EXPANDING INTEGRATED CARE ACROSS THE LIFESPAN: KNOWLEDGE AND SKILLS FOR PEDIATRIC AND GERIATRIC PRACTICE Colleen Fischer, Ph.D., Psychologist, Denver Health Medical Center Alison Lieberman, Psy.D., Psychologist, Denver Health Medical Center Matthew Tolliver, M.A., Doctoral Psychology Intern, Denver Health Medical Center Christopher Sheldon, Ph.D., Psychologist, Denver Health Medical Center Collaborative Family Healthcare Association 17 th Annual Conference October 15-17, 2015 Portland, Oregon U.S.A. Session #C2c October 16, 2015
Transcript
EXPANDING INTEGRATED CARE ACROSS THE LIFESPAN: KNOWLEDGE AND SKILLS FOR PEDIATRIC AND GERIATRIC PRACTICE
Colleen Fischer, Ph.D., Psychologist, Denver Health Medical Center
Alison Lieberman, Psy.D., Psychologist, Denver Health Medical Center
Matthew Tolliver, M.A., Doctoral Psychology Intern, Denver Health Medical Center
Christopher Sheldon, Ph.D., Psychologist, Denver Health Medical Center
Collaborative Family Healthcare Association 17th Annual ConferenceOctober 15-17, 2015 Portland, Oregon U.S.A.
Session #C2cOctober 16, 2015
Acknowledgments
Amy Starosta, M.A., Doctoral Psychology Intern, Denver Health Medical Center
Jill Hersh, M.A., Doctoral Psychology Intern, Denver Health Medical Center
This project is supported by funds from the Bureau of Health Workforce (BHW), Health Resources and Services Administration (HRSA), Department of Health and Human Services (DHHS) under Grant No. D40 HP 26858, $278,780. This information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by the BHW, HRSA, DHHS or the U.S. Government.
Faculty Disclosure
The presenters of this session:
Have NOT had any relevant financial relationships during the past 12 months.
Learning Objectives
At the conclusion of this session, the participant will be able to:
Describe the way in which behavioral health can be integrated into pediatric and geriatric primary care
Identify specific evidence-based assessment and intervention strategies useful with these populations
Discuss some of the challenges and opportunities for growth with these specialized populations
Learning Assessment
A learning assessment is required for CE credit.
A question and answer period will be conducted at the end of this presentation.
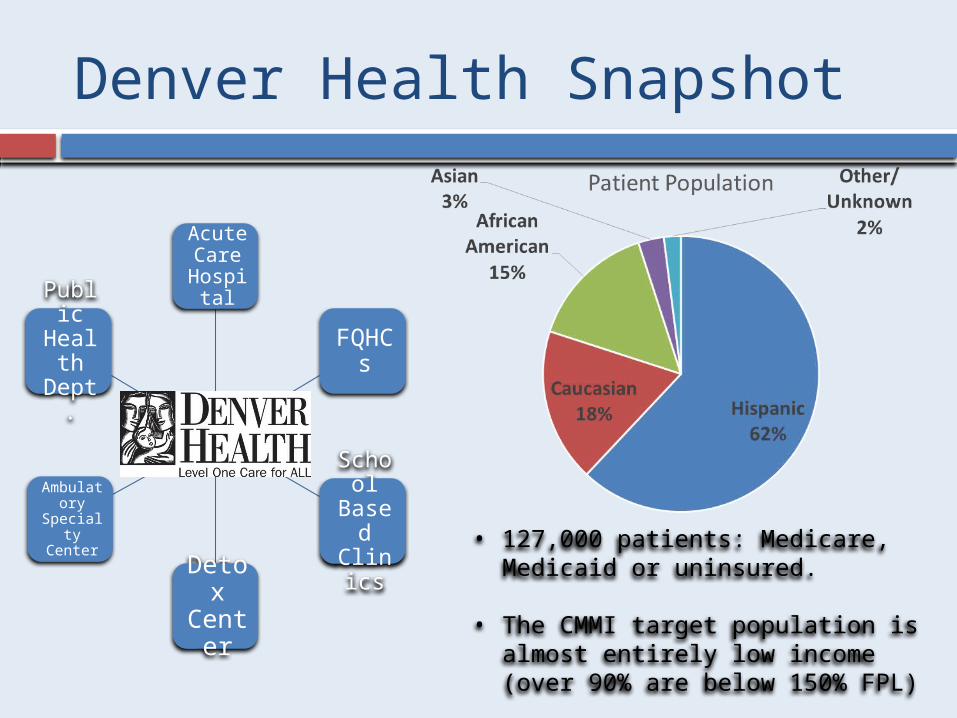
Denver Health Snapshot
Acute Care
Hospital
FQHCs
School
Based
Clinics
Detox
Center
Ambulatory
Specialty Center
Public Healt
h Dept.
• 127,000 patients: Medicare, Medicaid or uninsured.
• The CMMI target population is almost entirely low income (over 90% are below 150% FPL)
Rationale
Targeted Integrated Behavioral Care
Diverse and low SES populations: High levels of behavioral health need
Diverse and low SES populations: Low levels of behavioral health resources
Needs Assessment Gaps by Age: Elderly: special needs, few BHCs trained Pediatrics: unique presentations, few BHCs trained
Needs Assessment Gaps by Complexity: High-need, high cost adults include geriatric patients High-need, high cost children include developmental issues and
obesity
Mental Health in the Aging Population
Adults over 65 are predicted to represent 20% of the population by 2030 (Administration on Aging, 2009)
Higher co-morbidity of mental health issues with chronic illness, functional impairment
Complexity of the biopsychosocial assessment in the aging population
Risk assessment and changes in cognition (normal aging versus impairment)S
ub
. A
bu
se
An
xie
ty
Dem
en
tia
Dep
ressio
n
Geriatric Primary Care Clinic
Mental Health in Pediatric Primary Care
Integrated approaches reduce barriers to treatment of pediatric mental health concerns
Up to 70% of primary care appointments are for issues related to psychosocial concerns
Assessment and treatment of a wide range of pediatric emotional and behavioral concerns (birth to age 18)
Complexity of the biopsychosocial assessment in the pediatric population
Ob
esit
y/
Pre
dia
bete
s
Develo
pm
en
tal
Issu
es
AD
HD
/D
isru
pti
ve
Beh
avio
rs
Trau
ma/
An
xie
ty
/Dep
ressio
n
Pediatric Primary Care Clinic
What we do(Geriatrics and Pediatrics)
Taking all comers Collaboration takes multiple forms
(curbside, during medical visit, behavioral health visits)
Cultural and age sensitivity Biopsychosocial assessment Interventions Additional functions (referrals, etc)
Assessment
Diagnostic evaluation Screening measures Risk assessment Referrals for testing/long term
Intro to behavioral health/warm hand off Brief therapy Crisis management Curbside consultation Telephone care coordination Health behavior interventions/change
Case example (Geriatric clinic)
76yo divorced Caucasian female seen in the Geriatric primary care clinic referred for mood instability and anxiety in the context of functional decline.
Medical problems: Macular degeneration, complicated hip replacement, collagenous colitis, hypothyroidism, COPD, osteoarthritis
Cultural considerations: Living situation, aging, complex medical conditions
Case conceptualization/interventions Collaboration with PCP
Case example (Pediatric clinic)
15-year-old, Hispanic female, seen in the pediatric primary care clinic
Referred by her PCP for suicidal ideation, depression, anxiety/panic, extensive bullying, not sleeping Medical problems: Obesity
Cultural considerations, family factors (sibling of special needs children), gender identity issues
Case conceptualization/interventions Transition from primary care to outpatient setting
BHC Impact ScaleHow helpful have the psychologists or psychology resident been in
addressing the following clinical areas?
Clinical Areas Assessed
• Depression/Anxiety4.83• Identification/Tx of
Substance Abuse4.67• Severe mental illness4.40• Psychiatric medications3.20• Chronic medical conditions4.40• Chronic Pain4.50• Family/Parenting issues4.67
Likert scale: 1 (Very Poor) 5 (Very Good)
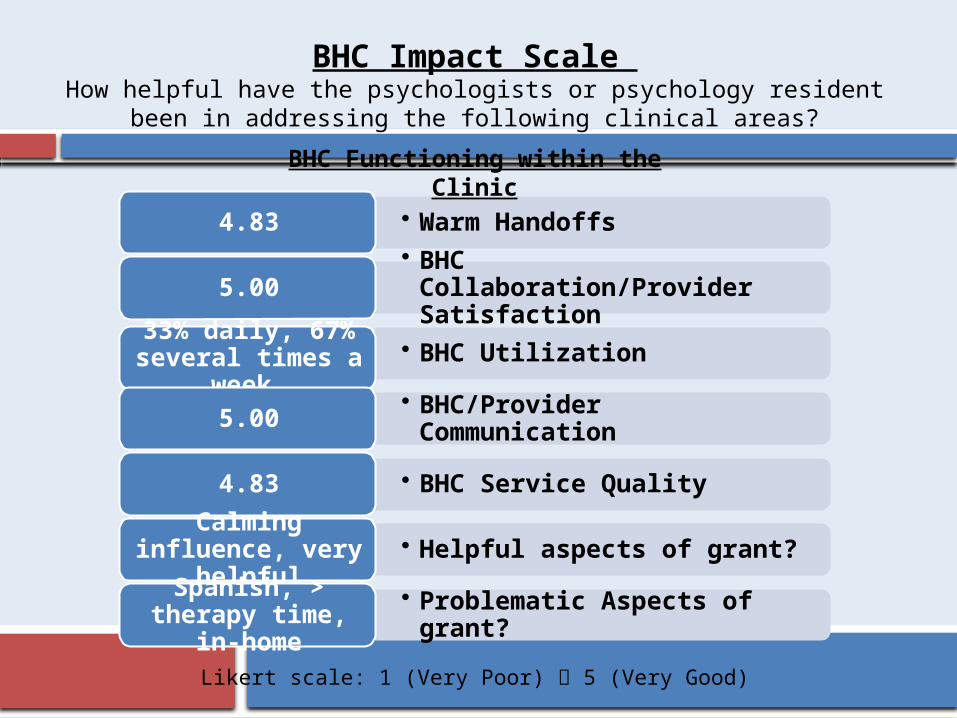
BHC Impact Scale How helpful have the psychologists or psychology resident been in
addressing the following clinical areas?
• Warm Handoffs4.83• BHC
Collaboration/Provider Satisfaction
5.00
• BHC Utilization33% daily, 67% several times a
week • BHC/Provider Communication5.00
• BHC Service Quality4.83
• Helpful aspects of grant?Calming
influence, very helpful
• Problematic Aspects of grant?
Spanish, > therapy time,
in-home
BHC Functioning within the Clinic
Likert scale: 1 (Very Poor) 5 (Very Good)
Lessons learned one year in
Timing of grant funding Buy in from clinics, teaching and marketing Provider variability Logistical challenges Need for modification/adaptation of interventions
specific to the population Underestimation of substance use disorders Importance of baseline screening measures to
identify changes in cognitive functioning and mood
Opportunities
• Additional coverage• Social work and psychiatric support• Group Therapy• Trainings for providers • Need for bilingual behavioral health
providers
References
Becker Herbst, R., Margolis, K. L., Millar, A. M., Muther, E. F., & Talmi, A. (2015). Lost in Translation: Identifying Behavioral Health Disparities in Pediatric Primary Care. J Pediatr Psychol. doi: 10.1093/jpepsy/jsv079.
Carey, W.B., & McDevitt, S.C. (2012). Child behavioral assessment and management in primary care: Theory and practice. Scottsdale, AZ: Behavioral-Developmental Initiatives. Cohen, D. J., Davis, M., Balasubramanian, B. A., Gunn, R., Hall, J., deGruy, F. V., 3rd, . . . Miller, B. F. (2015). Integrating Behavioral Health and Primary Care: Consulting, Coordinating and Collaborating Among Professionals. J Am Board Fam Med, 28 Suppl 1, S21-31. doi: 10.3122/jabfm.2015.S1.150042.
Hall, J., Cohen, D. J., Davis, M., Gunn, R., Blount, A., Pollack, D. A., . . . Miller, B. F. (2015). Preparing the Workforce for Behavioral Health and Primary Care Integration. J Am Board Fam Med, 28 Suppl 1, S41-51. doi: 10.3122/jabfm.2015.S1.150054.
Hill, J. M. (2015). Behavioral health integration: Transforming patient care, medical resident education, and physician effectiveness. Int J Psychiatry Med, 50(1), 36-49. doi: 10.1177/0091217415592357.
Karel, M., Gatz, M., & Smyer, M. A. (2012). Aging and mental health in the decade ahead: What psychologists need to know. American Psychologist, 67(3), 184-198. Lichtenberg, P.A., Mast, B.T., Carpenter, B.D., Loebach Wetherell, J. (2015). APA handbook of clinical geropsychology, Vol. 2: Assessment, treatment, and issues of later life. Washington, DC: American Psychological Association. Kapalka, G.M. (2011). Internship and fellowship experiences: Preparing psychology trainees for effective collaboration with primary care physicians. In G.M. Kapalka (Ed.), Pediatricians and pharmacologically trained psychologists: Practitioner’s guide to collaborative treatment. New York, NY: Springer-Verlag. Segal, D. L., Qualls, S. H., & Smyer, M. A. (2011). Aging and mental health (2nd edition). Hoboken, NJ: Wiley.
Session Evaluation
Please complete and return theevaluation form to the classroom monitor