25
Febrile Seizures Dr. Vinia Rusli Sp.A
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | andrew-sabastian-geraldyno-paago |
| View: | 23 times |
| Download: | 2 times |
Febrile Seizures
Dr. Vinia Rusli Sp.A
Febrile Seizures
O Most common type of seizures in the
pediatric population.
O Age dependent
O Usually occur in ages 6 months – 5 years
O Peak age at onset ± 18 months.
O Incidence : 3%-8% in children <5 years.
Febrile Seizures - Definition
O AAP:
Seizures occurring in childhood after age 1 month, associated with febrile illness but not caused by infection of the central nervous system (CNS), unassociated with previous neonatal seizures or unprovoked seizures, and not meeting criteria for other acute symptomatic seizures.
O IDAI:
Kejang demam ialah bangkitan kejang yang terjadi pada kenaikan suhu tubuh (suhu rektal di atas 38°C) yang disebabkan oleh suatu proses ekstrakranium.
Types of febrile seizures
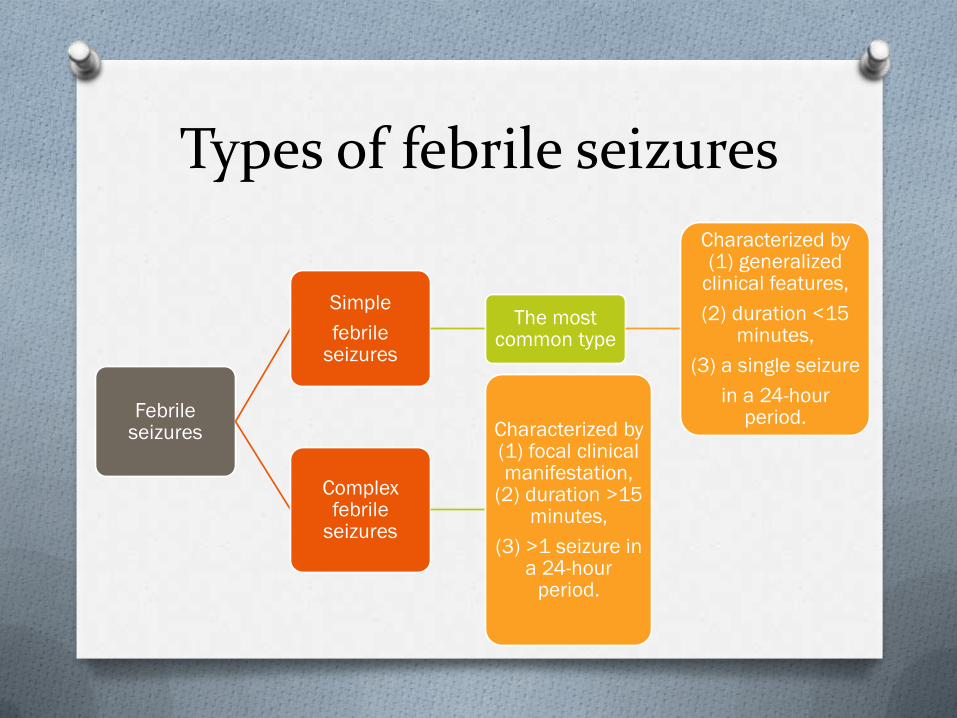
Febrile seizures
Simple
febrile seizures
The most common type
Characterized by (1) generalized
clinical features,
(2) duration <15 minutes,
(3) a single seizure
in a 24-hour period.
Complex febrile
seizures
Characterized by (1) focal clinical manifestation,
(2) duration >15 minutes,
(3) >1 seizure in a 24-hour
period.
Family history of febrile seizures
O ± 25% - 40% of children who have febrile
seizures have a family history of febrile
seizures
O 9% - 22% of children have a sibling who has
a history of febrile seizures.
Risk factors
O Peak temperature during the illness,
O History of febrile seizure in first-degree relatives,
O Neurodevelopmental delays,
O Vaccinations with MMR, DTP vaccines.
O Almost 50% of the children who present with febrile seizures will not have any identified risk factors.
Evaluation of children who have febrile seizures
O Main purpose : determine the cause of the fever
and exclude underlying CNS infections.
O Viral infections of the upper respiratory tract,
roseola, and acute otitis media are most frequently
the causes of febrile convulsions.
Laboratory testing in febrile seizures
O Not routine
O Should be ordered based on individual clinical
circumstances
O CBC to evaluate the cause of the fever
O Serum glucose determination
O Serum electrolytes when there is evidence of
dehydration.
Lumbal puncture
O Should be considered strongly in infants <12 months, those who have prolonged complex febrile seizures or febrile status epilepticus.
O Infants 12-18 months consider LP
O Infants >18 months not routine
O If any doubt exists about the possibility of meningitis, LP with examination of the cerebrospinal fluid (CSF) is indicated.
Neuroimaging in febrile seizures
O Routine EEG and neuroimaging not indicated
for simple febrile seizures.
O Neuroimaging is recommended in patients who
have complex febrile seizures, neurologic deficit
on examination, prolonged postictal state, and
signs of raised intracranial pressure.
O Patients who have febrile status epilepticus
require EEG testing.
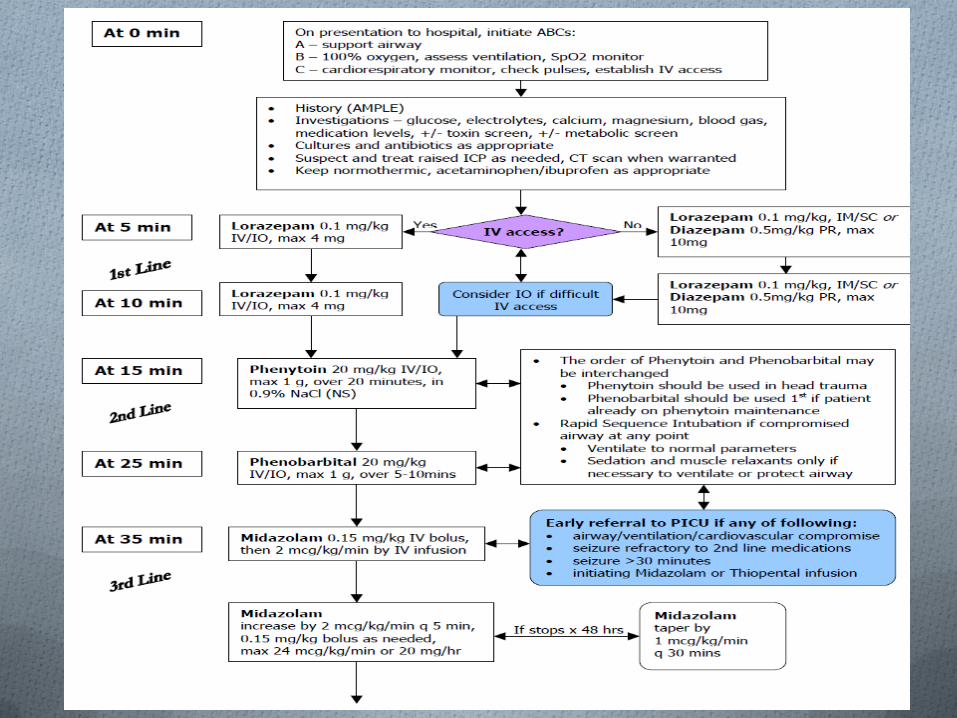
Management of febrile seizures
O Management of seizure: diazepam IV 0,3-0,5
mg/kg slowly in 3-5 minutes, max dose 20 mg
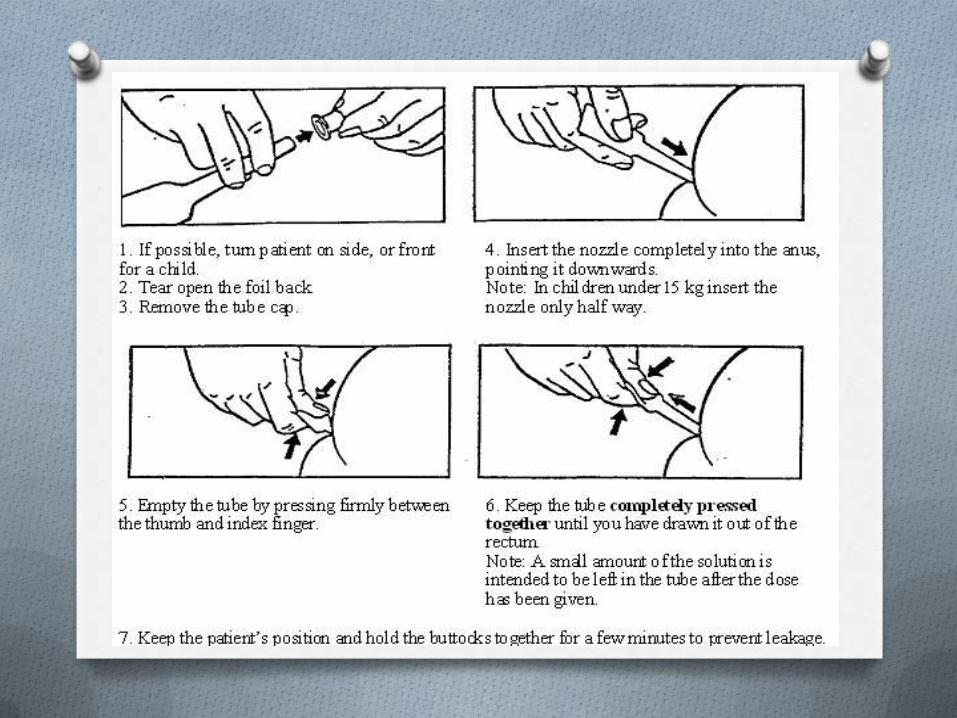
O Home management: rectal diazepam
O Dose: 0,5-0,75 mg/kg; or 5 mg for weight <10 kg
and 10 mg for weight >10 kg; or 5 mg for <3
years and 7,5 mg for> 3 years

Management of febrile seizures - Antipyretic
O No evidence to decrease the risk of febrile
convulsions
O Paracetamol 10 –15 mg/kg/dose
O Ibuprofen 5-10 mg/kg/dose
Management of febrile seizures – Anticonvulsant prophylaxis
O Oral diazepam effective and safe for reducing
the risk of recurrence of febrile seizures.
O At the onset of each febrile illness, oral
diazepam, 0.3 mg/kg q8h (1 mg/kg/24 hr), is
administered for the duration of the illness.
O Minor side effects : lethargy, irritability, and
ataxia, may be reduced by adjusting the dose.
Management of febrile seizures – Anticonvulsant maintenance
O Should be considered in:
• infants<12 months,
• complex febrile seizures,
• neurologic deficit before or after seizure.
O Valproic acid (drug of choice): 15-40 mg/kg/d q8-12h
• Possibility of valproate-induced hepatotoxicity in
children <2 years.
O Phenobarbital 3-4 mg/kg/d q12-24h.
O Duration of therapy: until 1 year with no seizure
Management of febrile seizures - Education
O Reassurance and counseling very important &
essential, given the high degree of anxiety
surrounding seizures
O Information on how to manage seizure, possibility
of recurrence
Recurrence
O Usually occurs within 1 to 2 years after the initial seizure.
O Risk of recurrence ± 60%.
O Risk factors for recurrence : younger age of onset, an initial febrile seizure associated with a relatively low temperature, family history of febrile seizures in a first-degree relative, and brief duration between the onset of the fever and seizure.
Risk factors for epilepsy
O ± 2% - 7% of children who have a history of febrile seizures have a
risk of developing epilepsy.
O Risk factors for developing subsequent epilepsy after febrile seizures:
• Complex febrile seizure,
• Positive family history of epilepsy,
• Initial febrile seizure <9 mo of age,
• Delayed developmental milestones,
• Pre-existing neurologic disorder.
O Incidence of epilepsy is ± 9% when several risk factors are present,
compared with an incidence of 1% in children who have febrile
convulsions and no risk factors.
Prognosis
O Generally excellent prognosis.
O No significant association between febrile
seizures and later significant cognitive
developmental delay or with sudden infant
death syndrome.
~fin~

















