239
Pathology of the Female GenitalTract DEPT OF PATHOLOGY
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | drsapna-harsha |
| View: | 674 times |
| Download: | 1 times |

Pathology of the Female GenitalTract
DEPT OF PATHOLOGY

LOWER GENITAL TRACT
Vulva, Vagina, Cervix-
Infections and neoplasms
Embroyology and Anatomy

Female Genital Infections-
CandidaTrichomoniasis Gardnerella – most common
Gonnorrhoea,Chlamydia –female infertility
Mycoplasma –spontaneous abortion
Viruses asHPV- cancer

HSV Type II-cervix, vagina, vulva
Papules-vescicle-ulcersCx and vagina-- Leukorrhea
Latent InfectionRecurrenceTo neonates
Diagnosis-serology,microscopy

Trichomonas Vaginalis flagellated ovoid protozoanStrawberry CxMycoplasmaCandida species

Pelvic inflammatory disease
SymptomsOrganisms_Gonococcus,Chlamydia trachomatis, Clostridium PerfringensMode of infection and spread

Gonococcus-an intracellular diplococcusDiagnosis-culture, papsmear
Endometrium spared
Cl .features--A/c Suppurative salpingitis salpingo-oophoritis Tubo ovarian abscesses Pyosalpinx, Hydrosalpinx

Complications
Peritonitis
Intestinal obstn
Bacteraemia
Infertility

Vulva
Vulvitis
Bartholin Cyst
Vestibular Adenitis

Non-neoplastic lesions
Leukoplakia
Lichen sclerosus-subepithelial fibrosis
Lichen simplex chronicus-acanthosis, and hyperkeratosis
Squamous Hyperplasia

Vulvar Leukoplakia� Leukoplakia: A descriptive clinical term; refers to a white plaque or patch on a mucosal surface
� Causes of vulvar leukoplakia:
1.Vitiligo (loss of pigment)
2.Inflammatory dermatosis: p.e. psoriasis
3.Squamous intraepithelial neoplasms of the vulva (VIN) and invasive carcinoma
4.Paget’s disease

Leukoplakia

Tumors of Vulva
Benign-Papillary hidradenomaCondyloma accuminatum(HPV 6&11)Venereal Wart,Mucosal PolypSyphilitic Condyloma latumViral cytopathic effect-Koilocytic atypia


Premalignant and malignant neoplasms – SCC,BCC,melanomas or adenocarcinomas.
SCC-HPV related SChyperplasia
Vulvar Intraepithelial Neoplasia
Extramammary Paget Disease






Paget’s Disease


Melanoma

Vagina
VIN and Sq.cell carcinoma
Adenocarcinoma
Embryonal Rhabdomyosarcoma



Uterine Cervix
Cervicitis
Tumors



Cervicitis“Erosions” and development of the transformation zone
(T zone). Nabothian cysts.
Infectious and non-infectious cervicitis
Vaginal flora, Chlamydia trachomatis, Ureaplasma urealyticum, Trichomonas vaginalis, Candida species, Neisseria gonorrhoeae, Herpes simplex II, and HPV.

acute nonspecific: postpartum, Staphylococci/Streptococci
Nonspecific (chronic) cervicitis
Gross: reddening, swelling, and granularity around margins of external cervical os.
Microscopy: Hyperplasia and reactive atypia of epithelium, no dysplasia, glycogen depletion . Mononuclear cell infiltrate, nabothian cysts. Viral inclusions (HSV). Plasma cells in C. trachomatis.



CervicitisLeukorrhea
Culture interpretation*.If severe >>>differentiation from carcinoma:
colposcopy and biopsy.Subsoil for carcinogenesis?
May lead to sterility (fibrosis/ unfavorable medium for sperm).


Endocervical polyp Inflammatory polypoid masses, cm. Smooth surface composed of columnar
mucus-secreting cells (endocervical epithelium) with underlying cystically dilated glands filled with mucus. Stromal edema inflammatory mononuclear cells.
Squamous metaplasia and ulceration.




Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
Cervical cancer was the most frequent form of cancer around the world.
Impact of Papanicolaou screening: Decrease incidence of invasive tumors and increase incidence in the detection of precursors (dysplasias/CINs) lesions.
Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
Peak incidence1. CIN : 30 Y2. Invasive carcinoma: 45 yRisk factors1. Early age at first intercourse2. Multiple sexual partners3. A male partner with multiple previous
sexual partners

Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
Higher incidence in lower socioeconomic groups
Genital infections
Exposure to oral contraceptives
Rarity among virgins
Multiple pregnancies
Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
T zone
High grade dysplasia/HPV 16 and 18
Viral isolation and typing do not predict the course.
Follow up: cytology, colposcopy (acetic acid test), biopsy*.


HPV: 85-90% of lesionsSerotypes: 1. High risk: 16, 18, 31, and 33.2. Low risk (associated with condylomas):
6, 11, 42, and 44.Integration of viral genes into host
genome>>transcription>>translation of specific proteins that inactivate p53 and retinoblastoma tumor suppressor genes.
Cervical Intraepithelial Neoplasia (CIN) and Carcinoma

Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
Viral infection does not mean that a women will develop cancer.
10-15% HPV: negative
Other carcinogens, genetic factors, host immunity, cigarette smoking.

Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
Importance of early detection, adequate follow up and management.
Histologic grading of precursor lesions:
1. CIN I: Mild dysplasia
2. CIN II: Moderate dysplasia
3. CIN III : Severe dysplasia/carcinoma in situ



Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
Cytologic grading of precursor lesions1) LOW GRADE SQUAMOUS
INTRAEPITHELIAL LESIONS
[CIN I and Condylomas (koilocytosis)]
2) HIGH GRADE SQUAMOUS INTRAEPITHELIAL LESIONS
[CIN II, CIN III/CIS]

Cervical Intraepithelial Neoplasia (CIN) and Carcinoma
Natural History
Different studies = different populations = different results
CIN I: 50 to 60% regress, persists 30%, and progress to CIN III 20%. 1 to 5% become invasive.
CIN III: 33% regress, progression varies from 6 to 74%.
Schilling test

Invasive Carcinoma of the Cervix80-95%: Squamous cell carcinomas
Multifactorial disease
Preventable
Gross (macroscopic appearance)
Fungating (exophytic)
Ulcerative (endophytic)
Infiltrative

Invasive Carcinoma of the Cervix
ROUTES OF INVASION
Direct spread-adjacent stroma, vagina, pelvic wall.
Local and distant spread to lymph nodes
Distant metastasis to lungs , liver ,bone marrow etc




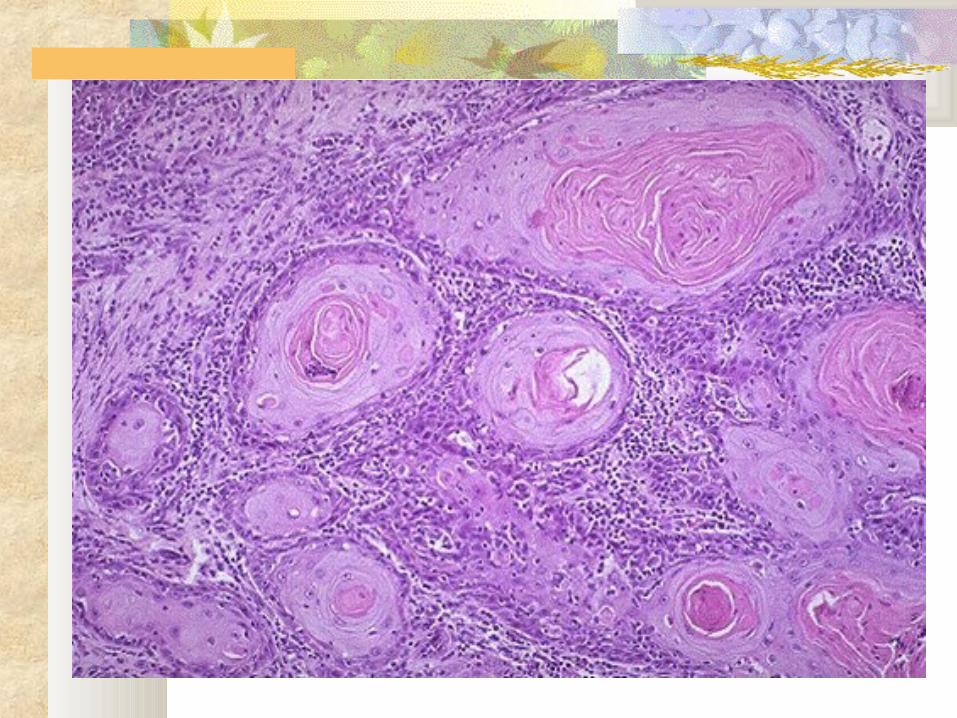
Invasive Carcinoma of the Cervix Squamous cell carcinoma
Well to poorly differentiated Adenocarcinomas Adenosquamous carcinomas Staging



Invasive Carcinoma of the Cervix CIS: Asymptomatic, Leukorrhea Carcinoma: Vaginal bleeding, leukorrhea,
painful coitus, and dysurea DX: Colposcopy: acetic acid test, Bx Mortality: Related to local extension*:
ureter obstruction or invasion of bladder or rectum.

Invasive Carcinoma of the Cervix Importance of early diagnosis Time….? 5-year survival rate:
1. Stage 0 (CIS): 100%
2. Stage I: 85% to 90%
3. Stage II: 70 to 75%
4. Stage III: 35%
5. Stage IV: 10%

Invasive Carcinoma of the CervixStage 0: Carcinoma in situStage I: Tumor confined to the cervixStage II: Tumor extends beyond the cervix but not
onto the pelvic side wallStage III: Tumor extends to the pelvic side wall or
to the lower one third of vagina, or causes hydronephrosis, or a nonfunctioning kidney
Stage IV: Tumor extends beyond true pelvis, or biopsy-proved involvement of bladder or rectal mucosa.

Invasive Carcinoma of the CervixManagement
LEEP Conization Hysterectomy Pelvic exenteration Radiotherapy

FEMALE GENITAL SYSTEM
Endometrium




Body of the Uterus
Endometritis
Adenomyosis
Endometriosis
Dysfunctional uterine bleeding
Endometrial hyperplasia
Endometrial polyps
Leiomyomas and leiomyosarcomas
Endometrial carcinomas

Endometritis Clinical settings:1. Chronic gonorrheal pelvic disease2. Tuberculosis3. Retained Product of conception4. IUD5. Spontaneously Histology: Irregular disposition and
proliferation of endometrial glands, plasma cells and lymphocytes in the stroma

Adenomyosis
Growth of the basal layer of endometrium (glands and stroma) down into the myometrium between the muscle bundles
Thick myometrium: reactive hypertrophy Nonfunctional: no bleeding* Menorrhagia, dysmenorrhea, and
premenstrual pain


Endometriosis Infertility, dysmenorrhea, pelvic pain. Foci of endometrial tissue in pelvis
(ovaries, pouch of Douglas, uterine ligaments, tubes, rectovaginal septum).
Sometimes in umbilicus, LNs, lungs, skin, heart, bone.
Theories of genesis: Regurgitation, metaplastic, and lymphovascular

Endometriosis Functional endometrium: cyclic bleeding
Complications:Fibrosis,adhesions: pain, sterility
Gross: red-blue to yellow-brown nodules, chocolate cysts in ovaries
Microscopy: Endometrial glands, stroma, and hemosiderin deposition

Endometriosis
Theories of genesis:
1. Regurgitation: menstrual backflow through fallopian tubes and subsequent implantation
2. Metaplastic: metaplasia of coelomic epithelium
3. Lymphovascular dissemination


EndometriosissitesOvaries,ligaments,rectovaginal areas,pelvisscars,umbilicus,vagina,vulva&appendix



Dysfunctional Uterine Bleeding
abnormal bleeding with no organic lesion
Etiology of uterine bleeding varies with age :prepuberty
, adolescence,
reproductive age,
perimenopause, and postmenopause.
Dysfunctional Uterine BleedingThree functional groups (E/P)
1. Anovulatory cycles-metabolic disorders, ovarian lesions,sys diseases,unexplainable
2. Inadequate luteal phase-inadequate corpus leuteum
3. Contraceptive induced bleeding

Anovulatory Cycles Common at both ends of reproductive life Hypothalamic-pituitary axis, thyroid, or adrenal
dysfunction Functioning ovarian producing lesion,
malnutrition, obesity, stress, debilitating disease Persistence of proliferative “growth” until
endometrium collapse, spiral arteries rupture, and bleeding occurs.

Inadequate Luteal Phase Corpus luteum fail to mature normally or regress
prematurely: less progesterone is produced: delay and inadequate secretory phase
Contraceptive Induced Bleeding Imbalance in the ratio Estrogen/Progesterone

Endometrial Hyperplasia
estrogen>>>>Progesterone: Polycystic ovaries(Stein-Leventhal syndrome), cortical stromal hyperplasia, granulosa-theca ovarian tumors
Simple Hyperplasia Complex Hyperplasia without atypia Complex Hyperplasia with atypia: 20/25% risk of
carcinoma Continuum of changes based on duration and level of
estrogen excess Causes irregular uterine bleeding Biopsy and follow up

Endometrial Hyperplasia


Endometrial Polyps
Uterine bleeding
Gross: Sessile(rarely pedunculated) rounded lesions: 0.5 to 3 cm
Microscopy: Surface lined by columnar epithelium, stroma (monoclonal stromal cells with rearrangement of 6p21) with thick-walled vessels, and endometrial glands some of which appear cystically dilated.
Occur at any age, but common around menopause
Endometrial Polyp


Uterine Malignancy
Endometrial- glands
Stroma
Both glands and stroma
Myometrial-
Leiomyoma
Benign smooth muscle tumor
“Fibroids”, “Myomas”
30 to 50% of women during reproductive life.
Estrogen stimulates their growth
Involutes after menopause
Monoclonal, 40% have non-random chromosomal abnormalities

Leiomyoma
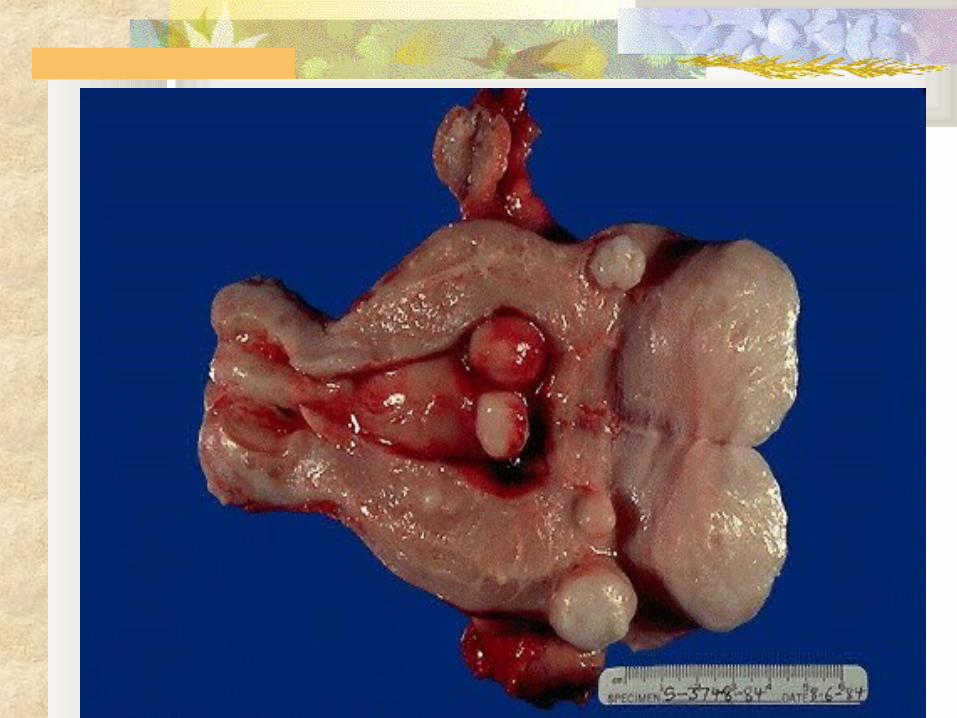
Gross: Well circumscribed, firm, gray, white mass. Whorled cut surface.
Singly or multiple. Few cm to large masses.
Intramucosal, intramural, and/or subserosal location. Parasitic leiomyomas
Microscopy: Interlacing bundles of smooth muscle cells. Foci of ischemic necrosis, fibrosis, cyst degeneration, hemorrhage, and calcification are not uncommon.

Leiomyoma
Leiomyoma


Leiomyoma
Asymptomatic
If Symptoms: Bleeding (menorrhagia) or “mass effect”
Progression to sarcomas?

Leiomyosarcoma
usually solitary tumorsDerived from mesenchymal myometrial cellsGross: 1. Bulky masses infiltrating uterine wall2. Polypoid lesions projecting into uterine
cavity3. Discrete tumors(~ leiomyomas)

Leiomyosarcoma

Leiomyosarcoma
Microscopy: Increased cellularity, mitosis, nuclear atypia, and necrosis.
Recurrence and metastasis are not uncommon
5 year survival rate: 40%

Leiomyosarcoma

Endometrial Carcinoma
Most frequent cancer of the female genital tract in USA
55 to 65 y (uncommon <40y)
Risk factors:1. Obesity: synthesis of estrogen in fat deposits2. Diabetes3. Hypertension4. Infertility: anovulatory cycles

Endometrial Carcinoma
Hyperestrinism : HRT, estrogen secreting ovarian tumors, etc.
Background of endometrial hyperplasia
20%: no Hyperestrinism and no hyperplasia: older patients, poor prognosis

Endometrial Carcinoma
Gross:Diffuse thickening of uterine wall: Infiltrative
Exophytic form
Filling of the endometrial cavity with a firm to soft partially necrotic tumor.
Myometrium invasion/ serosa/ LN


Endometrial Carcinoma
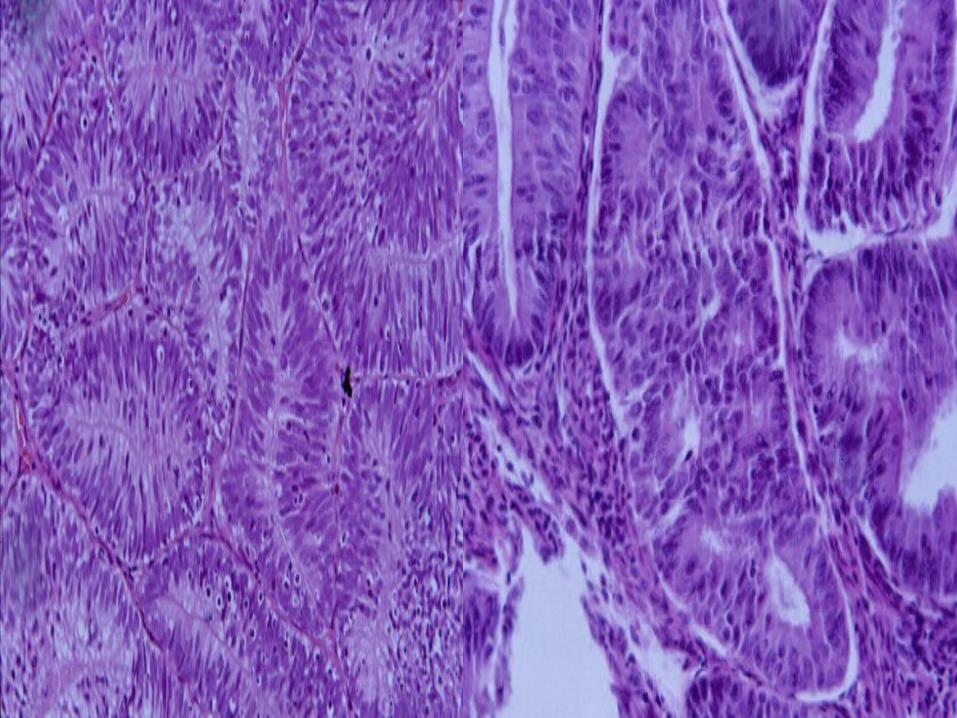
Adenocarcinomas (Adenocarcinomas with squamous metaplasia, Adenoacanthoma, Adenosquamous carcinoma)
Endometrioid
Papillary serous carcinoma
Clear cell adenocarcinoma


Endometrial Carcinoma
Grade: Degree of cytologic differentiation. GH1, G2, and G3
Stage: Spread of the tumor
1. I: Confined to corpus2. II: Extension to cervix3. III: Extension outside the uterus , but still
confined to pelvis4. IV: Extension outside the pelvis

Endometrial Carcinoma
Leukorrhea and irregular bleeding in a postmenopausal patient
Enlargement of uterus and fixation to surrounding structures
Late metastasizing neoplasm to LN and other organs5-year survival rate:1. Stage I: 90%2. Stage II: 30 to 0%3. Stage III and IV: less than 20%

Mixed Mullerian Tumors
adenofibromaadenosarcomaCarcinosarcoma
with or withoutdifferentiation(Cartilage,bone&muscle)

FEMALE GENITAL SYSTEM
FALLOPIAN TUBES AND OVARY

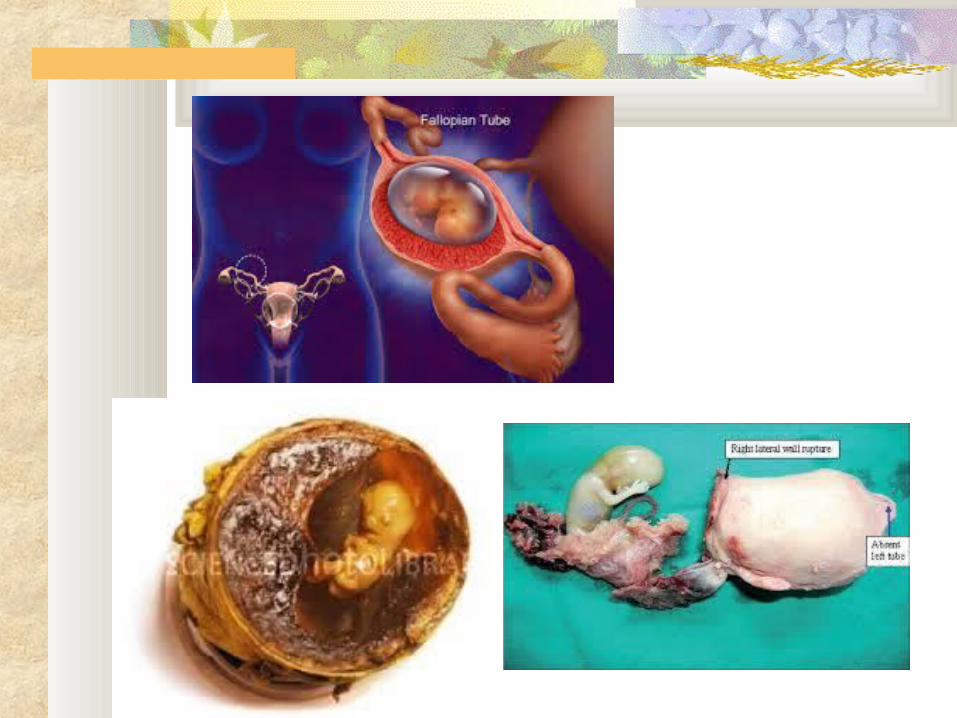
Fallopian tube
Common affliction is inflammation, pelvic inflammatory disease
gonorrhea, chlamydia, mycoplasma, streptococci and staphylococci
fever, lower abdominal pain and pelvic mass
•Tubal pregnancy
•Adenocarcinoma




Ovary
Normal ovary measures 3-5 x 1.5-3 x 0.6-1.5 cm and weighs 5-8 grams during reproductive age.

Newborn ovaryNote presence of numerous primordial follicles filling the cortex

Four Primordial Follicles and two primary follicles

Mature follicle, Granular cells, marked by an arrow, produce estradiol.(diameter 4-5mm)The preovulatory folliclereaches a diameter of 15-25mm.

Corpus LuteumThe cells produce progesterone.

Degenerating Corpus luteum

Hilar cells of ovarian medulla,these cells are mainly responsiblefor androgen production.

Luteinized stromalcells
Stromal luteinization (stromal hyperthecosis) are associated withandrogenic or estrogenicmanifestation.

Normal Cycle of Endometrium Proliferative phase: Active growth of
glands, stroma and vessels influenced by estradiol production by granular cells in the follicles ( follicular phase).
Secretory phase: reflects the effect of the combined production of progesterone and estradiol by luteinized granulosa and theca cells of the corpus luteum (luteal phase).

PAROVARIAN/PARATUBAL (MESONEPHRIC) CYST
Common lesions, vary in size, often bilateral
Large cysts may become palpable, undergo torsion with/without infarction, and cause pelvic pain
They are benignmesonephric cysts: lined by cuboidal cells;usually arise in ovarian hilumparamesonephric cysts: lined by columnar tubal - type epithelium; adjacent to fallopian tube

FOLLICLE AND LUTEAL CYSTS OF OVARIESFunctional Cysts
Very commonOriginate in unruptured Graffian follicles or in
follicles which have ruptured and resealedOften multiple, they are located immediately
subjacent to the serosaLined by granulosa cells or by luteal cellsUsually small (1 - 1.5 cm), filled with clear fluidOccasionally larger, up to 5cm, and may then be
palpableOccasionally rupture, causing pain and
intraperitoneal bleeding

FOLLICULAR CYST OF OVARY

CORPUS LUTEUM CYST OF OVARYCorpus luteum of pregnancy can be up to 20 cm.
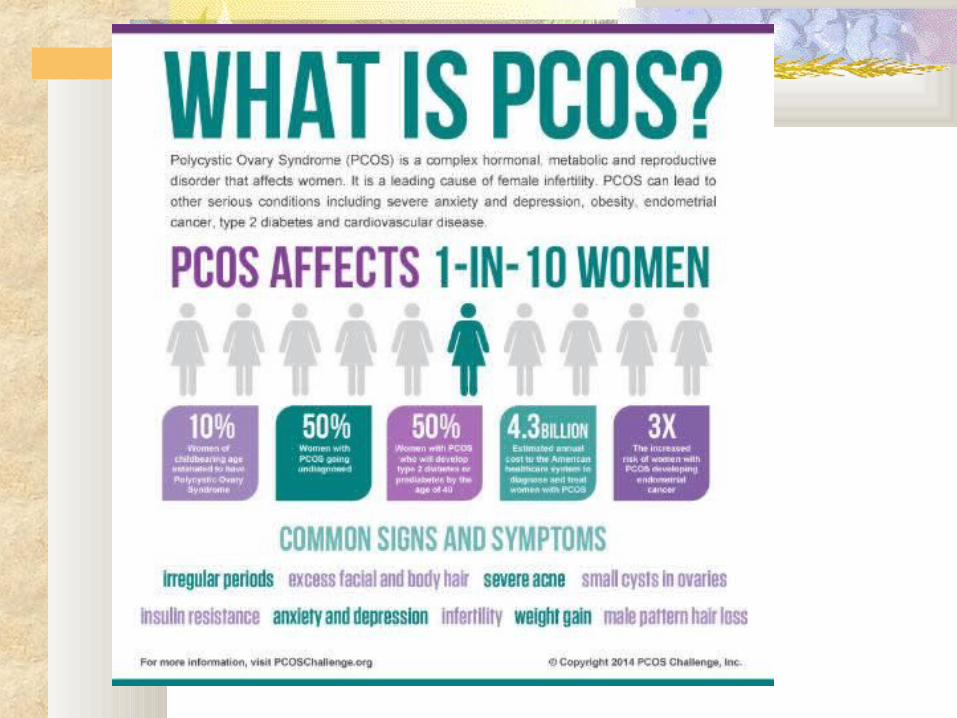



Polycystic Ovarian Disease

Ovarian Neoplasms Clinical Presentation
Despite their considerable pathologic diversity, the clinical presentation of ovarian neoplasms is similar:Usually asymptomatic until large enough to cause pressure symptoms (pain, GI complaints, urinary frequency)30% are discovered incidentally during routine GYN exams
Ovarian Neoplasms Clinical Presentationlarge masses may cause increased
abdominal girthOccasionally, the masses undergo torsion
severe abdominal pain and acute abdomen
Fibromas and malignant epithelial tumors can cause ascites
mucinous tumors can cause pseudomyxoma peritonei
tumors may cause endocrinopathies



Surface Coelomic Ovarian Neoplasm
SEROUS TUMORSMUCINOUS TUMORSENDOMETRIOID TUMORS - Most are
malignant; adenocarcinoma of endometrium present in 15-30% of cases
BRENNER TUMORS- Most are benign

Surface Coelomic Ovarian NeoplasmMost surface tumors present with
nonspecifically low abdominal pain and/or abdominal mass
Malignant tumors grow through capsule and widely seed the peritoneal cavity with tumor nodules and ascites; also distant metastases

Surface Epithelial TumorsThey are derived from coelomic
epithelium.They can be strictly epithelial, e.g.
serous, mucinous or endometroid.They can also have a distinct stromal
component, cystadenofibroma or Brenner tumor.
They are traditionally divided into benign, low malignant potential or malignant.

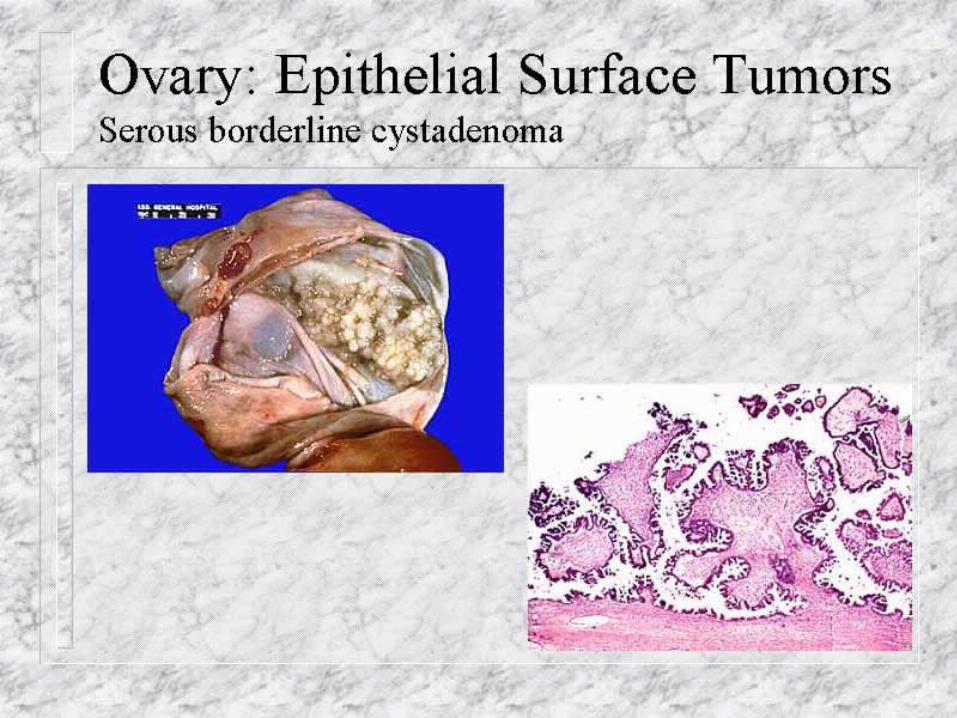
Serous Tumors60% Benign, 15% borderline (LMP),
and 25% malignant.Size ranges from 5-40cm.Unilocular or multilocular containing
clear serous fluid.Benign forms show smooth glistening
surface.The surface of the malignant forms
appears multinodular.

Serous Tumors of the Ovary
Single most common group of ovarian tumorsbenign and borderline: ages 20 - 50 yearsmalignant: ages 40 - 60+ years
Usually at least partially if not entirely cystic:“cystadenomas; cystadenocarcinomas”

Serous Tumors of the Ovary
Behavior depends on degree of differentiation and distribution
May occur on the ovarian surface, occasionally arises from peritoneal
surface






Serous Tumor of Low Malignant potential

Serous Tumor of Low Malignant Potential Papillary Tufting No evidence of
stromal invasion

Borderline Vs. Malignant Serous Tumors
Both may penetrate (or arise from) the ovarian surface, shedding cells which implant on peritoneal surfaces and produce ascites
Only malignant serous tumors invade the ovarian stroma and metastasize to lymph nodes or other sites
If confined to ovary, survival at 5 years: Borderline - 100% ;
Malignant - 70%

Serous Cystadenocarcinoma of OvaryThese tumor show stromal invasion
Cause elevated CA125 in serum

Serous Cystadenocarcinoma Involving both Ovaries


Mucinous tumors
Benign tumors usually occur between 3rd. And 5th. Decade of life
Most common tumor seen during pregnancy
most often associated with acute abdomen due to torsion

Mucinous Tumors of Ovary10% BENIGN - only 5% bilateral10% BORDERLINE10% MALIGNANT - only 20% BILATERAL
Note that Mucinous tumors are much less likely to be bilateral and to be malignant than serous tumors!
Often larger and more likely multiloculated than Serous tumors; lack psammoma bodies
have endocervix-like or intestine-like lining cells

Mucinous tumors
Benign
Low malignant potential
Malignant

Mucinous Tumors of the Ovary
5% of cases are complicated by pseudomyxoma peritonei:
peritoneal cavity becomes filled with gelatinous mucinous fluid (similar to cyst contents), which mats together the abdominal viscera.
Rx is surgical, and repeated operations are sometimes required


Benign Mucinous Tumor of Ovary


Mucinous tumor of low malignant potential10-15% of all mucinous tumors
6-8% of intestinal subtype are bilateral, Vs. 40% of endocervical type
100% long term survival in patients with stage I mucinous tumor of LMP ( no malignant potential)

Mucinous tumor of low malignant potential
10-15% of all mucinous tumors
6-8% of intestinal subtype are bilateral, Vs. 40% of endocervical type
100% long term survival in patients with stage I mucinous tumor of LMP ( no malignant potential)


Mucinous tumor of low malignant potential

Mucinous Carcinoma
Destructive stromal invasion, resemble mucin secreting adenocarcinoma of intestinal tract
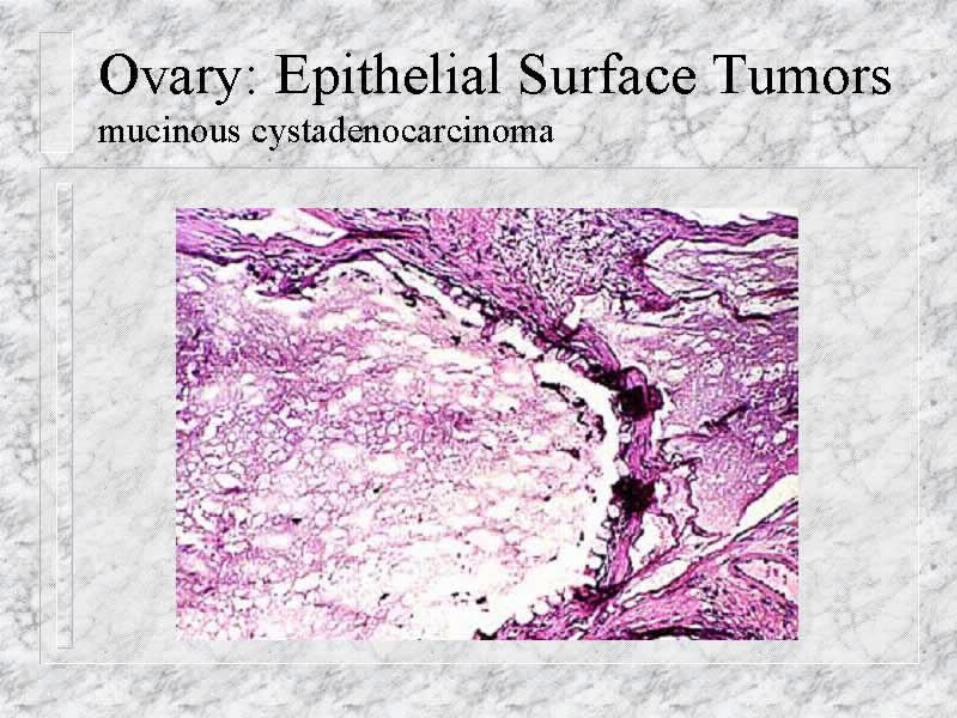

Mucinous Carcinoma
Endometroid tumorsBenign, unilateral masses, occurring in
older patient>57 Y/OEndometroid tumor of low malignant
potential, rare, defining criteria are not well established
Endometroid carcinoma, second most common of ovarian epithelial malignancy


Endometroid adenocarcinoma
Occur in 5th. and 6th. DecadeAbout 15-25% are associated with similar
lesion in the endometriumCan arise from endometriotic cyst, usually in
younger womenSynchronous or metachronous endometroid
adenocarcinoma of cervix has been reportedPrimary extraovarian site has been reported

Clear cell tumorBenign, rareLow malignant potential, rareMalignant can arise from areas of endometriosis, have
been seen in association with endometroid adenocarcinoma, both in ovary and endometrium. They can also be associated with hypercalcemia

Clear cell carcinomaThese tumors have the highest association
with pelvic endometriosis and Para endocrine hypercalcemia.


Brenner TumorOver 95% are diagnosed between the ages of
30-70.
Are usually unilateral and benign.

Fibroma Any age Unilateral Solid grey Most hormonally inactive Can produce hydrothorax and ascites
(Meigs Syndrome) Rarely malignant

Ovarian Fibroma


Thecoma
Any age Unilateral Yellow Can elaborate estrogen resulting in excess
endogenous estrogen Can also elaborate androgen resulting in
hirsutism



Sertoli Leydig Cell Tumor All ages Unilateral, usually small Gray to yellow brown Composed of tubuli or cords and plump
pink leydig cells Most are androgenic Small percentage are malignant

Leydig Cell TumorThese tumors are usually
yellow in color, high lipid content.
Uniform cell population, presence of crystals of Reinke are diagnostic.


Granulosa cell tumorAny age, two different type, adult form and
juvenile formUnilateralMost elaborate large amount of estrogen5-25% are malignant, adult form onlyComposed of mixture of cuboidal Granulosa
cells in cords, sheets, or strands with spindled or plump lipid laden theca cells

Granulosa cell tumorNote presence of Call Exner Bodies


Granulosa cell tumorDiffuse pattern

Germ Cell Tumors Dysgerminoma can occurs with gonadal
dysgenesis Mature teratoma (dermoid cyst) Immature teratoma Choriocarcinoma Endodermal sinus tumor (yolk sac tumor)

Dysgerminoma Peak incidence: 2nd and 3rd decade. 80-90% unilateral Gross: Solid small or large gray mass Micro: Sheets and cords of large cleared
cells separated by scant fibrous strands. Stroma contains lymphocytes.
Prognosis: malignant, but only 1/3 aggressive and spread; all radiosensitive with 80% cure

DysgerminomaAre occasionally encountered in phenotypic
females with gonadal dysgenesis.


Teratoma of the Ovary
BENIGN (MATURE) CYSTIC TERATOMAHistologically mature
IMMATURE MALIGNANT TERATOMAAverage age 18 yearsMost are predominantly solidFoci of immaturity, usually of neuroepithelial typeAggressive, metastasize widely
SPECIALIZED TERATOMASStruma ovarii: mature thyroid tissue; may cause
hyperthyroidismCarcinoid: may cause carcinoid syndrome

Mature (benign) Cystic Teratoma (“DERMOID CYST”) Unilocular cyst, bilateral in 10% of cases Lined by epidermis with all adnexal structures bone, cartilage, thyroid, and other organoid
formations including tooth anlage, bronchi, gut, brain, eye, etc. often present
Rarely exceed 10 cm diameter Young women (late teens, 20’s); present most often
as asymptomatic ovarian masses on PE or X-ray 10-15% undergo torsion, present as acute abdomen Karyotype of benign cystic teratoma always 46,XX Malignant transformation in 1%, squamous cell ca.


Mature Teratoma


Immature TeratomaUsually cause large solid
or partially cystic masses.
Show immature neural elements consisting of neuroepithelial tubules

Specialized TeratomaStruma ovarii can cause hyperthyroidism.

Endodermal Sinus TumorYolk Sac Tumor
Predominantly in young patients Large partially cystic ovarian mass Aggressive behavior, survival rate for
stage I tumors are 70-90% and 30-50% for higher stage tumors.

Endodermal Sinus tumorSerum AFP (alfa fetoprotein) is elevated in
almost all patients.
commonly show Shiller Duval Bodies.


Metastases to Ovary
Older women
Usually bilateral
Tumors can be up to 20 cm
Common primary sites include breast, lung, gastrointestinal tract

Krukenberg Tumor
Other tumors of the ovary Embroyonal carcinomas
Mixed germ cell tumors
Gonadoblastoma

FEMALE GENITAL SYSTEM
PLACENTA

Gestational Trophoblastic Disease Hydatidiform mole, complete and partial Invasive mole Choriocarcinoma Persistent trophoblastic Disease”
All elaborate human chorionic gonadotropin HCG, which can be detected in the blood and the urine.

Hydatidiform MoleIs a voluminous mass of swollen , sometimes
cystically dilated, chorionic villi, appearing grossly as grape like structures.
The swollen villi are covered by varying amount of banal to highly atypical chorionic epithelium.

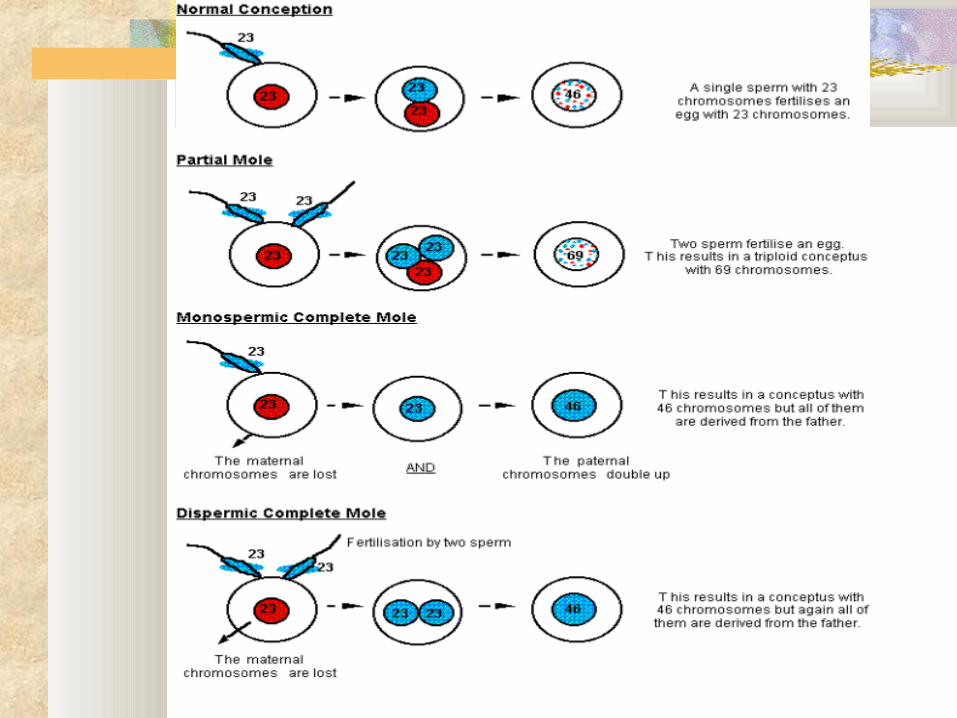

Complete Hydatidiform mole All of the chorionic villi are abnormal Chorionic epithelial cells are diploid, 46 XX or
uncommonly 46XY. An empty egg is fertilized by two spermatozoa. Incidence is 1-1.5/ 2000 pregnancies in US, higher
incidence in Asian countries. More common before age of 20 and after age of
40.

Complete hydatidiform mole The condition is usually discovered in 4th month
of gestation. Ultrasound studies show a diagnostic pattern
which resembles snowflakes. Fetal heart tone is usually absent.
The uterine cavity is filled with a delicate friable mass of thin-walled translucent cystic structures.
Striking proliferation of cytotrophoblasts and syncytiotrophoblasts present.
Markedly elevated serum HCG 2% progress to choriocarcinoma


Partial hydatidiform mole Is developed as the result of fertilization of
a normal egg by two spermatozoa. Is always triploid (69XXY). Villous edema is only seen in some villi. Trophoblastic proliferation is focal. Serum HCG level is less elevated. Rarely progresses to choriocarcinoma.

MOLAR PREGNANCY
Curettage produced this specimen, which consisted of 300 cc of bloody tissue.

GESTATIONAL TROPHOBLASTIC DISEASE:HYDATIDIFORM MOLE, COMPLETE TYPE
Swollen, avascular villi covered by chorionic epithelium (trophoblast) of varying atypia
Gross appearance is that of a voluminous mass of grape like structures

GESTATIONAL TROPHOBLASTIC DISEASE: COMPLETE VERSUS PARTIAL HYDATIDIFORM MOLE
FEATURE COMPLETE PARTIAL
Karyotype 46, XX (rare XY) 69, XXY
Villous edema all villi some villi
Trophoblast Pro- diffuse; circum- partial liferation ferential
Atypia often absent
serum HCG elevated less elevated
HCG in tissue ++++ +
Behavior 2% get chorio- rare chorio-
carcinoma carcinoma

GESTATIONAL TROPHOBLASTIC DISEASE:PARTIAL HYDATIDIFORM MOLE
A fetus or fetal parts may also be present
Some villi are normal
Almost always triploid
Normal egg + two spermatozoa 69,XXY
Rarely becomes malignant

Invasive Hydatidiform Mole An invasive mole retains hydropic villi, which
penetrate the uterine wall. Can cause uterine rupture and can be life
threatening. Hydropic villi may embolize to distant organs,
but this tumor does not have metastatic potential. Cure is possible by hysterectomy or
chemotherapy.

Choriocarcinoma Is very aggressive malignant tumor arises
either from gestational chorionic epithelium or less frequently, from totipotential cells within gonads or elsewhere.
Incidence is 1/ 30,000 pregnancies in US. More common in Asian and African
countries.

ChoriocarcinomaIncidence In US 1/30,000 pregnancies
50% follow complete molar pregnancy, 25% following abortion, remainder following normal pregnancy
In Asia and Africa can be as high as 1/2,000 pregnancies

Choriocarcinoma Most cases are discovered by the appearance of a
bloody, brownish discharge, accompanied by a rising titer of HCG, particularly the beta subunit.
Usually appear as very hemorrhagic, necrotic masses within the uterus.
The tumor is entirely composed of cytotrophoblasts and syncytiotrophoblasts.
Widespread dissemination via blood, lung (50%), vagina (30-40%), brain, liver and kidney.

Choriocarcinoma
Chemotherapy results in almost 100% cure or remission in all patients except some who have high risk metastatic trophoblastic disease.
Many of the cured patients have subsequent normal pregnancies.
By contrast, non-gestational choriocarcinoma are much more resistant to therapy.
Drug of choice is methotrexate.

GESTATIONAL TROPHOBLASTIC DISEASE: CHORIOCARCINOMA

CHORIOCARCINOMA

Placental Site Trophoblastic Tumor

Placental Site Trophoblastic Tumor
PLACENTA ACCRETA DEFINITION: Partial or complete absence of the decidua,
with adherence of the placental villi directly to the myometrium:
placenta increta - extends part way thru myometrium
placenta percreta - extends thru entire wall of uterus CLINICAL IMPORTANCE:
1. 60% of cases associated with placenta previa, in which implantation is in lower uterine segment or cervix ante partum bleeding; many cases occur in C-section scars
2. Postpartum bleeding, often life threatening, due to failure of placental separation

PLACENTA ACCRETA

PLACENTA ACCRETA, PERCRETA TYPE, WITH UTERINE RUPTURE


















