27
EXPERIENCE IN THE MANAGEMENT OF URETEROVAGINAL FISTULA IN SOUTH-EAST NIGERIA DR. DANIYAN ABC
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | audrey-simon |
| View: | 220 times |
| Download: | 0 times |

EXPERIENCE IN THE MANAGEMENT OF URETEROVAGINAL
FISTULA IN SOUTH-EAST NIGERIA
DR. DANIYAN ABC

Authors Daniyan ABC1
Dantani D1
Sunday-Adeoye I1
Uguru SM1
Lengman S1
1 National Obstetric Fistula Centre, Abakaliki, Ebonyi State
Correspondence:Daniyan ABCNational Obstetric Fistula Centre, Abakaliki
04/19/23 2

ABSTRACTBackground:Ureterovaginal fistula is a well-recognized complication of pelvic
surgeries. Objective: To document our experience in the management of women with
ureterovaginal fistula at the National Obstetric Fistula Centre, Abakaliki Methodology: A retrospective study carried out at the National Obstetric Fistula
Centre, Abakaliki from January 2011 to October 2014. The history, physical findings, diagnosis, operation notes and follow-up notes of the women were studied. Relevant information was extracted and entered into a proforma. The data was analysed using the SPSS version 20.
Results: During the period of study, 40 patients had surgery for ureterovaginal fistula constituting 4.4% of surgeries for genital fistula. Fistula resulted from emergency caesarean section in 36 (90%) patients, hysterectomy for ruptured uterus in 2 (5%), total abdominal hysterectomy in 1 (2.5%) and congenital malformation in 1 (2.5%). Of the 38 women who developed ureterovaginal fistula following delivery, 37 (97.4%) had prolonged obstructed labour. Diagnosis was made clinically in 38 (95%) patients. All the patients had ureteroneocystostomy. The transabdominal route was used in 36 (90%) patients while transvaginal route was used in 4 (10%). In 26 (65%) patients, the left ureter was affected while the right was affected in 14 (35%). Post-operatively, 3 (7.5%) patients had anaemia, 2 (5%) had wound breakdown and 1 (2.5%) had sepsis.
Conclusion: Emergency caesarean section for prolonged obstructed labour is the commonest cause of ureterovaginal fistula in this study and the left ureter is more commonly affected. Clinical diagnosis is reliable and ureteroneocystostomy gives excellent outcomes.
Keywords: Ureterovaginal, Fistula, Injury
04/19/23 3
INTRODUCTION
• Ureterovaginal fistula is a communication between the ureter and the vagina
• Urine flows directly from the ureter into the vagina without passing through the bladder 1
• It is a dreaded complication of gynaecological surgeries, usually occurring following injury to the ureter
• It has a profound impact on quality of life and psychosocial well-being due to the continuous leakage of urine that results 2
04/19/23 4

INTRODUCTION• Ureteric injury is due to the close
proximity of the ureters to the uterus and cervix
• Incidences varying from 0.2 – 1.2% during abdominal or pelvic surgeries have been reported 3,4
• The injury detection rate is increased when intraoperative diagnostic cystoscopy is employed 5,6
• The left ureter is more vulnerable 7,8
04/19/23 5
INTRODUCTION• The commonest site of ureteral
injury is near the uterine vessels • The injury may occur in the form
crushing, ligation, transection, resection and devascularization• Early diagnosis using
intraoperative cystoscopy and early repair advocated to prevent compromise of the ipsilateral kidney 5,6,9,10
04/19/23 6
INTRODUCTION• When injury is unrecognised or repair is
delayed, ureterovaginal fistula occurs from extravasation of urine
• The presentation is that of continuous urinary incontinence after an abdominal/pelvic surgery 11
• Unlike VVF, the patient experiences normal voiding and dye test is negative
• Diagnosis is established by cystoscopy and intravenous urography (IVU) 12
04/19/23 7

INTRODUCTION
• When diagnosis is delayed, correction is by re-implanting the affected ureter into the bladder or by end-to-end anastomosis 11,12
• We undertook a review of 40 patients to document our experience in the management of women with ureterovaginal fistula
04/19/23 8

Methodology• A retrospective study carried out at the
National Obstetric Fistula Centre, Abakaliki • The records of women who underwent
surgical repair of ureterovaginal fistula over a period of four years from January 2011 to October 2014 were reviewed
• The history, physical findings, diagnoses, operation notes and follow-up notes of these women were studied
• Relevant data was extracted and entered into a structured proforma
• The data was analysed for descriptive statistics using the Statistical Package for Social Sciences (SPSS) version 20 and presented in tabular form
04/19/23 9

RESULTS • During the period of study, 915
patients had surgery for genital fistula • Out of these, 40 patients underwent
repair of ureterovaginal fistula • Hence repair of ureterovaginal fistula
accounted for 4.4% of all fistula surgeries carried out
• The mean age of the patients was 34.3 + 11.4 years.
• Emergency caesarean section (EMCS) for prolonged obstructed labour was the cause in 36 (90%) patients04/19/23 10

Table 1 Causes of ureterovaginal fistula
Causes Frequencies (%)
EMCS for prolonged obstructed labour
36 (90.0)
Hysterectomy for ruptured uterus
2 (5.0)
Total abdominal hysterectomy
1 (2.5)
Congenital malformation 1 (2.5)
Total 40 (100.0)04/19/23 11

Table 2 Fetal outcomes among women who developed ureterovaginal fistula
following delivery
Fetal outcomes Frequencies (%)
Stillbirth 30 (78.9)Live neonate 8 (21.1)Total 38 (100.0)
04/19/23 12
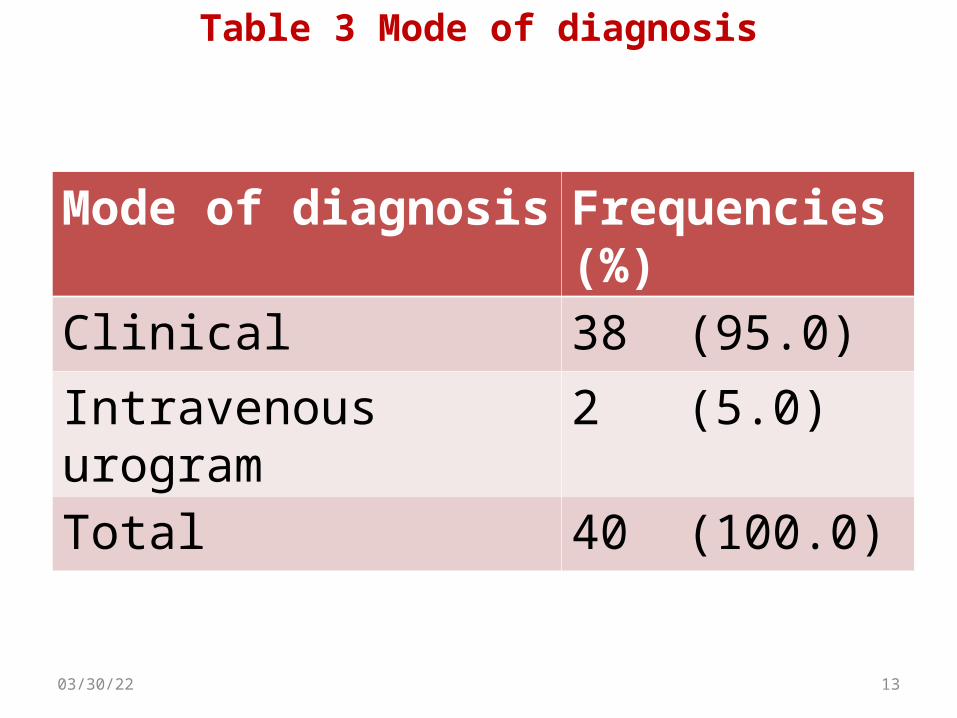
Table 3 Mode of diagnosis
Mode of diagnosis
Frequencies (%)
Clinical 38 (95.0)Intravenous urogram
2 (5.0)
Total 40 (100.0)
04/19/23 13
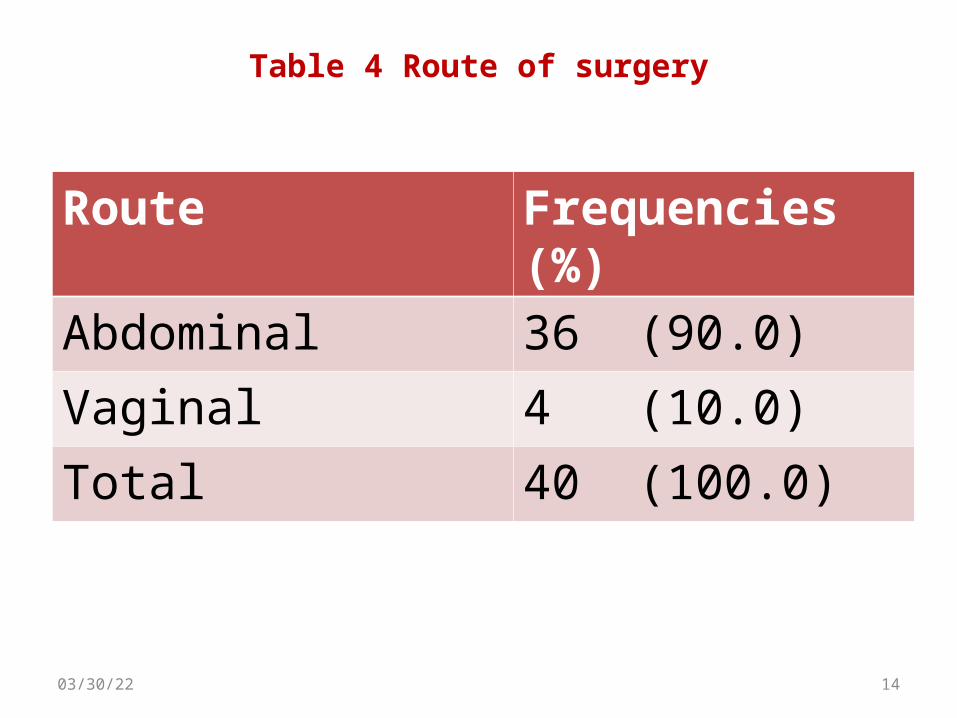
Table 4 Route of surgery
Route Frequencies (%)
Abdominal 36 (90.0)Vaginal 4 (10.0)Total 40 (100.0)
04/19/23 14

Table 5 Affected ureter
Affected ureter Frequencies (%)
Left ureter 26 (65.0)Right ureter 14 (35.0)Total 40 (100.0)
04/19/23 15

Table 6 Complications of repair
Complications Frequencies (%)
No complication 34 (85.0)Anaemia 3 (7.5)Wound breakdown
2 (5.0)
Sepsis 1 (2.5)Total 40 (100.0)
04/19/23 16

DISCUSSION• The vast majority of the cases of
ureterovaginal fistula resulted from EMCS for prolonged obstructed labour
• This finding is in sharp contrast to that of the developed world where hysterectomy is the commonest cause 2,3,12-15
• It does appear however, that obstetric procedures are the main causes in the developing world 16,17
04/19/23 17

DISCUSSION• A study done in Enugu reported
caesarean sections (38%) and caesarean hysterectomies (25%) as the leading causes of ureterovaginal fistula, together constituting up to 63% 18
• Reflects the poor standard of care available to pregnant women in this environment
• Portends serious medico-legal implications
04/19/23 18

DISCUSSION• The diagnosis of ureterovaginal fistula
was made clinically in 95% of the patients. IVU was used in 2 patients
• The diagnosis of this condition usually involves cystoscopy, ultrasound scan, IVU and retrograde ureterography 3,12
• However, these may not be feasible for extremely indigent patients seeking care in a resource-constrained setting04/19/23 19
DISCUSSION• To maximize the available resources,
symptoms, signs and dye test were used to make diagnosis
• Although the dye test may be used to differentiate ureterovaginal fistula from VVF, it does not identify the affected ureter. This was done intraoperatively
• The use of such well-known, simple diagnostic methods in resource-constrained settings has been documented 16
04/19/23 20

DISCUSSION• In 26 patients, the left ureter was affected while
the right was affected in 14• This is consistent with findings from other studies 7,8,15
• Most surgeons operate from the patients’ right making the left ureter to be further away from them
• Also, the left ureter is closer to the cervix than the right making it more prone to injury 19
• The left ureter is also said to be 1cm shorter than the right 20. It has been suggested that this makes it less free, hence more vulnerable to injury when securing haemostasis
04/19/23 21

DISCUSSION• All the patients had ureteroneocystostomy
with ureteric stents which were removed after one week
• They all had delayed repair as a result of late presentation
• Immediate repair is however advocated when feasible 5,6,9,10,15
• Another option is preliminary diversion via a percutaneous nephrostomy followed later by delayed repair 19
• The abdominal route was used in 36 patients while vaginal route was used in 4 patients
04/19/23 22

DISCUSSION• None of the patients had end-to-end
anastomosis of the ureter, Psoas hitch or Boari flap
• The choice of route/type of surgery had to do with familiarity on the part of the surgeon
• Postoperative complications seen in 6 (15%) patients - anaemia in 3, wound breakdown in 2 and sepsis in 1
• Outcomes were good - 100% continence rate at discharge and 95% at three months follow-up04/19/23 23
CONCLUSION
• Emergency caesarean section for prolonged obstructed labour is the commonest cause of ureterovaginal fistula in our environment
• The left ureter is more commonly affected• Clinical diagnosis is reliable • Ureteroneocystostomy gives good outcomes • We strongly recommend improved access to
quality maternity care
04/19/23 24
REFERENCES• Burivong W, Leelasithorn V, Varavithya V. Common lower urinary tract fistulas: A review
of clinical presentations, causes and radiographic imaging. International Journal of Case Reports and Images 2011;2:1-7.
• Murtaza B, Mahmood A, Niaz WA, Akmal M, Ahmad H. Ureterovaginal fistula - etiological factors and outcome. JPMA 2012; 62:999.
• Purandare CN. Urological injuries in gynecology. J Obstet Gynecol India 2007; 57:203-4.• Park JH, Park JW, Song K, Jo MK. Ureteral injury in gynecologic surgery: a 5-year review
in a community hospital. Korean J Urol 2012; 53: 120-5.• Ibeanu OA, Chesson RR, Echols KT, Nieves M, Busangu F, Nolan TE. Urinary tract injury
during hysterectomy based on universal cystoscopy. Obstet Gynecol 2009;113: 6-10.• Gilmour DT, Das S, Flowerdew G. Rates of urinary tract injury from gynecologic surgery
and the role of intraoperative cystoscopy. Obstet Gynecol 2006; 107: 1366-72.• Obarisiagbon, EO, Olagbuji BN, Onuora VC, Oguike TC, Ande ABA. Iatrogenic Urological
injuries complicating obstetric and gynaecological procedures. Singapore Med J 2011; 52: 738-41.
• Nnabugwu I, Amu O. Iatrogenic Ureteric injuries complicating open obstetric and gynaecological operations in South East Nigeria – case series. JWACS 2010; 1: 3
• Sternschuss G. Ureteral injury in gynecologic laparoscopy. World J Lap Surg 2012; 5: 46-8.
• Yu S, Wu H, Xu L, Li G, Zhang Z. early surgical repair of iatrogenic ureterovaginal fistula secondary to gynaecologic surgery. Int J Obstet Gynecol 2013; 123: 135-8.
04/19/23 25
REFERENCES• Rafique M, Arif MH. Management of iatrogenic Ureteric injuries associated with
gynecological surgery. International Urology and Nephrology 2002; 34: 31-5.• Ares Valdes Y, Romero Diaz CA, Mederos Curbelo ON, Hernandez Silverio D, Alonzo
Dominguez F, Cantero Ronquillo A. Ureteral lesions in gynecologic surgery. Arch Esp Urol 2003; 56: 119-24.
• Selzman AA, Spirnak JP, Kursh ED. The changing management of ureterovaginal fistulas. J Urol 1995; 153: 626-8.
• Mandal AK, Sharma SK, Vaidyanathan S, Goswami AK. Ureterovaginal fistula: summary of 18 years’ experience. Br J Urol 1990; 65: 453-6.
• Mahendran HA, Singam P, Ho C, Hong GE, Hee TG, Zainuddin ZM. Iatrogenic ureter injuries: eleven years experience in a tertiary hospital. Med J Malaysia 2012; 67: 169-72.
• Randawa A, Khalid L, Abbas A. Diagnosis and management of ureterovaginal fistula in a resource-constrained setting: experience at a district hospital in northern Nigeria. Libyan J Med 2009; 4: 41-3.
• Bennani S, Joual A, El Mrini M, Benjelloun S. Ureterovaginal fistulas. A report of 17 cases. J Gynecol Obstet Biol Reprod (Paris) 1996; 25: 56-9.
• Ozumba BC, Attah CA. Ureteral injury in obstetric and gynecologic operations in Nigeria. Int J Gynecol Obstet 1991; 36: 131-5.
• Onuora VC, al-Mohalhal S, Youssef AM, Patil M. Iatrogenic urogenital fistulae. Br J Urol 1993; 71: 176-8.
• Chan JK, Morrow J, Manetta A. Prevention of ureteral injuries in gynecologic surgery. Am J Obstet Gynecol 2003; 188: 1273-7.
04/19/23 26

THANK YOU














![Prosthodontic Management of Oroantral Fistula: A Case Report · prosthodontic management of oroantral fistula. Case Series Abstract Oroantral fistula (oroantral communications [OACs])](https://static.documents.pub/doc/80x56/5e7beca2e72ed6083b54888d/prosthodontic-management-of-oroantral-fistula-a-case-report-prosthodontic-management.jpg)


