Feasibility of Adapting a Classroom Balance Training Program to a Video Game Platform for People with Parkinson’s Disease Glenna A. Dowling, RN, PhD, FAAN, 1 Robert Hone, MS, MJ, 2 Charles Brown, BS, 2 Judy Mastick, RN, MN, 1 and Marsha Melnick, PhD 3 1 Departments of Physiological Nursing and 3 Physical Therapy and Rehabilitation, University of California, San Francisco, San Francisco, California. 2 Red Hill Studios, San Rafael, California. Abstract Objective: Decreased postural stability in people with Parkinson’s disease (PD) is a major component of disability. Rehabilitation inter- ventions are therefore targeted to improve balance, mobility, and strength. Virtual environment and gaming platforms can encourage therapeutic activity in the home and be challenging and fun. The aims of the project were to demonstrate the technical feasibility of adapting a classroom-based gait-and-balance training program to a video game platform. Ease of use, appeal, and safety of the proposed games were tested for both clinic and in-home use. Subjects and Methods: This cross-sectional observational study was carried out in three phases. Modifications in the game platform were made in an iterative fashion based on feedback from subjects and the observations of clinical and design team members. The first two phases of testing were performed in a laboratory setting, and the final phase was carried out in subjects’ homes. Results: Subjects (n = 20) scored the primary ‘‘Rail Runner’’ game 3.6 for ease of use (1 = hard, 5 = easy) and 3.9 for appeal (1 = did not like at all, 5 = liked very much). There were no safety issues en- countered, and the games performed without technical flaws in the final phase of testing. Conclusions: A computer-based video game that incorporates therapeutic movements to improve gait and balance for people with PD was appealing to subjects and feasible for home use. Key words: e-health, home health monitoring, telemedicine Introduction P arkinson’s disease (PD) is characterized by tremor, rigidity, bradykinesia/akinesia, postural instability, and impaired gait (decreased velocity and stride length). 1–4 These gait abnormalities place people with PD at high risk for falling. 5,6 Physical rehabilitation interventions are frequently prescribed to improve balance, mobility, strength, and activities of daily living. 7–12 These interventions may be prescribed on an individual or group basis. Computer-mediated virtual environment platforms have been used for motor rehabilitation for decades. Movements learned by people with disabilities in virtual environments transfer to real-world equivalent motor tasks in most cases and even generalize to other untrained tasks in some cases. 13 The Nintendo Ò WiiÔ system (Nin- tendo of America, Redmond, WA) offers a low-cost alternative to high-end head-mounted virtual environment systems. Players in- teract with the Wii system by making normal motions (i.e., swinging an arm) that control the movements of virtual objects on the screen. The input device, the Wiimote, detects acceleration in three dimen- sions as well as rotations about the two axes perpendicular to the force of gravity. The rapid response of the system provides a smooth, easy-to-learn, human–computer interface that is much less expen- sive than high-end virtual environment systems. There is increasing interest in the use of games within the health field. One of the benefits of games is that they can adapt to the patient’s actions to maintain a high level of engagement. Adaptive computer games evolve as players learn new skills by increasing the difficulty of challenges, thereby allowing the player to stay within an ‘‘area of maximal engagement,’’ which is similar to Vygotsky’s ‘‘zone of proximal development.’’ 14,15 In educational situations, the zone of proximal development is where maximum learning occurs. In physical training or rehabilitation situations, being in the ‘‘zone’’ fosters continued and mindful effort on the training goals. Developing games for people with disabilities involves unique design challenges because the ‘‘area of maximal engagement’’ for this type of player is likely to be different from that of an unaffected person. Game developers use a combination of usability testing and ‘‘tuning’’ approaches when targeting players with disabilities to properly calibrate the game difficulty to the players’ abilities. 16–18 Observation and rapid, iterative changes are essential for success. Studies in patients with stroke, 19–21 traumatic brain injury, 22,23 cerebral palsy, 24 and PD 25,26 have shown successful motor rehabili- tation using interactive technology. Esculier et al. 26 reported high functioning subjects with PD improved their balance, mobility, and functional ability playing preselected off-the-shelf Wii games. However, many commercially available games are not suitable for people with marked disability who require specifically targeted ex- ercises and routines to achieve therapeutic goals. Neurorehabilitation usability studies have found that off-the-shelf games may actually provide negative auditory and visual feedback because patients are not fast enough or efficient enough to perform the movements re- quired to successfully play the game. 27,28 Because of these user limitations, researchers are now developing games specifically tar- geted for rehabilitation in particular populations. After successfully offering a 1-hour group class for gait and bal- ance training for people with PD 8 at the University of California, San 298 TELEMEDICINE and e-HEALTH APRIL 2013 DOI: 10.1089/tmj.2012.0055
Transcript
Feasibility of Adapting a Classroom Balance Training Programto a Video Game Platform for People with Parkinson’s Disease
Glenna A. Dowling, RN, PhD, FAAN,1 Robert Hone, MS, MJ,2
Charles Brown, BS,2 Judy Mastick, RN, MN,1
and Marsha Melnick, PhD3
1Departments of Physiological Nursing and 3Physical Therapy andRehabilitation, University of California, San Francisco, SanFrancisco, California.
2Red Hill Studios, San Rafael, California.
AbstractObjective: Decreased postural stability in people with Parkinson’s
disease (PD) is a major component of disability. Rehabilitation inter-
ventions are therefore targeted to improve balance, mobility, and
strength. Virtual environment and gaming platforms can encourage
therapeutic activity in the home and be challenging and fun. The aims
of the project were to demonstrate the technical feasibility of adapting a
classroom-based gait-and-balance training program to a video game
platform. Ease of use, appeal, and safety of the proposed games were
tested for both clinic and in-home use. Subjects and Methods: This
cross-sectional observational study was carried out in three phases.
Modifications in the game platform were made in an iterative fashion
based on feedback from subjects and the observations of clinical and
design team members. The first two phases of testing were performed in
a laboratory setting, and the final phase was carried out in subjects’
homes. Results: Subjects (n = 20) scored the primary ‘‘Rail Runner’’
game 3.6 for ease of use (1 = hard, 5 = easy) and 3.9 for appeal (1 = did
not like at all, 5 = liked very much). There were no safety issues en-
countered, and the games performed without technical flaws in the
final phase of testing. Conclusions: A computer-based video game that
incorporates therapeutic movements to improve gait and balance for
people with PD was appealing to subjects and feasible for home use.
Key words: e-health, home health monitoring, telemedicine
Introduction
Parkinson’s disease (PD) is characterized by tremor, rigidity,
bradykinesia/akinesia, postural instability, and impaired
gait (decreased velocity and stride length).1–4 These gait
abnormalities place people with PD at high risk for falling.5,6
Physical rehabilitation interventions are frequently prescribed to
improve balance, mobility, strength, and activities of daily living.7–12
These interventions may be prescribed on an individual or group basis.
Computer-mediated virtual environment platforms have been
used for motor rehabilitation for decades. Movements learned by
people with disabilities in virtual environments transfer to real-world
equivalent motor tasks in most cases and even generalize to other
untrained tasks in some cases.13 The Nintendo� Wii� system (Nin-
tendo of America, Redmond, WA) offers a low-cost alternative to
teract with the Wii system by making normal motions (i.e., swinging
an arm) that control the movements of virtual objects on the screen.
The input device, the Wiimote, detects acceleration in three dimen-
sions as well as rotations about the two axes perpendicular to the
force of gravity. The rapid response of the system provides a smooth,
easy-to-learn, human–computer interface that is much less expen-
sive than high-end virtual environment systems.
There is increasing interest in the use of games within the health
field. One of the benefits of games is that they can adapt to the
patient’s actions to maintain a high level of engagement. Adaptive
computer games evolve as players learn new skills by increasing the
difficulty of challenges, thereby allowing the player to stay within an
‘‘area of maximal engagement,’’ which is similar to Vygotsky’s ‘‘zone
of proximal development.’’14,15 In educational situations, the zone of
proximal development is where maximum learning occurs. In
physical training or rehabilitation situations, being in the ‘‘zone’’
fosters continued and mindful effort on the training goals.
Developing games for people with disabilities involves unique
design challenges because the ‘‘area of maximal engagement’’ for this
type of player is likely to be different from that of an unaffected
person. Game developers use a combination of usability testing and
‘‘tuning’’ approaches when targeting players with disabilities to
properly calibrate the game difficulty to the players’ abilities.16–18
Observation and rapid, iterative changes are essential for success.
Studies in patients with stroke,19–21 traumatic brain injury,22,23
cerebral palsy,24 and PD25,26 have shown successful motor rehabili-
tation using interactive technology. Esculier et al.26 reported high
functioning subjects with PD improved their balance, mobility, and
functional ability playing preselected off-the-shelf Wii games.
However, many commercially available games are not suitable for
people with marked disability who require specifically targeted ex-
ercises and routines to achieve therapeutic goals. Neurorehabilitation
usability studies have found that off-the-shelf games may actually
provide negative auditory and visual feedback because patients are
not fast enough or efficient enough to perform the movements re-
quired to successfully play the game.27,28 Because of these user
limitations, researchers are now developing games specifically tar-
geted for rehabilitation in particular populations.
After successfully offering a 1-hour group class for gait and bal-
ance training for people with PD8 at the University of California, San
298 TELEMEDICINE and e-HEALTH APRIL 2013 DOI: 10.1089/tmj .2012.0055
Francisco (UCSF), training program developers G.A.D. and M.M.
sought to broaden access by providing a home-based program. In late
2007, Red Hill Studios (RHS), a developer of educational and health
games, suggested building a set of games that would utilize the re-
cently released Nintendo Wii motion-sensing system to detect pa-
tients’ movements as they performed the training exercises. RHS and
the UCSF clinicians partnered to obtain National Institutes of Health
funding through the Small Business Technology Transfer grant
program. The goal of this Phase I study was to test the feasibility of
creating a comprehensive computer game-based training program,
demonstrate safety for clinic and home use, and test usability and
appeal with end users. The team also sought to develop a remote data
capture transmission system with the ultimate goal of enabling
healthcare professionals to remotely prescribe personalized gaming
regimens and monitor progress.
The specific aims of the study were to demonstrate:
1. Technical feasibility of adapting the classroom training pro-
gram to a computer-based platform
2. Safety of the proposed program for clinic and in-home use
3. Ease of use of the proposed program and
4. Appeal of the proposed program.
Subjects and MethodsSAMPLES AND SETTINGS
The innovative nature of the program required extensive iterative
development with several rounds of evaluation:
1. The operational evaluation used a small sample (n = 3) to
gather initial data about the user interface and identify ther-
apeutic physical movements to be incorporated into the
computer-based games and took place at the UCSF Physical
Therapy Health and Wellness Center to enable the use of a
suspended safety harness.
2. The preliminary evaluation occurred in two stages (Stage 1,
n = 3; Stage 2, n = 4), again at the UCSF Physical Therapy
Health and Wellness Center. Subjects played the prototype
games, and the clinical and design teams in conjunction with
the subjects identified bugs and difficulties and assessed po-
tential safety issues.
3. In the in-home evaluation, we evaluated the final version of
the Phase I prototype games that had been redesigned based on
the findings of the preliminary evaluation, with subjects
(n = 10) in their homes.
In total, 20 subjects were enrolled in this study. Inclusion criteria
were consistent with the guidelines for idiopathic PD,29,30 and sub-
jects met criteria for Hoehn and Yahr disease Stage 1 (unilateral
disease) to 3 (bilateral disease, physically independent).31 Exclusion
criteria included persons with features of atypical PD30 or significant
other neurologic, orthopedic, or cardiac problems, cognitive im-
pairment as evidenced by five or more errors on the Mini Mental State
Examination,32 or visual or hearing impairments serious enough to
interfere with the ability to interact with the computer-based training
program. All subjects consented, and the study was approved by the
UCSF Committee on Human Research. At all evaluations, subjects
were tested 1–2 h after taking their routine dose of anti-parkinsonian
medication to facilitate being in the ‘‘on’’ state.
MEASUREMENTS/INSTRUMENTS
Demographics and functional status. Demographic, general
health information, and functional status ratings on the Unified
Parkinson’s Disease Rating Scale (Parts 2 and 3)31 and the Hoehn and
Yahr disease staging31 were collected on all subjects to characterize
the sample.
Perception of exertion. To determine subjective assessment of
physical activity intensity during game play, the Borg Rating of
Perceived Exertion Scale33 was administered upon completion of the
gaming session.
Experience feedback survey. Table 1 gives the survey used.
Computer platform. The PC-based games were developed using a
computer programming platform, Unity 3D (Unity Technologies, San
Francisco), and incorporated the Nintendo Wiimote controller, which
Table 1. Experience Feedback Survey
EVALUATION, QUESTION, SCALE
Operational evaluation
1. How difficult or easy was it to use the Wiimote? (scale from 1 to 5, with
1 = difficult and 5 = easy)
2. How difficult or easy were the instructions? (scale from 1 to 5, with
1 = difficult and 5 = easy)
3. How difficult or easy was it to perform the gestures? (scale from 1 to 5,
with 1 = difficult and 5 = easy)
4. Do you have any suggestions about the types of games you would like to
play with the Wiimote?
Preliminary evaluation and in-home evaluation
1. How enjoyable were the games? (scale of 1 to 5, with 1 = not enjoyable and
5 = very enjoyable)
2. How appealing were the graphics? (scale of 1 to 5, with 1 = not enjoyable
and 5 = very enjoyable)
3. How easy was it to play the games? (scale of 1 to 5, with 1 = not enjoyable
and 5 = very enjoyable)
4. How helpful was the audio? (scale of 1 to 5, with 1 = not enjoyable and
5 = very enjoyable)
5. How appropriate was the duration of one game? (scale of 1 to 5, with
1 = not enjoyable and 5 = very enjoyable)
6. Is there anything else that you would like to add?
Questions were developed for each stage of the testing.
VIDEO GAME FOR BALANCE IN PARKINSON’S DISEASE
ª M A R Y A N N L I E B E R T , I N C . � VOL. 19 NO. 4 � APRIL 2013 TELEMEDICINE and e-HEALTH 299
detects acceleration in three dimensions
(x,y,z) through the use of low-cost acceler-
ometers. The PC-based platform provided
greater flexibility in developing the proto-
type games (as opposed to the closed system
of the Nintendo Wii console). In addition,
the computer programming environment
allowed us to capture engineering data
necessary to properly tune the system for
the intended audience. Data from the Wii-
mote were acquired through the computer’s
Bluetooth� (Bluetooth SIG, Kirkland, WA)
receiver and sent to the Unity real-time
three-dimensional programming environ-
ment. The short transmission and response
time (tenths of a second) between the Wii-
mote and the computer minimized signal
latency creates a fluid interface in which the
user quickly learns to act through the in-
terface instead of acting with the inter-
face.34 This allows the user to focus on how
he or she is manipulating the virtual objects
on the screen, as opposed to how to operate
the interface device (Wiimote).
Procedures. There was close collabora-
tion between the RHS and UCSF teams
during development of the game proto-
types. The steps in the process of translating
the classroom training to a gaming format
are depicted in the flowchart given in Figure
1. The operational and preliminary evalua-
tion feedback enabled several rounds of it-
erative game redesign (Figs. 2 and 3). First,
the clinical team (UCSF) identified a set of
five therapeutic movements that could be
the focus of potential games. The design team (RHS) defined a set of
‘‘game gestures’’ designed to elicit the therapeutic movements se-
lected by the clinical team. The design team narrowed the number of
game gestures to three possible options (because of budget con-
straints of the Small Business Technology Transfer Phase I grant) and
developed algorithms to identify the game gestures based on the data
provided by the Wiimote. For example, in one game, the game ges-
ture consisted of the subject standing up and then sitting down. When
the game program detected that the game gesture had been suc-
cessfully performed, it provided feedback in the form of a game
action. For the standing up/sitting down gesture, the game action
involved propelling a railroad handcar down the track. Given the
exploratory nature of this research, we took advantage of production
efficiencies to develop rough prototypes for two other games. The
two other games provided different technical challenges, which al-
lowed us to expand our knowledge of gesture-based games. For the
second game, trunk rotation movement was developed into a
Fig. 1. Workflow chart showing the iterative design/evaluate/revise/re-evaluate process.
Fig. 2. Operational evaluation. (Left) First the subject was testedwith the support of a harness for safety. The apparatus did notallow for free range of motion; subsequent subjects were testedwith a gait belt. (Right) Subjects initially had the Wiimotesplaced on the ankle and forearm.
DOWLING ET AL.
300 TELEMEDICINE and e-HEALTH APRIL 2013
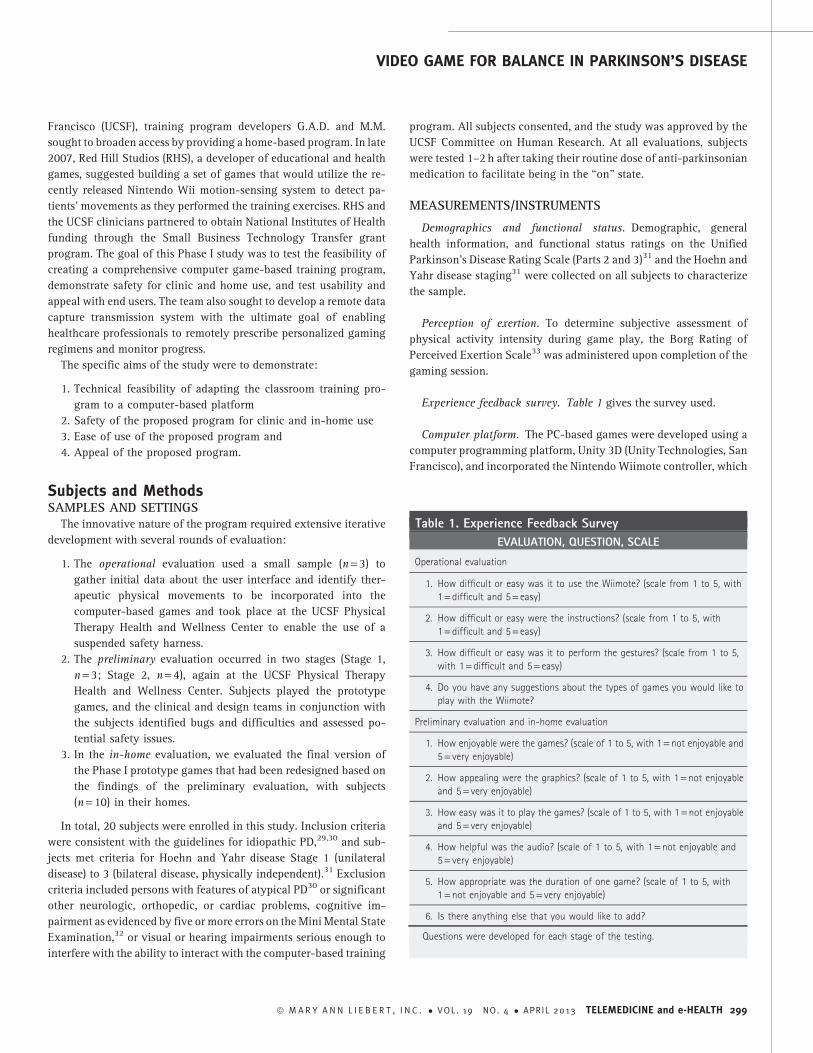
zoetrope game, where a movie would play at the correct speed if the
rotation was done at optimal speed and radius. For the third game,
diagonal reach across midline movement was developed into a
clothes toss game (Table 2).
For the in-home evaluations, subjects were outfitted with two
Wiimotes: one on the wrist and the other on the opposing thigh using
polychloroprene (Neoprene; DuPont�, Wilmington, DE) straps and
Velcro� (Velcro USA, Manchester, NH). Clinical team spotters were
situated on either side of the subject for safety. The subjects were
oriented to the equipment and to study procedures and were en-
couraged to ask questions along the way. Researchers reinforced the
fact we were testing the equipment, not the subject. Subjects
were prompted with the tutorial start screen that explained the
movement verbally and visually with a simple jointed figure as their
avatar (Fig. 4). Subjects practiced the game movements while
watching an on-screen avatar that mirrored their movements, pro-
viding real-time feedback on performance. Subjects also received
audio feedback that provided suggestions for improvement and en-
couragement. If subjects were having difficulty achieving the correct
movement, a clinical team member demonstrated and guided their
movement until the desired movement was achieved. After suc-
cessfully completing the tutorial, the subject then played the ‘‘Rail
Runner’’ prototype game several times. A design team member
monitored the subject’s level of engagement and/or frustration and
made adjustments to the speed and difficulty of the game manually
on the computer. The same process was carried out for the rough
tutorials and prototypes for the other two ‘‘back up’’ game concepts.
Fig. 3. Preliminary evaluation tutorial screen shots. ‘‘Gesturescreens’’ were originally developed for the operationalevaluation. With feedback from subjects, the screen shots wereexpanded, and audio cues were added for better instructionand guidance.
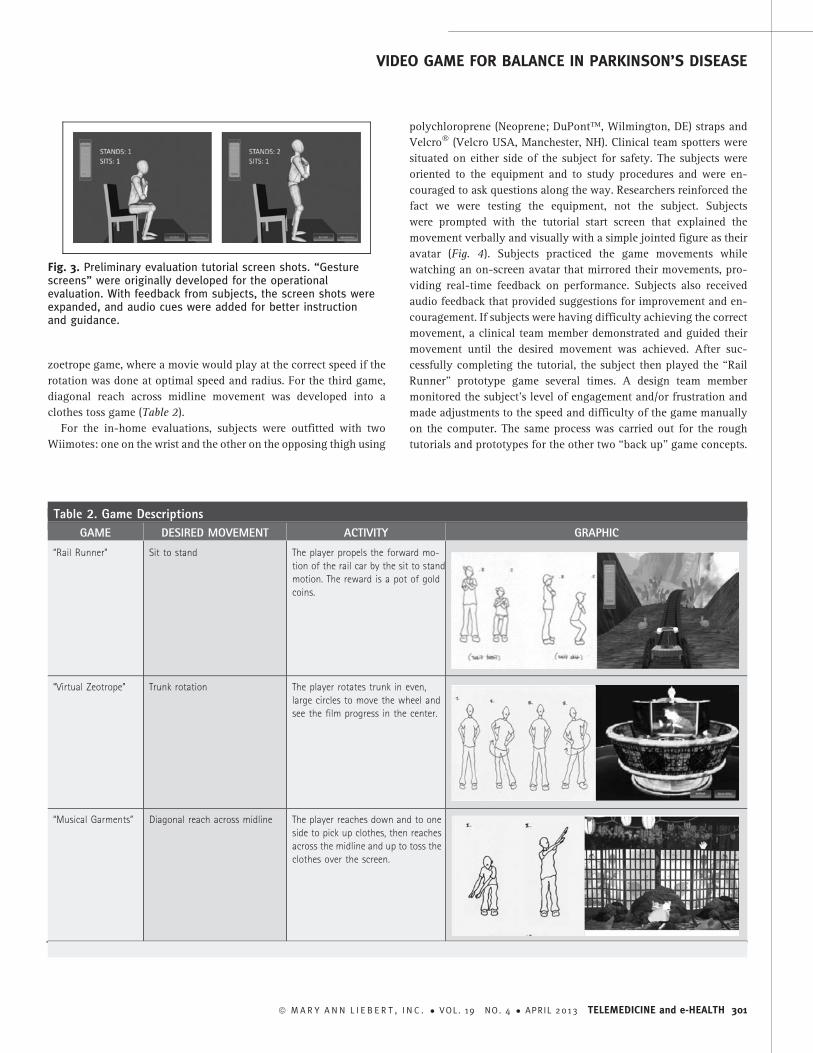
Table 2. Game Descriptions
GAME DESIRED MOVEMENT ACTIVITY GRAPHIC
‘‘Rail Runner’’ Sit to stand The player propels the forward mo-
tion of the rail car by the sit to stand
motion. The reward is a pot of gold
coins.
‘‘Virtual Zeotrope’’ Trunk rotation The player rotates trunk in even,
large circles to move the wheel and
see the film progress in the center.
‘‘Musical Garments’’ Diagonal reach across midline The player reaches down and to one
side to pick up clothes, then reaches
across the midline and up to toss the
clothes over the screen.
VIDEO GAME FOR BALANCE IN PARKINSON’S DISEASE
ª M A R Y A N N L I E B E R T , I N C . � VOL. 19 NO. 4 � APRIL 2013 TELEMEDICINE and e-HEALTH 301
Rest breaks were given as desired by subjects or if the clinical team
perceived the subject was experiencing fatigue. After completion of
game play, subjects rated their perceived exertion and answered
questions regarding their subjective sense of ease of use and appeal of
the games.
ResultsSample characteristics are described in Table 3. Operational and
preliminary testing subject feedback results and the game revisions
are described in Table 4 and depicted in Figures 1 and 2. During the
in-home testing, the games performed without technical bugs or
flaws during the in-home evaluations, and there were no falls or
injuries. After subjects played the ‘‘Rail Runner’’ game, their mean
ease-of-use rating score was 3.6 (standard deviation [SD] 1.3) (from
1 = very hard to use to 5 = very easy to use), and mean appeal score
was 3.9 (SD 1.1) (from 1 = did not like to 5 = liked very much). After
subjects played the ‘‘back up’’ game ‘‘Virtual Zoetrope,’’ their mean
rating score for ease of use was 2.7 (SD 1.6) (from 1 = very hard to use
to 5 = very easy to use), and mean appeal score was 2.8 (SD 1.6) (from
1 = did not like to 5 = liked very much). After subjects played the less
developed ‘‘back up’’ game ‘‘Musical Garments,’’ their mean rating
score for ease of use was 3.6 (SD 0.7) (from 1 = very hard to use to
5 = very easy to use), and mean appeal score was 3.1 (SD 1.2) (from
1 = did not like to 5 = liked very much).
DiscussionThe technical performance of the games was high, with no tech-
nical flaws occurring during the final prototype evaluation. In the
process of ‘‘getting under the hood’’ of the Wiimote system, we
identified two key limitations of the device. First, bias error and
sampling noise from the accelerometers quickly produced unac-
ceptably large error values for derived velocity and position (due to
single and double integration of force data). Gesture recognition
software typically used for the Wiimote (e.g., AILive) relies on rec-
ognizing sequences of relatively large, short-duration impulses in the
acceleration signature, which are suitable for detecting vigorous
gestures such as shaking or ‘‘batting.’’ However, the motions of in-
terest for this project were generally slower motions, lacking these
large, short-duration impulses. Second, although the accelerometers
produce relatively accurate limb orientation estimations when used
as three-axis ‘‘tilt meters,’’ they are unable on their own to discrim-
inate rotation purely around the vertical axis. This makes them less
reliable in detecting motions such as trunk rotation. We overcame these
limitations by focusing on the relatively accurate ability to deter-
mine limb orientation combined with the constraints of human body
mechanics and developed specific criteria to determine when game
gestures were successfully completed. For example, using the acceler-
ometer as a tilt meter (deviations from vertical force of gravity), we
Fig. 4. In-home evaluation, using a well-lighted room with a sturdystraight-backed chair for the ‘‘Rail Runner’’ game.
Table 3. Demographic and Functional Characteristicsof the Sample
EVALUATION,SUBJECT NUMBER
AGE(YEARS) GENDER
DIAGNOSIS(YEARS)a H&Yb
Operational
1 60 F 3 2.5
2 73 M 11 2
3 72 M 11 3
Preliminary Stage 1
4 75 F 6 2
5 83 M 16 3
6 68 M 6 2.5
Preliminary Stage 2
7 51 M 0.67 2
8 74 M 12 2.5
9 60 F 9 2
10 69 F 5 2.5
In-home
11 55 F 15 2.5
12 51 F 13 3
13 56 M 13 2.5
14 63 M 28 3
15 72 M 1.5 2
16 60 F 10 2.5
17 65 F 2 2
18 70 M 6 2
19 63 F 10 2.5
20 59 f 11 2
aDiagnosis is how many years have lapsed since the subject has been
diagnosed with PD.bH&Y is the Hoehn and Yahr score, on a scale of 1–5, with a higher number
reflecting more disability.
F, female; M, male.
DOWLING ET AL.
302 TELEMEDICINE and e-HEALTH APRIL 2013
calculated the deflection of the subject’s trunk and thigh from vertical
and used the combined signature of these values as they changed over
time to detect the ‘‘standing up’’ and ‘‘sitting down’’ movements.
The limitations of systems based solely on accelerometers will be
avoided moving forward by replacing the Wiimote with an enhanced
motion-sensing system that uses gyroscopes and a digital magne-
tometer to augment the three accelerometers. This modification
will allow far superior estimation of limb orientation in three-
dimensional space and thus a greater breadth of detectable gestures.
There were no falls or safety issues encountered in any of the three
Phase I evaluations. This can be attributed to the close collaboration
between UCSF and RHS that produced games suitable for the target
audience that did not foster dangerous situations or elicit overexer-
tion. It should be noted, however, that the UCSF team had to closely
monitor several subjects while they were playing to ensure safety.
Thus, safety strategies and close monitoring will be key components
in the subsequent phases of game testing.
The prototype game was challenging for subjects to play because it
required them to interact with a computer in a totally new way. The
fact that subjects were able to play the prototype game and rated it
highly is encouraging. However, each new game will present new user
interface challenges because this novel interface requires subjects to
physically interact with the game (as opposed to a simple Web activity).
The collaborative team’s experience in designing and developing
the ‘‘Rail Runner’’ game as well as the ‘‘back up’’ games ‘‘Virtual
Zoetrope’’ and ‘‘Musical Garments’’ reinforced the need to follow a
highly iterative design/evaluate/revise/re-evaluate process moving
forward as we design new games. The development of the two ‘‘back
up’’ games gave us the opportunity to test a broader range of motions
than would have been possible with just one game and anticipate
potential technical issues in new game designs. For example, the hip-
rotation game involved a continuous movement (rotating the hips) as
opposed to a sequence of discrete movements with specific end points
as in the ‘‘Rail Runner’’ game (sit, stand, sit, etc.). Some of the subjects
decreased the amplitude of rotation over time, finally reaching a
point where the system did not recognize the motion. Given that
progressive decrement in amplitude with repetitive motion is com-
mon in people with PD, this issue is likely to emerge with any
game that does not have specific end points. Our plan is to ensure
that the system continues to recognize the movements while
also encouraging subjects to exaggerate their motions to achieve
therapeutic benefit.
Overall, subjects were intrigued by and enthusiastic about the
possibility of using games to perform gait and balance training. The
preliminary nature of the Phase I prototype, in terms of graphics, au-
dio, and supporting material, may have affected the subjects’ rating of
appeal in the final in-home evaluation. Several subjects commented
specifically that they would have liked more tutorial/instructional
material about the games, which supports the findings of Robertson35
and the needs of ‘‘silver gamers.’’ Based on these results, we will in-
crease resources for instructional support moving forward.
Instructions were presented to the subjects as both audio prompts
and on-screen text instructions. In some cases, the text was not large
enough to be read clearly by all subjects. We will establish a mini-
mum text size (number of inches on screen) and dynamically adjust
the size of the type based on the subject’s system.
One of the issues with the ‘‘Virtual Zoetrope’’ game was that some
of the subjects did not know what a zoetrope was (an old-fashioned
mechanical device that rotates to display a sequence of images as a
movie). The project team assumed, incorrectly, that this device would
be familiar to subjects, but for some subjects it clearly was not, and
this impacted their performance. Moving forward, we will review
potential game concepts with typical end users at an early stage in
development.
Summary and ConclusionsThis study demonstrated the feasibility of using computer-based
games to provide gait and balance training to people with PD. As could
be expected when exploring innovative uses of technology, the study
involved a fair amount of experimentation and refinement. The ability
of the collaborative team of RHS and UCSF to respond to interim
challenges and find creative solutions bodes well for future develop-
ment. The design and production capabilities of the collaborative team
were also demonstrated by the ‘‘extra’’ development of two additional
prototype games. The inclusion of these games in the Phase I program
allowed us to gain valuable information that will greatly inform the
Phase II study. Finally, the moderately high variability in the sample
population in terms of game appeal, desired difficulty level, and per-
sonal abilities has directly informed the design of future games. We
will increase the number of games and increase the difficulty range to
customize the game challenge to individual abilities.
Table 4. Early Testing Design Iterations Based on Subjectand Team Feedback
TESTINGSTAGE
SUBJECTFEEDBACK REVISIONS
Operational evaluation
(n = 3)
Enjoyed experience, able
to understand how to
interact with game by
moving body, wanted
more instruction on what
to do.
Added more visual feed-
back. Graphic displays
were developed that
would respond to actions.
Preliminary evaluation
Stage 1 (n = 3) Subjects continue to de-
sire more introduction
and more feedback. Ease-
of-use average score 2.0.
Games appeal average
score 2.0.
Integrated audio
prompts, added the
original movements as a
tutorial.
Stage 2 (n = 4) Scores for ease of use
appeal improved. Ease-
of-use average score 3.8.
Games appeal average
score 4.3.
Detection of sit/stand
improved by placing
Wiimote at the lateral
thigh instead of on the
ankle for better move-
ment detection.
VIDEO GAME FOR BALANCE IN PARKINSON’S DISEASE
ª M A R Y A N N L I E B E R T , I N C . � VOL. 19 NO. 4 � APRIL 2013 TELEMEDICINE and e-HEALTH 303
Disclosure StatementR.H. and C.B. are employees of Red Hill Studios. G.A.D., J.M., and
M.M. declare no competing financial interests exist.
R E F E R E N C E S
1. Georgiou N, Bradshaw JL, Iansek R, Phillips JG, Mattingley JB, Bradshaw JA.Reduction in external cues and movement sequencing in Parkinson’s disease. JNeurol Neurosurg Psychiatry 1994;57:368–370.
2. Georgiou N, Iansek R, Bradshaw JL, Phillips JG, Mattingley JB, Bradshaw JA. Anevaluation of the role of internal cues in the pathogenesis of parkinsonianhypokinesia. Brain 1993;116:1575–1587.
3. Morris ME, Iansek R, Matyas TA, Summers JJ. Ability to modulate walkingcadence remains intact in Parkinson’s disease. J Neurol Neurosurg Psychiatry1994;57:1532–1534.
4. Morris ME, Iansek R, Matyas TA, Summers JJ. Stride length regulation inParkinson’s disease. Normalization strategies and underlying mechanisms.Brain 1996;119:551–568.
5. Morris ME, Huxham F, McGinley J, Dodd K, Iansek R. The biomechanics andmotor control of gait in Parkinson disease. Clin Biomech (Bristol, Avon)2001;16:459–470.
6. Winter DA. The biomechanics and motor control of human gait: Normal, elderly,and pathological. Waterloo, ON, Canada: University of Waterloo Press, 1991.
7. Comella CL, Stebbins GT, Brown-Toms N, Goetz CG. Physical therapy andParkinson’s disease: A controlled clinical trial. Neurology 1994;44:376–378.
8. Melnick ME, Dowling GA, Baum WC, Piper MS, Rust LL. Effects of rhythmicexercise on balance, gait, and depression in patients with Parkinson’s disease.Gerontologist 1999;39:293–294.
9. Melnick ME, Dowling GA, Dodd MJ. The pro-self program: Exercise forParkinson’s disease. Gerontologist 2001;41:282.
10. Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for themanagement of Parkinson’s disease (2001): Treatment guidelines. Neurology2001;56(11 Suppl 5):S1–S88.
11. Scandalis TA, Bosak A, Berliner JC, Helman LL, Wells MR. Resistance training andgait function in patients with Parkinson’s disease. Am J Phys Med Rehabil2001;80:38–43; quiz 44–36.
12. Viliani T, Pasquetti P, Magnolfi S, et al. Effects of physical training onstraightening-up processes in patients with Parkinson’s disease. Disabil Rehabil1999;21:68–73.
13. Holden MK. Virtual environments for motor rehabilitation: Review.Cyberpsychol Behav 2005;8:187–211; discussion 212–219.
14. Vygotsky LS. Mind and society: The development of higher psychologicalprocesses. Cambridge, MA: Harvard University Press, 1978.
15. Chaiklin S. The zone of proximal development in Vygotsky’s analysis of learningand instruction. In: Kozulin A, Gindis B, Ageyev V, Miller S, eds. Vygotsky’seducational theory and practice in cultural context. Cambridge, UK: CambridgeUniversity Press, 2003;39–64.
16. Pagulayan RJ, Keeker K, Wixon D, Romero RL, Fuller T. User-centered design ingames. In: Jacko JA, Sears A, eds. The human-computer interaction handbook:Fundamentals, evolving technologies and emerging applications. Mahwah, NJ:Lawrence Erlbaum Associates, 2002:883–906.
17. Medlock MC, Wixon D, Terrano M, Romero R, Fiulton B. Using the RITE methodto improve products: A definition and case study. Bloomingdale, IL: UsabilityProfessionals Association, 2002.
18. Fulton B, Medlock M. Beyond focus groups: Getting more useful feedback fromconsumers. Presented at the Game Development Conference, Santa Clara, CA, 2003.
19. Bisson E, Contant B, Sveistrup H, Lajoie Y. Functional balance and dual-taskreaction times in older adults are improved by virtual reality and biofeedbacktraining. Cyberpsychol Behav 2007;10:16–23.
20. Boian R, Sharma A, Han C, et al. Virtual reality-based post-stroke handrehabilitation. Stud Health Technol Inform 2002;85:64–70.
21. Holden MK, Dyar TA, Schwamm L, Bizzi E. Virtual-environment-basedtelerehabilitation in patients with stroke. Presence Teleoperators Virtual Environ2005;14:214–233.
22. Gil-Gomez JA, Llorens R, Alcaniz M, Colomer C. Effectiveness of a Wii BalanceBoard-based system (eBaViR) for balance rehabilitation: A pilot randomizedclinical trial in patients with acquired brain injury. J Neuroeng Rehabil2011;8:30.
23. Ustinova KI, Leonard WA, Cassavaugh ND, Ingersoll CD. Development of a 3Dimmersive videogame to improve arm-postural coordination in patients withTBI. J Neuroeng Rehabil 2011;8:61.
24. Howcroft J KS, Fehlings D, Wright V, Zabjek K, Andrysek J, Biddiss E. Active videogame play in children with cerebral palsy: Potential for physical activity promotionand rehabilitation therapies. Arch Phys Med Rehabil 2012;93:1448–1456.
25. Weghorst S. Augmented reality and Parkinson’s disease. Commun ACM1997;(Aug):47–48.
26. Esculier JF, Vaudrin J, Beriault P, Gagnon K, Tremblay LE. Home-based balancetraining programme using Wii Fit with balance board for Parkinsons’s disease: Apilot study. J Rehabil Med 2012;44:144–150.
27. Lange BS, Flynn SM, Rizzo AA. Initial usability assessment of the off-the-shelfvideo game consoles for clinical game-based motor rehabilitation. Phys TherRev 2009;14:355–363.
28. Lange B, Flynn S, Proffitt R, Chang CY, Rizzo A. Development of an interactivegame-based rehabilitation tool for dynamic balance training. Top Stroke Rehabil2010;17:345–352.
29. Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. ArchNeurol 1999;56:33–39.
30. Hughes AJ, Ben-Schlomo Y, Daniel SE, Lees AJ. What features improve theaccuracy of clinical diagnosis in Parkinson’s disease: A clinicopathologic study.Neurology 1992;42:1142–1146.
31. Fahn S, Elton R, UPDRS program members. Unified Parkinson’s disease ratingscale. In: Fahn S, Mardsen CD, Goldstein M, Calne D (eds). Recent developmentsin Parkinson’s disease. Florham Park, NJ: Macmillan Healthcare Information,1987:153–163.
32. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: A practical method forgrading the cognitive state of patients for the clinician. J Psychiatr Res1975;12:189–198.
33. Borg GA. Perceived exertion: A note on ‘‘history’’ and methods. Med Sci Sports1973;5:90–93.
34. Norman DA. The design of everyday things. New York: Basic Books,1988.
35. Robertson A. What gamers want: Silver gamers. 2008. Available atwww.gamasutra.com/view/feature/3720/what_gamers_want_silver_gamers.php (last accessed July 17, 2008).