Page 1
ExposuretoCommunityViolence:TraumaInformedCareinthePediatricMedicalHome
JamesDuffee,MD,MPH,FAAPOhioAAPAnnualMeeting
September,2016
MOCII:ExposuretoCommunityViolence
JamesDuffee,MD,MPH,FAAPNationwideChildren’sHospital
TraumaInformedCareinthePediatricMentalHomeMOCII:ExposuretoCommunityViolence
JamesDuffee,MD,MPH,FAAPDaytonChildren’sHospital
TraumaInformedCareinthePediatricMentalHome
Page 2
Disclosure
IhavenopersonalfinancialrelationshipsinanycommercialinterestrelatedtothisCME.
Idonotplantoreferenceofflabel/unapprovedusesofdrugsordevices.
Page 3
RecordingYourResponsesPaperForm• Foryourconvenience,wehavecreatedpaperanswerformsthat
areinyourpacket.Thestaffsessionleaderalsohashardcopies.• PleaseenteryourABPdiplomatenumberandanswersonthe
form.• TurntheformintoOhioAAPstaffmemberatthedoorontheway
outofthesession.• CreditwillbeenteredintoyourABPprofilewithin3businessdays.ElectronicLink• Ifyouprefertousetheweblink,enterthefollowinglinkintoyourbrowser,selectstep4andstartquiz:OhioAAP.org/MOCPartII/Trauma• Ifyouexperienceanytechnicalissues,intheinterestoftime,apaperformwillbegiventoyou.
Page 4
LearningObjectives1. Understandthefrequencyandextentofexposureto
differentformsofviolencebychildrenandadolescentsaccordingtodevelopmentalstage.
2. Describepossiblebehavioraloremotionalresponsesbychildrenexposedtocommunityviolence,strategiestoidentifychildrenatriskforprolongedormaladaptivereactions,andinterventionsthataresupportedbyevidence,eitherinpediatricpracticeorwithcommunitypartners.
3. Applytheconceptsoftrauma-informedpediatricpractice,includinginterviewingtechniques,staffdevelopmentandofficepoliciestoavoidrepeatorcontinuedtraumaexperiencedbychildrenpreviouslyexposedtocommunityviolence.
Page 5
CultureofViolence
• Continuumofviolence– Fromchildabuseandintimatepartnerviolence– throughbullyingandpeerviolence– toyouthviolenceandcriminality
• Eco-bio-developmentalmodelforunderstandingandprevention
• Requiresthepediatricmedicalhometobecometrauma-informed
Page 6
ShiftingParadigms• Theoriginsoflifelonghealthareinearlychildhood• Considerneuro-developmentaltrajectoriesratherthanbehaviors
• Strength-basedassessment– RiskandProtectiveFactors
• PopulationHealth(upstream)Perspective– Distributionofhealthoutcomes– Healthdeterminantsthatinfluencedistribution– Policiesthataffectdeterminants
• CommunityEngagement
Page 7
ChildhoodExposuretoViolence• Home
– Childmaltreatment– IntimatePartnerViolence– Siblingassault
• Community– Bullying,non-siblingassault– Sexualassault,datingviolence– Othercommunityorschoolviolencewww.DefendingChildhood.org
Page 8
ExposureatHome
• 40%ofteensreportexposuretoatleastonetypeofIPVoverlifetime
• 1in6childrenhavebeenexposedtophysicalIPVoverlifetime,about13.6million
• 14%reportpastyearmaltreatmentfromaparentorcaregiver,10millionchildren
Page 9
ExposureintheCommunity
• 60%ofchildrenandyouthreportthattheyhaveexperiencedorwitnessedviolentvictimizationinthepastyear
• About3in10childrenreportmoderateorfrequentbullying
• Overathirdofgirlsaged14to17reportsexualvictimizationovertheirlifetime
Page 10
Polyvictimization
• 11%ofchildrenreportexposureto5ormoredifferentkindsofviolenceinthepastyear
• Childrenexposedtoonetypeareathigherriskofothertypes– 4to6timeshigherriskofseriousvictimization,injuryorassaultwithweapon
– Mostlikelytoreportpost-traumasymptoms
Page 11
RacialandEthnicInequity
• Structuralviolencerelatedtoracismandethnicprejudicecompoundstheriskofexposuretocommunityviolence
• ParticularlyimportantforNativeAmerican,AlaskanNativeandAfricanAmericanchildren
• Spatialracism,criminaljusticeinequities(policing,sentencing)
• Hateorbiascrimes
Page 12
ConsequencesofExposure
• Youthexposedtoviolenceathigherriskofcriminalbehavior
• Exposureassociatedwithloweracademicachievementandhigherabsenteeism
• AdverseChildhoodExperiencesstudyfoundassociationswithaplethoraofpooradultphysicalandmentalhealthoutcomes
• Racismcompoundspooroutcomes
Page 13
NationalSurveyofChildren’sExposuretoViolence(NatSCEV)
• 4,549childrenandadolescents,twogroups• Representativesample• Oversampleofexchangesassociatedwithhighdensity(70%)ofAfrican-American,Latinoorlow-incomecommunities
• Telephonesurvey,adultsprovideddemographics,childrensurveyed
• Screeningquestionsincluded48typesofvictimization
Page 14
ScreeningQuestions
• Conventionalcrime– Assault,robbery,kidnapping
– Hateorbiascrime
• Childmaltreatment• Sexualvictimization• Peerandsiblingvictimization
• Schoolviolenceandthreat
• Internetvictimization• Witnessingandindirectvictimization
Page 15
ExposurebyDevelopmentalAge
• MiddleChildhood– Assaultwithoutaweapon
– Physicalbullying
• EarlyAdolescence(10to13)– Assaultwithweapon– Kidnapping– Witnessingfamilyassault
• OlderAdolescentsmostlikelytoexperiencemoreseriousformsofviolence– Assaultswithinjury,gangassaults
– Sexualvictimization– Exposuretoshooting,schoolbombthreat
Page 16
SomeSurveyResults
• 60%pastyear,10%fiveormorepastyear• Morethan70%witnessedviolencetoanotherpersonoverlifetime
• 3.5%preschoolershadwitnessedshooting,morethanoneinfive14to17yearolds
• Boysmorelikelytowitnessmurder,shootingsandotherformsofcommunityviolence
Page 17
AdverseChildhoodExperiences
• 10originalACEs– Childabuse– Childneglect– Householddysfunction
• Additions– Economicstress– Bullying,schoolviolence– Communityviolence
• MedicalStress• RefugeeStress• NaturalDisasters• Masstraumaevents
– Shootings– Terrorism
Page 18
SAMHSA’s ConceptofTrauma
• Referstoemotionaltrauma.• Definedasanevent,seriesofevents,orsetofcircumstancesthatisexperiencedasbyanindividualasphysicallyoremotionallyharmfulandthathaslastingadverseeffectsontheperson’sfunctioningandmental,physical,emotionalorspiritualwell-being.
• SAMHSA’s GuidanceforaTrauma-InformedApproach(2014)
Page 19
CumulativeBurdenofRecurrentorPersistentExposuretoTrauma
• Alterationsinbrainarchitecture• Changesingeneexpression• Endocrineandimmuneimbalance• Decreasedexecutivefunctionandaffectregulation
• Interferencewithrelationalhealth• Behavioralallostasis• Chronicillness,healthdisparities,decreasedqualityandlengthoflife
Page 20
EffectsonBrainArchitecture
• Epigenetic-interactionwithhormonesandinflammatoryfactors
• Neuronsthatfiretogether,wiretogether
• Decreasedgreymattervolume
• Smallerhippocampus• Decreasedprefrontaldendritic proliferationanddecreasedactivity
• Amygdala hypertrophy
Page 21
EffectsonNEIFunction
• Epigeneticchangeincontrolofchronicstressresponse
• ProlongedactivationFlight-Fight-Freeze(amygdala)
• Alterationsinhormonesthatenhanceandsustainpro-socialbehavior
• Imbalanceofactivationandsuppressionofinflammatorycytokines
Page 22
Sara B. Johnson et al. Pediatrics 2013;131:319-327
©2013 by American Academy of Pediatrics
NEIMediation
Page 23
DoseResponseIncreasedRisk• Alcoholismandalcohol
abuse• Liverdisease• Smoking• Chronicobstructive
pulmonarydisease• Illicitdruguse• Ischemicheartdisease• Depression• Suicideattempts
• Intimatepartnerviolence• Earlyinitiationofsexual
activity• Multiplesexualpartners• Sexuallytransmitted
diseases• Unintendedpregnancies• Prematurity,smallfor
gestationalage• Fetaldeath
Page 24
ACEStudyConclusion
• Adversechildhoodexperiencesmaybeamongthebasicfactorsthatunderliehealthrisks,illness,anddeath,andcanbeidentifiedearlybyroutinescreeningofallchildren.
• Earlyidentificationofchildrenatriskallowsforstratified,targetedinterventioninordertobuffertheeffectsandchangethedevelopmentaltrajectory
Page 25
FunctionalCorrelatestoStressActivation
• Increasedsympathetictone• Toiletingdifficulties,regressionofmilestones• Enuresis,Encopresis
• Anxietyrelatedinhibitionofsatiety• Foodhording• Lossofappetiteorstuffing
• Overstimulationofreticularactivatingsystem• Difficultywithsleeponset• nightmares
Page 26
BehavioralReactionstoTrauma
• Normativebehavioralreactions– Resolvewithinafewweeks
• Acutevs.ChronicExposure
• Mediators– Attachment– Resilience
• Maladaptiveresponses– Externalizing
• Non-compliance• Impairedself-regulation
– Internalizing• Depression• Anxiety• Posttraumaticstressdisorder
Page 27
NormativeResponsestoAcuteTrauma
• Sleepproblems– Nightmares– Nightawakenings
• Eatingproblems• Sadness• Anxiety• Irritability
• Difficultywithconcentration
• Exacerbationofrisk-takingbehavior
• Developmentalregression– Bedwetting– Tantrums
Page 28
OverviewofAttachment
• JohnBowlby 1907-1990 • Emotionalbondsarebasicforsurvival
• Interactivesystemstomaintainproximityorreadyaccess
• Workingmodelsofselfandotherinmind
• Careseeking/caregivingarecomplementary
Page 29
AttachmentPatternsSecure• Seeksprimary(secure
base)whendistressed• Curious,exploring
environment• Self-confident• Asksforhelp
Insecure• Avoidant
– Passive,withdrawn– Avoidsfeelings,doesn’t
expressdistress• Resistant
– Maybecharming,clingingoroveractivelikeADHD
– Entertainingtoadults,maybeindiscriminant
• Chaotic
Page 30
Resilience
• Theabilitytoavoidphysiologicandbehavioraldamagefromexposuretochronicstress
• Theprocessofadaptingwellinthefaceofadversity
• Theresultofusingprotectivefactorstomanagemultiplestressfulcircumstanceswithouttoxiceffects
• Transformstoxicstresstotolerablestress
Page 31
ResilientChildrenHaveinCommon
• Atleastonestable,caringandsupportiverelationship
• Asenseofself-efficacyormasteryoverlifecircumstances
• Strongexecutivefunctionandself-regulation• Solidgroundinginfaithorculturaltraditions
Page 32
OtherCharacterTraits
• Senseofhumor• Abilitytoformattachments• Innerpsychologicalspacethatprotects
– Innerlocusofcontrol– Tendencytogrowwhenpresentedwithadversity
• Threeyoucan’tdowithout– Flexibility,abilitytoimprovise– Acceptanceofreality– Strongfaiththatlifehasmeaning
Page 33
“Wemustneverforgetthatwemayalsofindmeaninginlifeevenwhenconfrontedwithahopelesssituation,whenfacingafatethatcannotbechanged.”– VictorFrankl,MD
Page 34
HowDoesResilienceDevelop?
• Combinationofinnate,intrinsicandextrinsicfactors
• Alsocombinationofsupportiverelationships,skill-buildingandpositiveexperiences
• Resilienceistheresultofmultipleinteractionsbetweenenvironmentalprotectivefactorsandhighlyresponsivebiologicsystems.
• HarvardCenterontheDevelopingChild
Page 35
ResilienceCanBeLearned
• Importantrelationshipsvaryoverthelifecourse– Parents,grandparents,siblings,peers,intimatepartners
– Groundedinearlyexperiences• Self-regulationandotherexecutivefunctionsstimulatedinearlychildhood
• Non-cognitiveskills(empathy)canbetaughtaslateasadolescence
• Contemporaryemphasisontwo-generationalinterventions
Page 36
ResilienceandRelationalHealth
Themostimportantandfrequentcommonalityofchildrenwhosucceedisthattheyhavehadaleastonestableandcommittedrelationshipwithasupportiveparent,caregiverorotheradult.
HarvardUniversityCenterontheDevelopingChildhttp://developingchild.harvard.edu
Page 38
Inspiration
https://www.youtube.com/watch?v=-LGHtc_D328
Page 39
PediatricMedicalTrauma
• Pain• Procedures• Sedation/lossofconsciousness
• Separation/Isolation• Exposuretosickness/death
• Life-threateningepisodes/relapse
• Responseandinterventiondependentondevelopmentalage– Pre-existingfactors– Personalresilience
• FamilyCrisis– Culturalunderstanding– Parentalroleadjustment– Siblingreaction
Page 40
CanHospitalizationPrecipitateToxicStress?
ShahAN,Jerardi KE,AugerKA,BeckAF.PEDIATRICSVolume137,number5,May2016:e 20160204
Page 41
Trauma-InformedPediatrics
• Family-centered,trauma-informedcare• Complexcaremanagementstrategies
– Applycarecoordination– Screenforsignsoftrauma,alsoforfamilystrengths
– Maintainresourceforlinkingtoservices• Multidisciplinary(multiagency)team• Buildonfamilystrengths
Page 42
Family-CenteredCare• Respectseachchildandfamily,andhonoringracial,ethnic,cultural,andsocioeconomicbackgroundandexperiences
• Ensuresflexibilityinpolicies,procedures,andpracticesinordertoadaptservicestotheneeds,beliefs,andculturalvalues
• Sharescomplete,unbiasedinformation• Providesformalandinformalsupport• Collaborateswithpatientsandfamiliesatalllevels• Buildsonfamilystrengths,empoweringdecisions
AmericanAcademyofPediatrics(AAP)CommitteeonHospitalCareandInstituteforPatient-andFamily-CenteredCare(2012)
Page 43
Trauma-InformedCare
§ Understandstheproximalanddistaleffectsofadversechildhoodexperiences
§ Recognizesthesignsandsymptomsoftrauma
§ Integratesknowledgeoftraumaintopoliciesandprocedures,andpracticemanagement
§ Resistsre-traumatization
www.samhsa.gov/nctic/trauma-interventions
Page 44
www.healthcaretoolbox.org
Page 45
Trauma-InformedPrimaryCare(TIPC)
• Foundations• Environment• Screening
– HistoryofTrauma– RiskandProtectiveFactor
Machtinger et.al.FromTreatmenttoHealing:ThePromiseofTrauma-InformedPrimaryCare.Women’sHealthIssues.2015;25(3)193-197
• Primaryprevention– StrengtheningFamilies– Promotingrelationalhealth
• Response– Integratedprimarycare– Coordinationwithcommunityprograms
Page 46
FoundationsofTIPC
• Safety• TrustworthinessandTransparency• PeerSupport• CollaborationandMutuality• Empowerment,VoiceandChoice• Recognitionofhistoricaltrauma,adoptionofpoliciesandprocessesresponsivetocultural,racialandethnicneeds
Page 47
PhysicalEnvironment
• Healthcaresettingsinwhichchildrenandfamiliesfeelsafe,physicallyandemotionally
• Soothingofficeenvironments– Noiselevel,therapydog– Welcomingarchitecturalfeatures,signage
• Parkinglots,bathroomsmonitored,welllit• Makesurepatients(andstaff)haveclearaccesstotheexamroomdoor
Page 48
EmotionalEnvironment
• Respectpersonalhistoryandexperience• Ensurestaffmaintainsafeinterpersonalboundariesandcanmanageconflicteffectively
• Maintainopen,compassionatecommunication
• Beawareofculturaldifferencesregardingtrauma,safetyandprivacy
Page 49
ModificationsofHealthCareDelivery
• Emphasizerelationshipsduringhealthpromotionvisits– StrengtheningFamiliesFramework– Promoterelationalhealth
• CircleofSecurity• PromotingFirstRelationships
• Screen– Historyoftrauma,currentexposure– Riskandprotectivefactors– Traumarelatedsymptoms
Page 50
StrengtheningFamiliesCenterforStudyofSocialPolicy
• TwoGenerationalApproach• ConsiderationofCulture
– Fromculturalcompetencetoculturalhumility• Strength-basedperspective• BiologyofStress• Resiliencetheory• FocusonWell-being• AwarenessofRiskandProtectiveFactors
Page 51
ProtectiveFactorsFramework
• Parentalresilience• Knowledgeofparentingandchilddevelopment
• Socialconnections• Concretesupportintimesofneed• Socialandemotionalcompetenceofchildren
Page 52
PromoteCaretakerResilience
• Identifystrengthsandprotectivefactorsinthefamily,nurtureparentalself-esteem
• Encouragesocialconnectedness• Rememberthatbeingconnectedmeansgivinghelpinadditiontoreceivinghelp
• Provideguidance,mentoringtoimproveself-efficacy
• “puttheoxygenmaskonyourselffirst”• Encourageself-reflectioninparent,childandmutualactivities,keepchildinmind
Page 53
TheCircleofSecurity
.www.circleofsecuritynetwork.org/the_circle_of_security.htm
Page 54
PromotingFirstRelationships
http://pfrprogram.org
Page 55
ScreenforTrauma
• Universalscreeninginprimarycarereducespotentialbias
• Apositivescreenisadisclosureandtheemotionalenvironmentmustbereadytoholdthetrauma.
• Screeningshouldalwaysbenefitthepatient—mustbeaddressedinsomeway
• Ifpositiveforonetypeoftrauma,askaboutothersymptomsandexposures
• Re-screeningshouldbeavoided.
Page 56
YoungChildren
• ASQ-SE• M-Chat-R• PreschoolPediatricSymptomChecklist• StrengthsandDifficultiesQuestionnaire
Page 57
SchoolAgethroughAdolescence
• FindyourACEscorehttps://acestoohigh.com• StrengthandDifficultiesQuestionnaire• PediatricSymptomChecklist• Anxiety:SCARED• PTSD:PC-PTSD• SubstanceAbuse:CRAFFT(preferred)orCAGE-AID
Page 58
Depression
Adolescents• Preferred:
– PHQ-2andPHQ-9– PHQ- A
• ASKsuicidescreen• Alternate:
– BeckDepressionInventory
• Eachyearfrom12to18
MaternalDepression• Preferred:
– PHQ-2andPHQ-9
• Alternate:– Edinburgh– CES-D
• 1,2,4and6months
Page 59
Author's personal copy
410 N.J. Burke et al. / Child Abuse & Neglect 35 (2011) 408– 413
BOD emaN
laitinI & etaD xH yrogetaC ECA deineD 1. esubA lacisyhP 2. esubA lanoitomE
3. esubA lauxeS tcatnoC
4. Alcohol and/or Drug Abuser in the Household
5. Incarcerated Household Me mbe r
6. So meone Chronically Depressed, Mentally Ill, Institutionalized, or Suicidal
7. yltneloiV detaerT rehtoM
8. One or No Parents, Parental Separation, or Divorce
9. Emotional or Physical Neglect
laitinI & etaD xH seirogetaC 1+ deineD Ho melessness (Hx or Current)
tnedicnI citamuarT Foster Care System (Hx or Current)
esubA/ecneloiV ot ssentiW
laitinI & etaD xH derocS toN/rehtO deineD gnisuoH cilbuP
erusopxE gurD eniretuartnI
Child Protective Services Involve ment
Fig. 1. Trauma Screen.
when the review process follows rigorous standards (Gilbert, Lowenstein, Koziol-McLain, Barta, & Steiner, 1996; Greenspan &Wieder, 1997; Luck, Peabody, Dresselhaus, Lee, & Glassman, 2000; Nagy & Szatmari, 1986; Sartwell, 1974). To minimize errorsin this chart review, we adopted the following approach: all chart documentation was completed by one of two pediatricianswithin the same practice, a standard abstraction form was used, inter rater reliability was calculated, researchers were trainedand monitored by experts, and meetings were held to discuss clinical discrepancies between the research team members.Individual charts were reviewed according to published ACEs guidelines (http://www.acestudy.org) and approved by theprincipal investigators (VC and NB).
The number of experiences endorsed was counted and coded as any of the nine ACE categories. Each category endorsedas a traumatic event received a score of 1, hence potential scores range from 0 to 9. Furthermore, individual participant datawas optimized by including relevant supplementary information from siblings’ charts. All sibling charts were reviewed bythe second author and every fifth chart was reviewed by a research assistant. For each documented case of sibling abuse anote was included on the referenced patient’s chart and all uncertainties were resolved via clinical consensus in consultationwith the principal investigator (NB).
The medical charts were reviewed in entirety. Most information was taken from the “Progress Notes” section, the “Confi-dential” section, “Social Services” section, and records from previous providers. Parameters were ascertained either througha medical history form filled out by the patient or by the MD during patient visits. Patient history obtained by a physicianwas gathered by a single physician (NB) for the first 1 1/2 years (April 2007–November 2008) and then by both NB andanother pediatrician trained by NB from November 2008 to April 2009. History of abuse was determined by caregiver reportof abuse, CPS report of confirmed child abuse or historical medical record report of abuse. Cases of abuse that were suspectedby an MD but unsubstantiated after a CPS investigation were not included.
Documentation of learning/behavior problems and overweight/obesity was taken from the medical charts. Over-weight/obesity was defined as having a BMI ≥ 85%. Classification of learning/behavior problems was obtained from a clinical
• NadineBurke-Harris,MD
• https://www.ted.com/talks/nadine_burke_harris_how_childhood_trauma_affects_health_across_a_lifetime?language=en
Page 60
Youmayconsider
• SEEKSafeEnvironmentforEveryKid– http://theinstitute.umaryland.edu/frames/seek.cfm
• IntimatePartnerViolence– ParentScreeningQuestionnaire
• Haveyoubeeninarelationshipinwhichyouwerephysicallyhurtorthreatenedbyapartner?
• Inthepastyear,haveyoubeenafraidofapartner?• Inthepastyear,haveyouconsideredgettingacourtorderforprotection?
– Doyoufeelsafeathome?• Hasanythingbad,sadorscaryhappenedsincelasttimewemet?
Page 61
SCAREDhttp://www.psychiatry.pitt.edu/sites/default/files/Documents/assessments/SCARED%20Child.pdf
TraumaSymptomChecklistforChildrenandTraumaSymptomChecklistforYoungChildren(TSCCandTSCYC)http://www4.parinc.com
ChildPTSDSymptomScale(CPSS)[email protected]
Univ.ofCaliforniaatLosAngelesPosttraumaticStressDisorderReactionIndex(UCLA-PTSDRI)http://www.istss.org/UCLAPosttraumaticStressDisorderReactionIndex.htm
ScreeningInstruments
Page 63
Response:PracticeConsiderations
• Allstaffshouldbetrainedin– Traumainformedcare– Conflictresolution– CulturalHumility
• Maintainreferralresource
• Engagepartners– Homevisitors– Peermentors
• Considerintegratedprimarycare
Page 64
Response:ManagementofAcuteExposure
• DEFoftraumainformedcare• Guidanceforparentsandfamilies
• Recognizingtraumarelatedsymptoms• Managementofmediaexposure
• Whentorefer• Evidencebasedtherapies• Linktocommunityresources• Attendtosecondarytrauma
Page 65
Trauma-InformedPediatrics–DEFModel• ReduceDistress
– Providechildasmuchcontrolaspossible– Provideinformation,repeatback
• PromoteEmotional Support– Listen,empower– Respectexperienceandexpertise
• RemembertheFamily– Encourageself-care– Respectculturalandreligioustraditions
Page 66
IllorInjuredChildren• Reduce Distress
– Assessandmanagepain– Askaboutfearsandworries,– Considergriefandloss
• Promote EmotionalSupport– Askwhoandwhatthepatientneedsnow.Whatdoyouneed?
– Findoutiftherebarrierstomobilizingexistingsupport.• Rememberthe Family
– Assessthedistressofotherfamilymembers.– Gaugepre-existingfamilyprotectiveandriskfactors– Addressotherneeds,socialdeterminantsofhealth
– http://www.nctsn.org
Page 67
PsychologicalFirstAid
• Acuteinterventiontohelpchildren,youthandfamiliesinimmediateaftermathofdisaster
• Evidencebased• Listen,ProtectandConnect• Fiveprinciples
– Safety -- SelfandCommunityEfficacy– Calming -- Hope– Connectedness
Page 68
PsychologicalFirstAid:Activities
• Establishhumanconnection
• Providephysicalandemotionalcomfort
• Calmandorient• Offerpracticalassistancetoaddressimmediateneeds
• Connectwithfamily,neighbors,friends
• Supportadaptivecoping,strengths,resilience
• Encourageadults,youthandfamiliestotakeactiverole
• Linktoresponseteamorcommunityresources
Page 70
GuidanceforParents
• Sleepdisturbance– Consistentbedtime– Noscreentimebeforebed
– Nightlight– Accept,empathizewithfears
– Re-introducetransitionalobject
• EatingDisturbance– Noreprimandsorforce-feeding
– Play
• Toileting– Eliminatenegativeassociations
– Rewardsystem
Page 71
GuidanceforParents:Emotions
• Modelbylabelingownemotionsandexpressingemotionsinacontrolledmanner
• Givedirectionspositivelyandcalmly• Don’ttakebehaviorpersonally• Practicerelaxationandself-calmingskillswithchild
• Schedulespecialplaytime• Returntousualroutineassoonaspossible
Page 72
GuidanceforParents:CommunicationandMedia
• Varytheamountofinformationaboutadisasterormassviolenceaccordingtodevelopmentallevel
• Turnoffmediatolimitsecondaryexposureandfurthertrauma(alsoclinicreceptionarea)
• Olderchildrenbenefitfrommoreinformation• Foryoungerchildren,startwithsimple,basicfactsandtaketheleadfromquestions
Page 73
MaladaptiveResponsetoTrauma
• Internalizing• Dissociation
– Detachment,Numbness– Depression,Anxiety
• Moreoftengirls,youngchildrenorthosewhowerepowerless
• Externalizing• Arousal
– Hypervigilance– Aggression,disorderedconduct
– Exaggeratedresponse
• Moreoftenboys,olderandwitnesstoviolence
Page 74
WhentoRefer• “Hairtrigger”emotionalresponse,difficultyregulatingarousal
• Reluctancetoturntoothersforhelp• Inabilitytodiscussfeelings• Insecurityorexcessiveanxietyaboutsafetyorsocialconnectedness
• Significantpre-existingrisk– Loss,attachmentdisturbance– Familychaos,parentaldifficultycoping– Natureoftrauma– OtherSDH
Page 75
PTSD• Conditionedresponsetospecifictrauma• Intrusionsymptoms,avoidance,hyper-reactivity,dissociation,self-injury,triggers
• NEIdysfunction– Increasecatecholamines,increasedCVresponse– Amygdalehyperactivity,fearandanger,failureofregulationbymedialPFC
– PFCvolumelow,lackofexecutivecontrol- inabilitytodistinguishthreatsfromnon-threats
– Hippocampusvolumedecrease- memorydisturbance
Page 76
PTSDinChildrenUnderSix
• Potentiallytraumaticsituations:childmaltreatment,war,naturaldisasters,dogbites,invasivemedicalprocedures
• Intrusivethoughts,avoidance,exaggeratedreactivity
• DSM5modificationschangetheneedtoremembertheevent
• Sub-corticalmemory,somato-sensory
Page 77
EBTherapies- EarlyChildhood
ImproveRelationships Decreasedisruptivebehaviors
IncredibleYears +
Triple P- PositiveParentingProgram
+
CircleofSecurity(COS) +
Child ParentPsychotherapy(CPP)
+
Parent ChildInteractionTherapy(PCIT)
+ +
MultidimensionalTreatmentFosterCareforPreschoolers(MTFC-P)
+ +
Page 78
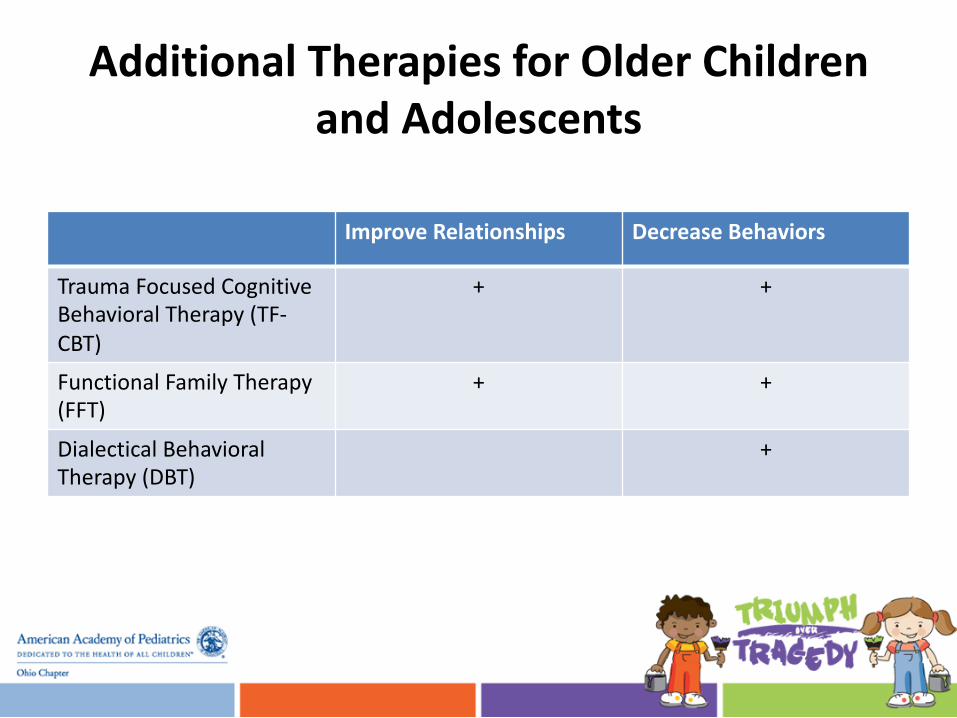
AdditionalTherapiesforOlderChildrenandAdolescents
ImproveRelationships DecreaseBehaviors
TraumaFocusedCognitiveBehavioral Therapy(TF-CBT)
+ +
FunctionalFamilyTherapy(FFT)
+ +
Dialectical BehavioralTherapy(DBT)
+
Page 79
Pharmacotherapy
• Nospecifictreatment• Symptommodification,treatco-morbidities
– Depression,othermooddisorders– ADHD,angerdyscontrol– Substanceabuse– Otheranxietydisorders
Page 80
CareofCaretakers
• Beawarethatcaretakers(includingofficestaff,nurses,doctors)oftenhavetheirowntraumahistories
• BereadytoapplyPFAtoresponders,coworkersandcolleaguesinadditiontoparents
• Bepreparedwithreferraloptions.• Modelproblemfocusedbehaviorandemotionalregulation.
• Helpparentssetclearboundariesforthemselvesandtheirchildren.
Page 81
RelationalHome
Developmentaltraumaoccurswhen“emotionalpaincannotfindarelationalhomeinwhichitcanbeheld.”
-RobertStolorow.TraumaandHumanExistence.(2007)
WikimediaCommons.commons.wikimedia.org
Page 82
Question#1TheNationalSurveyofChildrenExposuretoViolence(NatSCEV)surveyedover4,500childrenandadolescentsbyanonymoustelephoneinterviews.Thesurveyrevealedwhatpercentofchildrenwereexposedtoviolenceinthepreviousyear?
A. Lessthan50%B. AboutathirdC. Morethan60%D. Nearly90%
Epidemiology
Page 83
Question#2TheNatSCEV concludedthatchildrenintheUSaremorelikelytobeexposedtoviolencethanadults.Whichgroupismostlikelytoexperienceexposuretoassaultwithaweapon?
A. LateAdolescenceB. MiddleChildhoodC. ToddlersD. PreteensandEarlyAdolescence
Epidemiology
Page 84
Question#3Whichofthefollowingstatementsdescribesexposuretocommunityviolenceaccordingtogender,ageortimeframe?
A. Childrenexposedtoonetypeofviolenceareatfargreaterriskofexperiencingothertypesofviolence.
B. Boysandgirlsareequallylikelytowitnesscommunityviolence.
C. Reportsoflifetimeexposureweregenerallythesameasreportsofexposureduringthepreviousyear.
D. Lessthan10%of14to17yearsoldsreportwitnessingashootingovertheirlifetime.
Epidemiology
Page 85
Question#4Thepatternsofexposurechangeoverchildhoodandadolescence.Whichofthefollowingstatementsdescribestherisksofexposurebyagegroup?
A. Olderadolescentsareleastlikelytoexperiencemoresevereformsofviolence.
B. Kidnappingisathighestriskformiddleadolescents.C. Thereisa25-foldincreaseinratesofwitnessing
communityviolencefromtoddlerstoolderadolescents.
D. Preteensandearlyadolescents(10to13)aremostlikelytobeassaultedwithaweapon.
Epidemiology
Page 86
Question#5Intheimmediatewakeofacrisis,whiletriagingorexaminingchildren,pediatriciansmayengagewhichofthefollowingstrategiestominimizeexposurebychildrentorepeattrauma?
A. TurnoffTVsinwaitingarea.B. Keepcurtainsopenintriageandtreatmentareas.C. Makesurestaffmaintainopencommunicationwith
familiesaboutmediareportsasithappens.D. Physiciansandotherpediatricprovidersshouldbe
encouragedtoopenlyexpresstheirdistressasajoiningprocedurewithfamilies.
MediaExposure
Page 87
Question#6Whichofthefollowingismostlikelytobeincludedinanticipatoryguidanceforparentsaboutthemostcommonreactionsbychildrenafteranepisodeofmassviolenceordisaster?
A. Advisethatchildrenshouldbeallowedtosettheirownroutine.
B. Counselthatchildrenmayhavetroublefallingasleeporwakingwithnightmares.
C. Makesurethattheyarewatchingtelevisionaccountssotheyhavealltheinformation.
D. Askthemtonottalkabouteithertheeventortheirfeelingsabouttheevent.
GuidanceforParents
Page 88
Question#7Whichofthefollowingincreasestheriskofadjustmentproblemsafteracrisis?
A. Preexistinglosses,traumaorattachmentdisturbances
B. ImmediatereunificationwithparentsC. SupportivefamilycommunicationstyleD. Strongconnectionwithcommunitysupport
systems
EarlyIdentification
Page 89
Question#8PsychologicalFirstAid(PFA)isaninterventionfirstappliedinschoolsbutitusefulforothercommunitymembers,includingstaffofpediatricpractices.WhichofthefollowingisaPFAstrategy?
A. Offerreassuranceeveniffalse.B. Listen,ProtectandConnectC. Isolatefamiliesformnon-involvedfamily
membersinordertolimitfurthertrauma.D. RACE(rescue,alarm,contain,extinguish).E. Suicide
CommunityResponse
Page 90
Question#9Expandedmediacoverageofmassviolencehasledtoalargerpopulationatriskforbothprimaryandsecondaryexposure. Whichofthefollowingmaybeanticipatoryguidanceforparentsfollowingacatastrophicevent?
A. Parentsshouldnotlimitexposuretomediacoverage.B. Olderchildrenshouldfollowreportsonsocialmedia.C. Makesurechildrenviewthetraumaticeventin
graphicdetailsotherealitywillsinkin.D. Turnoffmediaifnofurtherunderstandingcanbe
gained.
AnticipatoryGuidance
Page 91
Question#10Whenelicitingtraumasymptoms,pediatricianscansupportfamiliesbywhichofthefollowing?
A. Openlyexpressanger,frustrationandgrief.B. Encourageproblem-solvingbuildingon
familystrengths.C. Avoiddirectdiscussionofevents.D. Informfamiliesthattheyarepowerlessand
nothingcanhelpthemnow.
PediatricianSupport
Page 92
Question#11TraumarelatedsymptomsareexpectedphysiologicresponsesoftheHPAaxisandimmunesystemandmaybemisinterpretedbyfamilies.Whichofthefollowingdescribesatraumarelatedphysiologicresponse?
A. Excessivesleepcausedbyreticularactivatingsystemactivation
B. Increasedordecreasedappetiteresultingfromanxietyanddysregulationofthesatietycenter
C. Increasedordecreasedappetiteresultingfromanxietyanddysregulationofthesatietycenter
D. Encopresisresultingfromdecreasedsympathetictone
ResponsetoExposure
Page 93
Question#12Behavioralresponsetotrauma,particularlyrecurrentevents,canbeeitherinternalizingorexternalizing.Whichofthefollowingdoesnotdescribethedistributionofbehavioralresponsesamongboysandgirls?
A. Dissociationandpsychicnumbingaremostcommoningirls.
B. Depressionisequallycommoningirlsandboys.C. Hyperactivityandaggressionaremorecommon
inboys.D. Anxietyismorecommoninboys
ResponsetoExposure
Page 94
Question#13Exposuretoearlychildhoodtraumamayresultinunderdevelopmentofpartsofthebrainresponsibleforexecutivefunction.Whichofthefollowingisnotanactivityoftheprefrontalcortexthatmightaffectschoolperformance?
A. Attention,concentrationB. WorkingmemoryC. ImpulsecontrolD. Flight/Fight/FreezereactionE. Recenttraumaorstress
ResponsetoExposure
Page 95
Question#14Becausetraumaissocommon,formalscreeningathealthsupervisionvisitsmaybereasonable. Whichofthefollowingisanappropriateresponsetodisclosureoftrauma?
A. Trytoremainbusinesslike,revealingnoemotion.
B. Exploreothersymptomsandotherexposures.C. Recordtheresultsofachecklist,thenmoveon.D. Telltheparentsthattheyhavefailedto
adequatelyprotecttheirchild.
ScreenforTraumaSymptoms
Page 96
Question#15Parentsmaybetraumatized,frustrated,confusedorangrybyeitheracatastrophiceventordisclosureoftraumabytheirchild. Whichofthefollowingisanappropriatetwo-generationalapproachtocare?
A. Telltheparentsthatyoudon’thavetimetoheartheparent’sproblems.
B. Helpparentsidentifyownsupportsystemandfamilystrengths.
C. Advisethatthechildrenshouldeatontheirownschedule.
D. Encourageparentstostepupandsolveproblemsontheirown.
ParentalExposure
Page 97
Question#16Parentsmayhavetheirowntraumahistory.Whichofthefollowingfailsasanappropriateresponsebyapediatricianwhenaparentdisclosestrauma?
A. Bepreparedwithreferraloptions.B. Modelproblemfocusedbehaviorandemotional
regulation.C. Tellthemthatyouarethechild'sdoctorand
theirproblemsarenotrelevant.D. Helpparentssetclearboundariesfor
themselvesandtheirchildren.
ParentalExposure
Page 98
Question#17Whentoreferandtowhomisoftenadifficultquestionforpediatricianswhenassessingchildrenexposedtotrauma.Whichifthefollowingisacorrectstatementaboutassessmentandtreatment?
A. Pre-existingemotionalproblemsarenotsignificantpredictorsforpooroutcomes.
B. Youngerchildrenarehelpedbyatwo-generationalapproachsuchasParent-ChildInteractionTherapy(PCIT).
C. Theintensityofadversityisnotcorrelatedwithseriousorenduringemotionalandphysiologicdisturbance.
D. Themosteffectiveevidence-basedtreatment(EBT)forchildrenyoungerthan5yearsisTraumaFocusedCognitiveBehavioralTherapy.
Evidence-basedTherapies
Page 99
Question#18Resiliencecanbeconsideredacapacity,outcomeorprocess.Whatisthesinglemostimportantfindingthatisassociatedwithchildrendoingwelldespiteserioushardship?
A. GeneticfactorsinfluencingtemperamentB. Thepresenceofonestable,committed
relationshipwithasupportiveadultC. Familysocio-economicstatusD. Frequentseparationsduringearlychildhood
Resillience
Page 100
Question#19Whichofthefollowingisakeycapacityorskillsetthatenableschildrentorespondsuccessfullytoadversity?
A. Abilitytomulti-taskB. Capacitytoplan,monitorandregulate
emotionalresponsesC. InsistenceonpredictabilityD. Establishmentofexternallocusofcontrolto
blameforadversity
Resillience
Page 101
Question#20Resilienceresultsfromaninteractionbetweeninternalpredispositionsandexternalexperiences.Whichphrasebestdescribesthedevelopmentofresilience?
A. Beingafavoredchild,firstinasib-shipB. Interactionofsupportiverelationships,gene
expressionandadaptivebiologicsystemsC. Solelyafunctionofpersonalfactors,commonly
knownas“grit”D. Interactionofzipcodeatbirthandparental
ethnicity
Resillience
Page 102
Question#21Resiliencecanbestrengthenedatanyage.Whichofthefollowingisatruestatementaboutinterventionsthatmaystrengthenthecapacitytobouncebackafteradversity?
A. Alternativeandcomplimentaryinterventionssuchasmindfulnesspracticeandyogaareineffective
B. Physicalexerciseisofnoimportanceintheexpressionofstressrelatedinflammatoryfactors
C. Activeskillbuildingprogramsforyoungadultsmayimproveexecutivefunctionsandcognitiveflexibility
D. Improvingparentalresiliencehasnoeffectonthechildren
Resillience
Page 103
Question#22Inadditiontotheavailabilityofatleastonestablerelationship,factorsthatpredisposechildrentopositiveoutcomesdespitesignificantadversityincludewhichofthefollowing?
A. QuickandstrongemotionalreactionsB. Exposuretoparentalsubstanceabuseormental
illnessC. Identificationwithanaffirmingfaithorcultural
traditionD. Protectionbyfamilyfromexposuretostress
Resillience
Page 104
Question#23Traumainformedcare(TIC)inamedicalsettingimpliesfullintegrationofknowledgeabouttraumaintopolicies,procedureandpractices,seekingtoresistre-traumatization.Whichofthefollowingstatementsdoesnotdescribetraumainformedcare?
A. Recognitionofhowtraumamayaffectpatients,families,staffandproviders.
B. Abilityofofficestafftomanagefracturesaswellasapplysplintsandcasts
C. Integrationofknowledgeoftraumaintopolicies,proceduresandpracticesforhealthcaredelivery
D. Activeresistanceagainstfurthertraumatochildrenorfamiliesinvolvedinthehealthsystem
Trauma-InformedCare
Page 105
Question#24Medicaltraumaticstressreferstoemotionalreactionstoinjury,illnessortreatmentinbothpatientsandfamilies.Whatisonewaythatapediatricpracticemightdecreasetheeffectofpotentiallytraumaticevent?
A. Trainonlyphysiciansinpsychologicalfirstaid(PFA).B. Ignorethelevelofdistress,maintainstandardizedtreatmentC. Keeptheparentsinaseparateareaduringpossiblepainful
proceduresD. AdopttheDEFprotocol(reduceDistress,Emotionalsupportand
remembertheFamily)E. Therewasnostatisticallysignificantdifferencebetweenthose
patientstreatedwithCBTalone,fluoxetinealoneandCBT+fluoxetine
Trauma-InformedCare
Page 106
Question#25Familycenteredcareandtraumainformedcareoverlapinwhatways?
A. Physicianleadershipassumescontroloveralldecisions
B. Communicationlimitedtowhatisnecessarytogetthejobdone
C. Involvementoffamiliesindecisionsandemphasisoncollaborationofcare
D. Providerself-careisirrelevant
Trauma-InformedCare
Page 107
ReferencesforTrauma-InformedCare• Workingwithchildrenandfamiliesexperiencingmedicaltraumaticstress.CenterforPediatricTraumaticStress.(2015)https://www.healthcaretoolbox.org/images/TherapistResourceGuide.pdf
• SAMHSA’s ConceptofTraumaandGuidanceforaTrauma-InformedApproach.(2014)http://store.samhsa.gov/shin/content/SMA14-4884/SMA14-4884.pdf
• KeyIngredientsforSuccessfulTrauma-InformedCareImplementation.CenterforHealthcareStrategies.(2016)http://www.chcs.org/media/ATC_whitepaper_040616.pdf
Page 108
ReferencesforTrauma-InformedCare
• Machtinger EL,etal.FromTreatmenttoHealing:ThePromiseofTrauma-InformedPrimaryCare.Women’sHealthIssues.2015;25(3):193-197
• Marsac ML,etal.ImplementingaTrauma-InformedApproachinPediatricHealthCareNetworks.JAMAPediatrics.2016;170(1):70-77
• OralR,etal.Adversechildhoodexperiencesandtraumainformedcare:thefutureofhealthcare.PediatricResearch.2016;79(1):227-233
Page 109
PrincipleMOCReferences1. DowdMD(ed).TheMedicalHomeApproachtoIdentifyingandRespondingtoExposureto
Trauma.In:TheTraumaToolboxforPrimaryCare.AmericanAcademyofPediatrics.(2014)https://www.aap.org/en-us/Documents/ttb_medicalhomeapproach.pdfAccessed03/04/2016
2. Finkelhor D,TurnerH,Ormrod R,HambySandKracke K.Children’sExposuretoViolence:AComprehensiveNationalSurvey.(2009).U.S.DepartmentofJustice,OfficeofJuvenileJusticeandDeliquency Prevention.https://www.ncjrs.gov/pdffiles1/ojjdp/227744.pdfAccessed03/04/2016
3. Marsac ML,Kassam-AdamsN,Hildenbrand AK,etal.ImplementingaTrauma-InformedApproachinPediatricHealthCareNetworks.JAMAPediatr.2016;170(1):70-77
4. NationalScientificCouncilontheDevelopingChild.(2015).SupportiveRelationshipsandActiveSkill-BuildingStrengthentheFoundationsofResilience:WorkingPaper13.
http://www.developingchild.harvard.eduAccessed03/04/2016
5. Schonfeld DJ,Demaria T,theDisasterPreparednessAdvisoryCouncilandCommitteeonPsychosocialAspectsofChildandFamilyHealth.ProvidingPsychosocialSupporttoChildrenandFamiliesintheAftermathofDisastersandCrises.Pediatrics.2015;136(4):e1120-e1130