Exhaled nitric oxide as a marker of asthma control in smoking patients _______________________________________ Alain Michils 1 , MD; Renaud Louis 2 , MD; Rudi Peché 3 , MD; Sandra Baldassarre 1 , MD; Alain Van Muylem 1 , PhD 1 Chest Department - CUB Erasme, Brussels, Belgium 2 Chest Department - CHU Sart-Tilmant, Liège, Belgium 3 Chest Department- CHU André Vésale, Montigny- le-Tilleul, Belgium Address for correspondence and reprint requests : Alain Van Muylem, PhD Chest Department CUB Erasme 808 Route de Lennik 1070 Brussels - Belgium Phone: 32-2-555.39.85 Fax: 32-2-555.44.11 Email: [email protected]Running head : Exhaled nitric oxide in smoking asthmatics Key words : Exhaled nitric oxide, asthma control, tobacco smoking Funding : AstraZeneca provided a grant for the exhaled biomarker laboratory Word count : 2583 . Published on January 22, 2009 as doi: 10.1183/09031936.00154008 ERJ Express Copyright 2009 by the European Respiratory Society.
Transcript
Exhaled nitric oxide as a marker of asthma control in
Data are presented as: #: geometrical mean [geometrical interval] § : mean±SD; * median [range]; $ : ICS dose in µg equ BDP.day-1; & : comparison between non-smoking and smoking group. N is the number of patients in each group. Except for FeNO, non-smoking and smoking groups are statistically similar.
15
Table 2: Cross-sectional assessment of asthma control.
N n+ P
(%)
Cut-off
(ppb)
Se
(%)
Sp
(%)
PPV
(%)
NPV
(%)
Acc
(%)
p
Non-smokers 411 197 48 50 72 56 61 68 64 <0.001
Smokers 59 15 25 25 66 48 30 81 53 0.39
Data are presented as: N, n+ and P are the total number of events, the number of positive cases, and the prevalence, respectively. Se, Sp, PPV, NPV and p are sensitivity, specificity, positive and negative predictive values, and the statistical significance of rejecting AUC=0.5, respectively. A positive event is controlled asthma (ACQ score < 1.5). A true positive case is defined as FeNO≤cut-off value associated with a controlled asthma. FeNO does not discriminate cross-sectionally controlled versus uncontrolled asthma in smoking patients (p=0.39).
16
Table 3: Assessment of a change from uncontrolled (ACQ score ≥ 1.5) to controlled (ACQ score < 1.5) asthma
.
N n+ P
(%)
Cut-off
(%)
Se
(%)
Sp
(%)
PPV
(%)
NPV
(%)
Acc
(%)
p
Non-smokers 283 133 47 -30 68 71 68 72 70 <0.001
Smokers 52 17 33 -20 71 66 50 82 67 0.016
Data are presented as: N, n+ and P are the total amount of events, the amount of positive cases, and the prevalence, respectively. Se, Sp, PPV, NPV, Acc and p are sensitivity, specificity, positive and negative predictive values, accuracy and the statistical significance of rejecting AUC=0.5, respectively. A positive event is a change from uncontrolled (ACQ score ≥ 1.5) to controlled (ACQ score < 1.5) asthma. A true positive case is defined as FeNO change≤cut-off value (e.g. -40% ) associated with a positive event. FeNO exhibits similar operating characteristics in both non-smoking and smoking group. Particularly, a high NPV is observed.
17
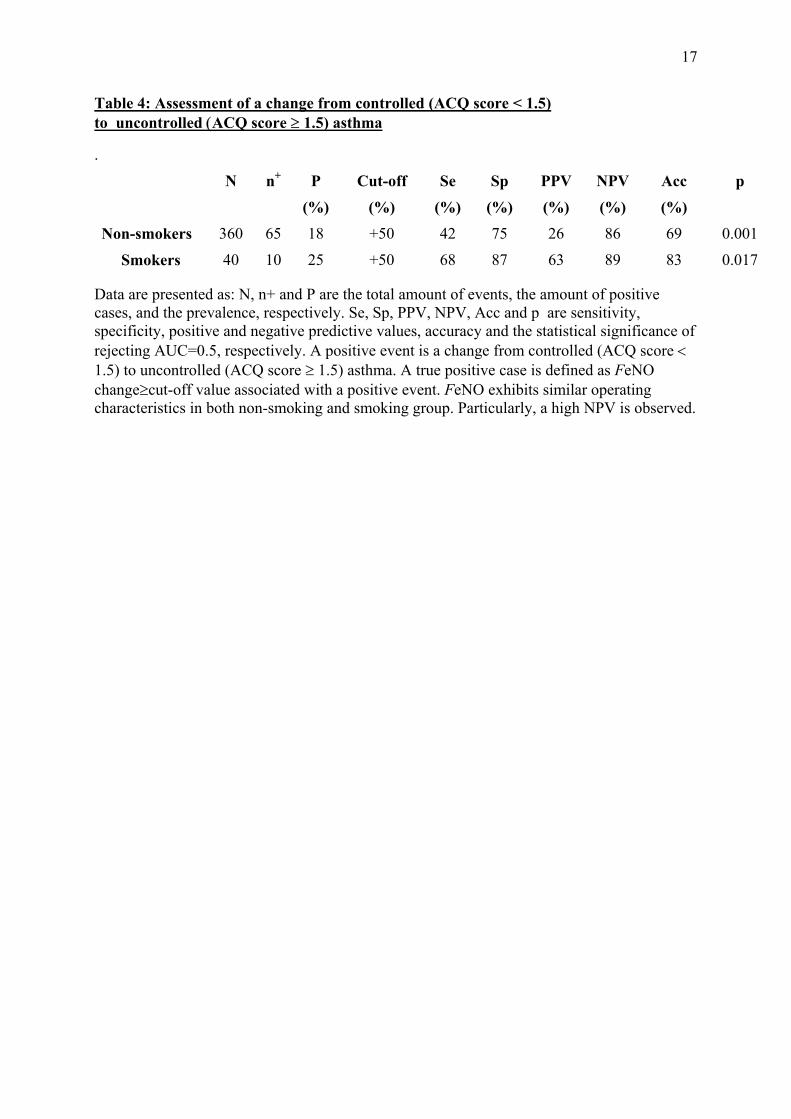
Table 4: Assessment of a change from controlled (ACQ score < 1.5) to uncontrolled (ACQ score ≥ 1.5) asthma
.
N n+ P
(%)
Cut-off
(%)
Se
(%)
Sp
(%)
PPV
(%)
NPV
(%)
Acc
(%)
p
Non-smokers 360 65 18 +50 42 75 26 86 69 0.001
Smokers 40 10 25 +50 68 87 63 89 83 0.017
Data are presented as: N, n+ and P are the total amount of events, the amount of positive cases, and the prevalence, respectively. Se, Sp, PPV, NPV, Acc and p are sensitivity, specificity, positive and negative predictive values, accuracy and the statistical significance of rejecting AUC=0.5, respectively. A positive event is a change from controlled (ACQ score < 1.5) to uncontrolled (ACQ score ≥ 1.5) asthma. A true positive case is defined as FeNO change≥cut-off value associated with a positive event. FeNO exhibits similar operating characteristics in both non-smoking and smoking group. Particularly, a high NPV is observed.
18
Table 5: Assessment of asthma control improvement (∆ACQ < -0.5)
Data are presented as: § : ICS dose (D) in µg equ BDP.day-1; & : cut-off value. ACQ<2 row tests the subgroup with an initial ACQ score < 2 and ∆D=0 row tests the sub-group without treatment modification between consecutive visits. N, n+ and P are the total amount of events, the amount of positive events, and the prevalence, respectively. Se, Sp, PPV, NPV, Acc and p are sensitivity, specificity, positive and negative predictive values, accuracy and the statistical significance of rejecting AUC=0.5, respectively. A positive event is defined as an improvement in asthma control. A true positive case is defined as a FeNO change ≤ cut-off value (e.g. -25%) associated with an improvement of asthma control between consecutive visits. When smoking patients are treated with high ICS dose, FeNO loses its ability to assess a control improvement (p=0.07).
19
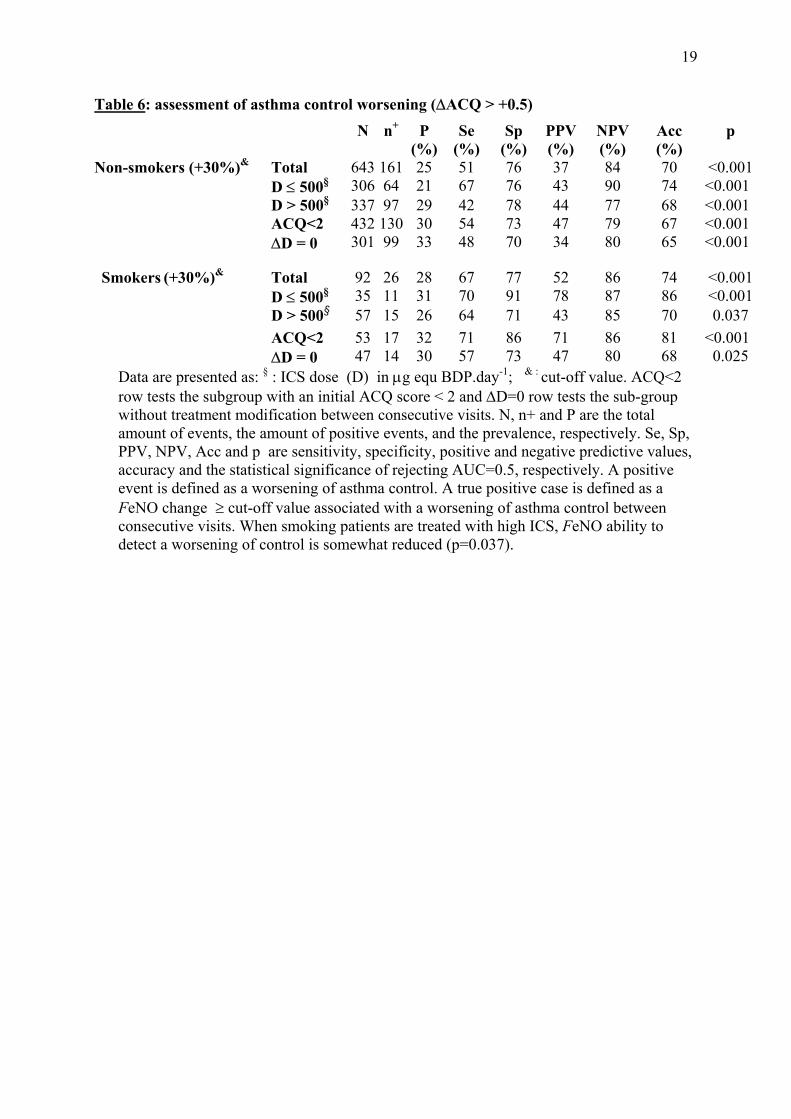
Table 6: assessment of asthma control worsening (∆ACQ > +0.5)
Data are presented as: § : ICS dose (D) in µg equ BDP.day-1; & : cut-off value. ACQ<2 row tests the subgroup with an initial ACQ score < 2 and ∆D=0 row tests the sub-group without treatment modification between consecutive visits. N, n+ and P are the total amount of events, the amount of positive events, and the prevalence, respectively. Se, Sp, PPV, NPV, Acc and p are sensitivity, specificity, positive and negative predictive values, accuracy and the statistical significance of rejecting AUC=0.5, respectively. A positive event is defined as a worsening of asthma control. A true positive case is defined as a FeNO change ≥ cut-off value associated with a worsening of asthma control between consecutive visits. When smoking patients are treated with high ICS, FeNO ability to detect a worsening of control is somewhat reduced (p=0.037).
20
References 1. Jones SL, Kittelson J, Cowan JO, Flannery EM, Hancox RJ, McLachlan CR, Taylor
DR. The predictive value of exhaled nitric oxide measurements in assessing changes in asthma control. Am J Respir Crit Care Med 2001; 164: 738-743.
2. Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Engl J Med 2005; 352: 2163-2173.
3. Shaw DE, Berry MA, Thomas M, Green RH, Brightling CE, Wardlaw AJ, Pavord ID. The use of exhaled nitric oxide to guide asthma management: a randomized controlled trial. Am J Respir Crit Care Med 2007; 176: 231-237.
4. Turner S. Exhaled nitric oxide in the diagnosis and management of asthma. Curr Opin Allergy Clin Immunol 2008; 8: 70-76.
5. Szefler SJ, Mitchell H, Sorkness CA, Gergen PJ, O'Connor GT, Morgan WJ, Kattan M, Pongracic JA, Teach SJ, Bloomberg GR, Eggleston PA, Gruchalla RS, Kercsmar CM, Liu AH, Wildfire JJ, Curry MD, Busse WW. Management of asthma based on exhaled nitric oxide in addition to guideline-based treatment for inner-city adolescents and young adults: a randomised controlled trial. Lancet 2008; 372: 1065-1072.
6. Olin AC, Rosengren A, Thelle DS, Lissner L, Bake B, Toren K. Height, age, and atopy are associated with fraction of exhaled nitric oxide in a large adult general population sample. Chest 2006; 130: 1319-1325.
7. Taylor DR, Pijnenburg MW, Smith AD, De Jongste JC. Exhaled nitric oxide measurements: clinical application and interpretation. Thorax 2006; 61: 817-827.
8. Persson MG, Zetterstrom O, Agrenius V, Ihre E, Gustafsson LE. Single-breath nitric oxide measurements in asthmatic patients and smokers. Lancet 1994; 343: 146-147.
9. Kharitonov SA, Robbins RA, Yates D, Keatings V, Barnes PJ. Acute and chronic effects of cigarette smoking on exhaled nitric oxide. Am J Respir Crit Care Med 1995; 152: 609-612.
10. Verleden GM, Dupont LJ, Verpeut AC, Demedts MG. The effect of cigarette smoking on exhaled nitric oxide in mild steroid-naive asthmatics. Chest 1999; 116: 59-64.
11. Hogman M, Holmkvist T, Walinder R, Merilainen P, Ludviksdottir D, Hakansson L, Hedenstrom H. Increased nitric oxide elimination from the airways after smoking cessation. Clin Sci (Lond) 2002; 103: 15-19.
12. Horvath I, Donnelly LE, Kiss A, Balint B, Kharitonov SA, Barnes PJ. Exhaled nitric oxide and hydrogen peroxide concentrations in asthmatic smokers. Respiration 2004; 71: 463-468.
13. McSharry CP, McKay IC, Chaudhuri R, Livingston E, Fraser I, Thomson NC. Short and long-term effects of cigarette smoking independently influence exhaled nitric oxide concentration in asthma. J Allergy Clin Immunol 2005; 116: 88-93.
21
14. Travers J, Marsh S, Aldington S, Williams M, Shirtcliffe P, Pritchard A, Weatherall M, Beasley R. Reference ranges for exhaled nitric oxide derived from a random community survey of adults. Am J Respir Crit Care Med 2007; 176: 238-242.
15. Dressel H, de la MD, Reichert J, Ochmann U, Petru R, Angerer P, Holz O, Nowak D, Jorres RA. Exhaled nitric oxide: independent effects of atopy, smoking, respiratory tract infection, gender and height. Respir Med 2008; 102: 962-969.
16. Gaston B, Drazen JM, Loscalzo J, Stamler JS. The biology of nitrogen oxides in the airways. Am J Respir Crit Care Med 1994; 149: 538-551.
17. Thomson NC, Chaudhuri R, Livingston E. Asthma and cigarette smoking. Eur Respir J 2004; 24: 822-833.
18. Michils A, Baldassarre S, Van Muylem A. Exhaled nitric oxide and asthma control: a longitudinal study in unselected patients. Eur Respir J 2008; 31: 539-546.
19. Juniper EF, O'Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J 1999; 14: 902-907.
20. Global initiative for Asthma. Global strategy for asthma management and prevention: NHLBI/WHO Workshop Report. Washington, DC, Government Printing Office, 2002. NHLBI Publication 02-3659.
21. Siroux V, Pin I, Oryszczyn MP, Le MN, Kauffmann F. Relationships of active smoking to asthma and asthma severity in the EGEA study. Epidemiological study on the Genetics and Environment of Asthma. Eur Respir J 2000; 15: 470-477.
22. Juniper EF, Bousquet J, Abetz L, Bateman ED. Identifying 'well-controlled' and 'not well-controlled' asthma using the Asthma Control Questionnaire. Respir Med 2006; 100: 616-621.
23. Juniper EF, Svensson K, Mork AC, Stahl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med 2005; 99: 553-558.
24. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med 2005; 171: 912-930.
25. Youden WJ. Index for rating diagnostic tests. Cancer 1950; 3: 32-35.
26. Jatakanon A, Lim S, Kharitonov SA, Chung KF, Barnes PJ. Correlation between exhaled nitric oxide, sputum eosinophils, and methacholine responsiveness in patients with mild asthma. Thorax 1998; 53: 91-95.
27. Chalmers GW, Macleod KJ, Little SA, Thomson LJ, McSharry CP, Thomson NC. Influence of cigarette smoking on inhaled corticosteroid treatment in mild asthma. Thorax 2002; 57: 226-230.
28. Lazarus SC, Chinchilli VM, Rollings NJ, Boushey HA, Cherniack R, Craig TJ, Deykin A, DiMango E, Fish JE, Ford JG, Israel E, Kiley J, Kraft M, Lemanske RF, Jr., Leone
22
FT, Martin RJ, Pesola GR, Peters SP, Sorkness CA, Szefler SJ, Wechsler ME, Fahy JV. Smoking affects response to inhaled corticosteroids or leukotriene receptor antagonists in asthma. Am J Respir Crit Care Med 2007; 175: 783-790.
29. Jatakanon A, Kharitonov S, Lim S, Barnes PJ. Effect of differing doses of inhaled budesonide on markers of airway inflammation in patients with mild asthma. Thorax 1999; 54: 108-114.
30. Jones SL, Herbison P, Cowan JO, Flannery EM, Hancox RJ, McLachlan CR, Taylor DR. Exhaled NO and assessment of anti-inflammatory effects of inhaled steroid: dose-response relationship. Eur Respir J 2002; 20: 601-608.
23
Legend to the figure
Figure 1: ROC curve characterizing the ability of FeNO to assess an improvement of asthma
control defined as a significant ACQ score decrease (∆ ACQ score > 0.5) between two
consecutive visits. The solid line and the dashed lines represent non-smoking and smoking
patients, respectively. FeNO exhibits similar operating characteristics in both populations.



















![oxide, and to improve asthma control in obese...recruited obese (body mass index [BMI] >30) asthmatics on controller therapy with a baseline fractional exhaled nitric oxide (FeNO)](https://static.documents.pub/doc/80x56/60329309f844087c8b43c44c/oxide-and-to-improve-asthma-control-in-obese-recruited-obese-body-mass-index.jpg)
















