100
Eye Emergencies Eye Emergencies UNC Department of Emergency UNC Department of Emergency Medicine Medicine Nikki Waller Nikki Waller 2009-2010 2009-2010

Eye EmergenciesEye Emergencies
UNC Department of Emergency UNC Department of Emergency MedicineMedicine
Nikki WallerNikki Waller2009-20102009-2010

InfectionsInfections
Stye (External Hordeolum)Stye (External Hordeolum)– Infected oil gland at the lid marginInfected oil gland at the lid margin– Treatment: Treatment:
Warm compressesWarm compressesErythromycin ointment for 7-10 daysErythromycin ointment for 7-10 days

StyeStye

InfectionsInfections
Chalazion (Internal Hordeolum)Chalazion (Internal Hordeolum)– Infected meibomian gland (acute or chronic)Infected meibomian gland (acute or chronic)– Treatment: same as styeTreatment: same as stye
Warm CompressesWarm CompressesErythromycin ointment for 7-10 daysErythromycin ointment for 7-10 daysPLUS: Doxycycline for 14-21 days in refractory PLUS: Doxycycline for 14-21 days in refractory casescasesRefer to ophthalmology for persistent casesRefer to ophthalmology for persistent cases

ChalazionChalazion

ChalazionChalazion

InfectionsInfections
ConjunctivitisConjunctivitisBacterialBacterial– Eyelash matting, mucopurulent discharge, conjunctival Eyelash matting, mucopurulent discharge, conjunctival
inflammation (without corneal lesions)inflammation (without corneal lesions)– Treatment: topical antibioticsTreatment: topical antibiotics
Adults: Trimethoprim-polymixin B or erythromycin dropsAdults: Trimethoprim-polymixin B or erythromycin dropsInfants: Sulfacetamide 10%Infants: Sulfacetamide 10%
– Contact lens wearers: need to cover Contact lens wearers: need to cover PseudomonasPseudomonasCipro, ofloxacin, or tobramycin topical coverageCipro, ofloxacin, or tobramycin topical coverage

Bacterial ConjunctivitisBacterial Conjunctivitis

Bacterial ConjunctivitisBacterial Conjunctivitis

InfectionsInfections
ConjunctivitisConjunctivitisBacterialBacterial– If severe purulent discharge and hyperacute onset If severe purulent discharge and hyperacute onset
(12-24 hours), need prompt ophtho eval for work-up (12-24 hours), need prompt ophtho eval for work-up of of Gonococcal conjunctivitisGonococcal conjunctivitis

Gonococcal ConjunctivitisGonococcal Conjunctivitis
InfectionsInfections
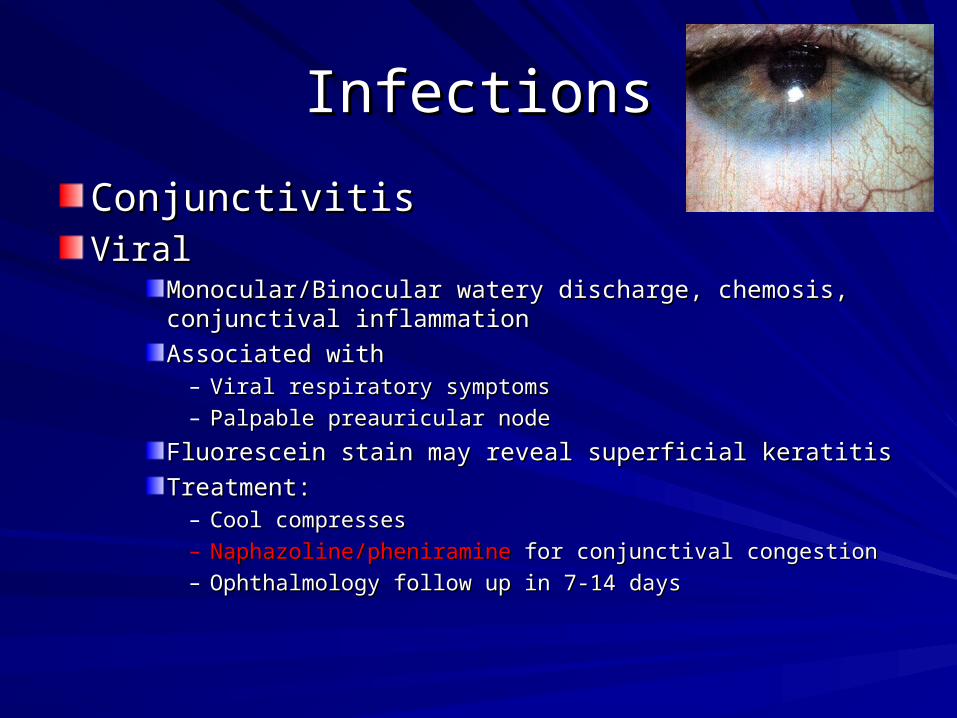
ConjunctivitisConjunctivitisViralViral
Monocular/Binocular watery discharge, chemosis, Monocular/Binocular watery discharge, chemosis, conjunctival inflammationconjunctival inflammationAssociated with Associated with
– Viral respiratory symptomsViral respiratory symptoms– Palpable preauricular nodePalpable preauricular node
Fluorescein stain may reveal superficial keratitisFluorescein stain may reveal superficial keratitisTreatment: Treatment:
– Cool compressesCool compresses– Naphazoline/pheniramineNaphazoline/pheniramine for conjunctival congestion for conjunctival congestion– Ophthalmology follow up in 7-14 daysOphthalmology follow up in 7-14 days

InfectionsInfections
ConjunctivitisConjunctivitisViralViral
Monocular/Binocular watery discharge, chemosis, Monocular/Binocular watery discharge, chemosis, conjunctival inflammationconjunctival inflammationAssociated with Associated with
– Viral respiratory symptomsViral respiratory symptoms– Palpable preauricular nodePalpable preauricular node
Fluorescein stain may reveal superficial keratitisFluorescein stain may reveal superficial keratitisTreatment: Treatment:
– Cool compressesCool compresses– Naphazoline/pheniramineNaphazoline/pheniramine for conjunctival congestion for conjunctival congestion– Ophthalmology follow up in 7-14 daysOphthalmology follow up in 7-14 days

InfectionsInfections
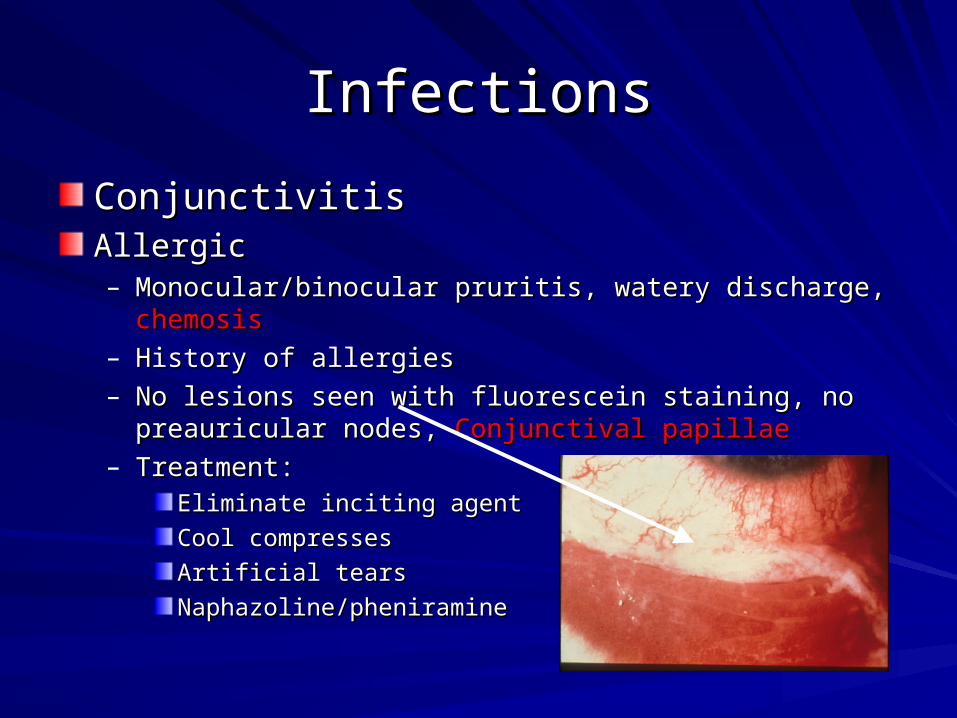
ConjunctivitisConjunctivitisAllergicAllergic– Monocular/binocular pruritis, watery discharge, Monocular/binocular pruritis, watery discharge, chemosischemosis– History of allergiesHistory of allergies– No lesions seen with fluorescein staining, no preauricular nodes, No lesions seen with fluorescein staining, no preauricular nodes,
Conjunctival papillaeConjunctival papillae– Treatment: Treatment:
Eliminate inciting agentEliminate inciting agentCool compressesCool compressesArtificial tearsArtificial tearsNaphazoline/pheniramineNaphazoline/pheniramine
InfectionsInfections
ConjunctivitisConjunctivitisAllergicAllergic– Monocular/binocular pruritis, watery discharge, Monocular/binocular pruritis, watery discharge, chemosischemosis– History of allergiesHistory of allergies– No lesions seen with fluorescein staining, no preauricular nodes, No lesions seen with fluorescein staining, no preauricular nodes,
Conjunctival papillaeConjunctival papillae– Treatment: Treatment:
Eliminate inciting agentEliminate inciting agentCool compressesCool compressesArtificial tearsArtificial tearsNaphazoline/pheniramineNaphazoline/pheniramine

InfectionsInfections
ConjunctivitisConjunctivitisAllergicAllergic– Monocular/binocular pruritis, watery discharge, Monocular/binocular pruritis, watery discharge, chemosischemosis– History of allergiesHistory of allergies– No lesions seen with fluorescein staining, no preauricular nodes, No lesions seen with fluorescein staining, no preauricular nodes,
Conjunctival papillaeConjunctival papillae– Treatment: Treatment:
Eliminate inciting agentEliminate inciting agentCool compressesCool compressesArtificial tearsArtificial tearsNaphazoline/pheniramineNaphazoline/pheniramine
InfectionsInfectionsHerpes Simplex VirusHerpes Simplex Virus– Classic: Classic: Dendritic epithelialDendritic epithelial defect defect– ED care depends on the site of infectionED care depends on the site of infection
Eyelid and conjunctivaEyelid and conjunctiva– Topical antivirals (trifluorothymidine drops/vidarabine ointment) Topical antivirals (trifluorothymidine drops/vidarabine ointment)
5 times/day5 times/day– Topical erythromycin ointmentTopical erythromycin ointment– Warm soaksWarm soaks
CorneaCornea– Topical antivirals Topical antivirals 9 times/day9 times/day
Anterior chamberAnterior chamber– CycloplegicCycloplegic agent may be used agent may be used
– First 3 days of infection: Acyclovir/famcyclovirFirst 3 days of infection: Acyclovir/famcyclovir

InfectionsInfectionsHerpes Simplex VirusHerpes Simplex Virus– Classic: Classic: Dendritic epithelialDendritic epithelial defect defect– ED care depends on the site of infectionED care depends on the site of infection
Eyelid and conjunctivaEyelid and conjunctiva– Topical antivirals (trifluorothymidine drops/vidarabine ointment) Topical antivirals (trifluorothymidine drops/vidarabine ointment)
5 times/day5 times/day– Topical erythromycin ointmentTopical erythromycin ointment– Warm soaksWarm soaks
CorneaCornea– Topical antivirals Topical antivirals 9 times/day9 times/day
Anterior chamberAnterior chamber– CycloplegicCycloplegic agent may be used agent may be used
– First 3 days of infection: Acyclovir/famcyclovirFirst 3 days of infection: Acyclovir/famcyclovir

InfectionsInfectionsHerpes Simplex VirusHerpes Simplex Virus– Classic: Classic: Dendritic epithelialDendritic epithelial defect defect– ED care depends on the site of infectionED care depends on the site of infection
Eyelid and conjunctivaEyelid and conjunctiva– Topical antivirals (trifluorothymidine drops/vidarabine ointment) Topical antivirals (trifluorothymidine drops/vidarabine ointment)
5 times/day5 times/day– Topical erythromycin ointmentTopical erythromycin ointment– Warm soaksWarm soaks
CorneaCornea– Topical antivirals Topical antivirals 9 times/day9 times/day
Anterior chamberAnterior chamber– CycloplegicCycloplegic agent may be used agent may be used
– First 3 days of infection: Acyclovir/famcyclovirFirst 3 days of infection: Acyclovir/famcyclovir
InfectionsInfections
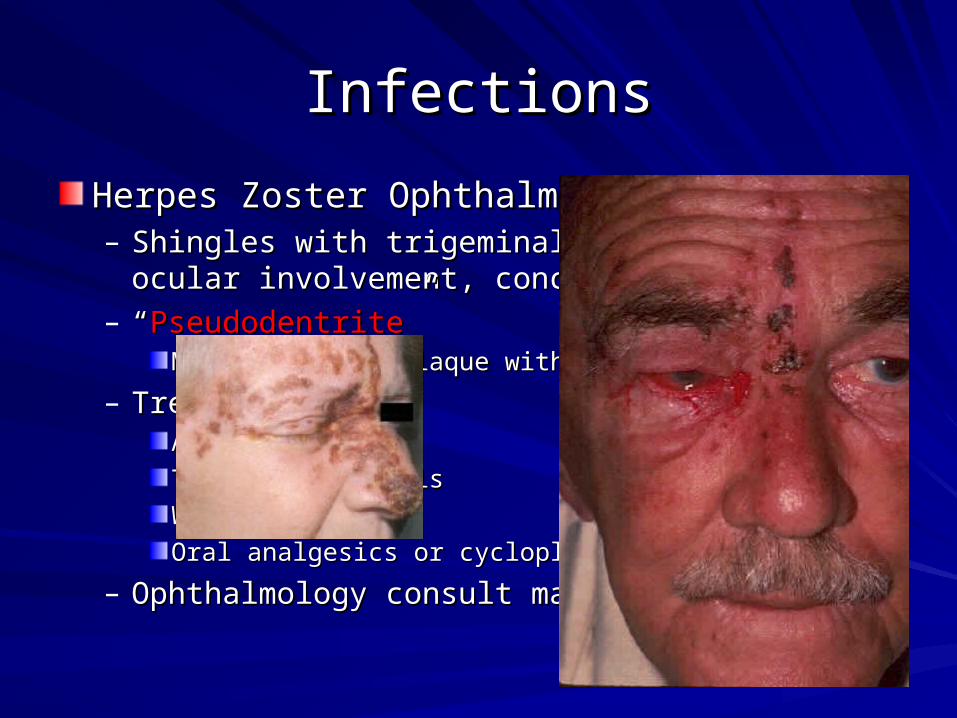
Herpes Zoster OphthalmicusHerpes Zoster Ophthalmicus– Shingles with trigeminal distribution, ocular Shingles with trigeminal distribution, ocular
involvement, concurrent iritisinvolvement, concurrent iritis– ““PseudodentritePseudodentrite””
Mucous corneal plaque with epithelial erosionMucous corneal plaque with epithelial erosion
– Treatment: Treatment: AcyclovirAcyclovirTopical antiviralsTopical antiviralsWarm compressesWarm compressesOral analgesics or cycloplegics for pain reliefOral analgesics or cycloplegics for pain relief
– Ophthalmology consult mandatoryOphthalmology consult mandatory

InfectionsInfections
Herpes Zoster OphthalmicusHerpes Zoster Ophthalmicus– Shingles with trigeminal distribution, ocular Shingles with trigeminal distribution, ocular
involvement, concurrent iritisinvolvement, concurrent iritis– ““PseudodentritePseudodentrite””
Mucous corneal plaque with epithelial erosionMucous corneal plaque with epithelial erosion
– Treatment: Treatment: AcyclovirAcyclovirTopical antiviralsTopical antiviralsWarm compressesWarm compressesOral analgesics or cycloplegics for pain reliefOral analgesics or cycloplegics for pain relief
– Ophthalmology consult mandatoryOphthalmology consult mandatory
InfectionsInfections
Herpes Zoster OphthalmicusHerpes Zoster Ophthalmicus– Shingles with trigeminal distribution, ocular Shingles with trigeminal distribution, ocular
involvement, concurrent iritisinvolvement, concurrent iritis– ““PseudodentritePseudodentrite””
Mucous corneal plaque with epithelial erosionMucous corneal plaque with epithelial erosion
– Treatment: Treatment: AcyclovirAcyclovirTopical antiviralsTopical antiviralsWarm compressesWarm compressesOral analgesics or cycloplegics for pain reliefOral analgesics or cycloplegics for pain relief
– Ophthalmology consult mandatoryOphthalmology consult mandatory

InfectionsInfectionsHerpes Zoster OphthalmicusHerpes Zoster Ophthalmicus– Shingles with trigeminal Shingles with trigeminal
distribution, ocular involvement, distribution, ocular involvement, concurrent iritisconcurrent iritis
– ““PseudodentritePseudodentrite””Mucous corneal plaque with Mucous corneal plaque with epithelial erosionepithelial erosion
– Treatment: Treatment: AcyclovirAcyclovirTopical antiviralsTopical antiviralsWarm compressesWarm compressesOral analgesics or cycloplegics Oral analgesics or cycloplegics for pain relieffor pain relief
– Ophthalmology consult Ophthalmology consult mandatorymandatory

InfectionsInfections
Periorbital Cellulitis (Preseptal Cellulitis)Periorbital Cellulitis (Preseptal Cellulitis)– Warm, indurated, erythematous eyelids onlyWarm, indurated, erythematous eyelids only– Treatment:Treatment:
Augmentin Augmentin (if older than 5 years)(if older than 5 years) if non-toxic if non-toxicToxic appearing, comorbidities, younger than 5Toxic appearing, comorbidities, younger than 5
– Hospital admission for IV Ceftriaxone/VancomycinHospital admission for IV Ceftriaxone/Vancomycin– < 5 years old: Septic workup (bacteremia/meningitis may < 5 years old: Septic workup (bacteremia/meningitis may
be present)be present)

InfectionsInfections
Periorbital Cellulitis (Preseptal Cellulitis)]Periorbital Cellulitis (Preseptal Cellulitis)]– Warm, indurated, erythematous eyelids onlyWarm, indurated, erythematous eyelids only– Treatment:Treatment:
Augmentin Augmentin (if older than 5 years)(if older than 5 years) if non-toxic if non-toxicToxic appearing, comorbidities, younger than 5Toxic appearing, comorbidities, younger than 5
– Hospital admission for IV Ceftriaxone/VancomycinHospital admission for IV Ceftriaxone/Vancomycin– < 5 years old: Septic workup (bacteremia/meningitis may < 5 years old: Septic workup (bacteremia/meningitis may
be present)be present)

InfectionsInfections
Periorbital Cellulitis (Preseptal Cellulitis)]Periorbital Cellulitis (Preseptal Cellulitis)]– Warm, indurated, erythematous eyelids onlyWarm, indurated, erythematous eyelids only– Treatment:Treatment:
Augmentin Augmentin (if older than 5 years)(if older than 5 years) if non-toxic if non-toxicToxic appearing, comorbidities, younger than 5Toxic appearing, comorbidities, younger than 5
– Hospital admission for IV Ceftriaxone/VancomycinHospital admission for IV Ceftriaxone/Vancomycin– < 5 years old: Septic workup (bacteremia/meningitis may < 5 years old: Septic workup (bacteremia/meningitis may
be present)be present)

InfectionsInfections
Orbital Cellulitis (Postseptal Cellulitis)Orbital Cellulitis (Postseptal Cellulitis)– Warm, indurated, erythematous eyelids onlyWarm, indurated, erythematous eyelids only– Fever, toxicity, proptosis, painful ocular motility, Fever, toxicity, proptosis, painful ocular motility,
limited limited ocular excursionocular excursion– Diagnosis: Diagnosis:
emergent orbital and sinus thin-slice CT w/o contrast, if emergent orbital and sinus thin-slice CT w/o contrast, if negativenegative::
– CT with contrast - may reveal subperiosteal abscessCT with contrast - may reveal subperiosteal abscess
– Treatment:Treatment:Ophtho consultOphtho consultHospital admission for IV CefuroximeHospital admission for IV Cefuroxime

InfectionsInfections
Orbital Cellulitis (Postseptal Cellulitis)Orbital Cellulitis (Postseptal Cellulitis)– Warm, indurated, erythematous eyelids onlyWarm, indurated, erythematous eyelids only– Fever, toxicity, proptosis, painful ocular motility, Fever, toxicity, proptosis, painful ocular motility,
limited limited ocular excursionocular excursion– Diagnosis: Diagnosis:
emergent orbital and sinus thin-slice CT w/o contrast, if emergent orbital and sinus thin-slice CT w/o contrast, if negativenegative::
– CT with contrast - may reveal subperiosteal abscessCT with contrast - may reveal subperiosteal abscess
– Treatment:Treatment:Ophtho consultOphtho consultHospital admission for IV CefuroximeHospital admission for IV Cefuroxime

InfectionsInfections
Corneal UlcerCorneal Ulcer– Pain,redness, photophobiaPain,redness, photophobia– Etiology: desiccation, trauma, direct invasion, contact Etiology: desiccation, trauma, direct invasion, contact
lens uselens use– Slitlamp exam:Slitlamp exam:
Staining corneal defect with hazy infiltrate,Staining corneal defect with hazy infiltrate,HypoponHypopon
– Treatment:Treatment:Topical ofloxacin or cipro drops every hourTopical ofloxacin or cipro drops every hourTopical cycloplegiaTopical cycloplegiaOptho eval within 24 hoursOptho eval within 24 hours

HypoponHypopon

Traumatic Eye InjuriesTraumatic Eye Injuries
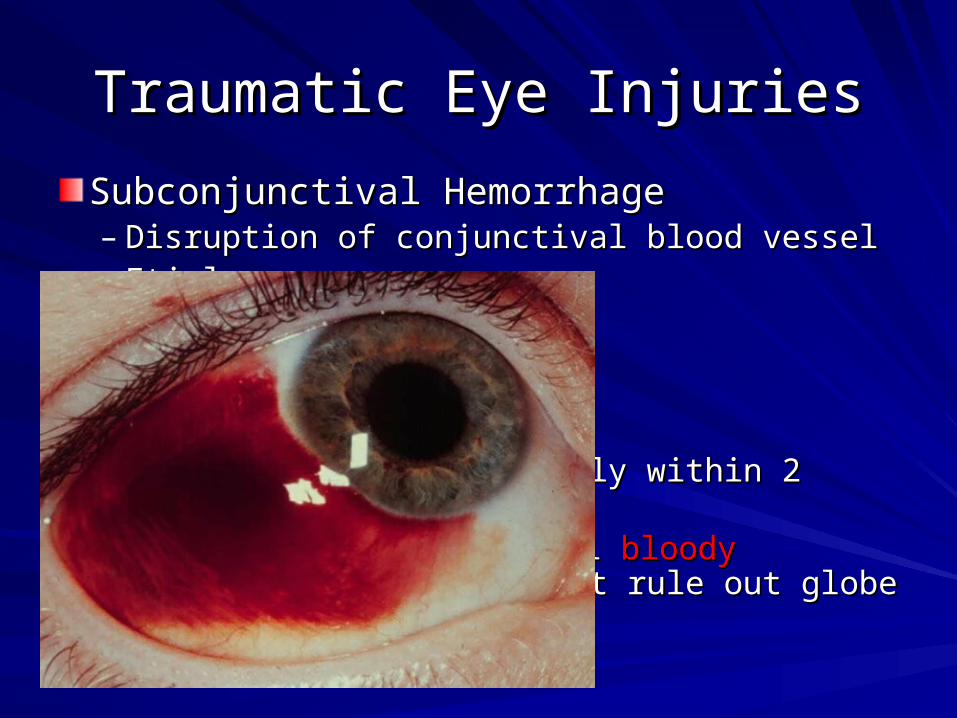
Subconjunctival HemorrhageSubconjunctival Hemorrhage– Disruption of conjunctival blood vesselDisruption of conjunctival blood vessel– EtiologyEtiology
TraumaTraumaSneezingSneezingGaggingGaggingValsalvaValsalva
– Will resolve spontaneously within 2 weeksWill resolve spontaneously within 2 weeks*If dense, circumferential *If dense, circumferential bloody chemosisbloody chemosis is is
present, must rule out globe rupturepresent, must rule out globe rupture

Traumatic Eye InjuriesTraumatic Eye Injuries
Subconjunctival HemorrhageSubconjunctival Hemorrhage– Disruption of conjunctival blood vesselDisruption of conjunctival blood vessel– EtiologyEtiology
TraumaTraumaSneezingSneezingGaggingGaggingValsalvaValsalva
– Will resolve spontaneously within 2 weeksWill resolve spontaneously within 2 weeks*If dense, circumferential *If dense, circumferential bloody chemosisbloody chemosis is is
present, must rule out globe rupturepresent, must rule out globe rupture
Traumatic Eye InjuriesTraumatic Eye Injuries
Subconjunctival HemorrhageSubconjunctival Hemorrhage– Disruption of conjunctival blood vesselDisruption of conjunctival blood vessel– EtiologyEtiology
TraumaTraumaSneezingSneezingGaggingGaggingValsalvaValsalva
– Will resolve spontaneously within 2 weeksWill resolve spontaneously within 2 weeks*If dense, circumferential *If dense, circumferential bloody chemosisbloody chemosis is is
present, must rule out globe rupturepresent, must rule out globe rupture
Traumatic Eye InjuriesTraumatic Eye Injuries
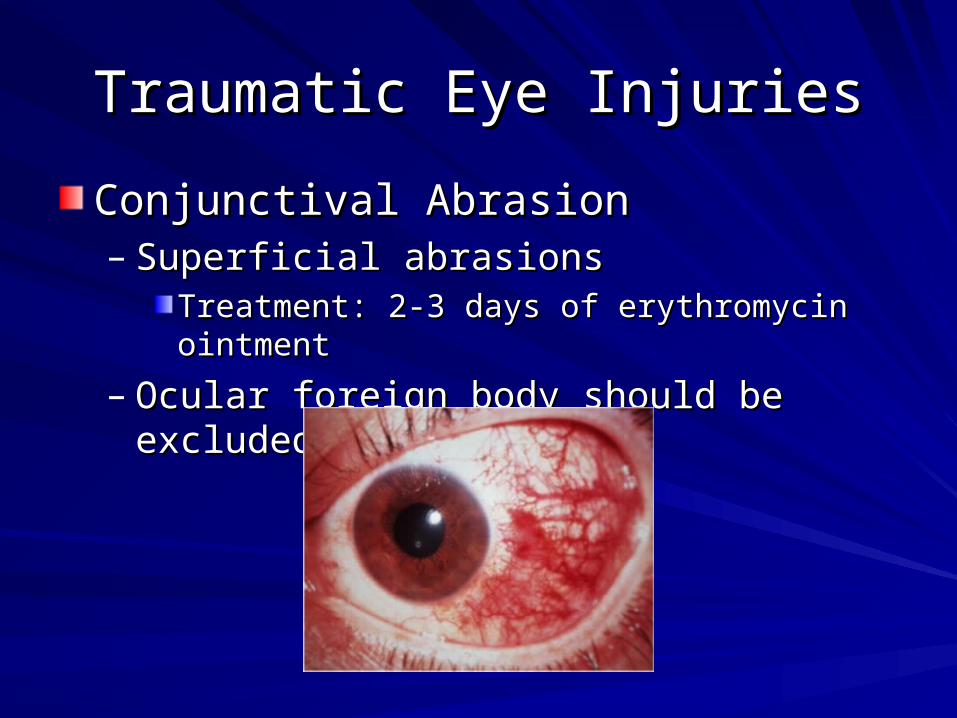
Conjunctival AbrasionConjunctival Abrasion– Superficial abrasionsSuperficial abrasions
Treatment: 2-3 days of erythromycin ointmentTreatment: 2-3 days of erythromycin ointment– Ocular foreign body should be excludedOcular foreign body should be excluded

Traumatic Eye InjuriesTraumatic Eye Injuries
Corneal AbrasionCorneal Abrasion– Tearing, photophobia, blepharospasm, severe painTearing, photophobia, blepharospasm, severe pain– Fluorescein: dye uptake at defect siteFluorescein: dye uptake at defect site– Rule out foreign bodyRule out foreign body– Treatment:Treatment:
CycloplegicCycloplegicTopical Tobramycin, Erythromycin, or Bacitracin/polymyxin Topical Tobramycin, Erythromycin, or Bacitracin/polymyxin dropsdropsContact lens wearers: Cipro, Ofloxacin, or Tobramycin dropsContact lens wearers: Cipro, Ofloxacin, or Tobramycin dropsTetanus shotTetanus shotOphthalmology consult within 24 hoursOphthalmology consult within 24 hours

Traumatic Eye InjuriesTraumatic Eye Injuries
Corneal AbrasionCorneal Abrasion– Tearing, photophobia, blepharospasm, severe painTearing, photophobia, blepharospasm, severe pain– Fluorescein: dye uptake at defect siteFluorescein: dye uptake at defect site– Rule out foreign bodyRule out foreign body– Treatment:Treatment:
CycloplegicCycloplegicTopical Tobramycin, Erythromycin, or Bacitracin/polymyxin Topical Tobramycin, Erythromycin, or Bacitracin/polymyxin dropsdropsContact lens wearers: Cipro, Ofloxacin, or Tobramycin dropsContact lens wearers: Cipro, Ofloxacin, or Tobramycin dropsTetanus shotTetanus shotOphthalmology consult within 24 hoursOphthalmology consult within 24 hours
Traumatic Eye InjuriesTraumatic Eye Injuries
Conjunctival Foreign BodiesConjunctival Foreign Bodies– Lid eversionLid eversion– Remove with a moistened sterile swabRemove with a moistened sterile swab

Traumatic Eye InjuriesTraumatic Eye Injuries
Conjunctival Foreign BodiesConjunctival Foreign Bodies– Lid eversionLid eversion– Remove with a moistened sterile swabRemove with a moistened sterile swab

Traumatic Eye InjuriesTraumatic Eye Injuries
Corneal Foreign BodiesCorneal Foreign Bodies– May be removed with fine needle tip, May be removed with fine needle tip, eye spudeye spud, or , or eye eye
burrburr after topical anesthetic applied after topical anesthetic applied– Then treat as a corneal abrasionThen treat as a corneal abrasion– Deep corneal stoma FB or those in central visual axis Deep corneal stoma FB or those in central visual axis
require ophtho consult for removalrequire ophtho consult for removal– Rust ringsRust rings can be removed with eye burr, but not can be removed with eye burr, but not
urgenturgent– Optho follow up in 24 hours for residual rust or deep Optho follow up in 24 hours for residual rust or deep
stromal involvementstromal involvement
Traumatic Eye InjuriesTraumatic Eye Injuries
Corneal Foreign BodiesCorneal Foreign Bodies– May be removed with fine needle tip, May be removed with fine needle tip, eye spudeye spud, or , or eye eye
burrburr after topical anesthetic applied after topical anesthetic applied– Then treat as a corneal abrasionThen treat as a corneal abrasion– Deep corneal stoma FB or those in central visual axis Deep corneal stoma FB or those in central visual axis
require ophtho consult for removalrequire ophtho consult for removal– Rust ringsRust rings can be removed with eye burr, but not can be removed with eye burr, but not
urgenturgent– Optho follow up in 24 hours for residual rust or deep Optho follow up in 24 hours for residual rust or deep
stromal involvementstromal involvement

Traumatic Eye InjuriesTraumatic Eye Injuries
Corneal Foreign BodiesCorneal Foreign Bodies– May be removed with fine needle tip, May be removed with fine needle tip, eye spudeye spud, or , or eye eye
burrburr after topical anesthetic applied after topical anesthetic applied– Then treat as a corneal abrasionThen treat as a corneal abrasion– Deep corneal stoma FB or those in central visual axis Deep corneal stoma FB or those in central visual axis
require ophtho consult for removalrequire ophtho consult for removal– Rust ringsRust rings can be removed with eye burr, but not can be removed with eye burr, but not
urgenturgent– Optho follow up in 24 hours for residual rust or deep Optho follow up in 24 hours for residual rust or deep
stromal involvementstromal involvement

Traumatic Eye InjuriesTraumatic Eye Injuries
Corneal Foreign BodiesCorneal Foreign Bodies– May be removed with fine needle tip, May be removed with fine needle tip, eye spudeye spud, or , or eye eye
burrburr after topical anesthetic applied after topical anesthetic applied– Then treat as a corneal abrasionThen treat as a corneal abrasion– Deep corneal stoma FB or those in central visual axis Deep corneal stoma FB or those in central visual axis
require ophtho consult for removalrequire ophtho consult for removal– Rust ringsRust rings can be removed with eye burr, but not can be removed with eye burr, but not
urgenturgent– Optho follow up in 24 hours for residual rust or deep Optho follow up in 24 hours for residual rust or deep
stromal involvementstromal involvement

Traumatic Eye InjuriesTraumatic Eye Injuries
Corneal Foreign BodiesCorneal Foreign Bodies– May be removed with fine needle tip, May be removed with fine needle tip, eye spudeye spud, or , or eye eye
burrburr after topical anesthetic applied after topical anesthetic applied– Then treat as a corneal abrasionThen treat as a corneal abrasion– Deep corneal stoma FB or those in central visual axis Deep corneal stoma FB or those in central visual axis
require ophtho consult for removalrequire ophtho consult for removal– Rust ringsRust rings can be removed with eye burr, but not can be removed with eye burr, but not
urgenturgent– Optho follow up in 24 hours for residual rust or deep Optho follow up in 24 hours for residual rust or deep
stromal involvementstromal involvement

Traumatic Eye InjuriesTraumatic Eye Injuries
Lid LacerationsLid Lacerations– Must exclude damage to eye and Must exclude damage to eye and
nasolacrimal systemnasolacrimal system– Fluorescein staining in the tear layer that Fluorescein staining in the tear layer that
appear in the adjacent lac confirm appear in the adjacent lac confirm nasolacrimal involvementnasolacrimal involvement
– Most require ophtho consultMost require ophtho consult

Traumatic Eye InjuriesTraumatic Eye Injuries
Lid LacerationsLid Lacerations– Must exclude damage to eye and Must exclude damage to eye and
nasolacrimal systemnasolacrimal system– Fluorescein staining in the tear layer that Fluorescein staining in the tear layer that
appear in the adjacent lac confirm appear in the adjacent lac confirm nasolacrimal involvementnasolacrimal involvement
– Most require ophtho consultMost require ophtho consult

Traumatic Eye InjuriesTraumatic Eye Injuries
Lid LacerationsLid Lacerations– Must exclude damage to eye and Must exclude damage to eye and
nasolacrimal systemnasolacrimal system– Fluorescein staining in the tear layer that Fluorescein staining in the tear layer that
appear in the adjacent lac confirm appear in the adjacent lac confirm nasolacrimal involvementnasolacrimal involvement
– Most require ophtho consultMost require ophtho consult

Traumatic Eye InjuriesTraumatic Eye Injuries
Traumatic Eye InjuriesTraumatic Eye Injuries
Blunt TraumaBlunt Trauma– Immediately assess integrity of globe and Immediately assess integrity of globe and
visual acuityvisual acuity– Eval depth of anterior chamber, pupil size, Eval depth of anterior chamber, pupil size,
monocular blindness monocular blindness ruptured globe ruptured globe

Traumatic Eye InjuriesTraumatic Eye Injuries
HyphemaHyphema

Traumatic Eye InjuriesTraumatic Eye Injuries
HyphemaHyphema

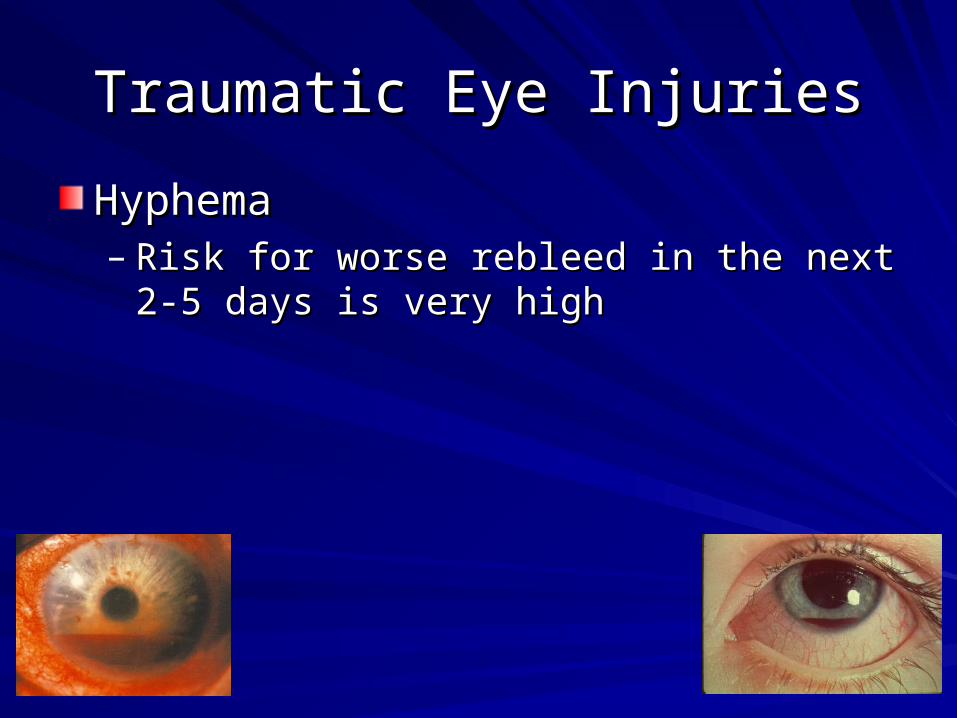
Traumatic Eye InjuriesTraumatic Eye InjuriesHyphemaHyphema– Blood in the anterior chamberBlood in the anterior chamber– Spontaneous or post-traumaSpontaneous or post-trauma– Treatment: Treatment:
Place the pt upright to allow inferior settling of bloodPlace the pt upright to allow inferior settling of bloodExclude ruptured globeExclude ruptured globeDilate the pupil with atropineDilate the pupil with atropineMeasure intraocular pressure – if > 30 mmHg apply topical Measure intraocular pressure – if > 30 mmHg apply topical TimololTimololEmergent Optho evalEmergent Optho eval
Traumatic Eye InjuriesTraumatic Eye Injuries
HyphemaHyphema– Risk for worse rebleed in the next 2-5 days is Risk for worse rebleed in the next 2-5 days is
very highvery high

Traumatic Eye InjuriesTraumatic Eye Injuries
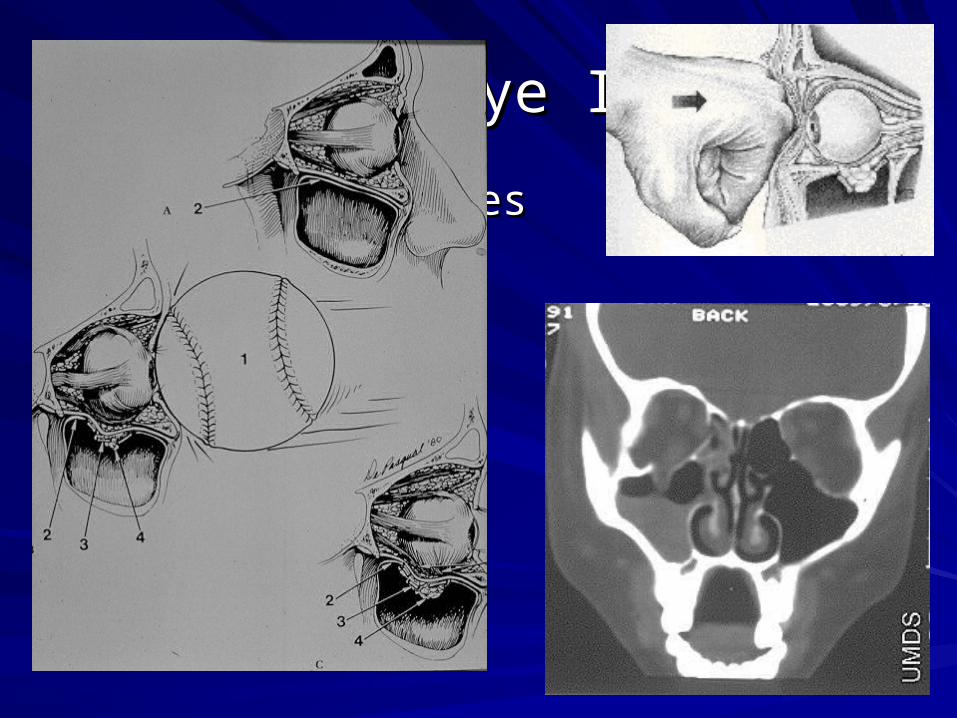
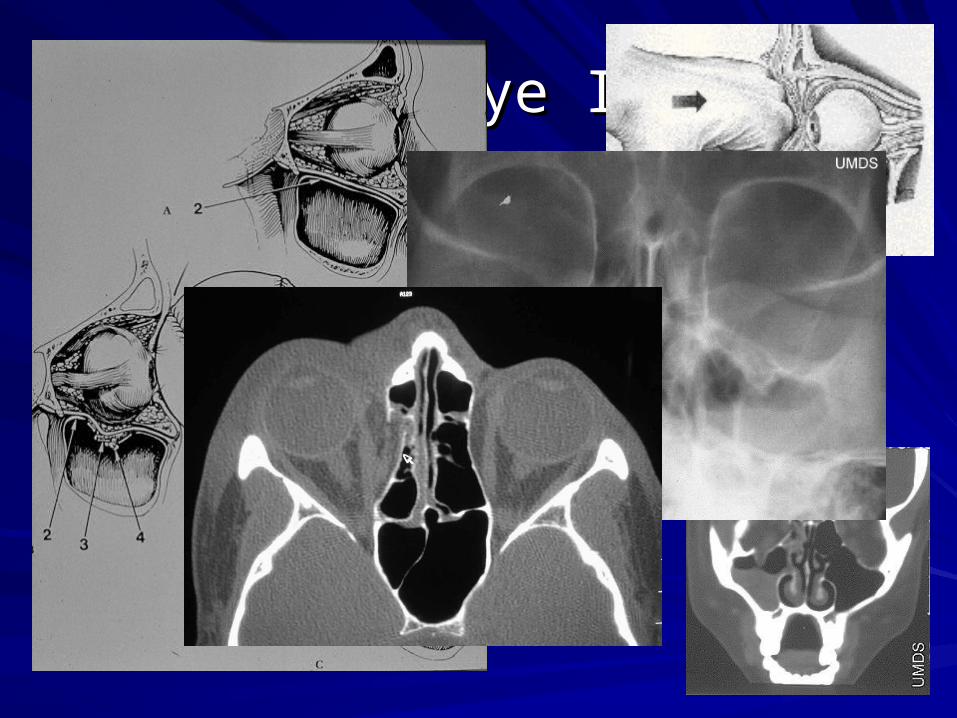
Blowout FracturesBlowout Fractures– Inferior and medial wall most at riskInferior and medial wall most at risk– Evaluate for Evaluate for
inferior rectus entrapment (diplopia on upward gaze)inferior rectus entrapment (diplopia on upward gaze)infraorbital nerve paresthesiainfraorbital nerve paresthesiasubcutaneous emphysema (when blowing the nose)subcutaneous emphysema (when blowing the nose)
– Orbital cut CT scanOrbital cut CT scan– Treatment: rule out ocular trauma and give oral KeflexTreatment: rule out ocular trauma and give oral Keflex– Isolated blowout fracture – ophtho eval in 3 – 10 daysIsolated blowout fracture – ophtho eval in 3 – 10 days

Traumatic Eye InjuriesTraumatic Eye Injuries
Blowout FracturesBlowout Fractures
Traumatic Eye InjuriesTraumatic Eye Injuries
Blowout FracturesBlowout Fractures

Traumatic Eye InjuriesTraumatic Eye Injuries
Blowout FracturesBlowout Fractures
Traumatic Eye InjuriesTraumatic Eye Injuries
Blowout FracturesBlowout Fractures
Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe– Severe subconjunctival hemorrhageSevere subconjunctival hemorrhage– Shallow or deep anterior chamber in one eyeShallow or deep anterior chamber in one eye– HyphemaHyphema– Tear-drop shaped pupilTear-drop shaped pupil

Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe– Severe subconjunctival hemorrhageSevere subconjunctival hemorrhage– Shallow or deep anterior chamber in one eyeShallow or deep anterior chamber in one eye– HyphemaHyphema– Tear-drop shaped pupilTear-drop shaped pupil
Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe– Severe subconjunctival hemorrhageSevere subconjunctival hemorrhage– Shallow or deep anterior chamber in one eyeShallow or deep anterior chamber in one eye– HyphemaHyphema– Tear-drop shaped pupilTear-drop shaped pupil– Limited extraocular motilityLimited extraocular motility– Extrusion of globe contentsExtrusion of globe contents– Significant reduction in visual acuitySignificant reduction in visual acuity

Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe– Seidel’s testSeidel’s test
Fluourescein Fluourescein streamingstreaming

Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe

Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe

Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe

Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe
Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe– If a globe injury is suspected: If a globe injury is suspected:
Don’t manipulate the eye any moreDon’t manipulate the eye any more……Step away from the eyeStep away from the eyePlace the pt uprightPlace the pt uprightNPONPOProtective eye shieldProtective eye shieldAdminister IV cephazolin and antiemeticAdminister IV cephazolin and antiemeticTetanusTetanus

Traumatic Eye InjuriesTraumatic Eye Injuries
Penetrating Trauma/Ruptured GlobePenetrating Trauma/Ruptured Globe– Orbital CT Orbital CT
If intraocular foreign body suspectedIf intraocular foreign body suspected– Call Ophtho right awayCall Ophtho right away
Traumatic Eye InjuriesTraumatic Eye Injuries
Chemical Ocular InjuryChemical Ocular Injury– Acid or alkali – treat the sameAcid or alkali – treat the same– Immediately flush (at the scene)Immediately flush (at the scene)– Continue to flush until pH is normal (7.0)Continue to flush until pH is normal (7.0)
Check with urine dipstickCheck with urine dipstick– Recheck pH after sweeping the fornices for Recheck pH after sweeping the fornices for
retained particlesretained particles– Measure IOPMeasure IOP
Traumatic Eye InjuriesTraumatic Eye Injuries
Chemical Ocular InjuryChemical Ocular Injury– Treatment:Treatment:
CycloplegicCycloplegicErythromycin ointmentErythromycin ointmentNarcotic pain medsNarcotic pain medsTetanusTetanus
– Immediate ophtho eval if not completely Immediate ophtho eval if not completely normal after initial measuresnormal after initial measures

Traumatic Eye InjuriesTraumatic Eye Injuries
Crazy Glue!Crazy Glue!

Traumatic Eye InjuriesTraumatic Eye Injuries
Crazy Glue!Crazy Glue!– Injury occurs only as a result of hard particles Injury occurs only as a result of hard particles
that form after dryingthat form after drying– Ophtho uses crazy glue as treatment in clinicOphtho uses crazy glue as treatment in clinic– Treatment:Treatment:
Erythromycin ointmentErythromycin ointmentRemove pieces that are easy to removeRemove pieces that are easy to removeOptho can remove residual glue within 48 hoursOptho can remove residual glue within 48 hours

Traumatic Eye InjuriesTraumatic Eye Injuries
Crazy Glue!Crazy Glue!– Mineral oil may help separate the lidsMineral oil may help separate the lids– Never use acetone or other substance that Never use acetone or other substance that
breaks up gluebreaks up glue

Acute Vision LossAcute Vision Loss
Acute Angle Closure GlaucomaAcute Angle Closure Glaucoma– Eye pain, headache, cloudy vision, colored Eye pain, headache, cloudy vision, colored
halos around lights, conjunctival injectionhalos around lights, conjunctival injection– Fixed, mid-dilated pupilFixed, mid-dilated pupil– Increased IOP (40-70 mm Hg)Increased IOP (40-70 mm Hg)
Normal range is 10 – 20 mm HgNormal range is 10 – 20 mm Hg– Nausea, vomitingNausea, vomiting

Acute Vision LossAcute Vision Loss
Acute Angle Closure GlaucomaAcute Angle Closure Glaucoma

Acute Vision LossAcute Vision Loss
Acute Angle Closure GlaucomaAcute Angle Closure Glaucoma

Acute Vision LossAcute Vision LossAcute Angle Closure GlaucomaAcute Angle Closure Glaucoma– Immediate treatment:Immediate treatment:
TimololTimololApraclonidineApraclonidinePrednisolone acetatePrednisolone acetate
– If IOP > 50 mm Hg or severe vision loss:If IOP > 50 mm Hg or severe vision loss:Acetazolamide 500mg IVAcetazolamide 500mg IV
– If no decrease in IOP or vision improvement:If no decrease in IOP or vision improvement:IV MannitolIV Mannitol
– Pilocarpine 1-2% in affected eye, pilocarpine 0.5% in Pilocarpine 1-2% in affected eye, pilocarpine 0.5% in contralateral eye (after IOP < 40 mm Hg)contralateral eye (after IOP < 40 mm Hg)
– Immediate Ophtho consultImmediate Ophtho consult

Acute Vision LossAcute Vision Loss
Optic NeuritisOptic Neuritis– Inflammation of the optic nerveInflammation of the optic nerve
Infection, demyelination, autoimmune dxInfection, demyelination, autoimmune dx– Presentation:Presentation:
Vision reduction (poor color perception)Vision reduction (poor color perception)Pain with extraocular movementPain with extraocular movementAfferent pupillary defectAfferent pupillary defect
– Swelling of the optic disc may be seenSwelling of the optic disc may be seen

Acute Vision LossAcute Vision Loss
Optic NeuritisOptic Neuritis

Acute Vision LossAcute Vision Loss
Optic NeuritisOptic Neuritis– DiagnosisDiagnosis
Red Desaturation TestRed Desaturation Test– Stare at bright red object with normal eye onlyStare at bright red object with normal eye only– Object will appear pink or light red in affected eyeObject will appear pink or light red in affected eye
– TreatmentTreatmentDiscuss with OphthoDiscuss with Ophtho

Acute Vision LossAcute Vision Loss
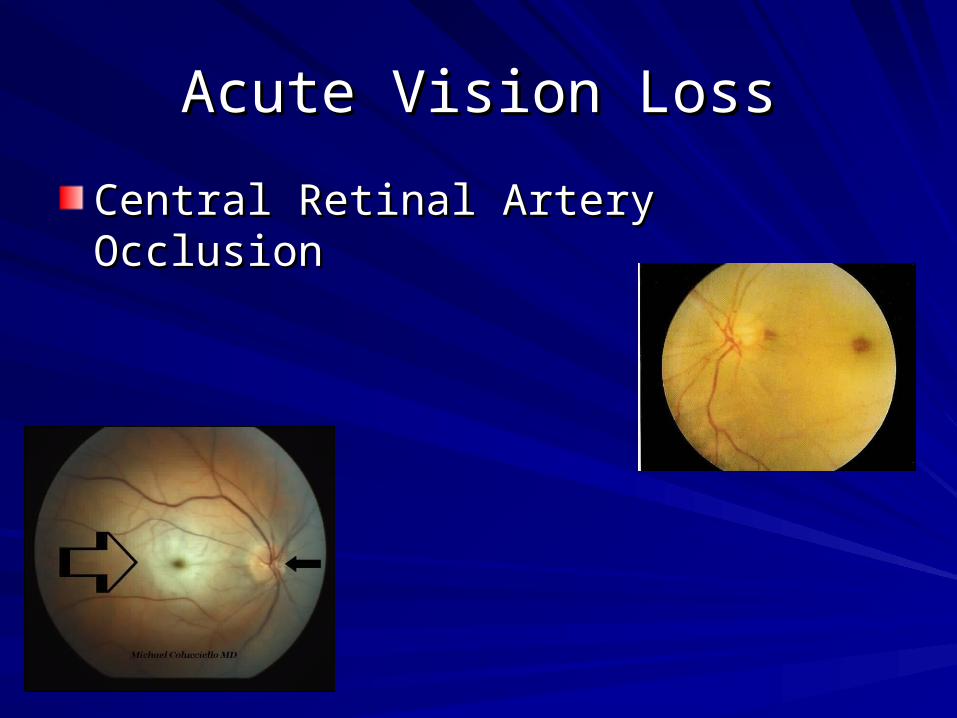
Central Retinal Artery OcclusionCentral Retinal Artery Occlusion– CausesCauses
Thrombosis, embolus, giant cell arteritis, vasculitis, sickle cell Thrombosis, embolus, giant cell arteritis, vasculitis, sickle cell disease, traumadisease, trauma
– Preceded by amaurosis fugaxPreceded by amaurosis fugax– Painless vision lossPainless vision loss
May be complete or partialMay be complete or partial
– Afferent pupillary defectAfferent pupillary defect– Pale fundus with narrowed arterioles and segmented Pale fundus with narrowed arterioles and segmented
flows (boxcars) and bright red macula (cherry red flows (boxcars) and bright red macula (cherry red spot)spot)
Acute Vision LossAcute Vision Loss
Central Retinal Artery OcclusionCentral Retinal Artery Occlusion

Acute Vision LossAcute Vision Loss
Central Retinal Artery OcclusionCentral Retinal Artery Occlusion– Treatment:Treatment:
Ocular massage!Ocular massage!– 15 seconds of direct pressure with sudden release15 seconds of direct pressure with sudden release
Topical timolol or IV acetazolamideTopical timolol or IV acetazolamideEmergent Optho evalEmergent Optho eval
Acute Vision LossAcute Vision Loss
Central Retinal Vein OcclusionCentral Retinal Vein Occlusion– Thrombosis – diuretics and oral Thrombosis – diuretics and oral
contraceptives predisposecontraceptives predispose– Painless, rapid monocular vision lossPainless, rapid monocular vision loss– Fundoscopy:Fundoscopy:
Diffuse retinal hemorrhageDiffuse retinal hemorrhageCotton wool spotsCotton wool spotsOptic disc edemaOptic disc edema““Blood and thunder”Blood and thunder”

Acute Vision LossAcute Vision Loss
Central Retinal Vein OcclusionCentral Retinal Vein Occlusion
Acute Vision LossAcute Vision Loss
Central Retinal Vein OcclusionCentral Retinal Vein Occlusion– Treatment:Treatment:
ASA 325ASA 325Ophtho referralOphtho referral

Acute Vision LossAcute Vision Loss
Temporal Arteritis (Giant Cell Arteritis)Temporal Arteritis (Giant Cell Arteritis)
Acute Vision LossAcute Vision Loss
Temporal Arteritis (Giant Cell Arteritis)Temporal Arteritis (Giant Cell Arteritis)– Systemic vasculitis that can cause ischemic Systemic vasculitis that can cause ischemic
optic neuropathyoptic neuropathy– UsuallyUsually
> 50 years old> 50 years oldFemaleFemalePolymyalgia rheumaticaPolymyalgia rheumatica
Acute Vision LossAcute Vision Loss
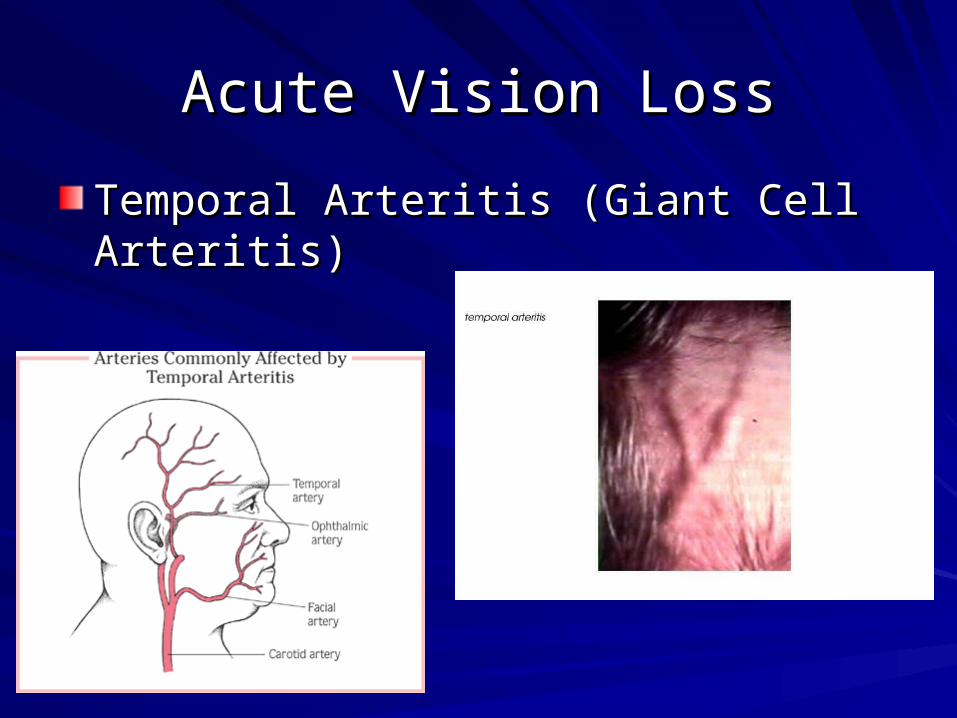
Temporal Arteritis (Giant Cell Arteritis)Temporal Arteritis (Giant Cell Arteritis)– Presentation:Presentation:
HeadacheHeadacheJaw claudicationJaw claudicationMyalgias, fatigueMyalgias, fatigueFever, anorexiaFever, anorexiaTemporal artery tendernessTemporal artery tendernessTIA or stroke?TIA or stroke?Afferent pupillary defectAfferent pupillary defect

Acute Vision LossAcute Vision Loss
Temporal Arteritis (Giant Cell Arteritis)Temporal Arteritis (Giant Cell Arteritis)– DiagnosisDiagnosis
Don’t waste your time if you suspect diagnosisDon’t waste your time if you suspect diagnosisESR, CRPESR, CRPTemporal artery biopsy (gold standard)Temporal artery biopsy (gold standard)
– TreatmentTreatmentIV steroids and Ophtho consultIV steroids and Ophtho consult
Acute Vision LossAcute Vision Loss
Temporal Arteritis (Giant Cell Arteritis)Temporal Arteritis (Giant Cell Arteritis)

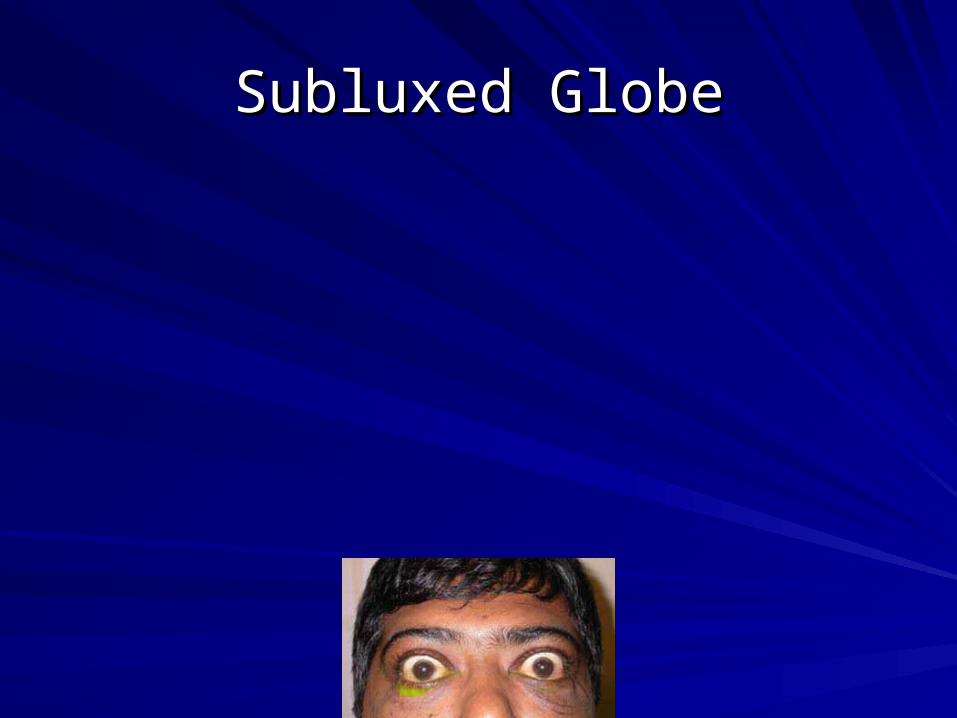
Subluxed GlobeSubluxed Globe
Subluxed GlobeSubluxed Globe

Subluxed GlobeSubluxed Globe

Subluxed GlobeSubluxed Globe

Subluxed GlobeSubluxed Globe

Subluxed GlobeSubluxed Globe

Subluxed GlobeSubluxed Globe
Subluxed GlobeSubluxed Globe

QUESTIONSQUESTIONS

QUESTIONSQUESTIONS

















