48
Excellence in primary care - recognising our strengths and weaknesses Patrick Holmes GP Darlington CCG lead for Diabetes & Obesity

Excellence in primary care - recognising our strengths and
weaknesses
Patrick Holmes GP
Darlington CCG lead for Diabetes & Obesity
Overview
• Standards of Care – Patient perspective
– NICE / clinical standards
– Government
• How are we doing? – Patients
– NICE/QOF
– Budgets
• Can we do better? How?

Practice Nurse for regular check-ups
GP for regular BP and medication checks
Foot calluses noted by practice nurse
Referred by GP for new patient
education classes
Education course at Health Centre delivered by community
education team
Referred by GP for retinopathy screen
Retinopathy screening at Community Hospital
Referred by practice nurse for podiatry
Bob has obesity issues
Referred by GP to dietitian
Dietitian appointments at
the Walk-in Centre
Bob confesses he has erectile dysfunction
Diabetic Specialist Nurse at the erectile dysfunction clinic at
Hospital
Podiatrist at surgery finds foot
neuropathy
Podiatrist refers to Diabetic foot clinic
Diabetic Foot Clinic seen by Diabetic Specialist Nurse, Podiatrist, and Consultant
at Hospital
Nurse Specialist at GP Surgery has recommended
exenatide
Referred by GP to Hospital
Consultant Diabetologist initiates exenatide
GP eventually thinks Bob
requires insulin
Referred by GP to
LES insulin initiation service
Nurse Specialist at the Surgery decides exenatide is a better option so refers
patient back to GP for referral to specialist team
On direct questioning, Bob has a painful
peripheral neuropathy
Podiatrist refers back to GP
Podiatry Clinic at Community Clinic
Foot neuropathy discovered
Paramedics are called because of an episode of
hypoglycaemia
Taken to A&E and admitted to
hospital BOB
AGE 60
Bob is referred for a hip replacement
Bob has an episode of hypoglycaemia as
an inpatient
Referred by GP to Erectile Dysfunction
Clinic

What do patients want from Primary Care?

What do patients want from Primary Care?
• Free Access
• Competent
• Up to date
• Continuity of care
• Good communicators
• Interested + sympathetic
• Time for care
Adapted from Coulter A. What do patients and the public want from primary care. BMJ 2005;331:1199-1200 Cheragbi-Sobi S et al. What patients want from primary care consultations. Ann Fam Med 2008;6:107-115

NSF Diabetes (2001)
1. Prevention of Type 2 diabetes
2. Identification of people with diabetes
3. Empowering people with diabetes
4. Clinical care of adults with diabetes
5. Clinical care of children and young people with diabetes
6. Management of diabetic emergencies
7. Care of people with diabetes during admission to hospital
8. Diabetes and Pregnancy
9. Detection and management of long-term complications

NICE CG 10, 15, 66, 87 & 119

NICE QS 6

NICE QS 6
1: Structured education
2: Nutrition and physical activity advice
3: Care planning
4: Glycaemic control
5: Medication
6: Insulin therapy
7: Preconception care
8: Complications
9: Psychological problems
10: 'At risk' foot
11: Foot problems requiring urgent medical attention
12: Inpatient care
13: Diabetic ketoacidosis
14: Hypoglycaemia

Government

An end to growth in NHS Budgets
NHS spend UK per year in millions £s
£0
£20,000
£40,000
£60,000
£80,000
£100,000
£120,000
£140,000
£160,000
£180,000
1999/00 2004/05 2009/10e 2014/15e

“Gross” Domestic Product



HOW ARE WE DOING? STRENGTHS & WEAKNESSES

GP Survey 2011/2
Q22. Did you have confidence and trust in the GP you saw or spoke to?
Jul 11 - Mar 12
(1,003,926)
%
Yes, definitely 66
Yes, to some extent 27
No, not at all 4
Don’t know / can’t say 3
Yes (total) 93
Q24. Did you have confidence and trust in the nurse you saw or spoke to?
Jul 11 - Mar 12
(961,185)
%
Yes, definitely 64
Yes, to some extent 22
No, not at all 2
Don’t know / can’t say 11
Yes (total) 86

GP Survey 2011/2
Q32. In the last 6 months, have you had enough support from local services or organisations to help you manage your long term health condition(s)?
Please think about all services and organisations, not just health services
Jul 11 -Mar 12 (471,946) % Yes, definitely 40 Yes, to some extent 24 No 11 I have not needed such support 22 Don’t know / can’t say 3 Yes (total) 64
Q33. How confident are you that you can manage your own health?
Jul 11 - Mar 12
(993,487)
%
Very confident 44
Fairly confident 49
Not very confident 6
Not at all confident 1
Confident (total) 93




National Diabetes Audit 2010/11
Care processes recorded All patients with diabetes T1DM under 55 years
All Care Processes 54.3% 33.1%
Urinary Albumin 75.0% 51.6%
Eye Screening 81.9% 74.8%
Foot Exam 84.4% 66.6%
Smoking Review 84.8% 76.9%
BMI 89.9% 80.9%
Cholesterol 91.6% 73.3%
Blood Creatinine 92.4% 76.2%
HbA1c 92.4% 82.7%
Blood Pressure 95.1% 85.6%

Treatment target Achievement
Target All patients with diabetes T1DM under 55 years
HbA1c < 6.5% (48mmol/mol) 24.8% 6.2%
HbA1c ≤7.5% (58mmol/mol) 63.3% 25.0%
HbA1c≤10.0% (86mmol/mol) 92.1% 79.2%
Cholesterol < 4mmol/l 40.7% 25.2%
Cholesterol < 5mmol/l 77.6% 67.6%
Target BP* 36.4% 56.1%
BP < 140/80 44.8% 58.5%
All** 19.8% 11.4%
*BP target <140/80 without kidney, eye or vascular disease (<130/80 with) **Where patient achieved HbA1c ≤ 7.5%, cholesterol <5mmol/l and BP target

Making better use of resources #2
The majority of people with diabetes fail to
take their tablets as prescribed
Donnan, Diabet Med (2002)

MONEY....

Direct Costs (NHS England)
Diabetes currently accounts for between £3.9b¹ to £10b² (4-10% of NHS expenditure)
• Prescribing - £649m¹ to £857m2
• Primary Care (inc. Ret screening) - £1b¹ to £1.2b²
• Hospital Care - £2.3b¹
• “Complications” - £7.7b²
• PCT Programme Budgets - £1.3b³
1. The management of adult diabetes services in NHS – National Audit Office / DoH – (May 2012) 2. Hex N et al. Diabet. Med. 29, 855-862 (2012) 3. Costing Care Pathways – National Audit Commission (2011)

Distribution of the cost of complications (£7.7 billion)
IHD & AMI
Heart Failure
Stoke
other CVD
Excess Inpatient Days
Renal
Foot Ulcers/Amputation
Neuropathy
other
Hex N et al. Diabet. Med. 29, 855-862 (2012)

Making better use of resources
There are only 3 ways to release money:
– People
– Real estate
– Prescribing
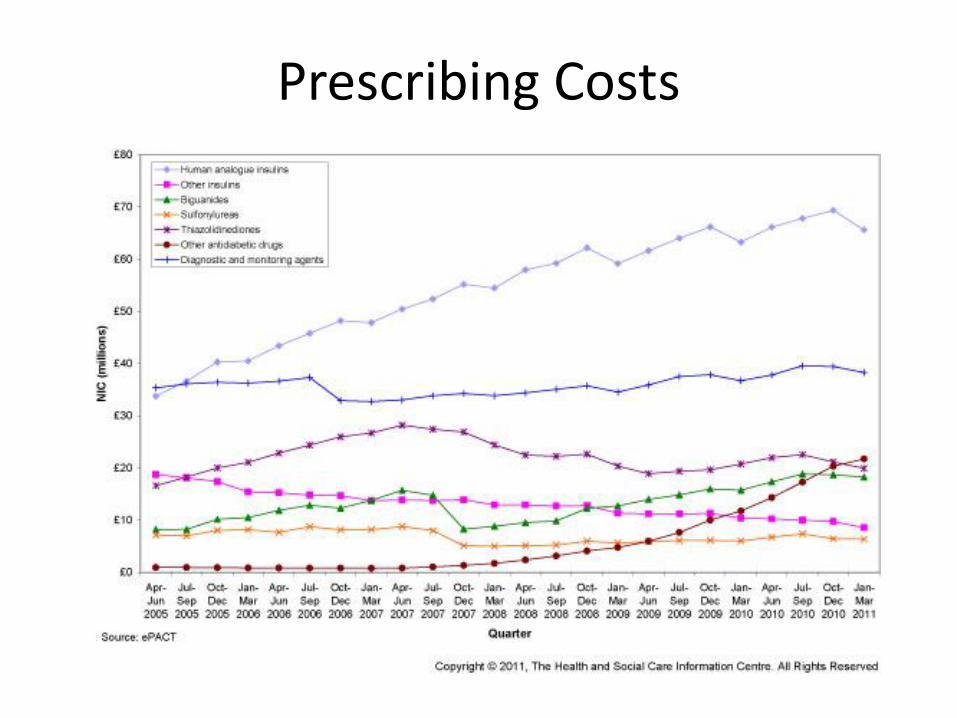
Prescribing Costs

£25
£111
£33
£34
£141
£434
£320
£830
£954
£955
£528
£702
£753
£496
£528
£1,010
£1,022
$0 $200 $400 $600 $800 $1,000 $1,200
Metformin 1g BD
Glucophage SR 1g BD
Glimiprimide 6mg OD
Gliclazide 160mg BD
Diamicon MR 120mg OD
Sitagliptin 100mg OD
Pioglitazone 45mg OD
Exenatide 10mcg BD
Exanetide 2mg QW
Liraglutide 1.2mg OD
Humulin M3 50u BD
Novomix 30 50u BD
Humalog Mix 25
Insulatard 50u BD
Humulin I 50u BD
Glargine 50u BD
Levemir 50u BD
Diabetes Treatments: Annual costs
Costs: BNF, June 2012
NB: Cost of treatment only: Some incur additional costs of counselling, administration and monitoring

£0
£2
£4
£6
£8
£10
£12
£14
NIC
(£
)/d
iab
eti
c p
ati
en
t
PCT
Spend on GLP-1 Analogues per person with diabetes October 2010 - September 2011
17 fold variation
Data: Information Centre Prescribing Support and Primary Care Services Oct 2010– Sept 2011

Spend per patient with diabetes on DPP-4
Oct ‘10 – Sept ‘11
0
2
4
6
8
10
12
NIC
(£)/
Dia
beti
c P
ati
en
t
PCT
22 fold variation
Data: Information Centre Prescribing Support and Primary Care Services Oct 2010– Sept 2011

R² = 0.0027
40
45
50
55
60
65
70
220 240 260 280 300 320 340 360 380
Targ
et
Perc
en
tag
e
NIC (£)/Diabetic Patient
All England PCTs: Weighted Prescribing Costs of Drugs Used in Diabetes October 2010 - September 2011 'v' Percentage of diabetic patients whose HbA1C has been 7 or less in the last 15 months April
2010 - March 2011
Data: Information Centre Prescribing Support and Primary Care Services Oct 2010– Sept 2011

Using drugs
cleverly
Using clever
drugs
• Huge cost of prescribing behaviours
• Unwarranted variation
– Does not reflect evidence
– Does not produce better outcomes
• Major source of waste
• Opportunity for better use of resources
Thinking Big
• Care Planning
• Integrating Care

“The greatest single advance in
medicine will not be some new
drug or procedure but an
increased ability of patients to
care for themselves”
Ivan Illich

Unleashing the largest under-utilised resource in healthcare
• 1% (5% of newly diagnosed) of patients with diabetes offered structured medical education in 2009-10¹
• Only one in three with Type 2 diabetes had adequate adherence to OHDs²
http://www.diabetes.org.uk/Professionals/Service-improvement/Year-of-Care/ 1. National Diabetes Audit 2010-11. 2. Donnan,PT. Diabet Med 2002;19(4):274-84
Care Planning

New models of care.....

Practice Nurse for regular check-ups
GP for regular BP and medication checks
Foot calluses noted by practice nurse
Referred by GP for new patient
education classes
Education course at Health Centre delivered by community
education team
Referred by GP for retinopathy screen
Retinopathy screening at Community Hospital
Referred by practice nurse for podiatry
Bob has obesity issues
Referred by GP to dietitian
Dietitian appointments at
the Walk-in Centre
Bob confesses he has erectile dysfunction
Diabetic Specialist Nurse at the erectile dysfunction clinic at
Hospital
Podiatrist at surgery finds foot
neuropathy
Podiatrist refers to Diabetic foot clinic
Diabetic Foot Clinic seen by Diabetic Specialist Nurse, Podiatrist, and Consultant
at Hospital
Nurse Specialist at GP Surgery has recommended
exenatide
Referred by GP to Hospital
Consultant Diabetologist initiates exenatide
GP eventually thinks Bob
requires insulin
Referred by GP to
LES insulin initiation service
Nurse Specialist at the Surgery decides exenatide is a better option so refers
patient back to GP for referral to specialist team
On direct questioning, Bob has a painful
peripheral neuropathy
Podiatrist refers back to GP
Podiatry Clinic at Community Clinic
Foot neuropathy discovered
Paramedics are called because of an episode of
hypoglycaemia
Taken to A&E and admitted to
hospital BOB
AGE 60
Bob is referred for a hip replacement
Bob has an episode of hypoglycaemia as
an inpatient
Referred by GP to Erectile Dysfunction
Clinic


Current Diabetes Care: Current organisation
GPs
Practice nurses
HCAs
1° care 2° care Intermediate care
Hospital doctors
Hospital DSNs
Hospital dietitians
Hospital podiatrists
GP surgeries Hospital diabetes
service
Community
provider arm
DSN = diabetes specialist nurse
Community DSNs
Community Dieticians
Community Podiatrists

Integrated Diabetes Care
HCAs
1° care 2° care Intermediate care
Specialist podiatrists
Diabetes service
Specialist dietitians
Specialist doctors Specialist DSNs
Practice nurses
GPs
“Ownership of the problem, ownership of the solution”

Integrated diabetes care: Derby
• Single delivery organisation: ‒ Joint venture between local clinicians
‒ Company limited by shares
‒ 50% owned by GPs, 50% owned by local hospital
‒ Holds contract with commissioners (PCT)
• Delivers clinical care along whole patient pathway ‒ Redesign of services in a collaboration between 1 & 2 care
‒ Joint venture working enabled clinical decision making to take priority
‒ Collaborative working enabled commissioning of a comprehensive service
Rea RD, Gregory S, Browne M...Tan GD. Integrated Diabetes Care in Derby. Practical Diabetes 2012;28:312-313.

Integrated diabetes care: levels of integration in Derby
• Governance integration: ‒ eg maintain standards across an organisation with ongoing
training and accreditation based on competencies.
‒ eg transfer of clinical risk from individuals to an organisation.
• Clinical integration:
– maximise efficiency throughout the system (eg IT, care planning).
• Financial integration:
– align financial incentives across the whole patient pathway,
rather than traditional organisational boundaries.
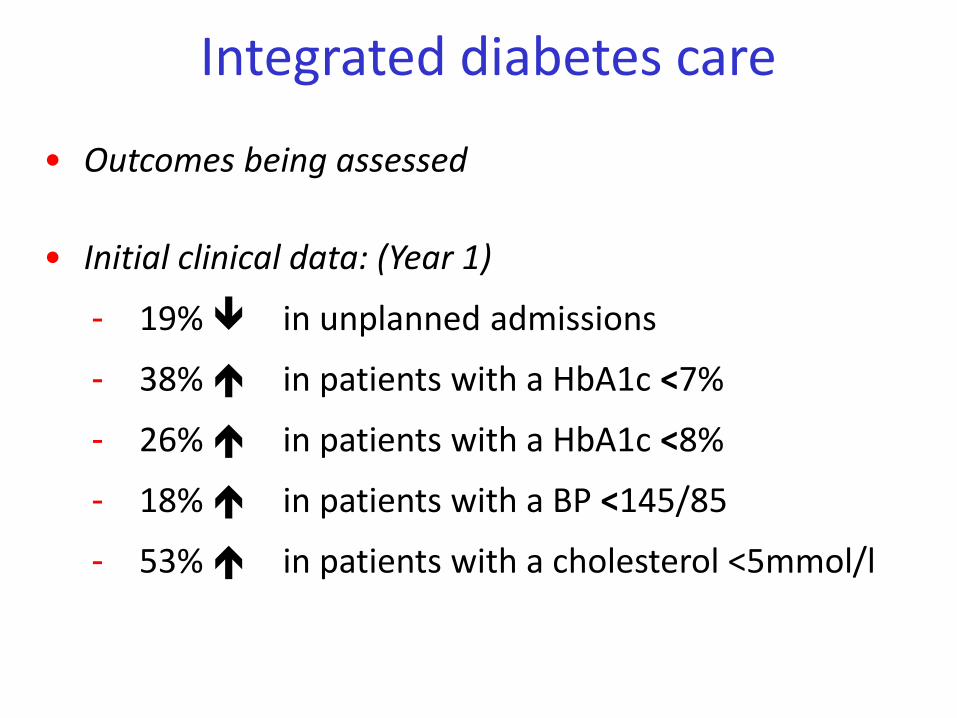
• Outcomes being assessed
• Initial clinical data: (Year 1)
- 19% in unplanned admissions
- 38% in patients with a HbA1c <7%
- 26% in patients with a HbA1c <8%
- 18% in patients with a BP <145/85
- 53% in patients with a cholesterol <5mmol/l
Integrated diabetes care

Integrated diabetes care: Portsmouth ‘Super Six’ Model
• Defined patients who should be managed in a hospital setting – Inpatient diabetes
– Antenatal diabetes
– Diabetic foot care
– Diabetic nephropathy (dialysis & progressive renal disease)
– Insulin Pumps
– Type 1 diabetes (poor control & adolescents)
• Community diabetic team (CDT) – Commissioned to care for all other patients
– Enhanced number of DSN + one GPwSI session per week.
– Consultant diabetologist team working partly for CDT & FT
– Regular contact with practices (visits, email and phone support)
Kar P . The Super Six Model. Diabetes & Primary Care 2012;14:277-283.
Portsmouth ‘Super Six’ Model Outcomes after a year
• 41/52 surgeries covered
• 712 patients discharged
• 6 patients needed to be re-referred back in after complaints
• New referrals from 14 to 2 per month
• Won a “Care Integration Award 2012” from the NHS commissioning board
Summary
• How are we doing? – Patients
• Highly value Medical, Nursing and NHS care in general
• Competence, ‘humaneness’ & continuity of care vaulued
– NICE/QOF • Curate’s egg
• Some patients needs not catered for?
– Budgets • Large, but challenged
• UK Diabetes epidemic
• Can we do better? How? – Service redesign with greater integration
– Working with all providers – dealing with vested interests
– Models out there working

Inspire (or protect) a generation

















