Female Reproductive Female Reproductive Issues Following Issues Following Bariatric Surgery Bariatric Surgery Joseph R. Wax, M.D. Professor of Obstetrics and Gynecology University of Vermont School of Medicine Maine Medical Center Portland, Maine
Transcript
Female Female Reproductive Issues Reproductive Issues Following Bariatric Following Bariatric
SurgerySurgery
Joseph R. Wax, M.D.Professor of Obstetrics and Gynecology
University of Vermont School of Medicine
Maine Medical CenterPortland, Maine
A Tale of Two A Tale of Two Patients… Patients… 1. 25 year old G0 12 months after
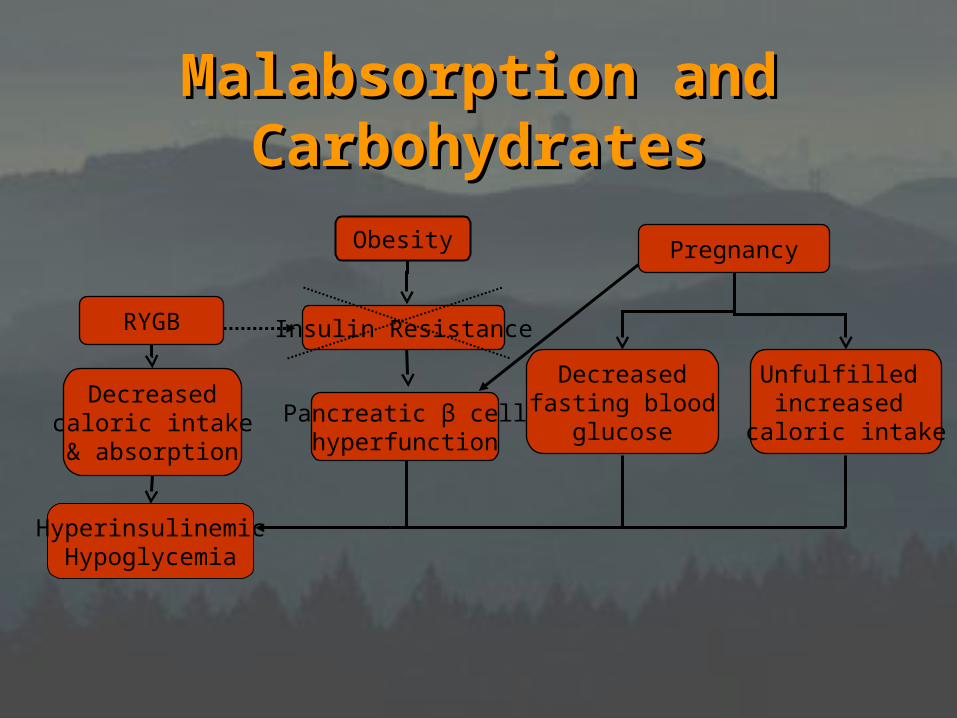
Hyperinsulinemic Hyperinsulinemic Hypoglycemia in Hypoglycemia in
PregnancyPregnancy• 36-year old at 24 weeks• RYGB 39 months earlier• Lightheadedness, syncope• Postprandial glucose 34-57 mg/dL• Normal glucose, no symptoms
– Acarbose (inhibits glucose absorption)• 25-50 mg after meals (TID)• S/E flatulence, diarrhea• category B
– Octreotide (somatostatin analog)• 25-100 mcgm SQ 15-60 min before meals• category B
Dumping Syndrome – Dumping Syndrome – Implications for Implications for
PregnancyPregnancy
• Avoid glucose challenge test– Home glucose monitoring
•1-2 weeks at 26-28 weeks•treat if consistently elevated
Pregnancy Outcomes Pregnancy Outcomes After Bariatric SurgeryAfter Bariatric Surgery
• Case reports and series• Case-control studies
– small– subjects as own controls– women without bariatric surgery as
controls• obese• non-obese
– unspecified bariatric surgical procedure
Pregnancy after LAGBPregnancy after LAGB
OutcomOutcomee
MartinMartin(n=23)(n=23)
WeissWeiss(n=7)(n=7)
Skull*Skull*(n=49)(n=49)
Dixon*Dixon*††(n=79)(n=79)
Years 1990-5 1996-2000 1996-2003 1995-2003
SAB 2 (9%) 2 (28.6%) - -
CS 4 (22%) 2 (40%) 0 -
BW 3676g - 0 0
Wt gain - - ↓ ↓
DM 0 (0) 0 (0) ↓ ↓
HTN 0 (0) 0 (0) ↓ ↓
Band 0 (0) 2 (28.6%) 2 (4.1%) 0 (0)* vs. last presurgical pregnancy* vs. last presurgical pregnancy† † vs. matched obese controlsvs. matched obese controls
Pregnancy After RYGB- Impact Pregnancy After RYGB- Impact of Timingof Timing
Outcome
Rand( 10 early, 8 late)
Dao(21 early, 13 late)
Wax(20 early, 32 late)
SAB - 0 -CS 0 0 0
BW - 0 0
Preterm
- 0 0
Wt gain - 0
DM - - 0
HTN - 0 0
Pregnancy After Pregnancy After LAGB/RYGBLAGB/RYGB
Compared to Pre-Surgical PregnancyCompared to Pre-Surgical Pregnancy
LessLess SimilarSimilar UnclearUnclear
Wt gain CS SAB
DM BW Growth restriction
HTN Preterm
BW ≥ 4kg
Bariatric Surgery and Bariatric Surgery and the Puerperiumthe Puerperium
• Weight loss– limited descriptive data– rate similar to nonbariatric delivered
patients and nonpregnant bariatric patients
Bariatric Surgery and Bariatric Surgery and LactationLactation
• Not contraindicated• Ensure maternal B12
supplementation– several cases of neonatal B12
deficiency
Grange, D.K. Pediatr Hematol Oncol 1994
Campbell, C.D. Haematologica 2005
SummarySummary
• Anatomic and physiologic changes associated with bariatric surgery have significant reproductive implications
• Nutritional deficiencies generally mild and easily treated
• Limited data suggest favorable pregnancy outcomes
Future ResearchFuture Research
• Pregnancy outcome– by specific bariatric procedure– account for
• past pregnancy complications• persistent obesity• obesity-related comorbidities
– congenital anomalies (ONTDs)
Guidelines for CareGuidelines for CarePreconception
Reliable contraception through period of maximal weight lossEvaluate and treat comorbiditiesEvaluate and treat micronutrient deficiencies (B12, folate, iron)Meet with bariatric surgeon and nutritionist, preconception consultation with Ob/Gyn or Maternal-Fetal MedicineFolic acid, B12 and iron supplementation
Pregnancy Folic acid, B12 and iron supplementationSecond trimester MSAFPConsider monthly growth ultrasounds after 20 weeksMonitor for signs and symptoms of hypoglycemiaAvoid NSAIDS if history of ulcer
Puerperium
Folic acid, B12 and iron supplementationBreast feeding compatible with bariatric surgeryNotify pediatrician of maternal surgical history to enable monitoring for micronutrient deficiency (likely very low risk if mother taking prescribed supplements) Avoid NSAIDS if history of ulcer