Child & Adolescent Psychiatry (a brief overview) Lance Feldman, MD, FAPA, MBA, BSN Vice Chair Clinical Affairs, Department of Psychiatry Affiliate Clinical Assistant Professor, University of South Carolina School of Medicine Greenville Diplomate, American Board of Psychiatry & Neurology, Psychiatry Diplomate, American Board of Psychiatry & Neurology, Child & Adolescent Psychiatry Diplomate, American Board of Addiction Medicine
Transcript
Child & Adolescent Psychiatry(a brief overview)
Lance Feldman, MD, FAPA, MBA, BSN
Vice Chair Clinical Affairs, Department of PsychiatryAffiliate Clinical Assistant Professor, University of South Carolina School of Medicine Greenville
Diplomate, American Board of Psychiatry & Neurology, PsychiatryDiplomate, American Board of Psychiatry & Neurology, Child & Adolescent Psychiatry
Diplomate, American Board of Addiction Medicine
Disclosures
• None
(We may, however, be discussing some possible off label medication uses, especially in the pediatric population.)
Outline
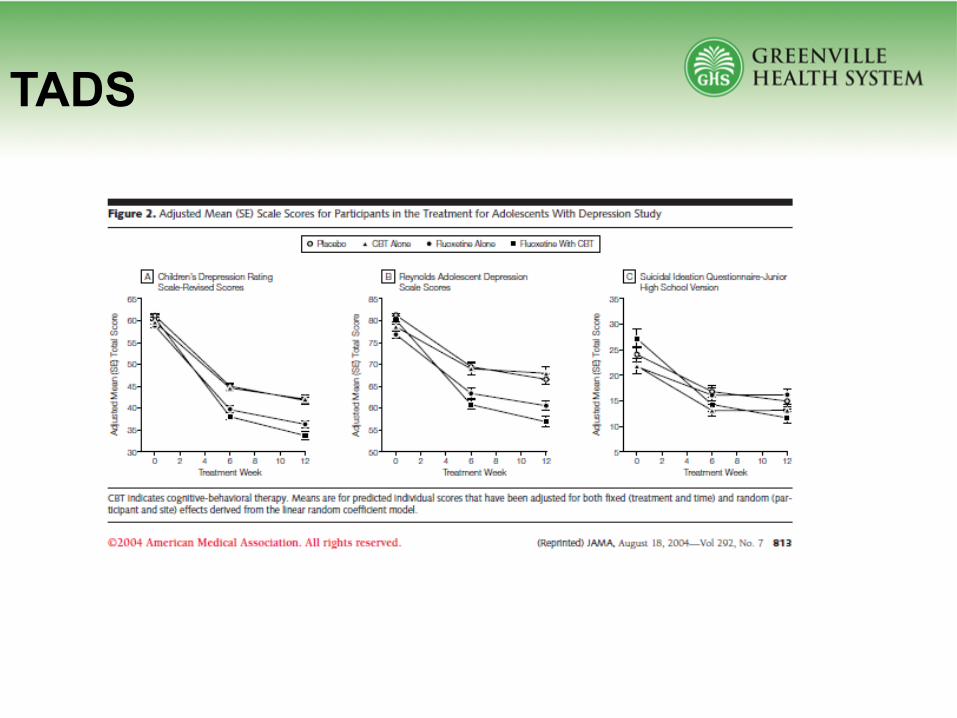
• Depression
• Anxiety
• Attention Deficit Hyperactivity Disorder (ADHD)
3
Prescribing Pearls
• Chlorpromazine (Thorazine) – FDA approved ages >6 months for schizophrenia / psychosis
• CDC – “the long term effects of ADHD medicine on young children are not known”
• FDA – Pregnancy Category C– “Methylphenidate has been shown to have
teratogenic effects in rabbits when given in doses of 200mg/kg/day”
4
Before Psychopharm…Modifiable Risk Factors• Sleep• Exercise• Nutrition• Family*• Friends*• Employer / Place of Employment*
5
Depression
6
Making the Diagnosis…
• Screening Tools – PHQ• Clinical Interview• Collateral Information (the “Fs”)• Criteria• Treatment
7
Depression Criteria• Five (or more) of the following symptoms have been present during the same 2-week
period and represent a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure.
– Depressed mood most of the day, nearly every day, as indicated by either subjective report (e.g., feels sad, empty, hopeless) or observation made by others (e.g., appears tearful). (Note: In children and adolescents, can be irritable mood.)
– Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated by either subjective account or observation).
– Significant weight loss when not dieting or weight gain (e.g., a change of more than 5% of body weight in a month), or decrease or increase in appetite nearly every day. (Note: In children, consider failure to make expected weight gain.)
– Insomnia or hypersomnia nearly every day.– Psychomotor agitation or retardation nearly every day (observable by others, not merely
subjective feelings of restlessness or being slowed down).– Fatigue or loss of energy nearly every day.– Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly
every day (not merely self-reproach or guilt about being sick).– Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by
subjective account or as observed by others).– Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific
plan, or a suicide attempt or a specific plan for committing suicide.
• Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance).
• The individual finds it difficult to control the worry. • The anxiety and worry are associated with three (or more) of the
following six symptoms (with at least some symptoms having been present for more days than not for the past 6 months):Note: Only one item is required in children.– Restlessness or feeling keyed up or on edge.– Being easily fatigued.– Difficulty concentrating or mind going blank.– Irritability.– Muscle tension.– Sleep disturbance (difficulty falling or staying asleep, or restless,
• Child/Adolescent Anxiety Multimodal Study (CAMS)• 488 participants with DSM-IV separation, generalized, or
social anxiety disorder• randomized to 12 weeks of cognitive-behavioral therapy
(CBT), sertraline (SRT), CBT+SRT (COMB), or medication management/pill placebo (PBO).
• Responders attended 6 monthly booster sessions in their assigned treatment arm; youth in COMB and SRT continued on their medication throughout this period.
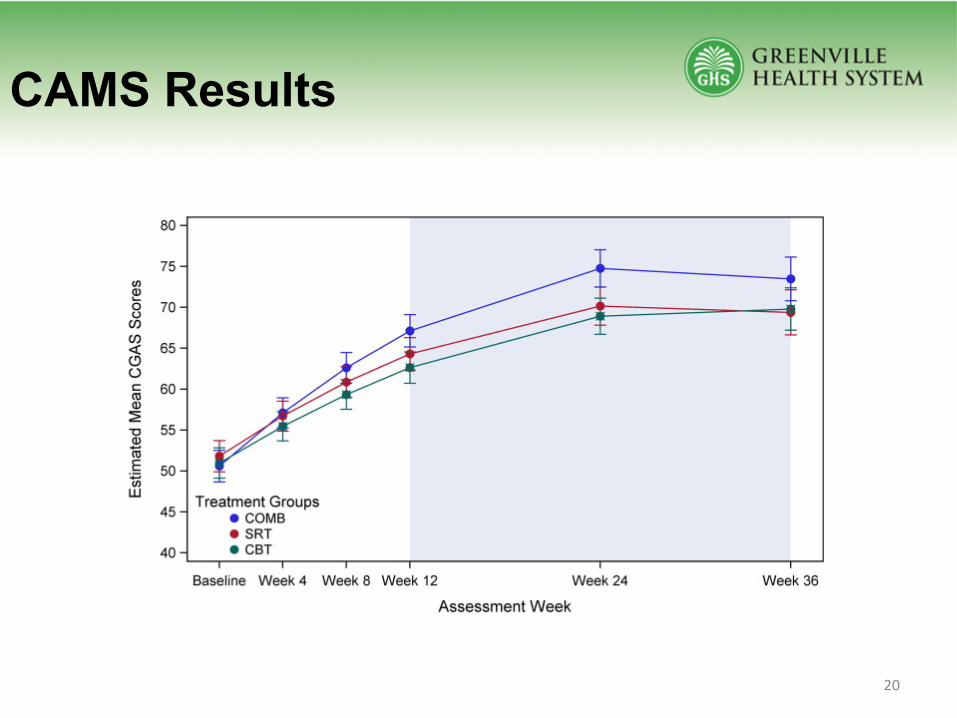
• Efficacy of COMB, SRT, and CBT (n = 412) was assessed at 24 and 36 weeks postrandomization.
• Youth randomized to PBO (n = 76) were offered active CAMS treatment if nonresponsive at week 12 or over
• Atomoxetine (Strattera)– Selective norepinephrine reuptake inhibitor– 10, 18, 25, 40, 60, 80, 100mg doses– 4-8 weeks at least– Up to 60% efficacy– No abuse potential– No withdrawal effects– Black Box: suicidal ideation– 2012 - $621.4 million (Eli Lilly, 2.7%)
31
Non-Stimulants: Alpha 2s
• Guanfacine– Guanfacine ER (Intuniv)– Guanfacine (Tenex)
• Clonidine– Clonidine ER (Kapvay)– Clonidine (Catapres)
behaviorally (e.g., physical aggression toward people or property) that are grossly out of proportion in intensity or duration to the situation or provocation.
• The temper outbursts are inconsistent with developmental level.• The temper outbursts occur, on average, three or more times per week.• The mood between temper outbursts is persistently irritable or angry most of the day,
nearly every day, and is observable by others (e.g., parents, teachers, peers).• Criteria A–D have been present for 12 or more months. Throughout that time, the
individual has not had a period lasting 3 or more consecutive months without all of the symptoms in Criteria A–D.
• Criteria A and D are present in at least two of three settings (i.e., at home, at school, with peers) and are severe in at least one of these.
• The diagnosis should not be made for the first time before age 6 years or after age 18 years.
• By history or observation, the age at onset of Criteria A–E is before 10 years.• There has never been a distinct period lasting more than 1 day during which the full
symptom criteria, except duration, for a manic or hypomanic episode have been met.










![Child and Adolescent[1]](https://static.documents.pub/doc/80x56/577cc5661a28aba7119c455e/child-and-adolescent1.jpg)







