Fielded: April 2015 Research Executed by: Survey Monkey Questions provided by: David Bernstein Analysis provided by: David Bernstein The Fly A Kite Foundation: Insights Survey DIPG Medical Provider Perception & Practice Management Study APRIL 2015
Transcript
Fielded: April 2015Research Executed by: Survey MonkeyQuestions provided by: David BernsteinAnalysis provided by: David Bernstein
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception &
Practice Management Study
APRIL 2015
The Fly A Kite Foundation: Insights Survey
About the Fly A Kite FoundationThe Fly A Kite Foundation Inc. was founded in August 2014 as an IRS 501 (c)(3) non-profit charity by David and Deena Bernstein after the loss of their son Zachary. Zachary was an 11 year-old boy who was diagnosed with, and suffered from DIPG (Diffuse Intrinsic Pontine Glioma). DIPG is a type of brain tumor found in the Pons, the part of the brainstem near the lower back of the head near the top of the spinal cord. The Fly A Kite Foundation is dedicated to three main objectives:
Partners In ArtThe Fly A Kite Foundation provides custom art packages for children with pediatric brain cancers. These packages are intended to provide a creative and therapeutic outlet for children suffering from diminished motor function. We have partnered with Patricia Kearney, a Neuro-Occupational Therapist (Therapy Partner) who works for Transitions of Long Island (part of the North Shore-LIJ Health System), an outpatient rehabilitation center specializing in helping people recover from neurological injury or illness. Patricia designs these art packages based on the therapeutic needs of each child.
Partners In CareThe Fly A Kite Foundation seeks to provide parents of newly diagnosed patients with support and guidance as they try to define and navigate treatment plans. The members of The Fly A Kite Foundation are passionate third parties available to guide, organize, support, listen, identify treatment options, and help bridge communications between family and medical provider.
Partners In ResearchThe Fly A Kite Foundation, Inc. (FAKF) is an IRS 501 (C)(3) non-profit charity dedicated to educating, aiding and funding the search for a cure for brainstem glioma and other forms of pediatric brain cancer in the hopes of curing all cancers.The Foundation seeks to fund research investigating cures for pediatric brain cancers with a focus on Diffuse Intrinsic Pontine Glioma (DIPG). Our focus is to support translational and clinical research projects in those areas.
April 2015
DIPG Medical Provider Perception & Practice Management Study
DIPG Insights Survey: Purpose
The Fly A Kite Foundation conducted its April 2015, DIPG Insights Survey, “DIPG Medical Provider Perception & Practice Management Study” in an effort to better understand the ongoing commitment to treatment of DIPG from a medical provider perspective. With a steady number of DIPG cases across the United States and the complexity of the disease, the Fly A Kite Foundation sought to gather information about the medical practitioners, those working behind the scenes in the trenches, trying to find a cure. But finding a cure is not without its own set of challenges.
The survey was designed to uncover the challenges the medical community and clinicians face every day while trying to find a cure. This study has been designed to uncover the distractions, complications, challenges and concerns the medical community faces as they continue to move the medical treatment of DIPG forward.
The goal of the study was to provide a better understanding about the obstacles that arise when managing quality care while providing perspective to the families seeking the advice and treatment from these clinicians. We hope the findings are valuable and insightful and help bridge the gap between medical provider and patient.
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
DIPG Insights Survey: Methodology
The Fly A Kite Foundation reached out to 375 medical practitioners from nationally recognized pediatric cancer hospitals in the United States. The Survey was conducted via e-mail and personal notes to individual practitioners who have devoted their practice to the treatment and cure of DIPG and other solid brain tumors. Although this is not the only pediatric cancer associated with these clinicians, they are public figures, published, admired by their colleagues and considered to be some of the best minds in the world in the DIPG arena.
Titles range from Associate Professor, Pediatric Neurosurgery; Professor, Pediatric Neuro Oncology; Professor, Pediatric Neuro Oncologist; Professor, Pediatric Neurosurgery; Vice Chair of Pediatric Neurosurgery; Vice Chair for Research.
We asked a series of 21 questions with the goal of obtaining 20 completed surveys, or a 5% response rate. The survey was disseminated to a sample of approximately 375 medical professionals with a 95% confidence level that the sample reflects the targeted population. We also factored a 6% margin of error that the answers by the respondents were “true value” and represent the DIPG medical community accurately.
Although this sample and audience response size is very small, the findings are very valuable for both the clinical side and parental side of DIPG. This is a peek inside the minds of 17 top specialists in the world, sharing their anonymous thoughts, feedback, challenges and perceptions about their practice and treatment.
Note: Although the methodology and fielded study meets the guidelines of the Marketing Research Association, this study should only be used for informational purposes. The Fly A Kite Foundation makes no guarantees that the research is 100% accurate or has been reviewed by a 3rd party research organization or analyst. This study was performed on the grounds of making a case to commission a full-service research organization to field a much more complete and comprehensive study. The opinions expressed in the Executive Summary & Personal Observations page(s) are those of the Author, David Bernstein and only David Bernstein.
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception &
Practice Management Study
Survey Questions
DIPG Insights Survey: Questions
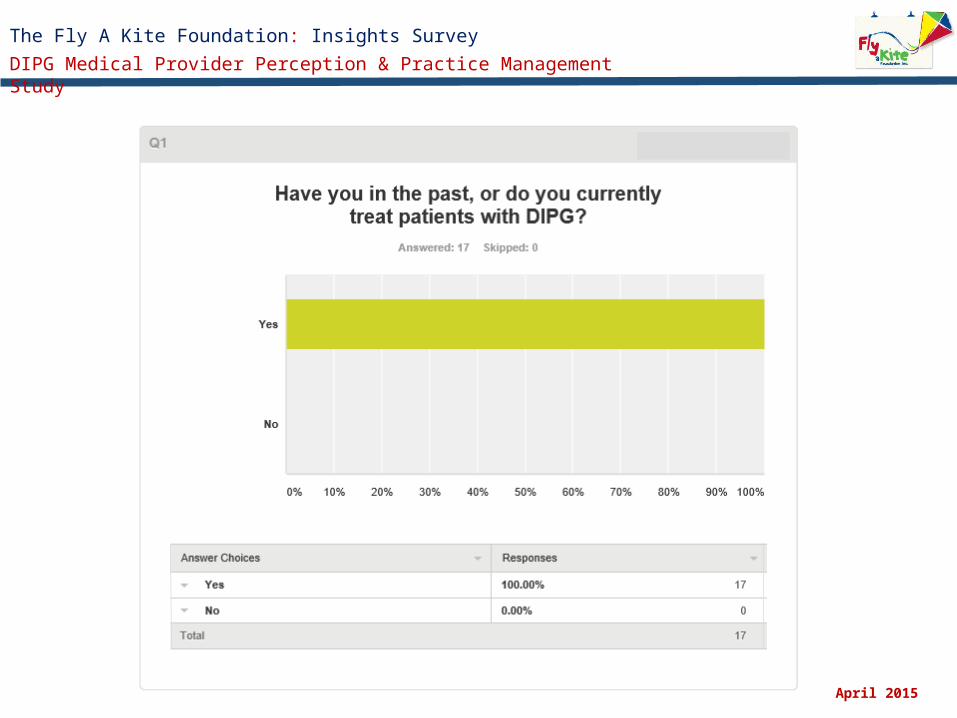
1. Have you in the past, or do you currently treat patients with DIPG?
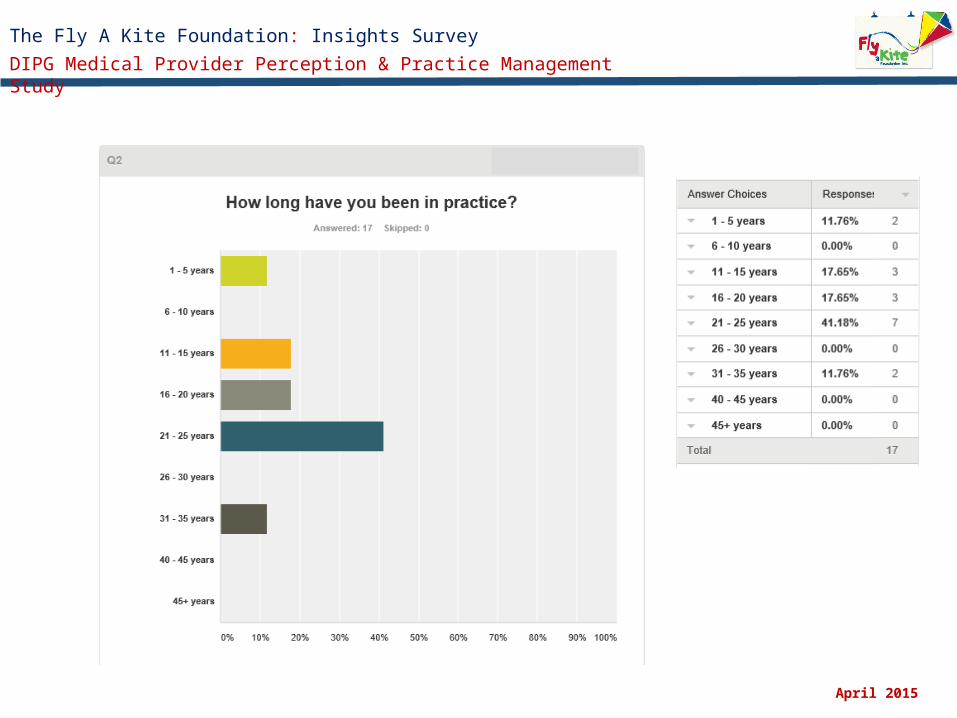
2. How long have you been in practice?
3. How long have you been treating patients with DIPG?
4. Please pick the title that best represents your current position.
5. Over the past 10 years, approximately how many DIPG cases have you personally treated?
6. What percentage (%) of your patients have you referred for a biopsy?
7. Select the challenges you face when providing care for your DIPG patient(s)?
8. On an annual average, how much of your time is devoted to raising funds for your research and trials?
9. On an annual average, how much of your time is devoted to learning about new treatments for your patients?
10. How do you keep up with the newest treatments and therapeutic innovations for DIPG?
11. Do you feel you are providing the best quality of care for your patients?
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
DIPG Insights Survey: Questions
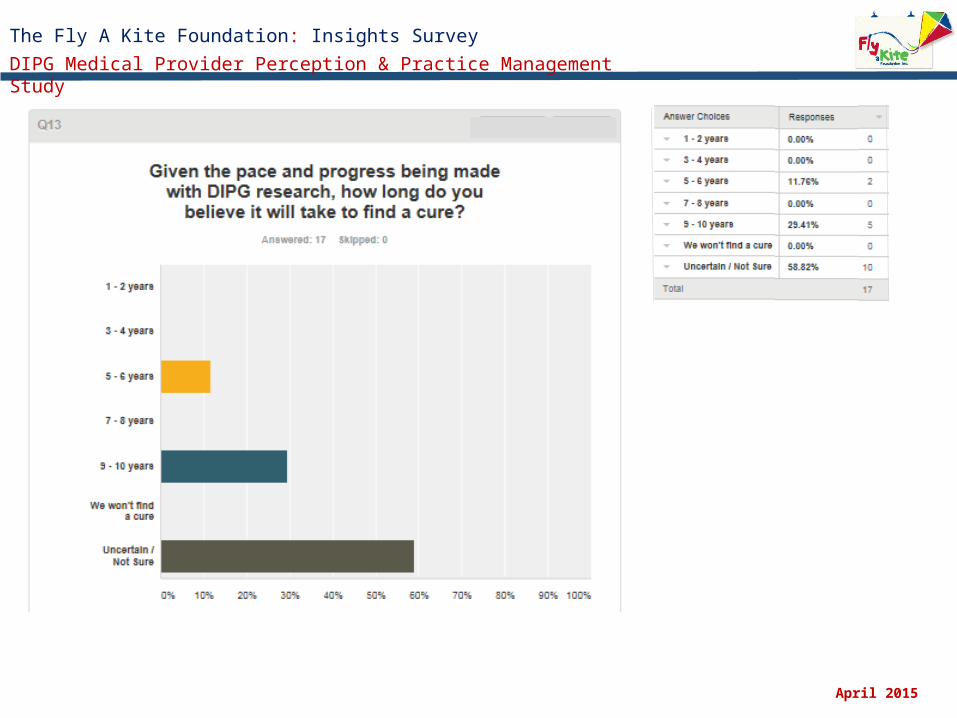
13. Given the pace and progress being made with DIPG research, how long do you believe it will take to find a cure?
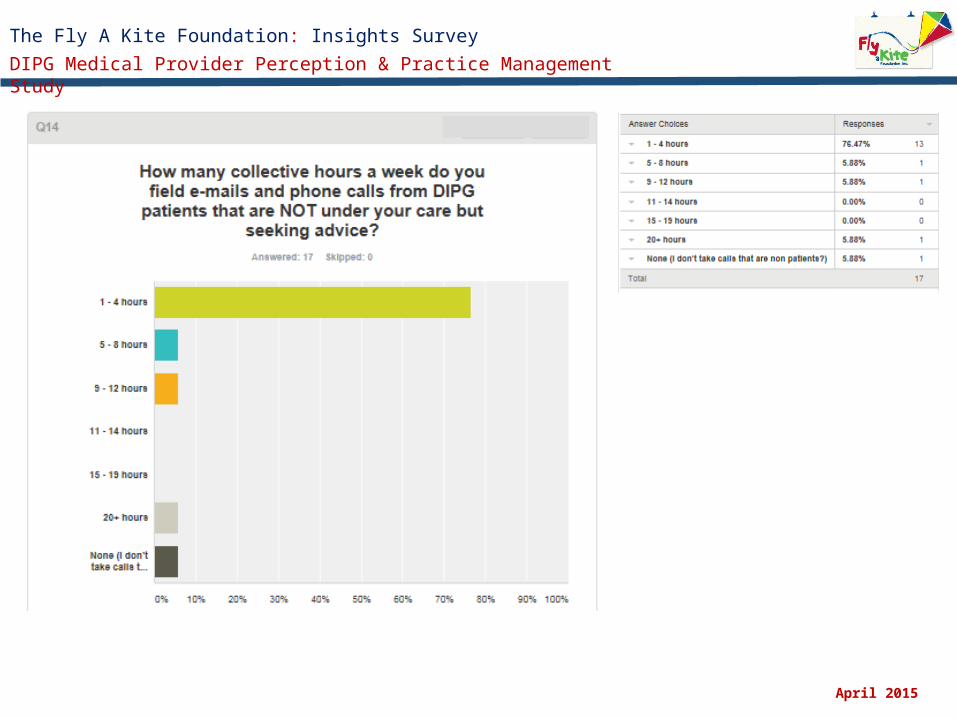
14. How many collective hours a week do you field e-mails and phone calls from DIPG patients that are NOT under your care but
seeking advice?
15. How many collective hours a week do you field e-mails and phone calls from DIPG patients that are under your care seeking
advice?
16. Do you think Personalized Medicine will be the future of DIPG treatment?
17. Understanding that all the DIPG cases are unique, in your opinion, what are the best practices or most novel in the way of
current treatment and care for DIPG patients?
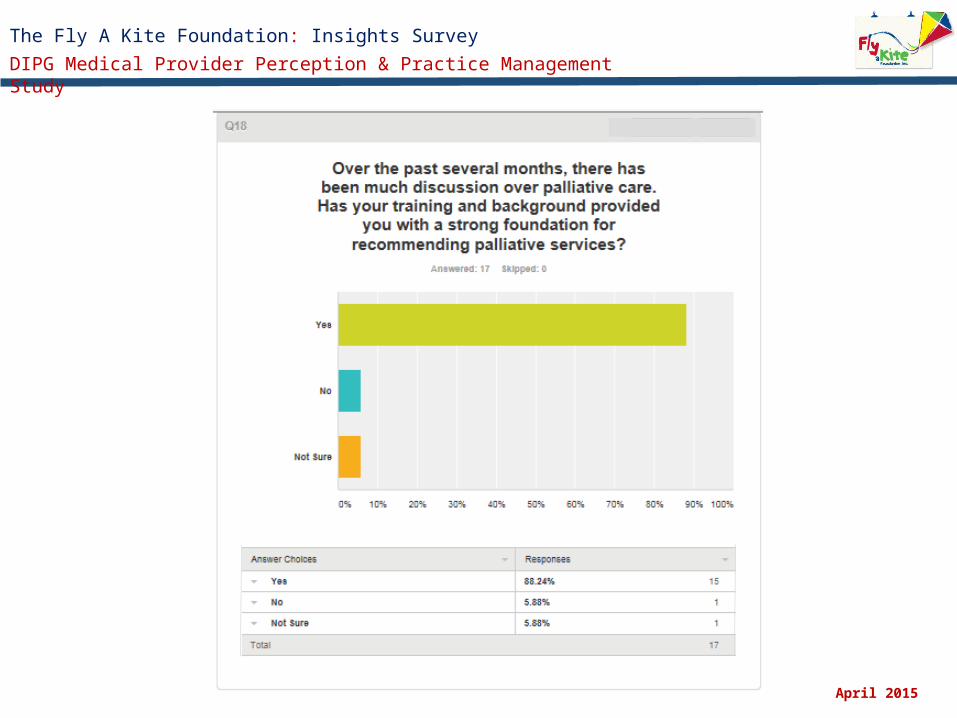
18. Over the past several months, there has been much discussion over palliative care. Has your training and background
provided you with a strong foundation for recommending palliative services?
19. Do you believe the medical community needs more training to properly discuss palliative care with families and patients?
20. With regard to DIPG Cases, What percentage of your time and conversations with families focus on palliative care?
21. We appreciate your valuable time and transparency when filling out this important survey, Our last question is designed to
elicit your feedback. Please feel free to elaborate on any of the following topics presented in this survey or offer up any
additional points that will help us better understand the needs of clinicians and their medical practices. (Open Comments)
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception &
Practice Management Study
Survey Responses
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
proceed with upfront biopsy in the united states
Histone inhibitors
Biopsy and molecular studies and banking.
I don't believe that there is a single most promising approach, but strongly encourage all of my families to participate in whatever seems to be the most important current clinical research trial available.
Offer of a biopsy, radiation for palliation, steroid sparing when possible, current clinical trial.
radiotherapy is best practice. Vaccine is most novel
the only established intervention is upfront XRT. Otherwise, there is no best practices approach otherwise.
There are no effective novel treatments identified; to date standard of care remains radiation alone
many novel things being tried but nothing successful yet.
Radiation plus experimental therapy
XRT is the only standard effective therapy. As I run the US upfront biopsy trial, we have made significant progress in the understanding of this disease. It will however take a while for these discoveries to impact care.
Small molecules as radio sensitizers. Immunotherapy- antibodies and engineered cells. Virotherapy.
Biopsy, molecular/genome testing, RT and hope for there to be a "hit" on the genomic data.
Q: Understanding that all the DIPG cases are unique, in your opinion, what are the best practices or most novel in the way of current treatment and care for DIPG patients? (Open Ended Comments)
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
Q21: We appreciate your valuable time and transparency when filling out this important survey, Our last question is designed to elicit your feedback. Please feel free to elaborate on any of the following topics presented in this survey or offer up any additional points that will help us better understand the needs of clinicians and their medical practices. (Open Comments)
education is needed for medical providers in discussions regarding limited autopsy tumor donation until we can standardize upfront biopsy in the united states.
I am very sorry to hear about Zachary's passing, and I want to thank you for creating this organization and working to help other children. It is a wonderful legacy for Zachary.
Keep going!
The biggest challenges are intrinsic to the tumor (e.g. lack of drugs that penetrate the tumor) rather than any external factor. More funding for clinical trials is needed but we need viable compounds to test. In my opinion, the barriers are not intrinsic to the provider but systemic.
Awareness and funding are critical to finding a cure. This is something that can and should be driven by parents/ families with support from the medical community.
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception &
Practice Management Study
Executive Summary
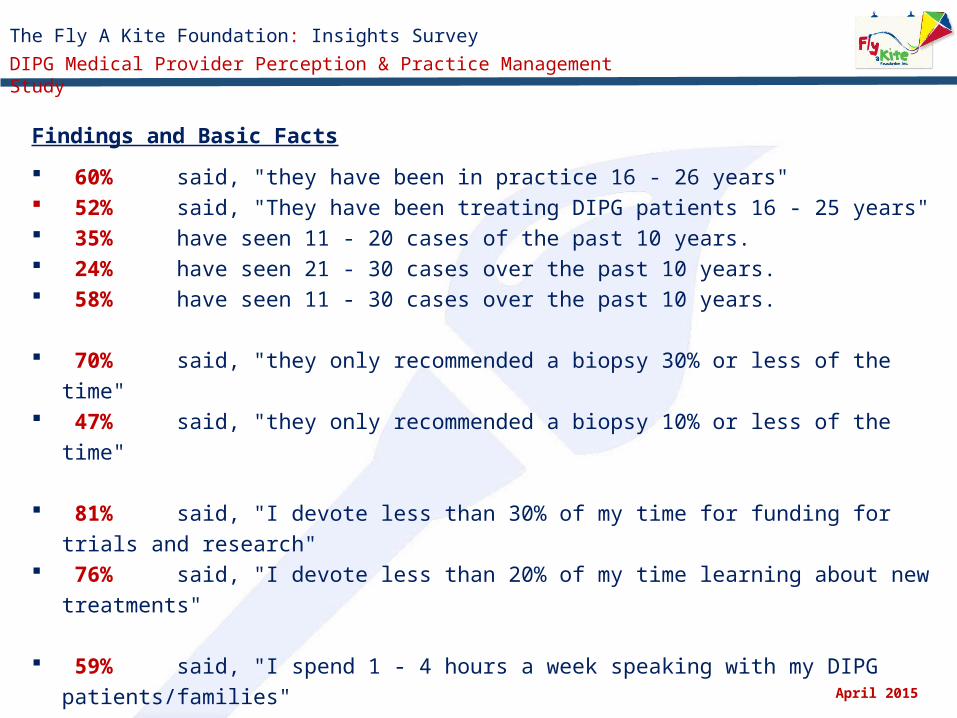
Findings and Basic Facts
60% said, "they have been in practice 16 - 26 years" 52% said, "They have been treating DIPG patients 16 - 25 years" 35% have seen 11 - 20 cases of the past 10 years. 24% have seen 21 - 30 cases over the past 10 years. 58% have seen 11 - 30 cases over the past 10 years.
70% said, "they only recommended a biopsy 30% or less of the time" 47% said, "they only recommended a biopsy 10% or less of the time"
81% said, "I devote less than 30% of my time for funding for trials and research"
76% said, "I devote less than 20% of my time learning about new treatments"
59% said, "I spend 1 - 4 hours a week speaking with my DIPG patients/families" 18% said, "I spend 5 - 8 hours a week speaking with my DIPG
patients/families" 18% said, "I don't spend any time during the week speaking with my DIPG
patients/families" April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
Challenges between Patient and Practitioner
14% said, "the communication between medical colleagues is fragmented"
14% said, "the communication between my patients is fragmented"
58% said, "There is lack of funding for my personal trials"
14% said, "I can't keep up with all the new research and data"
14% said, "There is a lack of information about the latest treatments."
Keeping up with new treatments and therapeutic innovations
41% said, "I read the trade journals"
100% said, "I read authored research and articles by colleagues"
47% said, "I go to www.clinicalTrials.gov"
100% said, "I attend conferences and seminars"
94% said, "I consult with my colleagues"
35% said, "I converse with patient parents
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
24% said, "Yes, I think personalized medicine is the future to cure DIPG"
6% said, "No, I don't think personalized medicine is the future to cure of
DIPG"
71% said, "I am not sure"
Cure for DIPG
12% said, "I think within 5 - 6 years we will see a cure"
30% said, "I think within 9 - 10 years we will see a cure"
58% said, "I am uncertain when there will be a cure"
Do you believe the medical community needs more training to properly discuss palliative care with families and patients?
81% said "Yes, more training is needed"
6% said "No, no more training is needed"
12% said, "Not sure"
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
DIPG Insights Survey: Executive Summary
After reviewing all the data, we hand selected a number of key practitioners who have been in practice for a combined average of 20 years. As shown in Question 1 , 76.48% have been in practice for 11 – 25 years, 41.18% have been practice from 21 – 25 years.
In Question 2, we asked, “How long have you been treating DIPG Patients?” The response is consistent with the answers in Question 1, over 70% have been treating patients for 11 – 25 years. In Question 5 we asked, “Over the past 10 year, approximately how many DIPG cases have you personally treated.” 41.17% said they treated 1 – 20 cases over the past 10 years and 58.82% said they treated approximately 11 – 30 cases.
It was interesting to learn that between 257 – 320 cases were treated by the clinicians who took this survey, 70.58% recommended a biopsy 30% or less of the time. As referenced in the DIPGRegistry.org,
It is not possible to treat DIPG by removing tumors surgically, but surgical biopsies to remove small amounts of tumor tissue for diagnostic testing are sometimes performed. Most diagnoses of DIPG are made from imaging scans such as MRI. Because of the risks of the procedure, surgical biopsy has usually only been performed when it has not been possible to confirm a diagnosis based on imaging. In the United States and Canada, most doctors do not generally recommend biopsy, and few patients undergo the procedure.
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
DIPG Insights Survey: Executive Summary
However, recent research has shown that advanced stereotactic surgical techniques greatly reduce the risks of surgical biopsy, which can sometimes yield useful diagnostic information and influence treatment decisions. Stereotactic surgical biopsy has now become a routine part of the diagnostic process at some European centers.
As researchers learn more about the genetics and biology of DIPG, they may discover that there are, in fact, important differences between different patients’ tumors. These differences could help physicians target future therapies to the right patients. In this case, surgical biopsy could become an important tool in treating the disease in the future.
Tumor tissue left over from surgical biopsy, as well as tumor tissue donated by families after children with DIPG have died, can be very helpful to researchers studying DIPG.
Up until 2012, biopsy's were under scrutiny for their surgical value and risks associated with the procedure. As technology and surgical skills progressed, so did the frequency with which medical professionals recommended biopsy for patients. Many patients and doctors as of late 2013 were using biopsy as a way to identify the tumor for certain mutations and apply customized treatment plans for patients. As Pediatric Neurosurgeons become more skilled with the technique and the risk to the patient decreased, the discussion of making biopsy a “Standard of Care” for all DIPG patients will be more common.
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
DIPG Insights Survey: Executive Summary
As outlined in Question 7, “Select the challenges you face when providing care for your patients”, over 57.14% said lack of funding for personal trials was the biggest challenge.
In Question 8 we asked, “On an annual average, how much of your time is devoted to learning about new treatments for your patients?” Over 47.06% said they spend anywhere between 11 – 20% and 76.47% said they spend 1 – 20% learning about new treatments.
In Question 9 we asked, “How do you keep up with the newest treatments and therapeutic innovations for DIPG?” Respondents indicated they read trade journals or authored pieces from colleagues, attend conferences or consult with their colleagues. It appears the medical community has challenges learning about new treatments but discussion among colleagues is the most direct route for information. It Is very apparent that collaboration among colleagues is necessary for the progression of information and treatment.
There is strong evidence that the DIPG community has gained insight into the biology of the DIPG cancer cell lines and what treatments may be used in the future. This includes, immunotherapies, customized medicine and advanced surgical procedures for drug delivery. In Question 13 we asked, “Given the pace and progress being made with DIPG research, how long do you believe it will take to find a cure?” Almost 60% were still uncertain / not sure, while 29.41% said 9 – 10 years and 11.76% said 5 – 6 years.
In Questions 14 and 15 we asked, “How many collective hours a week do you field e-mail and phone called from DIPG patients that are NOT under your care and that ARE under your care”. 74.47% of respondents said they spend 1 – 4 hours with patients who have DIPG that not under their care while 76.47% said they spend 8 hours or less with patients under their care.
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
proceed with upfront biopsy in the united states
Histone inhibitors
Biopsy and molecular studies and banking.
I don't believe that there is a single most promising approach, but strongly encourage all of my families to participate in whatever seems to be the most important current clinical research trial available.
Offer of a biopsy, radiation for palliation, steroid sparing when possible, current clinical trial.
radiotherapy is best practice. Vaccine is most novel
the only established intervention is upfront XRT. Otherwise, there is no best practices approach otherwise.
There are no effective novel treatments identified; to date standard of care remains radiation alone
many novel things being tried but nothing successful yet.
Radiation plus experimental therapy
XRT is the only standard effective therapy. As I run the US upfront biopsy trial, we have made significant progress in the understanding of this disease. It will however take a while for these discoveries to impact care.
Small molecules as radio sensitizers. Immunotherapy- antibodies and engineered cells. Virotherapy.
Biopsy, molecular/genome testing, RT and hope for there to be a "hit" on the genomic data.
Q17: Understanding that all the DIPG cases are unique, in your opinion, what are the best practices or most novel in the way of current treatment and care for DIPG patients? (Open Ended Verbatim Comments)
DIPG Insights Survey: Executive Summary
April 2015
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study
DIPG Insights Survey: Executive Summary
In Questions 18 and 19 we asked, “Over the past several months, there has been much discussion over palliative care. Has your training and background provided you with a strong foundation for recommending palliative services and do you believe the medical community needs to do more training to properly discuss palliative care with families and patients?” Over 88% said yes, they are trained in palliative discussion while over 81% said, they need more.
We also asked in Question 20, “What Percentage of your time and conversations focus on palliative care?” Anywhere between 10% - 80% of their time was equally distributed. Some practitioners spent 80% of their time with patients discussing palliative care while the same amount spent 10%. The spectrum of palliative conversation is fragmented. There is a movement among the American Cancer Society to encourage more training and personal interaction with medical practitioners and their patients on the direct discussion about palliative care. (Open Ended Verbatim Comments)
April 2015
In Question 21, we asked the respondents to elaborate on any of the following topics presented in this survey or offer up any additional points that will help us better understand the needs of clinicians and their medical practices.
education is needed for medical providers in discussions regarding limited autopsy tumor donation until we can standardize upfront biopsy in the united states.
The biggest challenges are intrinsic to the tumor (e.g. lack of drugs that penetrate the tumor) rather than any external factor. More funding for clinical trials is needed but we need viable compounds to test. In my opinion, the barriers are not intrinsic to the provider but systemic.
Awareness and funding are critical to finding a cure. This is something that can and should be driven by parents/ families with support from the medical community.
The Fly A Kite Foundation: Insights Survey
DIPG Medical Provider Perception & Practice Management Study