressure Ulcers
What do pressure ulcers look like?
A pressure ulcer can look like redness of the skinthat does not go away to an open sore that goesthrough to bone.
Head Shoulder Elbow Buttocks Heel
Toes
Heel
Ankle
Thigh(internal)
Hip Thigh(external)
Shoulder ElbowEar
Sacrum
Head
Shoulder
HeelIschion
Care Giver Tip
Don’t forget to check places like the ears and tipsof toes. These are common areas where pressureulcers develop and are often forgotten.
RISEReposition • Inspect • Skin Care • EatWellThis leaflet is intended as a guide only. If you are
concerned about anything in this leaflet pleasediscuss this with your healthcare professional.
Where on the body can you getPressure Ulcers?
RISEReposition • Inspect • Skin Care • EatWell
Project teamDr. Georgina Gethin, Professor Caroline McIntosh, Brid McGing, Fiona Mullins, Lauren Brennan, Sally Glynn, Orla Carey, Jacqui Hartigan, Ann Gardiner, and Moira GunningNoone.
EWMA Journal 2014 vol 14 no 2 53

Scientific Communication
STEPS OF THE PROJECTStep 1: Search and appraisalTo look for leaflets and information that are specifically aimed at carers for pressure ulcer prevention, we searched international wound care organizations’ websites and re-searched health information. We found only six examples of information leaflets. However, these were all produced for patients and not for carers. No other forms of infor-mation, such as videos or interactive education portals, were found.
The six leaflets were appraised by the team for readabil-ity, clarity of expression, language use, use of illustrations to convey messages, and general appeal. Of those identi-fied, only one from the United States was sponsored by a commercial organization and of high quality. This leaflet was twelve pages long, A5 sized, and well-illustrated with colour images. The language was also clear and easily un-derstood. However, the final four pages of the leaflet con-tained commercial advertising, along with product place-ments. One other leaflet contained excellent information but was of low readability. It was only available in text, used a font that was too small for the ease of reading, and had no illustrations. The remaining four leaflets were of even less quality, with technical language, small font sizes, and a lack of illustrations.
Having failed to find any available leaflets, the process of designing content and presentation style commenced. A key driver of the project was the readability of the final product and the ease with which it could be translated into other languages.
Step 2: R.I.S.E.The acronym, R.I.S.E., was devised to promote the basic principles of pressure ulcer prevention among carers.
Reposition – regular repositioning can help prevent tissue damage.Inspect – daily inspection of the skin can identify areas that are at risk of ulceration.Skin care – washing and drying the skin can prevent tissue damage.Eat well – good nutrition and hydration are essential for health and wellbeing.
We were mindful that this acronym could not be translated verbatim into other languages but recognized that it could be easily adapted by others. Although other acronyms have been suggested within the literature, none were targeted at carers. In addition, we wanted to keep the message simple and direct. Therefore, fewer letters would help in recall and understanding.
Step 3: Design and reviewOver six months, the leaflet went through numerous itera-tions, and a final design was chosen. Consultations with graphic designers, carers, and practice nurses took place, and further support, including project management and project promotion, was gained from the Explore team. Awareness and feedback on the project was also promoted at the Stop Pressure Ulcer Day at NUI Galway in Novem-ber 2013. The readability was appraised and deemed to be appropriate to the reading ability of a 10-year-old person. This was important, as some carers may have low literacy levels when reading in their non-native language.
FINAL LEAFLETThe final leaflet was launched at the Explore event in May 2014. In addition, samples of the leaflet were distributed by team members at the EWMA conference in Madrid in May 2014.
AVAILABILITyThe leaflet is freely available and has been uploaded on the websites of the Wound Management Association of Ireland (www.wmai.ie), IPNA (www.irishpracticenurses.ie), and Carers Association (www.carersireland.com). Plans are under way to have this available on other sites. As the aim was to increase awareness and promote pressure ulcer prevention, we agree that the leaflet can be downloaded by any wound care organization, health care provider, or patient support network. Furthermore, it can be trans-lated into other languages, as long as the original source is acknowledged. m
References
1. Gallagher, P., Barry, P., Hartigan, I., McCluskey, P., O’Connor, K. & O’Connor, M. Prevalence of pressure ulcers in three university teaching hospitals in Ireland. J Tissue Viabil. 2008;17(4):103-9.
2. McDermott-Scales, L., Cowman, S. & Gethin, G. Prevalence of wounds in a community care setting in Ireland. J Wound Care. 2009;18(10):405-6, 408, 410 passim.
3. Gethin, G., Jordan O-Brien, J. & Moore, Z. Estimating the costs of pressure area management based on a survey of ulcer care in one Irish hospital. J Wound Care. 2005;14(4):162-5.
4. EPUAP (2009) Guide to pressure ulcer grading. EPUAP review 3 (on-line), www.epuap.org/newsletter/epuap-reviews/vol10-issue1-2009/.
5. Vowden, K., Vowden, P. & Posnett, J. The resource costs of wound care in Bradford and Airedale primary care trust in the UK. J Wound Care. 2009; 18(3):93-4, 96-8, 100 passim.
6. Probst, S., Seppanen, S., Gethin, G., Gerber, V., Hopkins, A. & Rimdeika, R. EWMA Document Homecare WoundCare. J Wound Care. 2014;23(5):1-44.
7. Barry, U. Elderly care in Ireland-Provisions and Providers. In UCD School of Social Justice Working Papers Series (U, B. ed. University College Dublin, Dublin) 2010:10:1-34.
8. Bee, P.E., Barnes, P. & Luker, K.A. A systematic review of informal caregivers’ needs in providing home-based end-of-life care to people with cancer. J Clin Nurs, 2009;18(10):1379-93.
9. McConigley, R., Halkett, G., Lobb, E. & Nowak, A. Caring for someone with high-grade glioma: a time of rapid change for caregivers. Palliat Med. 2010;24(5):473-9.
10. CSO (2011) This is Ireland. Vol. www.cso.ie Central Statistics office, Dublin.
11. OECD (2007) International Adult Literacy Survey: Results for Ireland. Vol. www.nala.ie Department of Education and Science, Dublin.
EWMA Journal 2014 vol 14 no 2 54

Simple and ingenious:use haemoglobin to heal chronic wounds
Haemoglobin SprayGranulox now has distributors in more than 30 countries worldwidewww.granulox.de
Before Granulox After 187 days
Patient: 69 years, female, Arterial crural ulcerExisted for 46 months before Granulox
Before Granulox After 57 daysPatient: 65 years, female, diabetic gangreneExisted for 2 months before Granulox
VISIT US AT:
SICPRE, BERGAMO13.-15. OCTOBER 2014
VII. CHRONIC WOUNDS SYMPOSIUM,TUHELJSKE TOPLICE CROATIA 16.-17. OCTOBER 2014
CYPRUS BREAST RECON-STRUCTION MEETING, CYPRUS24.-25. OCTOBER 2014
NORDIC DIABETIC FOOT SYMPOSIUM, MALMÖ5.-6. NOVEMBER 2014
WOUNDS UK ANNUAL CONFERENCE, HARROGATE10.-12. NOVEMBER 2014
DANISH WOUND HEALING SOCIETY – ANNUAL MEETING, KOLDING21.-22. NOVEMBER 2014
NATIONAL WOUNDCARE ASSOCIATION CONGRESS, PORTO27.-28. NOVEMBER 2014
ANNUAL MEETING OF WOUNDCARE ORGANI-ZATION, HELSINKI 29.-30. JANUARY 2015
ICW, BREMEN 6.-8. MAY 2015
EWMA, LONDON 13.-15. MAY 2015
Start of treatment After 7 daysPatient: 18 years, male, second-degree burnacute wound
rz_granulox_anzeige_wundexperten_2014.indd 1 15.09.14 18:12
Same-Ekobo A.1,
Ehounou G.2, Comte E.3,
Vuagnat H.4
1Faculty of Medicine and Biomedical Sciences.
University of Yaoundé I. Cameroon.
2Medical Coordinator,
Doctors without Borders, Cameroon Mission
3Médecins sans Frontières Suisse
4University Hospitals of Geneva. Switzerland
Correspondence:[email protected]
Conflits of interest: None
Setting a course on chronic wounds in Cameroon
INTRODUCTIONThe first Buruli Ulcer (BU) cases were described in the Nyong valley in Cameroon in 1969 (47 patients1). At present, two factors are especially important to the development of BU in Cam-eroon. First, the incidence seems to be increas-ing in the three river basins and the two areas of rice-field irrigation in which BU is endemic (Fig. 1). Second, the Cameroon Ministry of Health (MoH) is facing additional difficulties resulting from the Médecins sans Frontières Suisse (MSF) withdrawal from the BU Control Programme in Akonolinga. Since 2002, MSF in partnership with the MoH has carried out a campaign against BU in the Health District of Akonolinga. That campaign expanded in 2011 to include patients suffering from chronic wounds. During the National Buruli Week in November 2013, the need to train health workers to face the global increase in cases of BU
was addressed, reinforced by the withdrawal of the MSF from the BU Control Program as well as the fact that medical schools in Cameroon teach neither the treatment of BU nor that of chronic wounds.
ABSTRACT Here, we describe a course developed in Cameroon with the aim of raising awareness and improving the treatment of Buruli Ulcer (BU) and chronic wounds. There are three specific objectives: 1) raise awareness of the problems associated with BU; 2) strengthen the capacity of the medical staff for building a multidisci-plinary approach to the management of BU and chronic wounds; and 3) to advocate for support and the certification of an Inter University Diploma (IUD) based on the course. A course was developed and implemented at Yaoundé University and the Akonolinga District Hos-pital. The preparatory phase involved weekly meetings to coordinate training activities. The second phase involved the selection of teaching strategies based on traditional pedagogy and adult education combining conferences and workshops as well as the actual teaching of the course programme to a group of participants. In July 2013 and April 2014, two work-shops based on the planned course were launched, respectively, in Yaoundé. The workshops focused on theoretical and practical training in wound epidemiol-ogy, basic sciences (the anatomy of the skin and the physiology of wound healing), holistic case manage-ment, and research on BU transmission and co-
infection with HIV. Physiotherapy was scheduled to teach patients and their families how to exercise or position (mostly by splints) limbs and joints to prevent disability. The use of compression bandages in order to reduce lymphoedema was also covered. Psychoso-cial assistance was considered to ensure that children’s schooling continues during hospitalisation and to help patients gain acceptance, and thus involvement, in social activities and work. Evaluations of the partici-pants’ knowledge, capabilities, and skills on both the theoretical and the practical levels prior to the work-shops and again at the conclusion were measured.On April 24, 2014, the Cameroon Wound Care Soci-ety (CaWoCS) was founded, adopting a triple com-mitment: integrate the EWMA and the World Alliance for Wound and Lymphedema Care networks; partner the CaWoCS with the Swiss Association for Wound Care; and organise a National Wound Day in Cam-eroon. It is hoped that our activities at the EWMA Confer-ence in Madrid 2014 and in the EWMA Journal will help raise awareness about the need for education regarding BU and chronic wounds in Cameroon as well as help the project gain momentum by reaching other networks and associations fighting against BU and chronic wounds.
adrid · Spain
EWMA n GNEAUPP 2014
Submitted to the EWMA Journal, based on a presentation given a free Paper Session (Free paper session: Education & Mis-cellaneous) at the EWMA · GNEAUPP 2014, Madrid.
EWMA Journal 2014 vol 14 no 2 56

In order to mitigate the effects of the MSF withdrawal, the Cameroon Wound Care Society (CaWoCS) was founded in on April 24, 2014 with three goals: integrate the EWMA and the World Alliance for Wound and Lymphedema Care networks; form a partnership with the Swiss Association for Wound Care (SAfW); and organise a National Wound Day in Cameroon. The CaWoCS is moving forward to propose a course on chronic wounds and BU in Cameroon with the aim to raise awareness about BU and elevate BU from its current state among neglected diseases2. Figure 2 shows examples of infectious chronic wounds that are typically seen under tropical conditions and will be taught in the course. The resources, both intellectual and finan-cial, for the course are expected to come from a partner-ship among universities, medical schools, and hospitals (both in Yaoundé and in Geneva), the EWMA, the SAfW, the World Alliance for Wound and Lymphedema Care (WAWLC), and the MoH. The following initiatives have been undertaken in order to achieve the aims of the course:n In 2013, an organising committee was constituted with members from the MSF, the Faculties of Medicine of Yaoundé and Douala, the MoH, and the Hôpitaux Universitaires de Genève (HUG).n In July 2013 and April 2014, two workshops on wound care and BU were launched, respectively, in Yaoundé. n The CaWoCS was founded.
The course was designed to reinforce the capacities of Cameroonian healthcare workers and students to manage and prevent chronic wounds and BU with three specific objectives in mind: 1. sensitise the national opinion to the problems of chronic wounds and BU in Cameroon; 2. strengthen the capacity of the medical staff to build a multidisciplinary approach to managing chronic wounds and BU;3. to advocate for support and the certification of an Inter University Diploma (IUD) based on the course.
COURSE CHARACTERISTICSThe course is designed to strengthen the skills, compe-tencies, and abilities of healthcare workers and medical students for holistic case management of chronic wounds and BU in Cameroon. The 2013 and 2014 editions were
Fig. 2. Examples of the infectious chronic wounds typically seen under tropical conditions. A (Guinea worm ulcer). B (Cutaneous Leishmaniosis ulcer, Dondji, 2008). C (Phagedenic Ulcer. Anophele,3, 2003). D (Chromomycosis). E (Buruli Ulcer, MSF, Akonolinga, 2011)
Scientific Communication
10 days long: 5 days of theory taught in Yaoundé followed by 5 days of practice in Akonolinga.In 2015, the course leading to the IUD will be conducted over a 3-week period comprising 2 weeks at Yaoundé Uni-versity for modules of theoretical training and workshops and 1 week in Akonolinga District Hospital for practical, hands-on training. In addition, e-learning will be imple-mented. Ideally, an initial 3-day module plus 5 days of hands-on training would be sufficient for those needing only to become familiarised with advanced wound care, whereas only the completion of the full 3-week course would provide the IUD. Most of the approximately 20 course trainers were re-cruited based on their fields of specialisation from among medical doctors, nurses, physiologists, psycho-sociologists, and physiotherapists at various Faculties of Medicine as well as doctors, nurses, and medical biologists at a Refer-ence Laboratory (Centre Pasteur) and District Hospitals. The 25 participants in the two initial workshops were re-cruited from among doctors, nurses, and medical students meeting the following criteria and quotas: n age (40 years maximum)n diploma (bachelor’s degree in scientific field or
equivalent) n professional experience (2 years minimum) n recommendation letter
(from the MoH or a Regional Health Officer) n written Commitment of Candidate
(to live in Yaoundé during the training period)n quotas
(Medical Doctors younger than 35 years of age, individuals with an undergraduate degree in a medi-cal specialisation, and other health workers should each represent 20% of the participants; state nurses should represent 40% of the participants)
n furthermore, curriculum vitae and official documents should confirm the candidate’s profile. The same criteria apply to the 2015 edition of the course. Prior to its teaching, the course content is to be approved both by the university administration (Deas of the Yaoundé and Douala medical schools) and the partners (MSF, HUG, EWMA, SAfW, and WAWLC), according to the standard teaching proce dures in Cameroon.
EWMA Journal 2014 vol 14 no 2 57
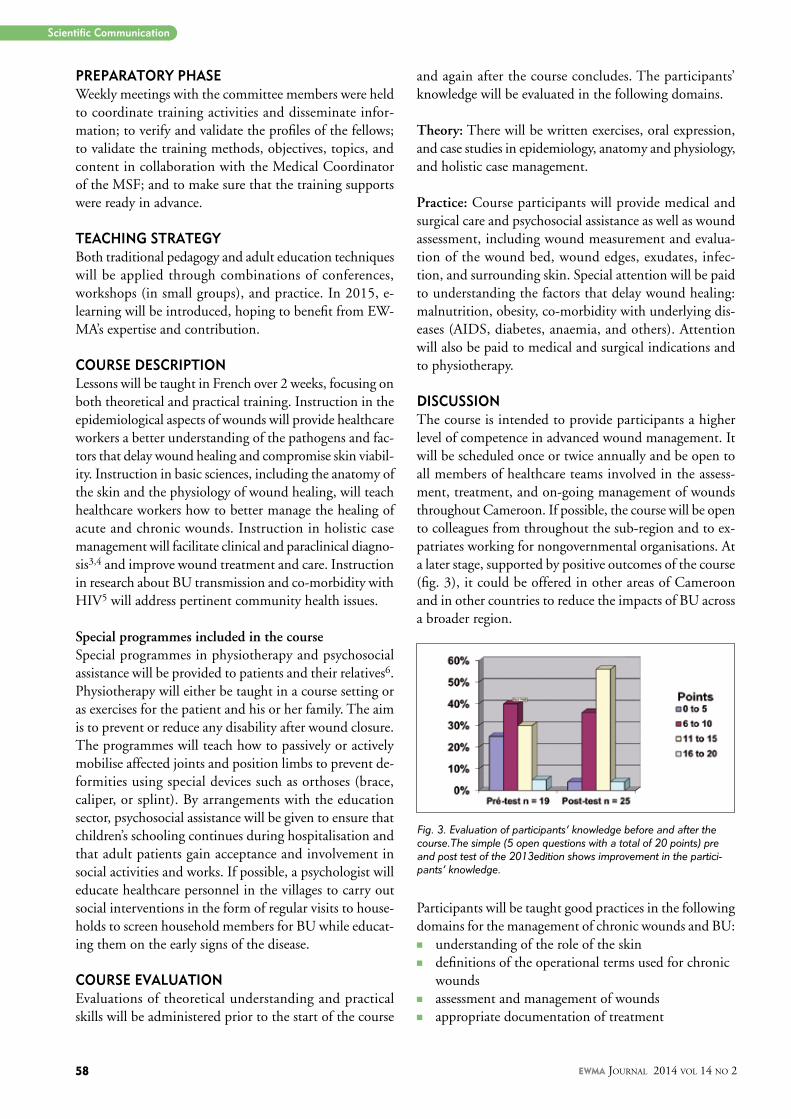
PREPARATORy PHASE Weekly meetings with the committee members were held to coordinate training activities and disseminate infor-mation; to verify and validate the profiles of the fellows; to validate the training methods, objectives, topics, and content in collaboration with the Medical Coordinator of the MSF; and to make sure that the training supports were ready in advance.
TEACHING STRATEGy Both traditional pedagogy and adult education techniques will be applied through combinations of conferences, workshops (in small groups), and practice. In 2015, e-learning will be introduced, hoping to benefit from EW-MA’s expertise and contribution.
COURSE DESCRIPTION Lessons will be taught in French over 2 weeks, focusing on both theoretical and practical training. Instruction in the epidemiological aspects of wounds will provide healthcare workers a better understanding of the pathogens and fac-tors that delay wound healing and compromise skin viabil-ity. Instruction in basic sciences, including the anatomy of the skin and the physiology of wound healing, will teach healthcare workers how to better manage the healing of acute and chronic wounds. Instruction in holistic case management will facilitate clinical and paraclinical diagno-sis3,4 and improve wound treatment and care. Instruction in research about BU transmission and co-morbidity with HIV5 will address pertinent community health issues.
Special programmes included in the courseSpecial programmes in physiotherapy and psychosocial assistance will be provided to patients and their relatives6. Physiotherapy will either be taught in a course setting or as exercises for the patient and his or her family. The aim is to prevent or reduce any disability after wound closure. The programmes will teach how to passively or actively mobilise affected joints and position limbs to prevent de-formities using special devices such as orthoses (brace, caliper, or splint). By arrangements with the education sector, psychosocial assistance will be given to ensure that children’s schooling continues during hospitalisation and that adult patients gain acceptance and involvement in social activities and works. If possible, a psychologist will educate healthcare personnel in the villages to carry out social interventions in the form of regular visits to house-holds to screen household members for BU while educat-ing them on the early signs of the disease.
COURSE EVALUATION Evaluations of theoretical understanding and practicalskills will be administered prior to the start of the course
and again after the course concludes. The participants’ knowledge will be evaluated in the following domains.
Theory: There will be written exercises, oral expression, and case studies in epidemiology, anatomy and physiology, and holistic case management.
Practice: Course participants will provide medical and surgical care and psychosocial assistance as well as wound assessment, including wound measurement and evalua-tion of the wound bed, wound edges, exudates, infec-tion, and surrounding skin. Special attention will be paid to understanding the factors that delay wound healing: malnutrition, obesity, co-morbidity with underlying dis-eases (AIDS, diabetes, anaemia, and others). Attention will also be paid to medical and surgical indications and to physiotherapy.
DISCUSSIONThe course is intended to provide participants a higher level of competence in advanced wound management. It will be scheduled once or twice annually and be open to all members of healthcare teams involved in the assess-ment, treatment, and on-going management of wounds throughout Cameroon. If possible, the course will be open to colleagues from throughout the sub-region and to ex-patriates working for nongovernmental organisations. At a later stage, supported by positive outcomes of the course (fig. 3), it could be offered in other areas of Cameroon and in other countries to reduce the impacts of BU across a broader region.
Participants will be taught good practices in the following domains for the management of chronic wounds and BU:n understanding of the role of the skinn definitions of the operational terms used for chronic
woundsn assessment and management of woundsn appropriate documentation of treatment
Fig. 3. Evaluation of participants’ knowledge before and after the course.The simple (5 open questions with a total of 20 points) pre and post test of the 2013edition shows improvement in the partici-pants’ knowledge.
Scientific Communication
EWMA Journal 2014 vol 14 no 2 58

UPCOMING INITIATIVES IN 2014 -2016
EWMA leg ulcer recommendationsThe objective of this project is to produce a practical guidance document on leg ulcer treatment, that may be applicable within the different clinical settings for leg ulcer treatment in Europe.
EWMA recommendations on negative pressure wound therapy (NPWT) These recommendations will describe the available NPWT devices (including their application and use), the health economic aspects of use of NPWT tech-nology and the eHealth perspectives on the use of NPWT technology.
Promoting appropriate use of antibiotics and non-antibiotic antimicrobial agents in wound careThe goal of this project is to develop a clinical deci-sion support tool. The tool will facilitate appropriate use of antibiotics and non-antibiotic antimicrobial agents in wound management.
Wound survey GermanyThe objective of the survey will be to identify the number and type of wounds under treatment, and provide an estimate of the resource consumption directly attributable to wound care at an organisa-tional level. This will be carried out in collaboration with the Ger-man Wound Organisation ICW.
Home care-wound care UKA guideline for wound care within the UK home care services will be developed, based on the recommen-dations provided by the EWMA Home Care - Wound Care document. This will be done in collaboration with relevant organisations in the UK.
EWMA recommendations for nurse educationThe recommendations will define learning outcomes related to the different levels of education. The objective is to eliminate inconsistencies in wound care education within European nurse education programmes.
At the end of the course, all participants will receive ref-erence documents related to the topics of the course and useful links for their future wound care practice.The quality of wound care is desperately lacking in many low-income countries. Advanced wound care does not require modern and expensive dressings, but it requires sound knowledge of wound physiology. We believe that the IUD program described here is a real opportunity to improve wound care in Cameroon and the surrounding region. Looking to the near future, our hope is to consolidate partnerships with universities (Yaoundé, Douala, Geneva), hospitals (HUG, Akonolinga, Ayos), and associations (Ca-WoCS, EWMA, WAWLC, SAfW, and Eloquent in South Africa) and to advocate for sustainable partnerships sup-porting improvements in wound care. By presenting this project at the EWMA Conference in Madrid in 2014 and to the EWMA Journal, we hope to reach networks and as-sociations who share our goals of fighting wounds specific to tropical conditions and improving wound care.
Companion documents:
n Innovation, Know-How and Technology in wound care. Peter Wowden. Marco Romanelli.Marie Muller. EWMA Journal . Vol.14 Number 1. May 2014.
n Wound Care Practice [by Paul J. Sheffield (Editor), Addrianne P. S. Smith (Editor), Caroline E. Fife (Editor)].
n Wound Care Practice, 2nd Edition, by Paul J. Sheffield (Editor), Caroline E. Fife (Editor [A1] ) Publisher: Best Publishing Company; 2nd edition (September 24, 2007) ISBN-10: 1930536380 ISBN-13: 978-1930536388
n Acute and chronic wounds; current management concepts. By Ruth A. Bryant and Denise P. Nix. 4th Edit Elsevier. Hardcover: 648 pages Publisher: Mosby; 4 edition (January 13, 2011) Language: English ISBN-10: 0323069436 ISBN-13: 978-0323069434
n LES SOINS DE PLAIE - GUIDE PRATIQUE Auteur COLLECTIF/AUTEUR, SAfW Section romande Editeur Médecine et Hygiène Langue Français Parution 15 nov. 2010 ISBN 978-2-88049-289-2
References
1. Ravisse et al. Une affection meconnue au Cameroon. L’ulcere a mycobacterie”. Medical. Tropical 1975;35:471-74
2. O’brien DP, Eric Comte, Micaela, Serafini, Genevieve Ehounou, Annick Antierens, Hubert Vuagnat, Vanesaa Christinet, Mitima Hamani.The urgent need for clinical, diagnostic and operational research for management of BU in Africa. Lancet Infect Dis. 2014 ;14(5) :435-40.
3. Depairon M, Vuagnat H. Ulcer management, a multidisciplinary approach. Praxis (bern 1994). 2008;20;97(4):165.
4. Walmsley, S. Advances in wound management: executive summary. In: Clinica Reports. Pjb Publications, ltd, London; 2002.
5. Vanessa Christinet, Caroline Di Benedetto, Alexandra Calmy, Eric Comte. Buruli et VIH : une interaction complexe et peu etudiee. Rev Med Suisse 2012;8:1792-3.
6. Teot L. The role of education in wound healing. Int J Low Extrem Wounds. 2006;5:9.
EWMA Journal 2014 vol 14 no 2

Wound healing has always had villains.Now it has a hero.
EXUDATE INFECTION BIOFILM
Our breakthrough new dressing attacks the key local barriers to wound healing, even biofilm.
T W O P O W E R F U L T E C H N O L O G I E SOur proven Hydrofiber™ Technology absorbs and retains excess exudate to help create an ideal
healing environment.*1-5 And now our revolutionary new Ag+ Technology destroys biofilm and kills infection-causing bacteria.*6-8
See how it helps you save the day at www.convatec.com.
®/™ Indicates trademarks of ConvaTec Inc. ©2014 ConvaTec Inc. AP-014181-MM
No dressing does more.
*As demonstrated in vitro^Defined as the ability to manage exudate, infection and biofilm, as demonstrated in vitro1. Newman GR, Walker M, Hobot JA, Bowler PG, 2006. Visualisation of bacterial sequestration and bacterial activity within hydrating Hydrober™ wound dressings. Biomaterials; 27: 1129-1139. 2. Walker M, Hobot JA, Newman GR, Bowler PG, 2003. Scanning electron microscopic examination of bacterial immobilization in a carboxymethyl cellulose (AQUACEL™) and alginate dressing. Biomaterials; 24: 883-890. 3. Bowler PG, Jones SA, Davies BJ, Coyle E, 1999. Infection control properties of some wound dressings. J. Wound Care; 8: 499-502. 4. Walker M, Bowler PG, Cochrane CA, 2007. In vitro studies to show sequestration of matrix metalloproteinases by silver-containing wound care products. Ostomy/Wound Management. 2007; 53: 18-25. 5. Assessment of the in vitro Physical Properties of AQUACEL EXTRA, AQUACEL Ag EXTRA and AQUACEL Ag+ EXTRA dressings. Scientific background report. WHRIA3817 TA297, 2013, Data on file, ConvaTec Inc. 6. Physical Disruption of Biofilm by AQUACEL® Ag+ Wound Dressing. Scientific Background Report. WHRI3850 MA232, 2013, Data on file, ConvaTec Inc. 7. Antimicrobial activity and prevention of biofilm reformation by AQUACEL™ Ag+ EXTRA dressing. Scientific Background Report. WHRI3857 MA236, 2013, Data on file, ConvaTec Inc. 8. Antimicrobial activity against CA-MRSA and prevention of biofilm reformation by AQUACEL™ Ag+ EXTRA dressing. Scientific Background Report. WHRI3875 MA239, 2013, Data on file, ConvaTec Inc.
ABSTRACTS OF RECENT COCHRANE REVIEWS
Sally Bell-Syer, MSc
Managing Editor Cochrane Wounds Group
Department of Health Sciences University of YorkUnited Kingdom
Correspondence:[email protected]
Conflict of interest: None
www.wounds.cochrane.org
Publication in The Cochrane Library Issue 2, 2014
Risk assessment tools for the prevention of pressure ulcersZena EH Moore, Seamus Cowman
Citation: Moore ZEH, Cowman S. Risk assessment tools for the prevention of pressure ulcers. Cochrane Database of Systematic Reviews 2014, Issue 2. Art. No.: CD006471. DOI: 10.1002/14651858.CD006471.pub3.
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: Use of pressure ulcer risk assessment tools or scales is a component of the assessment proc-ess used to identify individuals at risk of developing a pressure ulcer. Indeed, use of a risk assessment tool is recommended by many international pressure ulcer prevention guidelines, however it is not known whether using a risk assessment tool makes a difference to patient outcomes. We conducted a review to provide a summary of the evidence pertaining to pressure ulcer risk assessment in clinical practice.
Objectives: To determine whether using structured, systematic pressure ulcer risk assessment tools, in any health care setting, reduces the incidence of pressure ulcers.
Search methods: In December 2013, for this second update, we searched the Cochrane Wounds Group Specialised Register; The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library); Ovid MEDLINE; Ovid EMBASE; and EBSCO CINAHL.
Selection criteria: Randomised controlled trials (RCTs) comparing the use of structured, systematic, pressure ulcer risk assessment tools with no structured pressure ulcer risk assessment, or with unaided clinical judge-ment, or RCTs comparing the use of different struc-tured pressure ulcer risk assessment tools.
Data collection and analysis: Two review authors inde-pendently assessed titles and abstracts of the studies identified by the search strategy for eligibility, obtained full versions of potentially relevant studies and screened these against the inclusion criteria.
Main results: We included two studies in this review. One small, cluster randomised study found no statisti-cal difference in pressure ulcer incidence in patients who were assessed by nurses using the Braden risk assessment tool (n=74) compared with patients assessed by nurses who had receiving training and then used unstructured risk assessment (n=76) (RR 0.97, 95% CI 0.53 to 1.77) and those patients assessed by nurses using unstructured risk assessment alone (n=106) (RR 1.43, 95% CI 0.77 to 2.68) . The second study was a large single blind randomised controlled study which compared the effect of risk assessment on pressure ulcer incidence using the Waterlow risk assess-ment tool (n=411), the Ramstadius risk screening tool (n=420) and no formal risk assessment (n=420). There was no statistical difference in pressure ulcer incidence between the three groups (Waterlow 7.5% (n=31); Ramstadius 5.4% (n=22); clinical judgement 6.8% (n=28) (RR 1.10, 95% CI 0.68 to 1.81; Waterlow vs no formal risk assessment), (RR 0.79, 95% CI 0.46 to 1.35; Ramstadius vs no formal risk assessment), (RR 1.44, 95% CI 0.85 to 2.44; Waterlow vs Ramstadius).
Authors’ conclusions: Two studies were identified which evaluated the effect of risk assessment on patient outcomes; In one study, there was no statisti-cally significant difference in pressure ulcer incidence between people who were assessed using the Braden risk assessment tool compared with those receiving unstructured risk assessment. Methodological limita-tions of this study prevent firm conclusions being drawn. However, a further high quality RCT identified no statistical differences in pressure ulcer incidence when people were assessed using either the Waterlow risk assessment tool, the Ramstadius risk assessment tool, or using clinical judgement alone. There is no reli-able evidence to suggest that the use of structured, sys-tematic pressure ulcer risk assessment tools reduces the incidence of pressure ulcers.
Plain language summary:Risk assessment tools used for preventing pressure ulcersPressure ulcers (also known as bed sores, pressure sores and decubitus ulcers) are areas of localised injury to the skin, underlying tissue or both, usually over a bony prominence, as a result of pressure, or pressure in combination with shear (tissue distortion resulting from squeezing and stretching soft tissues between bony
Cochrane Reviews
EWMA Journal 2014 vol 14 no 2 61

structures and the skin). Pressure ulcers mainly occur in people who have limited mobility, nerve damage or both. Pressure ulcer risk assessment is part of the process used to identify individuals at risk of developing a pressure ulcer. Risk assessments generally use checklists and their use is recommended by pressure ulcer prevention guidelines. This review found two studies that were eligible for inclusion. The first study found no difference in the number of new pressure ulcers that developed in individuals assessed using the Braden risk assessment compared with an unstructured risk assessment. However, there were methodologi-cal limitations with this study. The second study also found no differences in the number of new pressure ulcers that developed in individuals assessed using the Waterlow risk assessment tool, the Ramstadius risk assessment tool, or using clinical judgement alone. This study did not have methodological limitations. Therefore, to date, there are no studies to suggest that the use of risk assessment tools, reduces the number of new pressure ulcers that develop.
Publication in The Cochrane Library Issue 3, 2014
Prophylactic antibiotics to prevent surgical site infection after breast cancer surgery
Daniel J Jones, Frances Bunn, Sophie V Bell-Syer
Citation: Jones DJ, Bunn F, Bell-Syer SV. Prophylactic antibiotics to prevent surgical site infection after breast cancer surgery. Cochrane Database of Systematic Reviews 2014, Issue 3. Art. No.: CD005360. DOI: 10.1002/14651858.CD005360.pub4.
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: Surgery has been used as part of breast cancer treatment for centuries; however any surgical procedure has the potential risk of infection. Infection rates for surgical treatment of breast cancer are documented at between 3% and 15%, higher than average for a clean surgical procedure. Pre- and perioperative antibiotics have been found to be useful in lower-ing infection rates in other surgical groups, yet there is no con-sensus on the use of prophylactic antibiotics for breast cancer surgery.
Objectives: To determine the effects of prophylactic (pre- or perioperative) antibiotics on the incidence of surgical site infec-tion (SSI) after breast cancer surgery.
Search methods: For this third update we searched the Cochrane Wounds Group Specialised Register (5 December 2013); the Cochrane Central Register of Controlled Trials (CEN-TRAL) (The Cochrane Library); the Database of Abstracts of Reviews of Effects (DARE) (The Cochrane Library); Ovid MEDLINE; Ovid MEDLINE (In-Process & Other Non-Indexed Citations); Ovid EMBASE; and EBSCO CINAHL. We applied no language or date restrictions.
Selection criteria: Randomised controlled trials of pre- and peri-operative antibiotics for patients undergoing surgery for breast cancer were included. Primary outcomes were rates of surgical site infection (SSI) and adverse reactions.
Data collection and analysis: Two review authors independently examined the title and abstracts of all studies identified by the search strategy, then assessed study quality and extracted data from those that met the inclusion criteria.
Main results: A total of eleven studies (2867 participants) were included in the review. Ten studies evaluated preoperative anti-biotic compared with no antibiotic or placebo. One study evalu-ated perioperative antibiotic compared with no antibiotic. Pool-ing of the results demonstrated that prophylactic antibiotics administered preoperatively significantly reduce the incidence of SSI for patients undergoing breast cancer surgery without recon-struction (pooled risk ratio (RR) 0.67, 95% confidence interval (CI) 0.53 to 0.85). Analysis of the single study comparing peri-operative antibiotic with no antibiotic found no statistically signif-icant effect of antibiotics on the incidence of SSI (RR 0.11, 95% CI 0.01 to 1.95). No studies presented separate data for patients who underwent reconstructive surgery at the time of removal of the breast tumour.
Authors’ conclusions: Prophylactic antibiotics administered pre-operatively reduce the risk of SSI in patients undergoing surgery for breast cancer. Further studies involving patients undergoing immediate breast reconstruction are needed as studies have identified this group as being at higher risk of infection than those who do not undergo immediate breast reconstruction.
Plain language summary:Antibiotics to prevent surgical site infection after breast cancer surgeryBreast cancer accounts for one in 10 of all new cancer cases diagnosed and surgical removal of the breast is a common treat-ment approach. An infection of the surgical wound is often a complication of surgery and taking antibiotics just before the operation significantly reduces the chances of developing an infection. The review is not able to establish which antibiotic is most appropriate. No trials were found which considered the effect of antibiotics when the operation involved immediate breast reconstruction.
Publication in The Cochrane Library Issue 4, 2014
Repositioning for pressure ulcer prevention in adults
Brigid M Gillespie, Wendy P Chaboyer, Elizabeth McInnes, Bridie Kent, Jennifer A Whitty, Lukman Thalib
Citation: Gillespie BM, Chaboyer WP, McInnes E, Kent B, Whitty JA, Thalib L. Repositioning for pressure ulcer prevention in adults. Cochrane Database of Systematic Reviews 2014, Issue 4. Art. No.: CD009958. DOI: 10.1002/14651858.CD009958.pub2.
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: A pressure ulcer (PU), also referred to as a ‘pres-sure injury’, ‘pressure sore’, or ‘bedsore’ is defined as an area of localised tissue damage that is caused by unrelieved pressure, friction or shearing forces on any part of the body. PUs com-
EWMA Journal 2014 vol 14 no 2 62

monly occur in patients who are elderly and less mobile, and carry significant human and economic impacts. Immobility and physical inactivity are considered to be major risk factors for PU development and the manual repositioning of patients in hospi-tal or long-term care is a common pressure ulcer prevention strategy.
Objectives: The objectives of this review were to:1) assess the effects of repositioning on the prevention of PUs in
adults, regardless of risk or in-patient setting;2) ascertain the most effective repositioning schedules for pre-
venting PUs in adults; and3) ascertain the incremental resource consequences and costs
associated with implementing different repositioning regi-mens compared with alternate schedules or standard prac-tice.
Search methods: We searched the following electronic data-bases to identify reports of the relevant randomised controlled trials: the Cochrane Wounds Group Specialised Register (searched 06 September 2013), the Cochrane Central Register of Controlled Trials (CENTRAL) (2013, Issue 8); Ovid MEDLINE (1948 to August, Week 4, 2013); Ovid EMBASE (1974 to 2013, Week 35); EBESCO CINAHL (1982 to 30 August 2013); and the reference sections of studies that were included in the review.
Selection criteria: Randomised controlled trials (RCTs), pub-lished or unpublished, that assessed the effects of any reposi-tioning schedule or different patient positions and measured PU incidence in adults in any setting.
Data collection and analysis: Two review authors independently performed study selection, risk of bias assessment and data extraction.
Main results: We included three RCTs and one economic study representing a total of 502 randomised participants from acute and long-term care settings. Two trials compared the 30º and 90º tilt positions using similar repositioning frequencies (there was a small difference in frequency of overnight repositioning in the 90º tilt groups between the trials). The third RCT compared alternative repositioning frequencies. All three studies reported the proportion of patients develop-ing PU of any grade, stage or category. None of the trials reported on pain, or quality of life, and only one reported on cost. All three trials were at high risk of bias. The two trials of 30º tilt vs. 90º were pooled using a random effects model (I² = 69%) (252 participants). The risk ratio for developing a PU in the 30º tilt and the standard 90º position was very imprecise (pooled RR 0.62, 95% CI 0.10 to 3.97, P=0.62, very low quality evidence). This comparison is under-powered and at risk of a Type 2 error (only 21 events). In the third study, a cluster randomised trial, participants were randomised between 2-hourly and 3-hourly repositioning on standard hospital mattresses and 4 hourly and 6 hourly repo-sitioning on viscoelastic foam mattresses. This study was also underpowered and at high risk of bias. The risk ratio for pressure ulcers (any category) with 2-hourly repositioning compared with 3-hourly repositioning on a standard mattress was imprecise (RR 0.90, 95% CI 0.69 to 1.16, very low quality evidence). The risk ratio for pressure ulcers (any category) was compatible with a large reduction and no difference between 4-hourly reposition-
ing and 6-hourly repositioning on viscoelastic foam (RR 0.73, 95% CI 0.53 to 1.02, very low quality evidence). A cost-effectiveness analysis based on data derived from one of the included parallel RCTs compared 3-hourly repositioning using the 30º tilt overnight with standard care consisting of 6-hourly repositioning using the 90º lateral rotation overnight. In this evaluation the only included cost was nursing time. The intervention was reported to be cost saving compared with standard care (nurse time cost per patient €206.6 vs €253.1, incremental difference €-46.5; 95%CI: €-1.25 to €-74.60).
Authors’ conclusions: Repositioning is an integral component of pressure ulcer prevention and treatment; it has a sound theoreti-cal rationale, and is widely recommended and used in practice. The lack of robust evaluations of repositioning frequency and position for pressure ulcer prevention mean that great uncer-tainty remains but it does not mean these interventions are inef-fective since all comparisons are grossly underpowered. Current evidence is small in volume and at risk of bias and there is cur-rently no strong evidence of a reduction in pressure ulcers with the 30° tilt compared with the standard 90º position or good evidence of an effect of repositioning frequency. There is a clear need for high-quality, adequately-powered trials to assess the effects of position and optimal frequency of repositioning on pressure ulcer incidence. The limited data derived from one economic evaluation means it remains unclear whether repositioning every 3 hours using the 30º tilt is less costly in terms of nursing time and more effective than standard care involving repositioning every 6 hours using a 90º tilt.
Plain language summary:Repositioning to prevent pressure ulcersPressure ulcers, also called pressure injury, pressure sores, decu-bitus ulcers and bed sores are caused by pressure, rubbing or friction at the weight-bearing bony points of the body (such as hips, heels and elbows). A pressure ulcer is characterised by an area of localised injury to the skin or underlying tissue over a bony prominence that results from pressure or shearing, or a combination of both. Pressure ulcers most commonly occur in the elderly, or those who are immobile, either when in bed or sitting. Repositioning (i.e. turning) is one strategy used alongside other preventative strategies to relieve pressure, and so prevent development of pressure ulcers. Repositioning involves moving the person into a different position to remove or redistribute pressure from a particular part of the body. We identified three studies which recruited 502 people. Evi-dence to support the use of repositioning to prevent pressure ulcers is low in volume and quality and we still do not know if particular positions or frequencies of repositioning reduce pres-sure ulcer development. None of the trials reported on pain or quality of life. There is a need for further research to measure the effects of repositioning on pressure ulcer development and to find the best repositioning regimen in terms of frequency and position. It is important to emphasise that this lack of evidence showing that repositioning is effective or which repositioning reg-imen is the best does not mean that repositioning is ineffective.
Cochrane Reviews
EWMA Journal 2014 vol 14 no 2 63

Publication in The Cochrane Library Issue 5, 2014
Intermittent pneumatic compression for treating venous leg ulcersE Andrea Nelson, Alex Hillman, Kate Thomas
Citation: Nelson EA, Hillman A, Thomas K. Intermittent pneu-matic compression for treating venous leg ulcers. Cochrane Database of Systematic Reviews 2014, Issue 5. Art. No.: CD001899. DOI: 10.1002/14651858.CD001899.pub4.
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: Intermittent pneumatic compression (IPC) is a mechanical method of delivering compression to swollen limbs that can be used to treat venous leg ulcers and limb swelling due to lymphoedema.
Objectives: To determine whether IPC increases the healing of venous leg ulcers. To determine the effects of IPC on health related quality of life of venous leg ulcer patients.
Search methods: In April 2014, for this third update, we searched the Cochrane Wounds Group Specialised Register; the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library); Ovid MEDLINE; Ovid MEDLINE (In-Process & Other Non-Indexed Citations); Ovid EMBASE; and EBSCO CINAHL.
Selection criteria: We included randomised controlled trials (RCTs) that compared the effects of IPC with control (sham IPC or no IPC) or made comparisons between IPC treatment regi-mens, in venous ulcer management.
Data collection and analysis: Two review authors reviewed titles and abstracts and agreed on full studies to be retrieved. One review author extracted data and assessed studies for risk of bias and this was checked by a second review author.
Main results: We identified nine randomised controlled trials (including 489 people in total). Only one trial was at low risk of bias overall having reported adequate randomisation, allocation concealment and blinded outcome assessment. In one trial (80 people) more ulcers healed with IPC than with dressings (62% vs 28%; p=0.002). Five trials compared IPC plus compression with compression alone. Two of these (97 people) found increased ulcer healing with IPC plus compression than with compression alone. The remaining three trials (122 people) found no evidence of a benefit for IPC plus compression compared with compression alone. Two trials (86 people) found no difference between IPC (without additional compression) and compression bandages alone. One trial (104 people) compared different ways of delivering IPC and found that rapid IPC healed more ulcers than slow IPC (86% vs 61%).
Authors’ conclusions: IPC may increase healing compared with no compression. It is unclear whether it can be used instead of compression bandages. There is some limited evidence that IPC may improve healing when added to compression bandages.
Rapid IPC was better than slow IPC in one trial. Further trials are required to determine the reliability of current evidence, which patients may benefit from IPC in addition to compression band-ages, and the optimum treatment regimen.Plain language summary:Intermittent pneumatic compression for treating venous leg ulcers.Venous leg ulcers (open sores) can be caused by a blockage or breakdown in the veins of the leg. Compression, using bandages or hosiery (stockings), can help heal ulcers. However, they do not always work, and some people are not willing or able to wear them. Intermittent pneumatic compression (IPC) uses an air pump to inflate and deflate an airtight bag wrapped around the leg. This technique is also used to stop blood clots develop-ing during surgery. However, the review of trials found conflict-ing evidence about whether or not IPC is better than compres-sion bandages and hosiery. Intermittent pneumatic compression (IPC) is better for healing leg ulcers than no compression. Some studies suggest IPC might be a beneficial addition to bandages for some ulcers, but these studies might be biased. Delivering the IPC therapy in a rapid manner by inflating and deflating the IPC device more quickly resulted in more ulcers being healed than with a slower deflation regime.
Publication in The Cochrane Library Issue 6, 2014
Nutritional interventions for preventing and treating pressure ulcersGero Langer, Astrid Fink
Citation: Langer G, Fink A. Nutritional interventions for prevent-ing and treating pressure ulcers. Cochrane Database of System-atic Reviews 2014, Issue 6. Art. No.: CD003216. DOI: 10.1002/14651858.CD003216.pub2.
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: Pressure ulcers affect approximately 10% of people in hospitals and older people are at highest risk. A correlation between inadequate nutritional intake and the development of pressure ulcers has been suggested by several studies, but the results have been inconsistent.
Objectives: To evaluate the effects of enteral and parenteral nutrition on the prevention and treatment of pressure ulcers.
Search methods: In March 2014, for this first update, we searched The Cochrane Wounds Group Specialised Trials Regis-ter, the Cochrane Central register of Controlled Trials (The Cochrane Library), the Database of Abstracts of Reviews of Effects (DARE) (The Cochrane Library), the Health Technology Assessment Database (HTA) (The Cochrane Library), the Cochrane Methodology Register (The Cochrane Library), NHS Economic Evaluation Database (The Cochrane Library), Ovid Medline, Ovid Embase and EBSCO CINAHL. No date, language or publication status limits were applied.
Selection criteria: Randomised controlled trials (RCTs) evaluat-ing the effects of enteral or parenteral nutrition on the preven-tion and treatment of pressure ulcers, which measured the inci-
EWMA Journal 2014 vol 14 no 2 64

dence of new ulcers, ulcer healing or changes in pressure ulcer severity. There were no restrictions on types of patient, setting, date, publication status or language.
Data collection and analysis: Two review authors independently screened for inclusion, and disagreement was resolved by dis-cussion. Two review authorsindependently extracted data and assessed quality using the Cochrane Collaboration tool for assessing risk of bias.
Main results: We included 23 RCTs, many were small (between 9 and 4023 participants, median 88) and at high risk of bias.Eleven trials compared a combination of nutritional supple-ments, consisting of a minimum of energy and protein in differ-ent dosages, for the prevention of pressure ulcers. A meta-analy-sis of eight trials (6062 participants) that compared the effects of mixed nutritional supplements with standard hospital diet found no clear evidence of an effect of supplementation on pressure ulcer development (pooled RR 0.86; 95% CI 0.73 to 1.00; P value 0.05; I2 = 13%, random effects). This outcome is at unclear or high risk of bias. Fourteen trials evaluated the effects of nutritional supple-ments on the healing of existing pressure ulcers: seven trials examined mixed nutritional supplements, three the effects of proteins, two trials examined zinc, and two studies examined ascorbic acid. The included trials were heterogeneous with regard to participants, interventions, comparisons and outcomes and meta-analysis was not appropriate. There was no clear evi-dence of an improvement in pressure ulcer healing from the nutritional supplements evaluated in any of these individual studies.
Authors’ conclusions: There is currently no clear evidence of a benefit associated with nutritional interventions for either the prevention or treatment of pressure ulcers. Further trials of high methodological quality are necessary.
Plain language summary:Dietary supplementation for preventing and treating pressure ulcersBackground: Pressure ulcers (also called bed sores) are wounds caused by pressure at the weight-bearing, bony points of immo-bilised people (such as hips, heels and elbows). Poor nutritional status, or dehydration, may weaken the skin and make people more vulnerable to developing pressure ulcers. Once a pressure ulcer has developed, it can become very large and difficult to heal.Review question: We wanted to find out whether changing the diet (for example by giving supplements) could prevent the development of pressure ulcers. We also wanted to find out if dietary changes could help heal pressure ulcers that had already occurred. The review of trials found that there is no clear evidence that nutritional interventions reduce the number of people who develop pressure ulcers or help the healing of existing pressure ulcers. More research is needed.
Perioperative corticosteroids for preventing com-plications following facial plastic surgery
Edina MK da Silva, Bernardo Hochman, Lydia M Ferreira
Citation: da Silva EMK, Hochman B, Ferreira LM. Perioperative corticosteroids for preventing complications following facial plas-tic surgery. Cochrane Database of Systematic Reviews 2014, Issue 6. Art. No.: CD009697. DOI: 10.1002/14651858.CD009697.pub2.
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: Early recovery is an important factor for people undergoing facial plastic surgery. However, the normal inflam-matory processes that are a consequence of surgery commonly cause oedema (swelling) and ecchymosis (bruising), which are undesirable complications. Severe oedema and ecchymosis delay full recovery, and may make patients dissatisfied with pro-cedures.Perioperative corticosteroids have been used in facial plastic surgery with the aim of preventing oedema and ecchymo-sis.
Objectives: To determine the effects, including safety, of periop-erative administration of corticosteroids for preventing complica-tions following facial plastic surgery in adults.
Search methods: In January 2014, we searched the following electronic databases: the Cochrane Wounds Group Specialised Register; the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library); Ovid MEDLINE; Ovid MEDLINE (In-Process & Other Non-Indexed Citations); Ovid Embase; EBSCO CINAHL; and Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS). There were no restrictions on the basis of date or language of publication.
Selection criteria: We included RCTs that compared the admin-istration of perioperative systemic corticosteroids with another intervention, no intervention or placebo in facial plastic surgery.
Data collection and analysis: Two review authors independently screened the trials for inclusion in the review, appraised trial quality and extracted data.
Main results: We included 10 trials, with a total of 422 partici-pants, that addressed two of the outcomes of interest to this review: swelling (oedema) and bruising (ecchymosis). Nine stud-ies on rhinoplasty used a variety of different types, and doses, of corticosteroids. Overall, the results of the included studies showed that there is some evidence that perioperative adminis-tration of corticosteroids decreases formation of oedema over the first two postoperative days. Meta-analysis was only possible for two studies, with a total of 60 participants, and showed that a single perioperative dose of 10 mg dexamethasone decreased oedema formation in the first two days after surgery (SMD = -1.16, 95% CI: -1.71 to -0.61, low quality evidence). The evi-dence for ecchymosis was less consistent across the studies, with some contradictory results, but overall there was some evidence that perioperatively administered corticosteroids decreased ecchymosis formation over the first two days after surgery (SMD
Cochrane Reviews
EWMA Journal 2014 vol 14 no 2 65

= -1.06, 95% CI:-1.47 to -0.65, two studies, 60 participants, low quality evidence ). The difference was not maintained after this initial period. One study, with 40 participants, showed that high doses of methylprednisolone (over 250 mg) decreased both ecchymosis and oedema between the first and seventh postop-erative days. The only study that assessed facelift surgery identi-fied no positive effect on oedema with preoperative administra-tion of corticosteroids. Five trials did not report on harmful (adverse) effects; four trials reported that there were no adverse effects; and one trial reported adverse effects in two participants treated with corticosteroids as well as in four participants treated with placebo. None of the studies reported recovery time, patient satisfaction or quality of life. The studies included were all at an unclear risk of selection bias and at low risk of bias for other domains.
Authors’ conclusions: There is limited evidence for rhinoplasty that a single perioperative dose of corticosteroids decreases oedema and ecchymosis formation over the first two postopera-tive days, but the difference is not maintained after this period. There is also limited evidence that high doses of corticosteroids decrease both ecchymosis and oedema between the first and seventh postoperative days. The clinical significance of this decrease is unknown and there is little evidence available regarding the safety of this intervention. More studies are needed because at present the available evidence does not sup-port the use of corticosteroids for prevention of complications following facial plastic surgery.
Plain language summary:Corticosteroids for preventing complications following facial plastic surgeryComplications following facial plastic surgery: Today, facial plas-tic surgery is one of the most common types of surgery. People frequently chose to have it for aesthetic (beauty) reasons, so doctors need to minimise the unpleasant effects (complications) associated with these procedures. All surgical procedures pro-duce an inflammatory response, which may cause swelling and bruising. Severe swelling and bruising are troublesome for patients, as they delay full recovery.
Why corticosteroids might help: Corticosteroids, more often known as ‘steroids’, are medicines that doctors prescribe to reduce inflammation in a wide range of conditions. They are commonly used in facial plastic surgery to reduce swelling and bruising, though it is not known how efficient or safe they might be.
The purpose of this review: This review tried to find out whether giving corticosteroids around the time of facial plastic surgery reduces swelling and bruising compared to another intervention, no intervention, or a fake medicine (placebo).
Findings of this review: The review authors searched the medical literature up to January 2014, and identified 10 relevant medical trials, with a total of 422 participants. Nine of these studies were on people having rhinoplasty (surgery to reshape the nose) and one was on people having a facelift.The trials investigated a variety of corticosteroid medicines, as well as different doses of corticosteroids. People in the studies were assessed for swelling and bruising for up to 10 days after surgery. None of the studies stated the funding source. There was some low quality evidence that a single dose of corticosteroid administered prior to surgery might reduce swell-ing and bruising over the first two days after surgery, but this advantage was not maintained beyond two days. One study, with 40 participants, showed that high doses of corticosteroid decreased both swelling and bruising between the first and sev-enth postoperative days. The usefulness of these results is uncer-tain and there is currently no evidence regarding the safety of the treatment. Five trials did not report on harmful (adverse) effects; four trials reported that there were no adverse effects; and one trial reported adverse effects in two participants treated with corticosteroids as well as in four participants treated with placebo. None of the studies reported recovery time, patient sat-isfaction or quality of life. Therefore, the current evidence does not support use of cor-ticosteroids as a routine treatment in facial plastic surgery. More trials will need to be conducted before it can be established whether this treatment works and is safe. m
Cochrane Reviews
EWMA Journal 2014 vol 14 no 2 66

Submit your next paper to
Organ der Deutschen Gesellschaft für Phlebologie
Organ der Schweizerischen Gesellschaft für Phlebologie, Bulletin de la Société Suisse de Phlébologie
Organ der Arbeitsgemeinschaft Dermatologische Angio-logie der Deutschen Dermatologischen Gesellschaft
Organ des Berufsverbandes der Phlebologen e.V.
Als Forum für die europäische phlebologische Wissenschaft widmet sich die CME-zertifizierte Zeitschrift allen relevanten phlebologischen Themen in Forschung und Praxis: Neue diagnostische Verfahren, präventivmedizinische Fragen sowie therapeutische Maßnahmen werden in Original- und Über-sichtsarbeiten diskutiert.
Die offiziellen Mitteilungen und Leitlinien der Deutschen Gesellschaft für Phlebologie werden regelmäßig publiziert, verschiedene Foren bieten Gelegenheit zum Erfahrungsaus-tausch zwischen Klinik und Praxis.
2015. 44. Jahrgang | 6 Hefte jährlich | ISSN 0939-978X
www.phlebologieonline.de
1407191.indd 1 07.08.2014 15:20:53

EWMA Journal Previous Issues
The EWMA Journals can be downloaded free of charge from www.ewma.org
Other JournalsEWMA wishes to facilitate the exchange of informa-tion on wound healing in a broad perspective with this section on International Journals.
Helcos, vol. 25, no. 2, 2014
Efficacy for preventing pressure ulcers of the virgin extra olive oil versus hyper-oxygenated fatty acids: intemediate results from a non-inferiory trialAntonio Diaz Valenzuela et al.Development of a protocol for the management of surgical wound in neck surgery. An effective and efficient treatment in laryngectomized patientsAntonio Rodriguez Valiente et al
Spanish
Haava, no. 2, 2014www.shhy.fi
Surgical Wound and Related ProblemsMikko TuulirantaGunshot Woundsed. Mikko Tuuliranta based on Tim Soderlund’s lectureBites – Crushes – Puncture Wounds caused by Animals and Humansed. Mikko Tuuliranta based on Leena Berg’s lectureImpact of Smoking to Wound Healinged. Mikko Tuuliranta based on Anne Flink’s lectureSkin Transplant TechniquesHeli KavolaManagement of Skin Crafts and Donor SiteHeli KallioDocumentation in Wound CareUlla-Mari KinnunenDeveloping Competence in Wound CareLeena Jalonen & Minna YlönenStop Pressure Ulcer – Campaing Reached Health Profes-sionals Maarit Ahtiala – The Unique Way to PresentAnsa Iivanainen & Heli Kallio Wound Care – Today and in the FutureAnsa Iivanainen, Tiina PukkiUnrealized Dream Sharifee Zarghounah
Finnish
Acta Vulnologica, vol. 12, no 2, 2014www.vulnologia.it
Gestione manageriale del paziente portatore di ulcere cutanee croniche: i percorsi clinico assistenziali nell’ottica del problem solvingSpano L. A, Cocchieri C, Pierangeli M, Tartaglione C, Bolletta E, Scalise AAttività antibatterica e anti-proliferativa in vitro di sulfa-diazina argentica utilizzata da sola e associata con acido ialuronicoFigura N, Biagi M, Collodel G, Gonnelli S, Moretti EPercorsi diagnostici e terapeutici delle lesioni cutaneeBasso G, et al.L’utilizzo della pressione topica negativa nelle medicazioni difficili: casistica clinica esaminata presso l’Ambulatorio di Chirurgia Vascolare Azienda Ulss 18 RovigoMocellin S, Schiesaro S, Ruzza L, Girotto E
Italian
Volume 13, no 1, April 2013
The Biofilm-forming capacity of staphylococcus aureus from chronic wounds can be useful for determining Wound-Bed Preparation methodsY. Yarets, L. Rubanov, I. Novikova, N. ShevchenkoIn vitro efficacy of various topical antimicrobial agents against multidrug-resistant bacteriaM. Hajská, L. Slobodníková, H. Hupková, J. KollerThe mTOR inhibitors and the skin wound healingF. Benhadou, V. del MarmolA Review of Evidence for Negative Pressure Wound Therapy (NPWT) use Post Spinal SurgeryR. A. Atkinson, K. J. Ousey, S. Lui, J. B. WilliamsonA randomized study on the effectiveness of a new pressure-relieving mattress overlay for the prevention of pressure ulcers in elderly patients at riskE. Ricci, C. Roberto, A. Ippolito, A. Bianco, M. T. ScaliseMotorcycle ride position, venous return, and symptoms of chronic venous insufficiencyEllie Lindsay, P. Vowden, K. Vowden, J. Megson Archagathus – History’s first wound expertE. Ricci
Volume 13, no 2, October 2013
Risk assessment scales for pressure ulcers in intensive care units: A systematic review with meta-analysisF. P. García-Fernández et al.Pressure-time integral of elastic versus inelastic bandages H. Partsch, G. MostiVERUM – A European approach for successful venous leg ulcer healingR. Brambilla et al. Effect of topical haemoglobin on venous leg ulcer healingM. Arenbergerova et al.The effects of an arginine-enriched oral nutritional supplement on chronic wound healing in non-malnourished patientsJ. Schols et al.Efficacy of honey gel in the treatment of chronic lower leg ulcersO. Tellechea et al.
Volume 14, no 1, May 2014
Prevalence of Pressure Ulcers in Hospitalized Patients in GermanyHeidi Heinhold, Andreas Westerfellhaus, Knut Kröger Excess use of antibiotics in patients with non-healing ulcersMarcus Gürgen Regenerative medicine in burn wound healing: Aiming for the perfect skinMagda MW Ulrich Promising effects of arginine-enriched oral nutritional supple-ments on wound healingJos M.G.A. Schols Efficacy of platelet-rich plasma for the treatment of chronic woundsVladimir N. Obolenskiy, Darya A. Ermolova, Leonid A. Laberko, Tatiana V. Semenova
Advances in Skin & Wound Care, vol. 27, sep, 2014www.aswcjournal.com
Wounds in Patients with HIVAlexander McMeeking, In Kim, BS, Frank Ross, Elizabeth A Ayello, Harold Brem, Patrick Linton, Daniel K. O’NeillExcision, Skin Grafting, Corticosteroids, AdjuvantRadio-therapy, Pressure Therapy, and Emancipation! The ESCAPE Model for Successful Taming of Giant Auricular KeloidsZulqarnain Masoodi, Imran Ahmad, M Fahud Khurram, Ansarul Haq, MCh-StdThe Pieper-Zulkowski Pressure Ulcer Knowledge TestBarbara Pieper, Karen Zulkowski
English
Volume 12, no 3, October 2012
Therapeutic strategies for diabetic foot ulcerationRJ Hinchliffe, JRW BrownriggOffloading the diabetic foot: Evidence and clinical decision makingS.A. BusSoft-tissue complications during treatment of children with congenital clubfootA. Baindurashvili, V. Kenis, Y. StepanovaAn evolution in Medical Tapes: From Latex to AcrylicL. GrysonBacteria and fungus binding mesh in negative pressure wound therapy – A review of the biological effects in the wound bedM. Malmsjö, S. Lindstedt, R. Ingemansson, L. Gustafsson
EWMA Journal 2014 vol 14 no 2 68
Wund Management, vol. 8, no 4, 2014 English abstracts are available from www.mhp-verlag.de
W.A.R. scores in patients with chronic leg ulcers: Results of a multicentre studyF. Jockenhöfer et al.Leg ulcers due to vasculitis: How much serologic diagnostic is meaningful?M. Stoffels-Weindorf, et al.How to treat this wound?K. Kröger et al.
German
Wounds (SÅR) vol. 22, no 2, 2014www.saar.dkThe challenges of sense making in the change project – implementation of pressure ulcer prevention effortsAnnette NW North, Helene Su-Min Ting DanielsenBiatain® silicone dressings: A case series evaluationChadwick P, et.alPressure ulcer – an adverse event – also in the municipalitiesBirgit AndersenPodiatrists are firmly rooted in the interdisciplinary cooperationJens FonnesbechThe field of amputation is missing enthusiasts – first conference on amputationJens FonnesbechPhototherapy as wound care – experiences from the treatment of a patientJelena Suljevic
Scandinavian
Journal of Wound Care, vol. 23, no 7, 2014www.journalofwoundcare.com
The effect of a ceramide-containing dressing in preventing pressure ulcers K. H. ParkA novel approach to reconstruct a large full thickness abdominal wall defect: Successful treatment with Matriderm® and Split E. Tong, F. Martin, O. ShelleyThe Fitzpatrick Skin Type Scale: A reliability and validity study in women undergoing radiation therapy for breast cancerO. Fasugba, A. Gardner, W. SmythPressure ulcer risk assessment and prevention: What difference does a risk scale make? A comparison between Norway and IrelandE. Johansen, Z. Moore, M. van Etten, H. Strapp
English
Phlebologie, no 4, 2014www.schattauer.de
Venous leg ulcer after acupuncture treatmentP. Gkogkolou, M. B. Lorenz, T. GoergeSourcing: Which varicose vein is relevant to the ulcer?M. Niemer, A. Miesel, B. KahleGenital lymphoedema as an early symptom of a signet-ring cell carcinomaT. Hirsch, H. UhlemannFoam sclerotherapy of a large postoperativeseroma after inguinal lymph node excisionL. Trog, A. L. Recke, B. KahlePrimary leiomyosarcoma of the venous vessel wall – A rare, fascinating case from routine vascular surgery and phlebologyJ. Bode, F. WolterA rare case: Vena cava inferior agenesis with aberrant hepatic vein in an asymptomatic patientT. O. Kalayci, et.alLong-term results after radiofrequency ablation in 1998T. Noppeney, A. Brunner, J. Noppeney,Patient positioning for duplex ultrasound scanning of the leg vesselsM. Marshall, C. Schwahn-Schreiber, M.-W. KleineDuplex Ultrasound investigation of perforating veinsE. Mendoza
German
Sårmagasinet vol. 1, no 1, 2014www.ntvw.nl
Theme Pressure ulcersFocus EPUAP, StockholmFrom shame to success, the journey of a geriatric hospitalSit/and position change clinicsPaediatric pressure ulcersPUCLAS 3New Clinical guidelines, pressure ulcersPressure ulcers in the spinal cord injuredPressure ulcers an African initiative
Swedish
Rane vol. 4, no 1, 2013www.lecenjerana.comNovel AG /alginate nanocomposites for wound treatments: animal studiesJasmina Stojkovska, et.alClinical forms of plantar necrotising fasciitisCedomir S Vucetic, et.alThe significance of D - dimer in early diagnosis of deep vein thrombosis in coagulation disorder patients (abstract)Ivana JelicThe possibilities of use of dermoscopy as a diagnostic method in chronic venous insufficiency and chronic venous ulceration (abstract)Javorka B. Delic, Vesna Mikulic
English
Lietuvos chirurgija, vol. 13, no 2, 2014www.chirurgija.lt
Colorectal cancer: is it possible to prevent it?Escalante RHemorrhoids and anal fissures during pregnancy and after child-birth: prevalence, risk factors and impact on women’s quality of lifeBuzinskiene D, Drasutiene G, Poskus TThe multimodal treatment of rectoceleDelgadillo-Pfenninger XElective colectomy after colonoscopic polypectomy for unexpected polypoid T1 cancerSamuolis N, Samalavicius NE, Mickys UEndoscopic treatment of fistulae, perforations and anastomotic leaks of the digestive tract with the OTSC clip (OVESCO)Radziūnas G, Kildusienū I, Stanaitis J, Krasauskas A, Samalavicius NE
Lithuanian
Leczenie Ran vol. 11, no 3, 2014
Protein metabolism in the patients with thermal injuryKucharzewski M, Ryszkiel I, Wilemska-Kucharzewska K, Rojczyk-Gołūbiewska E, Pałasz AThe evaluation of chosen extracellular matrix enzymes activity during regeneration of experimental thermal injuriesOlczyk P, Komosiūska-Vassev K, Winsz-Szczotka K, Stojko J, Klimek K, Gajewski K, Olczyk KThe speed of healing process of the leg venous ulcer after appli-cation of the foam dressing with silver ions – own experienceKucharzewski M, Mieszczaūsk P, Wilemska-Kucharzewska KIn vitro evaluation of the single and multispecies biofilm preven-tion capabilities of two wound irrigation solutions and a topical antisepticWestgate SJ, Cutting KC
Polish
Int. Journal of Lower Extremity Wounds vol. 13, no 3, 2014http://ijlew.sagepub.com
How to Cope With the Increasing Burden of the Diabetic Foot: “Better Three Hours Too Soon Than a Minute Too LateNikolaos Papanas, Raj ManiTransformation of the Multidisciplinary Diabetic Foot Clinic Into a Multidisciplinary Diabetic Foot Day Unit: Results From a Service EvaluationChris A. Manu et al.Role of Polymeric Biomaterials as Wound Healing AgentsPriyanka Agrawal et al.High Matrix Metalloproteinase Levels Are Associated With Dermal Graft Failure in Diabetic Foot UlcersValentina Izzo et al.Gender Differences of Lower Extremity Amputation Risk in Patients With Diabetic Foot: A Meta-AnalysisZhu-Qi Tang, Hong-Lin Chen, Fang-Fang Zhao
English
Journal of Tissue Viability, vol. 23, no 2, 2014www.journaloftissueviability.com
Personalized prediction of chronic wound healing: An exponen-tial mixed effects model using stereophotogrammetric measure-mentY. Xu, J. Sun, R.R. Carter, K.M. BogieUsing an extreme bony prominence anatomical model to examine the influence of bed sheet materials and bed making methods on the distribution of pressure on the support surfaceT. Iuchi, Y. Nakajima, M. Fukuda, J. Matsuo, H. Okamoto, H. Sanada, J. SugamaEffect of local cooling on pro-infl ammatory cytokines and blood fl ow of the skin under surface pressure in rats: Feasibility studyB. Lee, S. Benyajati, J.A. Woods, Y.-K. JanFlaminal ® enzyme alginogel: A novel approach to the control of wound exudate, bioburden and debridementR.J. White
English
EWMA
EWMA Journal 2014 vol 14 no 2 69

Gerrolt Jukema
Member of the EWMA Council
Former EWMA Scientific Recorder
Correspondence:[email protected]
T he 24th Conference of the Europe-an Wound Management Associa-tion (EWMA) was held in Madrid,
Spain, on 14-16 May 2014. The conference was organised in cooperation with Grupo Nacional para el Estudio y Asesoramiento en Úlceras por Presión y Heridas Crónicas (National Advisory Group for the Study of Pressure Ulcers and Chronic Wounds; GNEAUPP). The friendly Spanish hospi-tality and the beautiful warm weather in Madrid made this an unforgettable event.
cal and organisational needs for high quality serv-ices with the limited resources available in wound care. The discussion in the opening plenary ses-sion dealt with how European health care systems are addressing the challenges of aging populations and the increasing number of people living with chronic conditions who have a growing demand for optimised wound care. The session was very popular, and each and every participant was in-spired by the necessity of interdisciplinarity in wound management.
EWMA-GNEAUPP 2014 in Madrid, Spain
The opening plenary session on Innovation, Know-How, and Technology
The conference also included many interesting sessions that were prepared in collaboration with cooperating organisations and international part-ners. For example, EWMA hosted a symposium on veterinary wound healing for the first time. High-quality half-day presentations related to wound healing in animals as part of the ‘One Health Perspective’ received positive feedback and provided a new, thought-provoking angle from which to discuss wounds and their treatment.
With 3,500 delegates, Madrid 2014 proved more successful than any previous EWMA event, attracting the highest number of attendees in the history of the association. The conference provided an energetic academic and networking environ-ment in which colleagues within the field of wound management from all over the world came together for high-level scientific presentations and great networking opportunities. The conference featured more than 1,150 scientific presentations, and representatives from more than 80 countries attended, including many European key opinion leaders and industrial senior executives. The variety of sessions and conference workshops provided participants with opportunities for interactive and hands-on learning experi-ences. It is impossible to describe here all the innovations, out-comes, results, and novel techniques presented. It was encouraging to see the high standard of these presentations and to reflect upon the continued strong interest in wound healing across Europe. Our heartfelt appreciation goes out to all the speakers, presenters, and organisers who actively participated in the sessions.
The conference theme INNOVATION, KNOW-HOW AND TECHNOLOGY IN WOUND CARE reflects both the technologi-
EWMA Journal 2014 vol 14 no 2 70

also explored barriers to and facilitators of large-scale implementation of eHealth solutions.
Another conference highlight was when the honorary speaker Christina Lindholm described how she pushed the boundaries of research and practice in her career, trail-blazing her way toward improving clinical practice for the benefit of patients in Sweden and beyond. Christina start-ed on this path when she co-authored a ground-breaking research paper that changed the perception of how painful leg ulcers are for patients. Through this work, Christina
adrid · Spain
EWMA n GNEAUPP 2014
EWMA
During the conference, first-time presenters were evaluated by the different chairs, who decided that the first-time presenter award should go to the following speakers for the high quality of their presentations, which stood out as particularly outstanding:
Miriam Blokhuis-Arkes (Netherlands)Abstract No. 78: Rapid enzyme analyses as a diagnostic tool for wound infection: Comparison between clinical judgment, microbiological analyses and enzyme analyses
Claudia Navarro (Spain)Abstract No. 40: The effect of extracellular calcium on dermal fibroblasts with potential applications in skin wound healing
Full day symposia were also held on other issues. On Thursday, the Diabetic Foot Day/Pie Diabetico Sympo-sium discussed diagnostic and interventional strate-gies for diabetic foot ulcers and amputation preven-tion and highlighted the current status of diabetic foot management in Spain. On the last day of the conference, EWMA reviewed current trends in eHealth, developments at the policy level, the current imple-mentation status of telemedicine in wound care, and recent technological developments. The symposium
With 3,500 delegates, Madrid 2014 proved more successful than any previous EWMA event
stressed the importance of clinicians understanding patients’ experience, thereby bringing to the fore the sig-nificance of adopting a “human” ap-proach to wound care. She inspired us all with this valuable lesson.
The scientific programme would not have been complete without the con-tributions of the free paper, poster, and oral presenters. EWMA reviewed over 1000 abstracts, which is the highest number of submissions ever received. This formed a great basis for choosing the most interesting studies performed at very high scientific level to be presented through captivating sessions. EWMA greatly appreciates the interest from clinicians and re-searchers who submitted abstracts for the conference and we thank all the presenters for their effort and con-
tribution which made this years conference a great event.
Abstracts presented at the conference as oral or poster presenta-tions are available at www.ewma.org.
Over the duration of the event, six poster presentations were recognised as outstanding by the EWMA Scientific Committee, and two first-time presenters were also award-ed a prize. We congratulate all the prize winners and thank them for keeping our profession’s standards so high.
EWMA Journal 2014 vol 14 no 2 71
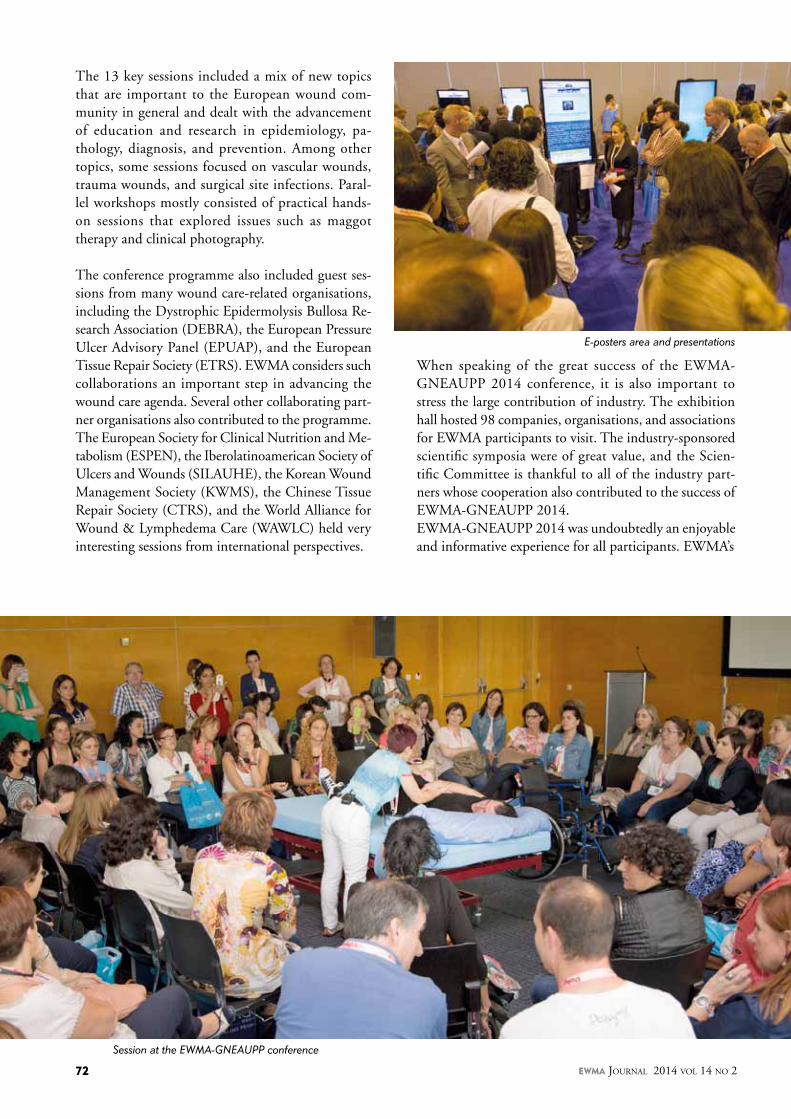
The 13 key sessions included a mix of new topics that are important to the European wound com-munity in general and dealt with the advancement of education and research in epidemiology, pa-thology, diagnosis, and prevention. Among other topics, some sessions focused on vascular wounds, trauma wounds, and surgical site infections. Paral-lel workshops mostly consisted of practical hands-on sessions that explored issues such as maggot therapy and clinical photography.
The conference programme also included guest ses-sions from many wound care-related organisations, including the Dystrophic Epidermolysis Bullosa Re-search Association (DEBRA), the European Pressure Ulcer Advisory Panel (EPUAP), and the European Tissue Repair Society (ETRS). EWMA considers such collaborations an important step in advancing the wound care agenda. Several other collaborating part-ner organisations also contributed to the programme. The European Society for Clinical Nutrition and Me-tabolism (ESPEN), the Iberolatinoamerican Society of Ulcers and Wounds (SILAUHE), the Korean Wound Management Society (KWMS), the Chinese Tissue Repair Society (CTRS), and the World Alliance for Wound & Lymphedema Care (WAWLC) held very interesting sessions from international perspectives.
E-posters area and presentations
Session at the EWMA-GNEAUPP conference
When speaking of the great success of the EWMA-GNEAUPP 2014 conference, it is also important to stress the large contribution of industry. The exhibition hall hosted 98 companies, organisations, and associations for EWMA participants to visit. The industry-sponsored scientific symposia were of great value, and the Scien-tific Committee is thankful to all of the industry part-ners whose cooperation also contributed to the success of EWMA-GNEAUPP 2014.EWMA-GNEAUPP 2014 was undoubtedly an enjoyable and informative experience for all participants. EWMA’s
EWMA Journal 2014 vol 14 no 2 72

EWMA
Conference evening at Finca la Alqueria in Madrid
The 25th Conference of the European Wound Management Association will be held
13-15 May 2015 at the ExCeL London.The conference will be organised
in cooperation with the Tissue Viability Society (TVS).More information about the conference
can be found on page 76.
highest priorities are bringing together the European wound healing community and, perhaps most impor-tantly, creating and strengthening links among national associations that strive to raise the profile of wound man-agement within their respective countries. In addition, so-cial events, including the celebration of GNEAUPP’s 20th anniversary at the IFEMA the conference centre and the main evening event held in the beautiful and traditional Spanish-style restaurant Finca La Alqueria, provided great opportunities for informal networking and simply having a great time with other conference attendees.
We will build on the success of this conference and make the next one even better. Therefore, come join EWMA’s 25th annual conference in London at EWMA 2015, 13-15 May. There will be sessions for everyone interested in wound care as the conference continues to grow and search for solutions and sessions that deal with the problems you face in your day-to-day work. With a theme of WOUND CARE – SHAPING THE FUTURE – A PATIENT, PRO-FESSIONAL, PROVIDER AND PAYER PERSPECTIVE, the conference will focus on the interdisciplinary team-work and collaboration among patients, professionals, and policy makers and how such collaboration is essential for facilitating good practice and providing continuity of care. This will be even more important in the future, as health care systems throughout Europe have to cope with increas-
ing pressure to demonstrate efficient and cost-effective use of resources to optimise wound care with the help of innovative procedures and practices. It is imperative that these different perspectives are considered if we are to re-alise the goal of successful wound management.
Please come join us for the next big adventure in London!
See you all in London for the EWMA 2015 conference 13-15 May!
www.ewma2015.org
EWMA Journal 2014 vol 14 no 2 73

Jan ApelqvistChair,
Cooperating Organisations Board
Immediate Past President.
Correspondence:[email protected]
The 2014 Cooperating Organisations Board Meeting and Cooperating Or-ganisations Workshop were held in
Spain’s sunny capital, Madrid, on 15 May 2014, during the EWMA-GNEAUPP Conference.
At the Cooperating Organisations Workshop four selected abstract were presented by Cooper-ating Organisations about projects in their own country.
Later in the afternoon the Cooperating Or-ganisations Board Meeting was held where there was time for socialising and discussions about collaboration between the partner organisations.
Cooperating Organisations Board MeetingAt the meeting, it was my pleasure to welcome 37 Cooperating Organisation Board Mem-bers or their appointed substitutes, 20 EWMA Council representatives, invited speakers, and visitors – a great number of participants.
Election for the EWMA Council During the board meeting three candidates for the council election presented themselves. The board members voted to elect Andrea Pokorná (Czech Wound Management Society, Czech Republic) and Hubert Vuagnat (Swiss Associa-tion for Wound Care – French section, Switzer-land) to the EWMA Council. On behalf of the EWMA council, I welcome the new members and look forward to collaborating with them during the next 3 years.
Sebastian Probst and Nada Kecelj Lesko-vec stepped down as council members. Their contributions to the EWMA Council are ac-knowledged in a separate entry in this EWMA Journal issue.
Presentations and debate sessionsThe following presentations were given at the meeting: n Feedback to the Cooperating Organisation’s
Board about activities carried-out during the latest year, Sebastian Probst
n Information about EWMA future conferences & project activities, Jan Apelqvist
n Antimicrobial 2.0: Promoting appropriate use of antibiotics and non-antibiotic antimicrobial agents in wound care, Jan Apelqvist
n Managing Wounds as a team: A universal model for the adoption of a team approach to wound care, Zena Moore
The topics that framed the debate sessions were: n How can EWMA better help the Cooperat-
ing Organisations to implement the EWMA documents or other EWMA messages? What are the barriers?
n Patient empowerment – help patients to be involved in their care: Share and discuss typi-cal questions from wound patients, with the objective of developing patient information material for chronic wound patients
All participants actively joined the debate sessions and contributed good ideas and comments. The EWMA secretariat will use these considerations during future document and project development.
During the first debate topic discussion, the participants recognised that cultural and political differences are important barriers to the implemen-tation of EWMA documents. Language differences represent a particularly important problem when implementing a document written in English. EWMA documents should be available in the local language. The EWMA secretariat pointed out that as long as the requirements are met, all cooperating organisations are welcome to translate documents into their own language. A list of these requirements can be obtained from the secretariat. Also discussed was that all new documents could be accompanied by an implementation guidance that focuses on how to implement the document and what must be re-membered during the process.
Cooperating Organisations Activities during the EWMA - GNEAUPP Conference
adrid · Spain
EWMA n GNEAUPP 2014
All presentations from the workshop
are available on www.ewma.org
EWMA Journal 2014 vol 14 no 2 74
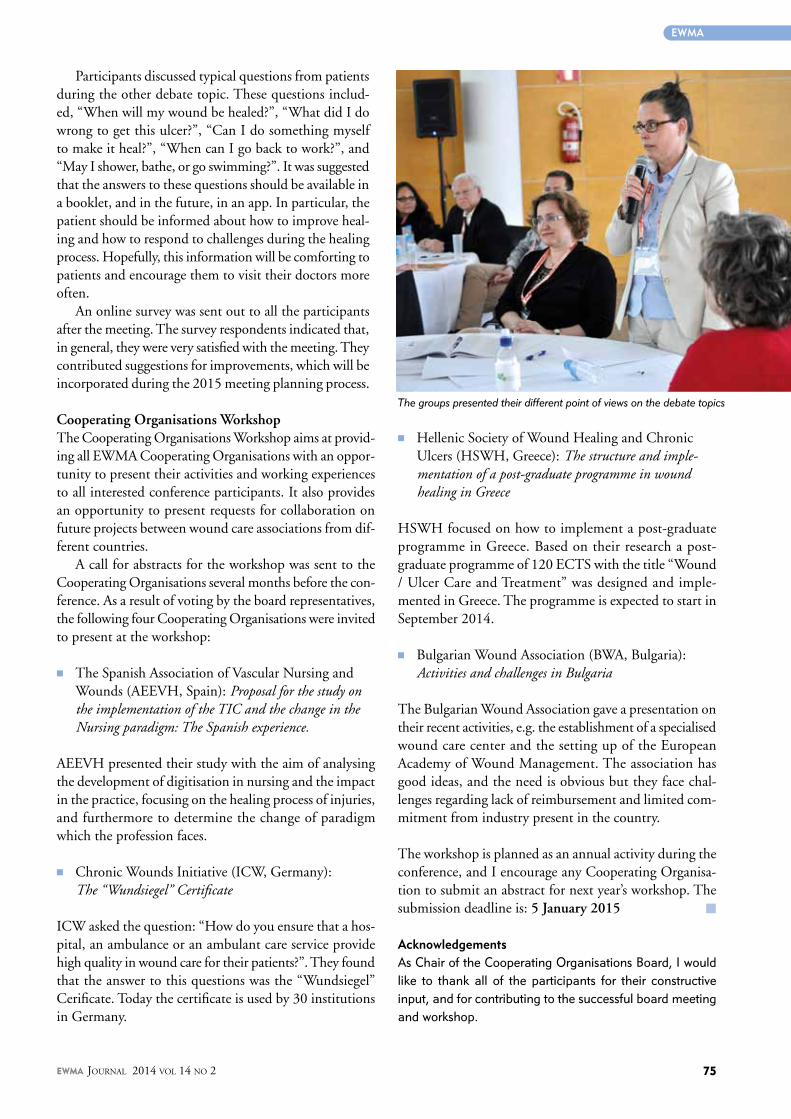
Participants discussed typical questions from patients during the other debate topic. These questions includ-ed, “When will my wound be healed?”, “What did I do wrong to get this ulcer?”, “Can I do something myself to make it heal?”, “When can I go back to work?”, and “May I shower, bathe, or go swimming?”. It was suggested that the answers to these questions should be available in a booklet, and in the future, in an app. In particular, the patient should be informed about how to improve heal-ing and how to respond to challenges during the healing process. Hopefully, this information will be comforting to patients and encourage them to visit their doctors more often.
An online survey was sent out to all the participants after the meeting. The survey respondents indicated that, in general, they were very satisfied with the meeting. They contributed suggestions for improvements, which will be incorporated during the 2015 meeting planning process.
Cooperating Organisations Workshop The Cooperating Organisations Workshop aims at provid-ing all EWMA Cooperating Organisations with an oppor-tunity to present their activities and working experiences to all interested conference participants. It also provides an opportunity to present requests for collaboration on future projects between wound care associations from dif-ferent countries.
A call for abstracts for the workshop was sent to the Cooperating Organisations several months before the con-ference. As a result of voting by the board representatives, the following four Cooperating Organisations were invited to present at the workshop:
n The Spanish Association of Vascular Nursing and
Wounds (AEEVH, Spain): Proposal for the study on the implementation of the TIC and the change in the Nursing paradigm: The Spanish experience.
AEEVH presented their study with the aim of analysing the development of digitisation in nursing and the impact in the practice, focusing on the healing process of injuries, and furthermore to determine the change of paradigm which the profession faces.
n Chronic Wounds Initiative (ICW, Germany): The “Wundsiegel” Certificate
ICW asked the question: “How do you ensure that a hos-pital, an ambulance or an ambulant care service provide high quality in wound care for their patients?”. They found that the answer to this questions was the “Wundsiegel” Cerificate. Today the certificate is used by 30 institutions in Germany.
The groups presented their different point of views on the debate topics
n Hellenic Society of Wound Healing and Chronic Ulcers (HSWH, Greece): The structure and imple-mentation of a post-graduate programme in wound healing in Greece
HSWH focused on how to implement a post-graduate programme in Greece. Based on their research a post-graduate programme of 120 ECTS with the title “Wound / Ulcer Care and Treatment” was designed and imple-mented in Greece. The programme is expected to start in September 2014.
n Bulgarian Wound Association (BWA, Bulgaria): Activities and challenges in Bulgaria
The Bulgarian Wound Association gave a presentation on their recent activities, e.g. the establishment of a specialised wound care center and the setting up of the European Academy of Wound Management. The association has good ideas, and the need is obvious but they face chal-lenges regarding lack of reimbursement and limited com-mitment from industry present in the country.
The workshop is planned as an annual activity during the conference, and I encourage any Cooperating Organisa-tion to submit an abstract for next year’s workshop. The submission deadline is: 5 January 2015 m
AcknowledgementsAs Chair of the Cooperating Organisations Board, I would like to thank all of the participants for their constructive input, and for contributing to the successful board meeting and workshop.
EWMA
EWMA Journal 2014 vol 14 no 2 75

xx
EWMA
Heidi SandozVice Chair,
Tissue Viability Society
www.tws.org.uk
Correspondence:[email protected]
The Tissue Viability Society (TVS) will celebrate 35 years as a registered charity next year. The mission of the TVS is “to
disseminate information, promote research, and in-crease awareness of all aspects of good clinical prac-tice in wound prevention and management”. The trustees of the TVS oversee its activities, manage its accounts, and ensure that the TVS meets the expectations of its members. The 16 TVS trustees and 3 co-opted trustees are active individuals who are engaged in many projects and activities on behalf of the TVS and its members.
2014 is and has been a year full of activities for the TVS, and for 2015 there are even more initiatives planned to fulfil the mission of TVS. The TVS is especially delighted to present, in conjunction with the European Wound Management Asso-ciation, the 25th annual EWMA conference on 13th -15th May in London, UK.
The conference theme is: WOUND CARE – SHAPING THE FUTURE and is set to attract over 2000 delegates from Europe and with the TVS stream running throughout the main confer-ence programme, we are confident that TVS will play an important role in supporting the shar-ing of knowledge and experience within wound management.
The TVS has always been active in educating both its members and the wider healthcare population. The society’s Journal of Tissue Viability (J. Tissue Viability), which is published quarterly by Else-vier, strives to maintain relevant and interesting content. The journal currently has an impact fac-tor of 1.8.
In 2011, the TVS organised and hosted a consen-sus conference to review pressure ulcer reporting. The document that resulted from this conference was published in J. Tissue Viability in 20121. Con-tinued promotional work around this agenda has resulted in a joint NHS England project, which
hopes to establish a robust national system for reporting and measuring the incidence of pressure ulcers. The work for this project will commence this year with a prevalence audit, which will be conducted alongside monthly safety thermometer audits in selected acute trusts.
The TVS is currently leading a national audit of pressure ulcers that cannot be staged. This audit hopes to identify how many unstaged ulcers will go on to present as grade 3 or 4 deep ulcers. We expect that the results of this audit will be ready for publication in early 2015.
The TVS is supporting the organisation and host-ing of the UK Wound Research Network. An ini-tial meeting of the key stakeholders was held at the TVS annual conference in April 2014. There was general support for a cross-specialty wound research network to support National Institute for Health Research activity. This network will be developed over the next 2 years.
In 2013, the TVS began a collaborative project with the EWMA to provide an overview of the main approaches to the organisation of wound care within homecare settings across Europe. This overview has now been published in the Journal of Wound Care2.
The TVS trustees have been asked by fellow charities, including the Multiple Sclerosis Society, the Alzheimer’s Society, and Marie Curie Cancer Care to work with them and/or peer review their work on pressure ulcer prevention and awareness within their member/user population.
The TVS holds several regional study days each year. These study days are popular, locally organ-ised events supported by a small company exhi-bition in which experts in tissue viability deliver informative lectures.
On February 27, 2014 the National Pressure
TVS 2014 activities
EWMA Journal 2014 vol 14 no 2 76
LONDON · UKEWMA 2015
13-15 MAY 2015
25th Conference of the European Wound Management Association
WOUND CARE – SHAPING THE FUTURE
A PATIENT, PROFESSIONAL, PROVIDER AND PAYER PERSPECTIVE
WWW.EWMA2015.ORGWWW.EWMA.ORG WWW.TVS.ORG.UK
Abstract submission
deadline: 1 December 2014
Ulcer Advisory Panel held “The Unavoidable Outcome: A Pressure Injury Consensus Conference”. The purpose of this meeting was to scientifically explore the multi-faceted issue of pressure ulcer unavoidability within an organ sys-tem framework, which considers the complexities of non-modifiable intrinsic and extrinsic risk factors.
There were 2 conference delegate streams: a voting panel made up of representatives from invited worldwide organisations (including USA, Canada, UK, Europe, Aus-tralia, New Zealand and Japan) and non-voting audience delegates. Two Tissue Viability Society Trustees attended, one on the voting panel and the other in the audience.
The TVS trustees regularly contribute as stakeholders to National Institute for Health and Care Excellence (NICE) guidance. The TVS Trustees encourage members to con-tribute comments.
Finally, the TVS continues to organise an annual confer-ence. The 2014 conference was attended by 240 delegates and 54 exhibiting companies. This year, the TVS was able to offer scholarships to help student nurses and post-grad-uate students to attend the TVS, European Pressure Ulcer Advisory Panel, and EWMA conferences.
On behalf of the TVS we welcome you to the EWMA/TVS conference in London in May 2015. We hope to see many familiar and new faces that share our common goal; to provide expertise in wound management. m
References
1. Dealey C., Chambers T., Beldon P., et al., Achieving Consensus in Pressure Ulcer Reporting. J. Tissue Viability 2012;21(3): 72-83.
2. Probst S., Seppänen S., Gethin G. et al., EWMA Document: Home Care-Wound Care, J. Wound Care 2014;23(5 Suppl.):S1–S44.
EWMA Journal 2014 vol 14 no 2
Healthcare for the population of the United King-dom is funded via central taxation and commis-sioned via four independent NHS systems: NHS England, NHS Wales, NHS Scotland and Health and Social Care Northern Ireland. The expectation in England is that to provide an excellent wound care service across a diverse population, it must be accessible to all, provide equity of care, be patient centred and be able to deliver excellent outcomes.
NHS funding is provided via general taxation and provision is via Clinical Commissioning groups (CCGs) at regional level. The funding available for the region is based on the number of residents and level of deprivation. The provider of commu-nity based services for wound management reside in primary care or GP Practices or Community Health Services, such as podiatry or district nurs-es that are part of an acute or large community Trust. The borough Tissue Viability service could be based in an acute or community services or both. Whilst most hospitals have some level of tis-sue viability provision, fewer community services have access to a Tissue Viability Nurse (TVN) who would visit the patients at home or within a community clinic.
MANAGEMENT, LEADERSHIP AND ORGANISATIONGPs tend not to lead on wound care in primary care, but rather act as the gate keeper to secondary care. Thus, wound care in England is generally nurse-led, providing critical leadership for this group of patients. The overall lead within primary care is the TVN. If this is not a community post, then access may be to the TVN in secondary care. The TVN leads on the provision of guidelines and education plus the co-ordination of patient care. Access to TVN advice is part of the referral guide-lines; expectation about the level of provision is clarified and can differ significantly across regions.
Wounds of all aetiologies, with the exception of some diabetic foot ulcers, can be referred to TVNs. TVNs provide specialist advice and management
in most trusts across England. They manage all wound types and co-ordinate the delivery of edu-cation and implementation of guidelines. Alterna-tively some Trusts have Leg Ulcer specialists who are important to the management and tracking of this particular group.
Wound care in England is often organised ac-cording to wound type or aetiology, duration and the mobility of the patient. Thus, where or-ganisational leadership is lacking, the approach to wound care delivery can be restricted to groups of practitioners rather than the provision of a com-prehensive and proactive service.The mobility of the patient is often the first fea-ture that will determine the patient pathway. Thus if the individual is mobile, they will be seen by their General practitioner (GP), Practice Nurse, local podiatry clinic or Walk-in Centre. Simple or post-surgical wound care can be managed ef-fectively within this environment. If the wound is of significant depth or requires negative pressure therapy, these patients will often be managed by district nurses with the support of TVNs.
Within the area of pressure ulcer prevention and management, the role of the physiotherapist and occupational therapist is being developed, par-ticularly around positioning, off-loading, seating and wheelchair provision. Due to the Department of Health’s drive to reduce avoidable pressure ul-cers, the role of the Therapist is slowly being rec-ognised. Portable pressure mapping is available to review seating and for risk assessment and is valuable for both clinicians and carers but access would vary across regions.
The role of Dermatologists and Vascular Surgeons often remains in Secondary Care, limiting their access to the caseload via a referral pathway; access to diagnostic and expert advice is once again a lot-tery. The UK system is predominantly influenced by individual practitioners and their passion for improving wound care; due to allocation of fund-ing, patients often only receive specialist care once they become complex or non-healing.
xx
Alison HopkinsTissue Viability NurseCEO Accelerate CIC
Co-author of the EWMA document:
Home Care - Wound Care.
Correspondence:alison.hopkins@
acceleratecic.com
The organisation of wound care in England
EWMA
LONDON · UK13-15 MAY 2015
EWMA 2015
EWMA Journal 2014 vol 14 no 2 78

What you see is what you get. Cutimed® Siltec
Sorbact®. Infection control and visible absorption built right in.right in.
Cutimed® Siltec Sorbact® offers you safe infection control and reliable fluid management in one dressing.
Cutimed®
Closing wounds. Together.
www.bsnmedical.com
• Bacteria are removed with each dressing change to reduce overall bacterial load • No chemicals are released into wound bed which could cause cytotoxicity or resistance• Vertical absorption draws excess exudate away from wound bed• Super-absorbers retain fluid, even under compression• Transparent PU top film allows easy saturation monitoring
BSN1403_CS6_210x297_CutiSilSorb_EWMA_AZ
Cedric Behrens
297mm
297mm
303mm
210mm
210mm
216mm
x
15:3119/03/2014
EWMA
-
-
-
x
-
x

On 13-15 May 2015, the 25th Conference of the European Wound Management Association will take place in the great capital city of Britain and will be organised in cooperation with the Tissue Viability Society (TVS). The conference theme is
WOUND CARE – SHAPING THE FUTURE – A PATIENT, PROFESSIONAL, PROVIDER
AND PAYER PERSPECTIVE
which will highlight the future interdisciplinary teamwork and collaboration among patients, professionals, and policy makers that will be es-sential for facilitating efficient and high-quality treatment for patients and for guaranteeing their continuity of care.
PRELIMINARy PROGRAMMEThe 2015 conference will offer a more varied mixture of topics within wound healing than ever before through plenary sessions, key ses-sions, workshops, full-day EWMA symposiums, and guest sessions. The programme will consist of an international assortment of scientists from across Europe and the rest of the world who will present new results and developments within the field of wound healing.
ABSTRACT SUBMISSIONAbstracts for free paper and poster presenta-tions play a very important role in the con-ference programme. We hope that many of you will wish to share your work at the 2015 conference. To submit an abstract for EWMA 2015, please visit www.ewma2015.org. Guidelines for abstract submission will be provided after entering the abstract sub-mission system.
Abstracts for oral presentation and electron-ic poster (e-poster) presentation can be sub-mitted for any topic in wound healing and wound management.
Primary categories are:Acute Wounds – Antimicrobials – Basic Science – Burns – Devices & Inter-vention – Diabetic Foot – Dressings – Education e-Health – Health Economics & Outcome – Home Care – Infection – Leg Ulcer – Negative Pressure Wound Therapy – Nutrition – Pain – Pressure Ulcer – Prevention – Quality of life – Wound Assessment – Case Studies – Professional Communication
VISIT EWMA 2015 IN LONDON, UNITED KINGDOM
Registration fees
Category Before 15 March 2015
15 March-1 May 2015
After 1 May 2015
Full conference registration:
EWMA and TVS Members1 € 385 (462 incl. VAT)
€ 450 (540 incl VAT)
€ 500 (600 incl. VAT)
Non-members € 460 (552 incl. VAT)
€ 525 (630 incl. VAT)
€ 575 (690 incl. VAT)
One day registration:
1-day registration € 250 (300 incl. VAT)
€ 275 (330 incl. VAT)
€ 325 (390 incl. VAT)
Conference dinner2 € 95 (114 incl. VAT)
€ 95 (114 incl. VAT)
€ 95 (114 incl. VAT)
IMPORTANT DATES
Conference dates13-15 May 2015
Abstract submission & registration openOctober 2014
Deadline for abstracts1 December 2014
Early registration deadline15 March 2015
1. Members of EWMA or one of EWMA’s cooperating organisations, see http://ewma.org/english/cooperating-organisations/cooperating-organisati-ons.html
2. Tickets for the conference dinner Thursday 14/5 2015 are not included in the registration fee and are non-refundable. Please note: Limited number of seats.
UK Nurse Students: A special fee for UK Nurse Students will apply. Please visit the conference website for more information.
EWMA Journal 2014 vol 14 no 2 80

VISIT EWMA 2015 IN LONDON, UNITED KINGDOM
LONDON · UK13-15 MAY 2015
EWMA 2015
The full-day streams and guest sessions are particu-larly popular among EWMA conference delegates, as they foster more in-depth discussions within the field. For more information about other focus areas, abstract submission, terms and conditions, and programme updates, please see the conference website: www.ewma2015.org.
KEy SESSIONSEWMA 2015 will include a mixture of new topics that are important to the European wound community in general in addition to topics that have had enormous appeal during previous EWMA conferences. The sessions will cover the advancement of education and research in relation to epidemiology, pathology, diagnosis, prevention, and management of wounds.
Key sessions this year will address EWMA and TVS focus areas, including:n Wound care – Shaping the future – A patient, pro-
fessional, provider and payer perspectiven Living with non-healing ulcers – Focus on patients’
quality of life n Wounds assessment – The art and sciencen Patient and organisational pressure – Ulcer risk
factors and their application in practice through an evidence -based risk assessment framework and active monitoring model of care
n Wounds and wellbeing – Using psychosocial resources to improve patient outcomes
n Wound care & geriatrics – Dementia in wound caren Palliative care – Evidence-based practice for
managing challenging skin lesionsn The importance of surveillance of infection in
acute and chronic woundsn Hard-to-heal wounds – A challenge for all involved n Paediatric wound caren Leg ulcer recommendations (Presentation of
EWMA document)n Negative Pressure Wound Therapy (Presentation of
EWMA document)
WORKSHOPSSeveral workshops will be offered at EWMA 2015. These are typically held in smaller settings than key sessions and free paper sessions. EWMA workshops are interactive and give participants an opportunity to ad-dress and elaborate on particular aspects of the session themes.
The workshops cover a variety of topics including:n Biofilmn Burns, acute, and traumatic woundsn Debridementn How to organise a system of registration of ulcersn Individualised targeted diagnostics and topical
wound therapyn Meet the experts: Everything you want to know
about maggot therapy n Nutritionn Podiatryn Pressure ulcers caused by medical devicesn Pressure ulcer Risk assessmentn Skincare of patients with a chronic woundn Soft casting for heelsn Use of information technology in wound care
ABSTRACT SUBMISSION DEADLINE: 1 DECEMBER 2014
FOR MORE INFORMATION ABOUT THE CONFERENCE, PLEASE VISIT: WWW.EWMA2015.ORG
EWMA Journal 2014 vol 14 no 2 81

Samantha Holloway EWMA Education
Committee, Chair of the Teacher
Network meeting and free paper session, 2014
David Hopkins eLearning Consultant,
Warwick University, Coventry, UK
Dubravko Huljev Chair of the EWMA
Education Committee
Correspondence:[email protected]
For the third time, teachers of wound manage-ment gathered to draw inspiration from their colleagues from institutions all over Europe. The meeting took place during the EWMA-GNEAUPP 2014 Conference in Madrid and was followed by the first-ever EWMA Teacher Net-work free paper session on the following day.
Since 2012, the members of the EWMA Teacher Network have met once a year during the EWMA Conference. The network offers an opportunity for teachers of wound management at educational institutions all over Europe to get together and share views, experiences, and ideas with peers from different teaching cultures and backgrounds. The theme of the meeting in Madrid was how the net-work and EWMA could mutually benefit from engaging and incorporating the network more in EWMA’s educational activities.
The main purpose of the meeting was to dis-cuss how to raise awareness of the importance of standardising wound education curricula for nurses across Europe. The intention is to provide a guidance document for educational institutions to follow to ensure that students throughout Europe graduate with an adequate knowledge level to en-able them to practise as a qualified practitioner in wound management.
INITIATING AN EDUCATION PROJECTA survey conducted by the then Teach the Teach-ers education development group of EWMA in 2009 among the EWMA Cooperating Organisa-tions showed inconsistencies in the level of wound education in Undergraduate European Nursing programmes. In more than half of cases, as lit-tle as 2 hours and a maximum of one day of the total nursing undergraduate programme were set aside for wound management. The survey also revealed a common perception that the student nurse is not adequately prepared for the practice of wound management on qualification (Moore and Clarke, 2011). Recently, an article published in The Lancet demonstrated that downgrading edu-cation qualifications can adversely affect patient outcomes (Aiken et al., 2014).
Therefore, the Teacher Network has suggested to the EWMA Council that a project should be initiated aimed at defining learning outcomes related to the different levels of education and eliminating the inconsistencies in wound manage-ment education in Europe. However, to undertake this significant piece of work, a model of funding is required to finance the project. Furthermore, a working plan for the project is needed. The debate at the EWMA Teacher Network Meeting presented many interesting and useful suggestions from the meeting participants, information that EWMA will take forward.
TEACHER-SPECIFIC FREE PAPER SESSIONThis year, the annual Teacher Network meeting was followed up by the inaugural free paper ses-sion where the network members were invited to present their work and experiences.
Mariann Csernus from Semmelweis Univer-sity, Budapest, Hungary presented her findings related to the Wound Management BSc module and how project work has made an increase in the number of lessons taught possible. Irina Bakhtina from the St. Petersburg Post Graduate School of Nursing in Russia presented her report on the pilot professional supplementary vocational edu-cation module, which was carried out for the first time in 2013 and is built on a competence-based multidisciplinary approach to wound treatment and care.
These presentations were accompanied by a talk by David Hopkins, a learning technologist from Warwick University in Coventry, UK. His presentation dealt with the challenge of engaging students through new technologies. The aim was to showcase the developments and strategies for engaging and supporting students with new tech-nologies in the delivery of teaching and learning.
A report from the EWMA Teacher Network
EWMA Journal 2014 vol 14 no 2 82

WHERE WILL TECHNOLOGy LEAD US? – A LEARNING TECHNOLOGIST’S PERSPECTIVE “The need for digital literacy… is not only a necessity for our children, but also for those who must educate them. To better educate our children, we need to better educate their educators.” Whitby, 2014.
Students are connected today more than they have ever been, whether it is with friends or family, or with their teachers or community leaders. The computing devices that they hold in their pockets have more computing power than NASA had when it put the first man on the Moon. However, how do we, as educators, manage the use of these devices in the classroom? How can we be sure that they are not being used for activities such as updating Facebook profiles, sending tweets or chat messages, playing games, or planning social events or a work shift? How can we engage the disengaged and bring their connections and connected lives into the classroom?
Called ‘Strategies for engaging students – where will technology lead us?’, the presentation focused on the as-sumption that those willing to come and listen were in-terested in what can be done with technology rather than what should be done.
From the appropriate and coherent use of an institutional virtual learning environment (VLE) to the use of moving images and broadcast video as part of a flipped classroom approach, the session briefly touched on different aspects of modern thinking and the tools available. It is not ad-equate to include an online assessment – i.e., a written assignment or multiple choice questions – into a module of study without considering the assessment strategy un-derpinning these. Such tests need to be implemented in a cohesive manner so they add value to the learning ex-perience. Ideally, both types of formative and summative assessments need to provide opportunities for more than just fact recall; they need to demonstrate critical thinking, reflection, and personal research.
Trying to tackle the rise in the use of personal and mobile devices in classrooms and in learning journeys is not one to be taken lightly but, with understanding and sympathy for the users, is one that can have both a rewarding and posi-tive influence. We know students are better connected than ever before and that they have the technological know-how to be prepared, sometimes more prepared than what the current learning materials allow. We need to meet the students in this world by utilising the Facebook-Twitter-SnapChat-Instagram-Tumblr networks they engage in so much to establish the advantages of these forms of commu-nication in relation to learning. This requires engagement by university administrators as well as managers.
It is important to appreciate that technology is an ena-bler and can enhance a task or objective that is set for a specific learning journey. Educationalists need to work out what the students should be able to achieve at the end of a task and what they should know or understand at the end of a seminar or lecture. Subsequently, they should look to technology to enhance these experiences through video, reading lists and eBooks, augmented reality or mobile de-vices, supplemented by the student’s own online research. This requires that teachers look beyond what is provided by their institution.
THE MORE WE SHARE THE BETTEREWMA and the EWMA Education Committee continue to find ways to improve the exchange of knowledge and experience for the Teacher Network members. New ini-tiatives suggested by the members were discussed at this year’s meeting – for example, exploring the opportunities of financing an exchange programme between education institutions and an increased online collaboration.
The network only exists because of its members and the more individuals that join should mean the more we will have to share. It is hoped that this will lead to further achievements.
To learn more about the work of the EWMA Teacher Network or to express your interest to join us at the next meeting, please go to www.ewma.org or email [email protected]. m
David Hopkins has just begun a new project in collaboration with some respected colleagues in the world of learning and educational technology to explore the question of what is learning technology, who are the learning technologists, and how they work, and hope to have some news regarding these topics very soon. For further information, follow the Twitter hashtag #edtech-book for updates.
References
Hopkins, D. (2014). EWMA 2014 – Strategies for engaging students: where will technol-ogy lead us? Online slideshow available at: www.slideshare.net/hopkinsdavid/strategies-for-engaging-students-where-will-technology-lead-us [Accessed 15 Aug. 2014].
Whitby, T. (2014) A Mobile dilemma. Edutopia [Blog]. Available from: www.edutopia.org/blog/a-mobile-dilemma-tom-whitby [Accessed August 12, 2014]
Aiken, L.H., Sloane, D.M., Bruyneel, L., Van den Heede, K., Griffiths, P., Busse, R., Diomidous, M., Kinnunen, J., Kozka, M., Lesaffre, E., McHugh, M.D., Moreno-Casbas, M.T., Rafferty, A.M., Schwendimann, R., Scott, P.A., Tishelman, C., van Achterberg, T., Sermeus, W., consortium, R.C., 2014. Nurse staffing and education and hospi-tal mortality in nine European countries: a retrospective observational study. Lancet 2014;383(9931):1824-30.
Moore, Z., Clarke, E., 2011. A survey of the provision of education in wound manage-ment to undergraduate nursing students. EWMA Journal 2011;11(1):35-8.
EWMA
EWMA Journal 2014 vol 14 no 2 83

Home Care – Wound Care
In light of an ageing popu-lation, changes in lifestyle trends, and increased healthcare demands, European health care systems are facing an enormous economic chal-lenge. Considering the shift in the provision of health servic-es from secondary to primary care, EWMA aims to ensure the best possible care is pro-vided in the community and home care sectors and to raise awareness of how to provide this care to individuals with wounds.
The publication of the Home Care – Wound Care (HCWC) document, launched at a key session dur-ing the EWMA-GNEAUPP Conference in Madrid in May 2014, provides a set of recommendations on wound care in the home care sector at the general Eu-ropean level and was the first step in achieving this aim. National follow-up projects for developing and implementing the guidance document in the UK and in Germany are planned and will involve key players in the fields of wound care, home and community care, and patient organisations.
To better understand the concept of HCWC and the challenges and perspectives involved, the EWMA Journal has asked two authors of the document to outline its key points and give readers some in-sights into the ideas behind the publication. Georgina and Sebastian, you were both deeply involved in developing the document. Could you describe in your own words what HCWC is about? Sebastian Probst (SP): For me, HCWC is a service provided by an interdisciplinary wound care team from either a profit or non-profit organisation that takes care of patients with wounds and their relatives, also called informal carers, at home. Georgina Gethin (GG): I agree, and I think HCWC is also about opening up conversations and raising aware-ness about the increased numbers of people who require
wound care in the home care setting. In essence, we want to highlight what it takes to achieve such care in a coor-dinated and multidiscipli-nary fashion.
Why is this important, and why should we be interested in it? SP: Since the introduction of the DRGs, we have seen
a shift from inpatient to outpatient care. Changes in the demographic profile of the population, changes in lifestyle trends, and the fact that governments and hos-pitals need to save money mean we need more nurses and physicians who are aware of the requirements for wound care at home.
GG: It is important because individuals in their own homes can sometimes be hidden from the discus-sions on what is happening in health care; therefore, resources are not often available to meet the needs of people in the home care setting. All of the data suggest more people will require wound care in the home care setting. We need to think about how we can provide that care in the best manner possible and what is re-quired to provide it. From the point of view of EWMA, HCWC is important because we are a group of profes-sionals who try to promote best practices in wound care and raise the profile of wound care on policy and professional agendas. The HCWC conversation is one means of doing that.
Now we have the HCWC document. What is its future? GG: I think we need to have the document incorpo-rated and used within policy considerations. It should also be used in terms of highlighting educational and resource needs.
SP: Having the HCWC document available in mul-tiple languages is key to national implementation so that health care professionals can read the document in their own language. I think it will be important to support EWMA’s Cooperating Organisations with inte-
Interview with Georgina Gethin, co-author of the Home Care-Wound Care
document and Sebastian Probst, chair and editor
EWMA Journal 2014 vol 14 no 2 84

EWMA
issues, and it would be wrong to just look at these fac-tors in isolation. What can appear to be less covered in terms of resources in one area can be very well sup-ported by, for example, a social care system or a volun-tary system. So, I think we have to be cautious in how much we compare. However, the key element identified from working with the different systems is that they all depend on some sort of referral system, which describes how people are referred to the most appropriate service or specialist. So, where wound care works well, you find a clearly-defined and efficient referral system, rather than success being a question of money.
SP: Even in the pathways, there are variations in how wound care works. One issue is a lack of integra-tion between primary and secondary care. There can be a very good home care service with skilled wound care nurses, but if there is a lack of transition, we have to start over again.
The discussion in the document about best practice and implementation of guidelines is on a general l evel. What are the obstacles for implementing best practice guide-lines for HCWC? SP: In primary care, nearly every hospital has its own guidelines. The problem we have identified is a lack of resources and adherence to these guidelines. So, when it comes to dissemination, there is a big challenge.
GG: When you look at the work on good guide-lines, one key component is to know who the target audiences are for the guidelines. In this case, the target audiences are individuals in the home care setting, but which individuals? Another big challenge is that we do not have many guidelines for the home care setting. Whether they are available or must first be developed,
we need an answer for whom they should be targeted: informal carers, nurses, GPs, or podiatrists? If the an-swer is that the guidelines are targeted at everybody, experience shows no one takes ownership of it. So, in general, there is a lack of HCWC guidelines. For those that do exist, we need to see how applicable they are to the home care setting. Then, we must address what resources are required to implement those guidelines. You also have to look at the readiness to accept the guidelines. Much work is required in terms of accept-ing, adapting, and implementing guidelines, and a huge gap exists when it comes to the home care setting.
You advocate for a model including both community and health services in a team centred around the patient. What problems do we face when organising a care team like this, and can you identify any solutions – technical, educational, or organisational – to alleviate them?
SP: The problem will often be communication and transferring information from primary care to second-ary care, which can be caused by a lack of resources, well-educated health professionals, and documentation.
GG: I do not think we know the solution. Tradi-tionally, each discipline holds its own records, so the sharing of information has always been a problem. I think what we are starting to find is more areas and teams are exploring how to better share information and communicate, and when you achieve that, you will have your true working model of shared care. One possible solution is to look at shared information sys-tems, which are most likely facilitated by technology and eHealth, and play an active part in shaping them.
Authors of the EWMA Home Care-Wound Care document: Sebastian Probst chair and editor, EWMA Salla Seppänen, co-editor, EWMA Veronika Gerber, Initiative Chronische Wunden,
ICW, Germany
Alison Hopkins, Tissue Viability Society, TVS, UK
Rytis Rimdeika, EWMA
Georgina Gethin, EWMA
TranslationThe EWMA documents can be translated into any language by the EWMA Cooperating Organisations. For more information, go to http://ewma.org/ or send an email to [email protected].
The Home Care - Wound Care document is published by the Journal of Wound Care,and can be downloaded free of charge at www.ewma.org
grating the document into their clinical practices. Perhaps in the long run, we can assist with developing implementa-tion plans like in the projects that are being initiated in the UK and in Ger-many. Experiences from these projects can help other countries.
You focus on three different geographical areas and therefore completely different health care systems and models of organising home care. What have you learned from working with the systems in Germany, England, and the Nordic countries, and what can other systems learn from your experiences?GG: The systems are completely differ-ent in terms of social care and funding
EWMA Journal 2014 vol 14 no 2 85

but also preventing another wound (e.g., pressure ul-cers) from developing. So, in that sense, education of carers is very, very important.
What about skills like the capacity for team work, social understanding, and cultural skills? GG: These skills are part of the community nurses’ education, like recognising the patient’s home environ-ment and essentially seeing yourself as a visitor. I cannot speak for other professionals, but from the community nursing perspective, they should be very conscious of these points.
SP: In the interdisciplinary team, everyone should know how to contribute, including the GP, pharmacist, nurse, or dietician.
GG: Ultimately, these skills should be acquired through education.
SP: Fortunately, most people working in social care or health care already bring some of these skills with them. You do not choose this line of work if you are not good with people. However, some skills you cannot learn. You can train the workers, but these skills cannot always be taught.
Do you think there are tasks that could be shifted with advantage from the clinical staff to the home care staff and vice-versa? GG: Many carers and patients are often willing to take over the care of their wounds as long as they are physically and mentally able and have the support from health professionals. They do not want to be solely in charge, but, from my own experience, they become much more involved in their own care if we let the pa-tients do much of their own work. In fact, they often do the work better because they are only looking after their
Is there anything we can do to approach the challenges we meet, whether cultural or based on insufficient knowledge, when relatives step into the role of the caregiver? SP: First, it is necessary to perform a proper assess-ment, which takes time, and it is important to include the relatives in this assessment. If the relatives agree, they will be educated and carefully instructed on how to apply a certain product, where to get it, and so on. The wound specialist should also see if dressings are available that only need to be changed every 2 or 3 days rather than several times a day.
GG: I agree that it starts with a thorough and com-prehensive assessment, which is where skilled commu-nity personnel will have the knowledge and skills to put plans and support services in place.
To conclude this interview, what key points would you highlight as important for giving individuals with wounds the proper care in their own homes?
GG: We must recognise the challenges inherent to being treated in the home environment. Often, prac-titioners may be going alone into a situation, so they must adapt what they have to provide a suitable home care setting. Building a team approach where the ex-pertise, views, and opinions of the patients and their informal carers is also critical. Together, team-building and adapting to the environment are important factors for successful HCWC.
SP: Yes, and the transfer of skills and knowledge to people who are working in home care is also important. In this regard, I see EWMA as a key player in providing this knowledge through its Cooperating Organisations.
m
HCWC Project in the UKEWMA is initiating the development of a guidance document with experience- and evidence-based recommendations for wound care in home and community care in the UK.
Special attention will be paid to these subjects:n Organisation of care on a political leveln Organisation of the wound care team on
a practical leveln Education, training, and competencies
for clinicians, service providers, patients, and their families
By involving relevant organisations, institutions, and universities in its preparation and imple-mentation, EWMA’s intention is to create a network in the UK.
When taking care of a patient in his or her home, rather than a clinic, what special skills are required of the care staff? SP: Communication is key in nursing; without it, we cannot do anything. However, the staff must have or acquire the skill to educate and transfer information to patients and informal carers in such a way that they understand what to do.
GG: If I look at the care staff, not health professionals, one topic people require support and infor-mation on is prevention. Care is not just about the actual wound
own wounds and no one else’s. Often, you will find that patients and carers can be very innovative in ways of dealing with exudate, odour, or other issues. So, yes, I think practices related to wound hygiene, cleansing, dressings, and even compression therapy could definitely be shared with willing patients and carers.
SP: Yes, self-management is very important. To ensure the con-tinuity of care in an interdiscipli-nary team where different people often do not see each other, eve-ryone has to know the importance of communication.
EWMA
EWMA Journal 2014 vol 14 no 2 86

Bremen
SAVE THE DATES11-13 MAY 2016
BREMEN · GERMANY
EWMA 2016
www.deutscher-wundkongress.dewww.wund-dach.org
www.ewma.org

INTRODUCTIONThe Nordic Diabetic Foot Task Force was estab-lished at the EWMA Conference in 2013 in Co-penhagen. The aim of the Task Force is to endorse implementation of international recommenda-tions for the treatment of the diabetic foot and in Nordic countries. Denmark, Finland, Iceland, Norway and Sweden are participating in the ini-tiative, which is supported by EWMA, the Inter-national Working Group on the Diabetic Foot (IWGDF), and the European Association for the Study of Diabetes (EASD).
THE NUMBER OF AMPUTATIONS IS HIGH The discrepancies between recommendations and actual practices are quite significant, as can be seen using the example of Denmark. In a Danish reg-ister study by phd student Pia Søe Lykten Jensen, the total number of lower extremity non traumat-ic amputations decreased from 2100 in 2001 to 1950 in 2011, despite an increasing population1. Major amputations had a similar decrease from 1450 to 1200 in the same period. Despite the observed decrease the number of amputations is still high. The picture is probably quite similar in all Nordic countries, and the reason is often inap-propriate organisation of care due to decentralisa-tion and fragmented, incomplete implementation of best clinical practices. It is our aim to address and change these conditions.
THE STRATEGIC APPROACHThe strategy to realise this objective is quite simple; national working groups have been es-tablished in each of the Nordic countries. The working groups consist of representatives from all relevant areas of expertise involved in diabetic foot care. Each individual working group will aim to outline the most effective path to follow in its respective country in order to spotlight dia-betic foot care and prioritise this on the national health agenda. The main problem in this regard is that conditions vary from country to country in terms of size and density of population, infra-structure, health care organisation, etc. Secondly, some countries (such as Denmark) already have
national guidelines in place, whereas others do not. This calls for different national strategies, which is why we have gathered national experts in the working groups, who, with their specific knowledge and experience in the field, are well suited to create such strategies.
The national working groups have been es-tablished over the summer of 2014 and are in the process of drafting their national approaches, which will include different activities depending on the specific situation in each country. It is ex-pected that a number of national meetings, posi-tion documents, and other initiatives will come out of these efforts in the near future.
A COMMON NORDIC PLATFORMTo orchestrate the work in each of the five partici-pating countries, a common Nordic Diabetic Foot Symposium is arranged to take place in Malmo during November 5-6, 2014. The Symposium is quite unique in that it brings together national and international wound care clinicians from multidisciplinary backgrounds. The program will teach participants best practices, principles of multidisciplinary organisation, and practical skills, all of which are prerequisites of good dia-betic foot care. The Symposium will also hold parallel national sessions in which participants will discuss ways to improve the organisation of diabetic foot care and the network in their respec-tive countries.
On behalf of The Nordic Diabetic Foot Task Force, we are very optimistic about the progress we will make, and we are confident that the work under way will set an example for other countries throughout Europe. The Nordic Diabetic Foot Task Force works for the improvement of dia-betic foot care and to reduce amputation rates, which are unnecessarily high. We look forward to sharing our work and experience with colleagues throughout the world. m
Nordic Diabetic Foot Task Force: Status and Activities
Klaus Kirketerp-MøllerChairman of the Nordic
Diabetic Foot Task Force
Orthopaedic ConsultantDepartment of Orthopaedics
Research Unit for Amputations and Wounds
Hvidovre Hospital, Denmark
www.nordicdiabeticfoot.com
EWMA
References
Jensen PSL. The effect of optimized nursing and periopera-tive nutritional therapy on the surgical stress response folloing lower limb amputation. [Study in progress]
EWMA Journal 2014 vol 14 no 2 88

Visit EWMA on our
Social Media platforms
Follow us and get the latest updates about
EWMA activities:
www.facebook.com/EWMA.Wound
www.linkedin.com/company/ european-wound-management-
association
Twitter: @ewmatweet
Supported by
Nordic Diabetic Foot Task Force & Symposium 2014 Sponsor:
www.nordicdiabeticfoot.org
Nordic Diabetic Foot Symposium 2014Join us to take an active role in implementing Best Practice Diabetic Foot Care in the Nordic countries
5-6 November 2014 Malmö, Sweden
The program will cover a mix of; n Traditional presentations n Hands on workshops n Meet the expert sessions
– addressing best practice treatment regimesn Interactive session with centre presentations
based on submitted contributionn Concluding panel debate defining strategies
to pursue implementation of Guidelines
Examples of topics to be covered; n Basic pathophysiology of diabetic foot problems n Introduction to IWGDF guidelinesn Overview of current situation of care in the Nordic Countriesn Screeningn Diagnosing neuropathyn Diagnosing and treating charcoot footn Vascular Assessmentn Surgery and use of flapsn Role of Negative Pressure Wound Therapyn Choice of dressingsn Offloadingn Amputation and rehabilitation n Role of podiatryn Organisation of diabetic foot teams n Quality control and registers n Patient education and compliance
Venue Symposium datesStadionmässan, Malmö 5-6 November 2014
Workshop Registration and information7 November 2014 www.nordicdiabeticfoot.org
Patricia Price
Chair of the EWMA Pa-tient Outcome Group Co-
Author of the EWMA Study Recommendation
Correspondence: [email protected]
The initiative to produce this document was taken
by the EWMA Patient Out-come Group (EWMA
POG). The members of the EWMA POG are:
Patricia Price(Chair)Jan Apelqvist
Luc GrysonFinn Gottrup
Robert Strohal
EWMA
To support the drive to raise the quality of evi-dence in wound management studies, EWMA commissioned the Patient Outcome Group1 to develop a series of recommendations to support researchers when planning investigating. The first of these focus on clinical investigations in leg ulcers and wound care, and was published in May 2014.
In 2010 the EWMA Patient Outcome Group (POG) published recommendations to im-prove the quality of evidence in wound
management2. As a companion piece of work, the EWMA POG has worked to provide a series of user-friendly documents to assist those new to (or inexperienced in) research in starting on the path to plan, conduct, interpret and disseminate findings from an investigation that will improve our understanding of clinical wound healing and raise the evidence level of the work undertaken in this important area. Given the range of wound types that clinicians are involved with, the POG has decided to limit the first of these to venous leg ulcers. In addition, as a European association, the focus will be on EU regulations and directives.
The target audience for this publication is hospital and community clinicians working collaboratively with other professions or industry. In particular, it aims to provide a clinical study guideline for the novice researcher working within wound care (leg ulcers), but the guideline may also be relevant for article reviewers, as educational material or a checklist for the experienced researcher. The text takes the format of a ‘step by step’ instruction manual to highlight activities to consider and out-line frequent mistakes that many of us have made along the way – with the aim of helping novice researchers avoid making them, and improve the quality of studies that are undertaken. The em-phasis focus on Randomised Controlled Trials (RCTs) and Cohort Studies that are prospective (i.e., retrospective studies are not included).
Throughout the document we sign post relevant existing documents and provide links to web-sites and documents where regulation specific issues are covered really well. The aim is to produce a user-friendly resource, which is practical. The format takes the form of short chapters on dif-ferent aspects of the research process – with many points made in bullet format. It is not anticipated that researchers will read every page and associ-ated web-link in order, but use it as a pathway through the process – with the text highlighting when it would be useful to take a detour into other resources to get additional information. The information is divided into chapters that reflect the different stages of the process; many chapters have multiple subsections so that you can easily find help with a specific issue. We hope that you will find this document useful in putting together your research plans and look forward to reading the papers at some point in the future as you contribute to the evidence base for improved wound healing outcomes. m
EWMA Study recommendations for clinical investigations in leg ulcers and wound care
1 http://ewma.org/english/ewma-projects-and-studies/patient-outcome-group.html
2 Gottrup, F., Apelqvist, J., Price, P. Outcomes in controlled and comparative studies on non-healing wounds: recommendations to improve the quality of evidence in wound management. J Wound Care 2010;19:6,237-68.
The document is published by the Journal of Wound Care and can be downloaded free of charge at www.ewma.org
EWMA Journal 2014 vol 14 no 2 90

Salla Seppänen
EWMA President and Chair of the
EWMA Advocacy Group
Correspondence:[email protected]
EWMA
EWMA is a collaborating partner in the Joint Action on Chronic Diseases (CHRODIS-JA), with specific focus on Work Package 7 (WP7): Diabetes: A case study on strengthening health care for people with chronic diseases. The first status meeting with the coordinators of WP7 was held in Rome on 8 July 2014.
Representing EWMA Council Professor Alberto Piaggesi participated in the meeting, which had two major purposes. First, project coordinators gave a thorough introduction to the project and the status of preparatory work. In particular, a sur-vey designed to establish a baseline for the current state of diabetes prevention strategies on the na-tional level was discussed in detail. Second, each of the collaboration partners introduced themselves in order to further networking and cooperation among the partners and the project.
EWMA in collaboration with the EU Joint Action on Chronic Diseases
CHRODIS-JA is a project under the EU-Commission, with the following seven specific outcomes:1. Providing a platform for knowledge exchange,
including a help desk and a clearinghouse.2. Developing a methodology for scaling up and
transferring good practices in health promotion and chronic disease prevention.
3. Selecting the most cost-effective practices to address the transfer of multi-morbid patients to other settings.
4. Providing a training programme for health professionals to address multi-morbidity.
5. Developing a set of best practices in primary prevention, early detection, secondary prevention, diabetes management, and patient empowerment programmes as well as methods for transferring these practices.
6. Reviewing existing national programmes on diabetes.
7. Establishing a Forum of Ministries of Health to discuss the continuity of CHRODIS-JA after this Joint Action.
Visit www.chrodis.eu for more information
EWMA Journal 2014 vol 14 no 2 92
CHRODIS-JA is an initiative by the European Commission with the objective to promote and facilitate the process of exchange and transfer of good practices between European countries and regions. Chronic conditions, with a specific focus on health promotion and the prevention of multi-morbidity and diabetes, will be addressed. WP7 focuses on diabetes as a model for multidiscipli-nary care covering the whole range from primary prevention to treatment and national plans.
As a collaborating partner, EWMA has an oppor-tunity to contribute with insight on diabetic foot ulceration, which can serve well as a model of a diabetic complication requiring multidisciplinary care. In the project, EWMA will:n Connect WP7 coordinators and partners to
relevant European and international key cli-nician stakeholders regarding the prevention and treatment of diabetic foot ulcers.
n Describe existing strategies to identify and treat high-risk patients.
n Identify information about the cost-effec-tiveness of prevention/treatment given the consequences of amputation/poor foot care.
n Describe good practices for the prevention and treatment of diabetic foot ulcers, includ-ing the use of a team approach for preven-tion and treatment.
n Disseminate results through the EWMA Journal and www.ewma.org website.
A multidisciplinary approach to care and treat-ment of the diabetic foot are EWMA focus ar-eas. Thus, the collaboration with the EU Joint Action on Chronic Diseases is an excellent op-portunity for EWMA to influence the future of multidisciplinary care and to advocate for the prevention and treatment solutions and strate-gies that EWMA promotes in collaboration with the International Working Group on the Diabetic Foot (IWGDF), amongst others. m
This 4 day theoretical course & practical training gives participants a thorough intro-duction to all aspects of diagnosis, manage-ment and treatment of the diabetic foot.
Lectures will be combined with practical sessions held in the afternoon at the diabetic foot clinic at the Pisa University Hospital.
Lectures will be in agreement with the International Consensus on the Diabetic Foot & Practical Guideline on the Management and Prevention on the Diabetic Foot.
·COURSE ENDORSED BY
·
EUR
OPEAN
· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
This course is endorsed by EWMA.
Management ofthe Diabetic Foot
Pisa International Diabetic Foot Course, 30 September - 3 October 2015Pisa, Italy
www.diabeticfootcourses.org
EWMA Journal 2014 vol 14 no 2

The second international course on the Neuro-pathic Osteoarthropathic Foot (Charcot Foot) was held in Rheine, Germany, 3-5 July 2014.
51 participants and faculty members from 22 different countries took part in the second International Charcot Foot Course. The 2½ day course gave the participants a rare opportu-nity to train skills and discuss treatment, diag-nosis and management of the Charcot Foot with highly recognised international experts.
The course consisted of a combination of the-oretical lectures, participant/faculty member debates, and especially practical workshops that took place in the specialised diabetic foot clinic at Mathias-Spital in Rheine.
During the practical sessions, participants were divided into small groups, in which they trained the diagnostic and treatment skills necessary for the interdisciplinary treatment of Charcot Foot patients.
The course also offered participants and faculty members plenty of opportunities to network and exchange knowledge during social events that took place every evening.
The next Charcot Foot Course will be held in Rheine in June 2016. Further information is available at www.charcotfootcourses.org
The Charcot Foot Course is open to anyone in-volved in the treatment and/or management of Neuropathic Osteoarthropathic Foot patients; however, the primary participant groups include orthopaedic surgeons, surgeons, podiatrists, and diabetologists working in a multidisciplinary foot clinic, as well as specialised nurses, orthopaedic shoemakers, orthotists, and other health care pro-fessionals involved in the management and treat-ment of Charcot Foot. m
Armin KollerDr. med.
Diabetologist Orthopedic Surgeon
Mathias-SpitalRheine
Germany
Maximillian SpraulProf. Dr. med.
Diabetologist Orthopedic Surgeon
Mathias-SpitalRheine
Germany
www.charcotfootcourses.org
Report from the 2nd Charcot Foot Course
Participants and faculty members of the 2014 Course
2nd International Course onThe Neuropathic Osteoarthropathic Foot (Charcot)Advanced Postgraduate Course
Rheine, Germany · 3 -5 July 2014
2 ½ DAY COURSE
EWMA Journal 2014 vol 14 no 2 94

EWMA is preparing a guidance document on Negative Pressure Wound Therapy (NPWT) which aims at establishing evidence and best practice for the use of the treatment. In addition, the docu-ment will explore the health economic aspects of the use of NPWT, cross-sectoral use of the treatment and digital health per-spectives.
Since EWMA published the first document on NPTW in 2007 , the treatment has developed considerably and is increasingly be-ing used in the treatment of wounds of various aetiologies. In-creased portability has enabled the use of NPWT outside the hos-pital setting, and the development of advanced sensors, links NPWT to the eHealth agenda, which broadens the scope of the treatment. In light of this, the document will provide:
n An overview of the evidence for the use of NPWT based on a literature search; n The health economic aspects of the use of NPWT technology; n The cross-sectoral use of NPWT with a focus on its barriers to implementation;n An overview of the eHealth perspectives on the use of NPWT technology; n An overview of links to other EWMA documents and intervention areas such as Home Care-Wound Care ect.
The final document will be published in 2015, and it is ex-pected that draft conclusions will be presented in a key ses-sion during the EWMA 2015 conference in London.
The EWMA NPWT guidance document will be prepared by a working group of experts and edited by EWMA Immediate Past President Jan Apelqvist.
EWMA GUIDANCE DOCUMENT ON NEGATIVE PRESSURE WOUND THERAPy
1 European Wound Management Association (EWMA). Position Document: Topical negative pressure in wound management. London: MEP Ltd, 2007
EWMA NEWS
HOME CARE – WOUND CARE PROJECT IN THE UK
EWMA is initiating the development of a guidance document with experience- and evidence-based recommendations for wound care in home and community care in the UK.
Like many other European healthcare systems, the UK’s Na-tional Health Service is facing an enormous economic chal-lenge. With the shift in the location of the provision of health services from secondary to primary care, EWMA aims to en-sure that modern, advanced wound care is provided in the community care and home care sectors, and thus advocates appropriate skills, knowledge, and level of education of the care providers.
With the publication of the Home Care – Wound Care docu-ment in May 2014, the first step to achieve this aim has been taken. The document provides a set of recommenda-tions on the above topics on a general European level.
Focus on United KingdomBy involving key clinicians from EWMA and relevant British organisations and educational institutions, EWMA will devel-op a guidance document with both experience- and evi-dence-based recommendations for wound care in home and community care in the UK. The document will pay special attention to these subjects:n Organisation of care on a political leveln Organisation of the wound care team on a practical leveln Education, training, and competencies for clinicians,
service providers, patients and their familiesn Range and use of products
Apart from developing a document aimed at the UK, the goal is to establish a network of home care providers, nurses, industry partners, and policy makers in the UK and thus create a body of experts to advocate the objectives of the project. The first results are to be presented during the EWMA 2015 Conference in May in London.
EWMA LEG ULCER GUIDANCE DOCUMENTIn 2015-2016 EWMA will work to update recommendations for leg ulcer prevention and treatment. The objective is to produce a practical guidance document which will address the challenges related to varying methods for leg ulcer treat-ment in the different European countries. The guidance doc-ument will include venous, arterial and mixed leg ulcers.These methods include the involvement of different types of
medical and nursing staff and differences in the selection of treatments. By addressing these differences, EWMA aims to produce a set of recommendations that will be suitable for implementation throughout Europe.
The EWMA Leg Ulcer Guidance Document will include: n A description of the specific issues related to diagnosis and treatment of arterial and venous leg ulcers;n Examination of national differences in the professionals involved in leg ulcer treatment and existing treatment structures; n An evaluation of which groups of professionals should be involved in the treatment team, and their responsibility within a multi-professional group;n Appropriate primary and secondary endpoints ;
n Health economic aspects of treatment choices; n Considerations concerning the patient perspective;n A treatment algorithm.
EWMA Journal 2014 vol 14 no 2 95
This fall marks the completion of the second year of the EU-funded SWAN-iCare project. The aim of the SWAN-iCare project is to develop a device that allows for the monitoring and personalised management of hard-to-heal Diabetic Foot Ulcers and Venous Leg Ul-cers.
For the remaining two years of the project, EWMA will play as active a role as ever in the in the project consortium.
One of EWMA’s key roles in the SWAN-iCare consor-tium is to facilitate the dissemination of information to raise awareness about the project. A central platform from which to provide that deliverable is the annual EWMA conference, and the SWAN-iCare project was represented there again this year. As part of the scientific program, Marco Romanelli, MD, PhD, of the University of Pisa gave the e-poster presentation entitled “Smart Wearable and Autonomous Negative Pressure Device (SWAN) for Wound Monitoring and Therapy”.
During the first part of the SWAN-iCare project, EWMA played an active role in defining the clinical and end-user requirements of the projected wound care device, and EWMA specialists aided the design and development process and eased decision making.
With that part of the project completed, EWMA’s role is about to change. For the remainder of the project, EWMA will focus on the verification and clin-ical validation of the developed prototype, and the immense resource of wound care competence in the EWMA network will again be put into play.
The current status of the SWAN-iCare project is that everything is progressing according to plan. A lot of challenging work is scheduled for the remaining two years of the project, but EWMA is dedicated to keep-ing the project moving forward and is excited to keep updating the progress.
The United4Health project was started in January 2013 and is now more than half way through the 3-year project period. A core ambition of the United4Helath project is to highlight the role of healthcare providers in the successful implementation of telehealth and telemedicine solutions in clinical practice. In order for these solutions to work, it is essential that healthcare providers adopt innovative health and care service models.
To support that objective, EWMA has been given the task of ensuring that the relevant medical scientific communities representing the healthcare providers are informed about the United4Health project and results as well as the results coming out of the previous EU-funded project on telehealth and telemedicine (the Renewing Health project). The final report on the previous project was released in June
2014 and can be downloaded at www.renewinghealth.eu. EWMA is also responsible for communicating the mes-sage about the central role of healthcare providers in the implementation and large-scale deployment of telehealth and telemedicine solutions.
We do this by: n Developing a dissemination tool kit targeting clini-
cians. This is developed for wound care and wound care clinicians. It includes activities during the an-nual EWMA conference, the publication of a docu-ment on eHealth in wound care, as well as a number of other dissemination activities. Those activities have been ongoing since the spring of 2013 and have been described in a report that will be used to inspire other medical societies (primarily those representing clinicians and researchers working within COPD, CHF, and diabetes) to initiate similar activities.
The author group responsible for the docu-ment on eHealth in wound care has been estab-lished and will start working in October 2014.
EWMA’s participation in EU-funded projects – Update
EWMA Journal 2014 vol 14 no 2 96

The expected publication date is May 2015. The document will be written in collaboration with the Australian Wound Management Association (AWMA), and the author group also includes representatives from the EWMA Council and the wound care pilot study conducted within the Re-newing Health project.
n Arranging 2-3 user advisory board meetings in col-laboration with the local pilot sites involved in the United4Health project and the medical societies working on a national level within the relevant dis-ease areas. These meetings will be arranged in 2015 and will aim to ensure that the perspectives of the different user groups (including clinicians, patients, and decision makers) are taken into consideration when the key messages of the United4Health project are formulated. The meetings will also aim to sup-port the engagement of the user groups in the large-scale deployment of telehealth and telemedicine solutions.
With regards to EWMA’s deliverables for the project, they are progressing according to plan, with some mi-nor delays. We look forward to continuing our work on the dissemination of key messages about eHealth in wound care and hope that our members and network of wound care clinicians will engage in discussions about those messages during the EWMA conference and by sending us feedback.
In this issue of the EWMA Journal, you will have the opportunity to read more about the telemedical wound assessment system used in Denmark as well as the national deployment of that system (page 43). m
7th Joint Meeting of the European Tissue Repair Society & the Wound Healing Society
21-23 October 2015Copenhagen, Denmark
www.etrs-whs2015.org
E T R S
WHS
For more information about the SWAN-iCare project, visit www.swan-icare.eu For more information about United4Health, visit www.united4health.eu
EWMA Journal 2014 vol 14 no 2

Appreciations by Salla Seppänen
Elia Ricci became a member of the council in 2011. With his vast experience from his work as Director of the Difficult Wound Healing Unit in Turin, Italy, he has brought significant expertise and insights to the EWMA Council and EWMA projects in general. Elia has been a team player and has shown good ability to adapt to multicultural environments, through his memberships and participation in several international organisations and conferences. Among oth-ers, Elia is a founding partner and member of the board of the Italian Associa-tion for the study of Cutaneous Ulcers (AIUC). I want to thank Elia for his effort during his 3 years in the EWMA Council and wish him best of luck in the future.
Paulo Alves joined the EWMA Council in 2008 and was re-elected in 2011. During these six years in the council, Paulo has played a big role in the EWMA Education Com-mittee and the Scientific Commit-tee. With his expertise and experi-ence, Paulo has shown great com-passion and brought creativity and good ideas to both committees. He has shown responsibility and embraced the different challenges with a high of professionalism. In addition, he has a great personal-ity and has been a reliable and pleasant person to work with. Paulo will remain engaged with EWMA in the years to come through his participation in the Education Committee. His participation has been of great value and I thank him for his time in the council.
Javorka Delic was elected into the EWMA Council for the 2011-2014 term. Javorka has much knowledge regarding practice and skills within the field of wound pathology which she works devoted with in her job as Head of the Department for preven-tion and treatment of peripheral vascular diseases in Belgrade, Serbia. As the President of the Serbian Wound Healing Society (SWHS), she has worked hard to put the im-portance of wound care on the agenda in Serbia. Her enthusiasm is inspiring and the collaboration between EWMA and the Serbian Wound Healing Society will contin-ue to grow in the years to come. Her presence in the EWMA Coun-cil will be missed. On behalf of the Council, I wish her good luck and look forward to collaborating with her in the future.
Nada Kecelj Leskovec was elected to the EWMA Council in 2011 by the Cooperating Organisations Board as the candidate of the Wound Management Association of Slovenia (WMAS). Nada works as an Assistant Professor in the Faculty of Medicine at the University of Ljubljana, Slove-nia and has written several publica-tions and research projects within wound care. Through her time in the EWMA Council, Nada has been a member of the Cooperating Organ-isations Liaison Group (COLG) and the EWMA Communication Group. She has been a valuable member of the EWMA Council and her contri-bution has been much appreciated. On behalf of the EWMA Council, I thank her for her time in the Coun-cil and look forward to continuing the collaboration with her, in her role as the Cooperating Organisations board representative of WMAS.
EWMA Journal 2014 vol 14 no 2 98

EWMA
New EWMA Council Members
The individual members and the Cooperating Organisations Board elected seven EWMA Council members during the EWMA-GNEUAPP 2014 Conference held in Madrid in May:
n Mark Collier (United Kingdom) [Re-election]n Edward Jude (United Kingdom)n Alberto Piaggesi (Italy)n José Verdú Soriano (Spain) [Re-election]n Jan Stryja (Czech Republic)n Andrea Pokorná (CSLR, Czech Republic)
(Elected by the EWMA Cooperating Organisations Board)n Hubert Vuagnat (SAfW Romande, Switzerland)
(Elected by the EWMA Cooperating Organisations Board)
After the Annual General meeting, the new EWMA Council elected Severin Läuchli (Switzerland) as President Elect. He will step up as President in 2015. Furthermore, José Verdú Soriano (Spain) became the new Scientific Recorder after Gerrolt Juke-ma, and Luc Gryson (Belgium) took over as the new Treasurer.
The EWMA Council welcomes the new members and looks forward to working with them.
Sebastian Probst was elected to join the EWMA Council in 2011 by the Cooperat-ing Organisations Board as the candidate of the Swiss Association for Wound Care (SAfW – German section). Sebastian has been a member of the Scientific Commit-tee and the Cooperating Organisations Li-aison Group (COLG). He has always been very active and present at the different meetings, bringing with him a lot of energy and enthusiasm. Next to these obligations he has played a crucial role as chair in the development and recent publication of the Home Care – Wound Care document, to which he devoted a great deal of his time. Sebastian has been a valued representative of EWMA to a variety of stakeholders on many different occasions. His contribution to the EWMA Coun-cil has been much appreciated and we hope to continue the collaboration in the future. Luckily, Sebastian is now a member of the Cooperating Organisations Board, repre-senting SAfW (German speaking section), so we will surely see him again.
Edward JudeAlberto Piaggesi Andrea Pokorná
Jan StryjaHubert Vuagnat
EWMA Journal 2014 vol 14 no 2 99

It is a true testament to any book to achieve a 4th edition, and so it is with the book Acute and Chronic Wounds: Current Management Concepts, 4th edition by Ruth Bryant and Den-ise Nix. The first view of this hardcover book invites the reader to pick it up and browse through the revised and updated 627 pages, which contain contributions by 42 well-known experts in their fields. Bringing together the writing styles of so many authors into a cohe-sive and seamless piece of work is a tribute to the authors and an acknowledgement of their own dedication to the revision of this much referenced textbook.
The book is divided into eight sections con-taining 39 chapters covering topics such as foundations of wound management, pressure ulcers, lower extremity wounds, wound bed preparation, biophysical and biological agents, critical cofactors, acute and traumatic wounds, and special patient populations. Each chapter includes many clear, concise, and easy to fol-low illustrations and diagrams. In particular, this edition includes 73 high quality images presented over 20 pages that are referenced throughout the book to provide a useful re-source for the reader to understand aetiolo-gies and treatment choices. The content re-flects the diversity of wound aetiologies and the challenges faced by wound care practition-ers in meeting patient needs. In addition to more prevalent wounds such as venous leg and pressure ulcers, the authors have also in-cluded sections on neonatal wounds; traumat-ic wounds due to bullets, blasts, and vehicle
crashes; and wound management strategies in palliative care.
The writing style is clear throughout the book and is easy to understand by students for whom English is not their first language. The clear index and logical flow of chapters makes it easy to find information and use the book to support practice and further education. The authors have provided many useful examples of documentation tools, policies, and proce-dures that readers can adapt to suit their local needs.
I believe this book should be an essential text for students who are undertaking further education in wound management. In particular, the self-assessment exercises at the end of each chapter are useful to help readers gauge their understanding of key concepts and knowledge of a subject area and can provide a means for ongoing assessment of their learning. m
Georgina GethinMember of the EWMA Council
PhD, RGN, PG Dip Wound Healing, FFNM
RCSI, Dip Anatomy, Dip Applied Physiology and
Senior Lecturer
School of Nursing and Midwifery,
National Universityof Ireland,
Galway, Ireland.
Correspondence:Georgina.gethin@
nuigalway.ie
Book Review
Acute and Chronic Wounds: Current Management Concepts, 4th editionRuth A. Bryant and Denise P. NixPublished by: Mosby, Inc., an affiliate of Elsevier, Inc., St. Louis, Missouri. 2012.
EWMA Journal 2014 vol 14 no 2 100

EWMA
At the European College of Veterinary Sur-geons’ (ECVS) 23rd Annual Scientific Meeting at the Bella Sky Conference Centre in Copen-hagen, past EWMA President (1997-1999) and founding council member Professor Finn Gottrup was invited to give the State of the Art Jorg Auer lecture. The Jorg Auer Lecture is a recurrent programme point at the ECVS yearly scientific meetings given by a special-ist in the field of surgery. It is named after the first President of ECVS, Jorg Auer (1991-1995).
The meeting took place 3-5 July 2014 and gath-ered veterinary surgeons and other specialists in veterinary health care for three days of sharing knowledge and best practices about treatment and surgery in animals. In his lecture, entitled “An integrated, multidisciplinary wound-healing department improves standards of patient care and outcomes, education, and clinical research”, Pro-fessor Gottrup presented important perspectives on the organisation of human wound care based on his many years of experience from the field.
Former EMWA President gives the honorary State of the Art Jörg Auer Lecture at the European College of Veterinary Surgeons’ annual meeting in Copenhagen
About the European College of Veterinary SurgeonsECVS was formed in 1991 by a group of European veterinarians involved in surgery who, inspired by the American sister organisation The American College of Veterinary Surgeons, decided to form a forum for the European advancement of veterinary surgery. The first annual meeting was held in Lenzburg in 1992; since then, the meeting has grown to be an important scientific veterinary event in Europe.
On behalf of Professor Gottrup EWMA is proud that he has been awarded the honour of closing the 23rd annual ECVS meeting by delivering the Jorg Auer lecture.
EWMA works continuously to reach beyond the professional borders of our field and sup-port the interdisciplinary sharing of knowl-edge and experience from experts with specialties other than wound care. Professor Gottrup has been deeply involved in these endeavours, and the invitation from ECVS is a very welcome outcome of this work.
In this issue of EWMA journal, you can read more about veterinary wound care in the article from the Veterinary Wound Healing Association on page 39. m
EWMA Journal 2014 vol 14 no 2 101
EWMA
Mölnlycke Health Care Abwww.molnlycke.com
Ferris Mfg. Corp.www.PolyMem.eu
Wound ManagementSmith & Nephew Medical Ltdwww.smith-nephew.com/wound
sorbion GmbH & Co. KGwww.sorbion.com
Curea Medical GmbHwww.curea-medical.de
DryMaxwww.absorbest.se/ drymax-woundcare
Nutricia Advanced Medical Nutritionwww.nutricia.com
SastoMedwww.sastomed.com
Corporate A
acelitywww.acelity.com
BSN medical GmbHwww.bsnmedical.comwww.cutimed.com
Coloplastwww.coloplast.com
3M Health Carewww.mmm.com
ABIGO Medical ABwww.abigo.se
B. Braun Medical www.bbraun.com
Chemvironwww.chemvironcarbon.com
ConvaTec Europewww.convatec.com
Flen Pharma NVwww.flenpharma.com
PAUL HARTMANN AGwww.hartmann.info
Lohmann & Rauscherwww.lohmann-rauscher.com
Corporate Sponsors
Corporate B
SOFAR S.p.A.www.sofarfarm.it
Söring Gmbwww.soering.com
Strykerwww.stryker.com
Laboratoires Urgowww.urgo.com
Welcare Industries SPAwww.welcaremedical.com
EWMA Journal 2014 vol 14 no 2 102

Conference Calendar
For web addresses please visit www.ewma.org
Organisations
Conferences 2014 Theme Month Days City Country
Pisa International Diabetic Foot Courses 2014 Oct 1-4 Pisa Italy
National multidisciplinary Conference for Wound Professionals (NOVW)
Wound Ecology Oct 7 Ede The Netherlands
23rd European Academy of Dermatology and Venereology (EADV) Congress
Building Bridges Oct 8-12 Amsterdam The Netherlands
XVII Congress of the Hungarian Wound Care Society (MSKT) Oct 16-17 Budapest Hungaria
Fall Symposium on Advanced Wound Care and Wound Healing Society (SAWC)
Oct 16-18 Las Vegas USA
8th National Congress of BEFEWO Oct 23 Uccle Belgium
II Congress for Chronic Wounds Management of the Serbian Wound Healing Society (SWHS)
Oct 24-25 Belgrade Serbia
Lymphoedema Seminar (Danish Lymphoedema Framework) Oct 30 Copenhagen Denmark
The 5th Inter-regional Conference Oct 30-31 Ekaterinburg Rusland
Conference of the Canadian Association of Wound Care (CAWC)
Action 2014: Skin Health For Canada
OctNov
30 - 2 Toronto Canada
Nordic Diabetic Foot Symposium Nov 5-6 Malmö Sweden
VII Ibero-Latin American Congress about Ulcers and Wounds (SILAUHE)
Nov 5-8 Tucuman Argentina
Total Contact Cast Workshop Nov 7 Malmö Sweden
Annual Meeting of the Danish Wound Healing Society (DSFS) Nov 20-21 Kolding Denmark
1st Iberian Symposium on Diabetes (ELCOS Sociedade de Feridas)
Nov 21-22 Arronches Portugal
Symposium APTFeridas 2014 Nov 27-28 Porto Portugal
9th National Wound Care Conference of the Turkish Wound Management Association (WMAT)
Nov 27-30 Antalya Turkey
2015
National Conference of Wound Healing (SFFPC) Jan 18-20 Paris France
XIII. National Congress (CSLR) Interdisciplinary collaboration in the treatment of wounds and skin defects
Jan 22-23 Pardubice Czech Republic
XVIII National Wound Management Conference (FWCS) Jan 29-30 Helsinki Finland
Annual Meeting of the Norwegian Wound Care Society (NIFS) Feb 5-6 Oslo Norway
4th Congress of the Spanish Society of Wounds (SEHER) Feb 5-7 Madrid Spain
12th EADV Spring Symposium Mar 5-8 Valencia Spain
Diabetic Foot Global Conference 2015 (DF Con) Mar 19-21 Los Angeles USA
Deutscher Pflegekongress /Deutscher Wundkongress (ICW Initiative Chronische Wunden, AWA Austrian Wound Asso-ciation, Swiss Association for Wound Care (SAfW))
May 6-8 Bremen Germany
25th Conference of the European Wound Management Associa-tion (EWMA)
Wound Care – Shaping The Future A Patient, Professional, Provider and Payer Perspective
May 13-15 London United Kingdom
7th International Symposium on the Diabetic Foot May 20-23 The Hague The Netherlands
New Zealand Wound Care Society 7th Annual Conference 2015 (NZWCS)
Wound Care – A Matter of Balance May 21-23 Blenheim New Zealand
16th EFORT Congress May 27-29 Prague Czech Republic
17th annual congress of the German Wound Healing Society (DGfW)
June 26-28 Bochum Germany
18th Annual European Pressure Ulcer Advisory Panel Meeting (EPUAP)
Sep 16-18 Ghent Belgium
16th European Burns Association Congress (EBA) 16-19 Hannover Germany
Pisa International Diabetic Foot Courses 2015 Oct Pisa Italy
7th Joint Meeting of the European Tissue Repair Society (ETRS) & the Wound Healing Society (WHS)
Oct 20-22 Copenhagen Denmark
Sep
7th Joint Meeting of the European Tissue Repair Society (ETRS) & the Wound Healing Society (WHS)
EWMA Journal 2014 vol 14 no 2 103

AAWC NEWS
Vickie R. DriverPresident of AAWC
AAWCAssociation for
the Advancement of Wound Care
EWMA international Partner Organisation
Dear Readers,
The Association for the Advancement of Wound Care (AAWC) is pleased to provide information about its activities and progress to the European Wound Management Association (EWMA). Due to the successful development of many unique and exciting programs and educational offerings, the AAWC has had nearly 20 years of organizational growth.
AAWC’s strategic plans are designed to promote growth in the United States (US) and across the globe. Our leadership is working toward a unified voice in the US government and public policy. One goal is to consolidate efforts among societies, such as the creation of clinical guidelines, so that wound care professionals and government agencies will refer to one set of resources. These resources will be crafted by united development teams that are supported by tens of thousands of professional organizational members. As we approach our 20th Anniversary in 2015, we will be collaborating on important initiatives with organizations such as the Centers for Medicare and Medicaid Services and the Food and Drug Adminis-tration. For example, clinically meaningful wound healing endpoints are important for the approval of products and the development of coverage policies in the US. Currently, “complete closure” is the only accepted relevant or meaningful measurement. Because this limits our patients’ access to important therapies, the AAWC will be involved in coordinat-ing a united effort to expand our wound healing endpoints. If you will be in the US April 30-May 3, 2015, please learn more by attending the AAWC’s 20th Anniversary Membership Meeting entitled “Help Shape Our Field!” at the Symposium on Advanced Wound Care (SAWC) Spring in San Antonio on May 1, 2015.
Additionally, we are thrilled to announce that the AAWC will host a special clinical practice track with 15 sessions at SAWC Spring 2015. These sessions are novel, clinical, and evidence-based. They include best practice pearls that can be implement-ed as early as Monday morning. This track will cov-er what to do to grow wound care as a professional practice and career. Furthermore, it will empower the learner with the knowledge about how to imple-ment the care.
Our leadership continues to develop a culture in which we assist one another and embrace our dif-ferences by providing attention to all facets of our field. It is with our members’ and supporters’ con-tinued commitment that we are able to accomplish our goals and objectives. I would be remiss not to mention how we greatly value our international partnerships, which have more recently led to the development of a joint manuscript entitled “Manag-ing Wounds as a Team” that was crafted by the AAWC, EWMA, and the Australian Wound Man-agement Association. This unprecedented joint manuscript on the multidisciplinary approach to wound care was launched this year and is available at www.journalofwoundcare.com/resources.
We are proud to be represented by many members from several countries. The AAWC thanks all of its multidisciplinary members and warmly welcomes international members to join us to take advantage of many AAWC membership benefits. m
ABOUT AAWCAs the leading interpro-
fessional organisation in the United States dedicated to
advancing the care of people with and at risk for
wounds, AAWC provides a whole year of valuable
benefits! Be sure to join us for near daily updates and
alerts on Facebook and LinkedIn.
www.aawconline.org
HELP SHAPE OUR FIELD!Attend the AAWC’s 20th Anniversary Membership Meeting at the Symposium on Advanced Wound Care (SAWC) San Antonio, US, April 30 - May 3, 2015
EWMA Journal 2014 vol 14 no 2 104
The World Alliance for Wound and Lymphoedema Care (WAWLC) organises its annual symposium 2014 in con-nection with the annual meeting of the Canadian Asso-ciation of Wound Care (CAWC) in Toronto, 30 October – 2 November.
WAWLC will host two international sessions during the CAWC conference:
Friday 31 October 10.30 – 11.30 (Session 5) New lessons and knowledge about wound care in limited resource countries Presenters: David Keast, John Macdonald, Terry Treadwell, Robyn Bjork; Moderator: David Keast
Friday 31 October 14.00 – 16.00 (Session 13)Debate around wound care kit for limited re-source countries Presenters: David Keast, John Macdonald, Hu-bert Vuagnat, Eric Comte Moderator: Terry Treadwell
The Friday afternoon session will present the final pro-posal for a wound care kit for use in resource limited settings. This is developed by WAWLC in collaboration with the Medecins Sans Frontieres (MSF). The development of the wound care kit has taken place during workshops at the EWMA 2013 and EWMA 2014 conferences. The final version of the kit will be circulated to wound care companies with the objective to receive their proposals for products to be included in the kit.Since 2013 WAWLC have organised its annual sympo-sium in connection with a major international wound or lymphoedema care conference.
“Action 2014: Skin Health For Canada”
Discussing Best Practice in Skin, Wound, Ostomy, Continence and Lymphedema
A joint meeting of the Canadian Association of Wound Care and the Canadian Association for Enterstomal Therapy, in collaboration with the World Alliance for Wound and Lymphedema Care. This first-time initiative will offer education, research, skills and networking opportunities. Don’t miss it! WAWLC was officially launched as a global partnership encouraged by the WHO in 2009. Read more about WAWLC activities at www.wawlc.org. WAWLC is an international partner organisation of EWMA.
WAWLC ANNUAL SYMPOSIUM 2014 WITH FOCUS ON WOUND CARE KIT
EWMA Journal 2014 vol 14 no 2 105
Science, Practice and Education

The 10th national conference of the Australian Wound Management Association (AWMA) was held in Gold Coast, Queensland from 7-10 May 2014. The theme of the conference was “A Gold Standard: Research and Clinical Practice”. The goal of the conference was to recognise the integral role that research has and should have in clinical prac-tice.
The AWMA also celebrated its 20th anniversary at the conference. The association was founded in Perth in 1993 and was formally recognised at the first AWMA conference in Melbourne in March 1994. The AWMA is a multidisciplinary association with approximately 3,000 members and has forged strong connections with other international wound healing societies, including the EWMA. The presi-dent of AWMA, Dr. William McGuiness, officially opened the 10th AWMA conference to 839 dele-gates, a new attendance record. The master of cer-emonies for the conference was the charismatic Dr. Sally Cockburn, a general practitioner who is better known as the Australian radio celebrity “Dr. Feelgo-od”. Her humorous and crazy ways of introducing each presenter set an easy and relaxing tone for the conference.
The plenary sessions were led by the “best-of-the-best” national and international keynote speakers, including the widely published American nurse-sci-entist Dr. Diane Cooper, the UK’s leading practi-tioner in diabetes foot management Dr. Gerry Ray-man, and the immediate past president of the AWMA Associate Professor Michael Woodward. The five plenary sessions were complemented by three concurrent free paper presentation sessions of
Ann-Mari FagerdahlMember of theEWMA council
Correspondence:[email protected]
AWMAAustralian
Wound Management
Association
EWMA international Partner Organisation
www.awma.com.au
Report from the 10th national conferenceof the Australian Wound Management Association in Gold Coast
high scientific and clinical quality. Each session consisted of five rooms with presentations in the topics of “science and technology”, “translation”, “best practice” (two rooms), and “research and policy”. Each presentation was scheduled for 10 minutes with 3 minutes for questions. Each presentation was met with enthusiasm and generated interesting discussion.
All in all, the delegates of the 10th AWMA confer-ence had access to 15 plenary presentations, 90 free paper presentations, and several industry-spon-sored sessions. The AMWA conference was also preceded by workshops and short seminars with a practical focus on topics such as difficult wound dressing and compression therapy techniques.In addition to the important and informative scien-tific programme, the conference facilitated net-working and informal gatherings of delegates from across Australia, a country that is equal in size to all of Europe. The welcome reception at the opening of the exhibition was well attended. The EWMA had a stand at the exhibition hall with many materials to distribute, including the debridement document, the antimicrobial document, and information sheets about the 2015 EWMA conference in Lon-don. The Australian delegates showed a huge inter-est in the EWMA and the 2015 conference in Lon-don, and all EWMA materials were completely dis-tributed within half an hour.
To further facilitate social networking, the confer-ence organizers arranged a fantastic conference dinner. The theme for the evening was “The Great Gatsby – the Golden Era.” Many of the guests were dressed in true 1920s spirit – there were many Al Capones and Jay Gatsbys and lots of feathers and glamour. Not only did the guests enjoy delicious food, but they also learned the Charleston and danced the night away to the superb eight-piece band Capitol Groove.
The conference closed with an interesting informal panel discussion of several famous wound experts who shared their vision for wound management 10 years from now in 2024. The panel ended the dis-cussion by handing over the conference to the 2016 AWMA organising committee in Melbourne. Overall, the 10th AWMA conference was a well organised programme of high scientific and clinical quality, with just the right balance between scientif-ic and social activities. The EWMA congratulates the AWMA on their 20th birthday and a successful conference. m
The EWMA stand was very well visited and the
delegates showed a large interest in the organisation and the upcoming EWMA
Conference in London.
Organisations
EWMA Journal 2014 vol 14 no 2 107

AWTVNFAll Wales
Tissue Viability Nurse Forum
Trudie youngDirector of Education and
Training, Welsh Wound Innovation Centre.
Chair All Wales Tissue Viability Nurses Forumr
EWMA Cooperating Organisation
www.welshwoundnetwork.
org
IntroductionTissue viability is an umbrella term covering skin health and wounding, within people of all ages regardless of case setting and at any point along the patient’s journey through their health care epi-sode. Tissue viability skills include the holistic assessment of patients with actual or potential skin/tissue damage and the implementation of appropri-ate prevention and treatment strategies. Tissue via-bility is a speciality that considers the protection of tissue integrity alongside all aspects of skin and soft tissue injuries ranging from simple to complex wounds, across acute and chronic wounds, in addi-tion to tissue damage consequential to underlying chronic disease – e.g., venous hypertension.
BackgroundAcross Wales, there are 32 specialist tissue viability nurses, and these individuals are members of the All Wales Tissue Viability Nurses Forum (AWTVNF). While providing a platform for sharing information and experience, they foster collaborative work between AWTVNF members and other healthcare organisations, communities and individuals. The AWTVNF was formed in 2003 to provide strategic guidance to facilitate quality tissue viability service
throughout Wales. The members provide clinical support and advice to patients in hospitals and their own homes. The AWTVNF meets three times a year at a central location in Wales, UK. The AWTVNF receives advice and guidance from its professional advisors. Professors Sue Bale and Michael Clark provide strategic advice and guid-ance. Pat Roberts and Ann Yates provide condition-specific advice (lymphoedema, continence).
Clinical guidanceThe AWTVNF has been proactive in providing clini-cal guidance to nurses in Wales. To date, the forum has produced the following documents: All Wales Guidelines for Faecal Management Systems (2010); All Wales Tissue Viability Nurse Forum, Best Practice Statement; the Assessment and Management of Skin Tears (2011); All Wales Tissue Viability Nurses Forum; All Wales Guidance for the Use of Larval Debridement Therapy (2013); and All Wales Tissue Viability Nurse Forum and All Wales Continence Forum; Best Practice Statement on the Prevention and Management of Moisture Lesions (2013).
The latest document from the AWTVNF.
Left to right: Barbara Pritchard, TVN, Ann Yates – Director of Continence Services, Jean White – Chief Nurse for Wales, Trudie Young – TVN & Chair AWTVNF, Julie Evans, TVN and past chair of AWTVNF.
In addition, the Forum adapted the NPUAP/EPUAP pressure ulcer prevention and management guide-lines for use in Wales (All Wales Guidance for the Prevention and Management of Pressure Ulcers (2011)). The AWTVNF documents can be found at the AWTVNF website, which is hosted on the Welsh Wound Network website www.welshwoundnetwork.org
Education and trainingThe AWTVNF members contribute to the curricu-lum planning and delivery of education and training with the universities based in Wales. In addition, they participate in local health board internal train-ing and induction programs.
All Wales Tissue Viability Nurse Forum
Organisations
EWMA Journal 2014 vol 14 no 2 108
The group has developed clinical competencies to assist in standardising tissue viability practice in Wales. The compe-tencies are for qualified and unqualified nursing staff and cover negative pressure wound therapy, pressure ulcer pre-vention and management, venous leg ulcer prevention and management, wound care and larval therapy. The compe-tencies have been validated by Agored Cymru (www.agored.org.uk/).
All Wales wound care formularyThe forum has worked alongside the national body to devel-op a wound care formulary that is used by all health boards in Wales. The selection of wound management products to be included in the formulary is subject to a rigorous and transparent process. This process has been utilised to devel-op a second initiative, the all Wales negative pressure wound therapy contract. It is hoped that these developments will lead to a cost-effective and standardised delivery of wound care within Wales.
Clinical auditThe forum has undertaken a clinical audit on the use of hon-ey dressings in wound management; this was presented at a symposium at the EPUAP conference in 2012.
PublicationThe forum published the results of a pressure ulcer preva-lence audit that was conducted at orthopaedic and commu-nity hospitals in Wales (James J, Evans J A, Young T, Clark M (2010). Pressure ulcer prevalence across Welsh orthopaedic units and community hospitals: surveys based on the Europe-an Pressure Ulcer Advisory Panel minimum data set. Interna-tional Wound Journal 7 (3): 147-152).
Recent developmentsThe forum focuses on the prevention of pressure ulceration as a main target and has recently completed a major project with the National Patient Safeguarding Team and Protection of Vulnerable Adults Team. The document provides guid-ance across Wales on the protection of vulnerable adults in relation to pressure ulcer development and investigation (Pressure Ulcer Reporting and Investigation-All Wales Guid-ance. This document will direct and streamline care within Wales. A past chair and the current secretary of the AWTVNF have recently won a national award for delivering cost-effec-tive leg ulcer care in a social model within one health board within Wales (www.nhswalesawards.wales.nhs.uk/news/33127). It is anticipated that more of these leg clubs will open within Wales with one planned for South Wales in the very near future (www.legclub.org/).
ConclusionThe AWTVNF is a cohesive body of tissue viability nurse spe-cialists that have been working together for 12 years to improve tissue viability practice within Wales through their many activities. The forum is proud to become a cooperating organisation of the European Wound Management Associa-tion and looks forward to sharing best practices and collabo-rating with our counterparts within Europe.
International.
This is how life feels to people with EB.Their skin is as fragile as a butterfly’s wing. They have Epidermolysis Bullosa, a painful and currently incurable skin blistering condition.
www.debra-international.org
65437_Debra_Bobbycar_EWMA_98x297_ICv2.indd 1 20.02.14 16:45
EWMA Journal 2014 vol 14 no 2

AEEVHSpanish Association of Vascular Nursing and Woundswww.aeevh.es
AFIScep.beFrench Nurses’ Association in Stoma Therapy, Wound Healing and Woundswww.afiscep.be
AISLeC Italian Nurses’ Cutaneous Wounds Associationwww.aislec.it
AIUCItalian Association for the study of Cutaneous Ulcerswww.aiuc.it
AMP RomaniaWound Management Association Romaniawww.ampromania.ro
APTFeridasPortuguese Association for the Treatment of Woundswww.aptferidas.com
AWTVNFAll Wales Tissue Viability Nurse Forumwww.welshwoundnetwork.org
AWAAustrian Wound Associationwww.a-w-a.at
BEFEWOBelgian Federation of Woundcarewww.befewo.org
BWABulgarian Wound Associationwww.woundbulgaria.org
CNCClinical Nursing Consulting – Wondzorgwww.wondzorg.be
Cooperating Organisations CSLRCzech Wound Management Societywww.cslr.cz
CWACroatian Wound Associationwww.huzr.hr
DGfWGerman Wound Healing Societywww.dgfw.de
Danish WoundHealing Society
DSFSDanish Wound Healing Societywww.saar.dk
FWCSFinnish Wound Care Societywww.suomenhaavanhoitoyhdistys.fi
GAIF Associated Group of Research in Woundswww.gaif.net
GNEAUPPNational Advisory Group for the Study of Pressure Ulcers and Chronic Woundswww.gneaupp.org
HSWH Hellenic Society of Wound Healing and Chronic Ulcers www.hswh.gr
ICWChronic Wounds Initiativewww.ic-wunden.de
LBAALatvian Wound Treating Organisation
LUFThe Leg Ulcer Forumwww.legulcerforum.org
LWMALithuanian Wound Management Associationwww.lzga.lt
MASCMaltese Association of Skin and Wound Carewww.mwcf.madv.org.mt/
Associated OrganisationsLeg ClubLindsay Leg Club Foundationwww.legclub.org
LSNThe Lymphoedema Support Networkwww.lymphoedema.org/lsn
International Partner OrganisationsAAWCAssociation for the Advancement of Wound Carewww.aawconline.org
AWMA Australian Wound Management Associationwww.awma.com.au
CAWCCanadian Association of Wound Carewww.cawc.net
Debra InternationalDystrophic Epidermolysis Bullosa Research Associationwww.debra.org.uk
EFORT European Federation of National Associa-tions of Orthopaedics and Traumatologywww.efort.org
ILFInternational Lymphoedema Frameworkwww.lympho.org
KWMSKorean Wound Management Societywww.woundcare.or.kr/eng
NZWCSNew Zealand Wound Care Societywww.nzwcs.org.nz
SILAUHEIberolatinoamerican Society of Ulcers and Woundswww.silauhe.org
SOBENFeEBrazilian Wound Management Association www.sobenfee.org.br
WAWLCWorld Alliance for Wound and Lymphedema Carewww.wawlc.org
EWMA Journal 2014 vol 14 no 2 110

For more information about EWMA’s Cooperating Organisations please visit www.ewma.org
MSKTHungarian Wound Care Societywww.euuzlet.hu/mskt/
MWMAMacedonian Wound Management Association
NATVNSNational Association of Tissue Viability Nurses, Scotland
NIFSNorwegian Wound Healing Associationwww.nifs-saar.no
NOVWDutch Organisation of Wound Care Nurseswww.novw.org
PWMAPolish Wound Management Associationwww.ptlr.pl
SAfWSwiss Association for Wound Care (German section)www.safw.ch
SAfWSwiss Association for Wound Care (French section)www.safw-romande.ch
SAWMASerbian Advanced Wound Management Associationwww.lecenjerana.com
SEBINKOHungarian Association for the Improvement in Care of Chronic Wounds and Incontinentiawww.sebinko.hu
SEHERThe Spanish Society of Woundswww.sociedadespanolaheridas.es
SFFPCThe French and Francophone Society f Wounds and Wound Healingwww.sffpc.org
SSiSSwedish Wound Care Nurses Associationwww.sarsjukskoterskor.se
SSOORSlovak Wound Care Associationwww.ssoor.sk
STW BelarusSociety for the Treatment of Wounds (Gomel, Belarus)www.burnplast.gomel.by
SUMSIcelandic Wound Healing Societywww.sums-is.org
SWHS Serbian Wound Healing Societywww.lecenjerana.com
SWHSSwedish Wound Healing Societywww.sarlakning.se
TVSTissue Viability Societywww.tvs.org.uk
URuBiHAssociation for Wound Management of Bosnia and Herzegovinawww.urubih.ba
UWTOUkrainian Wound Treatment Organisationwww.uwto.org.ua
V&VNDecubitus and Wound Consultants, Netherlandswww.venvn.nl
WMAIWound Management Association of Irelandwww.wmai.ie
WMAKWound Management Association of Kosova
WMASWound Management Association Slovenia www.dors.si
WMATWound Management Association Turkeywww.yaradernegi.net
Other CollaboratorsHome Care Europe
ICCInternational Compression Clubwww.icc-compressionclub.com
MSFMédecins Sans Frontièreswww.msf.org
WUWHSThe World Union of Wound Healing Societieswww.wuwhs.org
DFSGDiabetic Foot Study Groupwww.dfsg.org
EADVEuropean Academy of Dermatology and Venereologywww.eadv.org
EPUAPEuropean Pressure Ulcer Advisory Panelwww.epuap.org
ETRSEuropean Tissue Repair Societywww.etrs.org
EucomedEucomed Advanced Wound Care Sector Groupwww.eucomed.org
Organisations
EWMA Journal 2014 vol 14 no 2 111

Science, Practice and Education
Organisations
Cochrane Reviews
Scientific Communication
EWMA
5 Editorial
7 Economic outcomes of a new chronic wound treatment system in Poland. K. Grzegorz, W. Robert, O. N. Małgorzata 15 Dressings for split thickness skin graft donor sites
D. P. Barrit, H. Birke-Sorensen 21 The utility of pulse volume waveforms in the identification of lower limb arterial insufficiency. J. H. Davies, J. E. A. Lewis, E. M. Williams 27 The importance of using a nutritional risk analysis scale in patients admitted to continued care
J. M. Corrales, N. P. Gayo, M. C. P. Águila, A. M. Martín, A. Ribeiro 33 Neonatal facial pressure ulcers related to non-invasive ventilation L Bonell-Pons, P. García-Molina, E. Balaguer-López, M. Á. M., M. C. Rodríguez
35 Healthcare-associated infections (HCAIs). M. Kiernan, D. Leaper 39 The value of veterinary wound management for human wounds and wound care. J. M. Wilmink 43 Telemedical wound assessment on the way to large scale deployment in Denmark. E. W. Henneberg 48 Reflections on the use of telemedicine in wound Care. R. Jelnes 52 R.I.S.E for the prevention of pressure ulcers. G. Gethin, C. McIntosh 56 Setting a course on chronic wounds in Cameroon
A. Same-Ekobo, G. Ehounou, E. Comte, H. Vuagnat
61 Abstracts of recent cochrane reviews. S. Bell-Syer
68 EWMA Journal previous issues and other journals 70 EWMA-GNEAUPP 2014 in Madrid, Spain. G. Jukema 74 Cooperating Organisations activities during the EWMA - GNEAUPP Conference. J. Apelqvist 76 TVS 2014 activities. H. Sandoz 78 The organisation of wound care in England. A. Hopkins 80 Visit EWMA 2015 in London, United Kingdom 82 A report from the EWMA Teacher Network
S. Holloway, D. Hopkins, D. Huljev 84 Home Care – Wound Care. G. Gethin, S. Probst 88 Nordic Diabetic Foot Task Force: status and activities
K. Kirketerp-Møller 90 EWMA study recommendations for clinical investigations in leg ulcers and wound care. P. Price 92 EWMA in collaboration with the EU Joint Action on Chronic Diseases
S. Seppänen 94 Report from the 2nd Charcot Foot Course. A. Koller, M. Spraul 95 EWMA news 96 EWMA’s participation in EU-funded projects – Update 98 EWMA appreciations and new EWMA council members
S. Seppänen100 Book Review: Acute and Chronic Wounds: Current Management Concepts. G. Gethin101 Former EMWA President gives the honorary State of the Art Jörg Auer Lecture at the ECVS annual meeting 102 EWMA Corporate Sponsors
103 Conference calendar104 AAWC news. V. R. Driver105 WAWLC annual symposium 2014 with focus on wound care kit107 Report from the 10th national conferenceof AWMA in Gold Coast A. Fagerdahl108 All Wales Tissue Viability Nurse Forum T. Young110 Cooperating Organisations

















