87
GASTRO INTESTINAL SYSTEM GASTRO INTESTINAL SYSTEM PART-1 PART-1 . .
| Date post: | 03-Jul-2015 |
| Category: |
Documents |
| Upload: | guruindia2012 |
| View: | 430 times |
| Download: | 2 times |
GASTRO INTESTINAL SYSTEM GASTRO INTESTINAL SYSTEM PART-1PART-1..

1. SALIVARY GLAND 1. SALIVARY GLAND TUMORSTUMORS
Uncommon - <2% of tumors
Parotid – 65 – 80% (15 – 30 % malig)
Submandibular – 10% ( 40% malig)
Minor salivary glands – rare 50% malignant in minor salivary glands
70 – 90% malig in sublingual glands
PLEOMORPHIC ADENOMAPLEOMORPHIC ADENOMA(MIXED PAROTID TUMOR)(MIXED PAROTID TUMOR)Benign60% - parotid30 – 50 yrs.M:F=1:3-4Derived from epithelial &
myoepithelial cells
Show epithelial & mesenchymal differentiation
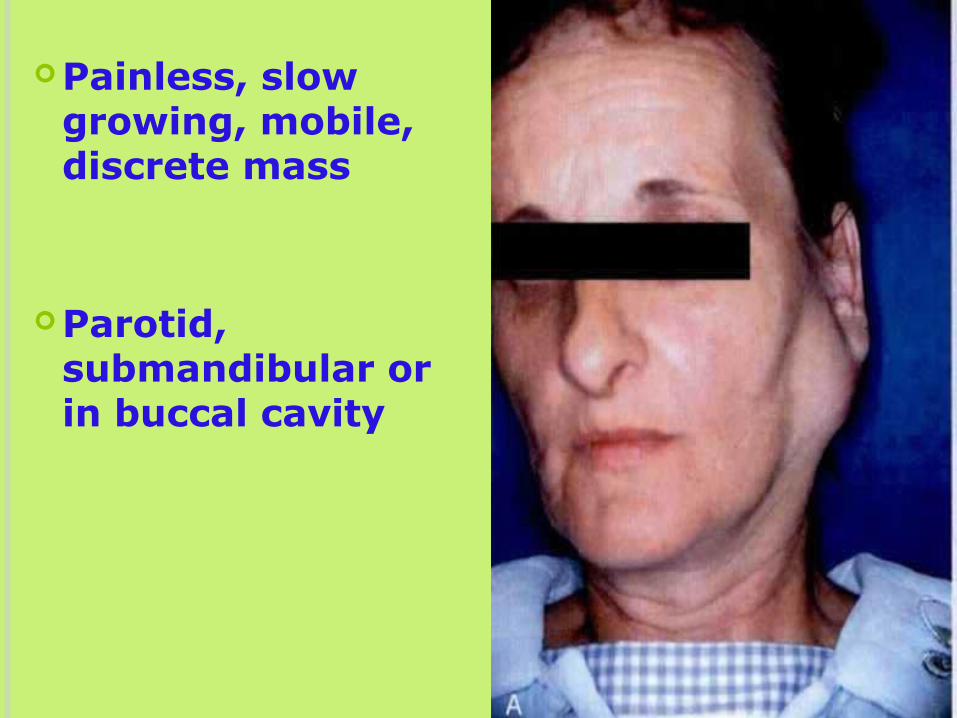
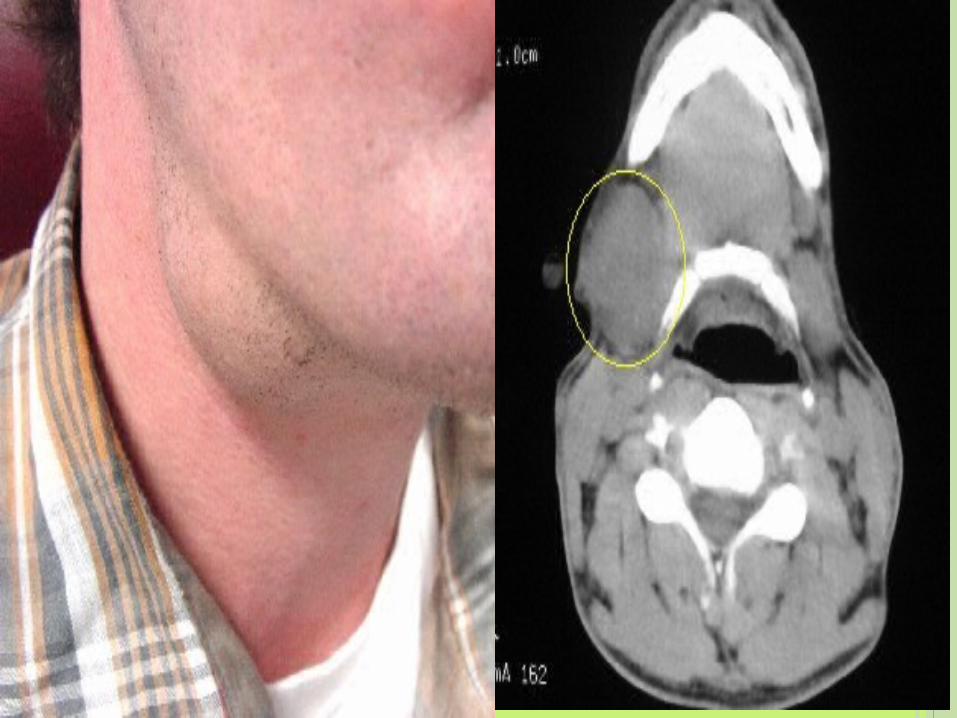
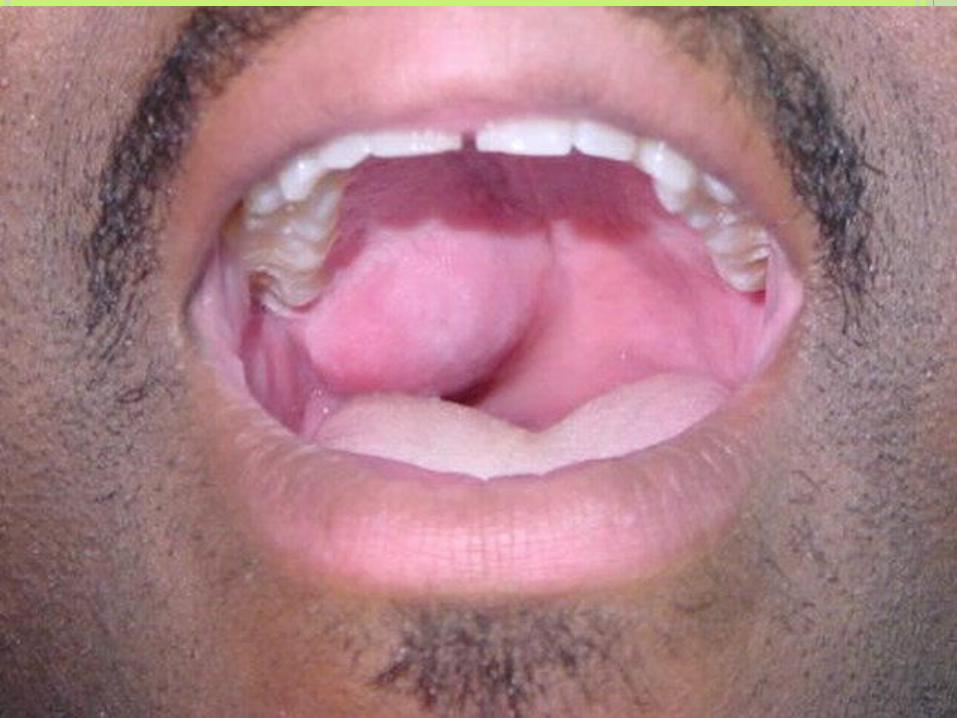
Painless, slow growing, mobile, discrete mass
Parotid, submandibular or in buccal cavity


GROSSGROSS
Round, well demarkatedEncapsulated, but capsule not
developed
Tongue like protrusions into surrounding gland
Enucleation hazardous
Recurrent tumor multifocal



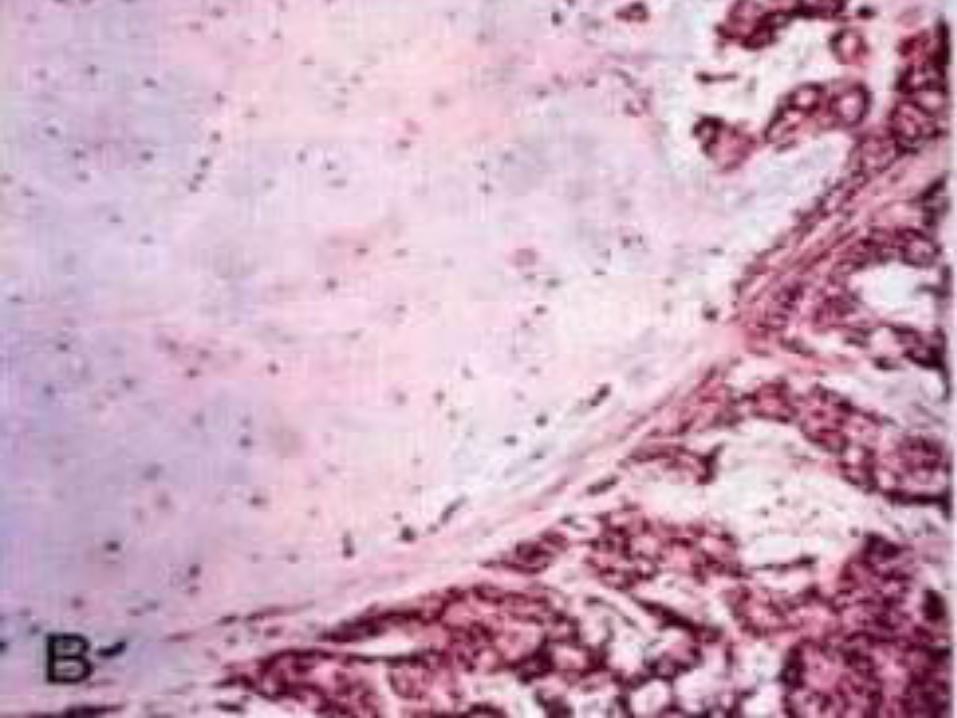
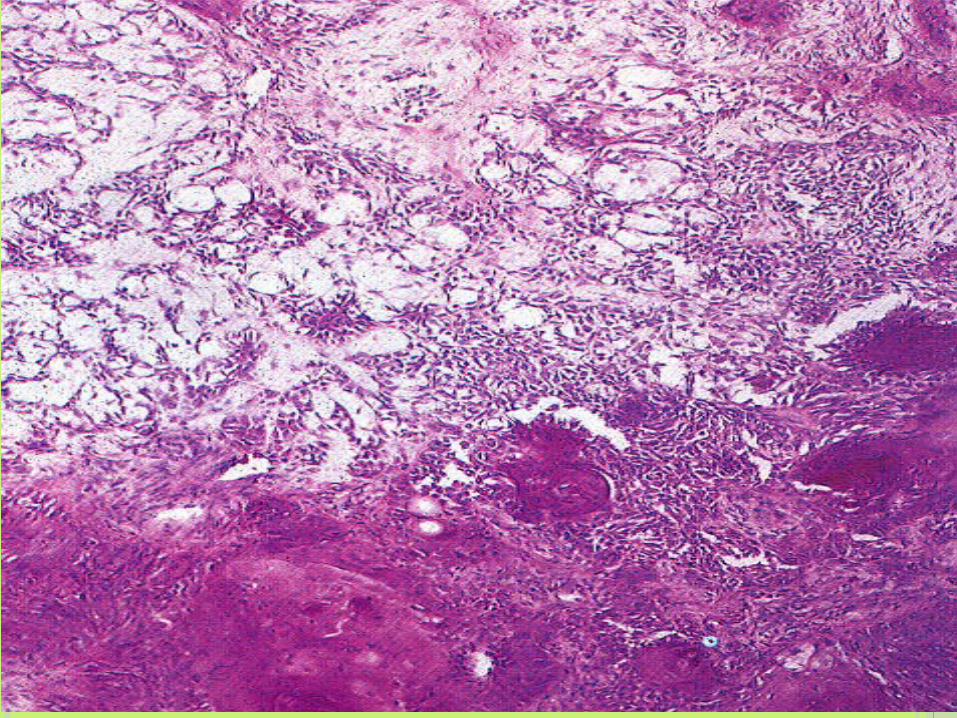
MICROSCOPYMICROSCOPYEpithelial elements
Ducts, acini, tubules, strands or sheetsDucts with cuboidal to columnar cells
with underlying deeply chromatic, small myoepithelial cells
OR Strands and sheets of Myoepithelial
cells Islands of squamous differentiation
Mesenchyme like backgroundLoose myxoid tissue with chondroid /
osteoid foci

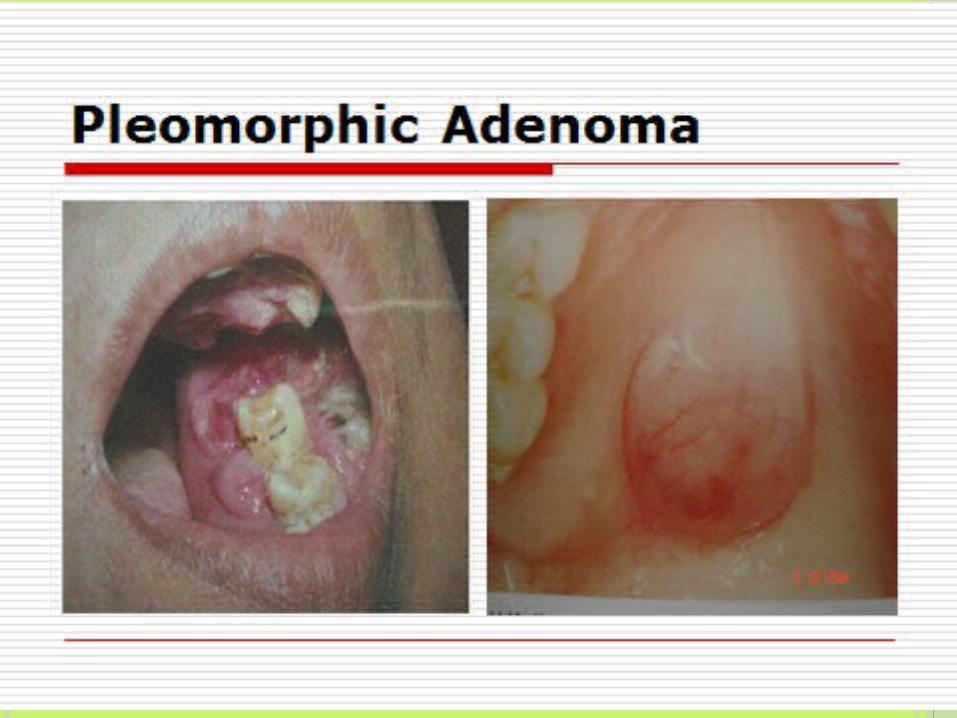
PLEOMORPHIC ADENOMA
Treatment: complete surgical excisionParotidectomy with facial nerve
preservationSubmandibular gland excisionWide local excision of minor
salivary gland
Avoid enucleation and tumor spill
Recurrence rate with parotidectomy 4%
Enucleation – 25%
Malignant mixed tumor / Ca ex pleomorphic adenoma2% for tumors < 5yrs10% for tumors > 15yrsAdenocarcinomas or undiff tumors Recognizable traces of the adenoma
MUST be found5yr mortality – 30 to 50%
WARTHIN’S TUMOR (WARTHIN’S TUMOR (AKA PAPILLARY CYSTADENOMA LYMPHOMATOSUM)
BenignParotid gland ONLYMale preponderance5th to 7th decade10% multifocal10% bilateral

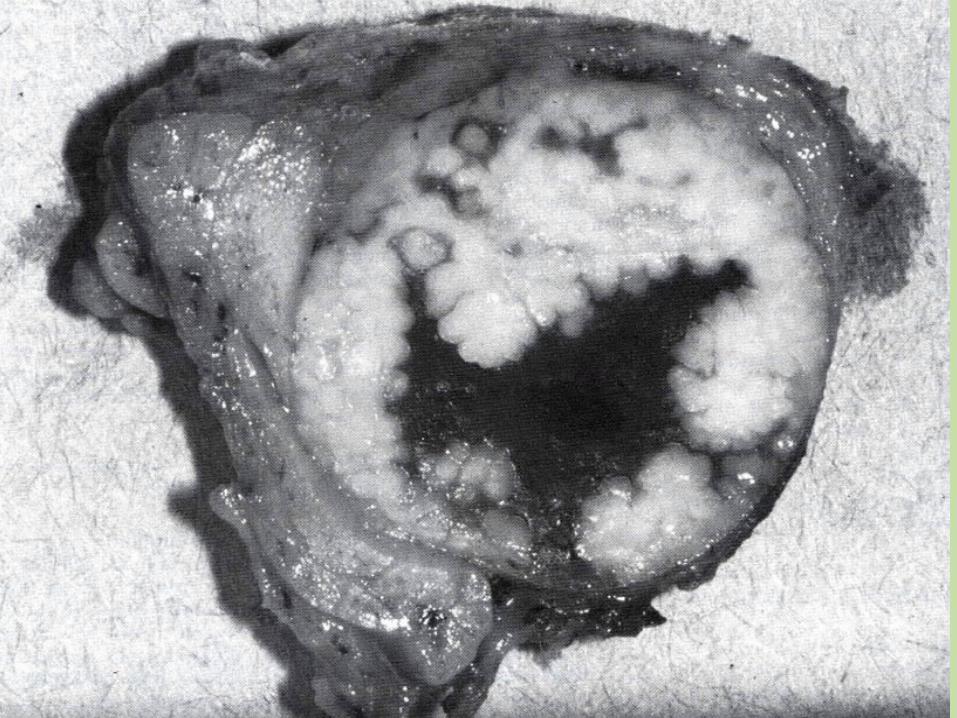
GROSSGROSSRound to oval
2 – 5 cm dia
Encapsulated
Arises in the superficial parotid gland
C/S – pale gray surface with narrow cystic or cleft like spaces filled with mucinous or serous secretion

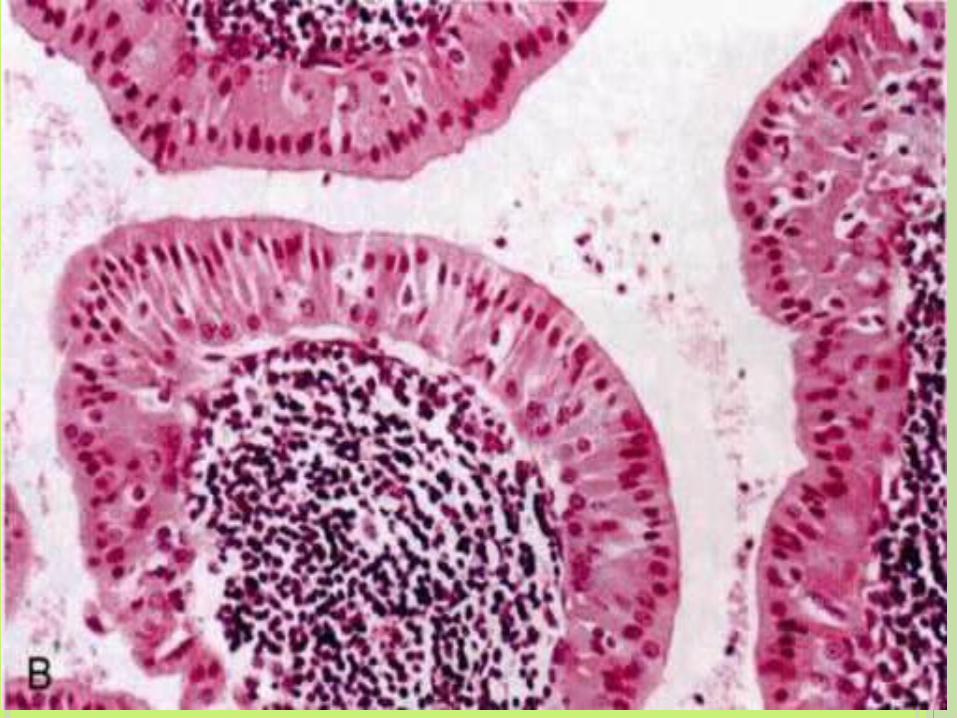
MICROSCOPYMICROSCOPYSpaces lined by double layer of neoplastic
epithelial cellsSurface palisade of columnar cells with
abundant, finely granular, eosinophilic cytoplasm – “oncocytic”
On a layer of cuboidal to polygonal cellsDispersed secretory cells in columnar
cell layerSquamous metaplasia
Dense lymphoid stroma ( GCs )
Recurrence rate 2% after resection
OTHER SALIVARY GLAND TUMORS
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Acinic cell carcinoma
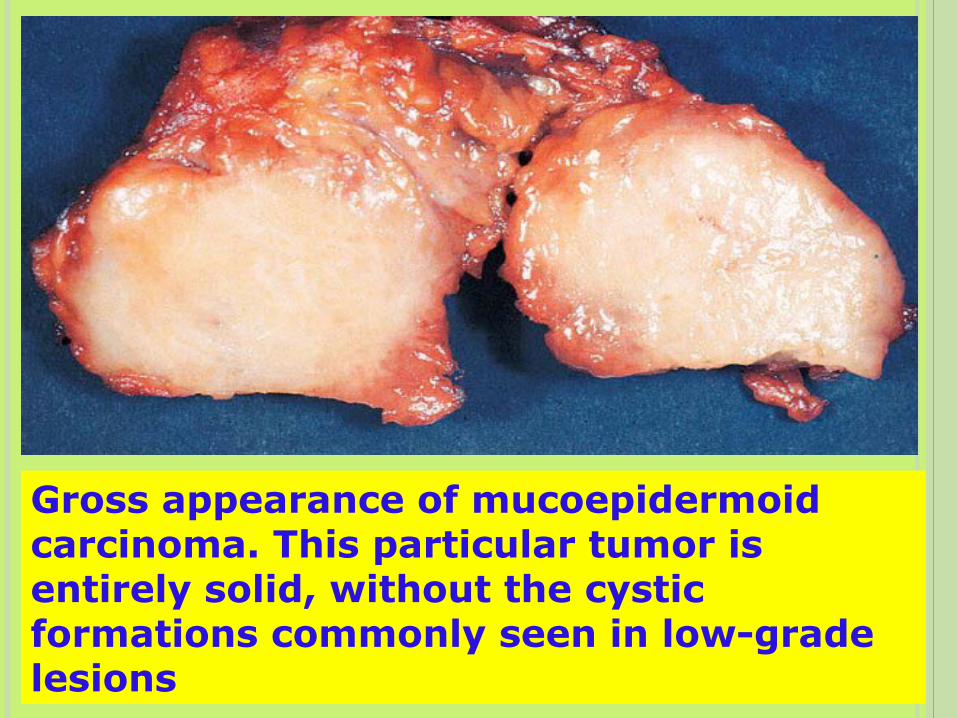
Gross appearance of mucoepidermoid carcinoma. This particular tumor is entirely solid, without the cystic formations commonly seen in low-grade lesions
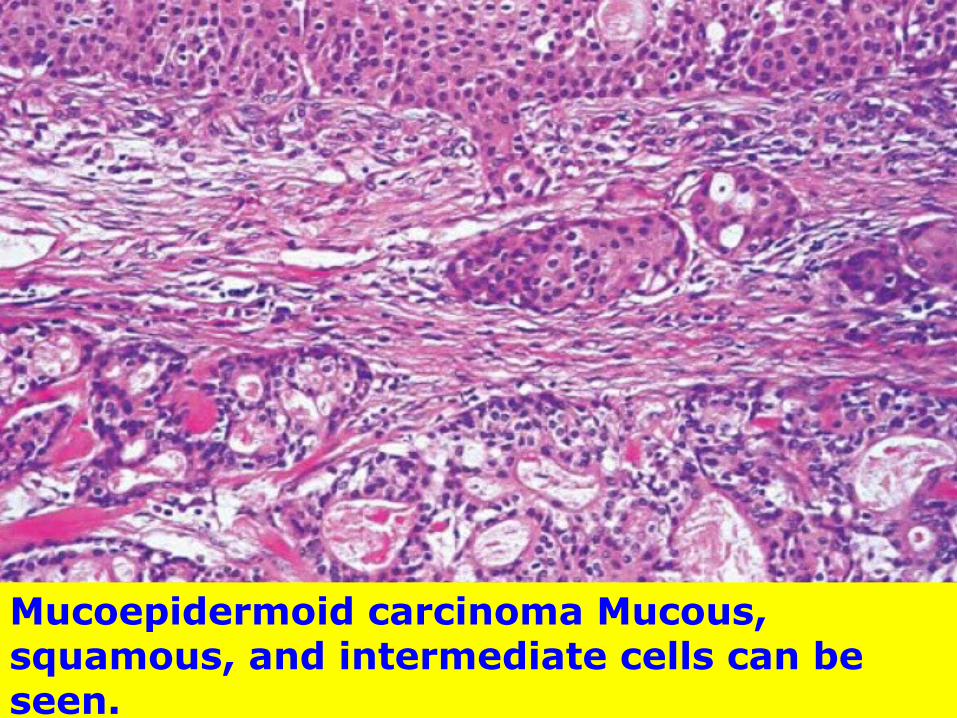
Mucoepidermoid carcinoma Mucous, squamous, and intermediate cells can be seen.

GASTROINTESTINAL TRACT

Oral cavity—Inflammatory diseases, precancerous lesions, Carcinoma
Salivary gland tumors
INFLAMMATORY LESIONS OF ORAL CAVITY
Stomatitis Aphthous ulcers [canker sores]—Painful oral
ulcers of unknown etiology ,Precipitated by emotional stress, Allergy, hormonal imbalence,Nutritional deficiencies and truma
Herpetic stomatitis --Herpes simplex virus
Cancrum oris or noma [Necrotising stomatitis ]—Necrosis of gingiva oral mucosa may lead to gangrene of cheek -- Feature of Kwashiorkor,measels, immunodeficiency states and stress
Mycotic infections –Actinomycosis and Candidiasis [ oral thrush]

ORAL CAVITY
Precancerous lesions LeukoplakiaErythroplakia
Carcinoma

LEUKOPLAKIA
White patch or plaque that cannot be scraped off and cannot be characterized clinically or pathologically as any other disease
Incidence – 3%, 5 – 25% of these are premalignant
Age – 40 -50 yrs.M:F = 2:1DD – Lichen planus, candidiasis
1. Homogeneous leukoplakia – lesion that was uniformly white and unscrapable.
2. Non Homogeneous leukoplakia – lesion predominantly white and speckled with red.
WHO CLASSIFICATIONS (1980)
1. Thin, smooth leukoplakia (preleukoplakia older terminology) – translucent thin gray soft flat plaques usually with sharply demarcated borders.
2. Thick, fissured leukoplakia – 2/3 of white plaques has distinctly white appearance (from thickening of keratin layer), fissured and are leathery to palpation.
3. Granular, verruciform leukoplakia – lesions have surface irregularities of nodular or granular nature with verrucous appearance.
4. Erythroleukoplakia – lesion showing intermixed red and white areas, because the epithelial cells are so immature that they no longer are able to produce keratin.
WHO CLASSIFICATIONS (1998)
In 2002 WHO reclassified the above variants depending on the probability of a malignant change and prognosis of these lesions as
1. Phase I: thin, smooth leukoplakia – better prognosis.
2. Phase II: thick, fissured leukoplakia. 3. Phase III: proliferative verrucous
leukoplakia (PVL) – higher malignant transformation rate.
4. Phase IV: erythroleukoplakia – poor prognosis.
WHO CLASSIFICATIONS (2002)
Leukoplakia is purely a clinical terminology and histopathologically it is reported as epithelial dysplasia.
WHO in 2005 proposed five grades of epithelial dysplasia based on architectural disturbances and cytological atypia.
HISTOPATHOLOGY

1. Squamous Hyperplasia – benign lesion.
2. Mild Dysplasia – better prognosis.
3. Moderate Dysplasia.
4. Severe Dysplasia.
5. Carcinoma In-situ – poor prognosis.
It has been recently proposed to modify the above 5-tier system into a binary system of ‘high risk’ and ‘low risk’ lesions to improve clinical management of these lesions.
Locations
Buccal mucosa Floor of the mouth Ventral surface of tongue Palate Gingiva

SMOOTH, THIN, WELL DEMARCATED

DIFFUSE & THICK
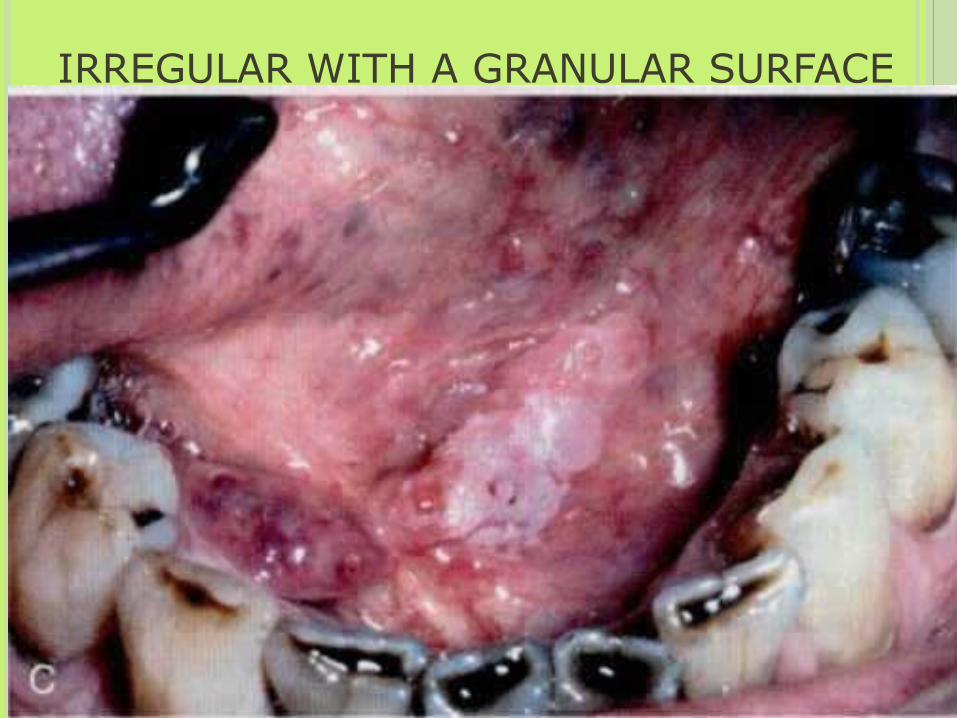
IRREGULAR WITH A GRANULAR SURFACE

DIFFUSE & CORRUGATED
MICROSCOPY
Hyperkeratosis
Thickened acanthotic but orderly epithelium
Markedly dysplastic changes
Carcinoma in situInflammation – lymphocytes and macrophages

Keratosis without dysplasia

Moderate dysplasia Mild dysplasia Severe dysplasia

EPITHELIAL DYSPLASIA
ERYTHROPLAKIA Red, velvety, possibly eroded
Usually flat, may be depressed
Intense subepithelial inflammatory reaction with vascular dilatation Redness
Epithelium shows marked atypia
90% show superficial erosions with dysplasia, Ca in situ or Ca at the margins

SQUAMOUS CELL CARCINOMA Most(95%) of the malignant tumours of
the oral cavity are SCC
Remainder includes salivary gland tumours and melanomas
Aggressive
PATHOGENESIS
Multifactorial
Middle aged men Smoking tobacco, alcohol HPV infection in 50% of oropharyngeal Ca
Other countries – chewing betel quid, paan
Protracted irritation from ill fitting dentures, jagged teeth, chr. infections



GROSS Raised, firm, pearly plaque
Irregular, roughened or verrucous
Background – leukoplakia or erythroplakia
Ulcerate and protrude as mass with irregular, firm and indurated (rolled) borders

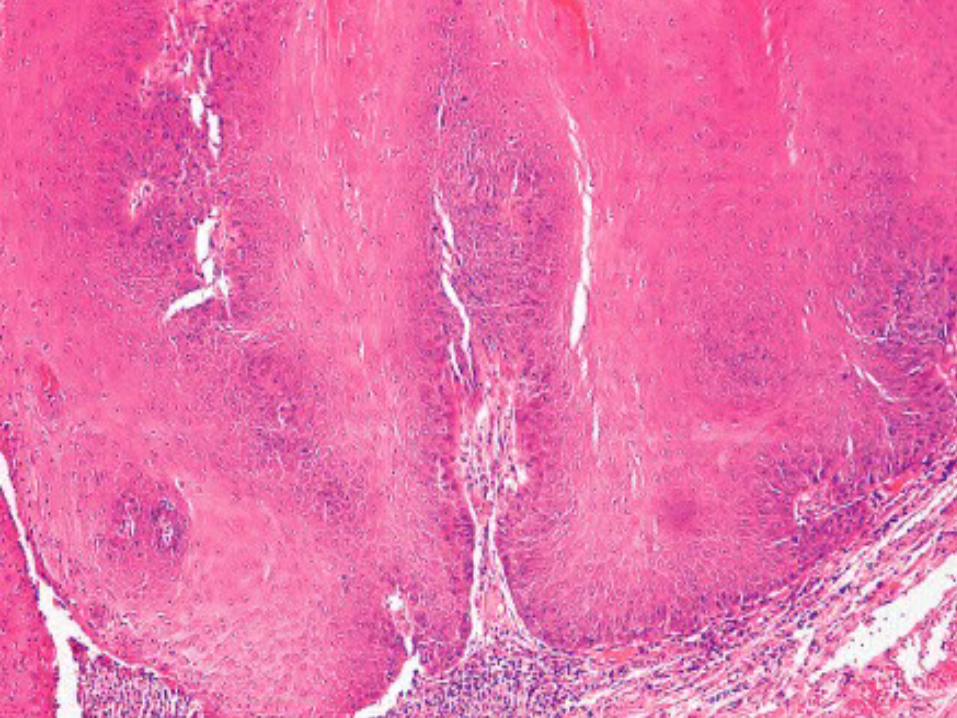
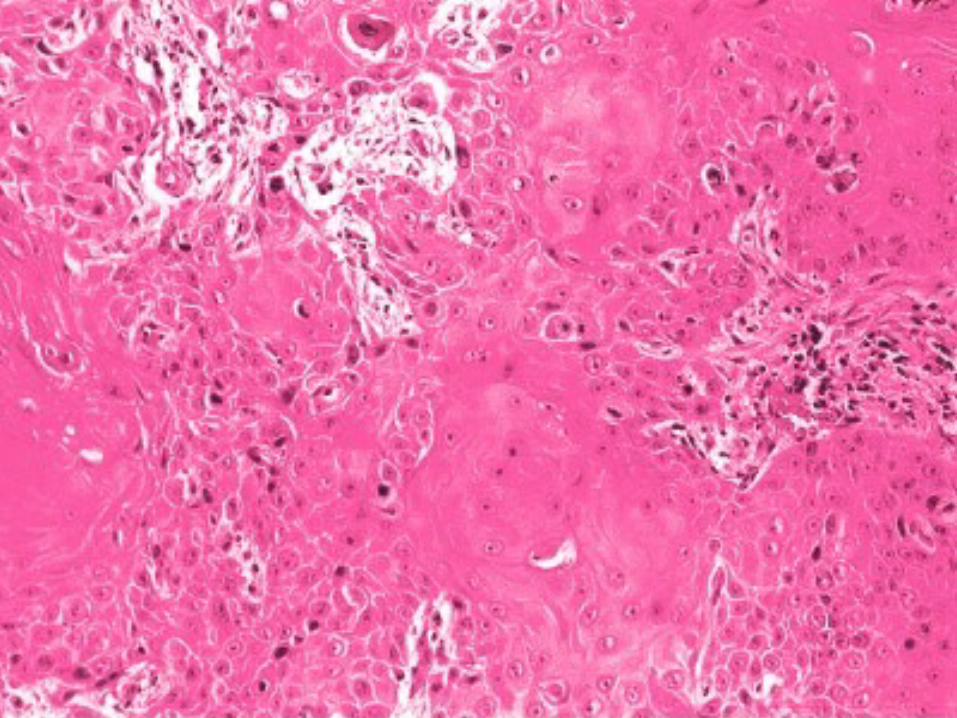
MICROSCOPY
Well differentiated keratinizing tumor to anaplastic, sometimes sarcomatoid tumor
But degree of differentiation does
not correlate with clinical behavior

Local metastasis – cervical LNs
Distant metastasis:# Mediastinal LNs# Lungs# Liver# Bones
PROGNOSIS
5yr survival Early oral cancer – 80%Late stage – 19%
TUMOURS OF THE OESOPHAGUS.

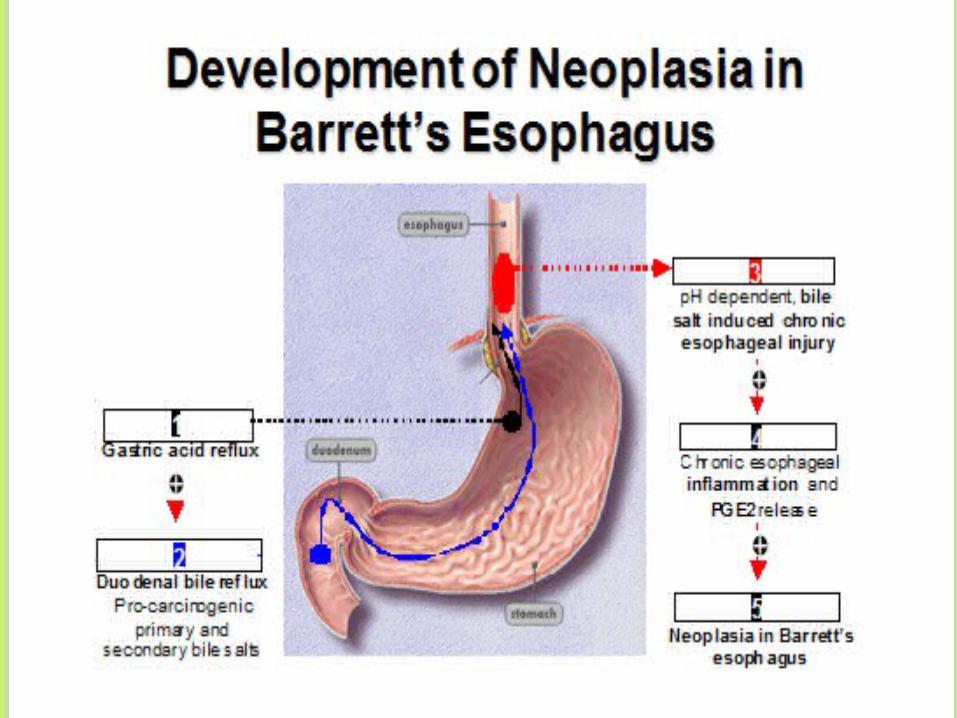
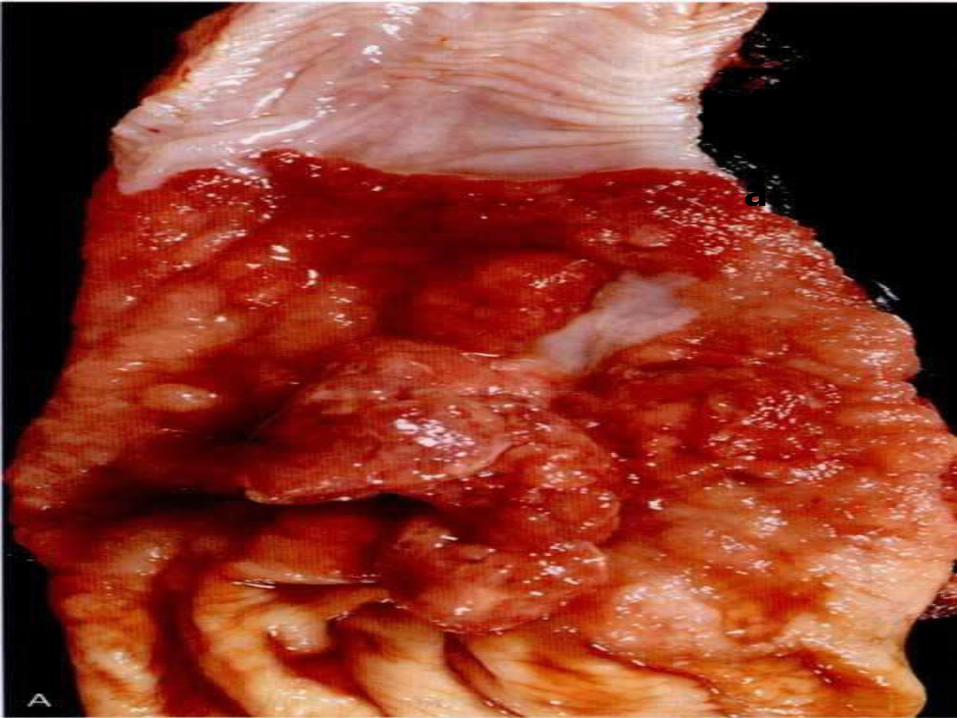
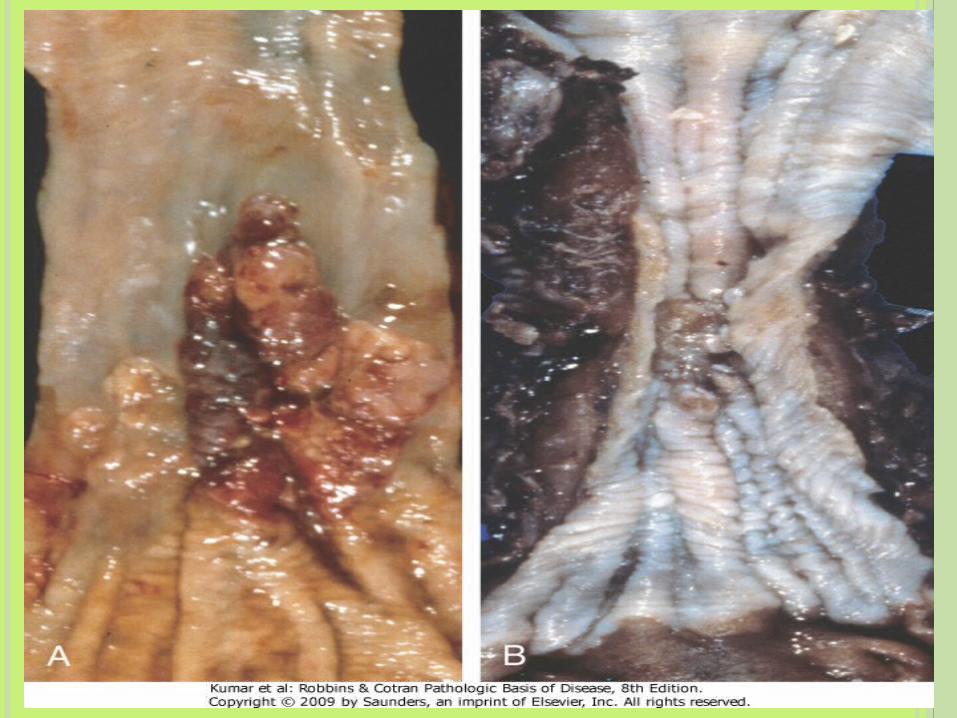
BARRETT ESOPHAGITIS Complication of long standing GERD Distal squamous mucosa is replaced by
metaplastic columnar epithelium as a result of prolonged injury
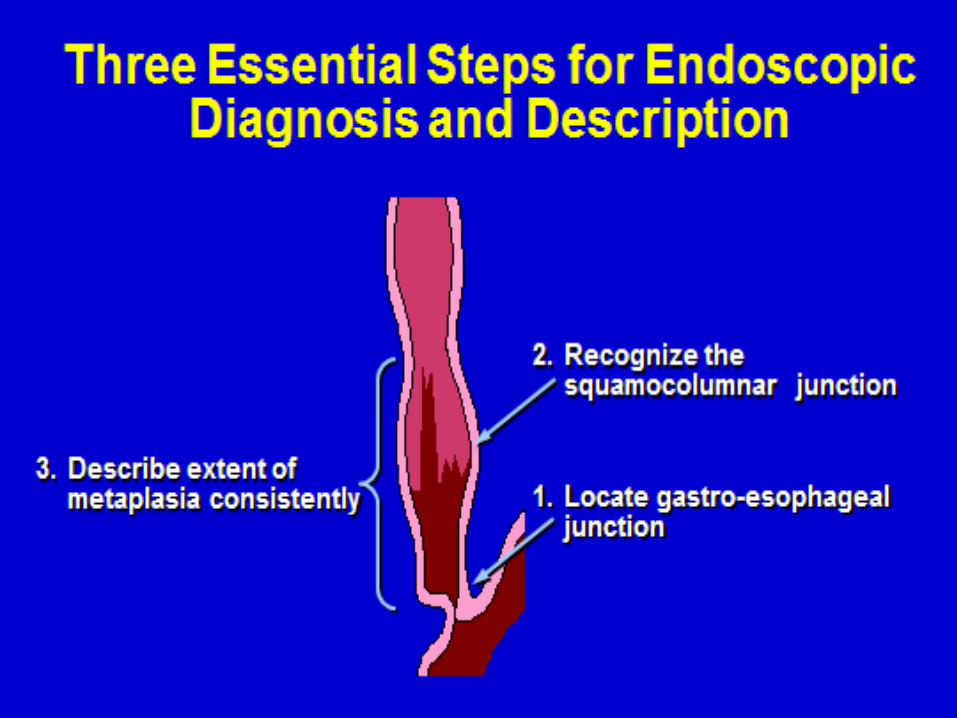
Short segment(<3 cm) / long segment 2 criteria – Endoscopic evidence of columnar
lining above GE junction, Histological evidence of intestinal metaplasia

MORPHOLOGY
Red velvety
mucosa
Between pale pink
esophageal
mucosa
Tongues/ patches/
circumferential
bands
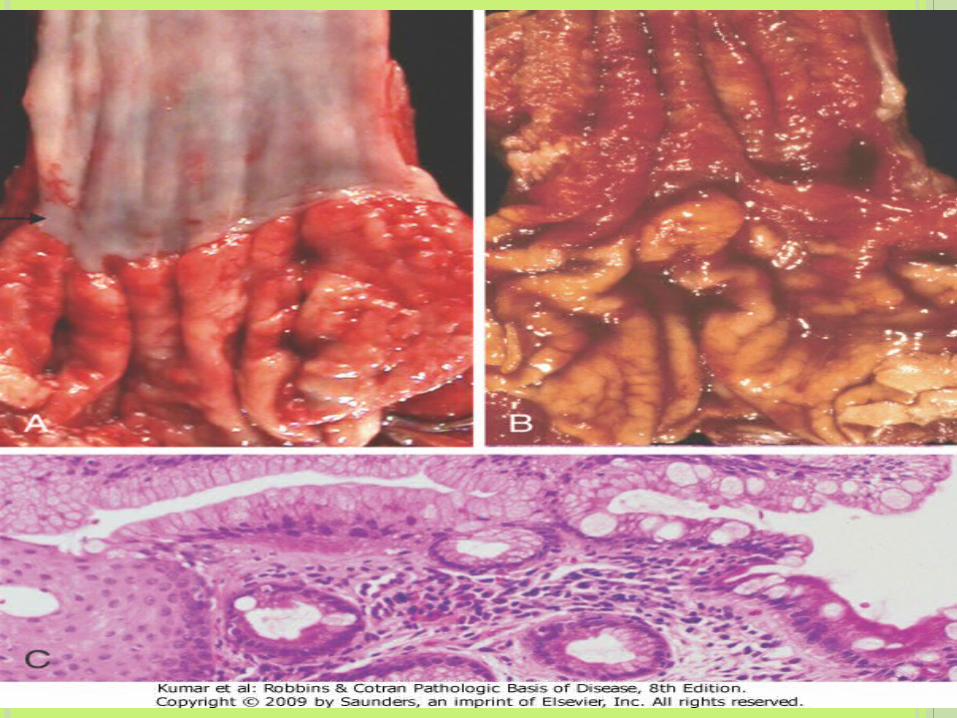
MICROSCOPYEsophageal squamous epithelium is replaced by metaplastic columnar epithelium.
Definitive diagnosis when columnar mucosa contains intestinal goblet cells
Dysplasia may be low/ high gradeEnlarged crowded hyperchromatic nuclei & loss of intervening stroma

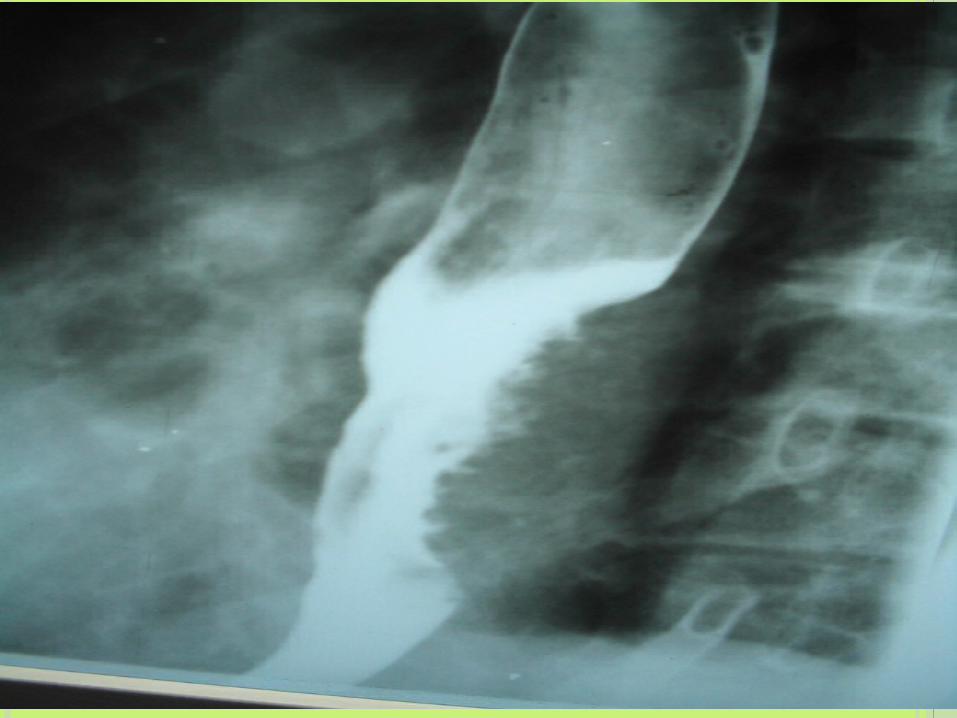
Barrett’s esophagitis
CLINICAL FEATURES White males – 40 to 60 yrs Reflux heart burn , strictures, bleeding 30 – 40% increase in risk of adeno carcinomaProgression to adeno carcinoma – multi step
process

TUMOURS OF THE OESOPHAGUS
Benign Malignant Squamous cell carcinoma Adenocarcinoma

RISK FACTORS
Human papilloma virus HPV serotype 16 was identified in 9 percent of resection specimens from 70 Chinese patients with esophageal SCC.
Tylosis rare disease associated with hyperkeratosis of the palms of the hands and soles of the feet and a high rate of esophageal SCC

GIT neoplasms
ESOPHAGUS: Squamous cell Carcinoma
Commoner in elderly, males, blacks
Incidence higher in Iran, Central China, S Africa, S Brazil
Dietary factors: Deficiency of vitamins, trace elements;
Fungal contamination of foodstuffs, Nitrites and
nitrosamines
Lifestyle: Alcohol, Tobacco, Betel, Burning hot food,
Urban life
Esophageal disorders: Esophagitis, Achalasia, P-V
syndrome
Genetic: Racial, Celiac disease, Ectodermal dysplasia


ESOPHAGUS: SQUAMOUS CELL CARCINOMA
Insidious onset and late presentation
Dysphagia and obstruction
Extreme weight loss
Ulceration, Tracheo-esophageal fistula,
Prognosis depends on early diagnosis and
treatment.
Prognosis also depends on presence /
absence of lymph node metastases

20% are in upper 1/3
50% are in mid 1/3
30% are in lower 1/3 Three morphological patterns
Polypoid (60%)
Flat (15)
Ulcerated (25%) Early local extension Metastases to
Cervical nodes
Mediastinal nodes
Gastric and celiac nodes
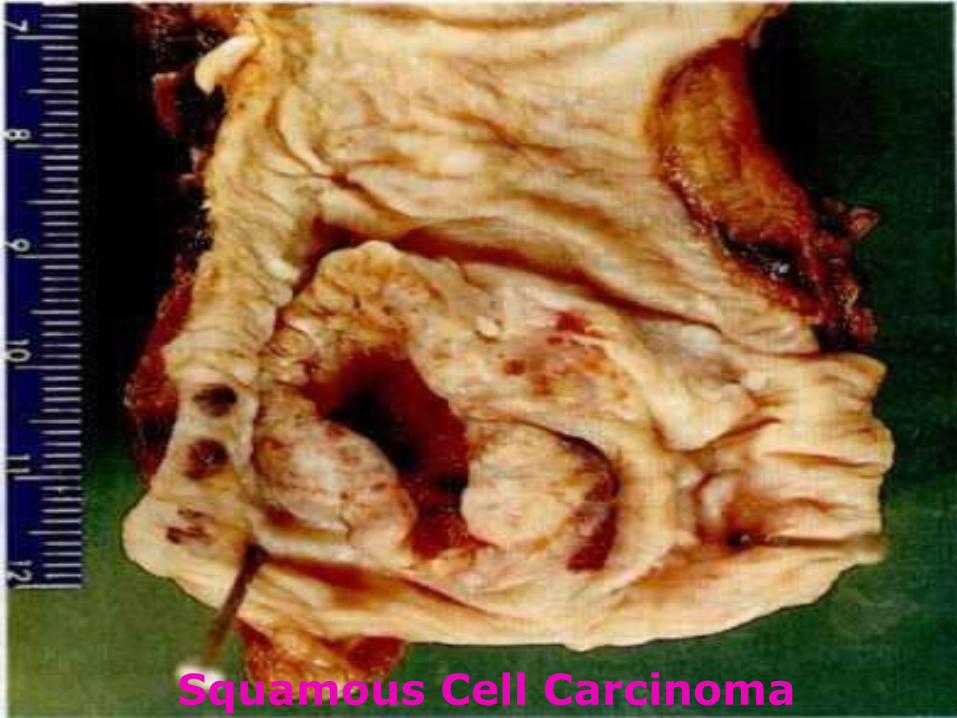
Squamous Cell Carcinoma


ESOPHAGUS: ADENOCARCINOMA
Higher incidence being reported from west
Seen in lower 1/3 of esophagus
Majority arise from Barrett Esophagus (10% risk)
More common above 40 years, in men, in whites
Present with long term dyspepsia, heart burn,
dysphagia, vomiting
Prognosis is poor with < 20% 5 year survival
Adenocarcinoma



THANK YOU

















