Expression of TGF, matrix metalloproteinases, and tissue inhibitors in Chinese chronic rhinosinusitis Xiaoyuan Li, MD, a * Juan Meng, MD, a * Xiaoming Qiao, MD, a Yafeng Liu, MD, a Feng Liu, MD, a Nan Zhang, MD, PhD, c Jie Zhang, MBBS, b Gabriele Holtappels, MBBS, c Ba Luo, MD, a Peng Zhou, MD, a Yongbo Zheng, MD, a Ping Lin, PhD, b Shixi Liu, MD, PhD, a and Claus Bachert, MD, PhD c Chengdu, China, and Ghent, Belgium Background: To date there is no information on the expression of mediators associated with tissue remodeling in Asian patients with chronic rhinitis with (CRSwNP) or without (CRSsNP) nasal polyps. Objectives: To study the expression of TGF-b1, matrix metalloproteinases (MMPs), tissue inhibitors of metalloproteinases (TIMPs), collagen, and regulatory T cells in Chinese patients with CRSwNP and CRSsNP. Methods: Thirty-six male and female subjects (12 patients with CRSwNP, 12 patients with CRSsNP, and 12 control subjects), age 17 to 60 years, were recruited into the study. Samples were collected from polyp and sinusoidal mucosal, ethmoidal mucosal, or inferior turbinate in the respective groups and assessed for TGF- b1, MMP-2, MMP-7, MMP-9, TIMP-1, TIMP-2, TIMP-3, and TIMP-4 by immunoassay; collagen by histochemistry; and forkhead box P3 (FOXP3) mRNA by real-time PCR. Results: Patients with CRSwNP showed significantly lower concentrations of TGF-b1, TIMP-1, TIMP-4, FOXP3, and collagen compared with patients with CRSsNP. Although there were no significant differences between the concentrations of MMP-7 and MMP-9 in patients with CRSwNP and CRSsNP, these were significantly increased compared with control patients. MMP-2 and TIMP-2 concentrations were not significantly different in any patient group, whereas TIMP-3 was not detectable. Conclusion: Chronic rhinosinusitis with nasal polyps is characterized by a relative lack of TGF-ß expression versus CRSsNP. This finding may be causal for decreased collagen, TIMP-1/4, and FOXP3 expression in CRSwNP versus CRSsNP. TGF-ß serves as a main switch for different remodeling patterns in sinus disease. (J Allergy Clin Immunol 2010;125:1061-8.) Key words: Chinese patients, chronic rhinosinusitis, collagen, fork- head box P3 (FOXP3), matrix metalloproteinase, nasal polyposis, regulatory T cells, tissue remodeling, TGF-b1, tissue inhibitor of metalloproteinase Chronic rhinosinusitis (CRS) is a heterogeneous group of sinus diseases that affect up to 15% of the population and impose a significantly increasing socioeconomic burden. 1-3 CRS is charac- terized by persistent inflammation of the nasal and paranasal mucosa 2 and is currently classified into 2 subgroups on the basis of the absence (CRSsNP) or presence (CRSwNP) of nasal polyps, with distinctive inflammatory cell and mediator profiles. 3-6 Evidence suggests that there may also be differences between the 2 subtypes with regard to certain features of remod- eling, such as basement membrane thickening, squamous meta- plasia, collagen deposition, and goblet cell and glandular hyperplasia. 7,8 Studies predominantly in Caucasian patients have demon- strated that CRSwNP is characterized by a T H 2-skewed eosino- philic inflammation made up of significantly higher levels of IL-5, IL-13, eotaxin, and eosinophil cationic protein (ECP) com- pared with CRSsNP, which is characterized by a T H 1 milieu made up of significantly higher levels of IFN-g and TGF-b. 3-6 There is some evidence that there may be differences in the inflammatory profiles of white and Asian patients with CRSwNP. Zhang et al 9 compared nasal mucosal tissue from Belgian and southern Chi- nese patients with CRSwNP and their healthy control counter- parts. The authors demonstrated that although the tissue samples from the Belgian patients were characterized by eosino- philic inflammation (eosinophil cationic protein/myeloperoxi- dase ratio > 2) and a significant increase in T H 2 cytokine and related marker levels, the samples from the Chinese patients were biased toward neutrophilic inflammation (eosinophil cati- onic protein/myeloperoxidase ratio 5 0.25) and a significant in- crease in T H 1/T H 17 cell pattern. 9 In another study, these authors demonstrated that nasal polyps from Chinese patients were char- acterized by significantly lower EG2 1 eosinophils compared with nasal polyps from white subjects. 10 In contrast with the inflamma- tory pathways in Chinese patients, remodeling patterns have not been well studied yet in those patients; remodeling pattern also may be dissociated from inflammatory mechanisms. Despite these differences, a common finding of studies inves- tigating mediators associated with tissue remodeling in patients with CRSwNP versus patients with CRSsNP and/or control subjects has been that the levels of TGF-b1 were significantly lower in the patients with CRSwNP, irrespective of race. 3,8,11 In- deed, studies investigating expression of TGF-b1 in nasal tissues From a the Department of Oto-Rhino-Laryngology, West China Medical School, and b the Upper Airway Research Laboratory, West China Hospital, Sichuan University; and c the Upper Airway Research Laboratory, Department of Oto-Rhino-Laryngology, Ghent University Hospital. *These authors contributed equally to this work. Supported by the Program of Science and Technology Foundation of Sichuan Province (grant no. 2009HH0027) and the National Natural Science Foundation of China (grant no. 30973291) to Shixi Liu, by a collaboration between Ghent University and Sichuan University, and by the Interuniversity Attraction Poles Programme - Belgian State -29 Belgian Science Policy, Nr. IAP P6/35. Disclosure of potential conflict of interest: The authors have declared that they have no conflict of interest. Received for publication September 23, 2009; revised January 8, 2010; accepted for pub- lication February 18, 2010. Available online April 15, 2010. Reprint requests: Shixi Liu, MD, PhD, Department of Oto-Rhino-Laryngology, West China Hospital, West China Medical School, Sichuan University, No. 37 Guo Xue Al- ley, Chengdu, Sichuan, 610041, PR China. E-mail: [email protected]. Ping Lin, PhD, Upper Airway Research Laboratory, West China Hospital, Sichuan University, 1 Keyuan 4 Road, Gaopeng Avenue, Hi-tech Development Zone, Chengdu, Sichuan, 610041, PR China. E-mail: [email protected]. 0091-6749/$36.00 Ó 2010 American Academy of Allergy, Asthma & Immunology doi:10.1016/j.jaci.2010.02.023 1061
Transcript
Expression of TGF, matrix metalloproteinases, and tissueinhibitors in Chinese chronic rhinosinusitis
Xiaoyuan Li, MD,a* Juan Meng, MD,a* Xiaoming Qiao, MD,a Yafeng Liu, MD,a Feng Liu, MD,a Nan Zhang, MD, PhD,c
Jie Zhang, MBBS,b Gabriele Holtappels, MBBS,c Ba Luo, MD,a Peng Zhou, MD,a Yongbo Zheng, MD,a Ping Lin, PhD,b
Shixi Liu, MD, PhD,a and Claus Bachert, MD, PhDc Chengdu, China, and Ghent, Belgium
Background: To date there is no information on the expressionof mediators associated with tissue remodeling in Asian patientswith chronic rhinitis with (CRSwNP) or without (CRSsNP)nasal polyps.Objectives: To study the expression of TGF-b1, matrixmetalloproteinases (MMPs), tissue inhibitors ofmetalloproteinases (TIMPs), collagen, and regulatory T cells inChinese patients with CRSwNP and CRSsNP.Methods: Thirty-six male and female subjects (12 patients withCRSwNP, 12 patients with CRSsNP, and 12 control subjects),age 17 to 60 years, were recruited into the study. Samples werecollected from polyp and sinusoidal mucosal, ethmoidal mucosal,or inferior turbinate in the respective groups and assessed forTGF- b1, MMP-2, MMP-7, MMP-9, TIMP-1, TIMP-2, TIMP-3,and TIMP-4 by immunoassay; collagen by histochemistry; andforkhead box P3 (FOXP3) mRNA by real-time PCR.Results: Patients with CRSwNP showed significantly lowerconcentrations of TGF-b1, TIMP-1, TIMP-4, FOXP3, andcollagen compared with patients with CRSsNP. Although therewere no significant differences between the concentrations ofMMP-7 and MMP-9 in patients with CRSwNP and CRSsNP,these were significantly increased compared with controlpatients. MMP-2 and TIMP-2 concentrations were notsignificantly different in any patient group, whereas TIMP-3was not detectable.Conclusion: Chronic rhinosinusitis with nasal polyps ischaracterized by a relative lack of TGF-ß expression versusCRSsNP. This finding may be causal for decreased collagen,TIMP-1/4, and FOXP3 expression in CRSwNP versus CRSsNP.
From athe Department of Oto-Rhino-Laryngology, West China Medical School, and bthe
Upper Airway Research Laboratory, West China Hospital, Sichuan University; andcthe Upper Airway Research Laboratory, Department of Oto-Rhino-Laryngology,
Ghent University Hospital.
*These authors contributed equally to this work.
Supported by the Program of Science and Technology Foundation of Sichuan Province
(grant no. 2009HH0027) and the National Natural Science Foundation of China
(grant no. 30973291) to Shixi Liu, by a collaboration between Ghent University and
Sichuan University, and by the Interuniversity Attraction Poles Programme - Belgian
State -29 Belgian Science Policy, Nr. IAP P6/35.
Disclosure of potential conflict of interest: The authors have declared that they have no
conflict of interest.
Received for publication September 23, 2009; revised January 8, 2010; accepted for pub-
lication February 18, 2010.
Available online April 15, 2010.
Reprint requests: Shixi Liu, MD, PhD, Department of Oto-Rhino-Laryngology, West
China Hospital, West China Medical School, Sichuan University, No. 37 Guo Xue Al-
Chronic rhinosinusitis (CRS) is a heterogeneous group of sinusdiseases that affect up to 15% of the population and impose asignificantly increasing socioeconomic burden.1-3 CRS is charac-terized by persistent inflammation of the nasal and paranasalmucosa2 and is currently classified into 2 subgroups on the basisof the absence (CRSsNP) or presence (CRSwNP) of nasalpolyps, with distinctive inflammatory cell and mediatorprofiles.3-6 Evidence suggests that there may also be differencesbetween the 2 subtypes with regard to certain features of remod-eling, such as basement membrane thickening, squamous meta-plasia, collagen deposition, and goblet cell and glandularhyperplasia.7,8
Studies predominantly in Caucasian patients have demon-strated that CRSwNP is characterized by a TH2-skewed eosino-philic inflammation made up of significantly higher levels ofIL-5, IL-13, eotaxin, and eosinophil cationic protein (ECP) com-pared with CRSsNP, which is characterized by a TH1 milieu madeup of significantly higher levels of IFN-g and TGF-b.3-6 There issome evidence that there may be differences in the inflammatoryprofiles of white and Asian patients with CRSwNP. Zhang et al9
compared nasal mucosal tissue from Belgian and southern Chi-nese patients with CRSwNP and their healthy control counter-parts. The authors demonstrated that although the tissuesamples from the Belgian patients were characterized by eosino-philic inflammation (eosinophil cationic protein/myeloperoxi-dase ratio > 2) and a significant increase in TH2 cytokine andrelated marker levels, the samples from the Chinese patientswere biased toward neutrophilic inflammation (eosinophil cati-onic protein/myeloperoxidase ratio 5 0.25) and a significant in-crease in TH1/TH17 cell pattern.9 In another study, these authorsdemonstrated that nasal polyps from Chinese patients were char-acterized by significantly lower EG21 eosinophils compared withnasal polyps from white subjects.10 In contrast with the inflamma-tory pathways in Chinese patients, remodeling patterns have notbeen well studied yet in those patients; remodeling pattern alsomay be dissociated from inflammatory mechanisms.
Despite these differences, a common finding of studies inves-tigating mediators associated with tissue remodeling in patientswith CRSwNP versus patients with CRSsNP and/or controlsubjects has been that the levels of TGF-b1 were significantlylower in the patients with CRSwNP, irrespective of race.3,8,11 In-deed, studies investigating expression of TGF-b1 in nasal tissues
of CRSsNP and nasal polyposis tissues of patients with CRSwNPhave also demonstrated that patients with CRSwNP have signif-icantly lower levels of TGF-b1,4,12 suggesting that this mediatoris likely to play an important role in the etiology of CRSsNP andCRSwNP. Similarly, several studies have indicated that there mayalso be significant differences between patients with CRSsNP andCRSwNP with respect to the nasal expression of specific extracel-lular matrix (ECM)–degrading matrix metalloproteinases(MMPs) and the tissue inhibitors of metalloproteinases(TIMPs),13-16 which play an integral role in tissue remodeling.Collectively, the findings of differences in these mediators couldpotentially explain any specific histologic changes noted in pa-tients with CRSsNP versus CRSwNP.
To date, no study has investigated differences in the expressionof the MMPs and TIMPs in Chinese patients with CRSwNP andCRSsNP. Because TGF-b is thought to play a role in airwayremodeling by modulating ECM production and activity of ECM-degrading proteases, the main objective of this study was there-fore to investigate any differences in the expression of TGF-b1,MMP-2, MMP-7, and MMP-9 as well as TIMP-1, TIMP-2,TIMP-3, and TIMP-4 in nasal tissues of patients with CRSwNPand CRSsNP. Differences in the expression of collagen andforkhead box P3 (FOXP3), a marker of activated regulatoryT (Treg) cells, were investigated as a secondary objective.
METHODS
Patients and study designA total of 36 subjects (25 male and 11 female; 12 patients with CRSsNP, 12
patients with CRSwNP, and 12 control subjects), age 17 to 60 years, presenting
for routine functional endonasal sinus surgery at the Department of Oto-Rhino-
Laryngology, West China Hospital, were recruited into the study between
April 2008 and January 2009. At screening, diagnosis of sinus disease was
based on history, clinical examination, nasal endoscopy, and computed
tomography (CT) scan of the sinuses according to the EP3OS (European Po-
sition Paper on Rhinosinusitis and Nasal Polyps 2007) guidelines.17 CT scans
were graded according to Lund-Mackay.18 The atopic status of each patient
was evaluated by skin prick tests to common inhalant allergens, and patients
were diagnosed for asthma. All patients were asked to stop taking oral cortico-
steroids for at least 2 months and topical medication for at least 4 weeks before
surgery.
Before surgery, rhinosinusitis symptoms were evaluated by a physician on a
4-point scale of 0 to 3 (0, no symptoms; 1, mild symptoms; 2, moderate
symptoms; 3, severe symptoms), and polyps were graded by size and extent in
both the left and right nasal fossa on a scale of 0 to 3, according to the
classification by Davos.17 In the case of patients with CRSsNP, tissue samples
were taken from the ethmoidal mucosa, whereas in the case of patients with
CRSwNP, samples were taken from the nasal polyps. Inferior turbinate samples
from patients without sinus disease undergoing septoplasty or rhinoseptoplasty
because of anatomical variations were collected as controls. All samples were
snap-frozen in liquid nitrogen on collection and stored at –808C until further
assessment by immunoassay or real-time PCR. For histochemistry, nasal tissue
was fixed in 4% formalin and subsequently embedded in paraffin.
The study was approved by the local Ethical Committee on Human
Experimentation of West China Hospital, Chengdu, and informed written
consent was obtained from all patients before collecting any samples for
experimental purpose.
ImmunoassaySamples to be assessed by immunoassay were weighed. A total of 1.0 mL
0.9% NaCl was added per 0.1 g of each sample, and all samples were
homogenized at 1000 rpm for 5 minutes. In the case of samples to be assessed
for TGF-b1, all samples were additionally treated with a protease inhibitor
cocktail (Complete Roche, Mannheim, Germany) before homogenization. All
homogenates were centrifuged at 15003 for 10 minutes at 48C, after which the
supernatants were collected and stored at –808C until analysis. Samples were
assessed for MMP-2, MMP-7, MMP-9, TIMP-1, TIMP-2, TIMP-3, and
TIMP-4 by using Fluorokine MAP Multiplex Kits (R&D Systems, Minneap-
olis, Minn) and analyzed on a Luminex 100 analyzer (Luminex 100 System,
Austin, Tex), and TGF-b1 by using commercially available ELISA kits
The total symptom score is the sum of the score for nasal congestion, sneezing, rhinorrhea, loss of smell, and postnasal drip. The level of significance (P) was obtained by ANOVA.
NS, Not significant.
*Fisher exact test. P < .05 was considered statistically significant.
�Control vs CRSsNP.
�control vs CRSwNP.
§CRSsNP vs CRSwNP.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 5
LI ET AL 1063
medians, ranges, and interquartiles. Statistical analysis was performed by
using the Kruskal-Wallis test and the Mann-Whitney U 2-tailed test for un-
paired comparisons. For comparisons between groups, the Kruskal-Wallis
test was used to establish the significance of intergroup variability, and the
Mann-Whitney U test was then used for between-group comparisons. Baseline
variables were analyzed by using a 1-way ANOVA test or the Fisher exact test.
The significance level was set at an a value of 0.05.9
RESULTS
Patient characteristicsTable I shows the demographic and clinical characteristics of
the 3 groups of subjects enrolled in the study. The groups weresimilar with regard to demographic characteristics, but with sig-nificant differences in clinical symptom scores. Particularly, thetotal symptom score was significantly higher in patients withCRSwNP, with nasal congestion, rhinorrhea, and loss of smell be-ing the most predominant symptoms, compared with patients withCRSsNP and control subjects. Similarly, patients with CRSwNPalso had a significantly higher bilateral CT score than patientswith CRSsNP and control subjects.
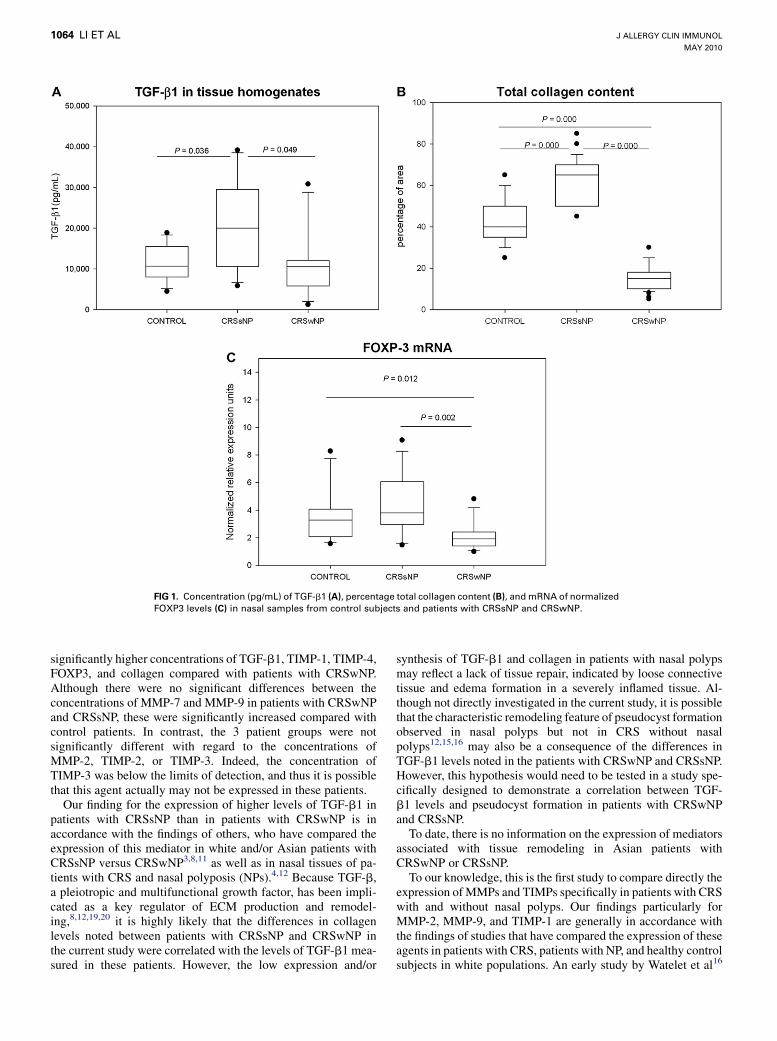
ImmunoassayAssessment of TGF-b1 concentrations demonstrated that these
were significantly higher in patients with CRSsNP compared withpatients with CRSwNP (P < .05) or control subjects (P < .05;Fig 1, A).
Matrix metalloproteinase 7 (P < .01) and MMP-9 (P < .05) con-centrations were found to be significantly increased in patientswith CRSwNP and CRSsNP compared with control subjectswithout significant difference between the CRS groups. In con-trast, there was no significant difference in MMP-2 concentrationsbetween any patient groups (Fig 2).
Assessment of TIMPs demonstrated that although TIMP-1 andTIMP-4 concentrations were significantly higher in patients withCRSsNP compared with patients with CRSwNP (P < .05), the
levels of these agents were not significantly different in eitherCRS group compared with control subjects (Fig 3). Similarly,there were no significant differences in TIMP-2 concentrationsbetween any patient groups. The expressions of TIMP-3 in allgroups were below the detection level of the Fluorokine Kit(Fig 3).
Picrosirius red stainings for collagenExamination of samples by polarized light microscopy dem-
onstrated the presence of larger collagen fibers, as indicated bybright orange luminescence, predominantly in patients withCRSsNP and to a lesser extent in control subjects, but not inpatients with CRSwNP (Fig 4). The absence of green lumines-cence under polarized light, however, indicated that thinner colla-gen fibers were not present in any of these patient groups.
The total collagen amount in the ECM was significantly higherin patients with CRSsNP (median, 64.2% of total area) andsignificantly lower in patients with CRSwNP (median, 14.8% oftotal area) compared with controls (median, 40% of total area;P < .001 respectively; Fig 1, B).
Real-time RT-PCRFig 1, C, shows the concentration of mRNA for FOXP3 deter-
mined in the 3 patient groups. The expression of FOXP3 wassignificantly downregulated in patients with CRSwNP comparedwith both patients with CRSsNP (P < .01) and control subjects(P < .05). These differences were independent of the atopicstatus.
DISCUSSIONOur study has demonstrated that there are significant differ-
ences in the synthesis/expression of TGF-b1, MMPs, TIMPs,FOXP3, and collagen in adult Chinese patients with CRSwNP andCRSsNP. In particular, patients with CRSsNP showed
FIG 1. Concentration (pg/mL) of TGF-b1 (A), percentage total collagen content (B), and mRNA of normalized
FOXP3 levels (C) in nasal samples from control subjects and patients with CRSsNP and CRSwNP.
J ALLERGY CLIN IMMUNOL
MAY 2010
1064 LI ET AL
significantly higher concentrations of TGF-b1, TIMP-1, TIMP-4,FOXP3, and collagen compared with patients with CRSwNP.Although there were no significant differences between theconcentrations of MMP-7 and MMP-9 in patients with CRSwNPand CRSsNP, these were significantly increased compared withcontrol patients. In contrast, the 3 patient groups were notsignificantly different with regard to the concentrations ofMMP-2, TIMP-2, or TIMP-3. Indeed, the concentration ofTIMP-3 was below the limits of detection, and thus it is possiblethat this agent actually may not be expressed in these patients.
Our finding for the expression of higher levels of TGF-b1 inpatients with CRSsNP than in patients with CRSwNP is inaccordance with the findings of others, who have compared theexpression of this mediator in white and/or Asian patients withCRSsNP versus CRSwNP3,8,11 as well as in nasal tissues of pa-tients with CRS and nasal polyposis (NPs).4,12 Because TGF-b,a pleiotropic and multifunctional growth factor, has been impli-cated as a key regulator of ECM production and remodel-ing,8,12,19,20 it is highly likely that the differences in collagenlevels noted between patients with CRSsNP and CRSwNP inthe current study were correlated with the levels of TGF-b1 mea-sured in these patients. However, the low expression and/or
synthesis of TGF-b1 and collagen in patients with nasal polypsmay reflect a lack of tissue repair, indicated by loose connectivetissue and edema formation in a severely inflamed tissue. Al-though not directly investigated in the current study, it is possiblethat the characteristic remodeling feature of pseudocyst formationobserved in nasal polyps but not in CRS without nasalpolyps12,15,16 may also be a consequence of the differences inTGF-b1 levels noted in the patients with CRSwNP and CRSsNP.However, this hypothesis would need to be tested in a study spe-cifically designed to demonstrate a correlation between TGF-b1 levels and pseudocyst formation in patients with CRSwNPand CRSsNP.
To date, there is no information on the expression of mediatorsassociated with tissue remodeling in Asian patients withCRSwNP or CRSsNP.
To our knowledge, this is the first study to compare directly theexpression of MMPs and TIMPs specifically in patients with CRSwith and without nasal polyps. Our findings particularly forMMP-2, MMP-9, and TIMP-1 are generally in accordance withthe findings of studies that have compared the expression of theseagents in patients with CRS, patients with NP, and healthy controlsubjects in white populations. An early study by Watelet et al16
FIG 2. Concentration (pg/mL) of MMP-2, MMP-7, and MMP-9 in nasal sam-
ples from control subjects and patients with CRSsNP and CRSwNP. FIG 3. Concentration (pg/mL) of TIMP-1, TIMP-2, and TIMP-4 in nasal
samples from control subjects and patients with CRSsNP and CRSwNP.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 5
LI ET AL 1065
investigated the synthesis of MMP-7, MMP-9, and TIMP-1 in na-sal samples from 3 groups of patients with NP, patients with CRS,and control subjects.16 These authors demonstrated that MMP-9was significantly increased in patients with NP and CRS com-pared with control subjects, whereas MMP-7 was significantly in-creased in patients with NP compared with controls only.Similarly, studies comparing protein expression of MMP-2 and/or MMP-9 in nasal samples from patients with NP versus control
subjects14,21 have demonstrated that MMP-9 but not MMP-2expression and/or activity was significantly increased in patientswith NP compared with control subjects. In contrast, 1 study in-vestigating the expression of MMP-2, MMP-7, MMP-9, andTIMP-1 in a group of patients with NP, patients with CRS, andcontrol subjects has demonstrated that whereas the expressionMMP-2 was significantly increased in NP, and MMP-7
FIG 4. Picrosirius red–stained sections of nasal tissue from control subjects and patients with CRSsNP and
CRSwNP assessed for total collagen by bright-field microscopy (A-C) and collagen fibers by polarized light
microscopy (D-F).
J ALLERGY CLIN IMMUNOL
MAY 2010
1066 LI ET AL
significantly increased in CRS, TIMP-1 was significantly in-creased in the control group compared with CRS and NP.13
It is likely that the discrepancies in the findings from thesestudies are a consequence of several factors, of which experi-mental/methodical differences between the studies, differencesin the control subjects studied,21 and absence or presence of eo-sinophilia in patients with nasal polyps9,15,22 are possibly themost important. However, despite these discrepancies, it is likelythat differences in the expression of specific MMPs and TIMPslead to specific differences in tissue remodeling in patientswith CRSsNP and CRSwNP. The findings for MMP-9 (gelatin-ase B), which preferentially degrades gelatin, elastin, aggrecan,and collagens, suggest that this enzyme is likely to be associatedwith airway remodeling in nasal polyposis,14-16,21,23 although itsprecise role in polyp and pseudocyst formation remainsunclear.16,21 Moreover, it is likely that the overall effect ofMMP-9 in polyp formation will be governed by the levels ofTIMP-1, which binds pro–MMP-9 and thus limits the activityof MMP-9.21 In contrast, the roles for MMP-2 and MMP-7 in re-modeling in CRSsNP and CRSwNP appear to be less clear.Indeed, Eisenberg et al14 have suggested that MMP-2 is of littlerelevance in patients with CRSwNP, whereas Can et al13 havesuggested that enhanced expression of MMP-2 in the nasal
mucosa leads to polyp formation and enhanced expression ofMMP-7 to manifestation of CRS without nasal polyps. Further-more, there is some evidence that MMP-224 and MMP-716 maystimulate the activity of MMP-9.
Because TIMPs are known to modulate the activity of MMPs,differences in the levels of these agents and the MMP/TIMPimbalance24 will probably reflect differences in tissue remodelingpatterns in patients with CRSsNP and CRSwNP. Our finding forthe presence of significantly lower concentrations of TIMP-1 inpatients with CRSwNP is clearly concordant with the high con-centrations of MMP found in patients with nasal polyps and in ac-cordance with the findings of others.13,21 Although there is anincreasing body of evidence for the expression and synthesis ofTIMP-1 in patients with CRS and NP, there is little or no such in-formation for TIMP-2, TIMP-3, or TIMP-4 in these conditions. Inthis regard, our study is also the first to investigate the expressionof these mediators in patients with CRS and nasal polyps. Ourfindings suggest that TIMP-4 may also play an integral role inthe etiology of nasal polyps, whereas the role of TIMP-2 is lessclear. In contrast, TIMP-3 is unlikely to be involved in theseconditions.
Our findings for the significantly decreased expression ofFOXP3 mRNA in patients with CRSwNP compared with patients
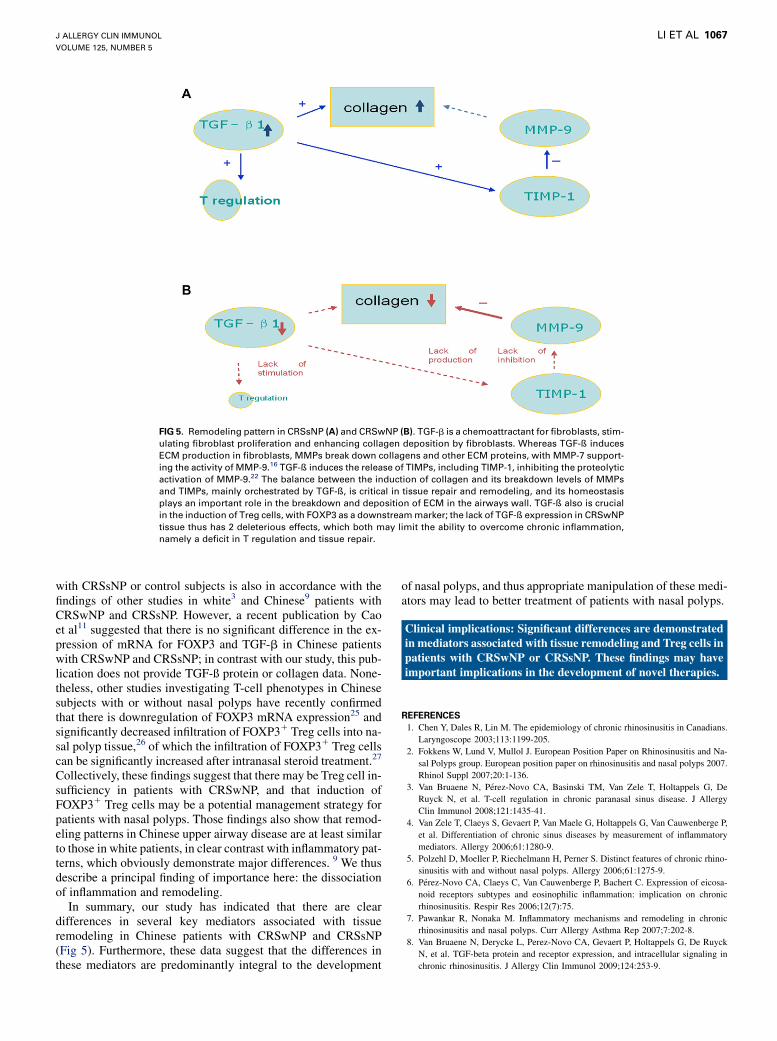
FIG 5. Remodeling pattern in CRSsNP (A) and CRSwNP (B). TGF-b is a chemoattractant for fibroblasts, stim-
ulating fibroblast proliferation and enhancing collagen deposition by fibroblasts. Whereas TGF-ß induces
ECM production in fibroblasts, MMPs break down collagens and other ECM proteins, with MMP-7 support-
ing the activity of MMP-9.16 TGF-ß induces the release of TIMPs, including TIMP-1, inhibiting the proteolytic
activation of MMP-9.22 The balance between the induction of collagen and its breakdown levels of MMPs
and TIMPs, mainly orchestrated by TGF-ß, is critical in tissue repair and remodeling, and its homeostasis
plays an important role in the breakdown and deposition of ECM in the airways wall. TGF-ß also is crucial
in the induction of Treg cells, with FOXP3 as a downstream marker; the lack of TGF-ß expression in CRSwNP
tissue thus has 2 deleterious effects, which both may limit the ability to overcome chronic inflammation,
namely a deficit in T regulation and tissue repair.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 5
LI ET AL 1067
with CRSsNP or control subjects is also in accordance with thefindings of other studies in white3 and Chinese9 patients withCRSwNP and CRSsNP. However, a recent publication by Caoet al11 suggested that there is no significant difference in the ex-pression of mRNA for FOXP3 and TGF-b in Chinese patientswith CRSwNP and CRSsNP; in contrast with our study, this pub-lication does not provide TGF-ß protein or collagen data. None-theless, other studies investigating T-cell phenotypes in Chinesesubjects with or without nasal polyps have recently confirmedthat there is downregulation of FOXP3 mRNA expression25 andsignificantly decreased infiltration of FOXP31 Treg cells into na-sal polyp tissue,26 of which the infiltration of FOXP31 Treg cellscan be significantly increased after intranasal steroid treatment.27
Collectively, these findings suggest that there may be Treg cell in-sufficiency in patients with CRSwNP, and that induction ofFOXP31 Treg cells may be a potential management strategy forpatients with nasal polyps. Those findings also show that remod-eling patterns in Chinese upper airway disease are at least similarto those in white patients, in clear contrast with inflammatory pat-terns, which obviously demonstrate major differences. 9 We thusdescribe a principal finding of importance here: the dissociationof inflammation and remodeling.
In summary, our study has indicated that there are cleardifferences in several key mediators associated with tissueremodeling in Chinese patients with CRSwNP and CRSsNP(Fig 5). Furthermore, these data suggest that the differences inthese mediators are predominantly integral to the development
of nasal polyps, and thus appropriate manipulation of these medi-ators may lead to better treatment of patients with nasal polyps.
Clinical implications: Significant differences are demonstratedin mediators associated with tissue remodeling and Treg cells inpatients with CRSwNP or CRSsNP. These findings may haveimportant implications in the development of novel therapies.
REFERENCES
1. Chen Y, Dales R, Lin M. The epidemiology of chronic rhinosinusitis in Canadians.
Laryngoscope 2003;113:1199-205.
2. Fokkens W, Lund V, Mullol J. European Position Paper on Rhinosinusitis and Na-
sal Polyps group. European position paper on rhinosinusitis and nasal polyps 2007.
Rhinol Suppl 2007;20:1-136.
3. Van Bruaene N, Perez-Novo CA, Basinski TM, Van Zele T, Holtappels G, De
Ruyck N, et al. T-cell regulation in chronic paranasal sinus disease. J Allergy
Clin Immunol 2008;121:1435-41.
4. Van Zele T, Claeys S, Gevaert P, Van Maele G, Holtappels G, Van Cauwenberge P,
et al. Differentiation of chronic sinus diseases by measurement of inflammatory
mediators. Allergy 2006;61:1280-9.
5. Polzehl D, Moeller P, Riechelmann H, Perner S. Distinct features of chronic rhino-
sinusitis with and without nasal polyps. Allergy 2006;61:1275-9.
6. Perez-Novo CA, Claeys C, Van Cauwenberge P, Bachert C. Expression of eicosa-
noid receptors subtypes and eosinophilic inflammation: implication on chronic
rhinosinusitis. Respir Res 2006;12(7):75.
7. Pawankar R, Nonaka M. Inflammatory mechanisms and remodeling in chronic
rhinosinusitis and nasal polyps. Curr Allergy Asthma Rep 2007;7:202-8.
8. Van Bruaene N, Derycke L, Perez-Novo CA, Gevaert P, Holtappels G, De Ruyck
N, et al. TGF-beta protein and receptor expression, and intracellular signaling in
10. Zhang N, Holtappels G, Claeys C, Huang G, van Cauwenberge P, Bachert C. Pat-
tern of inflammation and impact of Staphylococcus aureus enterotoxins in nasal
polyps from southern China. Am J Rhinol 2006;20:445-50.
11. Cao PP, Li HB, Wang BF, Wang SB, You XJ, Cui YH, et al. Distinct immunopath-
ologic characteristics of various types of chronic rhinosinusitis in adult Chinese.
J Allergy Clin Immunol 2009 Jun 19 [Epub ahead of print].
12. Watelet JB, Claeys C, Perez-Novo C, Gevaert P, Van Cauwenberge P, Bachert C.
Transforming growth factor beta1 in nasal remodeling: differences between
chronic rhinosinusitis and nasal polyposis. Am J Rhinol 2004;18:267-72.
13. Can IH, Ceylan K, Caydere M, Samim EE, Ustun H, Karasoy DS. The expression
of MMP-2, MMP-7, MMP-9, and TIMP-1 in chronic rhinosinusitis and nasal pol-
yposis. Otolaryngol Head Neck Surg 2008;139:211-5.
14. Eisenberg G, Pradillo J, Plaza G, Lizasoain I, Moro MA. Increased expression and
activity of MMP-9 in chronic rhinosinusitis with nasal polyposis. Acta Otorinolar-
ingol Esp 2008;59:444-7.
15. Kostamo K, Tervahartiala T, Sorsa T, Richardson M, Toskala E. Metalloproteinase
function in chronic rhinosinusitis with nasal polyposis. Laryngoscope 2007;117:
638-43.
16. Watelet JB, Bachert C, Claeys C, Van Cauwenberge P. Matrix metalloproteinases
MMP-7, MMP-9 and their tissue inhibitor TIMP-1: expression in chronic sinusitis
vs nasal polyposis. Allergy 2004;59:54-60.
17. Fokkens W, Lund V, Bachert C, Clement P, Helllings P, Holmstrom M, et al.
EAACI position paper on rhinosinusitis and nasal polyps executive summary.
Allergy 2005;60:583-601.
18. Lund VJ, Kennedy DW. Staging for rhinosinusitis. Otolaryngol Head Neck Surg
1997;117(suppl):S35-40.
19. Verrecchia F, Mauviel A. Transforming growth factor-beta and fibrosis. World
J Gastroenterol 2007;13:3056-62.
20. Verrecchia F, Mauviel A. Transforming growth factor-beta signaling through the
Smad pathway: role in extracellular matrix gene expression and regulation.
J Invest Dermatol 2002;118:211-5.
21. Kahveci OK, Derekoy FS. Yılmaz MD, Serteser M, Altuntas A. The role of MMP-
9 and TIMP-1 in nasal polyp formation. Swiss Med Wkly 2008;138:684-8.
22. Lee YM, Kim SS, Kim HA, Suh YJ, Lee SK, Nahm DH, et al. Eosinophil inflam-
mation of nasal polyp tissue: relationships with matrix metalloproteinases, tissue
inhibitor of metalloproteinase-1 and transforming growth factor-b1. J Korean
Med Sci 2003;18:97-102.
23. Lechapt-Zalcman E, Coste A, d’Ortho MP, Frisdal E, Harf A, Lafuma C, et al. In-
creased expression of matrix metalloproteinase-9 in nasal polyps. J Pathol 2001;
193:233-41.
24. Raffetto JD, Khalil RA. Matrix metalloproteinases and their inhibitors in vascular
remodeling and vascular disease. Biochem Pharmacol 2008;75:346-59.
25. Shi J, Fan Y, Xu R, Zuo K, Cheng L, Xu G, et al. Characterizing T-cell phenotypes
in nasal polyposis in Chinese patients. J Investig Allergol Clin Immunol 2009;19:
276-82.
26. Xu G, Xia J, Hua X, Zhou H, Yu C, Liu Z, et al. Activated mammalian target of
rapamycin is associated with T regulatory cell insufficiency in nasal polyps. Respir
Res 2009;10:13.
27. Li HB, Cai KM, Liu Z, Xia JH, Zhang Y, Xu R, et al. Foxp31 T regulatory cells
(Tregs) are increased in nasal polyps (NP) after treatment with intranasal steroid.
Clin Immunol 2008;129:394-400.
Correction
With regard to the June 2007 article entitled ‘‘Fluticasone furoate nasal spray: A single treatment option for the symptoms ofseasonal allergic rhinitis’’ (J Allergy Clin Immunol 2007;119:1430-7), in Table IV on page 1436, the sample size (n) for theplacebo group is incorrect. The number should be 148, rather than 48.