56
BY KAUSHIK.D.S
| Date post: | 22-Jan-2018 |
| Category: |
Healthcare |
| Upload: | kaushik-ds |
| View: | 116 times |
| Download: | 5 times |

BY
KAUSHIK.D.S

Why is it necessary?
When should be done?

DETAILS
HISTORY
Family history
Gestational history
Delivery details
Neonatal history
GENERAL EXAMINATION
VITALS
APGAR score
ANTHROPOMETRY
HEAD TO FOOT EXAMINATION
NEONATAL REFLEXES

Colour :- Pink, cyanosis, pallor
Appearance of skin :- Vernix, Lanugo hair
Activity :- Normal or diminished
Tremulous movements
Temperature (36.6-37 degree centigrade)
Respiratory rate (30-50 breaths/minute)
Heart rate (100-160beats/minute)
Capillary filling time (less then 3seconds)

score 0 1 2
A-Appearance(colour)
Pale or Blue Body pinkPeriphery blue
Pink throughout
P-Pulse Absent <100/minute >100/minute
G-Grimace(response to suction)
Absent Facial grimace Coughing/crying
A-Activity(muscle tone)
Flaccid Some flexion of limbs
Good activity
R-Respiration Absent Weak,Gasping,
Irregular
Regular respiration,Crying lustily

Weight (2.7-2.9kg)
Length (50 cm)
Head circumference(35cm)
Chest circumference(1.25-2.5cm less than HC)
Upper segment to lower segment ratio (7:1)

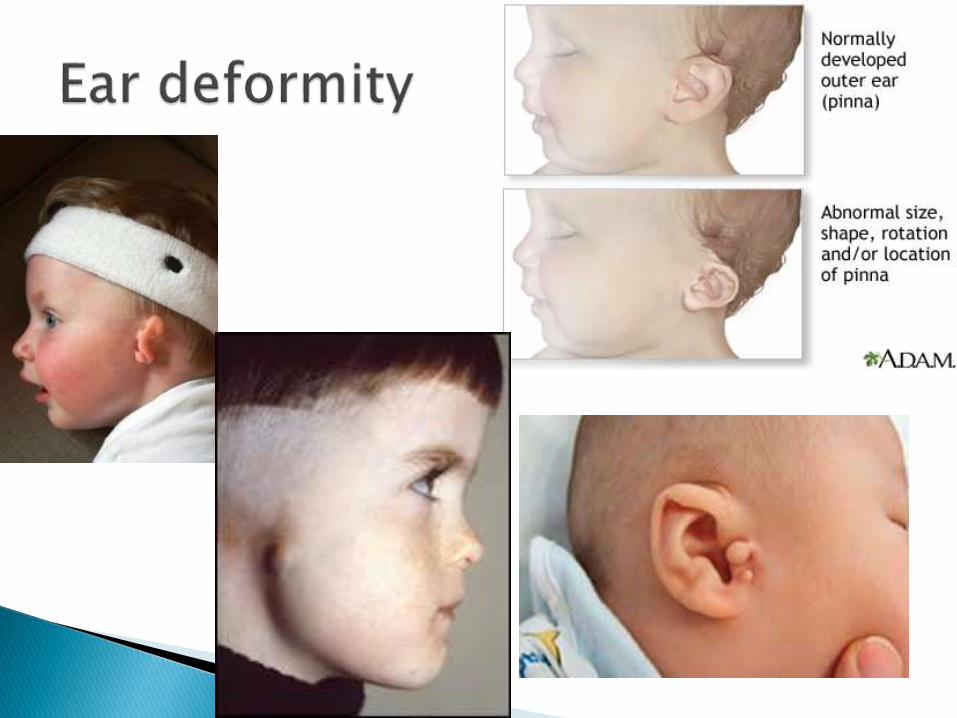
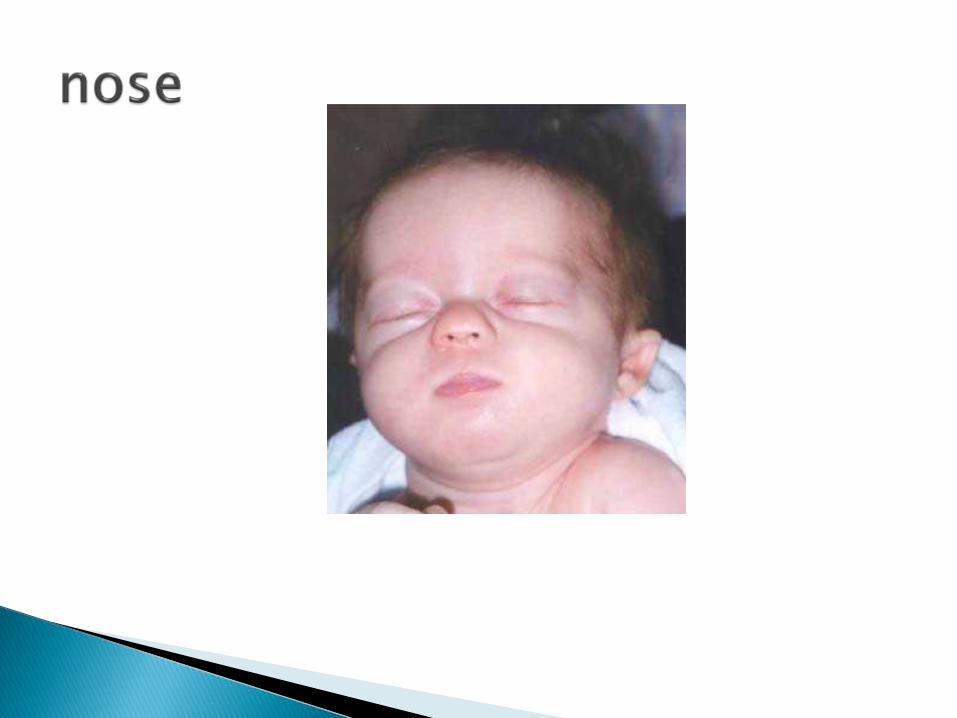
FaceSkullEyesEar deformitiesMouthNoseNeckSkinChest
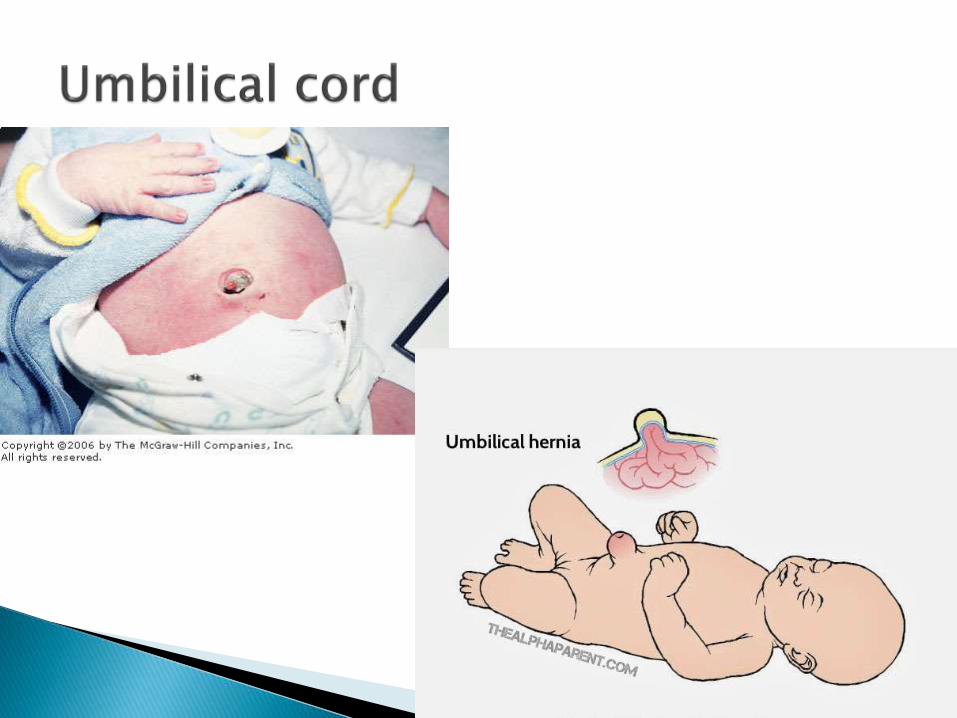
Umbilical cordGenitaliaAnusLimbsSpineHip

oAnterior and posterior fontanelles
oMolding
oCaput succedaneum
oCephalhematoma







Chest
Chest deformities
Breathing
Heart :- location, heart rate, peripheral pulses


Abdomen
Shape, distension
Organomegaly
Unusual masses


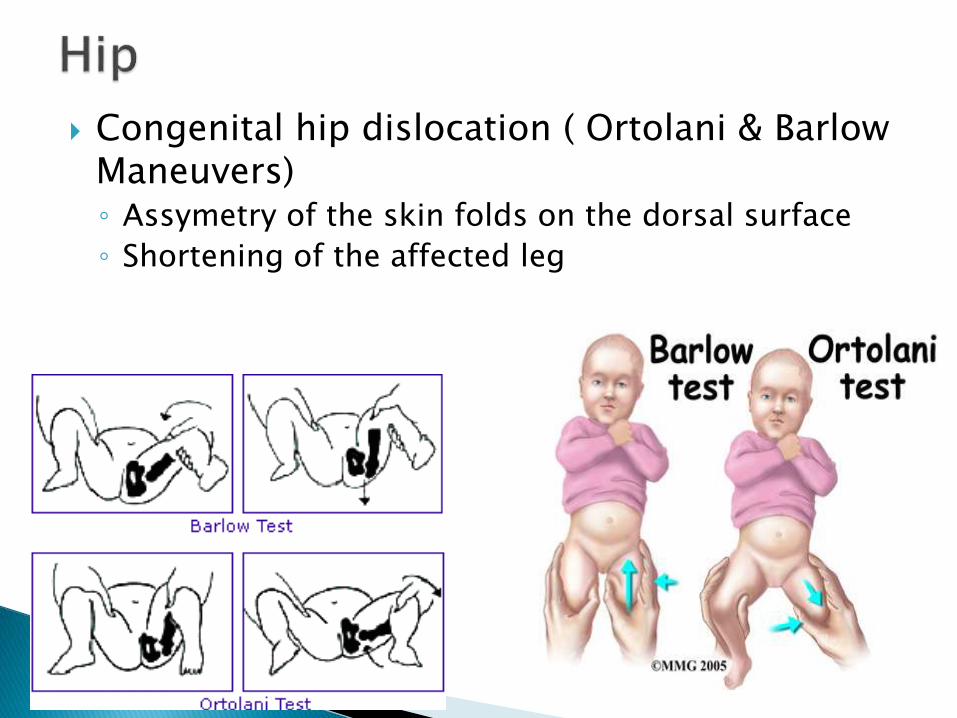
Congenital hip dislocation ( Ortolani & Barlow Maneuvers)◦ Assymetry of the skin folds on the dorsal surface
◦ Shortening of the affected leg

Moro reflex
Palmer grasp
Suckling and rooting reflexes
Tonic neck response



Final impression should be recorded as
Gestational age classification
Gestational age in weeks
Diagnosis
E.g: small for gestational age, 34 weeks, chromosomal anomaly.
INTRODUCTION
the process of birth brings the fetus from a fluid environment to an air environment.
This transition is accompanied by physiological and biochemical changes.
Most infants adapt to changes successfully and do not require any intervention,4-6% of them require resuscitation

Preterm
27%
Sepsis &
pneumonia
26%
Asphyxia
23%
Congenital
7%
Tetanus
7%
Diarrhoea
3%
Others
7%

Fetal lungs are filled with lung fluid that is derived from amniotic fluid that the fetus inhales regularly.
This fluid is expelled from the lung as the fetus is squeezed through the birth canal, the rest is expelled by initial breaths.

CONDITION AFFECTING MOTHER
OBSTETRIC COMPLICATION
FETAL FACTORS
MALFORMATIONS OF RESPIRATORY TRACT AND LUNG
INFANTS DELEVERED FOLLOWING INSTRUMENTATION

Most infants have apgar score between 7/10 to 10/10 at one minute and do not require resuscitation .
Infants with apgar score 4-6 require some intervention while those with <3/10 are severly compromised and warrant urgent resuscitation.
The primary goal is to provide adequate oxygen to the vital organs particularly the brain, preventing hypoxia and its consequence.
The general principles of resuscitation
A : Air way
B :Breathing
C :circulation
D :Drugs

INVERTED PYRAMID OF NEONATAL RESUSCUTATION


Place an appropriate size face mask
Hold the face mask between the index finger and thumb of the left hand, with the middle finger supporting the jaw.
Extend the neck of the baby slightly and lift the jaw forwards.
Manually compress the bag at a rate of 40-60/min ,using air or air-oxygen mixture at a flow rate of
5-10/min
Ensure good chest expansions in order to provide adequate ventilation

If bag mask ventilation last for >2min aspirate air from stomach at the end of procedure to prevent gaseous abdominal distention.
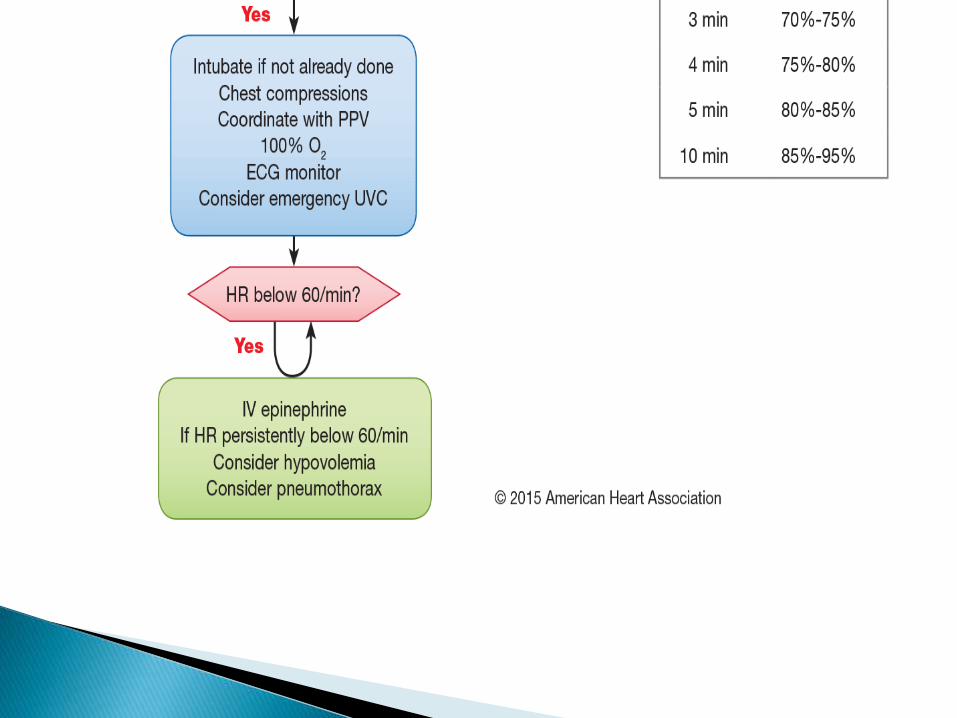
If the baby does not improve with bag mask ventilation in 30seconds, proceed to endotracheal intubation.
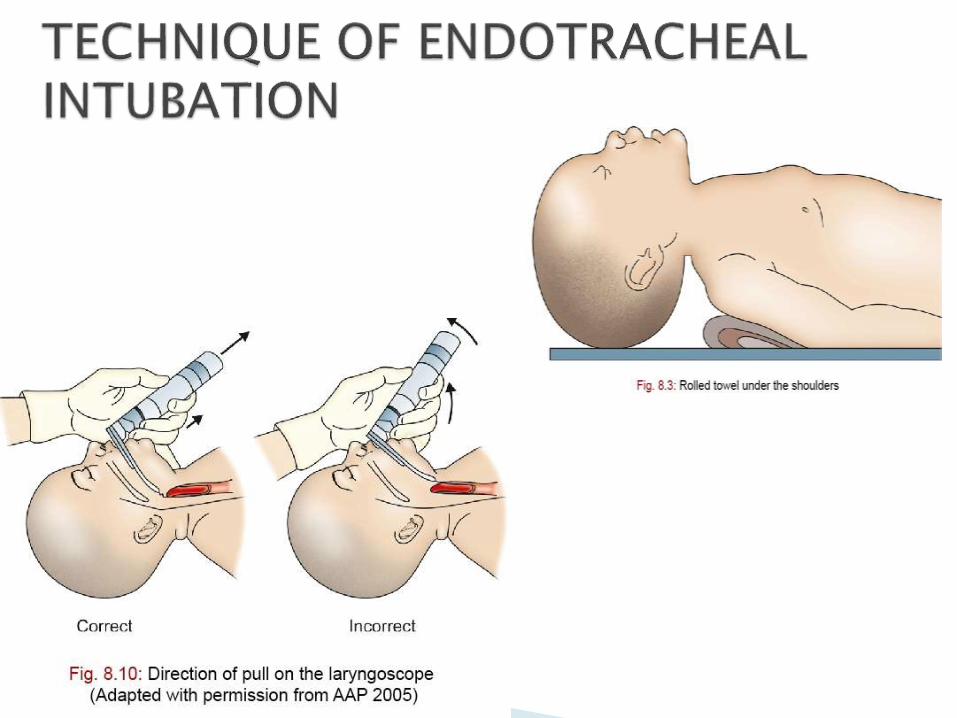
Put the baby flat or with the head slightly tilted downwards and suck out the fluid from oropharynx
Extend the neck of the baby slightly
Introduce an appropriate size laryngoscope with straight blade
Advance the blade to the vallecula and lift the tongue forward, exposing the epiglottis and laryngeal opening.
Introduce an appropriate size ETT into the trachea, past the vocal chords, to the depth of 2-2.5cm to avoid selective intubation of the right main bronchus.
Hold the ETT at that position or tape it to the angle of the mouth.
Connect the ETT to the resuscitation bag and apply positive pressure ventilation at the rate of 30/min and Fio2, pressure of 20-25 cm of water.
Auscultate the chest and stomach to confirm the position of the tip pf the ETT.
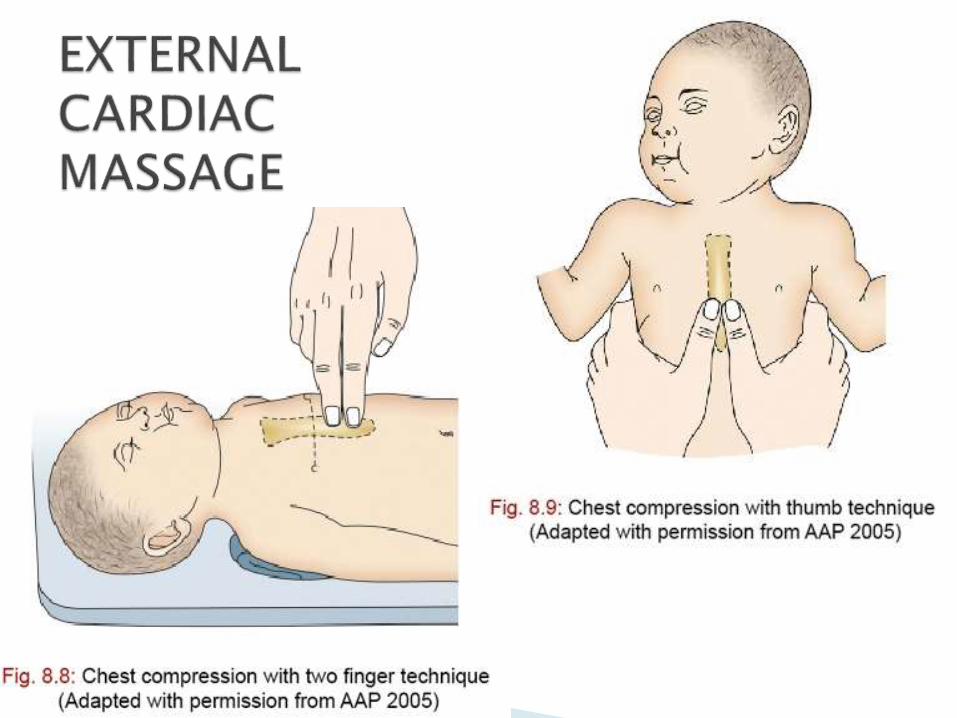

Stand by the side or feet of the baby Encircle the infant’s chest with both hands such that the
fingers support the back of the chest and the two thumbs placed over the lower third of the sternum.
Compress the chest to the depth of onethird the anteroposterior diameter of the chest . This can also be carried out with 2 finger compressing the lower sternum.
The ratio of ECM to lung inflation is 3:1 , 90chest compression and 30 breaths in 1min.
Give adrenalin if the heart rate remains less than 60/min despite 30 seconds of intermittent positive pressure ventilation and ECM
When the asphyxiated infant do not respond to resuscitation , check for technical errors
Oxygen source, tubing and connecting points.
Bag may not deliver enough pressure to inflate the lungs adequately.
Endotracheal tube(ETT) has been dislodged or esophageal intubation has occurred, reintubate the baby.
Endotracheal tube may be blocked(by blood clot or mucus) in which case the airway resistance is high. Either lavage the tube or change the ETT
Endotracheal tube is in the right main bronchus. Air entry will be diminished on the left, withdraw the ETT slightly until the air entry is equal.

Doing the simple things better is probably the most cost-effective policy.
Resuscitation can come as complete surprise So be prepared for resuscitation.
It may take several hours to learn but it should be implemented over seconds.
Practice makes one perfect.


















