17
Extending life for women with HER2-positive MBC Andreas Makris Mount Vernon Hospital Middlesex, UK
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | walker-hearrell |
| View: | 218 times |
| Download: | 0 times |
Extending life for women with HER2-positive MBCAndreas MakrisMount Vernon HospitalMiddlesex, UK
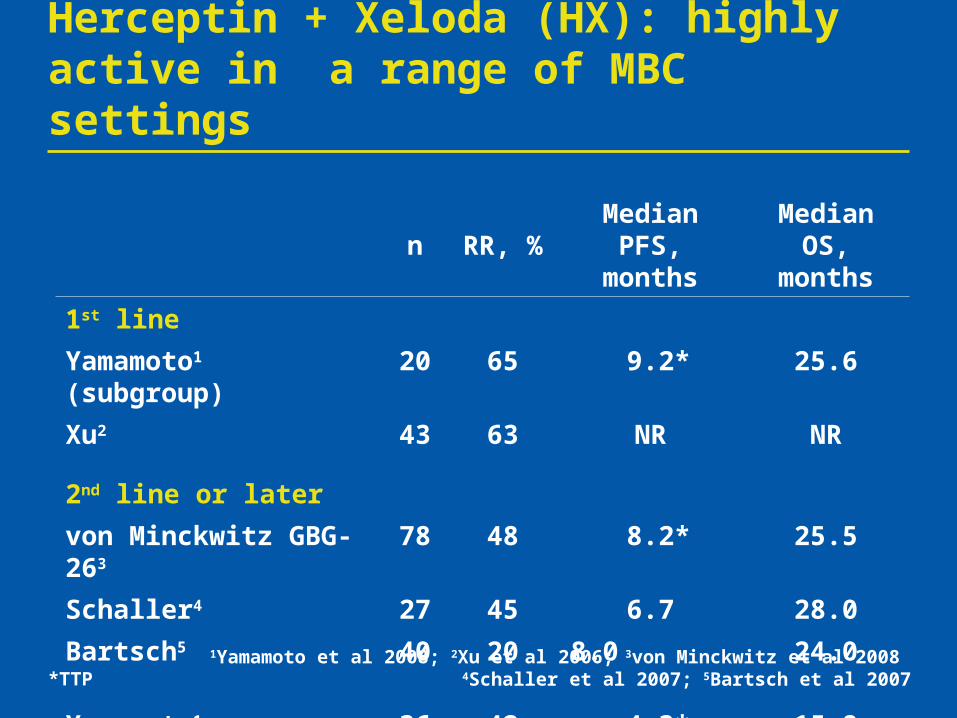
1Yamamoto et al 2008; 2Xu et al 2006; 3von Minckwitz et al 2008 4Schaller et al 2007; 5Bartsch et al 2007
Herceptin + Xeloda (HX): highly active in a range of MBC settings
n RR, %Median PFS,
monthsMedian OS,
months
1st line
Yamamoto1 (subgroup) 20 65 9.2* 25.6
Xu2 43 63 NR NR
2nd line or later
von Minckwitz GBG-263 78 48 8.2* 25.5
Schaller4 27 45 6.7 28.0
Bartsch5 40 20 8.0 24.0
Yamamoto1 (subgroup) 36 42 4.3* 15.8
*TTP

Can the efficacy of Herceptin-taxane regimens be further improved?
Rationale for adding Xeloda to HT
– adding Xeloda to docetaxel improves efficacy in patients unselected for HER2 status1
Could the addition of Xeloda have the same effect in HER2-positive disease?
1O’Shaughnessy et al 2002
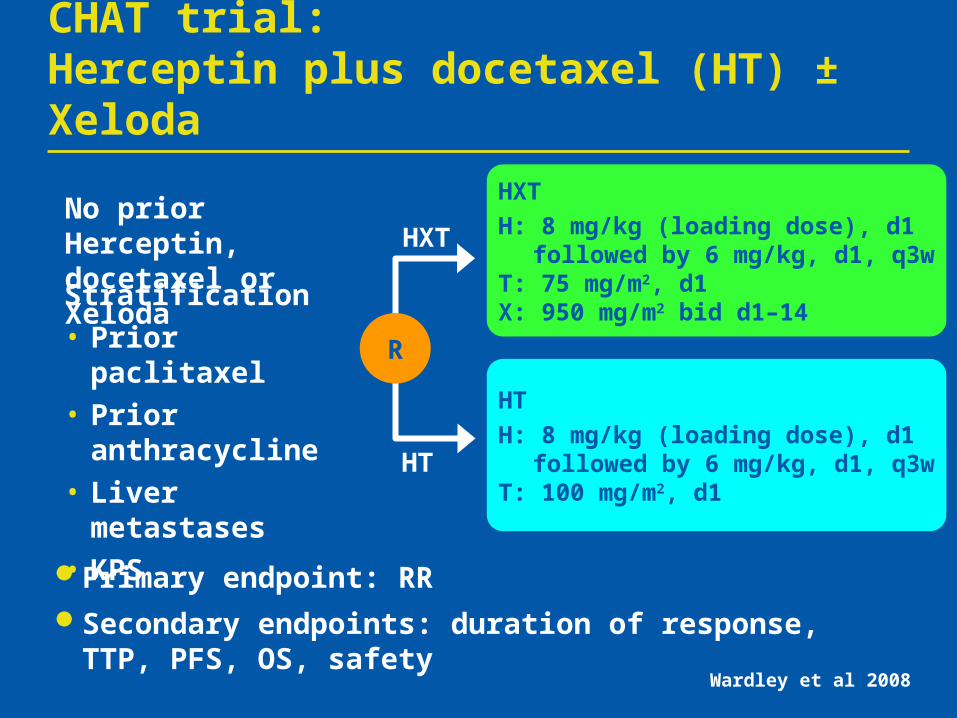
HXT
H: 8 mg/kg (loading dose), d1 followed by 6 mg/kg, d1, q3wT: 75 mg/m2, d1 X: 950 mg/m2 bid d1–14
CHAT trial: Herceptin plus docetaxel (HT) ± Xeloda
No prior Herceptin, docetaxel or Xeloda
Primary endpoint: RRSecondary endpoints: duration of response, TTP, PFS,
OS, safety
Stratification
• Prior paclitaxel
• Prior anthracycline
• Liver metastases
• KPS
R
Wardley et al 2008
HXT
HT
HT
H: 8 mg/kg (loading dose), d1followed by 6 mg/kg, d1, q3w
T: 100 mg/m2, d1

Case history: May 2003
44-year-old premenopausal woman
– married with one child
Cancer of the right breast
– invasive ductal carcinoma (IDC) grade II, 4 cm
– ER positive, PgR positive, HER2 positive (IHC 2+)
– staging CT scan and bone scan normal
– no comorbidities

Initial treatment
Neoadjuvant FEC x 6 (600/60/600)
– clinical PR after 2nd cycle
– radiological PR after 6th cycle
Wide local excision and axillary node dissection level II
– 22 mm, grade II, IDC, (4/9 nodes positive)
Radiotherapy and tamoxifen

Clinical course
September 2004: local relapse in breast, axillary nodes and multiple liver metastases
– CT scan: numerous large lesions within the right lobe of the liver consistent with metastases
– MRI scan: local breast relapse plus axillary relapse, multiple liver metastases
– LVEF 60%
– normal liver function tests

Relapse: September 2004
CT scanMultiple liver metastases
MRI scanRight breast multifocal relapse
MRI scanRight axillary relapse

Treatment choice
Patient consented to CHAT trial
Enrolled on 1 November 2004
– Xeloda/docetaxel stopped after six cycles
– continued Herceptin
Complete response in breast/axilla; PR in liver(CT scans)

Response in liver after enrolment in CHAT
6 months 20 months

CHAT: HXT significantly prolongs PFS versus HT
1.0
0.8
0.6
0.4
0.2
Estimated probability
0 5 10 15 20 25 30 35 40 45 50
Months
12.8 17.9
HR 95% CI p value
HXT 0.725 0.529, 0.99 0.0402HT
Wardley et al 2008
Summary of CHAT: consider first-line HXT
HXT is an effective first-line regimen for HER2-positive MBC
HXT significantly prolonged PFS versus HT
– median 5 months’ increase
High RR and good tolerability
Survival data immature

Right axilla relapse:31 months after entry into CHAT
May 2007
Relapse in the right axilla
Stable disease in the liver

Clinical course continuedAt relapse → Herceptin + pertuzumab trial Herceptin and pertuzumab:
– bind to different regions1
– inhibit signalling through different mechanisms1
– show preclinical synergy2
1Hubbard 20052Scheuer et al 2006
Herceptin
Pertuzumab

Clinical course continued
Response to Herceptin + pertuzumab
– after 3 months: PR in axilla; SD in liver; 1 cm lesion
– at 6 months: axillary nodes normal size; liver lesion unchanged
May 2008: clinically good response
Total length of Herceptin therapy: 3 years, 6 months

Response in axillary nodes, stable disease in liver
May 2007 July 2007 January 2008

Conclusions
Xeloda + Herceptin is effective in HER2-positive disease
– after Herceptin and chemotherapy
– first line alone
– first line with docetaxel
Herceptin + pertuzumab is an active therapy at disease progression

















