Feasibility of time-delayed teleoperation Human limitations in critical tasks Tamás Haidegger Lab. of Biomedical Engineering, Budapest University of Technology and Economics (BME) Austrian Center for Medical Innovation and Technology (ACMIT) NASA Future In-Space Operations 07.27.2011. Telecon
Transcript
Feasibility of time-delayed teleoperationHuman limitations in critical tasks
Tamás Haidegger
Lab. of Biomedical Engineering, Budapest University of Technology and Economics (BME)Austrian Center for Medical Innovation and Technology (ACMIT)
NASA Future In-Space Operations
07.27.2011. Telecon
A year at Johns Hopkins
2001–06 MSc in EE at Budapest Univ. of Technology and Economics2005–08 MSc in Biomedical Engineering at BME2006–09 EE doctoral school at BME2007–08 visiting scholar at CISST ERC, Johns Hopkins2009– 11 doctoral candidate 2010– assistant research fellow at BME 2010–11 visiting research fellow/postdoc at ACMIT2012– adjunct professor at BME2011– CEO/CTO Clariton Ltd.
Background
NASA Future In-Space Operations 07.27.2011.
2
Content
• Space healthcare
• Introduction to teleoperated surgical robots
• s
3
A year at Johns Hopkins
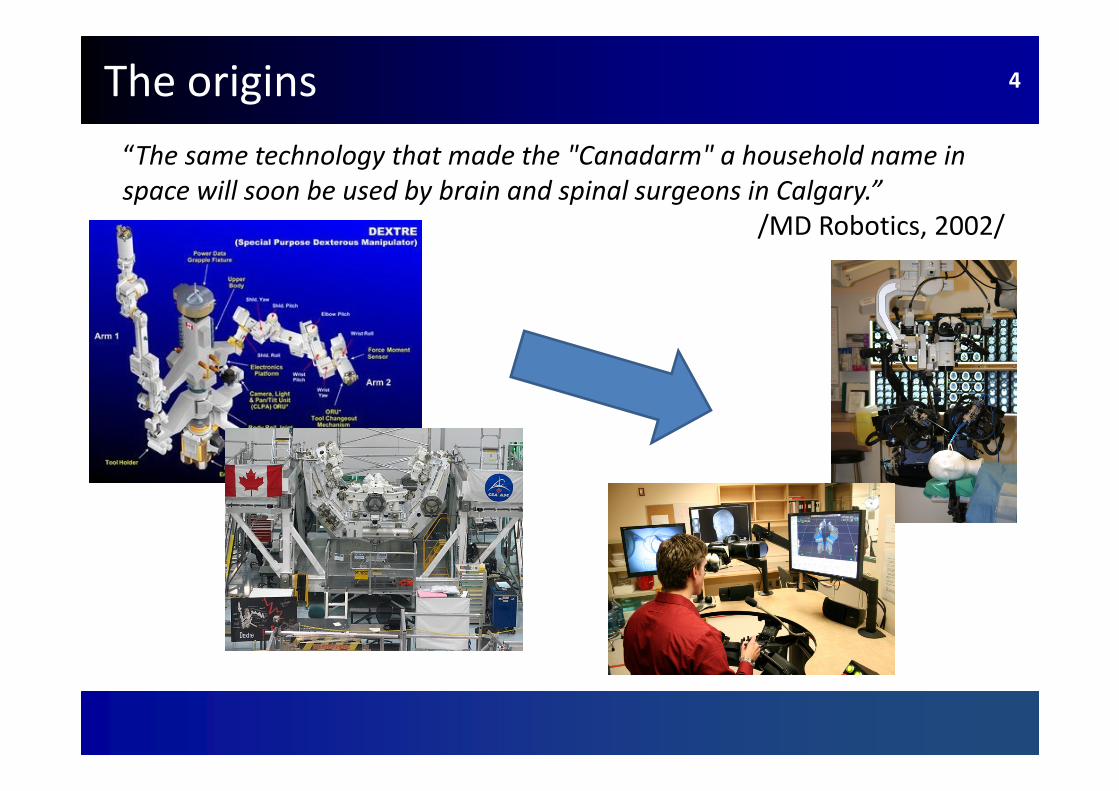
“The same technology that made the "Canadarm" a household name in
space will soon be used by brain and spinal surgeons in Calgary.”
/MD Robotics, 2002/
The origins 4
DARPA projekt 5
NASA Future In-Space Operations 07.27.2011.
Requirements for safe human space exploration
Sending humans to space 6
NASA Future In-Space Operations 07.27.2011.
• To meet the mission objectives � Ties to the military
• With best people� Thorough screening� Advanced technology � Ethical questions
• With the best tools to support� Best devices/equipment� Use of modern medtech� Computer-Integrated Surgery (CIS)� Simulate patients
Courtesy of Rick Satava
Motivation
“The future of surgery is not about blood and guts;
the future of surgery is about bits and bytes.”
/Rick Satava/
Clinical: healing lesions
• Reducing error margins during surgery
Imag
e c
red
it:
Eday
a
7
Engineering: applying technical innovation
• Conquering new fields
• Improving effectiveness, benefits while reducing costs
“If at first an idea is not absurd, then there is no hope for it.”
/Albert Einstein/
NASA Future In-Space Operations 07.27.2011.
A year at Johns HopkinsMotivation
Effective Space Medicine
Handling latency
Handling environmental constraints
Software support Hardware support
Human capability assessment
Skill training
8
Enabling technologies for remote operation• critical tasks: e.g. health care
Source: Joel Jensen, SRI International, Menlo Park, CA
MIS/open surgery
Pre-op planning
Intra-operative navigation
Telesurgery
Simulation, practice and warm-up
Sensor fusion
Robot-assisted surgery
New paradigm
in medicine
INFORMATION Augmented reality
Crew health management
Crew Health Care System (CHeCS)/ Integrated Medical System
• on the ISS
• on the Moon
• L1, L2
• beyond[Campbell 2008]
10
[Allen 2003]
Deployment of telemedicine 11
Risk control
Various metrics and standards
• Probability of serious illness or injury: 0.9
� 2.5-year-long Mars mission with six crew members [Allen 2003]
• Health Care Standard – Level of Care 5 recommended
� For any mission longer than 210 days; Johnson Space Center Space Medicine Division [NASA SFHSS, 2007]
• Probability of death during a mission: <0.03/year
� European Space Agency standard [Homeck 2001].
12
NASA Future In-Space Operations 07.27.2011.
DARPA projekt 13
NASA Future In-Space Operations 07.27.2011.
Robots for space medicine
Robotics for interventional medicine
• Seed idea: NASA should provide surgical care for astronauts with remote controlled robots [Alexander 1972]
• DoD finance for a battlefield remote rescue system [Satava 1995]
• Telesurgery systems Zeus and da Vinci made it out of lab
DARPA: Trauma Pod project
Operating Room of the Future
14
NASA Future In-Space Operations 07.27.2011.
Why robots?
[Taylor 1997]
NASA Future In-Space Operations 07.27.2011.
15
Teleoperating a robot
• Non time-critical teleoperation
• Time-critical teleoperation
NASA Future In-Space Operations 07.27.2011.
16
Exploration of unstructured,
dynamic environments
Facing the challenges
• Human-in-the-loop control
– Leave the mapping to the surgeon
• Registration (image) based
– Human oversight
Different approaches
Cre
dit
: C
UR
EX
O In
c.
Methods to improve the accuracy of treatment delivery
NASA Future In-Space Operations 07.27.2011.
17
DARPA projekt 18
NASA Future In-Space Operations 07.27.2011.
Current surgical robot systems and prototypes
master slave
Complete teleoperational system 19
NASA Future In-Space Operations 07.27.2011.
The da Vinci surgical system
• 1900 systems, 600 000++ operations, 120 types of procedures
Focusing on applicationsFrom Canadian experiments [Nguan 2008]• robotic data transport delay: 70 ms• commanded robotic motion on the patient side: 85.7 ms• CCD and camera controller latency: 20 ms• video transport delay: 70 ms• video compression/decompression (CODEC): 90 ms• video synchronizer delay: 33.6 ms
25
[Rayman 2007]
[Credit: CSTAR]
Human operator model
Classical control in telesurgical tasks
Simple master–slave teleoperation task
• equalizaQon type (look and move)―developed for pilots in the ‘60s• Possible to observe adaptation to latency
Cross-over model
Fitts’ law
Human learning
[McRuer 1965]
[Chien et al. 2010]
26
Human adaptation
Short/long term learning
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Based on various experiments
• Unnoticeable <100 ms• Most humans: max. 500 ms• Some might be able to adapt to 1000 ms• Jitter/consistent latency • Short term adaptation• Haptic feedback• Completion time, path length, forces
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
27
NASA Future In-Space Operations 07.27.2011.
[Rayman 2005]
[Tholey 2007]
Measuring adaptation
Reducing the degrees of freedom
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Fundamentals of Laparoscopic Surgery (FLS)
• Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
28
NASA Future In-Space Operations 07.27.2011.
[Lum 2008]
[Thompson 1999]
DARPA projekt 29
NASA Future In-Space Operations 07.27.2011.
Experiments and concepts to support teleoperation
over large distance
Teleoperation experiments— non-critical
Internet is the ultimate platform
• Using mostly UDP or TCP/IP• Internet latency is decreasing
� 85 ms across the U.S. (2009)� 400 ms world-wide
Telemedicine on the rise
• Simulated experiences, early ‘90s
• 1st telesurgery consultation, 1996
• 1st professional telementoring, 1997
• 1st international and mobile procedures, 1999
• 1st regular telemedicine network
(Centre for Minimal Access Surgery)
30
[Rayman 2005]
[Anvari 2004]
[Fabrizio 2000]
Telesurgical experiments—critical
Long range procedures around the world
The Lindbergh operation
• 7th Sept, 2001 • New York <---> Strasbourg• Hour-long gallbladder removal• Master setup in France Telecom office• Average latency: 150 ms
CSTAR
• Canadian Surgical Technologies and Advanced Robotics London (ON, Canada)
PlugFest 2009
• Telesurgery experiment w/14 systems world wide
• 21–112 ms latency for the U.S. • 115–305 ms for intercontinental
31
Credit: IRCAD
DARPA projektNEEMO 32
NASA Future In-Space Operations 07.27.2011.
32
NASA Extreme Environment Mission Operation
7th NEEMO (October, 2004)
● Reference procedures with a Zeus ● Telesurgery from 2500 km ● 0.1–2 s delay● Feasibility test for telementoring
9th NEEMO (April, 2006)
● Simulated procedures with M7 ● Test of wheeled in-vivo robots ● Satellite comm., up to 3s delay ● Telemedicine tests
12th NEEMO (May, 2007)
● Telesurgery with Raven and M7 robots ● Suturing test in zero gravity simulation● Laparoscopic object manipulation● Max. 1 s communication lag time ● Automated robotic operations
Concept of complete telemedical support
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Haidegger&Benyó2008
33
Concept of complete telemedical support I
■ Earth Orbit (near Earth):
. Classical telesurgery
� App. within 380 000km
� Under 2 s signal delay• Excellent for ISS• On Earth spin-offs
.
34
Enhancing human capabilities
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
35
VIDEO: UTwente‘s TELEFLEX HMI
Determining control models II
Slave robot model
Tissue characteristics
[Kawashima et al. 2008]
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization
efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization
efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization
efforts ¤ Case study ¤ ConclusionNASA Future In-Space Operations 07.27.2011.
36
Cascade control
Applicability• secondary loop dynamics must be faster than primary loop dynamics,• secondary loop must have influence on the primary loop,• secondary loop must be observable and controllable.
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
NASA Future In-Space Operations 07.27.2011.
37
Controller design methods
Empirical methods:
Kessler’s method extended to both loopsModulus Criteria (CM) or (Extended) Symmetrical Optimum (SO)
Soft computing methods:
PID–Fuzzy controllersModern control theories:
Model predictive methodsCommunication disturbance observers (ND – CDOB)
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Realistic control task
• Stability criteria• Bilateral and transparent teleoperation• Appropriate parameters• Tolerate 1 s delay in a telesurgical system
NASA Future In-Space Operations 07.27.2011.
38
Concept of complete telemedical support II
Middle range: Telementoring
� App. within 10 000 000km
� Under 50–70s signal delay
� Permanent video contact with the ground
39
40
Concept of complete telemedical support III
� Long distance: Consultancy telemedicine
� Within the range of the Mars
( 200 000 000 km)
� App. 10–40 min signal delay
� Preoperative simulations and consulting
� Prerecorded and locally adapted procedures
4040
Automation on the horizon
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
Outline ¤ Introduction ¤ Motivation ¤ Metrics in use ¤ Accuracy numbers ¤ Standardization efforts ¤ Case study ¤ Conclusion
41
We are in the age of intelligent tools • No real automation in the OR yet
• Automated manufacturing• Enhancement (e.g. tremor filtering, auto-navigation, camera handling)• Voice, eye-gaze control
VIDEOS: enhanced da Vinci robot at JHU; collaborative surgery; endosuturing device
DARPA projekt 42
NASA Future In-Space Operations 07.27.2011.
The real prospects of telesurgery in space
• Heavy weight, big size
• High R&D costs
– da Vinci was created with $0.5B investment
• Long development time
– From idea to product: 8–10 years
• Universality vs. added value
• Further uses of a robot on board
– To gain routine and to improve performance
– To conduct research, servicing
– For micromanipulation ops, repetitive functions
– Post-operative care
Cost / benefit 43
NASA Future In-Space Operations
SSSA
NTU
Environmental constraints
Surgery in weightlessness is challenging
Lack of experience
• Slower motion • Higher failure rate• Question of evaluation
• Diagnostics difficulties• Managing body fluids• Retraction
44
[Panait 2004]
[Rafiq 2005][Broderick 2005]
Surgery in space
NASA zero G experiments
• On board of a DC-9 hyperbolic aircraft• Simulated surgery (2007)• Suturing with M7 robot• Human control / automated task execution
Zero G surgeries
• Laparotomy and celiotomy on rabbits by cosmonauts (1967)• Feasibility of endoscopic surgery [Campbell 2001]• First survival surgery in weightlessness on a rat (2003)• Removal of a cyst from the arm of a human (2006)
• Through 25 parabolic sessions of microgravity• ESA Zero-G plane (modified Airbus A-300)
Non-invasive diagnostics on the ISS
• Ultra Sound experiments• BioLab module within Columbus
Cre
dit
: ES
A, N
ASA
45
DARPA projektOther requirements 46
NASA Future In-Space Operations 07.27.2011.
Software infrastructure
• Complete health monitoring system• On-line clinical information database access• Strategic health care research planner
(for data analysis and support)
• Medical knowledge base (to identify the risks and hazards)
• Astronauts should receive comprehensive medical training
On Earth support• Terrestrial health support centre• Complete surgical simulator on Earth• Multimodal physiologic model of astronauts
(for reference on health status)
DARPA projektConclusion 47
NASA Future In-Space Operations 07.27.2011.
Teleoperation through time-delayed channels is challenging • Various hardware and software issues• Question of human adaptation• Lack of standards (both for instruments and communication)• Ethical issues
• User confidence
Space medicine is also hard • Physical and ergonomical challenges• Environmental constraints
Fundamental research is required to develop the science behind
Thank you for your attention!
SurgRoba blog on CIS and medical robotics
http://surgrob.blogspot.com
Post script
Thesis is available: http://tinyurl.com/3v3dmwt
IEEE RAS society 50
• http://ieee-ras.org
Acknowledgment
My research projects were funded by:
Austrian COMET-K1, EU FP7-PEOPLE-2009-IIF,
US NSF EEC 9731748, Hungarian NKTH OTKA T80316,New Hungary Development Plan
(Project ID: TAMOP-4.2.1/B-09/1/KMR-2010-0002)
Stiftung Aktion Österreich-Ungarn (AÖU) grants
I am deeply grateful to all my supervisors, colleagues and students.