February 2, 2004 9:00 A.M. Washington, D.C. David Shaffer, F.R.C.P., F.R.C.Psych. Columbia University/New York State Psychiatric Institute 1051 Riverside Drive, New York, NY 10032 SUICIDE AND RELATED PROBLEMS IN ADOLESCENCE FOOD AND DRUG ADMINISTRATION FDA Meeting
Transcript
February 2, 20049:00 A.M.
Washington, D.C.
David Shaffer, F.R.C.P., F.R.C.Psych.Columbia University/New York State Psychiatric Institute
1051 Riverside Drive, New York, NY 10032
SUICIDE AND RELATED PROBLEMS
IN ADOLESCENCE
FOOD AND DRUG ADMINISTRATIONFDA Meeting
1EPIDEMIOLOGY
CAUSE # OF DEATHSAccidents 6646Homicide 1899Suicide 1611Cancer 732Heart Disease 347Congenital Anomalies 255Chronic Lower
Respiratory Disease 74Stroke 68Influenza and Pneumonia 66Blood Poisoning 57
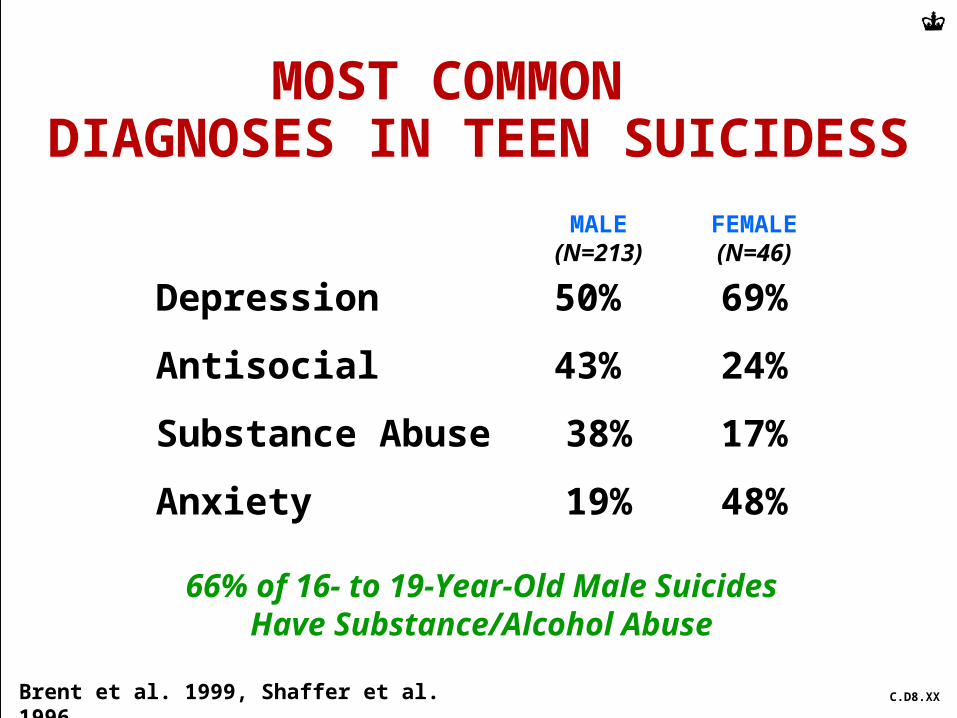
66% of 16- to 19-Year-Old Male Suicides Have Substance/Alcohol Abuse
MOST COMMON DIAGNOSES IN TEEN SUICIDESS
Brent et al. 1999, Shaffer et al. 1996 C.D8.XX
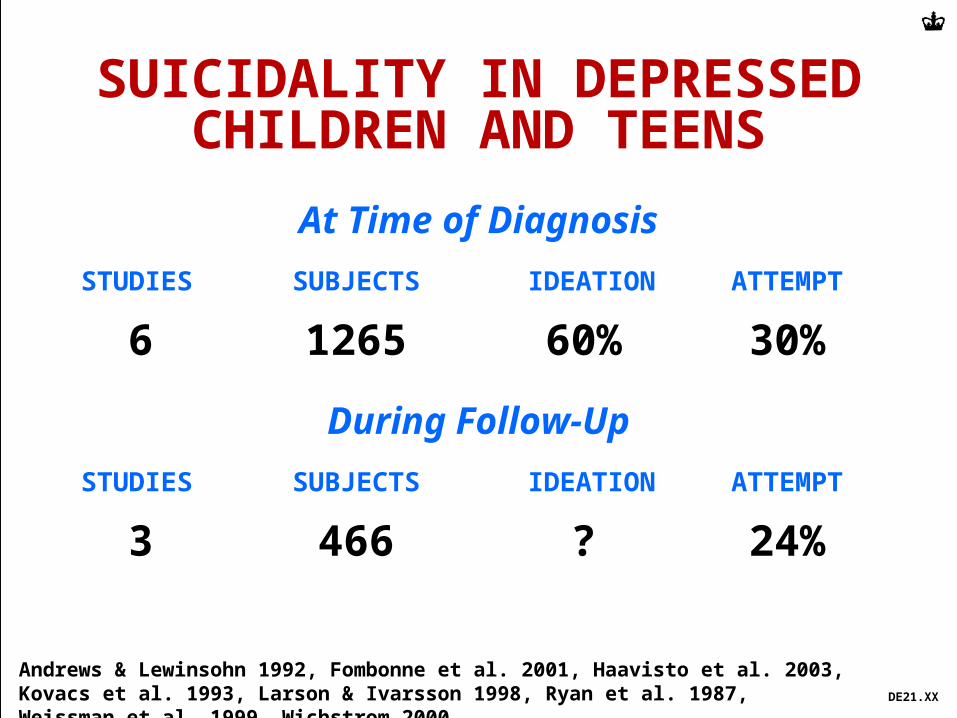
SUICIDALITY IN DEPRESSED CHILDREN AND TEENS
Andrews & Lewinsohn 1992, Fombonne et al. 2001, Haavisto et al. 2003, Kovacs et al. 1993, Larson & Ivarsson 1998, Ryan et al. 1987, Weissman et al. 1999, Wichstrom 2000
At Time of Diagnosis
STUDIES SUBJECTS IDEATION ATTEMPT
6 1265 60% 30%
During Follow-Up
STUDIES SUBJECTS IDEATION ATTEMPT
3 466 ? 24%
DE21.XX
OTHER FACTORS THAT PREDISPOSE TO SUICIDE
2004 January
Imitation
Biological abnormalities that ?predispose to impulsive response to stress
A family history of suicide
C.MO1.XX
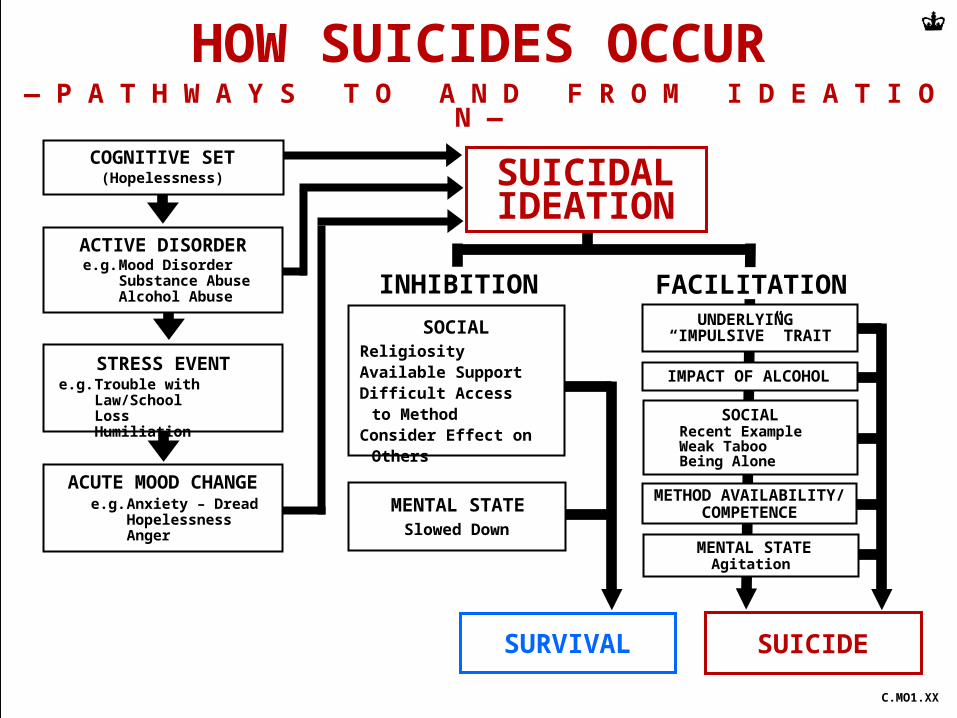
STRESS EVENTe.g. Trouble with Law/School
LossHumiliation
ACUTE MOOD CHANGEe.g. Anxiety – Dread
HopelessnessAnger
ACTIVE DISORDERe.g. Mood Disorder
Substance AbuseAlcohol Abuse
(Hopelessness)COGNITIVE SET
HOW SUICIDES OCCUR— P A T H W A Y S T O A N D F R O M I D E A T I O N —
TeensSTUDY RECENT TREATMENTFinland 23%Pittsburgh 15%New York City 21%Norway 7%
TEENS WHO SUICIDE RECEIVE LESS
TREATMENT THAN ADULTS
C.Rx18.XX
Marttunen et al. 1992 Brent et al. 1993, Shaffer et al. 1996, Groholt et al. 1997, Foster et al. 1997, Appleby et al. 1999, Lesage et al. 1994
Prescribed antidepressants 24%
Antidepressants found at autopsy 0%
DEPRESSED TEENS WHO COMMIT SUICIDE DO NOT TAKE THEIR MEDICATIONS
— U T A H Y O U T H S U I C I D E S T U D Y, N = 49 —
Gray et al. 2003 DR30.XX
SUICIDALITY DURING THE TREATMENT OF TEEN DEPRESSION
Cautions & Considerations -1
2004 February
Ideation and attempts are common in depressed teens and recur frequently.
Teens often conceal ideation and attempts unless asked about them directly.Self report facilitates disclosure.
Event Reports may be influenced by mode of elicitation. They are not used with a glossary, misclassification can occur.
SUICIDALITY DURING THE TREATMENT OF TEEN DEPRESSION
Cautions & Considerations -2
2004 February
“Self harm” is a heterogeneous descriptor - not all types of self harm are associated with suicidal intent.
There have been no direct studies -with frequent and careful measurements -examining whether SSRI’s increase, decrease or have no effect on suicidal ideation and behavior.
SUICIDALITY DURING THE TREATMENT OF TEEN DEPRESSION
Cautions & Considerations -3
2004 February
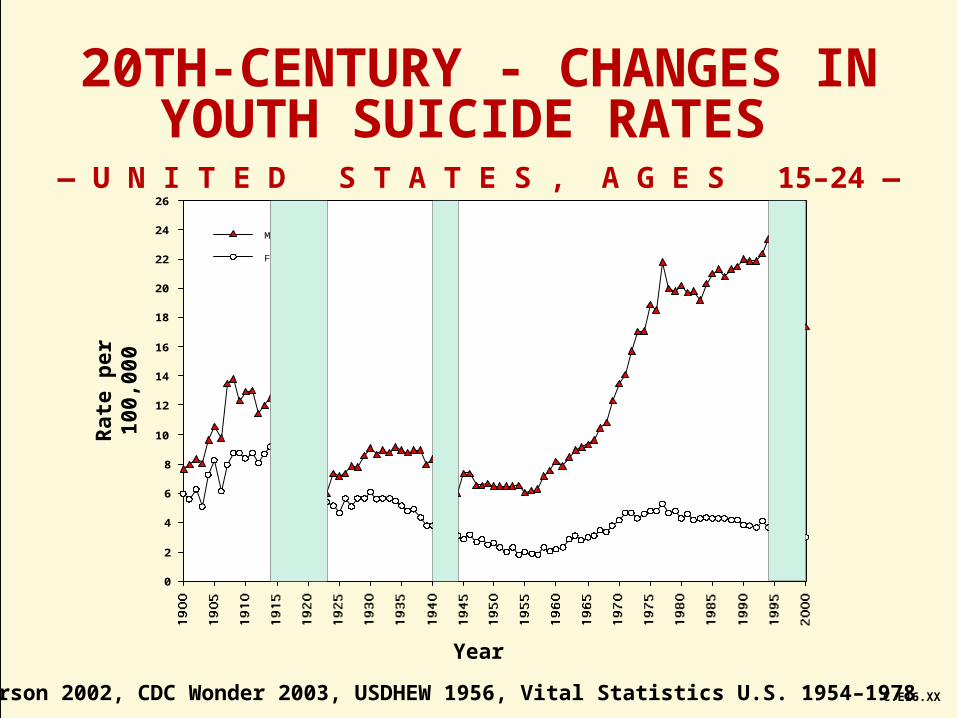
After increasing for 35 years teen suicide rates have been declining consistently in many countries.
During this period there has been a marked increase in exposure of teens to SSRI antidepressants.
These trends could be related. We do not - currently - have a better explanation for the turnabout of a condition that led to the death of tens of thousands of young people.