59
Fecal Incontinence and Constipation 3/18/2015 1 PELVIC FLOOR DYSFUNCTION Toyia James-Stevenson, MD September 12, 2015
| Date post: | 31-Dec-2015 |
| Category: |
Documents |
| Upload: | shon-benson |
| View: | 216 times |
| Download: | 1 times |

Fecal Incontinence and Constipation
3/18/2015 1
PELVIC FLOOR DYSFUNCTION
Toyia James-Stevenson, MDSeptember 12, 2015
Discuss epidemiology, etiology and risk factors
Explore potential barriers to care Evaluation of pelvic floor disordersExplore options for evaluation and
management
04/19/23 2
FOCUS OF TALK

04/19/23 3
FECAL INCONTINENCE

Fecal Incontinence - Unintentional loss of solid or liquid stool
Anal Incontinence - Includes leakage of gas and/or fecal incontinence
04/19/23 4
DEFINITION

Prevalence in US of 7-15%Incidence will likely increase as population
agesIn adults > 65 dwelling in community
incidence of 17% over 4 yrs 6% have monthly symptoms
Most studies show a higher prevalence in Caucasian women than African American women
Prevalence = in Caucasian and AA Men04/19/23 5
EPIDEMIOLOGY
Whitehead WE, Borrud L, Goode PS et al. FI in US adults: epidemiology and risk factors. Gastro 2009;137:512–7

04/19/23 6
PREVALENCE BY SEX AND AGE
I. Ditah, P. Devaki, H.N. Luma, et al. Prevalence, trends, and risk factors for fecal incontinence in United States adults, 2005-2010; Clin Gastroenterol Hepatol, 12 (2013), pp. 636–643.

Chronic DiarrheaRectal UrgencyBurden of Chronic Illness (Comorbid count, DM)
Urinary IncontinencePelvic SurgeryCaucasian Race
Smoking (also RF for external sphincter atrophy on MRI)
ObesityInstrumented
Vaginal DeliveryDecreased physical
activityAdvanced Age
04/19/23 7
RISK FACTORS
Bharucha AE, et al;Am J Gastro. 2015 Jan;110(1):127-36

Chronic DiarrheaRectal UrgencyBurden of Chronic Illness (Comorbid count, DM)
Urinary IncontinencePelvic SurgeryCaucasian Race
Smoking (also RF for external sphincter atrophy on MRI)
ObesityInstrumented
Vaginal DeliveryDecreased physical
activityAdvanced Age
04/19/23 8
RISK FACTORS
Bharucha AE, et al;Am J Gastro. 2015 Jan;110(1):127-36
Instrumented vaginal deliveryThird and fourth-degree lacerations Incidence has declined over past 2 decades from 13% to 8% following vaginal delivery
Sphincter Injury not major risk factor for FI occurring decades later after adjusting for bowel disturbance
04/19/23 9
OBSTETRICAL INJURY
Prevalence: 15% in community-dwelling 18-33% in hospitalized 50-70% in NH
Within 10 months of NH admission, 20% of continent develop FI ? NH practices low functional status high comorbidity
Risk Factors- dementia, chronic dz, mobility impairment
04/19/23 10
ELDERLY
Nelson RL. Epidemiology of FI. Gastro 2004;126(Suppl 1):S3–S7.

04/19/23 11
Pathogenesis and Etiology of Fecal IncontinenceAnal Sphincter Weakness Injury: obstetric, surgical (hemorrhoidectomy, internal sphincterotomy, fistulotomy) Nontraumatic: scleroderma, IAS thinning of unknown etiology Neuropathic: stretch injury, obstetric, DM
Anatomical Disturbance of Pelvic Floor: fistula, rectal prolapse, descending perineum syndrome
Anorectal Inflammation: Crohn’s, Ulcerative colitis, radiation proctitis, anorectal infection
CNS Disease: dementia, stroke, brain tumors. spinal cord lesions, MS, multisystem atrophy (Shy-Drager’s syndrome)
Bowel Disturbance: diarrhea (e.g. IBS, post-cholecysectomy) constipation with or without impaction or overflow diarrhea

Passive – stool leakage with little or no forewarning (often have low resting pressure)
Urge – occurs despite active efforts to retain stool May have abnl squeeze pressure and durationMay have reduced rectal capacity with rectal hypersensitivity
Seepage – Leakage after BMIncomplete evacuation or impaired sensation
04/19/23 12
CLINICAL SUB-TYPES OF FI

Can have devastating impact on quality of life
Loss of dignity, modesty, confidenceMany do not share with closest relatives,
friends or physiciansProviders may consider it less important that
screening for other health issues (triglycerides, DM, excessive ETOH, urinary incontinence)
Caregiver burden >>urinary incontinence04/19/23 13
WHY IS THIS IMPORTANT?

HELPING OUR AGING POPULATION MAINTAIN DIGNITY AND AUTONOMY IS
IMPORTANT!
04/19/23 14

REASONS GIVEN FOR NOT CONSULTING PHYSICIAN
04/19/23 15
Kunduru et al, Clinical Gastroenterology and Hepatology 2015;13:709–716
124 pts surveyed88 consulters36 nonconsulltersSimilar Fecal Incontinence Severity Index (FISI)
Mean age: 5687.9% women
Consulters had higher depressom scpres (P=0.04)
Nonconsulters less aware of available treatments (P<0.01)

PT SUGGESTIONS FOR IMPROVING FI CONSULTATION
Patients may prefer that their provider initiate conversation about FI
04/19/23 16
Kunduru et al, Clinical Gastroenterology and Hepatology 2015;13:709–716

BARRIERS TO CARE
A small email survey of 11/56 physician responders found that in nonscreeners:- 50% felt time constraints was major barrier to screening
- 75% thought FI was rare (<5% prevalence)- All felt it was pt or caregivers responsibility to address
- All felt screening for FI less important than screening for other health issues (DM, excessive Etoh intake, urinary incontinence, cholesterol)
04/19/23 17
Kunduru et al, Clinical Gastroenterology and Hepatology 2015;13:709–716

Routine screening by practitioners is important“Accidental Bowel Leakage” may be better term
An Internet study of women >45 yoOnly 30.9% of 1095 pt had heard term “FI”71.1% preferred “Accidental Bowel Leakage”22.5% preferred “bowel incontinence”6.4% preferred “FI”
04/19/23 18
IMPROVING ACCESS FOR PATIENTS
Brown HW, Wexner SD. Int J Clin Pract 2012;66:1101–8.

CAN CHANGES IN TERMINOLOGY AFFECT ACCESS TO CARE?
• Access improved when “impotence” was replaced with “erectile dysfunction”
04/19/23 19
1995 2015

Lack of US data on economic impactNo prospective studies comparing cost
effectiveness of conservative therapy versus SNS or bulking agents
In UK, each increment in quality-adjusted life year gained with SNS for FI costs $35,000
Largest burden likely from indirect costsIncreases likelihood of NH admissionLoss of productivity
04/19/23 20
ECONOMIC IMPACT

IAS- smooth muscle, 70-85% of resting tone
Stool causes rectal distentionRectal contractionUrgency sensationRelaxation of IAS (RAIR)
EAS, PR and levator ani can be voluntarily contracted to maintain continence
04/19/23 21
NORMAL ANORECTAL FUNCTION

Lower resting and squeeze pressures (decrease by 30-40% in pts >70 yo
Denervation of anal sphincterDecreased rectal compliance (stiffer rectum)
Decreased rectal sensationPerineal laxity
04/19/23 22
CHANGES IN ANORECTUM WITH AGE
Fox et al, Dis Colon and Rectum, Nov 2006
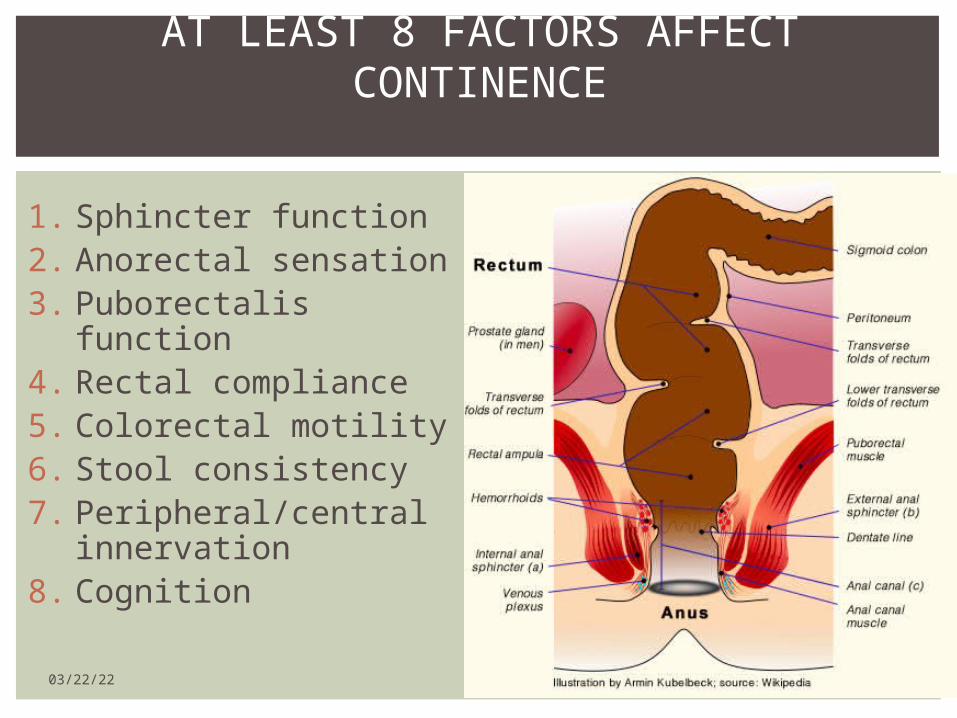
1. Sphincter function2. Anorectal sensation3. Puborectalis
function4. Rectal compliance5. Colorectal motility6. Stool consistency7. Peripheral/central
innervation8. Cognition
04/19/23 23
AT LEAST 8 FACTORS AFFECT CONTINENCE

Obtain history of co-morbid conditions (DM, UI)
Inspect for fecal matter, skin irritation, external hemorrhoids, gapping anus, lack of creases
Can identify rectal prolapse or excessive perineal descent (>3cm outward bulge)
Assess sensation and anocutenous reflexDigital rectal exam – can identify patients
with fecal impaction and overflow 04/19/23 24
INITIAL EVALUATION

Semi-formed or liquid stool stresses pelvic floor continence mechanisms more than formed stool
Harder stools may point towards overflow and/or an evacuation disorder
04/19/23 25
STOOL CONSISTENCY IS IMPORTANT

Avoiding offending foods (Fodmaps, caffeine)Ritualizing bowel habitsImproving skin hygieneHigh fiber – 2-6 grams/d can bulk stools by
absorbing water and increase stool transit time methocellulose 100% soluble and non-fermentable
psyllium 70% soluble*fermentable fibers may cause diarrhea
04/19/23 26
SUPPORTIVE MEASURES
“Overflow” fecal incontinence? Laxative use? Rectal impaction? Evacuation d/o
Enable evacuation with suppositoriesAnorectal testing for evacuation
disorderpelvic floor retraining as indicated
04/19/23 27
MANAGING CONSTIPATION IN FI

Evaluate for organic cause (biopsies for microscopic colitis, ? bacterial overgrowth)
ManagementConsider eliminating fructose, lactose, caffeineLoperamide Tricyclic antidepressant (desipramine, amitryptiline)
Bile Salt agents (especially post-cholecystectomy)
Alosetron for healthy pts with IBS-D
04/19/23 28
MANAGING DIARRHEA IN FI

Norton, et al; Gastro: 126, 1, 2004, S64 - S70
Group 1: Standard medical/nursing care (up to 6 one hr sessions of info/advice)Group 2: Same as group 1 + verbal instruction and leaflet explaining KegelsGroup 3: Same as group 2 + computer-assisted biofeedbackGroup 4: Same as group 3 + home EMG biofeedback
No significant difference between treatment groups for all improvements
For all groups median number of incontinence episodes per week from 2 to 0 (p <0.001)
BEHAVIORAL MANAGEMENT OF FI IN ADULTS

Avoid rushing to the toilet Increases abdominal wall contractionsReduces focus on pelvic floor Instead, stop and perform Kegels bf proceeding to toilet
Clean, squeeze, recleanAfter BM, clean anus, perform 2-3 Kegels, reclean
Delay BM after biofeedback therapyStart with brief periods, then increase, which improves confidence
Wean off laxatives and anti-diarrheals04/19/23 30
EXAMPLE OF BEHAVIORAL TECHNIQUES
25% of pts will improve with behavioral modification

A few small single-center studies have shown benefit of biofeedback over pelvic floor exercises
Benefit may be highest in those with urge incontinence and predominantly EAS weakness
04/19/23 31
BIOFEEDBACK
Haymen, S, Dis Colon Rectum 2009

EAS muscles overlapped in the anterior midlineBetter outcome than end-to-end repairLong-term data shows suboptimal improvement
04/19/23 32
OVERLAPPING SPHINCTEROPLASTY

Temperature-controlled energy to anorectal junctionProduces scarring and narrowingVariable results with no large randomized trials
04/19/23 33
SECCA

04/19/23 34LESS COMMON TECHNIQUES

Low-amplitude electric current applied to S3 via electrode in sacral foramen
Temporary lead can be placed in office and left for 7 days or surgically for up to 14 days
Patients with >50% symptom improvement can go on to have permanent stimulator placed
Meta-analysis from 2000-2008 shows complication rate of 15% with removal in 2.7&
Newer device smaller but expensive ($40K)
04/19/23 35
SACRAL NEUROMODULATION

Data from 67/ 120 pts available at 5-8yrsFI episodes per week from a mean of 9.1 at baseline to 1.7
at 5 years, 89% (n = 64/72) had ≥50% improvement (p < 0.0001) 36% (n = 26/72) had complete continence27/76 (35.5%) pts required a device revision, replacement, or
explant.
04/19/23 36
SACRAL NEUROMODULATION LONG-TERM
Tjandra, Disease of Colon and Rectum, Feb 2013

04/19/23 37
SACRAL NEUROMODULATION LONG-TERM
Tjandra, Disease of Colon and Rectum, Feb 2013

Dextranomer microsphere in hyaluronic acid (Solesta)
Randomized, study evaluating 50% improvement at 6mos71pts (52%) in Tx group 22 (31%) in sham group had 50% improvement
No difference in 3 of 4 FIQOL
04/19/23 38
INJECTABLE BULKING AGENTS

BenefitsOffice procedure with no sedationLow complication rates w/pain being most commonAt 12 mos, 69% noted improvement (higher than 6mo improvement data)
DisadvantagesMay need 2-3 injectionsCost of $4000-$5000/ injectionNo sx or anorectal data on which pts may benefit6% fully continent at 6mo, 11% at 12 mos
04/19/23 39
SOLESTA
04/19/23 40
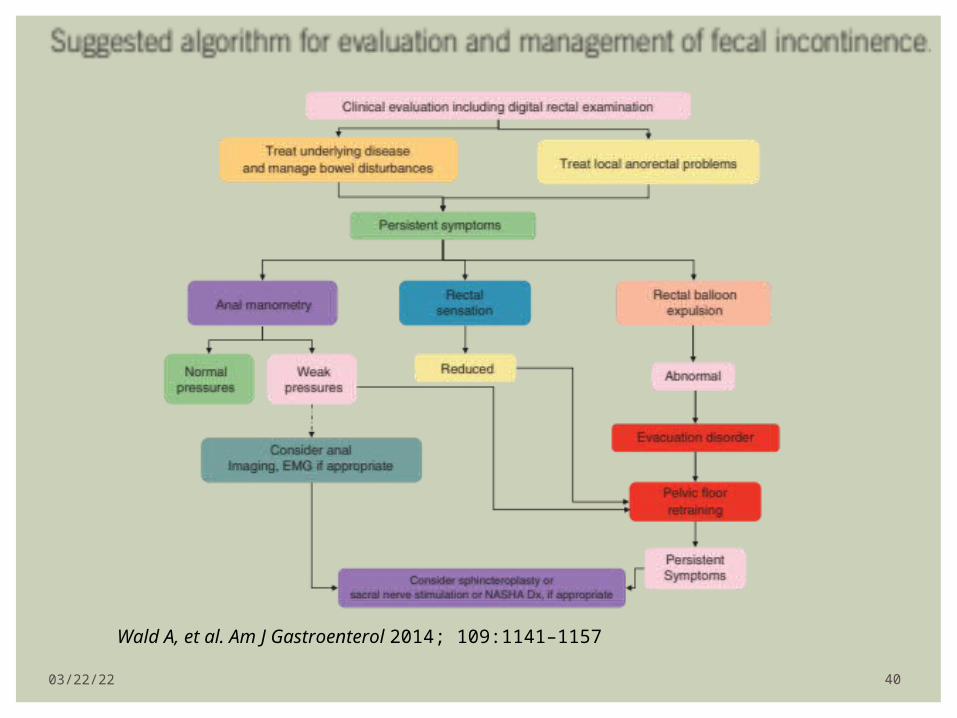
Wald A, et al. Am J Gastroenterol 2014; 109:1141–1157

04/19/23 41
CONSTIPATION

CONSTIPATION- ROME III

Prevalence of 14% (3-30% depending on population assessed)
Cumulative incidence of 17% over 12-yr period
555,000 ER visits yearly38,000 hospitalizationsIn 2004, direct costs of $1.6 billion
EPIDEMIOLOGY

Advanced age Often results from hard stool and excessive straining
Causes may include food intake, mobility, weakening of abdominal wall and pelvic muscles, chronic illness, psychological factors, medications
Female gender (2-3X higher)Low level of educationLow level of physical activityLow socioeconomic statusNonwhite ethnicity
RISK FACTORS
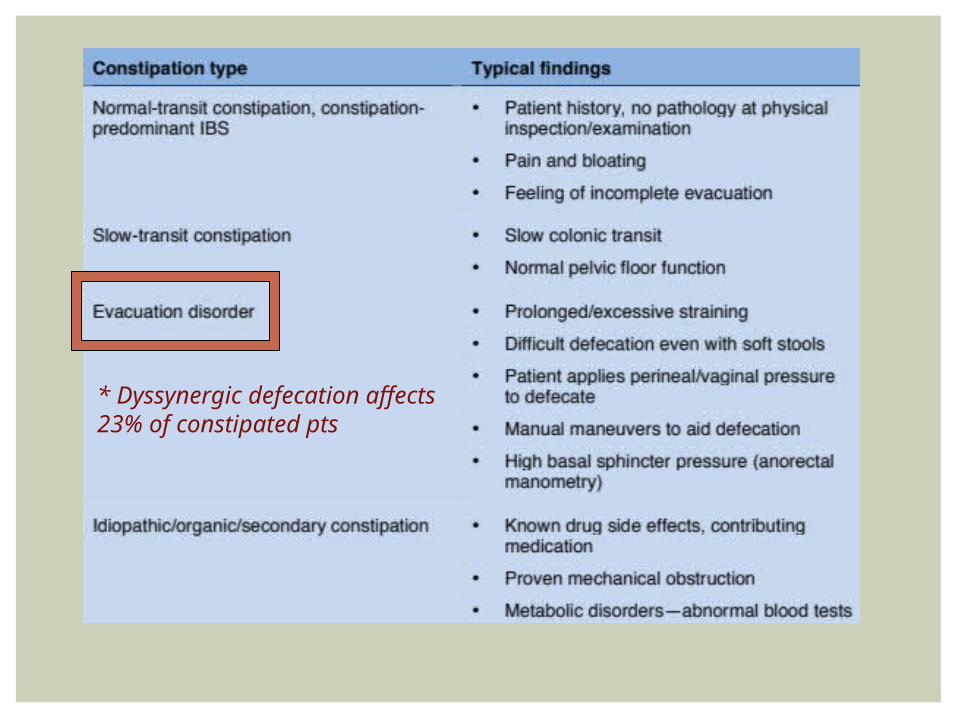
* Dyssynergic defecation affects 23% of constipated pts

CONSTIPATION SUBTYPES- FUNCTIONAL DEFECATION
DISORDERS
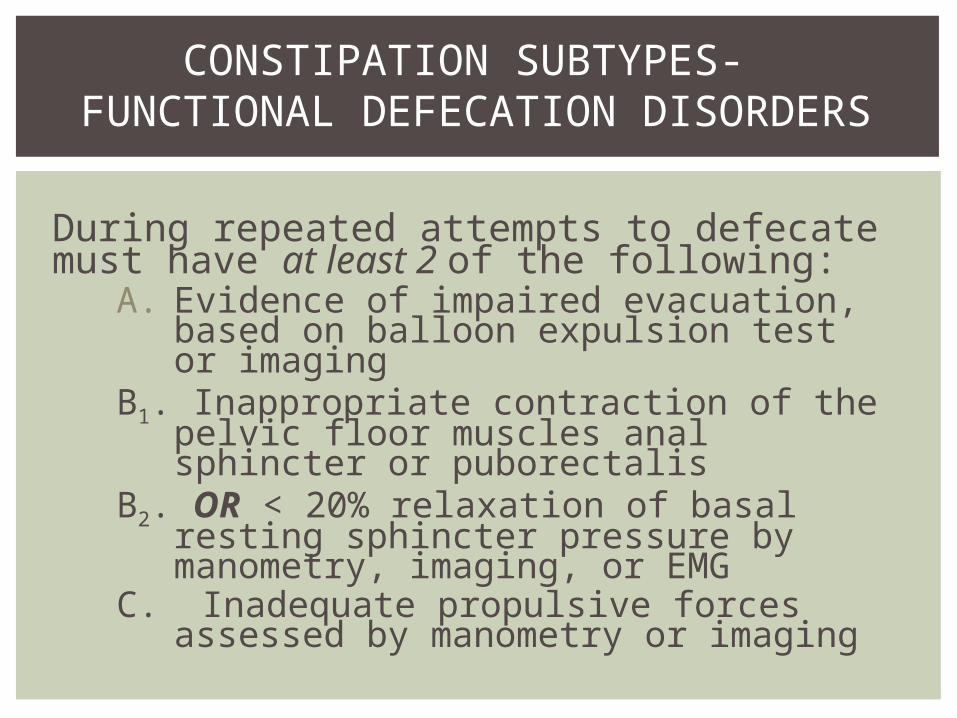
During repeated attempts to defecate must have at least 2 of the following:
A. Evidence of impaired evacuation, based on balloon expulsion test or imaging
B1. Inappropriate contraction of the pelvic floor muscles anal sphincter or puborectalis
B2. OR < 20% relaxation of basal resting sphincter pressure by manometry, imaging, or EMG
C. Inadequate propulsive forces assessed by manometry or imaging

INITIAL EVALUATION - DIGITAL RECTAL EXAM
Resting tone Augmentation of sphincter tone with squeeze Contraction of puborectalis during squeeze Tenderness of PR may indicate levator ani syndrome Palpate anteriorly for rectocele Have pt bear down or “expel my finger”
Should note descent of PR Should note relaxation of sphincter tone

DYSSYNERGIC DEFECATION (DD)
Defined as paradoxical contraction or failure to relax the pelvic floor

Abnormal Push Maneuver with Increase in EAS Pressure
04/19/23 50
ANORECTAL MANOMETRY
BALLOON EXPULSION TEST
Balloon tipped catheter inserted into the rectum and inflated with 50mL of H2O
Timed measurement of patient’s ability to evacuate balloon in privacy
Balloon expulsion time of >2 min is abnlAbnl study suggests obstructive defecation
etiologies include DD, Hirschsprung’s, rectal prolapse, rectocele, enterocele, strictures

BALLOON EXPULSION TEST
Concordance of failed BET and DD of 72-94%
04/19/23 52
Wald A, Bharucha AE, Cosman BC, Whitehead WE.Am J Gastroenterol. 2014 Aug;109(8):1141-57
Sensitivity and Specificity of BET as defined by ARM

Capsule contains 24 radio-opaque markers
Patient takes 1 capsule by mouth with water on Day 0
Patient should not use laxatives, enemas or suppositories for 24hrs before or for 5 days after
X-ray on Day 5 Abnl if 20% (>5-6 markers
remain)
STANDARD SITZ-MARKER TEST

If over 80% (5 or fewer markers remain) of markers are passed by day 5, colonic transit is grossly normal
If most rings are gathered in the rectosigmoid, may have functional outlet obstruction (may need anorectal manometry with balloon expulsion or defecography)
If most rings are scattered about the colon, patient most likely has hypomotility or ‘colonic inertia’
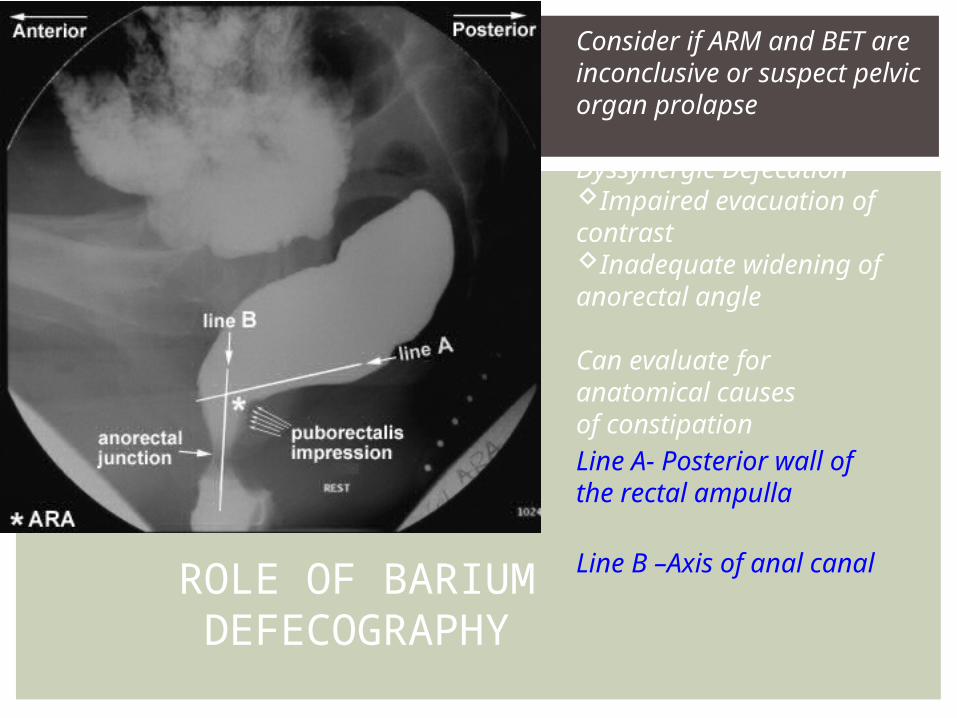
Line A- Posterior wall of the rectal ampulla
Line B –Axis of anal canalROLE OF BARIUM DEFECOGRAPHY
Consider if ARM and BET are inconclusive or suspect pelvic organ prolapse
Dyssynergic DefecationImpaired evacuation of contrast Inadequate widening of anorectal angle
Can evaluate foranatomical causesof constipation

OTHER CAUSES OF DEFECATION D/O
Rectal Prolapse
Descending Perineum Syndrome
Rectocele
Enterocele

Lee, et al. Neurogastroenterology & Motility 25 MAR 2015
Long‐term efficacy of biofeedback therapy in patients with dyssynergic defecation: results of a median 44 months follow‐up
Biofeedback therapy is an instrument-based behavioral learning process centered on operant conditioning

http://youtu.be/lrTxCLUDDAQ
BIOFEEDBACK VIDEO
04/19/23 58

Pelvic Floor Disorders are common but under-recognized
Bowel disturbance (diarrhea) biggest risk factor for fecal incontinence
Initial management should include behavioral modification/biofeedback and treatment of bowel disturbance
Newer options Like Sacral Neuromodulcation offer hope from chronic sufferers from fecal incontinence (? constipation)
04/19/23 59
CONCLUSION

















