FELANPE Asuncion, October 2010 Prof. Rémy Meier Prof. Rémy Meier MD MD University University Hospital Hospital Liestal, Liestal, Enteral and Enteral and Parenteral Parenteral Guidelines Guidelines ESPEN ESPEN
Enteral and Parenteral Enteral and Parenteral GuidelinesGuidelines
ESPENESPEN
ResearchResearch
Clinical resultsClinical results
GuidelinesGuidelines
Aims of the Aims of the ESPEN-GuidelinesESPEN-Guidelines
The ESPEN-Guidelines „Enteral and The ESPEN-Guidelines „Enteral and Parenteral Nutrition“ Parenteral Nutrition“ aimaim to assist clinical to assist clinical practitioners, dietitians and nurses who practitioners, dietitians and nurses who provide enteral and parenteral nutrition provide enteral and parenteral nutrition support to patients in all care settings as support to patients in all care settings as well as to give information to decision-well as to give information to decision-makers in the health care system makers in the health care system
Methodology for the Methodology for the development of the ESPEN development of the ESPEN Guidelines on enteral and Guidelines on enteral and parenteral nutritionparenteral nutrition
• Systemic reviewSystemic review
• Evidence basedEvidence based
• Consensus basedConsensus based
Manpower ENManpower EN
• 13 disease-specific working 13 disease-specific working groupsgroups
• 88 experts in clinical nutrition88 experts in clinical nutrition
• 20 countries20 countries
Manpower PNManpower PN
• 11 disease-specific working 11 disease-specific working groupsgroups
• 87 experts in clinical nutrition87 experts in clinical nutrition
• 16 countries16 countries
Evidence gatheringEvidence gathering
• Structured literature searchStructured literature search
• Defined search strategyDefined search strategy(including criteria, specific key words)(including criteria, specific key words)
• Assessment of the quality and the Assessment of the quality and the strength of the literaturestrength of the literature
• Defining the level of evidenceDefining the level of evidence
• Defining the grade of recommendationDefining the grade of recommendation
• According to the criteria of SIGN (ScottishAccording to the criteria of SIGN (ScottishIntercollegiale Guideline Network, No 39,Intercollegiale Guideline Network, No 39,1999) and1999) and
• According to the criteria of AHCPRAccording to the criteria of AHCPR(Agency for Health Care Policy and Research, (Agency for Health Care Policy and Research, No 92-0023, 1993)No 92-0023, 1993)
The quality and strength of the The quality and strength of the
supporting evidence was gradedsupporting evidence was graded
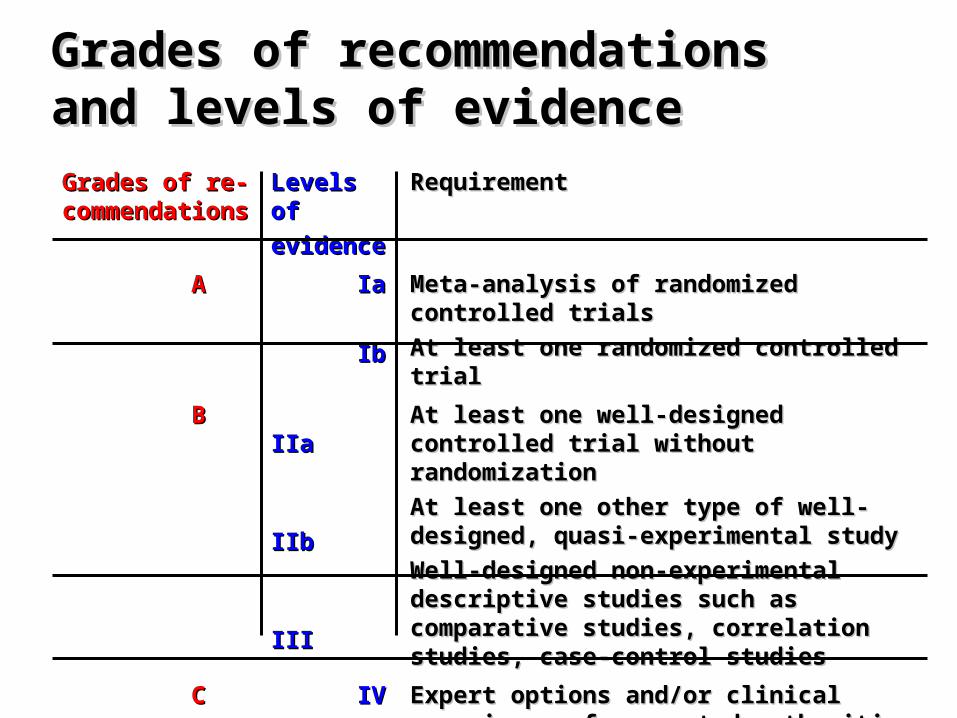
Grades of recommendations and Grades of recommendations and levels of evidencelevels of evidence
Grades of re-Grades of re-commendationscommendations
Levels of Levels of
evidenceevidence
RequirementRequirement
AA IaIa
IbIb
Meta-analysis of randomized controlled trialsMeta-analysis of randomized controlled trials
At least one randomized controlled trialAt least one randomized controlled trial
BB IIaIIa
IIbIIb
IIIIII
At least one well-designed controlled trial At least one well-designed controlled trial without randomizationwithout randomization
At least one other type of well-designed, At least one other type of well-designed, quasi-experimental studyquasi-experimental study
Well-designed non-experimental descriptive Well-designed non-experimental descriptive studies such as comparative studies, studies such as comparative studies, correlation studies, case-control studiescorrelation studies, case-control studies
CC IVIV Expert options and/or clinical experience of Expert options and/or clinical experience of respected authoritiesrespected authorities
The recommendations were not The recommendations were not only based on the evidence levels only based on the evidence levels of the studies of the studies but also on the but also on the judgement of the working group judgement of the working group concerning the consistency, concerning the consistency, clinical relevance and validity of clinical relevance and validity of the evidencethe evidence
The preparation and publication of theThe preparation and publication of the
ESPEN-Guidelines on Enteral and ESPEN-Guidelines on Enteral and Parenteral Nutrition Parenteral Nutrition
were exclusively funded by ESPENwere exclusively funded by ESPEN
Problems with Problems with RecommentationsRecommentations
4-5 levels of recommendations 4-5 levels of recommendations A-EA-E
ESPEN-EN-Guidelines 2006 ESPEN-EN-Guidelines 2006 Surgery ISurgery I
Recommendation ARecommendation A
• Preoperative fasting from midnight isPreoperative fasting from midnight is
unnecessary in most patientsunnecessary in most patients• Interruption of nutritional intake is Interruption of nutritional intake is
unnecessary after surgery in most patients unnecessary after surgery in most patients • Use nutritional support in patients with Use nutritional support in patients with
severe nutritional risk for 10-14 days prior severe nutritional risk for 10-14 days prior
to major surgery even if surgery has to be to major surgery even if surgery has to be
delayed. delayed.
Nutritional risk refers to at Nutritional risk refers to at least one idem:least one idem:
- Weight loss > 10-15% within 6 monthsWeight loss > 10-15% within 6 months- BMI < 18.5 kg/m2BMI < 18.5 kg/m2- Subjective Global Assessment Grade CSubjective Global Assessment Grade C- Serum albumin <30 g/l Serum albumin <30 g/l
(with no evidence of hepatic or renal (with no evidence of hepatic or renal
dysfunction)dysfunction)
ESPEN-EN-Guidelines 2006ESPEN-EN-Guidelines 2006 Surgery IISurgery II
Recommendation ARecommendation A
• Patients undergoing surgery who are considered to Patients undergoing surgery who are considered to have no specific risk for aspiration, may drink clear have no specific risk for aspiration, may drink clear fluids until 2 h before anaesthesia. Solids are allowed fluids until 2 h before anaesthesia. Solids are allowed until 6 h before anaesthesia until 6 h before anaesthesia
• Initiate normal food intake or enteral feeding early Initiate normal food intake or enteral feeding early after gastrointestinal surgeryafter gastrointestinal surgery
• Oral intake, including clear liquids, can be initiated Oral intake, including clear liquids, can be initiated within hours after surgery to most patients within hours after surgery to most patients undergoing colon resectionsundergoing colon resections
ESPEN-EN-Guidelines 2006 ESPEN-EN-Guidelines 2006 Surgery IIISurgery III
Recommendation ARecommendation A• Apply tube feeding in patients in whom early oral Apply tube feeding in patients in whom early oral
nutrition can not be initiated, with special regard to nutrition can not be initiated, with special regard to thosethose- undergoing major head and neck or - undergoing major head and neck or
gastrointestinal surgery for cancergastrointestinal surgery for cancer- with severe trauma- with severe trauma- with obvious undernutrition at the time of surgery- with obvious undernutrition at the time of surgery
• Initiate tube feeding for patients in need within 24 h Initiate tube feeding for patients in need within 24 h after surgeryafter surgery
• Placement of a needle catheter jejunostomy or Placement of a needle catheter jejunostomy or
naso-jejunal tube is recommended for all candidates naso-jejunal tube is recommended for all candidates for for TFTF undergoing major abdominal surgery undergoing major abdominal surgery
ESPEN-EN-Guidelines 2006 ESPEN-EN-Guidelines 2006 Surgery IVSurgery IV
Recommendation ARecommendation A
• Placement of a needle catheter Placement of a needle catheter jejunostomy or naso-jejunal tube is jejunostomy or naso-jejunal tube is recommended for all candidates for recommended for all candidates for TFTF undergoing major abdominal surgery. undergoing major abdominal surgery.
• Use EN preferably with Use EN preferably with immuno-modulating substrates immuno-modulating substrates (arginine, (arginine, ωω-3 fatty acids and nucleotides) -3 fatty acids and nucleotides)
perioperatively independent of perioperatively independent of the nutritional risk for those patients the nutritional risk for those patients
This patients are specifiedThis patients are specified
Those patients who benefit are patientsThose patients who benefit are patients
- undergoing major neck surgery for cancer- undergoing major neck surgery for cancer
(laryngectomy, pharyngectomy)(laryngectomy, pharyngectomy)- undergoing major abdominal cancer surgeryundergoing major abdominal cancer surgery
(oesophagectomy, gastrectomy, and (oesophagectomy, gastrectomy, and pancreato-duodenectomy)pancreato-duodenectomy)
- after severe trauma- after severe trauma
ESPEN-PN-Guidelines 2009ESPEN-PN-Guidelines 2009
• What was new ?What was new ?
The recommendations of the The recommendations of the EN guidelines were taken EN guidelines were taken and and the evidences of parenteral the evidences of parenteral nutrition of each topic were nutrition of each topic were added added
ESPEN-PN-Guidelines 2009 ESPEN-PN-Guidelines 2009 Surgery ISurgery I
The main goals of perioperative The main goals of perioperative nutritional support are to minimize nutritional support are to minimize negative protein balance bynegative protein balance byavoiding starvation, with theavoiding starvation, with thepurpose of maintaining muscle,purpose of maintaining muscle,immune, and cognitive function, immune, and cognitive function, and to enhance postoperativeand to enhance postoperativerecovery!recovery!
ESPEN-PN-Guidelines 2009ESPEN-PN-Guidelines 2009Surgery IISurgery II
Recommendation ARecommendation A
• Preoperative parenteral nutrition is Preoperative parenteral nutrition is indicated in severely undernourished indicated in severely undernourished patients who cannot be adequately patients who cannot be adequately orally or enterally fedorally or enterally fed
• Postoperative parenteral nutrition is Postoperative parenteral nutrition is beneficial in undernourished patients in beneficial in undernourished patients in whom enteral nutrition is not feasable whom enteral nutrition is not feasable or not toleratedor not tolerated
ESPEN-PN-Guidelines 2009 ESPEN-PN-Guidelines 2009 Surgery IIISurgery III
Recommendation ARecommendation A
• Postoperative parenteral nutrition is Postoperative parenteral nutrition is beneficial in patients with beneficial in patients with postoperative complications impairing postoperative complications impairing gastrointestinal function who are gastrointestinal function who are unable to receive and absorb unable to receive and absorb adequate amounts of oral/enteral adequate amounts of oral/enteral feeding for at least 7 daysfeeding for at least 7 days
ESPEN-PN-Guidelines 2009 ESPEN-PN-Guidelines 2009 Surgery IVSurgery IV
Recommendation ARecommendation A
• In patients who require postoperative In patients who require postoperative artificial nutrition, enteral feeding or a artificial nutrition, enteral feeding or a combination of enteral and combination of enteral and supplementary parenteral feeding is supplementary parenteral feeding is the first choicethe first choice
• Weaning from parenteral nutrition is Weaning from parenteral nutrition is not necessary not necessary
Recommendations Recommendations on Enteral Nutritionon Enteral Nutrition
• Total number of recommendationsTotal number of recommendations 226 226• Recommendations ARecommendations A = 55= 55
(25%)(25%)• Redommendations BRedommendations B = 39 = 39
(17%)(17%)• Recommendations CRecommendations C = 132 = 132
(58%)(58%)
Recommendations Recommendations on Parenteral Nutritionon Parenteral Nutrition
• Total number of recommendationsTotal number of recommendations 300 300• Recommendations ARecommendations A = 48= 48
(16%)(16%)• Redommendations BRedommendations B = 94 = 94
(28%)(28%)• Recommendations CRecommendations C = 158 = 158
(56%)(56%)
Over 50% of the recommendationsOver 50% of the recommendationsare are only C only C „Expert opinions and/or„Expert opinions and/orclinical experience of respected clinical experience of respected authorities“authorities“
There is still a lack of There is still a lack of good clinical studiesgood clinical studiesin clinical nutrition!!in clinical nutrition!!
The guidelines do provide evience-The guidelines do provide evience-based information about based information about somesome specific specific problems like timing, dosing, problems like timing, dosing, composition and route of application, composition and route of application, and under which conditions limitation or and under which conditions limitation or withdrawal of nutritional support like withdrawal of nutritional support like other therapies might be adequateother therapies might be adequate
but but
they also show they also show where additional studies where additional studies are neededare needed
• Guidelines shows were Guidelines shows were no no enough evicence for a clear enough evicence for a clear
recommendation is availablerecommendation is available• This can help to design new This can help to design new
studies to fill in the missing studies to fill in the missing informationinformation
Genereation of newGenereation of newhypothesis using guidelineshypothesis using guidelines
• Selection of endpoints is crucial!Selection of endpoints is crucial!• Mortality is difficult in nutritinal studies Mortality is difficult in nutritinal studies (high number of patients needed)(high number of patients needed)• Morbidity is often used Morbidity is often used • Changes in body composition Changes in body composition butbut• QoL, function, mood, costs …. can be important in special situation QoL, function, mood, costs …. can be important in special situation
EndpointsEndpoints
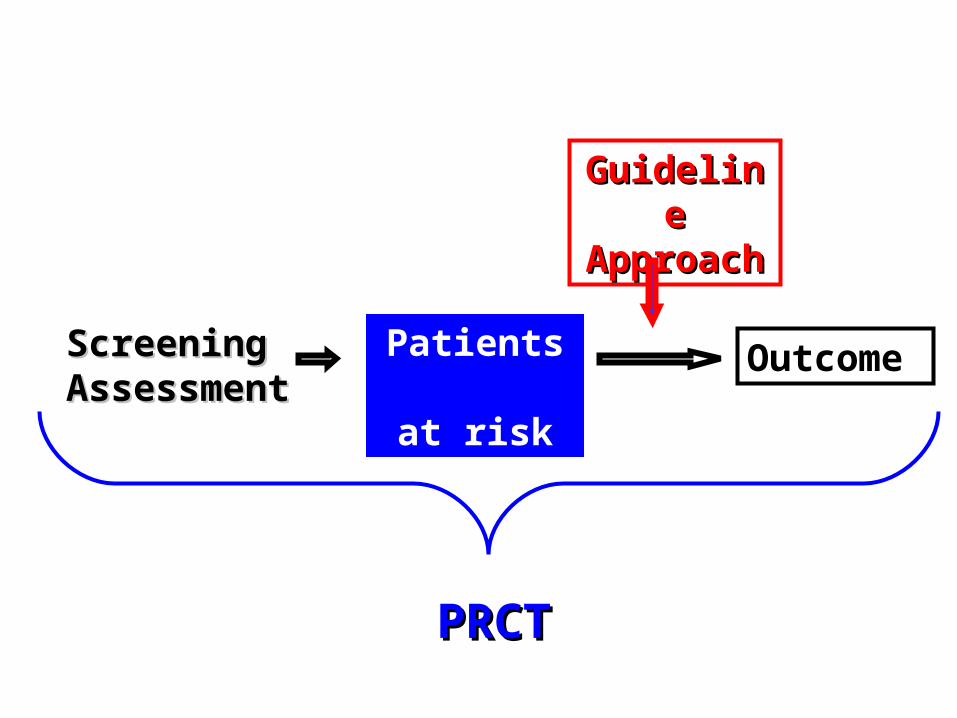
Nutritional screening of all patientsNutritional screening of all patients
Nutritional support using Nutritional support using guidelinesguidelines
Regular auditsRegular audits
Continuous trainingContinuous training
MonitoringMonitoring
Implementation of guidelinesImplementation of guidelines
GuidelineGuidelineApproachApproach
OutcomePatients at risk
ScreeningScreeningAssessmentAssessment
PRCTPRCT
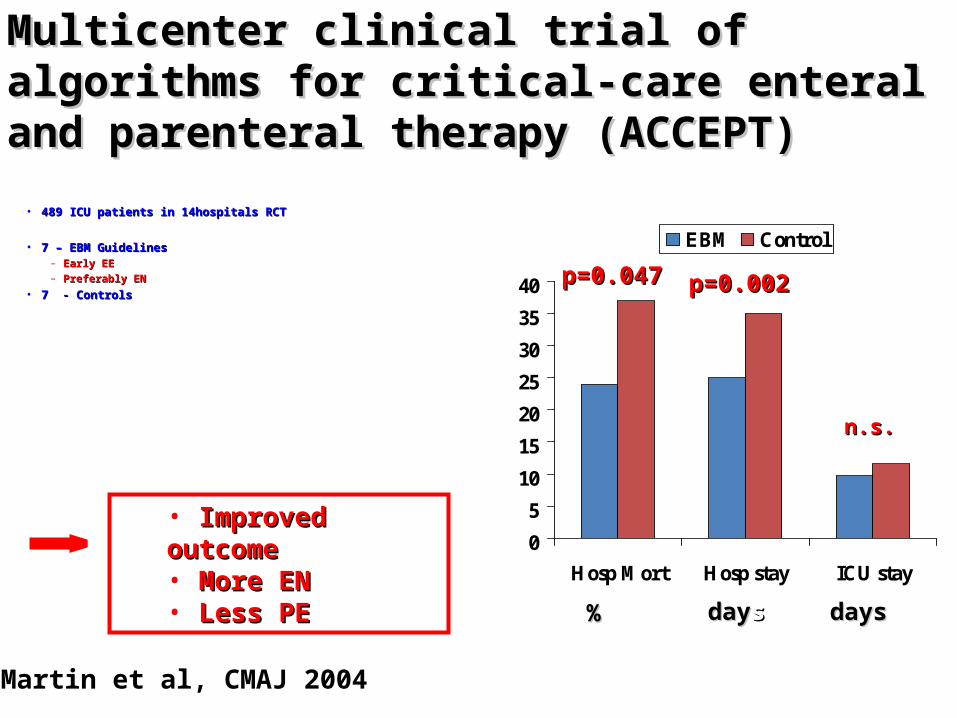
• 489 ICU patients in 14hospitals RCT489 ICU patients in 14hospitals RCT
• 7 – EBM Guidelines7 – EBM Guidelines– Early EEEarly EE– Preferably ENPreferably EN
• 7 - Controls7 - Controls
0
5
10
15
20
25
30
35
40
Hosp Mort Hosp stay ICU stay
EBM Control
%% daydayss daysdays
p=0.047p=0.047 p=0.002p=0.002
n.s.n.s.
Multicenter clinical trial of algorithms for Multicenter clinical trial of algorithms for critical-care enteral and parenteral therapy critical-care enteral and parenteral therapy (ACCEPT)(ACCEPT)
Martin et al, CMAJ 2004
• Improved outcomeImproved outcome• More ENMore EN• Less PELess PE
Appropriate use of PN
• First monitoringFirst monitoring
Implementation of clinical Implementation of clinical practice guidelinespractice guidelines
• Control monitoringControl monitoring
• Appropriate / inappropriate wasAppropriate / inappropriate was
pre-definedpre-defined
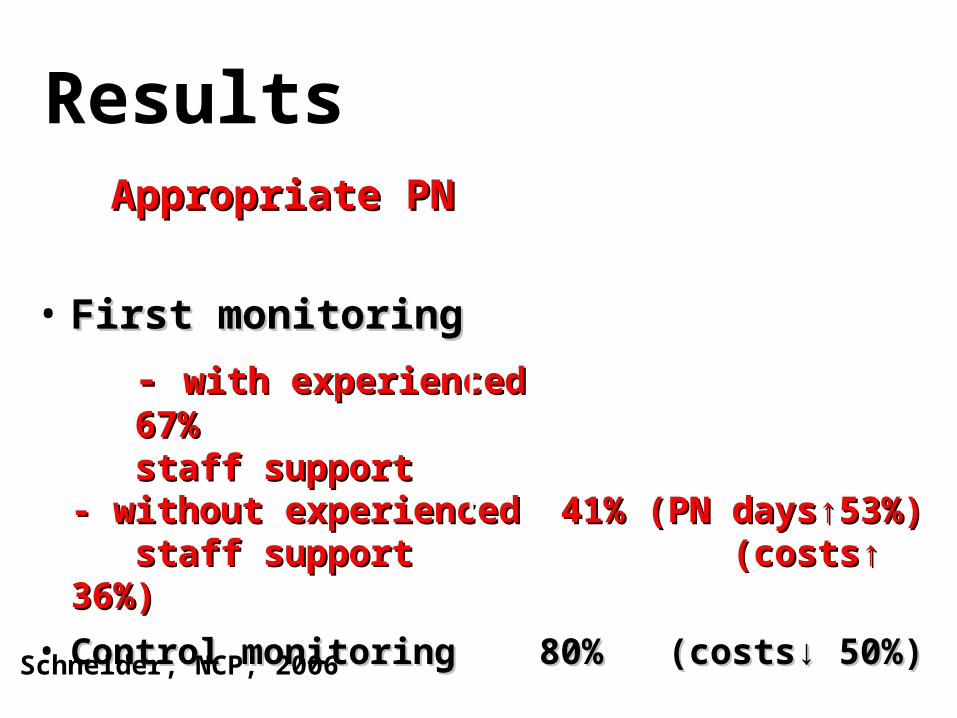
Results Appropriate PNAppropriate PN
• First monitoringFirst monitoring
- - with experienced 67%with experienced 67% staff support staff support- without experienced- without experienced 41% (PN days 41% (PN days↑53%)↑53%) staff support staff support (costs↑ 36%) (costs↑ 36%)
• Control monitoringControl monitoring 80% (costs↓ 50%)80% (costs↓ 50%)
Schneider, NCP, 2006
SummarySummary
The guidelines do provide evience-based The guidelines do provide evience-based information about specific problems like information about specific problems like timing, dosing, composition and route of timing, dosing, composition and route of applicationapplication
They also show They also show where additional studies are where additional studies are needed needed and under which conditions and under which conditions limitation or withdrawal of nutritional limitation or withdrawal of nutritional support like other therapies might be support like other therapies might be adequateadequate
• The ESPEN-Guidelines are The ESPEN-Guidelines are separate for enteral- and separate for enteral- and parenteral nutritionparenteral nutrition
• It would be easier to have It would be easier to have combined guidelinescombined guidelines
LimitationsLimitations
ConclusionConclusionThe ESPEN guidelines on enteral and The ESPEN guidelines on enteral and parenteral nutrition parenteral nutrition reflect the current reflect the current medical knowledge in the field of enteral medical knowledge in the field of enteral and parenteral nutrition therapy and parenteral nutrition therapy and and summarize the evidence when enteral summarize the evidence when enteral nutrition is indicated and which goals nutrition is indicated and which goals can be reached in regard to nutritional can be reached in regard to nutritional state, quality of life and outcome state, quality of life and outcome
PublicationPublication
• Clinical Nutrition Vol 25 (2), Clinical Nutrition Vol 25 (2), April 2006 (Enteral)April 2006 (Enteral)• Clinical Nutrition Vol 28, August 2009Clinical Nutrition Vol 28, August 2009