38
CHRONIC OTITIS AND CHOLESTEATOMA F. Benoudiba, Jl Sarrazin Service de Neuroradiologie CHU Kremlin Bicêtre JFIM BARCELONA nov 2014
| Date post: | 23-Jan-2018 |
| Category: |
Health & Medicine |
| Upload: | jfim-journees-francophones-dimagerie-medicale |
| View: | 759 times |
| Download: | 3 times |

CHRONICOTITISANDCHOLESTEATOMA
F.Benoudiba,JlSarrazinServicedeNeuroradiologieCHUKremlinBicêtre
JFIMBARCELONAnov2014

Cholesteatoma
Chronicotitis
Cholesteatoma Nocholesteatoma
Retractionpocketprecholesteatoma
state
AcquiredCholesteatoma

Retractionpocket§ Mesotympanic pocket
retraction uncontrollable and no self cleaning
§ (accumulation of epidermal scales
Precholesteatoma state

Acquiredcholesteatoma
u Aetiology Pocket retraction or marginal perforation with malpighian epithelium migration coming from the external cavity
u 80% of cholesteatoma

Fromapocketretraction…tocholesteatoma

Imaging
§ CHOLESTEATOMA IS A CLINICAL DIAGNOSIS § Modern imaging plays a key role in management of
cholesteatoma: § In pre operative § In post operative : minimally invasive supervision
(avoid surgical 2nd look) § Technical imaging:
ú CT scan (+++) ú MRI : growing up
Essentially in post operative Before surgery when complications

Imaging § Which imaging technique:
ú CT scan without enhancement: first choice modality To assess the diagnosis when otoscopy is
inclonclusive (closed tympanic membran) To screen for complications For the staging Anatomical assessment of the tympanomastoid cavity Surgical approach Choice

Imagingsemiology§ Nodular tisssular mass
ú Convex, rounded, polycyclic
ú location : Prussak’s space (External attical wall)
ú Attical extension
§ Mass effect on ossicular chain

Imagingsemiology
§ Bone erosion ú Erosion of the external
epitympanic wall (scutum): early sign
ú Ossicular erosion: 70% ú Not specific
Long process of incus Incus body Head of malleus

Imagingsemiology
§ Mastoid antrum extension § Enlargement of additus § Disappearanceofmastoid
celltrabeculation
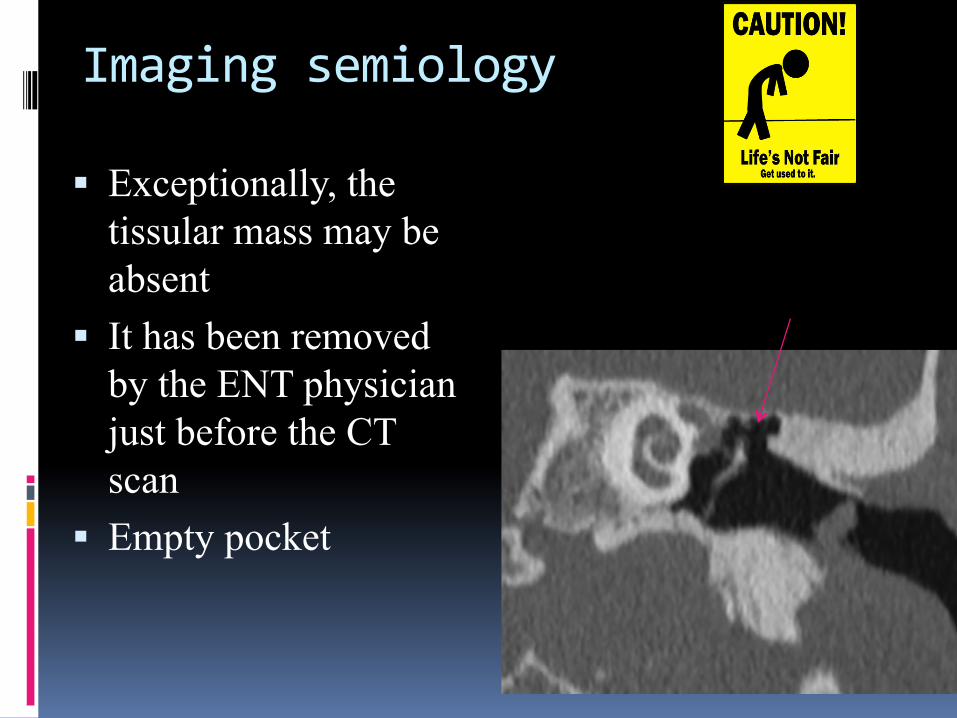
Imagingsemiology
§ Exceptionally, the tissular mass may be absent
§ It has been removed by the ENT physician just before the CT scan
§ Empty pocket

Congenitalcholesteatoma
§ Unusual § Pathogenetic explanation:
persistence of residual squamous cells usually existing in embryo between the 10th and the 30th week of gestation (Mickaels’ theory).

CongénitalCholesteatoma§ Petrous apex
§ EAC
§ Hypotympanum
§ Petrous pyramid
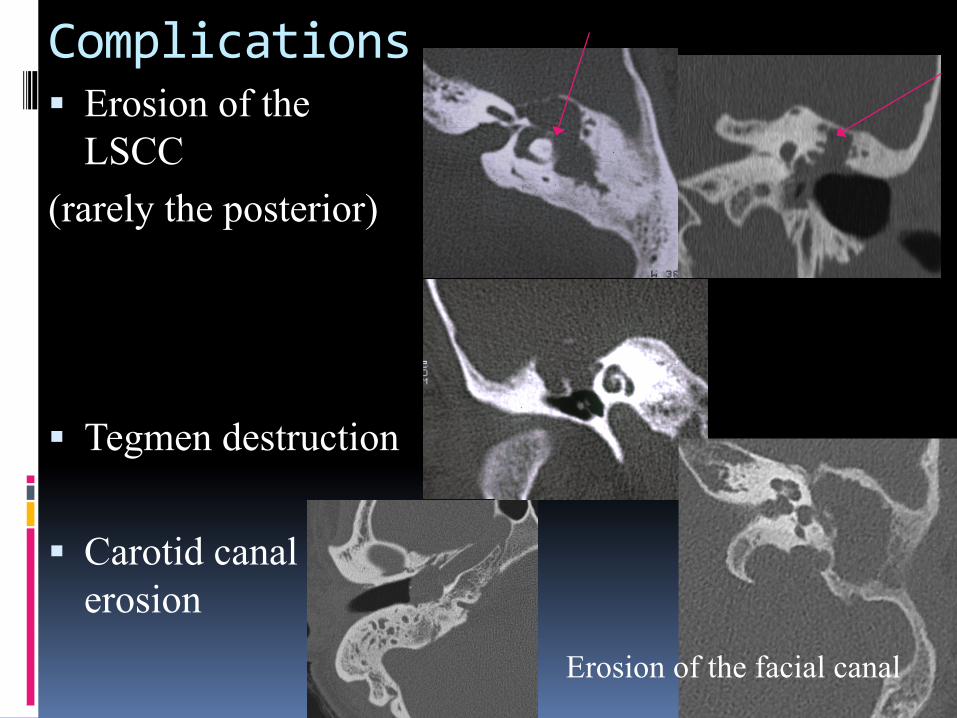
Complications§ Erosion of the
LSCC (rarely the posterior)
§ Tegmen destruction
§ Carotid canal erosion
Erosion of the facial canal

Complications§ Intralabyrinthine
Extension (MRI+++)
§ Intra cranial extension
§ Cerebral infection

Surgicalapproach§ Canalwallupwithtympanoplasty

CAUTION§ Prolapsedandsuperficialsigmoidsinus
§ Jugularvein
§ Emissaryvein
§ Intrapetrouscarotid

CAUTION§ ProlapsedTegmen
§ Temporalmeningocele

Surgicalapproach§ Canalwalldownmastoidectomy

Hearingrehabilitation
KurzTTPVario(Collin)
Universalprosthesistitane(Xomed-Medtronic)
Spiggle&TheisTitaniummiddleearpartial-totalimplant(PouretMédical)

Ossicularprosthesis
II
III

ProsthesisPORP TORP

Rehabilationprosthesis
TORP
PORP
Doubletraytympanoplasty
Incustransposition

Cholesteatoma:postoperativefollowing§ Imaging of post operative cholesteatoma
ú To assess a residual cholesteatoma ú Staging (extension/complications) if residual or
recurrent cholesteatoma. ú Post operative hearing loss without explanation
ú Best choice of imaging: depends on the situation

MRI:u Technical MRI T2 HR T1 SE Diffusion non EPI or SE +/- T1 with contrast
enhancement

MRI:results
T1 T2b1000 ADC T1Gado
Cholesteatoma
Fibrosis
granuloma
abcess
Thiriat S Am J Neuroradiol 2009

MRIdiffusion:Falsepositive
§ Cerumen
§ Sebaceouscyst
§ CholesterolGranuloma

Howtoavoidthefalsepositive§ Welllocatedthelesion
ú CorrelatedifferentsequencesandtheCTscan
§ CorrelatenonEpiandADC§ Cholesteatoma:decreaseADC
§ T1WIwithoutcontrast:ú hyperintense:It’snotacholesteatoma

Residualcholesteatoma

Residualcholesteatoma

Imagefusion:anatomicallocation

Children
§ Avoid iterative CT scan (radiation) § Prefer MRI diffusion § 1 month after surgery § No injection § Binary response: chole + or chole –
ú Chole + : surgery (+/- CT) ú Chole – : MRI (1 month later)

Adult
§ Good audition , no otorrhea: 1 question ú Residual Cholesteatoma?
§ Conductive hearing loss or mixed: 2 questions ú Residual Cholesteatoma? ú Functional evaluation

Clinical
No opacity
Audition OK Hearing loss
CT
Partial opacity Total opacity
Postoperativemonitoring
Dubuous image No doubt Residual No
residual
Audition OK Hearing loss
surgery Surgery Ossicular rehabilita
tion CT Ossicular
rehabilitation CT CT or MRI
MRI
12 months
12,24 months 12 ,24months 12 ,24months

Postoperativehearingloss
§ Failure : persistence or recurrence of conductive hearing loss
§ Complication : occured of a sensorineural hearing loss

Failureofrehabilitation
Incustranspositiondisplacement
PORPdislocation

A sensorineural hearing loss
Labyrinthitisossificant

Conclusion
§ Major role of imaging for the diagnosisof pre operative cholesteatoma
§ Systematic in pre operative: the first modality imaging is CT scan without contrast
§ CT may be supplemented by MRI if complications (labyrinthine fistula or extension, tegmen erosion, intra cranial extension, meningocele)

















