14 FEATURE by Goutam Brahmachari Laboratory of Natural Products and Organic Synthesis, Department of Chemistry, Visva-Bharati University, Santiniketan-732 235, West Bengal, India [email protected]Natural Products in the Drug Discovery Programmes in Alzheimer’s: Impacts and Prospects
Transcript
14
FEATURE
by Goutam BrahmachariLaboratory of Natural Products and Organic Synthesis, Department of Chemistry,
Visva-Bharati University, Santiniketan-732 235, West Bengal, [email protected]
Natural Products in the Drug Discovery Programmes in
Alzheimer’s: Impacts and Prospects
15
FEATURE
In 1906 Dr. Alois Alzheimer, a German psychiatrist and neuropathologist, described the first published case of
“presenile dementia” based on the observation of amyloid plaques, neurofibrillary tangles and vascular anomalies during the autopsy of his patient, Mrs. Auguste Deter who had died 7 months earlier with severe cognitive defects,1 and the disease became known as Alzheimer’s disease (AD) or simply Alzheimer’s after the name of the inventor.2 Alzheimer’s, a progressive neurodegenerative disorder leading to the most common form of dementia, very particularly in elderly people, has already affected approximately 36 million population worldwide as of 2010;3 it is a matter of great concern that 1,000 new cases of AD are reported daily throughout the United States.4 Such neurodegenerative disease is characterized by progressive and irreversible decline of memory and other cognitive functions including language, judgment, reasoning along with progressive loss of physical functioning and associated neuropsychiatric symptoms, which become severe enough to impede social or occupational functioning.5
Although other major causes of death have been decreasing, deaths attributable to AD have been rising dramatically. Between 2000 and 2006, cardiovascular mortality decreased 11.1%, stroke deaths decreased 18.2%, and prostate cancer-related deaths decreased 8.7%, whereas deaths attributed to AD increased 46.1%.6 In fact, the overall case number in developed countries is estimated to increase by 100% between 2001 and 2040, but by more than 300% in India and China. Recent estimates indicate that nearly 5 million additional new dementia cases are diagnosed per year. Alzheimer’s is predicted to affect 1 in 85 people globally by 2050.7 The 2003 World Health Report estimates that dementing diseases contribute a greater overall burden of disability than cardiovascular disease, stroke, and cancer.
Neuropathology of ADDespite decades of research and many s i gn i f i can t advances , the p rec i s e neuropathology of AD is still not completely understood; however, amyloid plaques and
neurofibrillary tangles are considered as the two primary pathological hallmarks of the disease. Histopathological studies of the AD brain revealed dramatic ultra-structural changes triggered by two classical lesions, the senile plaques, mainly composed of amyloid-β (Aβ) peptides, and the neurofibrillary tangles, composed of hyperphosphorylated tau proteins.8,9 Amyloid plaques are insoluble, dense cores of 5-10 nm fibrils containing aggregates of amyloid precursor protein (APP) fragments that are primarily composed 42-amino acid β-amyloid peptide (Αβ42) as found in AD patients.10–12 On the other hand, neurofibrillary tangles contain aggregates of phosphorylated tau, a microtubule-associated protein. Some hypotheses of Alzheimer’s pathology suggest that the aggregation of hyperphosphorylated tau protein causes the degeneration of the microtubule network required for neuronal survival.13 Ultimately, the insoluble neurofibrillary tangle of tau protein is left as a “tombstone” for dead neurons.
Although neurofibrillary tangles can occur independently, and cause neuronal death in frontotemporal dementia,14 the presence of both lesions in the neocortex is essential to the diagnosis of AD. The pathogenesis of the disease is complex and is driven by both environmental and genetic factors. The molecular identification and
characterization of different genes associated with familial AD has provided strong support to the so-called amyloid cascade hypothesis as a causative event in the pathogenesis of AD.15 This hypothesis states that Aβ generated from deregulated proteolysis of the amyloid precursor protein (APP) undergoes accelerated Aβ oligomerization, fibril formation, and amyloid deposition in a process that initiates the AD pathology.15 In the past ten years, the large majority of the pharmacological research on AD has focused on understanding how Aβ is generated from APP via β- and γ-secretase cleavages, with the goal of designing specific inhibitors that will block Aβ production and the associated pathology. Besides, newer approaches aimed at better understanding of various molecular pathways involved in Aβ clearance have been gaining considerable attention over the last several years.16,17
The inflammatory response to the deposition of these amyloid plaques and neurofibrillary tangles is thought to play an important role in producing the “halo” of degenerated neurons, reactive astrocytes and activated microglia around these protein deposits that is observed in microscopic sections.18 Over time there is gross atrophy of affected regions, including the temporal, parietal, frontal lobes (in particular the
Dr. Alois Alzheimer
16
FEATURE
ventral forebrain), and the cingulate gyrus. Eventually, neuronal loss leads to global neurotransmitter deficiencies, specifically in norepinephrine and acetylcholine.
One of the earliest molecular observations in AD was the finding of a deficiency of overall acetylcholine and decreased activity of enzymes involved in the synthesis and degradation of this neurotransmitter in AD autopsy and biopsy tissue.19,20 During the course of the disease plaques and tangles develop within the structure of the brain. This causes brain cells to die. Current models suggest a prodromal period of amyloid accumulation, followed by a progression of tau pathology, inflammation, and neurodegeneration that tracks cognitive decline. Oxidative damage to proteins, lipids, and DNA in the brains of AD patients likely accompanies the widespread inflammation.
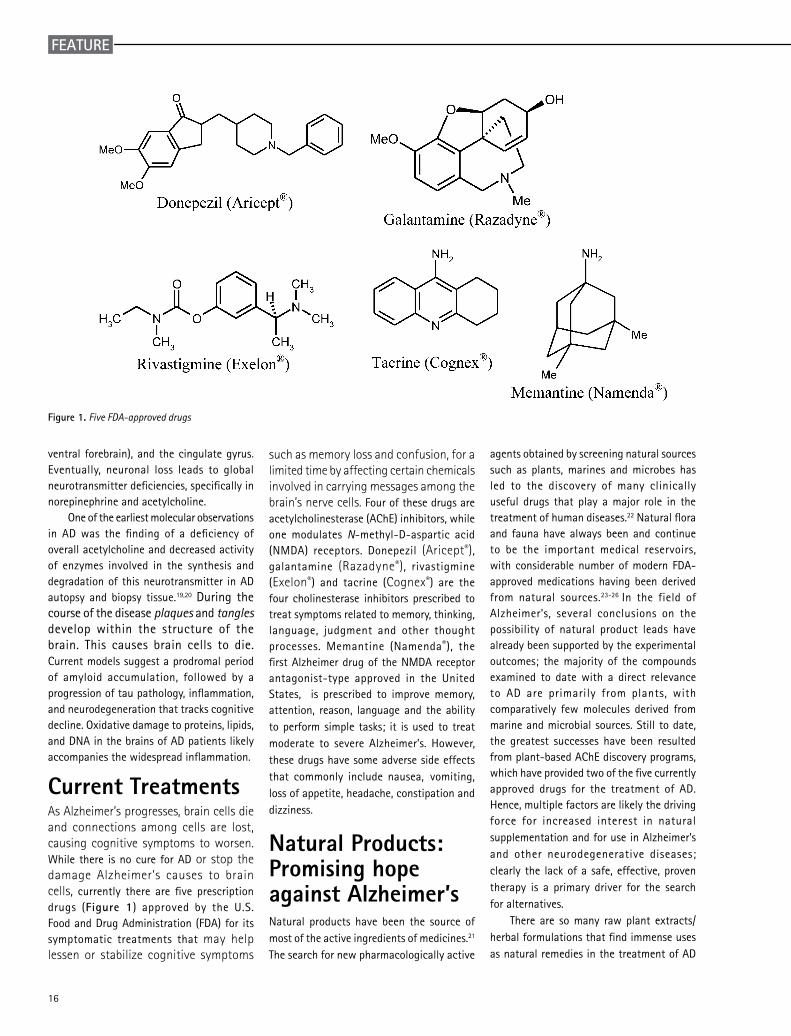
Current Treatments As Alzheimer’s progresses, brain cells die and connections among cells are lost, causing cognitive symptoms to worsen. While there is no cure for AD or stop the damage Alzheimer’s causes to brain cells, currently there are five prescription drugs (Figure 1) approved by the U.S. Food and Drug Administration (FDA) for its symptomatic treatments that may help lessen or stabilize cognitive symptoms
such as memory loss and confusion, for a limited time by affecting certain chemicals involved in carrying messages among the brain’s nerve cells. Four of these drugs are acetylcholinesterase (AChE) inhibitors, while one modulates N-methyl-D-aspartic acid (NMDA) receptors. Donepezil (Aricept®), galantamine (Razadyne®), rivastigmine (Exelon®) and tacrine (Cognex®) are the four cholinesterase inhibitors prescribed to treat symptoms related to memory, thinking, language, judgment and other thought processes. Memantine (Namenda®), the first Alzheimer drug of the NMDA receptor antagonist-type approved in the United States, is prescribed to improve memory, attention, reason, language and the ability to perform simple tasks; it is used to treat moderate to severe Alzheimer’s. However, these drugs have some adverse side effects that commonly include nausea, vomiting, loss of appetite, headache, constipation and dizziness.
Natural Products: Promising hope against Alzheimer’s Natural products have been the source of most of the active ingredients of medicines.21 The search for new pharmacologically active
Figure 1. Five FDA-approved drugs
agents obtained by screening natural sources such as plants, marines and microbes has led to the discovery of many clinically useful drugs that play a major role in the treatment of human diseases.22 Natural flora and fauna have always been and continue to be the important medical reservoirs, with considerable number of modern FDA-approved medications having been derived from natural sources.23-26 In the field of Alzheimer’s, several conclusions on the possibility of natural product leads have already been supported by the experimental outcomes; the majority of the compounds examined to date with a direct relevance to AD are primarily from plants, with comparatively few molecules derived from marine and microbial sources. Still to date, the greatest successes have been resulted from plant-based AChE discovery programs, which have provided two of the five currently approved drugs for the treatment of AD. Hence, multiple factors are likely the driving force for increased interest in natural supplementation and for use in Alzheimer’s and other neurodegenerative diseases; clearly the lack of a safe, effective, proven therapy is a primary driver for the search for alternatives.
There are so many raw plant extracts/herbal formulations that find immense uses as natural remedies in the treatment of AD
17
FEATURE
and other neurodegenerative diseases.27-31 Essentially, all traditional natural medical systems including Chinese, Indian, Native American, and medieval European have had various “brain tonics” and memory enhancers.32-42 These include “Ashwagandha” (Withania somnifera; Solanaceae) and Brahmi (Bacopa monnieri L. Pennell; Scophulariaceae) mentioned in Indian Ayurveda as memory enhancers, the common ‘Sage’ plants (Salvia species; Labiatae) described in Roman texts as being “good for the memory”, and Gingko biloba (Ginkgoaceae) discussed in Chinese literature as a possible remedy for memory loss as early as 2800 BC. Indian turmeric (Curcuma longa; Zingiberaceae), which contains an antioxidant and anti-inflammatory compound called curcumin, is found to be very effective in the treatment of AD. Vegetables such as pumpkin, carrot and other foods and spices like zinger, sesame and
sunflower seeds that contain various chemical agents find very useful for enhancing the function of the brain. Consumption of blueberries/grapes and pomegranate juice has recently been proven to have beneficial effect in AD. Food supplements of vitamin B
6 & B12, folic acid, vitamin E, vitamin C and co-enzyme Q10 also have been found to exert beneficial effect in AD patients.
Numerous literatures are available on the chemical, pharmacological and clinical studies of natural substances used in the treatment of AD and related diseases, including their medicinal efficacy, safety, and other relevant matters. Good review articles have also been published detailing on the naturally occurring compounds of varying skeletons that showed potential efficacy against AD and other neurodegenerative disorders.27,44-45 More than 200 compounds of natural origin are reported so far to
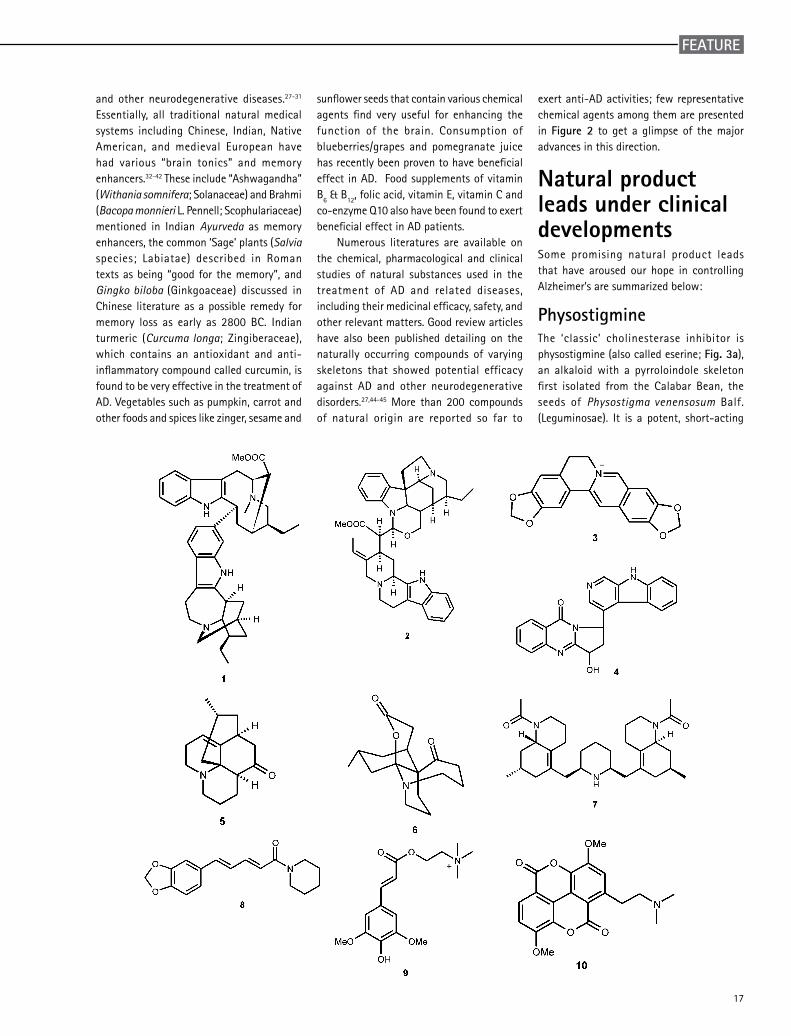
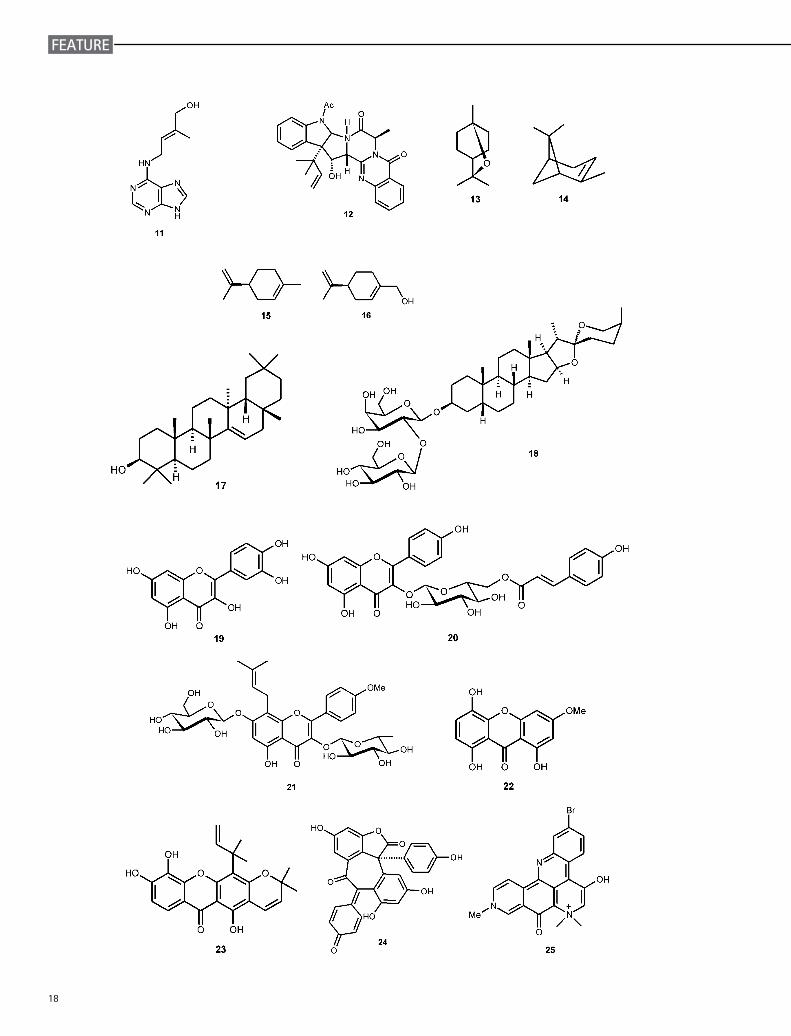
exert anti-AD activities; few representative chemical agents among them are presented in Figure 2 to get a glimpse of the major advances in this direction.
Natural product leads under clinical developments Some promising natural product leads that have aroused our hope in controlling Alzheimer’s are summarized below:
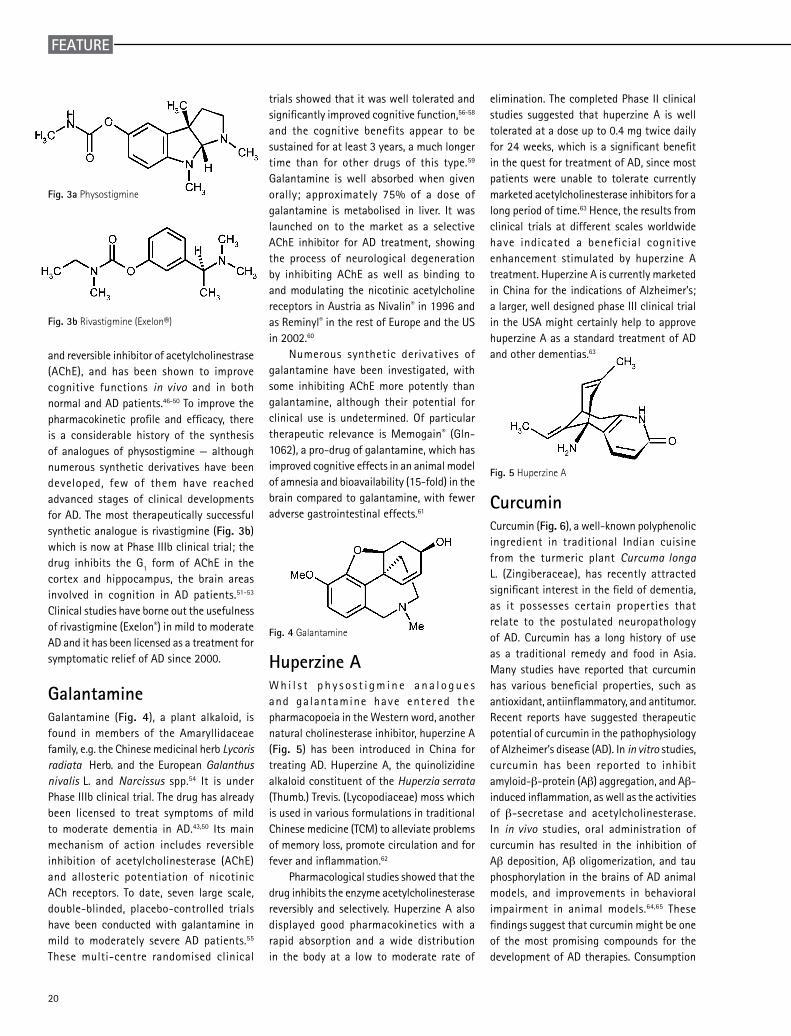
PhysostigmineThe ‘classic’ cholinesterase inhibitor is physostigmine (also called eserine; Fig. 3a), an alkaloid with a pyrroloindole skeleton first isolated from the Calabar Bean, the seeds of Physostigma venensosum Balf. (Leguminosae). It is a potent, short-acting
18
FEATURE
19
FEATURE
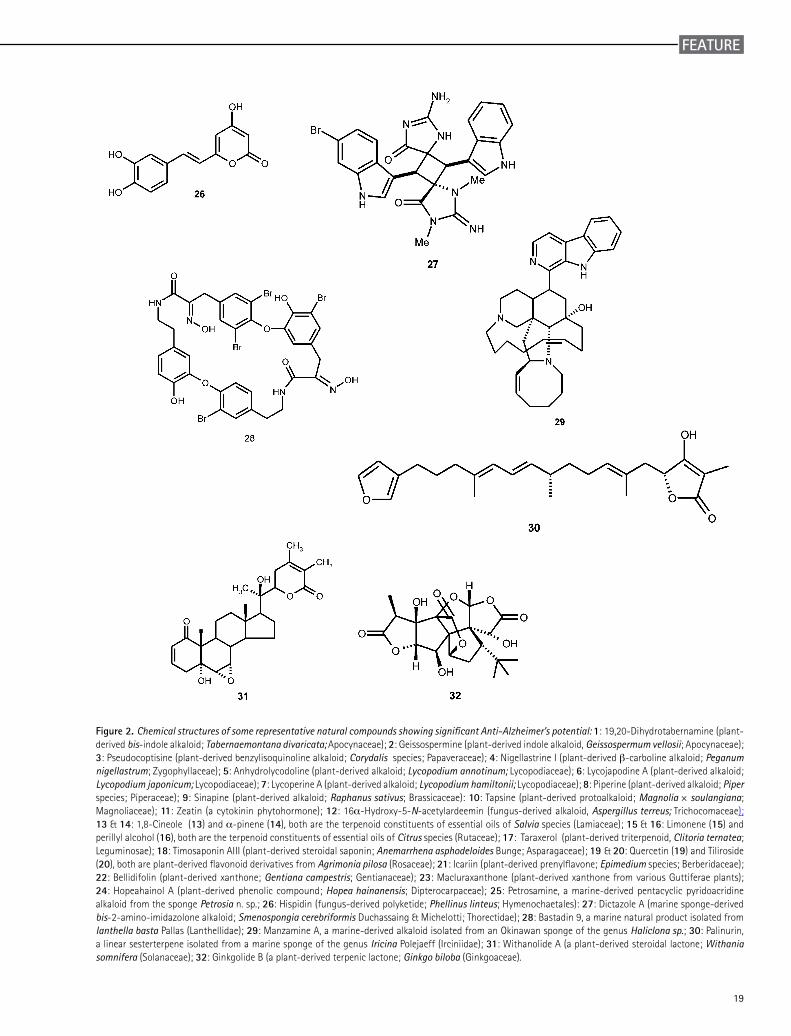
Figure 2. Chemical structures of some representative natural compounds showing significant Anti-Alzheimer’s potential: 1: 19,20-Dihydrotabernamine (plant-derived bis-indole alkaloid; Tabernaemontana divaricata; Apocynaceae); 2: Geissospermine (plant-derived indole alkaloid, Geissospermum vellosii; Apocynaceae); 3: Pseudocoptisine (plant-derived benzylisoquinoline alkaloid; Corydalis species; Papaveraceae); 4: Nigellastrine I (plant-derived β-carboline alkaloid; Peganum nigellastrum; Zygophyllaceae); 5: Anhydrolycodoline (plant-derived alkaloid; Lycopodium annotinum; Lycopodiaceae); 6: Lycojapodine A (plant-derived alkaloid; Lycopodium japonicum; Lycopodiaceae); 7: Lycoperine A (plant-derived alkaloid; Lycopodium hamiltonii; Lycopodiaceae); 8: Piperine (plant-derived alkaloid; Piper species; Piperaceae); 9: Sinapine (plant-derived alkaloid; Raphanus sativus; Brassicaceae): 10: Tapsine (plant-derived protoalkaloid; Magnolia × soulangiana; Magnoliaceae); 11: Zeatin (a cytokinin phytohormone); 12: 16α-Hydroxy-5-N-acetylardeemin (fungus-derived alkaloid, Aspergillus terreus; Trichocomaceae); 13 & 14: 1,8-Cineole (13) and α-pinene (14), both are the terpenoid constituents of essential oils of Salvia species (Lamiaceae); 15 & 16: Limonene (15) and perillyl alcohol (16), both are the terpenoid constituents of essential oils of Citrus species (Rutaceae); 17: Taraxerol (plant-derived triterpenoid, Clitoria ternatea; Leguminosae); 18: Timosaponin AIII (plant-derived steroidal saponin; Anemarrhena asphodeloides Bunge; Asparagaceae); 19 & 20: Quercetin (19) and Tiliroside (20), both are plant-derived flavonoid derivatives from Agrimonia pilosa (Rosaceae); 21: Icariin (plant-derived prenylflavone; Epimedium species; Berberidaceae); 22: Bellidifolin (plant-derived xanthone; Gentiana campestris; Gentianaceae); 23: Macluraxanthone (plant-derived xanthone from various Guttiferae plants); 24: Hopeahainol A (plant-derived phenolic compound; Hopea hainanensis; Dipterocarpaceae); 25: Petrosamine, a marine-derived pentacyclic pyridoacridine alkaloid from the sponge Petrosia n. sp.; 26: Hispidin (fungus-derived polyketide; Phellinus linteus; Hymenochaetales): 27: Dictazole A (marine sponge-derived bis-2-amino-imidazolone alkaloid; Smenospongia cerebriformis Duchassaing & Michelotti; Thorectidae); 28: Bastadin 9, a marine natural product isolated from Ianthella basta Pallas (Lanthellidae); 29: Manzamine A, a marine-derived alkaloid isolated from an Okinawan sponge of the genus Haliclona sp.; 30: Palinurin, a linear sesterterpene isolated from a marine sponge of the genus Iricina Polejaeff (Irciniidae); 31: Withanolide A (a plant-derived steroidal lactone; Withania somnifera (Solanaceae); 32: Ginkgolide B (a plant-derived terpenic lactone; Ginkgo biloba (Ginkgoaceae).
20
FEATURE
and reversible inhibitor of acetylcholinestrase (AChE), and has been shown to improve cognitive functions in vivo and in both normal and AD patients.46-50 To improve the pharmacokinetic profile and efficacy, there is a considerable history of the synthesis of analogues of physostigmine — although numerous synthetic derivatives have been developed, few of them have reached advanced stages of clinical developments for AD. The most therapeutically successful synthetic analogue is rivastigmine (Fig. 3b) which is now at Phase IIIb clinical trial; the drug inhibits the G1 form of AChE in the cortex and hippocampus, the brain areas involved in cognition in AD patients.51-53 Clinical studies have borne out the usefulness of rivastigmine (Exelon®) in mild to moderate AD and it has been licensed as a treatment for symptomatic relief of AD since 2000.
Galantamine Galantamine (Fig. 4), a plant alkaloid, is found in members of the Amaryllidaceae family, e.g. the Chinese medicinal herb Lycoris radiata Herb. and the European Galanthus nivalis L. and Narcissus spp.54 It is under Phase IIIb clinical trial. The drug has already been licensed to treat symptoms of mild to moderate dementia in AD.43,50 Its main mechanism of action includes reversible inhibition of acetylcholinesterase (AChE) and allosteric potentiation of nicotinic ACh receptors. To date, seven large scale, double-blinded, placebo-controlled trials have been conducted with galantamine in mild to moderately severe AD patients.55 These multi-centre randomised clinical
Fig. 3a Physostigmine
Fig. 3b Rivastigmine (Exelon®)
trials showed that it was well tolerated and significantly improved cognitive function,56-58 and the cognitive benefits appear to be sustained for at least 3 years, a much longer time than for other drugs of this type.59 Galantamine is well absorbed when given orally; approximately 75% of a dose of galantamine is metabolised in liver. It was launched on to the market as a selective AChE inhibitor for AD treatment, showing the process of neurological degeneration by inhibiting AChE as well as binding to and modulating the nicotinic acetylcholine receptors in Austria as Nivalin® in 1996 and as Reminyl® in the rest of Europe and the US in 2002.60
Numerous synthetic derivatives of galantamine have been investigated, with some inhibiting AChE more potently than galantamine, although their potential for clinical use is undetermined. Of particular therapeutic relevance is Memogain® (Gln-1062), a pro-drug of galantamine, which has improved cognitive effects in an animal model of amnesia and bioavailability (15-fold) in the brain compared to galantamine, with fewer adverse gastrointestinal effects.61
Fig. 4 Galantamine
Huperzine A W h i l s t p h y s o s t i g m i n e a n a l o g u e s and galantamine have entered the pharmacopoeia in the Western word, another natural cholinesterase inhibitor, huperzine A (Fig. 5) has been introduced in China for treating AD. Huperzine A, the quinolizidine alkaloid constituent of the Huperzia serrata (Thumb.) Trevis. (Lycopodiaceae) moss which is used in various formulations in traditional Chinese medicine (TCM) to alleviate problems of memory loss, promote circulation and for fever and inflammation.62
Pharmacological studies showed that the drug inhibits the enzyme acetylcholinesterase reversibly and selectively. Huperzine A also displayed good pharmacokinetics with a rapid absorption and a wide distribution in the body at a low to moderate rate of
elimination. The completed Phase II clinical studies suggested that huperzine A is well tolerated at a dose up to 0.4 mg twice daily for 24 weeks, which is a significant benefit in the quest for treatment of AD, since most patients were unable to tolerate currently marketed acetylcholinesterase inhibitors for a long period of time.63 Hence, the results from clinical trials at different scales worldwide have indicated a beneficial cognitive enhancement stimulated by huperzine A treatment. Huperzine A is currently marketed in China for the indications of Alzheimer’s; a larger, well designed phase III clinical trial in the USA might certainly help to approve huperzine A as a standard treatment of AD and other dementias.63
Fig. 5 Huperzine A
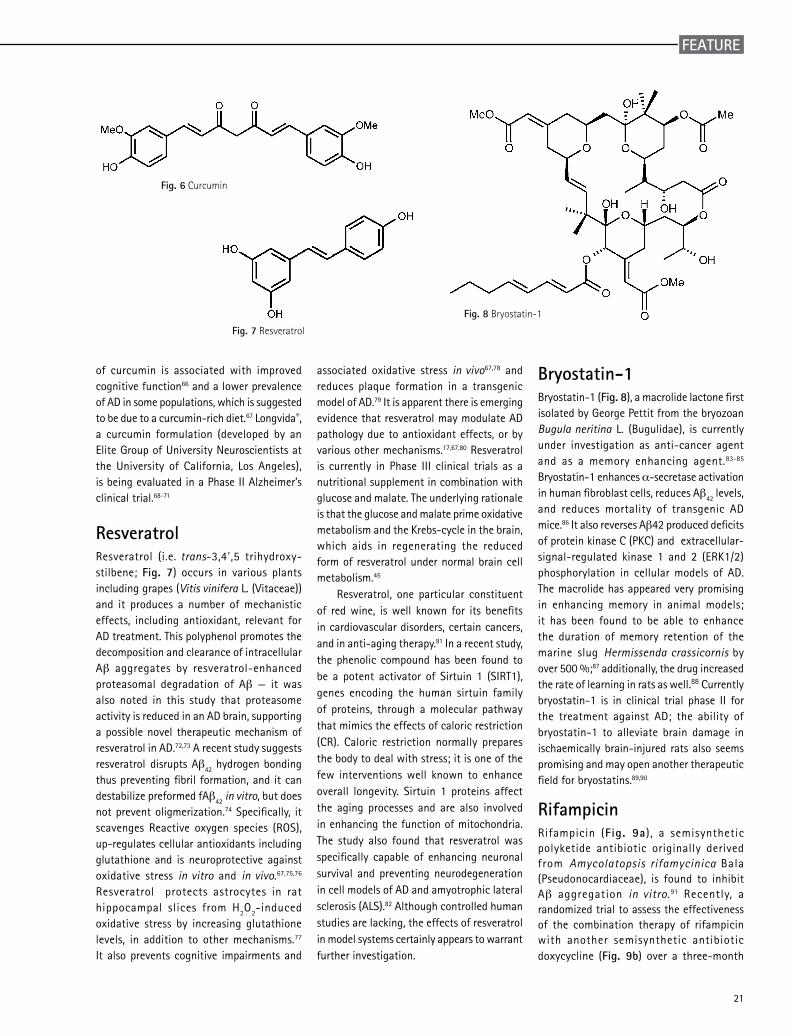
Curcumin Curcumin (Fig. 6), a well-known polyphenolic ingredient in traditional Indian cuisine from the turmeric plant Curcuma longa L. (Zingiberaceae), has recently attracted significant interest in the field of dementia, as it possesses certain properties that relate to the postulated neuropathology of AD. Curcumin has a long history of use as a traditional remedy and food in Asia. Many studies have reported that curcumin has various beneficial properties, such as antioxidant, antiinflammatory, and antitumor. Recent reports have suggested therapeutic potential of curcumin in the pathophysiology of Alzheimer’s disease (AD). In in vitro studies, curcumin has been reported to inhibit amyloid-β-protein (Aβ) aggregation, and Aβ-induced inflammation, as well as the activities of β-secretase and acetylcholinesterase. In in vivo studies, oral administration of curcumin has resulted in the inhibition of Aβ deposition, Aβ oligomerization, and tau phosphorylation in the brains of AD animal models, and improvements in behavioral impairment in animal models.64,65 These findings suggest that curcumin might be one of the most promising compounds for the development of AD therapies. Consumption
21
FEATURE
of curcumin is associated with improved cognitive function66 and a lower prevalence of AD in some populations, which is suggested to be due to a curcumin-rich diet.67 Longvida®, a curcumin formulation (developed by an Elite Group of University Neuroscientists at the University of California, Los Angeles), is being evaluated in a Phase II Alzheimer’s clinical trial.68-71
ResveratrolResveratrol (i.e. trans-3,4′,5 trihydroxy-stilbene; Fig. 7) occurs in various plants including grapes (Vitis vinifera L. (Vitaceae)) and it produces a number of mechanistic effects, including antioxidant, relevant for AD treatment. This polyphenol promotes the decomposition and clearance of intracellular Aβ aggregates by resveratrol-enhanced proteasomal degradation of Aβ — it was also noted in this study that proteasome activity is reduced in an AD brain, supporting a possible novel therapeutic mechanism of resveratrol in AD.72,73 A recent study suggests resveratrol disrupts Aβ42 hydrogen bonding thus preventing fibril formation, and it can destabilize preformed fAβ42 in vitro, but does not prevent oligmerization.74 Specifically, it scavenges Reactive oxygen species (ROS), up-regulates cellular antioxidants including glutathione and is neuroprotective against oxidative stress in vitro and in vivo.67,75,76
Resveratrol protects astrocytes in rat hippocampal slices from H2O2-induced oxidative stress by increasing glutathione levels, in addition to other mechanisms.77 It also prevents cognitive impairments and
Fig. 6 Curcumin
associated oxidative stress in vivo67,78 and reduces plaque formation in a transgenic model of AD.79 It is apparent there is emerging evidence that resveratrol may modulate AD pathology due to antioxidant effects, or by various other mechanisms.17,67,80 Resveratrol is currently in Phase III clinical trials as a nutritional supplement in combination with glucose and malate. The underlying rationale is that the glucose and malate prime oxidative metabolism and the Krebs-cycle in the brain, which aids in regenerating the reduced form of resveratrol under normal brain cell metabolism.45
Resveratrol, one particular constituent of red wine, is well known for its benefits in cardiovascular disorders, certain cancers, and in anti-aging therapy.81 In a recent study, the phenolic compound has been found to be a potent activator of Sirtuin 1 (SIRT1), genes encoding the human sirtuin family of proteins, through a molecular pathway that mimics the effects of caloric restriction (CR). Caloric restriction normally prepares the body to deal with stress; it is one of the few interventions well known to enhance overall longevity. Sirtuin 1 proteins affect the aging processes and are also involved in enhancing the function of mitochondria. The study also found that resveratrol was specifically capable of enhancing neuronal survival and preventing neurodegeneration in cell models of AD and amyotrophic lateral sclerosis (ALS).82 Although controlled human studies are lacking, the effects of resveratrol in model systems certainly appears to warrant further investigation.
Fig. 7 Resveratrol
Bryostatin-1 Bryostatin-1 (Fig. 8), a macrolide lactone first isolated by George Pettit from the bryozoan Bugula neritina L. (Bugulidae), is currently under investigation as anti-cancer agent and as a memory enhancing agent.83-85 Bryostatin-1 enhances α-secretase activation in human fibroblast cells, reduces Aβ42 levels, and reduces mortality of transgenic AD mice.86 It also reverses Aβ42 produced deficits of protein kinase C (PKC) and extracellular-signal-regulated kinase 1 and 2 (ERK1/2) phosphorylation in cellular models of AD. The macrolide has appeared very promising in enhancing memory in animal models; it has been found to be able to enhance the duration of memory retention of the marine slug Hermissenda crassicornis by over 500 %;87 additionally, the drug increased the rate of learning in rats as well.88 Currently bryostatin-1 is in clinical trial phase II for the treatment against AD; the ability of bryostatin-1 to alleviate brain damage in ischaemically brain-injured rats also seems promising and may open another therapeutic field for bryostatins.89,90
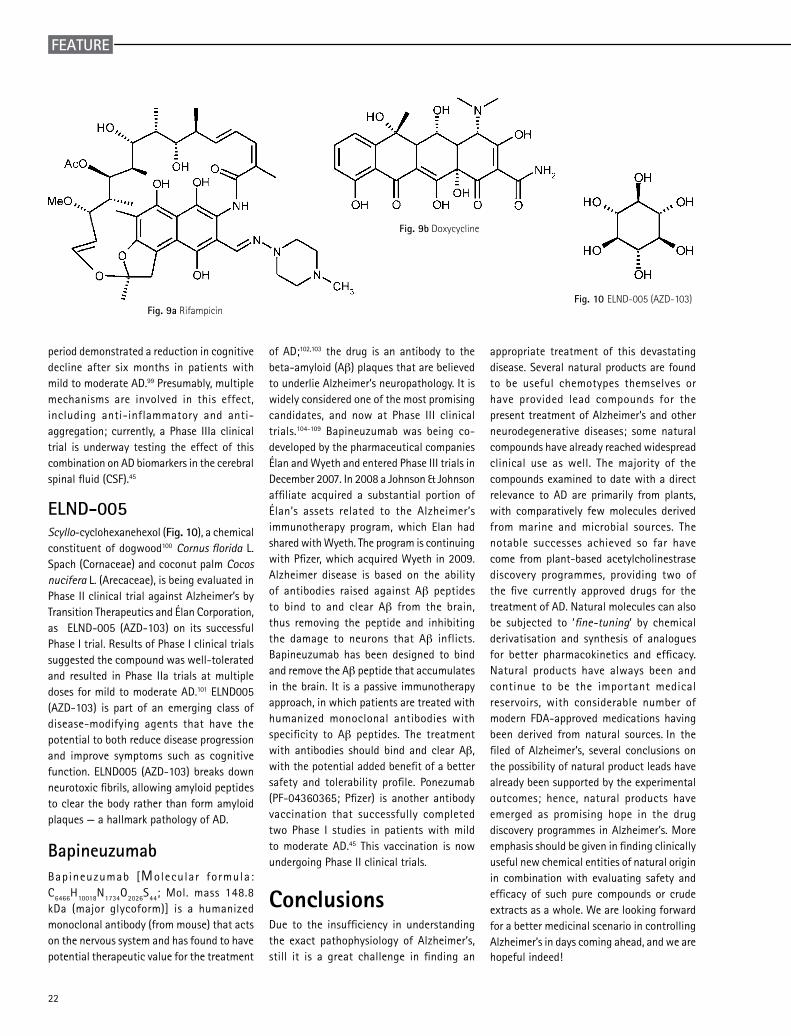
Rifampicin Rifampicin (Fig. 9a), a semisynthetic polyketide antibiotic originally derived from Amycolatopsis rifamycinica Bala (Pseudonocardiaceae), is found to inhibit Aβ aggregation in vitro.91 Recently, a randomized trial to assess the effectiveness of the combination therapy of rifampicin with another semisynthetic antibiotic doxycycline (Fig. 9b) over a three-month
Fig. 8 Bryostatin-1
22
FEATURE
period demonstrated a reduction in cognitive decline after six months in patients with mild to moderate AD.99 Presumably, multiple mechanisms are involved in this effect, including anti-inflammatory and anti-aggregation; currently, a Phase IIIa clinical trial is underway testing the effect of this combination on AD biomarkers in the cerebral spinal fluid (CSF).45
ELND-005 Scyllo-cyclohexanehexol (Fig. 10), a chemical constituent of dogwood100 Cornus florida L. Spach (Cornaceae) and coconut palm Cocos nucifera L. (Arecaceae), is being evaluated in Phase II clinical trial against Alzheimer’s by Transition Therapeutics and Élan Corporation, as ELND-005 (AZD-103) on its successful Phase I trial. Results of Phase I clinical trials suggested the compound was well-tolerated and resulted in Phase IIa trials at multiple doses for mild to moderate AD.101 ELND005 (AZD-103) is part of an emerging class of disease-modifying agents that have the potential to both reduce disease progression and improve symptoms such as cognitive function. ELND005 (AZD-103) breaks down neurotoxic fibrils, allowing amyloid peptides to clear the body rather than form amyloid plaques — a hallmark pathology of AD.
Bapineuzumab Bapineuzumab [Molecular formula: C6466H10018N1734O2026S44; Mol. mass 148.8 kDa (major glycoform)] is a humanized monoclonal antibody (from mouse) that acts on the nervous system and has found to have potential therapeutic value for the treatment
Fig. 10 ELND-005 (AZD-103)
of AD;102,103 the drug is an antibody to the beta-amyloid (Aβ) plaques that are believed to underlie Alzheimer’s neuropathology. It is widely considered one of the most promising candidates, and now at Phase III clinical trials.104-109 Bapineuzumab was being co-developed by the pharmaceutical companies Élan and Wyeth and entered Phase III trials in December 2007. In 2008 a Johnson & Johnson affiliate acquired a substantial portion of Élan’s assets related to the Alzheimer’s immunotherapy program, which Elan had shared with Wyeth. The program is continuing with Pfizer, which acquired Wyeth in 2009. Alzheimer disease is based on the ability of antibodies raised against Aβ peptides to bind to and clear Aβ from the brain, thus removing the peptide and inhibiting the damage to neurons that Aβ inflicts. Bapineuzumab has been designed to bind and remove the Aβ peptide that accumulates in the brain. It is a passive immunotherapy approach, in which patients are treated with humanized monoclonal antibodies with specificity to Aβ peptides. The treatment with antibodies should bind and clear Aβ, with the potential added benefit of a better safety and tolerability profile. Ponezumab (PF-04360365; Pfizer) is another antibody vaccination that successfully completed two Phase I studies in patients with mild to moderate AD.45 This vaccination is now undergoing Phase II clinical trials.
Conclusions Due to the insufficiency in understanding the exact pathophysiology of Alzheimer’s, still it is a great challenge in finding an
appropriate treatment of this devastating disease. Several natural products are found to be useful chemotypes themselves or have provided lead compounds for the present treatment of Alzheimer’s and other neurodegenerative diseases; some natural compounds have already reached widespread clinical use as well. The majority of the compounds examined to date with a direct relevance to AD are primarily from plants, with comparatively few molecules derived from marine and microbial sources. The notable successes achieved so far have come from plant-based acetylcholinestrase discovery programmes, providing two of the five currently approved drugs for the treatment of AD. Natural molecules can also be subjected to ‘fine-tuning’ by chemical derivatisation and synthesis of analogues for better pharmacokinetics and efficacy. Natural products have always been and continue to be the important medical reservoirs, with considerable number of modern FDA-approved medications having been derived from natural sources. In the filed of Alzheimer’s, several conclusions on the possibility of natural product leads have already been supported by the experimental outcomes; hence, natural products have emerged as promising hope in the drug discovery programmes in Alzheimer’s. More emphasis should be given in finding clinically useful new chemical entities of natural origin in combination with evaluating safety and efficacy of such pure compounds or crude extracts as a whole. We are looking forward for a better medicinal scenario in controlling Alzheimer’s in days coming ahead, and we are hopeful indeed!
Fig. 9a Rifampicin
Fig. 9b Doxycycline
23
FEATURE
References
1. Alzheimer, A. Über eine eigenartige Erkrankung der Hirnrinde. Allg. Z. Psychiat. Psych.-Gerichtl. Med., 64: 146–148, 1907; Alzheimer A, Centrablat fur Nevenheilkunde Psychiatrie, 30: 177–179, 1907.2. Berchtold NC, Cotman CW, Evolution in the conceptualization of dementia and Alzheimer’s disease: Greco-Roman period to the 1960s. Neurobiol Aging, 19: 173–819, 1998.3. Alzheimer’s Disease International, World Alzheimer Report, 1–24. 2009.4. Hebert LE, Scherr PA, Bennett DR, Evans DA, Alzheimer disease in the US population: prevalence estimates using the 2000 census. Arch Neurol, 61: 802–803, 2004.5. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), 4th edition, American Psychiatric Association, Washington, DC, American Psychiatric Press Inc, 1994.6. Alzheimer’s Association, 2010 Alzheimer’s disease facts and figures. Alzheimer’s Dement, 6: 158–194, 2010.7. Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM, Forecasting the global burden of Alzheimer’s disease. Alzheimer’s Dement, 3: 186–191, 2007. 8. Selkoe DJ, Alzheimer’s disease: genes, proteins, and therapy. Physiol Rev, 81: 741–766, 2001.9. Davies P, A very incomplete comprehensive theory of Alzheimer’s disease. Ann N Y Acad Sci, 924: 8–16, 2000.10. Burdick D, Soreghan B, Kwon M, Kosmoski J, Knauer M, Henschen A, Yates J, Cotman C, Glabe C, Assembly and aggregation properties of synthetic Alzheimer’s A4/beta amyloid peptide analogs. J Biol Chem, 267: 546–554, 1992.11. Roher AE, Lowenson JD, Clarke S, Wolkow C, Wang R, Cotter RJ, Reardon IM, Zürcher-Neely HA, Heinrikson RL, Ball MJ, Greenberg B, Structural alterations in the peptide backbone of beta-amyloid core protein may account for its deposition and stability in Alzheimer’s disease. J Biol Chem, 268: 3072–3083, 1993.12. Iwatsubo T, Odaka A, Suzuki N, Mizusawa H, Nukina N, Ihara Y, Visualization of Abeta42(43) and Abeta40 in senile plaques with end- specific Abeta monoclonals: Evidence that an initially deposited species is Abeta42(43). Neuron, 13: 45–53, 1994.13. Mudher A, Lovestone S, Alzheimer’s disease-do tauists and Baptists finally shake hands? Trends Neurosci, 25: 22–26, 2002.14. Goedert M, Spillantini MG, Tau mutations in frontotemporal dementia FTDP-17 and their relevance for Alzheimer’s disease. Biochim Biophys Acta, 1502: 110–121, 2000.15. Hardy J, Selkoe DJ, The amyloid hypothesis of Alzheimer’s disease: progress and problems on the road to therapeutics. Science, 297: 353–356, 2002.16. Tanzi RE, Moir RD, Wagner SL, Clearance of Alzheimer’s Abeta peptide: the many roads to perdition. Neuron, 43: 605–608, 2004.17. Vingtdeux V, Dreses-Werringloer U, Zhao H, Davies P, Marambaud P, Therapeutic potential of resveratrol in Alzheimer’s disease. BMC Neurosci, 9(Suppl 2): S6, 2008.18. Di Patre PL, Read SL, Secor DL, Tomiyasu U, Cummings JL, Vartavarian LM, Vinters HV, Progression of clinical deterioration and pathological changes in patients with Alzheimer disease evaluated at biopsy and autopsy. Arch Neurol, 56: 1254–1261, 1999.19. Turner AJ, Fisk L, Nalivaeva NN, Targeting amyloid-degrading enzymes as therapeutic strategies in neurodegeneration. Ann N Y Acad Sci, 1035: 1–20, 2004.20. Collen D, Ham-Wasserman lecture: role of the plasminogen system in fibrin-homeostasis and tissue remodeling. Hematology (Am Soc Hematol Educ Program), 1: 1–9, 2001.21. Vickers A, Zollman C, ABC of complementary medicine: Herbal medicine. BMJ 319: 1050–1053, 1999.22. Brahmachari G, Handbook of Pharmaceutical Natural Products, vol. 1 & 2, 1st edition, Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim, Germany, 2010.23. Shu Y-Z, Recent natural products based drug development: a pharmaceutical industry perspective. J Nat Prod, 61: 1053–1071, 1998.24. Newman DJ, Cragg GM, Snader KM, Natural products as sources of new drugs over the period 1981-2002. J Nat Prod, 66: 1022–1037, 2003.25. Harvey AL, Natural products in drug discovery. Drug Discov Today, 13: 894–901, 2008.26. Brahmachari G (editor), Bioactive Natural Products: Opportunities and Challenges in Medicinal Chemistry, World Scientific Publishing Co., Singapore, 2011.27. Houghton PJ, Howes M-J, Natural products and derivatives affecting neurotransmission relevant to Alzheimer’s and Parkinson’s disease. Neurosignals, 14: 6–22, 2005.28. Howes M-JR, Houghton PJ, Plants used in Chinese and Indian traditional medicine for improvement of memory and cognitive function. Pharm Biochem Behavior, 75: 513–527, 2003.29. Howes M-JR, Perry NSL, Houghton PJ, Plants with traditional uses and activities, relevant to the management of Alzheimer’s disease and other cognitive disorders. Phytother Res, 17: 1–18, 2003.30. Quid PM, A review of nutrients and botanicals in the integrative management of cognitive dysfunction. Altern Med Rev, 4: 144–161, 1999.31. Perry EK, Pickering AT, Wang WW, Houghton PJ, Perry NS, Medicinal plants and Alzheimer’s disease: from ethnobotany to phytotherapy. J Pharm Pharmacol, 51: 527–534, 1999.
24
FEATURE
32. Singh HK, Dhawan BN, Neuropsychopharmacological effects of the Ayurvedic nootropic Bacopa monniera Linn. (Brahmi). Indian J Pharmacol, 29: S359–S365, 1997.33. Stough C, Lloyd J, Clarke J, Downey LA, Hutchison CW, Rodgers T, Nathan PJ, The chronic effects of an extract of Bacopa monniera on cognitive function in healthy human subjects. Psychopharmacology (Berl), 156: 481–484, 2001.34. Mehta K, Binkley P, Gandhi SS, Ticku MK, Pharmacological effects of Withania somnifera root extract on GABAA receptor complex. Indian J Med Res, 94: 312–315, 1991.35. Schliebs R, Liebmann A, Bhattacharya SK, Kumar A, Ghosal S, Bigl V, Systemic administration of defined extracts from Withania somnifera (Indian Ginseng) and Shilajit differentially affects cholinergic but not glutamatergic and gabaergic markers in rat brain. Neurochem Int, 30: 181–190, 1997.36. Kanowski S, Herrmann WM, Stephen K, Wierich W, Horr R, Proof of efficacy of the Ginkgo biloba special extract Egb 761 in outpatients suffering from primary degenerative dementia of the Alzheimer’s type and multi infract dementia. Pharmacopsychiatry, 29: 47–56, 1996.37. Perry NSL, Houghton PJ, Jenner P, Keith A, Perry EK, Salvia lavandulaefolia essential oil inhibits cholinesterase in vivo. Phytomedicine, 9: 48–51, 2002.38. Jenner P, Houghton P, Perry N, Theobald A, Perry E, In vitro inhibition of human erythrocyte acetylcholinesterase by Salvia lavandulaefolia essential oil and constituent terpenes. J Pharm Pharmacol, 52: 895–902, 2000.39. Tildesley N, Salvia lavandulaefolia (Spanish sage) enhances memory in healthy young volunteers. Pharmacol Biochem Behav, 75: 669–674, 2003.40. Ballard CG, Scholey AB, Perry EK, Kennedy DO, Wesnes KA, Tildesley NTJ, Tasker A, An extract of salvia (sage) with anticholinesterase properties improves memory and attention in healthy older volunteers. J Psychopharmacol, 198: 127–139, 2008.41. Jamshidi AH, Noroozian M, Ohadinia S, Mohammadi M, Khani M, Akhondzadeh S, Salvia officinalis extract in the treatment of patients with mild to moderate Alzheimer’s disease: A double blind, randomized and placebo-controlled trial. J Clin Pharm Ther, 28: 53–59, 2003.42. Wang J, Zhao W, Teplow DB, Ho L, Rosensweig C, Ono K, Pasinetti GM, Humala N, Chen L, Grape-derived polyphenolics prevent Aβ oligomerization and attenuate cognitive deterioration in a mouse model of Alzheimer’s disease. J Neurosci, 28: 6388–6392, 2008.43. Houghton PJ, Ren Y, Howes M, Acetylcholinesterase inhibitors from plants and fungi. Nat Prod Rep, 23: 181–199, 2006.44. Viegas Jr C, Bolzani VS, Barreiro EJ, Fraga CAM, New Anti-Alzheimer Drugs from Biodiversity: The Role of the Natural Acetylcholinesterase Inhibitors. Mini-Rev Med Chem, 5: 915–926, 2005.45. Williams P, Sorribasa A, Howes M-JR, Natural products as a source of Alzheimer’s drug leads. Nat Prod Rep, 28: 48–77, 2011. 46. McCaleb R, Nature’s medicine for memory loss. HerbalGram, 23: 15, 1990.47. Sitaram N, Weingartner H, Gillin JC, Physostigmine: Improvement of long-term memory processes in normal humans. Science, 201: 272–276, 1978.48. Julian PL, Pikl J, Studies in the Indole Series. V. The Complete Synthesis of Physostigmine (Eserine); Percy L. J Am Chem Soc, 57: 755–757, 1935.49. Kamal MA, Greig NH, Alhomida AS, Al-Jafari AA, Kinetics of human acetylcholinesterase inhibition by the novel experimental alzheimer therapeutic agent, tolserine. Biochem Pharmacol, 60: 561–570, 2000.50. Howes MR, Houghton P, Acetylcholinesterase Inhibitors of Natural Origin. Int J Biomed Pharm Sci, 3: 67–86, 2009.51. Polinsky RJ, Clinical pharmacology of rivastigmine: A new-generation acetylcholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin Ther, 20: 634–647, 1998.52. Grossberg G, Desai A, Review of rivastigmine and its clinical applications in Alzheimer’s disease and related disorders. Expert Opin Pharmacother, 2: 653–666, 2001.53. Spencer CM, Noble S, Rivastigmine – a review of its use in Alzheimer’s disease. Drugs Aging, 13: 391–411, 1998.54. Bores GM, Huger FP, Petko W, Mutlib AE, Camacho F, Rush DK, Selk DE, Wolf V, Kosley RW, Davis Jr L, Vargas HM, Pharmacological evaluation of novel Alzheimer’s disease therapeutics: Acetylcholinesterase inhibitors related to galanthamine. J Pharmacol Exp Ther, 277: 728–738, 1996.55. Razay G, Wilcock GK, Galantamine in Alzheimer’s disease. Expert Rev Neurother, 8: 9–17, 2008.56. Wilcock GK, Lilienfeld S, Gaens E, On behalf of the Galantamine International-1 Study Group: Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: Multicentre randomised controlled trial. BMJ, 321: 1445–1449, 2000.57. Wilkinson D, Murray J, Galantamine: A randomised, double-blind, dose comparison in patients with Alzheimer’s disease. Int J Geriatr Psychiatry, 16: 852–857, 2001.58. Marcusson J, Bullock R, Gauthier S, Kurz A, Schwalen S, Galantamine demonstrates efficacy and safety in elderly patients with Alzheimer’s disease. Alzheimer Dis Assoc Disord, 17S3: S86–S91, 2003.59. Raskind MA, Peskind ER, Truyen L, Kershaw P, Venkata Damaraju CR, The cognitive benefits of galantamine are sustained for at least 36 months: A long term extension trial. Arch Neurol, 61: 252–256, 2004.60. Quinn R, Isaac M, Tabet N, Vitamin E for Alzheimer’s disease and mild cognitive impairment. Cochrane Database Syst Rev, 3: CD002854, 2008.
25
FEATURE
61. Maelicke A, Hoeffle-Maas A, Ludwig J, Maus A, Samochocki M, Jordis U, Koepke AKE, Memogain is a Galantamine Pro-drug having Dramatically Reduced Adverse Effects and Enhanced Efficacy. J Mol Neurosci, 40: 135–137, 2010.62. Skolnick AA, Old herbal Chinese medicine used for fever yields possible new Alzheimer disease therapy. JAMA, 277: 776, 1997.63. Ha GT, Wong RK, Zhang Y, Huperzine A as Potential Treatment of Alzheimer’s Disease: An Assessment on Chemistry, Pharmacology, and Clinical Studies. Chem Biodiver, 8: 1189–1204, 2011.64. Aggarwal BB, Kumar A, Bharti AC, Anticancer Potential of Curcumin: Preclinical and Clinical Studies. Anticancer Res, 23: 363–398, 2003.65. Yang F, Lim GP, Begum AN, Ubeda OJ, Simmons MR, Ambegaokar SS, Chen PP, Kayed R, Glabe CG, Frautschy SA, Cole GM, Curcumin inhibits formation of amyloid beta oligomers and fibrils, binds plaques, and reduces amyloid in vivo. J Biol Chem, 280: 5892–5901, 2005.66. Ng T-P, Chiam P-C, Lee T, Chua H-C, Lim L, Kua E-H, Curry consumption and cognitive function in the elderly. Am J Epidemiol, 164: 898–906, 2006.67. Kim J, Lee HJ, Lee KW, Naturally Occurring Phytochemicals for the prevention of Alzheimer’s disease. J Neurochem, 112: 1415–1430, 2010.68. Rajakrishnan V, Viswanathan P, Rajasekharan KN, Menon VP, Neuroprotective role of curcumin from curcuma longa on ethanol-induced brain damage. Phytother Res, 13: 571–574, 1999.69. Agrawal R, Mishra B, Tyagi E, Nath C, Shukla R, Effect of curcumin on brain insulin receptors and memory functions in STZ (ICV) induced dementia model of rat. Pharmacol Res, 61: 247–252, 2010.70. Yaari R, Kumar S, Tariot PN, Non-cholinergic drug development for Alzheimer’s disease. Expert Opin Drug Discov, 3: 745–760, 2008.71. Hamaguchi T, Ono K, Yamada M, Curcumin and Alzheimer’s disease. CNS Neurosci Ther, 16: 285–297, 2010. 72. Marambaud P, Zhao H, Davies P, Resveratrol promotes clearance of Alzheimer’s disease amyloid-beta peptides. J Biol Chem, 280: 37377–37382, 2005.73. Zhao H, Davies P, Marambaud P, Resveratrol promotes clearance of Alzheimer’s disease amyloid-beta peptides. J Bio Chem, 280: 37377–37382, 2005.74. Feng Y, Wang X, Yang S, Wang Y, Zhang X, Du X, Sun X, Zhao M, Huang L, Liu R, Resveratrol inhibits beta-amyloid oligomeric cytotoxicity but does not prevent oligomer formation. Neuro Toxicology, 30: 986–995, 2009.75. Jang JH, Surh YJ, Protective effect of resveratrol on β-amyloid-induced oxidative PC12 cell death. Free Radical Biol Med, 34: 1100–1110, 2003.76. Rossignol E, Debiton E, Fabbro D, Moreau P, Prudhomme M, Anizon F, In-vitro antiproliferative activities and kinase inhibitory potencies of meridianin derivatives. Anti-Cancer Drugs, 19: 789–792, 2008.77. de Almeida LMV, Leite MC, Thomazi AP, Battu C, Nardin P, Tortorelli LS, Zanotto C, Posser T, Wofchuk ST, Leal RB, Goncalves C, Gottfried C, Resveratrol protects against oxidative injury induced by H
2O2 in acute hippocampal slice preparations from Wistar rats. Arch Biochem Biophys, 480: 27–32, 2008.78. Kumar A, Naidu PS, Seghal N, Padi SSV, Neuroprotective effects of resveratrol against intracerebroventricular colchicine-induced cognitive impairment and oxidative stress in rats. Pharmacology, 79: 17–26, 2007.79. Karuppagounder SS, Pinto JT, Xu H, Chen HL, Beal MF, Gibson GE, Dietary supplementation with resveratrol reduces plaque pathology in a transgenic model of Alzheimer’s disease. Neurochem Int, 54: 111–118, 2009.80. Pall M, Casades G, Smith MA, Coto-Montes A, Pelegri C, Vilaplana J, Camins A, Resveratrol and neurodegenerative diseases: activation of SIRT1 as the potential pathway towards neuroprotection. Curr Neurovasc Res, 6: 70–81, 2009.81. Anekonda TS, Resveratrol — a boon for treating Alzheimer’s disease? Brain Res Rev, 52: 316–326, 2006.82. Kim D, Nguyen MD, Dobbin MM, Fischer A, Sananbenesi F, Rodgers JT, Delalle I, Baur JA, Sui G, Armour SM, Puigserver P, Sinclair DA, Tsai LH, SIRT1 deacetylase protects against neurodegeneration in models for Alzheimer’s disease and amyotrophic lateral sclerosis. EMBO J, 26: 3169–3179, 2007.83. Pettit GR, Cherry Herald L, Doubek DL, Herald DL, Arnold E, Clardy J, Isolation and structure of bryostatin 1. J Am Chem Soc, 104: 6846–6848, 1982. 84. Hale KJ, Manviazar S, New approaches to the total synthesis of bryostatin antitumor macrolides. Chem Asian J, 5: 704–754, 2010.85. Mackay HJ, Twelves CJ, Targeting the protein kinase C family: are we there yet? Nat Rev Cancer, 7: 554–562, 2007. 86. Etcheberrigaray R, Tan M, Dewachter I, Kuiperi C, Van der Auwera I, Wera S, Qiao L, Bank B, Nelson TJ, Kozikowski AP, Van Leuven F, Alkon DL, Therapeutic effects of PKC activators in Alzheimer’s disease transgenic mice . Proc Natl Acad Sci USA, 101: 11141–11146, 2004.87. Kuzirian AM, Epstein HT, Gagliardi CJ, Nelson TJ, Sakakibara M, Taylor C, Scioletti AB, Alkon DL, Bryostatin enhancement of memory in Hermissenda. Biol Bull, 210: 201–214, 2006.88. Sun MK, Alkon DL, Dual effects of bryostatin-1 on spatial memory and depression. Eur J Pharmacol, 512: 43–45, 2005. 89. Sun MK, Hongpaisan J, Alkon DL, Postischemic PKC activation rescues retrograde and anterograde long-term memory. Proc Natl Acad Sci USA, 106: 14676–14680, 2009.
26
FEATURE
90. Drug Given 24 Hours After Stroke Helps Repair Brain Tissue” (http://www.bio-medicine.org/medicine-news-1/Drug-Given-24-Hours- After-Stroke-Helps-Repair-Brain-Tissue-26027-1/). Bio-medicine.org. March 2008. http://www.bio-medicine.org/medicine-news-1/ Drug-Given-24-Hours-After-Stroke-Helps-Repair-Brain-Tissue-26027-1/. Retrieved 2011-08-22.91. Tomiyama T, Kaneko H, Kataoka K, Asano S, Endo N, Rifampicin inhibits the toxicity of pre-aggregated amyloid peptides by binding to peptide fibrils and preventing amyloid-cell interaction. Biochem J, 322: 859–865, 1997.99. Loeb MB, Molloy DW, Smieja M, Standish T, Goldsmith CH, Mahony J, Smith S, Borrie M, Decoteau E, Davidson W, Mcdougall A, Gnarpe J, O’donnell M, Chernesky M, A randomized, controlled trial of doxycycline and rifampin for patients with Alzheimer’s disease. J Am Geriatr Soc, 52: 381–387, 2004.100. Hann RM, Sando CE, Scyllitol from flowering dogwood (Cornus florida). J Biol Chem, 68: 399–402, 1926.101. McLaurin J, Kierstead ME, Brown ME, Hawkes CA, Lambermon MHL, Phinney AL, Darabie AA, Cousins JE, French JE, Lan MF, Chen F, Wong SSN, Mount HTJ, Fraser PE, Westaway D, George-Hyslop PS, Cyclohexanehexol inhibitors of Aβ aggregation prevent and reverse Alzheimer phenotype in a mouse model. Nat Med, 12: 801–808, 2006.102. Schenk D, Barbour R, Dunn W, Gordon G, Grajeda H, Guido T, Hu K, Huang J, Johnson-Wood K, Khan K, Kholodenko D, Lee M, Liao Z, Lieberburg I, Motter R, Mutter L, Soriano F, Shopp G, Vasquez N, Vandevert C, Walker S, Wogulis M, Yednock T, Games D, Seubert P, Immunization with amyloid-β attenuates Alzheimer-disease-like pathology in the PDAPP mouse. Nature, 400: 173–177, 1999.103. Kerchner GA, Boxer AL, Bapineuzumab. Expert Opin Biol Ther, 10: 1121–1130, 2010.104. Rinne JO, Brooks DJ, Rossor MN, Fox NC, Bullock R, Klunk WE, Mathis CA, Blennow K, Barakos J, Okello AA, Rodriguez Martinez de Liano S, Liu E, Koller M, Gregg KM, Schenk D, Black R, Grundman M, 11C-PiB PET assessment of change in fibrillar amyloid-beta load in patients with Alzheimer’s disease treated with bapineuzumab: a phase 2, double-blind, placebo-controlled, ascending-dose study. Lancet Neurol, 9: 363–372, 2010. 105. Gilman S, Koller M, Black RS, Jenkins L, Griffith SG, Fox NC, Eisner L, Kirby L, Rovira MB, Forette F, Orgogozo JM, AN1792(QS-21)-201 Study Team. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology, 164: 1553–1562, 2005.106. Hock C, Konietzko U, Streffer JR, Tracy J, Signorell A, Muller-Tillmanns B, Lemke U, Henke K, Moritz E, Garcia E, Wollmer MA, Umbricht D, de Quervain DJ, Hofmann M, Maddalena A, Papassotiropoulos A, Nitsch RM, Antibodies against beta-amyloid slow cognitive decline in Alzheimer’s disease. Neuron, 38: 547–554, 2003.107. Pfeifer M, Boncristiano S, Bondolfi L, Stalder A, Deller T, Staufenbiel M, Mathews PM, Jucker M, Cerebral hemorrhage after passive anti-Abeta immunotherapy. Science, 29: 1379, 2002.; Morgan D, Diamond DM, Gottschall PE, Ugen KE, Dickey C, Hardy J, Duff K, Jantzen P, DiCarlo G, Wilcock D, Connor K, Hatcher J, Hope C, Gordon M, Arendash GW. A beta peptide vaccination prevents memory loss in an animal model of Alzheimer’s disease. Nature, 408: 982–985, 2001.108. DeMattos RB, Bales KR, Cummins DJ, Dodart JC, Paul SM, Holtzman DM. Peripheral anti-A beta antibody alters CNS and plasma A beta clearance and decreases brain A beta burden in a mouse model of Alzheimer’s disease. Proc Natl Acad Sci USA, 98: 8850–8855, 2001.109. Bard F, Cannon C, Barbour R, Burke RL, Games D, Grajeda H, Guido T, Hu K, Huang J, Johnson-Wood K, Khan K, Kholodenko D, Lee M, Lieberburg I, Motter R, Nguyen M, Soriano F, Vasquez N, Weiss K, Welch B, Seubert P, Schenk D, Yednock T. Peripherally administered antibodies against amyloid beta-peptide enter the central nervous system and reduce pathology in a mouse model of Alzheimer disease. Nat Med, 6: 916–919, 2000.
Goutam Brahmachari studied Chemistry at Visva-Bharati University in India from 1987-1992. Having obtained his Ph.D. degree in Natural Products Chemistry in 1997, he started his academic career in the next year at the same University, where he is now an Associate Professor of Chemistry. He has been deeply involved both in teaching and research during the last thirteen years. His research interests focus on chemical and biological studies of phytochemicals from medicinal plants, including organic synthesis. Besides publishing about fifty scientific research articles in the fields of organic chemistry in leading national and international journals, he has authored and edited several books from reputed National/International Presses; among the books, five are the major reference volumes in the field of natural products (Chemistry of Natural Products: Recent Trends & Developments-2006; Natural Products: Chemistry, Biochemistry and Pharmacology-2009; Handbook of Pharmaceutical Natural Products, Vol. 1 & 2 – 2010, Bioactive Natural Products: Opportunities & Challenges in Medicinal Chemistry -2011). He is a member of the Indian Association for the Cultivation of Science (IACS).