7th Annual Meeting of the Americas Committee for Treatment and Research in Multiple Sclerosis 18th Congress of the European Committee for Treatment and Research in Multiple Sclerosis Baltimore Marriott Waterfront Hotel 700 Aliceanna Street Baltimore, Maryland, USA Wednesday, September 18 through Saturday, September 21 2002 Final Program,Abstract Listing and Meeting Information
Transcript
A
7th Annual Meeting of the Americas Committee for Treatment and Research
in Multiple Sclerosis
18th Congress of the European Committee for Treatment and Research
Final Program,Abstract Listing and Meeting Information
Acknowledgement of SponsorsThe ACTRIMS-ECTRIMS 2002 Steering Committee
acknowledges the generous support of our Gold Sponsors:
This program is offered in collaboration with the National Multiple Sclerosis Society.
The Steering Committee also acknowledges the support of Wyeth Pharmaceuticals
Welcome Letter
Dear Colleagues and Friends,
We cordially welcome you to Baltimore, Maryland, and ACTRIMS-ECTRIMS 2002, the second joint meeting of theAmericas and European Committees for Research and Treatment in Multiple Sclerosis. This is an exciting time in MSresearch and clinical care. Decades of basic investigation have resulted in greatly improved understanding of MS,which is now being translated into proven therapies. However, we—and the patients we serve—cannot be satisfiedwith the current state of our knowledge and treatments. We hope that the information provided during this impor-tant meeting will further advance the goal of finally conquering MS and its resulting disability.
Our three key areas of research highlighted at the conference are:
• Inflammation, Demyelination, and Axonal Loss: Pathological and MRI Perspectives• Neuroprotection• Methodological Issues in Clinical Trials
In addition to the official program, we are pleased to offer two pre-conference symposia sponsored by groups longassociated with the treatment of MS and five satellite symposia supported by our gold sponsors.
We extend our appreciation to our Program Committee, chaired by Drs. Suhayl Dhib-Jalbut and Paul O’Connor,for their tireless effort in guiding and shaping the content of this comprehensive meeting.
We hope that you will join us for each of the social activities, planned by our Local Arrangements Committeechaired by Drs. Chris Bever and Peter Calabresi, and that you will allow some time to explore the harbor city ofBaltimore, with its array of shopping destinations, historical sites, museums and galleries.
We look forward to your active participation in this very interesting program. Thank you for joining us.
Dr. Kenneth Johnson Dr.Alan ThompsonChair, ACTRIMS President, ECTRIMS
MS affects different people in different ways each and
every day. Rebif ® has been proven to provide patients
with the following treatment benefits in the main
measures of disease activity:
• Reduces MRI lesion activity1*
• Reduces frequency of relapse1,2
• Delays progression of disability1,2
References:1. PRISMS (Prevention of Relapses and Disability by Interferon beta-1a Subcutaneously in Multiple Sclerosis) Study Group. Randomized
double-blind placebo-controlled study of interferon beta-1a in relapsing/remitting multiple sclerosis. Lancet. 1998;352:1498-1504.2. Rebif® (interferon beta-1a) Prescribing Information. Serono, Inc; 2002.3. Data on File.Amendment to BLA File, Study 21125, Serono, Inc; 2002.
Please see brief summary directly following MS LifeLinesTM ad
*The exact relationship between MRI findings and the clinical status of patients is unknown.
Rebif is the market leader outside the US.Rebif is available in more than 70 countries.
5
Results.Rebif®.
Adverse reactions at 24 weeks were generally similar despitehigher, more frequent, subcutaneous dosing with Rebif 2.Exceptions included injection-site disorders, hepatic functiondisorders, and leukopenia2,3.
Rebif® (interferon beta-1a) is indicated for the treatmentof patients with relapsing multiple sclerosis to decreasethe frequency of clinical exacerbations and delay theaccumulation of physical disability. Rebif should be usedwith caution in patients with depression, pre-existingseizure disorders, and liver problems.
For more information on the benefits of Rebif therapy,please visit www.rebif.com or call 1-877-44-Rebif (447-3243)
Please see brief summary directly followingMS LifeLinesTM ad
• Rebif® is the first and only interferon available in ready-to-use, prefilled syringes• Rebif is administered subcutaneously• Rebiject™ injection device ensures proper injection technique • Injection training with a licensed nurse• Travel Kit including prepaid phonecard makes travel easier• Patients are just one toll-free phone call away from professionals who
Patients with MS are just one toll-free phone call away from professionals who can offer immediate assistance.Patients can call todayPhone: 1-877-44-Rebif (1-877-447-3243)Fax: 1-866-22-Rebif (1-866-227-3243)or visit our websites at:www.MSLifeLines.com www.rebif.com
Response• Dedicated team of trained Customer Support Specialists
available Monday through Friday from 8 AM to 8 PM EST• English and Spanish language support available
Exhibits and Poster DisplaysHarborside and Grand Ballroom Levels
Wednesday: 1:00 pm–5:00 pm Thursday and Friday: 8:00 am–5:00 pm
Satellite Symposium I5:00 pm–6:00 pmGrand Ballroom VI
Satellite Symposium III6:00 pm–7:00 pm
Grand Ballroom VI–X
Satellite Symposium II4:30 pm–5:30 pm
Grand Ballroom I–V
Social EventB&O Railroad
Museum7:30 pm–10:00 pm
Satellite Symposium V6:00 pm–7:00 pm
Grand Ballroom VI–X
Satellite Symposium IV4:30 pm–5:30 pm
Grand Ballroom I–V
Closing Lunch12:00 pm–1:00 pm
Harborside Ballroom
9
®
Biogen and Elan –pioneers in adhesion molecule biotechnology
General Information
AttireSince meeting room temperature and personal comfortlevels vary, it is recommended that you bring a sweateror jacket to the conference activities. Attire for meetingsand social events is business casual.
BadgesAttendees will be required to wear their delegate badgeat all times to access the exhibition area, the conferencerooms and the posters area. Colored ribbons denotethe following:
Committee Members WHITEExhibitors ORANGEPoster Presenters LIGHT BLUEPress PINKSpeakers BLUEStaff REDVolunteers GREEN
BaltimoreFor information regarding airports, activities, ground trans-portation, etc., consult the Baltimore Area Conventionand Visitors Association website at www.baltimore.org.
Child Care InformationA variety of child care options are available in Baltimore.You may wish to check with the concierge at your hotelupon arrival.
Contact InformationACTRIMS-ECTRIMS 2002c/o NMSS733 Third Avenue 6th FloorNew York, NY 10017 USAPhone: 212-476-0465Fax: 212-661-9735E-mail: [email protected]
E-Mail StationsComplimentary e-mail stations and printers will be avail-able in the Harborside Level Foyer. Please limit your useto 15 minutes. This service is available to registered par-ticipants only. Thank you for your cooperation.
LanguageEnglish is the official language of the conference. Nosimultaneous translation is available.
MealsThe registration fee for conference participants includescontinental breakfast, coffee breaks, lunches during theconference, and the evening social events organized bythe Steering Committee.
Mobile PhonesThe Steering Committee request that attendees turncellular phones and pagers to vibrate upon entering allexhibit and social functions.
No SmokingFor the health and comfort of everyone, smoking is pro-hibited at any meeting function. This includes all scientificactivities, exhibits and social functions.
Optional Social ToursFor half-day and whole-day excursions to sites in andaround Baltimore,please consult the conciege at your hotel.
PhotographyFlash picture taking is not allowed during the scientificactivities or in the exhibit area.
Recording of ProgramsAudio and videotaping are not allowed in the meetingrooms, exhibit area, or at social functions.
Special NeedsIf you have a special need that requires an accommo-dation, please stop by the registration desk and speakwith an organizing staff member.
WeatherSeptember temperatures range from 65 F (18 C) to 80 F (27 C).
11
12
Floor Diagrams
Level 4
Level 3
Conference10:00 am–10:00 pmA
Conference6:00 am–7:30 pmA
Conference6:30 am–7:30 pmA
Conference7:00 am–2:00 pmA
8:30 pm–11:00 pmC 8:30 pm–11:00 pmE
Aquarium Party7:00 pm–7:30 pmB
B&O Party7:00 pm–8:00 pmD
Committee Reception(by invitation)
6:30 pm–10:30 pmF
13
Transportation Schedule
Wednesday Thursday Friday SaturdaySeptember 18 September 19 September 20 September 21
A Continuous shuttle service between auxiliary hotels and BaltimoreMarriott Waterfront Hotel
B Transportation from Baltimore Marriott Waterfront Hotel to theNational Aquarium in Baltimore for those unable/reluctant to walk
C Transportation from the National Aquarium in Baltimore to auxiliaryhotels and to Baltimore Marriott Waterfront Hotel
D Transportation from Baltimore Marriott Waterfront Hotel to B&ORailroad Museum
E Transportation from B&O Railroad Museum to auxiliary hotels andto Baltimore Marriott Waterfront Hotel
F Round-trip water taxi service from Baltimore Marriott WaterfrontHotel to the Baltimore Museum of Industry
So does her treatmentAVONEX® in relapsing forms of MS• Strong against both disability and relapses– reduces the progression to sustained disability by 37%
and lowers relapse rates1
• Strong against inflammation– 91% reduction in T2 lesion volume and 89% reduction
in gadolinium-enhanced lesions2,3
• Strong against atrophy– decreased brain atrophy by 55% in year 2 of a clinical trial 4
• Strong with patients– AVONEX® is the #1 prescribed MS therapy and delivers 95%
patient satisfaction5,6
• The difference is in the delivery– IM administration keeps effective amounts of AVONEX®
in the body longer than the SC route7
The most common side effects associated with AVONEX® treatment are flu-like symptoms,muscle ache (myalgia), fever, and chills. Other common side effects seen, but not statisticallydifferent from placebo, were headache (AVONEX®: 67%, placebo: 57%), pain (AVONEX®:24%, placebo: 20%), and asthenia (AVONEX®: 21%, placebo: 13%).
AVONEX® should be used with caution in patients with depression and in patients withseizure disorders. AVONEX® should not be used by pregnant women. Patients with cardiac dis-ease should be closely monitored. Routine periodic blood chemistry and hematology tests arerecommended during treatment with AVONEX®.
The exact relationship between MRI findings and the clinical status of patients is unknown.Changes in lesion area often do not correlate with changes in disability progression.
®
AVONEX® (Interferon beta-1a)
For more detailed information, consult full prescribing information. A brief summary follows.
INDICATIONS AND USAGEAVONEX® ( Interferon beta-1a) is indicated for the treatment of relapsing forms of
multiple sclerosis to slow the accumulation of physical disability and decrease the fre-quency of clinical exacerbations. Safety and efficacy in patients with chronic progressivemultiple sclerosis have not been evaluated.
CONTRAINDICATIONS AVONEX® (Interferon beta-1a) is contraindicated in patients with a history of hypersen-
sitivity to natural or recombinant interferon beta, human albumin, or any other componentof the formulation.
WARNINGS AVONEX® (Interferon beta-1a) should be used with caution in patients with depression.
Depression and suicide have been reported to occur in patients receiving other interferoncompounds. Depression and suicidal ideation are known to occur at an increased frequency in the multiple sclerosis population. A relationship between occurrence ofdepression and/or suicidal ideation and the use of AVONEX® has not been established. Anequal incidence of depression was seen in the placebo-treated and AVONEX® -treatedpatients in the placebo-controlled multiple sclerosis study. Patients treated with AVONEX®
should be advised to report immediately any symptoms of depression and/or suicidalideation to their prescribing physicians. If a patient develops depression, cessation of AVONEX® therapy should be considered.
PRECAUTIONS
GeneralCaution should be exercised when administering AVONEX® ( Interferon beta-1a) to
patients with pre-existing seizure disorder. In the placebo-controlled study, 4 patientsreceiving AVONEX® experienced seizures, while no seizures occurred in the placebogroup. Three of these 4 patients had no prior history of seizure. It is not known whetherthese events were related to the effects of multiple sclerosis alone, to AVONEX®, or to acombination of both. For patients with no prior history of seizure who develop seizuresduring therapy with AVONEX®, an etiologic basis should be established and appropriateanti-convulsant therapy instituted prior to considering resumption of AVONEX® treatment.The effect of AVONEX® administration on the medical management of patients with seizuredisorder is unknown.
Patients with cardiac disease, such as angina, congestive heart failure, or arrhythmia,should be closely monitored for worsening of their clinical condition during initiation andcontinued treatment with AVONEX®. While AVONEX® does not have any known direct-acting cardiac toxicity, during the post-marketing period infrequent cases of congestiveheart failure, cardiomyopathy, and cardiomyopathy with congestive heart failure havebeen reported in patients without known predisposition to these events or other known eti-ologies; in rare cases, these events have been temporally related to the administration ofAVONEX®. In rare cases, these events have recurred upon rechallenge in patients withknown predisposition.
Information to PatientsPatients should be informed of the most common adverse events associated with
AVONEX® administration, including symptoms associated with flu syndrome (see AdverseReactions section). Symptoms of flu syndrome are most prominent at the initiation oftherapy and decrease in frequency with continued treatment. In the placebo-controlledstudy, patients were instructed to take 650 mg acetaminophen immediately prior to injec-tion and for an additional 24 hours after each injection to modulate acute symptoms asso-ciated with AVONEX® administration.
Patients should be cautioned to report depression or suicidal ideation (see Warnings). Patients should be advised about the abortifacient potential of interferon beta (see
Pregnancy – Teratogenic Effects).When a physician determines that AVONEX® can be used outside of the physician’s
office, persons who will be administering AVONEX® should receive instruction in recon-stitution and injection, including the review of the injection procedures (see full prescribing information). If a patient is to self-administer, the physical ability of that patientto self-inject intramuscularly should be assessed. The first injection should be performedunder the supervision of a qualified health care professional. A puncture-resistant con-tainer for disposal of needles and syringes should be used. Patients should be instructedin the technique and importance of proper syringe and needle disposal and be cautionedagainst reuse of these items.
Laboratory TestsIn addition to those laboratory tests normally required for monitoring patients with mul-
tiple sclerosis, complete blood and differential white blood cell counts, platelet counts,and blood chemistries, including liver function tests, are recommended during AVONEX®
( Interferon beta-1a) therapy. During the placebo-controlled study, these tests were per-formed at least every 6 months. There were no significant differences between the placeboand AVONEX® groups in the incidence of liver enzyme elevation, leukopenia, or thrombo-cytopenia. However, these are known to be dose-related laboratory abnormalities asso-ciated with the use of interferons. Patients with myelosuppression may require more inten-sive monitoring of complete blood cell counts, with differential and platelet counts.
Drug InteractionsNo formal drug interaction studies have been conducted with AVONEX® ( Interferon
beta-1a). In the placebo-controlled study, corticosteroids or ACTH were administered fortreatment of exacerbations in some patients concurrently receiving AVONEX®. In addi-tion, some patients receiving AVONEX® were also treated with anti-depressant therapy and/ororal contraceptive therapy. No unexpected adverse events were associated with theseconcomitant therapies.
Other interferons have been noted to reduce cytochrome P-450 oxidase-mediated drugmetabolism. Formal hepatic drug metabolism studies with AVONEX® in humans have notbeen conducted. Hepatic microsomes isolated from AVONEX®-treated rhesus monkeysshowed no influence of AVONEX® on hepatic P-450 enzyme metabolism activity.
As with all interferon products, proper monitoring of patients is required if AVONEX® isgiven in combination with myelosuppressive agents.
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Carcinogenesis: No carcinogenicity data for Interferon beta-1a are available in animalsor humans.
Mutagenesis: Interferon beta-1a was not mutagenic when tested in the Ames bacterialtest and in an in vitro cytogenetic assay in human lymphocytes in the presence andabsence of metabolic activation. These assays are designed to detect agents that interactdirectly with and cause damage to cellular DNA. Interferon beta-1a is a glycosylated pro-tein that does not directly bind to DNA.
Impairment of Fertility: No studies were conducted to evaluate the effects of interferonbeta on fertility in normal women or women with multiple sclerosis. It is not known whetherInterferon beta-1a can affect human reproductive capacity.
Menstrual irregularities were observed in monkeys administered interferon beta at adose 100 times the recommended weekly human dose (based upon a body surface areacomparison). Anovulation and decreased serum progesterone levels were also noted tran-siently in some animals. These effects were reversible after discontinuation of drug.
Treatment of monkeys with interferon beta at 2 times the recommended weekly humandose (based upon a body surface area comparison) had no effects on cycle duration orovulation.
The accuracy of extrapolating animal doses to human doses is not known. In theplacebo-controlled study, 6% of patients receiving placebo and 5% of patients receivingAVONEX® (Interferon beta-1a) experienced menstrual disorder. If menstrual irregularitiesoccur in humans, it is not known how long they will persist following treatment.
Pregnancy – Teratogenic EffectsPregnancy Category C: The reproductive toxicity of AVONEX® has not been studied in
animals or humans. In pregnant monkeys given interferon beta at 100 times the recom-mended weekly human dose (based upon a body surface area comparison), no teratogenicor other adverse effects on fetal development were observed. Abortifacient activity wasevident following 3 to 5 doses at this level. No abortifacient effects were observed in mon-keys treated at 2 times the recommended weekly human dose (based upon a body sur-face area comparison). Although no teratogenic effects were seen in these studies, it is notknown if teratogenic effects would be observed in humans. There are no adequate andwell-controlled studies with interferons in pregnant women. If a woman becomes pregnantor plans to become pregnant while taking AVONEX®, she should be informed of the poten-tial hazards to the fetus, and it should be recommended that the woman discontinuetherapy.
Nursing MothersIt is not known whether Interferon beta-1a is excreted in human milk. Because of the
potential of serious adverse reactions in nursing infants, a decision should be made toeither discontinue nursing or to discontinue AVONEX®.
Pediatric UseSafety and effectiveness in pediatric patients below the age of 18 years have not been
established.
Geriatric UseSafety and effectiveness in geriatric patients above the age of 65 years have not been
established.
ADVERSE REACTIONSThe safety data describing the use of AVONEX® ( Interferon beta-1a) in multiple scle-
rosis patients are based on the placebo-controlled trial in which 158 patients ran-domized to AVONEX® were treated for up to 2 years (see Clinical Studies).
The 5 most common adverse events associated (at p ≤ 0.075) with AVONEX® treatmentwere flu-like symptoms (otherwise unspecified), muscle ache, fever, chills, and asthenia.The incidence of all 5 adverse events diminished with continued treatment.
One patient in the placebo group attempted suicide; no AVONEX®-treated patientsattempted suicide. The incidence of depression was equal in the 2 treatment groups.However, since depression and suicide have been reported with other interferon products,AVONEX® should be used with caution in patients with depression (see Warnings).
In the placebo-controlled study, 4 patients receiving AVONEX® experienced seizures,while no seizures occurred in the placebo group. Three of these 4 patients had no prior his-tory of seizure. It is not known whether these events were related to the effects of multi-ple sclerosis alone, to AVONEX®, or to a combination of both (see Precautions).
The following table enumerates adverse events and selected laboratory abnormalitiesthat occurred at an incidence of 2% or more among the 158 multiple sclerosis patientstreated with 30 mcg of AVONEX® once weekly by IM injection. Reported adverse eventshave been classified using standard COSTART terms. Terms so general as to be unin-formative and those events that were equal in incidence or more common in theplacebo-treated patients have been excluded.
AVONEX® ( Interferon beta-1a) has also been evaluated in 290 patients with illnessesother than multiple sclerosis. The majority of these patients were enrolled in studies toevaluate AVONEX® treatment of chronic viral hepatitis B and C, in which the doses studiedranged from 15 mcg to 75 mcg, given SC, 3 times a week, for up to 6 months. The inci-dence of common adverse events in these studies was generally seen at a frequency sim-ilar to that seen in the placebo-controlled multiple sclerosis study. In these non-multi-ple sclerosis studies, inflammation at the site of the SC injection was seen in 52% oftreated patients. In contrast, injection site inflammation was seen in 3% of multiple scle-rosis patients receiving 30 mcg AVONEX® by IM injection. Subcutaneous injections werealso associated with the following local reactions: injection site necrosis, injection siteatrophy, injection site edema and injection site hemorrhage. None of the above wasobserved in the multiple sclerosis patients participating in the placebo-controlled study.
Other events observed during premarket and postmarket evaluation of AVONEX®,administered either SC or IM, are listed in the paragraph that follows. Because most of the events were observed in open and uncontrolled studies, or in marketed use, the role of AVONEX® ( Interferon beta-1a) in their causation cannot be reliably determined.Body as a Whole: abscess, ascites, cellulitis, facial edema, hernia, injection site fibro-sis, injection site hypersensitivity, injection site pain, lipoma, neoplasm, photosensitiv-ity reaction, rigors, sepsis, sinus headache, toothache; Cardiovascular System:arrhythmia, arteritis, cardiomyopathy, congestive heart failure, heart arrest, hemor-rhage, hypotension, palpitation, pericarditis, peripheral ischemia, peripheral vasculardisorder, postural hypotension, pulmonary embolus, spider angioma, tachycardia,telangiectasia, vascular disorder; Digestive System: blood in stool, colitis, constipa-tion, diverticulitis, dry mouth, gallbladder disorder, gastritis, gastrointestinal hemorrhage,gingivitis, gum hemorrhage, hepatitis, hepatoma, hepatomegaly, increased appetite,intestinal perforation, intestinal obstruction, liver function test abnormalities, periodon-tal abscess, periodontitis, proctitis, thirst, tongue disorder, vomiting; Endocrine System:hyperthyroidism, hypothyroidism; Hemic and Lymphatic System: coagulation timeincreased, ecchymosis, lymphadenopathy, petechia; Metabolic and Nutritional Dis-orders: abnormal healing, dehydration, hypoglycemia, hypomagnesemia, hypokalemia;Musculoskeletal System: arthritis, bone pain, myasthenia, osteonecrosis, synovitis;Nervous System: abnormal gait, amnesia, anxiety, Bell’s Palsy, clumsiness, confu-sion, depersonalization, drug dependence, emotional lability, facial paralysis, hyper-esthesia, hypertonia, increased libido, neurosis, paresthesia, psychosis, transientsevere weakness; Respiratory System: bronchospasm, emphysema, hemoptysis,hiccup, hyperventilation, laryngitis, pharyngeal edema, pneumonia; Skin andAppendages: basal cell carcinoma, blisters, cold clammy skin, contact dermatitis,erythema, furunculosis, genital pruritus, nevus, pruritus, rash, seborrhea, skin ulcer,skin discoloration; Special Senses: abnormal vision, conjunctivitis, earache, eye pain,labyrinthitis, vitreous floaters; Urogenital: breast fibroadenosis, breast mass, dysuria,epididymitis, fibrocystic change of the breast, fibroids, gynecomastia, hematuria, kidney
Serum Neutralizing ActivityThroughout the placebo-controlled multiple sclerosis study, serum samples from patients
were monitored for the development of Interferon beta-1a neutralizing activity. During thestudy, 24% of AVONEX®-treated patients were found to have serum neutralizing activity atone or more time points tested. Fifteen percent of AVONEX®-treated patients tested pos-itive for neutralizing activity at a level at which no placebo patient tested positive. Thesignificance of the appearance of serum neutralizing activity is unknown.
DRUG ABUSE AND DEPENDENCEThere is no evidence that abuse or dependence occurs with AVONEX® (Interferon beta-
1a) therapy. However, the risk of dependence has not been systematically evaluated.
DOSAGE AND ADMINISTRATIONThe recommended dosage of AVONEX® (Interferon beta-1a) for the treatment of relaps-
ing forms of multiple sclerosis is 30 mcg injected intramuscularly once a week.AVONEX® is intended for use under the guidance and supervision of a physician.
Patients may self-inject only if their physician determines that it is appropriate and withmedical follow-up, as necessary, after proper training in intramuscular injection technique.
References:1. Jacobs LD, Cookfair DL, Rudick RA, et al, and the Multiple Sclerosis Collaborative Research Group(MSCRG). Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. AnnNeurol. 1996;39:285-294. 2. Jacobs LD, Beck RW, Simon JH, et al, and the CHAMPS (Controlled High-RiskSubjects Avonex Multiple Sclerosis Prevention Study) Study Group. Intramuscular interferon beta-1a therapy initiated during a first demyelinating event in multiple sclerosis. N Engl J Med. 2000;343:898-904.3. Data on file: Jacobs LD; Phase III pivotal trial. Biogen, Inc. 4. Rudick RA, Fisher E, Lee J-C, Simon J,Jacobs L, and the Multiple Sclerosis Collaborative Research Group. Use of the brain parenchymal fractionto measure whole brain atrophy in relapsing-remitting MS. Neurology. 1999;53:1698-1704. 5. IMS Health,Inc., through Oct 2001. 6. Taylor-Nelson Sofres Healthcare MS Patient Study 2001. 7. Alam J, McAllister A,Scaramucci J, Jones W, Rogge M. Pharmacokinetics and pharmacodynamics of interferon beta-1a (IFNß-1a) in healthy volunteers after intravenous, subcutaneous or intramuscular administration. Clin Drug Invest. 1997;14:35-43.
YOUNG SCIENTIFICINVESTIGATORS SESSIONCo-chairs: D Brassat (San Francisco, USA)
A Petzold (London, UK)S Dhib-Jalbut (Baltimore, USA)
Grand Ballroom I–V
2:00 WELCOME and ANNOUNCEMENT, 2002 YOUNG NEUROLO-GISTS AND TRAINEES (YNT)–SCHERING FELLOWSHIP AWARDS Hickmann (London, UK)
2:10 1 HLA-DRB5*0101 AND -DRB1*1501 EXPRESSION IN THEMULTIPLE SCLEROSIS-ASSOCIATED HLA-DR15DW2 HAPLOTYPEE Prat,WW Kwok, N Kruse, R Pujol-Borrell, MP Bettinotti, HF McFarland, R Martin(Bethesda, USA)
2:25 2 QUALITATIVE AND QUANTITATIVE ANALYSIS OF THEBLOOD TCR � CHAIN TRANSCRIPTOME AT DIFFERENT TIME POINTSOF MULTIPLE SCLEROSIS COURSE DA Laplaud, S Wiertlewski, M Guillet,C Ruiz, B Melchior, G Edan, P Damier, J Soulillou (Nantes, France)
2:40 3 EXPRESSION OF METABOTROPIC GLUTAMATE RECEPTORSIN MULTIPLE SCLEROSIS BRAIN: UPREGULATION IN AXONS ANDREACTIVE ASTROCYTES J J Geurts,W Kamphorst, P van der Valk, EM Aronica(Amsterdam, Netherlands)
2:55 4 GROUP CONNECTIVITY MAPS OF OPTIC RADIATIONSAFTER ISOLATED OPTIC NEURITIS O Ciccarelli, SJ Hickman, AT Toosy,GJ Parker, CA Wheeler-Kingshott, GJ Barker, DH Miller, AJ Thompson (London, UK)
3:10 5 FUNCTIONAL DIVERSITY OF ANTIBODIES AGAINSTMYELIN/OLIGODENDROCYTE GLYCOPROTEIN IN EXPERIMENTALAUTOIMMUNE DEMYELINATION H von Büdingen, SL Hauser,A Fuhrmann,CB Nabavi, CP Genain (San Francisco, USA)
3:25 6 MRI EVIDENCE OF MORE EXTENSIVE TISSUE DAMAGE INMS PATIENTS WITH THE �4 ALLELE OF APOLIPOPROTEIN E: HIGHERPROPORTION OF LESIONS EVOLVING TO BLACK HOLES DURINGTWO-YEAR FOLLOW-UP C Enzinger, S Ropele, S Strasser-Fuchs, P Kapeller,T Seifert, B Poltrum, H Schmidt, R Schmidt, F Fazekas (Graz,Austria)
3:40 7 EVIDENCE FOR AXONAL PATHOLOGY AND ADAPTIVECORTICAL REORGANIZATION IN PATIENTS AT PRESENTATION WITHCLINICALLY ISOLATED SYNDROMES SUGGESTIVE OF MULTIPLE SCLE-ROSIS MA Rocca, D Mezzapesa,A Falini,A Ghezzi,V Martinelli, M Rodegher,G Scotti, G Comi, M Filippi (Milan, Italy)
3:55 8 A 36-MONTH LONGITUDINAL STUDY ON THE EVALUA-TION OF THE EFFECT OF INTERFERON BETA IN THE DURATION OFBLACK HOLES IN MULTIPLE SCLEROSIS F Bagnato, N Jeffries, J Ohayon,R Stone, N Richert, C Bash, HF McFarland, JA Frank (Bethesda, USA)
4:10 9 DOES FUNCTIONAL MRI ALLOW INFERENCES ABOUTCOGNITIVE TRAINING EFFICACY IN MULTIPLE SCLEROSIS? I Penner,L Kappos, M Rausch, K Opwis, E Radü (Basel, Switzerland)
4:25 10 COMBINATION THERAPY OF MS PATIENTS WITHINCOMPLETE RESPONSE TO INTERFERON-BETA WITH HUMANIZEDANTIBODY AGAINST THE INTERLEUKIN-2 RECEPTOR ALPHA CHAINB Bielekova, S Reichert-Scrivner, J Wuerfel, J Ohayon, J McCartin, N Richert, J Frank,T Waldmann, H McFarland, R Martin (Cambridge, UK)
5:05 CELLULAR ADHESION PATHWAYS: POTENTIAL TARGETS FORFUTURE MULTIPLE SCLEROSIS THERAPIES P Calabresi (Baltimore, USA)
5:25 EMERGING CLINICAL DATA FOR SELECTIVE ADHESIONMOLECULE INHIBITION IN THE TREATMENT OF MULTIPLE SCLEROSISD Miller (London, UK)
5:40 CLOSING REMARKS C Confavreux
5:50 PANEL DISCUSSION
Sponsored by the Division of Continuing Medical Education,Discovery International
Supported through an education grant from Biogen, Inc.and Elan
20
Thursday, September 19
8:15 am–9:30 am OPENING SESSIONGrand Ballroom I–X
8:15 am WELCOME K Johnson (Baltimore, USA) and A Thompson (London, UK)Opening Remarks Mike Dugan, General, USAF Ret.
President and CEO, National Multiple Sclerosis Society, New York, USAVictor Rivera, President, LACTRIMS
8:45 am KEYNOTE ADDRESS11 Inflammation, Demyelination and Axonal Loss: Unraveling the RelationshipsSK Ludwin★ (Kingston, Canada)
9:30 am BREAK
10:00 am–12:00 pm PARALLEL SESSIONS
SESSION IInflammation, Demyelination and Axonal Loss: Insights from Pathology
Co-chairs: C Polman (Amsterdam, Netherlands)E Radue (Basil, Switzerland)
Grand Ballroom I–V
10:00 12 MECHANISMS OF AXONAL LOSS BDTrapp★, C Bjartmar,J Peterson,A Chang, R Rudick (Cleveland, USA)
10:25 13 RELATIONSHIP BETWEEN INFLAMMATION ANDAXONAL LOSS W Brueck★ (Berlin, Germany)
10:50 14 DIFFERENTIAL GENE EXPRESSION ANALYSIS OF MULTI-PLE SCLEROSIS TISSUE: COMPARISON OF ACTIVE AND INACTIVELESIONS MP Mycko, R Papoian, U Boschert, CS Raine, KW Selmaj (Lodz,Poland)
11:00 15 MICROARRAY ANALYSIS OF NORMAL APPEARINGWHITE MATTER (NAWM) AND LESIONS IN SECONDARY PROGRESSIVEMS VERIFIES MS AS A GENERALIZED CNS DISEASE RL Lindberg,CJ De Groot, U Certa, R Ravid, F Hoffmann, L Kappos, D Leppert (Basel, Switzer-land)
11:10 16 MULTIPLE SCLEROSIS: EXPANDED CSF B CELLS ARE ALSOPRESENT IN THE BRAIN TISSUE N Goebels, H Weber, M Hofbauer,H Wekerle, R Hohlfeld (Munich, Germany)
11:20 17 HIGH VULNERABILITY OF HUMAN NEURONS TO T CELLCYTOTOXICITY:A NEW MODEL TO EXPLAIN NEURODEGENERATIONIN MULTIPLE SCLEROSIS F Giuliani,V Yong (Calgary, Canada)
11:30 18 LEUKEMIA INHIBITORY FACTOR LIMITS IMMUNE-MEDIATED DEMYELINATION BY ENHANCING OLIGODENDROCYTESURVIVAL H Butzkueven, J Zhang, M Soilu-Hanninen, PF Bartlett, TJ Kilpatrick(Parkville,Australia)
11:40 19 CILIARY NEUROTROPHIC FACTOR ENHANCES MYELINFORMATION:A NOVEL ROLE FOR CNTF AND CNTF-RELATED MOLE-CULES S Bruno, N Frederic, A Marie Stephane, Z Bernard, L Catherine (Paris,France)
11:50 CONCLUSIONS
SESSION IIImpact of Relapses on Disability;Natural History and Clinical Trials Data
Co-chairs: L Kappos (Basel, Switzerland)H Panitch (Burlington, USA)
Grand Ballroom VI–X
10:00 20 THE ROLE OF EXACERBATIONS IN PERSISTENT IMPAIR-MENT IN MS F Lublin★, G Cutter, M Baier (New York, USA)
10:20 21 RELAPSES ARE NOT AN IMPORTANT CAUSE OF DIS-ABILITY C Confavreux★ (Lyon, France)
10:40 PANEL DISCUSSION Moderator: K Kappos
11:00 22 ONSET OF CLINICAL BENEFIT OF GLATIRAMER(COPAXONE®) ACETATE IN PATIENTS WITH RELAPSING REMITTINGMULTIPLE SCLEROSIS (RRMS) KP Johnson, BR Brooks, CC Ford, A Goodman,JB Guarnaccia, RP Lisak, LW Myers, HS Panitch, AA Pruitt, N Kachuck, JS Wolinsky,and the Copolymer 1 MS Study Group (Baltimore, USA)
11:15 23 EFFECT OF EARLY INTERFERON TREATMENT ON CON-VERSION TO DEFINITE MULTIPLE SCLEROSIS: THE ETOMS STUDY—4-YEAR RESULTS G Comi, M Filippi, F Barkhof, L Durelli, G Edan, O Fernandez,H Hartung, P Seeldrayers, P Soelberg Sorensen, O Hommes (Turin, Italy)
11:30 24 NEUTRALIZING ANTIBODIES AGAINST INTERFERON(IFN)-BETA REDUCE THE CLINICAL EFFECT IN RELAPSING-REMITTINGMULTIPLE SCLEROSIS PS Sorensen, N Koch-Henriksen, C Ross, KM Clemme-sen, M Svenson, K Bendtzen, J Frederiksen, K Jensen, O Kristensen, T Petersen,E Stenager, (Copenhagen, Denmark)
11:45 25 THE SYLVIA LAWRY CENTRE FOR MULTIPLE SCLEROSISRESEARCH (SLCMSR): BACKGROUND AND PROGRESS REPORTJH Noseworthy and SLCMSR Staff, Scientific Oversight Committee and Working Groups (Rochester, USA)
21
★ Invited speaker
Thursday, September 19
12:00 pm–2:00 pm LUNCH and POSTER SESSION IHarborside Level
2:00 pm–4:00 pm PARALLEL SESSIONS
SESSION IIIInflammation, Demyelination and Axonal Loss: Insights from Imaging
Co-chairs: J Simon (Denver, USA)N Richert (Bethesda, USA)
Grand Ballroom I–V
2:00 26 RELATIONSHIP BETWEEN CONTRAST ENHANCINGLESIONS AND AXONAL LOSS JA Frank★ (Bethesda, USA)
2:20 27 IN VIVO MONITORING OF AXONS AND MYELIN INMULTIPLE SCLEROSIS Z Caramanos, DL Arnold★ (Montreal, Canada)
2:40 28 CAN WE IMAGE REMYELINATION? F Barkhof★ (Amster-dam, Netherlands)
3:00 29 WHAT IS NORMAL-APPEARING WHITE MATTER?R Grossman★ (San Francisco, USA)
3:20 30 BRAIN VOLUME CHANGES IN PATIENTS AT PRESENTA-TION WITH SUSPECTED MULTIPLE SCLEROSIS: RESULTS FROM THEETOMS STUDY G Comi, M Inglese, N De Stefano, S Smith, F Barkhof, L Durelli,G Edan, O Fernandez, HP Hartung, PM Matthews, P Seeldrayers, PS Sorensen,V Martinelli, OR Hommes, M Filippi (Milan, Italy)
3:30 31 PREDICTIVE VALUE OF INFRATENTORIAL LESIONS INPATIENTS WITH CLINICALLY ISOLATED SYNDROMES FOR LONGTERM DISABILITY A Minneboo, F Barkhof, CH Polman, BM Uitdehaag,D Knol, J A Castelijns (Amsterdam, Netherlands)
3:40 32 A 48-MONTH LONGITUDINAL STUDY ON THE RELA-TIONSHIP BETWEEN THE DURATION OF THE ENHANCEMENT IN AN ACTIVE LESION AND THE DURATION OF A BLACK HOLE INMULTIPLE SCLEROSIS F Bagnato, N Jeffries, J Ohayon, R Stone, JA Frank,HF McFarland (Bethesda, USA)
3:45 P133 THE EFFECT OF INTERFERON B-1B ON QUANTITIESDERIVED FROM MT MRI IN SECONDARY PROGRESSIVE MS M Inglese,J vanWaesberghe, M Rovaris, K Beckmann, F Barkhof, D Hahn, L Kappos, D Miller,C Polman, C Pozzilli, A Thompson,T Yousry, K Wagner, G Comi, M Filippi (Milan,Italy)
3:50 P40 ISOLATED SPINAL DEMYELINATING EVENTS WITHNORMAL BRAIN MRI: PROGRESSION TO MS, CLINICAL AND MRIFOLLOW UP R Milo,T Katz, J Corat-Simon (Ashkelon, Israel)
3:55 CONCLUSIONS
SESSION IVThe Blood-Brain-Barrier as a Target for Treatment
Co-chairs: S Dhib-Jalbut (Baltimore, USA)J Oger (Vancouver, Canada)
Grand Ballroom VI–X
2:00 33 ADHESION MOLECULES AND THEIR ROLE IN PATHO-GENESIS JP Antel★, K Biernacki, R Seguin, A Prat (Montreal, Canada)
2:20 34 CHEMOKINES AND CHEMOKINE RECEPTORS:WHAT’STHE ATTACTION RM Ransohoff★ (Cleveland, USA)
2:40 35 MATRIX METALLOPROTEINASES IN MS VW Yong★(Calgary, Canada)
3:00 36 CLINICAL TRIALS OF AGENTS TARGETING THE BLOODBRAIN BARRIER: SUCCESSES AND FAILURES D Miller★ (London, UK)
3:20 P143 RANTES AND CHEMOKINE RECEPTOR 5 POLYMOR-PHISMS: SUSCEPTIBILITY TO AND OUTCOME IN MULTIPLE SCLEROSISJM Partridge, A Fryer,W Ollier, M Boggild, R Strange, C Hawkins (Stoke-on-Trent,UK)
3:25 P145 MMP-9 MICROSATELLITE POLYMORPHISM INCREASESTHE RISK OF MULTIPLE SCLEROSIS N Fiotti, R Zivadinov, N Altamura,D Nasuelli, A Bratina, MA Tommasi, A Bosco, L Locatelli, A Grop, G Cazzato,C Giansante, M Zorzon (Trieste, Italy)
3:30 P114 IL-12 DEPENDENT/IFN GAMMA INDEPENDENTEXPRESSION OF CCR5 BY MYELIN-REACTIVE CD4+ T CELLSCORRELATES WITH ENCEPHALITOGENICITY L Bagaeva, LP Williams, BMSegal (Rochester, USA)
3:35 P91 LONGITUDINAL ANALYSIS OF CSF EXPANDED CD8+CLONOTYPES IN THE PERIPHERAL BLOOD OF MULTIPLE SCLEROSISPATIENTS S Cepok, D Zhou, F Vogel, N Sommer, B Hemmer (Marburg,Germany)
3:40 P98 MOLECULAR TRACKING OF MYELIN BASIC PROTEIN-SPECIFIC T CELL EXPANSION IN MULTIPLE SCLEROSIS PA Muraro,K Wandinger, B Bielekova, HF McFarland, R Martin (Bethesda, USA)
3:45 P149 IMMUNE REGULATORY EFFECTS OF GLATIRAMERACETATE (GA) ON HUMAN MONOCYTES: BYSTANDER SUPPRESSIONREVISITED? H Kim, M Duddy, A Bar-Or (Montreal, Canada)
3:50 CONCLUSIONS
22
★ Invited speaker
Thursday, September 19
SATELLITE SYMPOSIA
7:30 pm–10:30 pm RECEPTION and DINNER BUFFET
National Aquarium in Baltimore
6:00 pm–7:00 pm
SATELLITE SYMPOSIUM IIIDefining Factors That Impact Efficacy in the Treatment of Relapsing RemittingMultiple Sclerosis
Program Chair: HP Hartung (Dusseldorf, Germany)
Panel Discussion Chair: H McFarland (Washington,DC, USA)
Grand Ballroom VI–X
6:00 WELCOMING REMARKS/INTRODUCTIONS HP Hartung
6:05 SELECTING HIGH-RISK PATIENTS FOR EARLY TREATMENTF Munschauer (Buffalo, USA)
6:15 DO DOSE AND DOSE FREQUENCY IMPACT EFFICACY? A REVIEW OF THE EUROPEAN DOSE COMPARISON STUDY AND SUPPORTING DATA X Montalban (Barcelona, Spain)
Sponsored by the Health Science Center for Continuing Medical Education
Supported by an unrestricted educational grant from Biogen
4:30 pm–5:30 pm
SATELLITE SYMPOSIUM IIExploring the Boundaries of Multiple Sclerosis Treatment
Chair: D Goodin (San Francisco, USA)
Grand Ballroom I–V
4:30 WELCOME D Goodin
4:35 EXPLORING TREATMENT OPTIONS FOR PRIMARY PROGRES-SIVE MULTIPLE SCLEROSIS X Montalban (Barcelona, Spain)
4:50 LONG TERM EXPERIENCE WITH MULTIPLE SCLEROSIS THERA-PIES G Rice (London, Canada)
5:05 BEYOND THE STANDARD DOSE OF BETA INTERFERON INMULTIPLE SCLEROSIS HP Hartung (Dusseldorf, Germany)
5:20 DISCUSSION AND CLOSING REMARKS D Goodin
Sponsored by Bio-Medical Communications, Inc.
Supported by an unrestricted educational grant fromSchering AG, Germany / Berlex
23
Friday, September 20
8:30 am–9: 30 am OPENING SESSIONGrand Ballroom I–X
8:30 am WELCOME S Dhib-Jalbut (Baltimore, USA)PRESENTATION: ACTRIMS LIFE ACHIEVEMENT AWARD Kenneth P. Johnson, Honoree
8:45 am KEYNOTE ADDRESS37 Neural Stem Cells to Rebuild the Diseased Brain: How Realistic Is This Approach?E Snyder★ (Boston, USA)
9:30 am BREAK
10:00 am–12:00 pm PARALLEL SESSIONS
SESSION V
Neuroprotection
Co-chairs: A Cross (St Louis, USA)R Lisak (Detroit, USA)
Grand Ballroom I–V
10:00 38 MOLECULAR BASIS OF LIMITED REMYELINATION INMULTIPLE SCLEROSIS CS Raine★, G John, CF Brosnan (Bronx, USA)
10:25 39 COMPLEMENT: DUAL ROLE IN INJURY AND PROTEC-TION ML Shin★, H Rus (Baltimore, USA)
10:50 40 IS NEUROPROTECTION A REALISTIC OPTION IN MS?R Hohlfeld★ (Munich, Germany)
11:15 41 CNTF IS A MAJOR PROTECTIVE FACTOR IN DEMYELI-NATING CNS DISEASE:A NEUROTROPHIC CYTOKINE AS MODULA-TOR IN NEUROINFLAMMATION RA Linker, M Maurer, S Gaupp, R Martini,B Holtmann, H Lassmann, KV Toyka, M Sendtner, R Gold (Wurzburg, Germany)
11:30 42 INTERFERON-BETA GENE THERAPY FOR CENTRALNERVOUS SYSTEM DISEASE USING BONE MARROW CELLS AS ADELIVERY SYSTEM S Dhib-Jalbut,TK Makar, S Wilt, Z Dong, P Fishman,M Mouradian (Baltimore, USA)
11:45 43 HIGH-DOSE IMMUNOABLATIVE THERAPY WITHAUTOLOGOUS STEM CELL SUPPORT IN PATIENTS WITH MALIGNANTCOURSE OF MULTIPLE SCLEROSIS E Havrdova, T Kozak, J Kobylka, J Pitha,J Fiedler, V Koza, J Maaloufova, D Horakova, V Ticha, I Novakova, S Vodvarkova,E Gregora, E Medova (Prague, Czech Republic)
SESSION VI
Hot topics in Neuroimmunology
Co-chairs: M Racke (Dallas, USA)J Richert (Washington, DC, USA)
Grand Ballroom VI–X
10:00 44 CYTOKINE REGULATION IN MULTIPLE SCLEROSISHWeiner★, SJ Khoury (Boston, USA)
10:25 45 ARE SPECIFIC IMMUNOTHERAPIES AN OPTION FOR MS?R Martin★ (Bethesda, USA)
10:50 46 TCR PEPTIDE THERAPY IN AUTOIMMUNE DISEASEAAVandenbark★ (Portland, USA)
11:15 47 LARGE SCALE TRANSCRIPTIONAL AND PROTEOMICANALYSIS OF MS TISSUE YIELDS NEW TARGETS FOR THERAPYL Steinman★ (Stanford, USA)
11:40 48 RE-INDUCTION OF TOLERANCE IN ESTABLISHEDAUTOIMMUNE DISEASE:A STRATEGY FOR THE TREATMENT OFMULTIPLE SCLEROSIS G Pryce, JK O’Neill, S Amor, D Baker, G Giovannoni(London, UK)
11:50 49 KV1.3 IS A UNIQUE FUNCTIONAL MARKER OF EFFEC-TOR MEMORY T CELLS IN MULTIPLE SCLEROSIS R Allie, S Yun, PA Cala-bresi, H Wullf, K Chandy, M Pennington (Baltimore, USA)
★ Invited speaker
24
Friday, September 20
12:00 pm–2:00 pm LUNCH and POSTER SESSION IIHarborside Level
2:00 pm–4:00 pm PARALLEL SESSIONS
SESSION VIIMethodological Issues in Clinical Trials
Co-chairs: HP Hartung (Dusseldorf, Germany)R Rudick (Cleveland, USA)
Grand Ballroom I–V
2:00 50 THE NEW DIAGNOSTIC CRITERIA AND THEIR IMPLICA-TIONS FOR CLINICAL TRIALS JSWolinsky★ (Houston, USA)
2:25 51 APPLICATION OF MCDONALD CRITERIA TO CLINICALLYISOLATED SYNDROMES SUGGESTIVE OF MULTIPLE SCLEROSISM Tintore,A Rovira, J Rio, C Nos, E Grive, J Sastre-Garriga, I Pericot, E Sanchez,M Comabella, X Montalban (Barcelona, Spain)
2:35 52 METHODOLOGICAL ISSUES IN SHORT-TERM CLINICALTRIALS JH Noseworthy★ (Rochester, USA)
3:00 53 THE ROLE OF MRI AS A SURROGATE MARKER IN MSH McFarland★ (Bethesda, USA)
3:25 54 A STANDARDIZED MRI SCAN IN THE DIAGNOSIS ANDFOLLOW-UP OF MS PATIENTS D Paty★, DK Li,A Traboulsee, J Simon, J Frank(Vancouver, Canada)
3:50 P227 COURSE AND PROGNOSIS IN EARLY ONSET MULTI-PLE SCLEROSIS IL Simone, D Carrara, C Tortorella, M Liguori,V Lepore, F Pelli-grini,A Bellacosa,A Ceccarelli, I Pavone, F Girolamo, P Livrea (Bari, Italy)
3:55 P308 PLACEBO-CONTROLLED DOUBLE-BLINDED DOSERANGING STUDY OF FAMPRIDINE-SR IN MULTIPLE SCLEROSISAD Goodman,A Blight, JA Cohen,AH Cross, M Katz, MA Rizzo,T Vollmer(Rochester, USA)
SESSION VIIIGenetics and Hormonal Influence
Co-chairs: M Freedman (Ottawa, Canada)D Hafler (Boston, USA)
Grand Ballroom VI–X
2:00 55 GENETIC ANALYSIS OF MULTIPLE SCLEROSIS IN EURO-PEANS (GAMES) A Compston★, S Sawcer (Cambridge, UK)
2:20 56 INSIGHTS INTO THE GENETICS OF MS FROM THE CANA-DIAN COLLABORATIVE PROJECT GC Ebers★, D Sadovnick, N Risch(Vancouver, Canada)
2:40 57 THE ROLE OF THE HLA REGION IN MULTIPLE SCLEROSISS Hauser★, LF Barcellos, MA Pericak-Vance, JL Haines, RR Lincoln, S Schmidt,A Swerdlin, JR Oksenberg (Durham, USA)
3:00 58 HORMONAL INFLUENCES IN MS RVoskuhl★ (Los Angeles,USA)
3:20 59 OVARIAN HORMONES DIFFERENTIALLY EFFECT NEURONDEATH MEDIATED BY TNF� VIA EXPRESSION OF ANTI-APOPTOTICPROTEINS AND ACTIVATION OF JNK1 PRO-APOPTOTIC SIGNALCASCADE CL Koski, S Hila,T Popescue, G Hoffman (Baltimore, USA)
3:30 60 A NEW GENE OVEREXPRESSED IN MULTIPLE SCLEROSISAND RHEUMATOID ARTHRITIS C Greene, R Crusio, L Chen, C Rose,D Connelly, M Grekova, JR Richert (Washington, USA)
3:40 P325 ASSOCIATION OF APOLIPOPROTEIN E AND MYELO-PEROXIDASE GENOTYPES WITH THE CLINICAL COURSE OF FAMILIALAND SPORADIC MULTIPLE SCLEROSIS B Zakrzewska-Pniewska,A Podlecka, M Styczynska, R Samocka, B Peplonska, M Barcikowska,H Kwiecinski (Warsaw, Poland)
3:45 P314 TUMOR NECROSIS FACTOR RECEPTOR II POLYMOR-PHISM IN PATIENTS WITH MULTIPLE SCLEROSIS R Ehling, C Gassner,F Fazekas, H Kollegger,W Kristoferitsch, M Reindl, T Berger (Innsbruck,Austria)
3:50 P297 A SYNTHETIC ANDROSTENE DERIVATIVE WITHOUTGENDER-RELATED SIDE EFFECTS INHIBITS EAE. CANDIDATE FORCLINICAL TRIALS IN MS? H Offner,A Zamora,A Matejuk, D Auci, E Morgan,C Reading (Portland, USA)
3:55 CONCLUSIONS
★ Invited speaker
25
Friday, September 20
SATELLITE SYMPOSIA
7:30 pm–10:00 pm RECEPTION and DINNER BUFFETB&O Railroad Museum
6:00 pm–7:00 pm
SATELLITE SYMPOSIUM VThe Modern Management of Multiple Sclerosis:An Evidence-Based Approach
Chair: D Bates (Newcastle, UK)
Grand Ballroom VI–X
6:00 A CRITICAL ANALYSIS OF DISEASE-MODIFYING DRUGS INCLINICAL STUDIES: IMPLICATIONS AND TREATMENT GUIDELINESD Goodin (San Francisco, USA)
6:15 THE EVIDENCE FOR EFFICACY OF DISEASE-MODIFYINGDRUGS: IMPLICATIONS FOR THE CLINICIAN M Freedman (Ottawa,Canada)
6:35 THE PATIENT PERSPECTIVE: LIVING WITH MULTIPLE SCLEROSISAFTER STARTING A DISEASE-MODIFYING DRUG
6:50 Q&A AND CLOSING REMARKS
Sponsored by Serono
4:30 pm–5:30 pm
SATELLITE SYMPOSIUM IVMilestones in Immunomodulatory Therapy:Decisions in the Treatment of Multiple Sclerosis
Co-chairs: G Comi (Milan, Italy)J Wolinsky (Houston, USA)
Grand Ballroom I–V
4:30 IMMUNE-MEDIATED INJURY AND NEUROPROTECTION IN MSW Yong (Calgary, Canada)
4:50 LESSONS FROM MRI: EVIDENCE OF EARLY AND PROGRESSIVECNS INJURY D Arnold (Montreal, Canada)
5:10 GLATIRAMER ACETATE IN MS:A NEW LOOK AT THE CLINICALEFFECTS IN THE LIGHT OF MECHANISMS OF ACTION R Lisak (Detroit,USA)
Sponsored by Postgraduate Institute for Medicine
Supported by an unrestricted educational grant from Teva Pharmaceuticals, LTD,Teva Neuroscience, and Aventis
26
Saturday, September 21
8:30 am–10:30 am PARALLEL SESSIONS
SESSION XLate Breaking NewsCo-chairs: P O’Connor (Toronto, Canada)
A Thompson (London, UK)Grand Ballroom VI–X
8:30 WELCOME P O’Connor
8:45 LB1 VALIDATION OF DIAGNOSTIC MRI CRITERIA FOR MSAND RESPONSE TO TREATMENT WITH INTERFERON-BETA-1A FBarkhof, M Rocca, G Francis, J van Waesberghe, B Uitdehaag, O Hommes, H Har-tung, L Durelli, G Edan, O Fernández, P Seeldrayers, P Sorenson, S Margrie, GComi, M Filippi (Milan, Italy)
9:00 LB2 ANTI-MOG ANTIBODIES PREDICT EARLY CONVERSIONTO CLINICALLY DEFINITE MS IN PATIENTS WITH A FIRST DEMYELINAT-ING EVENT. T Berger, P Rubner, F Schautzer, R Egg, H Ulmer, I Mayringer, EDilitz, F Deisenhammer, M Reindl (Innsbruck,Austria)
9:15 LB3 NEUROREHABILITATION IN MULTIPLE SCLEROSISCONTRIBUTES TO FUNCTIONAL RECOVERY ACCOMPANIED BYCHANGES OF BRAIN ACTIVITY ON FMRI—PRELIMINARY RESULTS.K Rasova, J Krasensky, E Havrdova, J Obenberger, M Zalisova, Z Seidl (Prague,Czech Republic)
9:30 LB4 TIGHT JUNCTION ABNORMALITY IN MS AFFECTS ALLCALIBRES OF VESSEL AND CORRELATES WITH LESION ACTIVITY. J Kirk,J Plumb, M Mirakhur, S McQuaid (Belfast, UK)
9:45 LB5 SINGLE CENTRE, DBPC, RANDOMISED TRIAL OFINTERFERON� 1B IN PRIMARY PROGRESSIVE AND TRANSITIONALPROGRESSIVE MULTIPLE SCLEROSIS:AN EXPLORATORY PHASE IISTUDY. X Montalban, L Brieva, M Tintore, C Borras, J Rio, C Nos, X Aymerich,J Alonso, R Horno, M Vicente,A Rovira (Barcelona, Spain)
10:00 LB6 SUCCESSFUL TREATMENT WITH IFN-�1B IN RR MSPATIENTS IS ASSOCIATED WITH AN INCREASE IN THE NUMBER OF IL-10 PRODUCING (REGULATORY) CD4 +T CELLS. A van Boxel-Dezaire, MSmits, B Uitdehaag, C Polman, L Nagelkerken (Leiden, Netherlands)
10:15 LB7 MULTIPLE SCLEROSIS DOCUMENTATION SYSTEM—MSDS 2.0 M Eulitz,T Kugel, PA Muraro, M Pette (Dresden, Germany)
SESSION IXLong Term Management Issues in MultipleSclerosisCo-chairs: C Bever (Baltimore, USA)
J Cohen (Cleveland, USA)Grand Ballroom I–V
8:30 WELCOME C Bever
8:45 61 NEUROPSYCHOLOGICAL ASPECTS OF MULTIPLE SCLE-ROSIS A Feinstein★ (Toronto, Canada)
9:05 62 PATHOPHYSIOLOGY OF MS FATIGUE G Comi★, L Leocani,P Rossi, B Colombo (Milan, Italy)
9:25 63 STEREOTACTIC SURGERY EB Montgomery★ (Cleveland,USA)
9:45 64 CHILDHOOD ONSET MULTIPLE SCLEROSIS (THE KID-MUS STUDY): NATURAL HISTORY AND PROGNOSTIC FACTORS INTHE LYON COHORT C Renoux,Y Mikaeloff, S Vukusic, L Gignoux, F Durand-Dubief, I Achiti, C Confavreux (Lyon, France)
9:55 65 DISEASE-MODIFYING DRUGS FOR MULTIPLE SCLEROSIS.CAN TREATMENT FAILURES BE PREDICTED? M Johnson, H Ford, S Den-ton (Leeds, UK)
10:05 66 GADOLINIUM ENHANCING LESIONS AS A SURROGATEMARKER OF INTERFERON RESPONSE RA Rudick, G Cutter, M Baier, DDougherty, B Weinstock-Guttman, M Mass, E Fisher, DM Miller,A Sandrock, JSimon (Cleveland, USA)
10:15 67 MITOXANTRONE (NOVANTRONE) FOR TREATMENTOF RECURRENT NEUROMYELITIS OPTICA BWeinstock-Guttman, JFeichter, R Bakshi, C Brownscheidle, N Lincoff (Buffalo, USA)
7:00 pm–10:00 pm COMMITTEE RECEPTIONBaltimore Museum of Industry (by invitation)
★ Invited speaker
27
Consistent. Convenient. Complete.
COPAXONE® PRE-FILLED SYRINGE
COPAXONE® is indicated for the reduction of relapses in relapsing-remitting multiple sclerosis.Please see brief summary of prescribing information on next page.COPAXONE® is a registered trademark of Teva Pharmaceutical Industries Ltd.
The only MS therapy with■ A presumed mechanism of action that distinguishes it
from interferons1,2
■ No evidence of neutralizing antibodies3
■ No recommended monitoring of liver function or complete blood count4
■ Pregnancy Category B rating4
Significant relapse rate reduction■ Long-term efficacy demonstrated over 2 years5,6
■ Efficacy confirmed in 4 additional studies7-10
Reduction in Gd-enhancing lesions■ 35% reduction in median cumulative number of lesions
vs placebo11
Safety and tolerability you can count on■ No increase in incidence of flu-like symptoms,
depression, or fatigue when compared to placebo4
■ Most common adverse effects in controlled trials were injection site reactions, vasodilatation, chest pain, asthenia,infection, pain, nausea, arthralgia, anxiety, and hypertonia
■ About 10% of patients experienced an immediate postinjectionreaction (flushing, chest pain, palpitations, anxiety, dyspnea,throat constriction, and urticaria). The symptoms were transientand self-limited, and did not require specific treatment
■ Transient chest pain was noted in 26% of COPAXONE®
patients (vs 10% placebo); no long-term sequelae
COPAXONE®
(glatiramer acetate injection)Brief Summary of Prescribing Information
INDICATIONS AND USAGECOPAXONE® Injection is indicated for reduction of the frequency of relapses in patients with Relapsing-Remitting Multiple Sclerosis.
CONTRAINDICATIONSCOPAXONE® Injection is contraindicated in patients with known hypersensitivity to glatiramer acetate ormannitol.
WARNINGSThe only recommended route of administration of COPAXONE® Injection is the subcutaneous route.COPAXONE® Injection should not be administered by the intravenous route.
PRECAUTIONSGeneralPatients should be instructed in self-injection techniques to assure the safe administration of COPAXONE®
Injection (see PRECAUTIONS: Information for Patients and the COPAXONE® INJECTION PATIENTINFORMATION Leaflet). Current data indicate that no special caution is required for patients operating anautomobile or using complex machinery.
Considerations Regarding the Use of a Product Capable of Modifying Immune Responses Because glatiramer acetate can modify immune response, it could possibly interfere with useful immunefunctions. For example, treatment with glatiramer acetate might, in theory, interfere with the recognition offoreign antigens in a way that would undermine the body’s tumor surveillance and its defenses againstinfection. There is no evidence that glatiramer acetate does this, but there has as yet been no systematicevaluation of this risk. Because glatiramer acetate is an antigenic material, it is possible that its use may leadto the induction of host responses that are untoward, but systematic surveillance for these effects has not beenundertaken.
Although glatiramer acetate is intended to minimize the autoimmune response to myelin, there is thepossibility that continued alteration of cellular immunity due to chronic treatment with glatiramer acetatemight result in untoward effects.
Glatiramer acetate-reactive antibodies are formed in practically all patients exposed to daily treatment with therecommended dose. Studies in both the rat and monkey have suggested that immune complexes are depositedin the renal glomeruli. Furthermore, in a controlled trial of 125 RR MS patients given glatiramer acetate,20 mg, subcutaneously every day for 2 years, serum IgG levels reached at least 3 times baseline values in 80%of patients by 3 months of initiation of treatment. By 12 months of treatment, however, 30% of patients stillhad IgG levels at least 3 times baseline values, and 90% had levels above baseline by 12 months. Theantibodies are exclusively of the IgG subtype-and predominantly of the IgG-1 subtype. No IgE type antibodiescould be detected in any of the 94 sera tested; nevertheless, anaphylaxis can be associated with theadministration of most any foreign substance, and therefore, this risk cannot be excluded.
Information for PatientsTo assure safe and effective use of COPAXONE® Injection, the following information and instructions shouldbe given to patients:
1. Inform your physician if you are pregnant, if you are planning to have a child, or if you become pregnantwhile taking this medication.
2. Inform your physician if you are nursing.
3. Do not change the dose or dosing schedule without consulting your physician.
4. Do not stop taking the drug without consulting your physician.
Patients should be instructed in the use of aseptic techniques when administering COPAXONE® Injection.Appropriate instructions for the self-injection of COPAXONE® Injection should be given, including a careful review of the COPAXONE® INJECTION PATIENT INFORMATION Leaflet. The first injectionshould be performed under the supervision of an appropriately qualified health care professional. Patientunderstanding and use of aseptic self-injection techniques and procedures should be periodically reevaluated.Patients should be cautioned against the reuse of needles or syringes and instructed in safe disposalprocedures. They should use a puncture-resistant container for disposal of used needles and syringes. Patientsshould be instructed on the safe disposal of full containers according to local laws.
Awareness of Adverse Reactions: Physicians are advised to counsel patients about adverse reactionsassociated with the use of COPAXONE® Injection (see ADVERSE REACTIONS section). In addition,patients should be advised to read the COPAXONE® INJECTION PATIENT INFORMATION Leaflet andresolve any questions regarding it prior to beginning COPAXONE® Injection therapy.
Laboratory TestsData collected during premarketing development do not suggest the need for routine laboratory monitoring.
Drug InteractionsInteractions between COPAXONE® Injection and other drugs have not been fully evaluated. Results fromexisting clinical trials do not suggest any significant interactions of COPAXONE® Injection with therapiescommonly used in MS patients, including the concurrent use of corticosteroids for up to 28 days.COPAXONE® Injection has not been formally evaluated in combination with Interferon beta.
Drug/Laboratory Test InteractionsNone are known.
Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenesisIn a two-year carcinogenicity study, mice were administered up to 60 mg/kg/day glatiramer acetate bysubcutaneous injection (up to 15 times the human therapeutic dose on a mg/m2 basis). No increase in systemicneoplasms was observed. In males of the high dose group (60 mg/kg/day), but not in females, there was anincreased incidence of fibrosarcomas at the injection sites. These sarcomas were associated with skin damageprecipitated by repetitive injections of an irritant over a limited skin area.
In a two-year carcinogenicity study, rats were administered up to 30 mg/kg/day glatiramer acetate bysubcutaneous injection (up to 15 times the human therapeutic dose on a mg/m2 basis). No increase in systemicneoplasms was observed.
MutagenesisGlatiramer acetate was not mutagenic in four strains of Salmonella typhimurium and two strains ofEscherichia coli (Ames test) or in the in vitro mouse lymphoma assay in L5178Y cells. Glatiramer acetate wasclastogenic in two separate in vitro chromosomal aberration assays in cultured human lymphocytes; it was notclastogenic in an in vivo mouse bone marrow micronucleus assay.
Impairment of FertilityIn a multigeneration reproduction and fertility study in rats, glatiramer acetate at subcutaneous doses of up to36 mg/kg (18 times the human therapeutic dose on a mg/m2 basis) had no adverse effects on reproductiveparameters.
PregnancyPregnancy Category B. No adverse effects on embryofetal development occurred in reproduction studies inrats and rabbits receiving subcutaneous doses of up to 37.5 mg/kg of glatiramer acetate during the period oforganogenesis (18 and 36 times the therapeutic human dose on a mg/m2 basis, respectively). In a prenatal andpostnatal study in which rats received subcutaneous glatiramer acetate at doses of up to 36 mg/kg from day 15 of pregnancy throughout lactation, no significant effects on delivery or on offspring growth anddevelopment were observed.
There are no adequate and well-controlled studies in pregnant women. Because animal reproduction studiesare not always predictive of human response, glatiramer acetate should be used during pregnancy only ifclearly needed.
Labor and DeliveryIn a prenatal and postnatal study, in which rats received subcutaneous glatiramer acetate at doses of up to36 mg/kg from day 15 of pregnancy throughout lactation, no significant effects on delivery were observed.The relevance of these findings to humans is unknown.
Nursing MothersIt is not known whether glatiramer acetate is excreted in human milk. Because many drugs are excreted inhuman milk, caution should be exercised when COPAXONE® is administered to a nursing woman.
Pediatric UseThe safety and efficacy of COPAXONE® Injection have not been established in individuals under 18 years ofage.
Use in the ElderlyCOPAXONE® Injection has not been studied specifically in elderly patients.
Use in Patients with Impaired Renal FunctionThe pharmacokinetics of glatiramer acetate in patients with impaired renal function have not been determined.
ADVERSE REACTIONSDuring premarketing clinical trials approximately 900 individuals received at least one dose of glatirameracetate.
In controlled clinical trials the most commonly observed adverse experiences associated with the use ofglatiramer acetate and not seen at an equivalent frequency among placebo-treated patients were: injection sitereactions, vasodilatation, chest pain, asthenia, infection, pain, nausea, arthralgia, anxiety, and hypertonia.
Approximately 8% of the 893 subjects receiving glatiramer acetate discontinued treatment because of anadverse reaction. The adverse reactions most commonly associated with discontinuation were: injection sitereaction (6.5%), vasodilatation, unintended pregnancy, depression, dyspnea, urticaria, tachycardia, dizziness,and tremor.
Immediate Post-Injection ReactionApproximately 10% of MS patients exposed to glatiramer acetate in premarketing studies experienced aconstellation of symptoms immediately after injection that included flushing, chest pain, palpitations, anxiety,dyspnea, constriction of the throat, and urticaria. In clinical trials, the symptoms were generally transient andself-limited and did not require specific treatment. In general, these symptoms have their onset several monthsafter the initiation of treatment, although they may occur earlier, and a given patient may experience one orseveral episodes of these symptoms. Whether or not any of these symptoms actually represent a specificsyndrome is uncertain. During the postmarketing period, there have been reports of patients with similarsymptoms who received emergency medical care.
Whether an immunologic or non-immunologic mechanism mediates these episodes, or whether several similarepisodes seen in a given patient have identical mechanisms, is unknown.
Chest PainApproximately 21% of glatiramer acetate patients in the pre-marketing controlled studies (compared to 11%of placebo patients) experienced at least one episode of what was described as transient chest pain. Whilesome of these episodes occurred in the context of the Immediate Post-Injection Reaction described above,many did not. The temporal relationship of this chest pain to an injection of glatiramer acetate was not alwaysknown. The pain was transient (usually lasting only a few minutes), often unassociated with other symptoms,and appeared to have no important clinical sequelae. There has been only one episode of chest pain duringwhich a full EKG was performed; that EKG showed no evidence of ischemia. Some patients experienced morethan one such episode, and episodes usually began at least 1 month after the initiation of treatment. Thepathogenesis of this symptom is unknown.
Incidence in Controlled Clinical Studies: The following table lists treatment-emergent signs and symptomsthat occurred in at least 2% of MS patients treated with glatiramer acetate in the pre-marketing placebo-controlled trials. These signs and symptoms were numerically more common in patients treated withglatiramer acetate than in patients treated with placebo. These trials include the first two controlled trials inRR MS patients and a controlled trial in patients with Chronic-Progressive MS. Adverse reactions wereusually mild in intensity.
The prescriber should be aware that these figures cannot be used to predict the frequency of adverseexperiences in the course of usual medical practice where patient characteristics and other factors may differfrom those prevailing during clinical studies. Similarly, the cited frequencies cannot be directly compared withfigures obtained from other clinical investigations involving different treatments, uses, or investigators. Aninspection of these frequencies, however, does provide the prescriber with one basis on which to estimate therelative contribution of drug and nondrug factors to the adverse reaction incidences in the population studied.
Controlled Trials in Patients with Multiple Sclerosis:Incidence of Glatiramer Acetate Adverse Reactions 2%
and More Frequent than Placebo
3815411101717481930111038602425
282410
71114174
66
Body as a WholeAstheniaBack PainBacterial InfectionChest PainChillsCystFace EdemaFeverFlu SyndromeInfectionInjection Site ErythemaInjection Site HemorrhageInjection Site IndurationInjection Site InflammationInjection Site MassInjection Site PainInjection Site PruritusInjection Site UrticariaInjection Site WeltNeck PainPain
Urogenital System: Urinary tract infection, urinary frequency, urinary incontinence, urinary retention, dysuria,cystitis, metrorrhagia, breast pain, and vaginitis.
Data on adverse reactions occurring in the controlled clinical trials were analyzed to evaluate differences basedon sex. No clinically significant differences were identified. Ninety-two percent of patients in these clinicaltrials were Caucasian. This percentage reflects the racial composition of the MS population. In addition, thevast majority of patients treated with COPAXONE® were between the ages of 18 and 45. Consequently, dataare inadequate to perform an analysis of the adverse reaction incidence related to clinically relevant agesubgroups.
Laboratory analyses were performed on all patients participating in the clinical program for glatiramer acetate.Clinically significant laboratory values for hematology, chemistry, and urinalysis were similar for bothglatiramer acetate and placebo groups in blinded clinical trials. No patient receiving glatiramer acetatewithdrew from any trial because of abnormal laboratory findings.
Other Adverse Events Observed During Clinical TrialsGlatiramer acetate was administered to 979 individuals during premarketing clinical trials, only some of whichwere placebo-controlled. During these trials, all adverse events were recorded by the clinical investigators,using terminology of their own choosing. To provide a meaningful estimate of the proportion of individualshaving adverse events, similar types of events were grouped into standardized categories using COSTARTdictionary terminology. All reported events occurring at least twice and potentially important events occurringonce are listed below, except those already listed in the previous table, those too general to be informative,trivial events, and other reactions which occurred in at least 2% of treated patients and were present at equalor greater rates in the placebo group. Additional adverse reactions reported during the post-marketing periodare included.
Events are further classified within body system categories and listed in order of decreasing frequency usingthe following definitions: Frequent adverse events are defined as those occurring in at least 1/100 patients;Infrequent adverse events are those occurring in 1/100 to 1/1000 patients; Rare adverse events are thoseoccurring in less than 1/1000 patients.
Body as a Whole: Frequent: Injection site edema, injection site atrophy, abscess, injection site hypersensitivity. Infrequent: Injection site hematoma, injection site fibrosis, moon face, cellulitis, generalized edema,
hernia, injection site abscess, serum sickness, suicide attempt, injection site hypertrophy, injectionsite melanosis, lipoma, and photosensitivity reaction.
Special Senses: Frequent: Visual field defect. Infrequent: Dry eyes, otitis externa, ptosis, cataract, corneal ulcer, mydriasis, optic neuritis,
photophobia, and taste loss.Urogenital:
Frequent: Amenorrhea, hematuria, impotence, menorrhagia, suspicious papanicolaou smear,urinary frequency and vaginal hemorrhage.
Infrequent: Vaginitis, flank pain (kidney), abortion, breast engorgement, breast enlargement,carcinoma in situ cervix, fibrocystic breast, kidney calculus, nocturia, ovarian cyst, priapism,pyelonephritis, abnormal sexual function, and urethritis.
Postmarketing Clinical ExperiencePostmarketing experience has shown an adverse event profile similar to that presented above. Reports ofadverse reactions occurring under treatment with COPAXONE® (glatiramer acetate for injection) notmentioned above that have been received since market introduction and that may have or not have causalrelationship to the drug include the following:
Body as a Whole: sepsis; LE syndrome; hydrocephalus; enlarged abdomen; injection site hypersensitivity;allergic reaction; anaphylactoid reaction
References: 1. Data on file. Teva Neuroscience, Inc. 2. Neuhaus O, Farina C, Wekerle H, et al.Neurology. 2001;56:702-708. 3. Duda PW, Schmied MC, Cook SL, et al. J Clin Invest.2000;105(7):967-976. 4. Johnson KP, the U.S. Phase III Copolymer 1 Study Group, Teitelbaum D,et al. Ann Neurol. 1995;38(6):973. 5. COPAXONE® prescribing information. Teva Neuroscience, Inc.6. Johnson KP, Brooks BR, Cohen JA, et al. Neurology. 1995;45(7):1268-1276. 7. Bornstein MB,Miller A, Slagle S, et al. N Engl J Med. 1987;317:408-414. 8. Comi G, Filippi M, Wolinsky JS, et al.Ann Neurol. 2001;49(3):290-297. 9. Khan OA, Tselis AC, Kamholz JA, et al. Multiple Sclerosis.2001;7:349-353. 10. Mancardi GL, Sardanelli F, Parodi RC, et al. Neurology. 1998;50:1127-1133.11. Miller A, Shapiro S, Gershtein R, et al. J Neuroimmunol. 1998;92:113-121.
The Steering Committee acknowledges the exhibitors’ participation in ACTRIMS-ECTRIMS 2002. Stopby and visit exhibitors during the following hours:
Wednesday, September 18 from 1 pm–5 pmThursday, September 19 from 8 am–5 pmFriday, September 20 from 8 am–5 pm
GOLD SPONSOR EXHIBITORS
Biogen Booth 12Biogen, Inc., winner of the US National Medal of Technology, is the world's oldest independent biotechnologycompany and a recognized leader in the field of multiple sclerosis research. Biogen produces and marketsAVONEX® (Interferon beta-1a), the leading treatment for relapsing forms of multiple sclerosis.
Biogen/Elan Booth 13Biogen, Inc. and Elan Corporation have established a worldwide, collaboration to develop, manufacture, and com-mercialize Antegren® (natalizumab), the first Selective Adhesion Molecule (SAM) Inhibitor. Natalizumab, a human-ized monoclonal antibody binds to the cell surface receptors known as alpha-4-beta-1 (VLA-4) and alpha-4-beta-7 integrins, which are believed to play an important role in the trafficking of mononuclear cells, such aslymphocytes, into sites of inflammation. Natalizumab is currently in Phase III clinical trials for MS and Crohn’sDisease and further trials could determine its potential in the treatment of a range of autoimmune diseases.
32
Exhibition Information
1
5
13
12
11
6 7 8 9 10
2
3
4
Floor Plan
Schering AG Germany / Berlex Booth 11Betaseron® was the first therapy approved in the United States to treat relapsing-remitting multiple sclerosis.Berlex has filed a supplemental (sBLA) Biologics License Application to expand the indication of Betaseron® toinclude secondary progressive MS. A new room-temperature formulation of Betaseron® is now available.Betaseron® is the first and only therapy available as a room-temperature formulation (25°C/77°F) for relapsing-remitting MS, providing a convenient option for MS patients in the United States.
Serono Booth 1Rebif (interferon beta-1a) was approved for sale in the United States on March 7, 2002, for the treatment of relaps-ing forms of multiple sclerosis based upon the results of two large multi-center studies. Rebif provides significanttreatment benefits for people with relapsing forms of MS by decreasing the frequency of relapses and delaying theaccumulation of physical disability. Efficacy in chronic progressive MS has not been established. Rebif is available inready-to-use, pre-filled syringes and can be administered using Rebiject, an autoinjector developed exclusively foruse with Rebif. For more information on Rebif visit www.Rebif.com or call MS LifeLines at 877-44-REBIF.
Teva Neuroscience Booth 5Teva Neuroscience invites you to visit our booth to discuss Copaxone (glatiramer acetate for injection).We willalso be discussing MSWatch, the first fully integrated, interactive disease management Web application for peoplewith Multiple Scleross. MSWatch is available free of charge to all MS patients and their health care providers.
ASSOCIATION AND COMMERCIAL EXHIBITORS
Arnold Publishers Booth 10Multiple Sclerosis is published by Arnold Publishers and is now in its 9th year. It focuses on the etiology andpathogenesis of demyelinating and inflammatory diseases of the central nervous system and on the application ofsuch studies to scientifically based therapy. Multiple Sclerosis is a vital journal for research in the following areas:clinical neurology; myelin chemistry; neuroimaging; pathobiology of the blood/brain barrier; glialpathobiology/myelin repair; pathology; epidemiology; therapeutics; genetics; immunology; and virology. Editor-in-Chief, Donald H Silberberg, Department of Neurology, University of Pennsylvania School of Medicine, USA. Formore information, visit www.multiplesclerosisjournal.com.
Cephalon Booth 2Cephalon, Inc., headquartered in West Chester, PA., is an international biopharmaceutical company dedicated tothe discovery, development and marketing of products to treat neurological disorders, sleep disorders, cancer andpain. The Company currently markets three products in the United States: PROVIGIL® (modafinil) Tablets [C-IV]for the treatment of excessive daytime sleepiness associated with narcolepsy, which is being developed for otherpotential uses; GABITRIL® (tiagabine hydrochloride) for the adjunctive treatment of partial seizures associatedwith epilepsy; and ACTIQ® (oral transmucosal fentanyl citrate) for the treatment of breakthrough cancer pain.
Consortium of Multiple Sclerosis Centers Booth 7The Consortium of Multiple Sclerosis Centers (CMSC) is the largest organization of MS healthcare professionalsin the world. Our membership includes MS Centers, Clinics,VA members, and individual healthcare providers. TheCMSC has established standards of care in MS that are being adopted worldwide. CMSC/NARCOMS, the NorthAmerican Research Committee on MS, facilitates multi-center studies and clinical trials through its web site andregistry of 23,000 patients. Our journal is The International Journal of MS Care.The Foundation of the CMSCprovides funds to train healthcare professionals in research and care in MS.
Serono is pleased to bring you the Liv-ing with MS Art andMusic Festival.
Proud sponsor of the Living with MS Art and Music Festival
This therapeutic happening is an exhibition of American and international art created by patients, neurologists, and nurses in the MS community.
Evening festivities include:Gallery viewing and receptionBuffet dinner served on Waterside BoulevardJazz concert under the Pavilion on Pier Six
Please join us at 7:00PM on Pier Siximmediately following the Satellite Symposiumon Friday, September 20, 2002.
Please visit us at booth #1 for more information.
Art ontheWaterfront
EDMUS Booth 4The European Database for Multiple Sclerosis (EDMUS) is a standardised computerised databasing system whichhas been conceived within consecutive European Concerted Actions on Multiple Sclerosis (MS) since 1990.EDMUS is a working tool available for clinical and research purposes. It is the result of joint reflections of clini-cians and researchers from the whole European Union, all involved in MS.A specific Steering Committee with atleast one delegate from each country of the European Union has been set up for this purpose.Today the EDMUSsystem is established in more than 190 centers over 26 countries. It is used for the clinical follow-up of patients,independent research projects and collaborative multicenter studies where a “common language” is mandatory.A new version of the software has been developed in order to come up to all users’ expectations.
European Charcot Foundation Booth 8The European Charcot Foundation started in 1990 as the legal carrier of a Concerted Action in MultipleSclerosis (MS) Research funded by the European Communities. From 1994 on the European Charcot Founda-tion continued as a non-profit Foundation, supported by private organisations, National MS Societies andIndustries. Its working base in Europe now consists of more than 550 institutions and 1700 investigators.With their dedication the Foundation wants to realize a European dimension in MS Research and capitalizeon the great resources of European co-operation and co-ordination to overcome this debilitating disease.
Multiple Sclerosis International Federation Booth 6The Multiple Sclerosis International Federation (MSIF) was established in 1967 and links the work of its 42national Member Societies worldwide. It is committed to working with these Societies and with the interna-tional research community to eliminate MS and its devastating effects. The MSIF also speaks out on a global levelfor those affected by MS.
National Multiple Sclerosis Society Booth 9Through our Professional Resource Center, the NMSS provides timely and expert information to physicians andother healthcare professionals involved in the care of people with MS and their families. Contact us for informa-tion and consultation about the disease and its management; library and literature search services; informationabout insurance and long-term care; continuing education opportunities; and consultation on the development ofNational MS Society-affiliated clinical facilities. For further information, contact the PRC by phone at 1-866-MS-TREAT, by e-mail at [email protected], or visit us online at www.nationalmssociety.PRC/asp.
The Sylvia Lawry Centre for Multiple Sclerosis Research (SLCMSR) Booth 6The SLCMSR was founded in February 2001 at the Technical University of Munich under the direction of Prof.Albrecht Neiß and sponsored by the Multiple Sclerosis International Federation (MSIF). Using the combination ofcomputer science, mathematics and medicine, it aims to make future development of MS therapies faster and lesscostly.This will be achieved by identifying clinical and MRI markers, which will be more reliably predictive of thefuture course of MS than those so far identified, using mathematical models based on an unequalled collection ofplacebo data from clinical trials and natural history data. It is an excellent example of what can be done whenindustry and academics work together.
WebMD Booth 3WebMD Corporation provides a comprehensive suite of information, transaction and technology solutions thathelp consumers, physicians, providers and other participants navigate the complexity of the healthcare system.Our products and services promote informed decision-making, increased efficiency and, ultimately, higher qualitypatient care at a lower cost. WebMD Corporation consists of three divisions, each a leader in their respectivefield: WebMD Envoy,WebMD Medical Manager and WebMD Health.
For ambulatory patients with relapsing-remitting multiple sclerosis (MS) to treat clinical exacerbations...
Betaseron is a registered trademark and the design and MS Pathways are service marks of Berlex Laboratories, Inc.
Carol—Betaseron usersince 1994.
Serious side effects include depression, suicide, suicidal ideation, and injection-site necrosis (skin breakdown, drainage of fluid, and tissue destruction), which has been reported in 5% of patients in a controlled MS trial. The necrotic lesions are typically 3 cm or less in diameter, but larger areas have been reported, and they may occur at single or multiple sites. Patients should be advised of the importance of rotating areas of injection with each dose, and of consulting with their physician if they experience any of the above signs or symptoms.(See WARNINGS, PRECAUTIONS, and ADVERSE REACTIONS sections of the full prescribing information.)Common side effects of Betaseron therapy include flu-like symptoms, shortness of breath, menstrual disorders, and injection-site reactions; redness, pain,swelling, and blue-black discoloration have been reported.
Please see full prescribing information on adjacent page.
• Deliver NEW Convenience that Helps Improve Compliance —NEW Refrigeration-Free Betaseron is the only therapy that can be stored and transportedat room temperature — and as always, with a neutral pH of approximately 7.4
• Deliver the Full Effect With Frequent Dosing — taken every other day subcutaneously, Betaseron (250 mcg) is specifically designed to maintain a constanteffect on biological response markers
• Deliver Manageability — common side effects are usually easily managed andoften improve over time
• Deliver the Full Support of MS PathwaysSM — helps you assist your patients inmanaging their therapy through a 24/7 toll-free hot line that features MS-specializedregistered nurses
and deliver the full effect of the only Refrigeration-Free interferon therapy — Betaseron
SM
DESCRIPTIONBetaseron® (Interferon beta-1b) is a purified, sterile, lyophilized protein product produced by recombinant DNA techniques and formulated foruse by injection. Interferon beta-1b is manufactured by bacterial fermentation of a strain of Escherichia coli that bears a genetically engineeredplasmid containing the gene for human interferon betaser17. The native gene was obtained from human fibroblasts and altered in a way that sub-stitutes serine for the cysteine residue found at position 17. Interferon beta-1b is a highly purified protein that has 165 amino acids and anapproximate molecular might of 18,500 daltons. It does not include the carbohydrate side chains found in the natural material.The specific activity of Betaseron is approximately 32 million international units (IU)/mg Interferon beta-1b. Each vial contains 0.3 mg ofInterferon beta-1b. The unit measurement is derived by comparing the antiviral activity of the product to the World Health Organization (WHO)reference standard of recombinant human interferon beta. Mannitol USP and Albumin Human USP (15 mg each/vial) are added as stabilizers.Prior to 1993, a different analytical standard was used to determine potency. It assigned 54 million IU to 0.3 mg Interferon beta-1b.Lyophilized Betaseron is a sterile, white to off-white powder intended for subcutaneous injection after reconstitution with the diluent supplied(Sodium Chloride, 0.54% Solution). CLINICAL PHARMACOLOGYGeneral: Interferons are a family of naturally occurring proteins, which have molecular weights ranging from 15,000 to 21,000 daltons. Threemajor classes of interferons have been identified: alfa, beta, and gamma. Interferon beta-1b, interferon alfa, and interferon gamma have over-lapping yet distinct biologic activities.1-5 The activities of Interferon beta-1b are species-restricted and, therefore, the most pertinent pharmaco-logic information on Betaseron is derived from studies of human cells in culture and in humans.Biologic Activities: Interferon beta-1b has been shown to possess both antiviral and immunoregulatory activities. The mechanisms bywhich Betaseron exerts its actions in multiple sclerosis (MS) are not clearly understood. However, it is known that the biologic response-modifying properties of Interferon beta-1b are mediated through its interactions with specific cell receptors found on the surface of humancells. The binding of Interferon beta-1b to these receptors induces the expression of a number of interferon-induced gene products (e.g.,2’,5’-oligoadenylate synthetase, protein kinase, and indoleamine 2,3-dioxygenase) that are believed to be the mediators of the biologicalactions of Interferon beta-1b.1,3,6-10 A number of these interferon-induced products have been readily measured in the serum and cellular frac-tions of blood collected from patients treated with Interferon beta-1b.11,12
Pharmacokinetics: Because serum concentrations of Interferon beta-1b are low or not detectable following subcutaneous administration of0.25 mg or less of Betaseron, pharmacokinetic information in patients with MS receiving the recommended dose of Betaseron is not available.Following single and multiple daily subcutaneous administrations of 0.5 mg Betaseron to healthy volunteers (N =12), serum Interferon beta-1bconcentrations were generally below 100 IU/mL. Peak serum Interferon beta-1b concentrations occurred between 1 to 8 hours, with a meanpeak serum interferon concentration of 40 IU/mL. Bioavailability, based on a total dose of 0.5 mg Betaseron given as two subcutaneous injec-tions at different sites, was approximately 50%.After intravenous administration of Betaseron (0.006 mg to 2.0 mg), similar pharmacokinetic profiles were obtained from healthy volunteers(N=12) and from patients with diseases other than MS (N=142). In patients receiving single intravenous doses up to 2.0 mg, increases in serumconcentrations were dose proportional. Mean serum clearance values ranged from 9.4 mL/min·kg-1 to 28.9 mL/min·kg-1 and were independent ofdose. Mean terminal elimination half-life values ranged from 8.0 minutes to 4.3 hours and mean steady-state volume of distribution valuesranged from 0.25 L/kg to 2.88 L/kg. Three-times-a-week intravenous dosing for 2 weeks resulted in no accumulation of Interferon beta-1b inthe serum of patients. Pharmacokinetic parameters after single and multiple intravenous doses of Betaseron were comparable.Clinical Trials: The effectiveness of Betaseron in relapsing-remitting MS was evaluated in a double-blind, multiclinic (11 sites: 4 Canadian and7 United States), randomized, parallel, placebo-controlled clinical investigation of 2 years duration. The study enrolled MS patients, aged 18 to50, who were ambulatory (Kurtzke expanded disability status scale [EDSS] of ≤ 5.5), exhibited a relapsing-remitting clinical course, met Poser’scriteria13 for clinically definite and/or laboratory supported definite MS and had experienced at least two exacerbations over 2 years precedingthe trial without exacerbation in the preceding month. Patients who had received prior immunosuppressant therapy were excluded.An exacerbation was defined, per protocol, as the appearance of a new clinical sign/symptom or the clinical worsening of a previous sign/symp-tom (one that had been stable for at least 30 days) that persisted for a minimum of 24 hours.Patients selected for study were randomized to treatment with either placebo (N =123), 0.05 mg of Betaseron (N =125), or 0.25 mg of Betaseron (N =124) self-administered subcutaneously every other day. Outcome based on the 372 randomized patients was evaluat-ed after 2 years.Patients who required more than three 28-day courses of corticosteroids were removed from the study. Minor analgesics (acetaminophen, codeine),antidepressants, and oral baclofen were allowed ad libitum but chronic nonsteroidal anti-inflammatory drug (NSAID) use was not allowed.The primary, protocol defined, outcome assessment measures were 1) frequency of exacerbations per patient and 2) proportion of exacerbationfree patients. A number of secondary outcome measures were also employed as described in TABLE 1.In addition to clinical measures, annual magnetic resonance imaging (MRI) was performed and quantitated for extent of disease as determinedby changes in total area of lesions. In a substudy of patients (N=52) at one site, MRIs were performed every 6 weeks and quantitated for dis-ease activity as determined by changes in size and number of lesions.Results at the protocol designated endpoint of 2 years (see TABLE 1): In the 2-year analysis, there was a 31% reduction in annual exacerbationrate, from 1.31 in the placebo group to 0.9 in the 0.25 mg group. The p-value for this difference was 0.0001. The proportion of patients free ofexacerbations was 16% in the placebo group, compared with 25% in the Betaseron® (Interferon beta-1b) 0.25 mg group.Of the 372 patients randomized, 72 (19%) failed to complete 2 full years on their assigned treatments. The reasons given for withdrawal varied withtreatment assignment. Excessive use of steroids accounted for 11 of the 26 placebo withdrawals, but only 2 of the 21 withdrawals from the 0.05 mgassigned group and 1 of the 25 withdrawals from the 0.25 mg assigned group. Withdrawals for adverse events attributed to study article, however,were more common among Betaseron-treated patients: 1, 5, and 10 withdrew from the placebo, 0.05 mg, and 0.25 mg groups, respectively.Over the 2-year period, there were 25 MS-related hospitalizations in the 0.25 mg Betaseron-treated group compared to 48 hospitalizations inthe placebo group. In comparison, non-MS hospitalizations were evenly distributed among the groups, with 16 in the 0.25 mg Betaseron groupand 15 in the placebo group. The average number of days of MS-related steroid use was 41 days in the 0.25 mg Betaseron group and 55 days inthe placebo group (p = 0.004).
MRI data were also analyzed for patients in this study. A frequency distribution of the observed percent changes in MRI area at the end of 2 years was obtained by grouping the percentages in successive intervals of equal width. Figure 1 displays a histogram of the proportions ofpatients who fell into each of these intervals. The median percent change in MRI area for the 0.25 mg group was –1.1% which was signifi-cantly smaller than the 16.5% observed for the placebo group (p = 0.0001).
In an evaluation of frequent MRI scans (every 6 weeks) on 52 patients at one site, the percent of scans with new or expanding lesions was 29%in the placebo group and 6% in the 0.25 mg treatment group (p = 0.006).MRI scanning is viewed as a useful means to visualize changes in white matter that are believed to be a reflection of the pathologic changesthat, appropriately located within the central nervous system (CNS), account for some of the signs and symptoms that typify relapsing-remittingMS. The exact relationship between MRI findings and the clinical status of patients is unknown. Changes in lesion area often do not correlatewith clinical exacerbations probably because many lesions affect so-called “silent” regions of the CNS. Moreover, it is not clear what fraction ofthe lesions seen on MRI become foci of irreversible demyelinization (i.e., classic white matter plaques). The prognostic significance of the MRIfindings in this study has not been evaluated. At the end of 2 years on assigned treatment, patients in the study had the option of continuing ontreatment under blinded conditions. Approximately 80% of patients under each treatment accepted. Although there was a trend toward patientbenefit in the Betaseron® (Interferon beta-1b) groups during the third year, particularly in the 0.25 mg group, there was no statistically signifi-cant difference between the Betaseron-treated vs. placebo-treated patients in exacerbation rate, or in any of the secondary endpoints describedin Table 1. As noted above, in the 2-year analysis, there was a 31% reduction in exacerbation rate in the 0.25 mg group, compared with placebo.The p-value for this difference was 0.0001. In the analysis of the third year alone, the difference between treatment groups was 28%. The p-value was 0.065. The lower number of patients may account for the loss of statistical significance, and lack of direct comparability among thepatient groups in this extension study makes the interpretation of these results difficult. The third year MRI data did not show a trend towardadditional benefit in the Betaseron arm compared with the placebo arm.Throughout the clinical trial, serum samples from patients were monitored for the development of antibodies to Interferon beta-1b. In patientsreceiving 0.25 mg of Betaseron (N=124) every other day in the clinical trial, 45% were found to have serum neutralizing activity at one or more ofthe time points tested. The relationship between antibody formation and clinical efficacy is not known.INDICATIONS AND USAGEBetaseron is indicated for use in ambulatory patients with relapsing-remitting multiple sclerosis to reduce the frequency of clinical exacerbations.(See CLINICAL PHARMACOLOGY, Clinical Trials section.) Relapsing-remitting MS is characterized by recurrent attacks of neurologic dys-function followed by complete or incomplete recovery. The safety and efficacy of Betaseron in chronic-progressive MS has not been evaluated.CONTRAINDICATIONSBetaseron is contraindicated in patients with a history of hypersensitivity to natural or recombinant interferon beta, Albumin Human USP, or anyother component of the formulation.WARNINGSOne suicide and 4 attempted suicides were observed among 372 study patients during a 3-year period. All five patients received Betaseron (three inthe 0.05 mg group and two in the 0.25 mg group). There were no attempted suicides in patients on study who did not receive Betaseron. Depressionand suicide have been reported to occur in patients receiving interferon alfa, a related compound. Patients to be treated with Betaseron should beinformed that depression and suicidal ideation may be a side effect of the treatment and should report these symptoms immediately to the prescrib-ing physician. Patients exhibiting depression should be monitored closely and cessation of therapy should be considered.Injection site necrosis (ISN) has been reported in 5% of patients in controlled clinical trials (see ADVERSE REACTIONS section). Typically,injection site necrosis occurs within the first 4 months of therapy, although post-marketing reports have been received of ISN occurring over 1 year after initiation of therapy. Necrosis may occur at single or multiple injection sites. The necrotic lesions are typically 3 cm or less in diame-ter, but larger areas have been reported. While necrosis has commonly extended only to subcutaneous fat, there are also reports of necrosisextending to and including fascia overlaying muscle. In some lesions where biopsy results are available, vasculitis has been reported. For somelesions debridement and, infrequently, skin grafting has been required. As with any open lesion, it is important to avoid infection and, if it occurs, to treat the infection. Time to healing has varied depending on theseverity of the necrosis at the time treatment was begun. In most cases healing was associated with scarring.Some patients have experienced healing of necrotic skin lesions while Betaseron® (Interferon beta-1b) therapy continued; others have not.Whether to discontinue therapy following a single site of necrosis is dependent on the extent of necrosis. For patients who continue therapywith Betaseron after injection site necrosis has occurred, Betaseron should not be administered into the affected area until it is fully healed. Ifmultiple lesions occur, therapy should be discontinued until healing occurs.Patient understanding and use of aseptic self-injection techniques and procedures should be periodically reevaluated, particularly if injectionsite necrosis has occurred.PRECAUTIONSGeneral: Patients should be instructed in injection techniques to assure the safe self-administration of Betaseron. (See PRECAUTIONS,Information to patients, and Betaseron Patient Information sheet.)Information to patients:
Instruction on self-injection technique and procedures. Patients should be instructed in the use of aseptic technique when adminis-tering Betaseron. Appropriate instruction for reconstitution of Betaseron and self-injection should be given including careful review of theBetaseron Patient Information sheet. If possible, the first injection should be performed under the supervision of an appropriately quali-fied health care professional.Patients should be cautioned against the re-use of needles or syringes and instructed in safe disposal procedures. A puncture resistant con-tainer for disposal of used needles and syringes should be supplied to the patient along with instructions for safe disposal of full containers.Patients should be advised of the importance of rotating areas of injection with each dose, to minimize the likelihood of severe injection sitereactions or necrosis (see Rotating Injection Sites section of Patient Information sheet).Patients should be cautioned not to change the dosage or the schedule of administration without medical consultation. Awareness of adverse reactions. Serious adverse reactions associated with the use of Betaseron have been reported including depres-sion and injection site necrosis (see WARNINGS section).Patients should immediately report symptoms of depression or suicidal ideation to their physician. The symptoms of depression should beclosely monitored by a physician. Injection site necrosis was reported in 5% of patients in a controlled MS trial. If the patient experiences any break in the skin, which may beassociated with blue-black discoloration, swelling, or drainage of fluid from the injection site, the patient should be advised to promptly con-tact their physician prior to continuing their Betaseron therapy. Other injection site reactions occurred in eighty-five percent of patients in the controlled MS trial, at one or more times during therapy. Therewas redness, pain, swelling and discoloration. In general, these were transient and did not require discontinuation of therapy, but the natureand severity of all reported reactions should be carefully assessed (see ADVERSE REACTIONS section).Flu-like symptoms are common following initiation of therapy with Betaseron. In the controlled MS clinical trial, acetaminophen was permit-ted for relief of fever or myalgia (see ADVERSE REACTIONS section).Patients should be cautioned about the abortifacient potential of Betaseron (see PRECAUTIONS, Pregnancy — Teratogenic effects).
Laboratory tests: The following laboratory tests are recommended prior to initiating Betaseron therapy and at periodic intervals thereafter:hemoglobin, complete and differential white blood cell counts, platelet counts and blood chemistries including liver function tests. In the con-trolled MS trial, patients were monitored every 3 months. The study protocol stipulated that Betaseron therapy be discontinued in the event theabsolute neutrophil count fell below 750/mm3. When the absolute neutrophil count had returned to a value greater than 750/mm3, therapy couldbe restarted at a 50% reduced dose. No patients were withdrawn or dose reduced for neutropenia or lymphopenia.Similarly, if hepatic transaminase (SGOT/SGPT) levels exceeded 10 times the upper limit of normal, or if the serum bilirubin exceeded 5 timesthe upper limit of normal, therapy was discontinued. In each instance during the controlled MS trial, hepatic enzyme abnormalities returned tonormal following discontinuation of therapy. When measurements had decreased to below these levels, therapy could be restarted at a 50%dose reduction, if clinically appropriate. Two patients were dose reduced for increased liver enzymes; one continued on treatment and one wasultimately withdrawn.Drug interactions: Interactions between Betaseronand other drugs have not been fully evaluated. Although studies designed to examine druginteractions have not been done, it was noted that corticosteroid or ACTH treatment of relapses for periods of up to 28 days has been adminis-tered to patients (N=180) receiving Betaseron.Betaseron administration to three cancer patients over a dose range of 0.025 mg to 2.2 mg led to a dose-dependent inhibition of antipyrine elim-ination.14 The effect of alternate-day administration of 0.25 mg of Betaseron on drug metabolism in MS patients is unknown.Carcinogenesis: The carcinogenic potential of Betaseron was evaluated by studying its effect on the morphological transformation of themammalian cell line BALBc-3T3. No significant increases in transformation frequency were noted. No carcinogenicity data are available in ani-mals or humans.
40Betaseron 0.25 mg
30
20
% o
f Pat
ient
s
10
0
40
From –60
Placebo
Percent Change in MRI Area
Median Change = –1.1%n=95
Figure 1Distribution of Change in MRI Area
Median Change = +16.5%n=10030
20
% o
f Pat
ient
s
10
0–40 –20 0 20 40 60 80 100 120 140+
To <–40 <–20 <0 <20 <40 <60 <80 <100 <120 140
TABLE 12 Year Study Results
Primary and Secondary Clinical Endpoints
Statistical ComparisonsEfficacy Parameters Treatment Groups
≥ 5 21 16 8Secondary Endpoints††Median number of months 5 6 9 0.299 0.097 0.010to first on-study exacerbationRate of moderate or severe 0.47 0.29 0.23 0.020 0.257 0.001exacerbations per year
Mean number of moderate or severe 44.1 33.2 19.5 0.229 0.064 0.001exacerbation days per patientMean change in EDSS 0.21 0.21 –0.07 0.995 0.108 0.144score‡ at endpoint
Mean change in Scripps –0.53 –0.50 0.66 0.641 0.051 0.126score‡‡ at endpointMedian duration in days 36 33 35.5 ND ND NDper exacerbation% change in mean MRI 21.4% 9.8% –0.9% 0.015 0.019 0.0001lesion area at endpoint
ND - Not done† 14 exacerbation-free patients (0 from placebo, 6 from 0.05 mg, and 8 from 0.25 mg) dropped out of the study before completing
6 months of therapy. These patients are excluded from this analysis.†† Sequelae and Functional Neurologic Status, both required by protocol, were not analyzed individually but are included as a function
of the EDSS.‡ EDSS scores range from 0–10, with higher scores reflecting greater disability.‡‡ Scripps neurologic rating scores range from 0–100, with smaller scores reflecting greater disability.
Betaseron®
Interferon beta-1b
Betaseron® (Interferon beta-1b) was not mutagenic when assayed for genotoxicity in the Ames bacterial test in the presence or absence ofmetabolic activation.Impairment of fertility: Studies in rhesus monkeys at doses up to 0.33 mg/kg/day (32 times the recommended human dose based on body sur-face area comparison*) in normally cycling rhesus female monkeys had no apparent adverse effects on the menstrual cycle or on associatedhormonal profiles (progesterone and estradiol) when administered over 3 consecutive menstrual cycles. The extrapolability of animal doses tohuman doses is not known. Effects of Betaseron on normal cycling human females are not known.*body surface dose based on 70 kg femalePregnancy — Teratogenic effects: Pregnancy Category C: Betaseron was not teratogenic at doses up to 0.42 mg/kg/day in rhesus monkeys,but demonstrated a dose-related abortifacient activity when administered at doses ranging from 0.028 mg/kg/day (2.8 times the recommendedhuman dose based on body surface area comparison) to 0.42 mg/kg/day (40 times the recommended human dose based on body surface areacomparison). The extrapolability of animal doses to human doses is not known. Lower doses were not studied in monkeys. Spontaneous abor-tions while on treatment were reported in patients (n= 4) who participated in the Betaseron MS clinical trial. Betaseron given to rhesus monkeyson gestation days 20 to 70 did not cause teratogenic effects, however, it is not known if teratogenic effects exist in humans. There are no ade-quate and well-controlled studies in pregnant women. If the patient becomes pregnant or plans to become pregnant while taking Betaseron, thepatient should be apprised of the potential hazard to the fetus and it should be recommended that the patient discontinues therapy.Nursing mothers: It is not known whether Betaseron is excreted in human milk. Because many drugs are excreted in human milk and becauseof the potential for serious adverse reactions in nursing infants from Betaseron, a decision should be made as to whether either to discontinuenursing or discontinue the drug, taking into account the importance of drug to the mother.Pediatric use: Safety and efficacy in children under 18 years of age have not been established.ADVERSE REACTIONSExperience with Betaseron in patients with MS is limited to a total of 147 patients at the recommended dose of 0.25 mg every other day or more(see CLINICAL PHARMACOLOGY, Clinical Trials section). Consequently, adverse events that are associated with the use of Betaseron inMS patients at a low incidence may not have been observed in premarketing studies. Clinical experience with Betaseron in other populations(patients with cancer, HIV positive patients, etc.) provides additional data regarding adverse reactions; however, experience in non-MS popula-tions may not be fully applicable to the MS population.Injection site reactions (85%) and injection site necrosis (5%) occurred after administration of Betaseron. Inflammation, pain, hypersensitivity,necrosis, and non-specific reactions were significantly associated (p<0.05) with the 0.25 mg Betaseron-treated group. Only inflammation, pain,and necrosis were reported as severe events (see WARNINGS and PRECAUTIONS sections). The incidence rate for injection site reactions
P292–P313Experimental AllergicEncephalomyelitis (II)Healthcare Systems
New Clinical Trials (II)
DoverLevel 3
P137–P167Genetics (I)
Immunotherapy (I)Pathology
P314–P345Genetics (II)
Immunotherapy (II)
GrandBallroom
FoyerLevel 3
40
Poster Display Schedule
Poster Session I Poster Session IIThursday Friday
September 19 September 20
The Program Committee congratulates authors whose abstracts were selected forposter display at ACTRIMS-ECTRIMS 2002. Posters are on display from 8 am–5 pm.Presenting authors will stand by their posters from Noon–2 pm.
Further information regarding poster room assignments will be available onsite.
Surrogate Markers
P1 CEREBROSPINAL FLUID PROTEIN STATUS ANDITS CLINICAL USE Adam P, Sobek O,Taborsky L,Vesela B,Prucha M
P2 INTERLEUKIN-10 / INTERLEUKIN-12 COEFFI-CIENT AS POTENTIAL INDICATOR OF POSITIVERESPONSE TO INTERFERON � TREATMENT Bartosik-Psujek H, Mitosek-Szewczyk K, Belniak E, Stelmasiak Z
P3 LEPTIN AS PREDICTIVE MARKER OF MULTIPLESCLEROSIS ACTIVITY DURING INTERFERON� 1ATHERAPY Batocchi A, Rotondi M, Caggiula M, Frisullo G,Odoardi F, Nociti V, Carella C,Tonali P, Mirabella M
P4 ANTI-NEUROFILAMENT ANTIBODIES ARE ASSO-CIATED WITH DISEASE PROGRESSION IN MULTIPLESCLEROSIS Ehling R, Reindl M, Schanda K,Wanschitz J,Deisenhammer F, BergerT
P5 RELATIONSHIP BETWEEN THE MS FUNCTIONALCOMPOSITE AND MRI IN IMPACT Cohen JA, GoodmanAD, Heidenreich FR, Kooijmans MF, Sandrock AW, Simon JH,Tsao EC
P6 A FOUR-MONTH LONGITUDINAL STUDY ONTHE RELATIONSHIP BETWEEN CLINICAL ACTIVITYAND SERA CONCENTRATION OF S100 PROTEIN ANDNEURON SPECIFIC ENOLASE IN MULTIPLE SCLEROSIS.Finamore L, Zivadinov R, Cecchinelli D, Pichi A, Pierallini A, Bas-tianello S, Nasuelli D, Bratina A, Locatelli L, Grop A, Reale M,Zorzon M, Millefiorini E
P7 WHOLE BRAIN N-ACETYLASPARTATE ASSESS-MENT IN RELAPSING-REMITTING MULTIPLE SCLERO-SIS—EVIDENCE FOR DIFFERENT CLINICAL COHORTSGonen O, Moriarity DM, Li BS, Babb JS, Markowitz CM, Gross-man RI
P8 INTERFERON BETA-1A IN COMBINATION WITHAZATHIOPRINE AND LOW DOSE STEROIDS FORRELAPSING-REMITTING MULTIPLE SCLEROSIS: PILOTMODEL FOR PREDICTIVE MULTIVARIATE TYPOLOGYOF RELAPSES BASED ON CLINICAL AND MRI DATAHavrdova E, Horakova D, Krasensky J, Dusek L,Vaneckova M,Seidl Z,Ticha V, Novakova I,Tyblova M
P9 PLASMA LEVELS OF BRAIN-SPECIFIC OXYSTEROLMAY REFLECT PROGRESSION OF MS MastermanT,Leoni V, Diczfalusy U, Melzi d’Eril G, Hillert J, Björkhem I
P10 MATRIX METALLOPROTEINASE-9 IN MULTIPLESCLEROSIS CLINICAL FORMS Sastre-Garriga J, ComabellaM, Rovira À,Aymerich X, López C,Téllez N, Montalban X
P11 DYNAMICS OF AXONAL PATHOLOGY IN MUL-TIPLE SCLEROSIS Petzold A, Eikelenboom MJ, Keir G, Laze-ron RC, Polman CH, Uitdehaag BJ,Thompson EJ, Giovannoni G
P12 INCREASED SERUM NITRIC OXIDE METABO-LITES ARE RELATED TO DISEASE ACTIVITY IN PATIENTSWITH MULTIPLE SCLEROSIS Rejdak K, Petzold A,Chard D, Griffin C, Miszkiel KA, Davis G, Rashid W, Miller DH,Stelmasiak Z,Thompson EJ, Giovannoni G
P13 IMMUNOLOGICAL MARKERS OF DISEASEACTIVITY IN NEWLY-DIAGNOSED MULTIPLE SCLERO-SIS:A ONE YEAR FOLLOW-UP STUDY IN MRI MONI-TORED PATIENTS Rinaldi L, Motta M, Calabrese M,Guglielmo A, Ranzato F,Tiberio M, Dalle Carbonare M, Leon A,Gallo P
P14 COGNITIVE FATIGUE DURING A TEST REQUIR-ING SUSTAINED ATTENTION Schwid SR,Weinstein A,Goodman AD, Scheid EA,Tyler CM, McDermott MP
P15 RELATIVE SENSITIVITY OF TIME TO WALK 25 FEET FOR PROGRESSION OF DISABILITY Schwid SR,Goodman AD, Scheid EA, McDermott MP
P16 CYTOCHROME P46,A SUITABLE MARKER FORNEURODEGENERATION IN EAE-MODELS AND MS?Teunissen CE, Dijkstra CD
Clinical Aspects of MS (Part 1)
P17 SCREENING FOR DEPRESSION IN MULTIPLESCLEROSIS:YALE SINGLE QUESTION VS. BECK DEPRES-SION INVENTORY SCALE Avasarala JR, Cross A,Trinkaus K
P18 MULTIPLE SCLEROSIS AND HASHIMOTO’S THY-ROIDITIS:TWO CASES Balc´y BP,Yayla V, Özer F
P19 EFFECT OF INTERFERON-BETA-1B ON COG-NITIVE FUNCTIONS IN MULTIPLE SCLEROSIS BarakY,Achiron A
P20 COMPUTERIZED ISOMETRIC MUSCLESTRENGTH—NATURAL HISTORY IN MULTIPLE SCLE-ROSIS Brooks BR, Sanjak M, Belden D, Dogan S, Konopacki R,Roelke K, Peper S, Parnell J
P21 MS FUNCTIONAL COMPOSITE.A TRANSVERSALPOPULATION BASED STUDY Casanova B, Coret F,Bernat A, García E, Pascual A,Valero C, De Vera A
P22 EFFECT OF TRAINING ON THE MULTIPLE SCLE-ROSIS FUNCTIONAL COMPOSITE SCALE IN EARLYRELAPSING AND REMITTING MS.A LONGITUDINALONE YEAR FOLLOW-UP STUDY Casanova B, Coret F,García E, Bernat A,Valero C, De Vera A, Pascual A
P23 PROBABLE CUTANEOUS SARCOIDOSIS ASSO-CIATED WITH INTERFERON-BETA 1B TREATMENT INMULTIPLE SCLEROSIS. Clerc C, Chevalier Y, Bataillard M,Rumbach L, Richard P
P24 BENIGN MULTIPLE SCLEROSIS IN SARDINIA:A RETROSPECTIVE STUDY Cocco EE, Lai MM, Marchi PP,Floris GG, Fadda LL, Sanna SS, Marrosu MM
P25 ACUTE PARTIAL TRANSVERSE MYELOPATHY:A 7-YEAR PROSPECTIVE STUDY Cordonnier C, de Seze J,Breteau G, Ferriby D, Michelin E, Stojkovic T, Pruvo J,Vermersch P
P26 MS GENDER ISSUES: CLINICAL PRACTICES OFWOMEN NEUROLOGISTS Coyle PK, Christie S, Fodor P,Fuchs K, Giesser B, Gutierrez A, Lynn J,Weinstock-Guttman B,Pardo LG
P27 IS DEVIC NEUROMYELITIS OPTICA A SEPARATEDISEASE? A COMPARATIVE STUDY WITH MULTIPLESCLEROSIS de seze J, Lebrun C, Stojkovic T, Ferriby D,Chatel M,Vermersch P
P28 DIFFERENTIAL DIAGNOSIS BETWEEN MULTIPLESCLEROSIS AND SJOGREN SYNDROME: INTEREST OFALPHA-FODRIN ANTIBODIES de seze J, Dubucquoi S,Matthias T, Lefranc D, Dussart P,Vermersch P,Witte T
P29 QUANTITATIVE COMPUTERIZED TREMORASSESSMENT IN MULTIPLE SCLEROSIS:TREMOR PREVA-LENCE,TYPE, LONGITUDINAL EVOLUTION IN 321PATIENTS Dogan S, Konopacki R, Brooks BR
P30 CLINICAL, CEREBROSPINAL FLUID AND NEU-ROIMAGING FINDINGS IN OPTICOSPINAL INVOLVE-MENT IN THE SPECTRUM OF INFLAMMATORYDEMYELINATING DISEASES Eraksoy M,Turan N, Kur-tuncu M,Akman-Demir G,Yapici Z, Deniz E, Ozcan H
P31 RECURRENT SYNCOPE AS THE PRESENTINGSYMPTOM IN MULTIPLE SCLEROSIS Fazio MC, Musolino R,Buccafusca M, Dattola V, Scalfari A, Girlanda P, Messina C
P32 THE ITALIAN DEVIC’S STUDY GROUP (IDESG)—PART 1: CLINICAL CHARACTERISTICS OF DEVIC’SNEUROMYELITIS OPTICA AT ONSET Ghezzi A, Berga-maschi R, Martinelli V, Filippi M,Tola R,Trojano M, Zaffaroni M,Comi G
P33 THE ITALIAN DEVIC’S STUDY GROUP (IDESG)—PART 2: COURSE AND PROGNOSIS OF DEVIC’S NEU-ROMYELITIS OPTICA Ghezzi A, Bergamaschi R, Filippi M,Martinelli V,Tola R,Trojano M, Zaffaroni M, Comi G
P34 THERAPY RELATED ACUTE MYELOGENOUSLEUKEMIA IN A PATIENT WITH MULTIPLE SCLEROSISTREATED WITH MITOXANTRONE Heesen C, Brueg-mann M, Koch E, Gold SM, Moench A, Gbadamosi J
P36 A PROSPECTIVE STUDY OF MULTIPLE SCLERO-SIS PRESENTING WITH LARGE FOCAL TUMOR-LIKELESIONS OF THE BRAIN. Jean P, Bertrand A, Laurent S,Jean Philippe R, Sylviane C, Patrick C,Andre A
P37 A PROSPECTIVE STUDY OF MULTIPLE SCLERO-SIS PRESENTING WITH ACUTE MYELOPATHY Jean P,Bertrand A, Jean Philippe R, Laurent S,Alban D, Sylviane C,Patrick C,Andre A
P38 CLINICAL PROFILE AND APPLICATION OFDIAGNOSTIC CRITERIA IN PRIMARY PROGRESSIVEMULTIPLE SCLEROSIS Khan O, Caon C, Ching W, Sonen-virth E,Tselis A, Zvartau-Hind M
P39 RELIABILITY OF EDSS AND FS-SCORE RATINGCAN BE IMPROVED BY STANDARDISED TRAININGLienert C, Lechner-Scott J, Müller U, Kappos L
P40 ISOLATED SPINAL DEMYELINATING EVENTSWITH NORMAL BRAIN MRI: PROGRESSION TO MS,CLINICAL AND MRI FOLLOW UP Milo R, Katz T, Corat-Simon J
P41 ASSESSMENT OF SIGNS AND SYMPTOMS INMULTIPLE SCLEROSIS (MS) AND EVALUATION OF DIS-ABILITY CONDITION IN PATIENTS REFERRED TO MSRESEARCH CLINICS FROM 1997–2001 (2412 CASES)Pakdaman H, Pakdaman R
P42 ONE CASE OF VERY LATE ONSET OF MULTIPLESCLEROSIS WITH ACUTE NEUROPSYCHOLOGICALIMPAIRMENT RaduTD, Marc D, Rene A, Luc T, Herve V
P43 APHASIA IN MULTIPLE SCLEROSIS Berger E,Chopard G,Vidry E, Revenco E, Moulin T, Rumbach L
P45 FACTORS ASSOCIATED WITH DIFFICULTY INI-TIATING AND MAINTAINING IMMUNE MODULATINGTHERAPY Stoian CA, Metz LM
P46 NON-ADHERENCE TO THE BETA-INTERFERONSFOR MULTIPLE SCLEROSIS IN CLINICAL PRACTICETremlett H, Oger J, Special Therapies Group M
P47 VISUAL FUNCTION IN MULTIPLE SCLEROSISPATIENTS: 20 YEARS LATER Vorobeychik G, Anderson D,Lindley J, Paty DW, UBC MS Clinic t
Poster Session I: Thursday, September 19
41
Epidemiology
P48 COMPARISON OF DIAGNOSTIC CRITERIA FORMULTIPLE SCLEROSIS Balcy BP,Yayla V, Özer F
P49 LOOKING FOR THE DEFINITION OF BENIGNMULTIPLE SCLEROSIS Coustans M, Le Page E, Le Duff F,Leray E, Sartori E, Edan G
P50 INCIDENCE AND PREVALENCE OF MULTIPLESCLEROSIS IN AN HMO IN ARGENTINA Cristiano E,Patrucco LB, Soriano ER,Videla GC, Figar S, Hares D, Bauso Toselli PL
P51 DEVIC’S NEUROMYELITIS OPTICA (NMO) ANDMULTIPLE SCLEROSIS (MS): CLINICAL AND EPIDEMIO-LOGIC FINDINGS IN AN MS CENTER IN ARGENTINAPatrucco LB, Cristiano E,Videla GC, Bauso Toselli PL
P52 FIRST LACTRIMS’ (LATIN AMERICAN COM-MITTEE FOR TREATMENT AND RESEARCH IN MS) E-CENSUS: UNDERSTANDING THE PRESENT TODEVELOP THE FUTURE Cristiano E, Patrucco L, Rivera V,Gold L, Correale J,Videla G
P53 OPTIC NEURITIS AS EARLY MANIFESTATION OF MULTIPLE SCLEROSIS Eleonora K, Jarmila S
P54 MULTIPLE SCLEROSIS PREVALENCE AND HLACLASS II ALLELE DISTRIBUTION IN GYPSIES FROMMALAGA, SOUTHERN SPAIN FernándezV, Mayorga C,Leyva L, Guerrero R,Arnal C, Hens M, Luque G, Fernández O
P55 COURSE, DISABILITY AND IMMUNOMODULA-TORY TREATMENT OF PATIENTS WITH MULTIPLE SCLE-ROSIS BASED ON A POPULATION BASED REGISTRYFrederiksen J
P56 INCIDENCE OF MULTIPLE SCLEROSIS IN ANINE-YEAR PERIOD IN THE PROVINCE OF SEVILLE(SOUTH-WEST SPAIN) Izquierdo G, Navarro G, GarciaMoreno J, Durán E, Gamero M, Ruiz-Peña J, Dinca L, Páramo D
P57 THE PREVALENCE OF MULTIPLE SCLEROSIS INBELO HORIZONTE, BRAZIL Lana-Peixoto MA, Frota E,Campos GB, Botelho CM,Aragão AL
P58 STUDIES ON MULTIPLE SCLEROSIS: A GEO-GRAPHICAL DISTRIBUTION Lana-Peixoto MA, Araujo CR,Macedo R, Haase VG
P59 THE NATURAL HISTORY OF MULTIPLE SCLERO-SIS IN BRAZIL. I. CLINICAL DATA AND DISABILITYLana-Peixoto MA, Callegaro D, Moreira MA, Gama PD, Maciel D,Sá PN
P60 CLINICAL ASPECT, COURSE AND PROGNOSISOF MULTIPLE SCLEROSIS IN SOUTH OF FRANCE:STUDY FROM 500 CONSECUTIVE MS PATIENTS USINGEDMUS Soriani M, Lebrun C, Bourg V, Chatel M
P61 SEASON OF BIRTH IN MULTIPLE SCLEROSISLuetic GG
P62 BIRTH WEIGHT IN MULTIPLE SCLEROSISLuetic GG
P63 USE OF ALTERNATIVE PROVIDERS IN MULTIPLESCLEROSIS Marrie R, Cohen JA, Hadjimichael O, Vollmer T
P64 THE PREVALENCE OF MULTIPLE SCLEROSIS INIRELAND McGuigan C, McCarthy A, Hutchinson M
P65 UNCONVENTIONAL THERAPY USE AMONGMULTIPLE SCLEROSIS PATIENTS Sastre-Garriga J,Munteis E, Rio J, Pericot I,Tellez N,Tintore M, Montalban X
P66 ACUTE DISSEMINATED ENCEPHALOMYELITIS(ADEM) IN ADULTS: COMPARISON WITH AN ADEMPEDIATRIC POPULATION Papayannis CE, Ferreira J,Caceres F, Fernandez Liguori N, Sandoval G,Tenembaum S,Garcea O
P67 MULTIPLE SCLEROSIS IN BOTUCATU, BRAZIL—A POPULATION STUDY Rocha FC, Herrera LC,Morales RR, and the Brazilian Committee for Z
P68 CLINICAL CHARACTERISTICS OF NON-RESPONDERS TO INTERFERON BETA (IFNB) THERAPYIN RELAPSING-REMITTING MULTIPLE SCLEROSIS(RRMS) Waubant EL,Vukusic S, Gignoux L, Durand-Dubief F,Achiti I, Blanc S, Renoux C, Confavreux C
Imaging (Part 1)
P69 LONGITUDINALLY DIFFUSION TENSOR IMAG-ING TO MONITOR MULTIPLE SCLEROSIS COURSECassol E, Ibarrola D, Ranjeva J, Manelfe C, Clanet M, Berry I
P70 MACROPHAGE CELLULAR IMAGING TO MONI-TOR ANTI-VLA4 ANTIBODY TREATMENT Dousset V,Deloire-Grassin M,Touil T, Petry KG, Brochet B
P71 COMPARATIVE STUDY OF CELLULAR IMAGINGWITH SINEREM® AND USPIO 7228 IN EXPERIMENTALAUTOIMMMUNE ENCEPHALOMYELITIS Deloire-Grassin M, Dousset V,Touil T, Petry KG, Brochet B
P72 CORRELATION BETWEEN DIFFUSION MAG-NETIC RESONANCE IMAGING HISTOGRAM ANALYSISAND TOTAL LESION LOAD IN MULTIPLE SCLEROSISCallegaro D, Otaduy M, Lacerda M, Costa M, Bacheschi L,Leite C
P73 DIFFUSE ABNORMALITY OF THE NORMALAPPEARING WHITE MATTER IN MS MAY PREDATESYMPTOM ONSET: LONGITUDINAL HISTOGRAMANALYSIS OF T1 RELAXATION TIME Davies G, Hadji-procopis A,Altmann D, Rashid W, Griffin C, Chard D, Kapoor R,Thompson A, Miller D
P74 LONGITUDINAL STUDY OF PROGRESSIVEBRAIN ATROPHY IN MULTIPLE SCLEROSIS. PRELIMI-NARY DATA Durand Dubief F, Pachai C,Vukusic S,Gignoux L, Renoux C, Cotton F, Froment J, Confavreux C
P75 SERIAL MAGNETIZATION TRANSFER IMAGINGIN OPTIC NEURITIS Hickman SJ,Toosy AT, Miszkiel KA,Jones SJ,Altmann D, MacManus DG, Barker GJ, Plant GT,Thompson AJ, Miller DH
P76 CORTICOSTEROIDS AND OPTIC NERVE ATRO-PHY FOLLOWING OPTIC NEURITIS Hickman SJ,Kapoor R, Jones SJ,Altmann D, Plant GT, Miller DH
P77 SERIAL MAGNETIC RESONANCE IMAGING INOPTIC NEURITIS USING TRIPLE DOSE GADOLINIUMHickman SJ,Toosy AT, Miszkiel KA, Jones SJ, MacManus DG,Plant GT,Thompson AJ, Miller DH
P78 A LONGITUDINAL STUDY OF BRAIN ATROPHYWITH TRANSCRANIAL ULTRASOUND IN RELAPSINGMULTIPLE SCLEROSIS Kallmann B, Rieckmann P,Toyka KV,Mäurer M
P79 FUNCTIONAL MRI CHANGES DURING RECOV-ERY FROM OPTIC NEURITIS Langkilde AR, Rostrup E, Fred-eriksen J, Olsen D, Jensen J, Lauritzen M, Larsson HB
P80 DEVELOPMENT OF A BRAIN TUMOUR IN MS:A CASE REPORT Laule C,Traboulsee A, Keogh C, MaGuire J,Redekop G, MacKay A
P81 GUIDELINES FOR A STANDARDIZED MRI PRO-TOCOL FOR THE DIAGNOSIS AND FOLLOW-UP OFMULTIPLE SCLEROSIS Li D,Traboulsee A, Paty D,WorkGroup on Standardized MRI Protocol C
P82 SPONTANEOUS MAGNETOENCEPHALOGRA-PHY RECORDINGS IN MS PATIENTS Ramo C,Amo C,Fernandez S, Carmen M, Maestú F, Fernandez A, Ortiz T
P83 THE HYPOINTENSE LESION (“BLACK HOLE”)ON T1-WEIGHTED MAGNETIC RESONANCE IMAGINGIN SECONDARY PROGRESSIVE MS: OBSERVATIONSWITH T1-WEIGHTED SPIN-ECHO, MPRAGE AND MAG-NETIZATION TRANSFER IMAGING Redmond IT,Tench CR, Blumhardt LD
P84 STEREOTAXIC CO-REGISTRATION OF MRI AND HISTOPATHOLOGY IN POST-MORTEM MS BRAINSLICES Schmierer K, Scaravilli F, Barker GJ, MacManus DG,Miller DH
P85 QUANTITATIVE ASSESSMENT OF LESIONPATHOLOGY IN POST-MORTEM MS BRAIN:A CORREL-ATIVE MRI/HISTOLOGY STUDY Schmierer K, Scaravilli F,Griffin CM, Barker GJ, Miller DH
P86 T2 LESION BURDEN AND T1-HYPOINTENSE(T1-BLACK HOLE) MRI RESULTS FROM THE IMPACTTRIAL Simon JH, Cohen JA, Goodman A, Heidenreich F, Kooij-mans M, Sandrock A,Tsao EC, IMPACT Investigators
P87 NEURONAL TRACT DEGENERATION PATTERNSBASED ON DIFFUSION TENSOR VERSUS T2 MRICHANGES IN THE CORPUS CALLOSUM IN MSCoombs B, Corboy J, Simon JH
P88 EFFECT OF GLATIRAMER ACETATE (GA) THER-APY ON REGIONAL CEREBRAL METABOLIC ABNOR-MALITIES IN MS PATIENTS (PILOT STUDY) Stoliarov I,Ilves A, Prakhova L, Kataeva G,Totolian N
Immunology (Part 1)
P89 EARLY IMMUNOLOGIC CHANGES IN SEVERELYPROGRESSIVE MULTIPLE SCLEROSIS PATIENTS RECEIV-ING MITOXANTRONE Altintas A, Demir G, Siva A
P90 EFFECT OF 24 MONTHS INTERFERON� TREAT-MENT ON CD4, CD8, CD4CD45RO AND CD4CD45RACELLS IN MULTIPLE SCLEROSIS Belniak E, Bartosik-Psujek H, Mitosek-Szewczyk K, Stelmasiak Z
P91 LONGITUDINAL ANALYSIS OF CSF EXPANDEDCD8+ CLONOTYPES IN THE PERIPHERAL BLOOD OFMULTIPLE SCLEROSIS PATIENTS Cepok S, Zhou D,Vogel F, Sommer N, Hemmer B
P92 THE PIVOTAL ROLE OF PEROXYNITRITE IN THEESTABLISHMENT OF CENTRAL NERVOUS SYSTEMINFLAMMATION: INDUCTION OF BLOOD-BRAINBARRIER PERMEABILITY CHANGES Hooper DC,Spitsin SV, Scott GS
P93 T-CELL REACTIVITY IN MULTIPLE SCLEROSIS:PREDICTIVE VALUE FOR EFFICACY OF INTERFERON-BETA Killestein J, Hintzen R, Uitdehaag B, van Lier R,Polman C
P94 INTERFERON-� LEADS TO STABILIZATION OFTHE BARRIER FUNCTION IN BOVINE, MURINE ANDHUMAN BRAIN CAPILLARY ENDOTHELIAL CELLS INVITRO Kraus J, Ling AK, Hamm S, Kim KS,Voigt K, Osch-mann P, Engelhardt B
Poster Session I: Thursday, September 19
42
Immunology (Part 1) (continued)
P95 FINE SPECIFICITY OF ANTIBODY RESPONSESTO MYELIN SEQUENCES IN ASSOCIATION WITH HLACLASS II ALLELES IN THE SERUM OF BRAZILIANPATIENTS WITH MULTIPLE SCLEROSIS Carvalho A,Liem AM, Santos CC, Sant’Anna G, Frugulhetti I, Leon SV,Quirico-Santos T
P96 INTERFERON GAMMA SECRETION IN MULTIPLESCLEROSIS PATIENS TREATED WITH INTERFERON BETAAND GLATIRAMER ACETATE Lochmanova A, Dolezil D,Zapletalova O, Hradilek P
P97 A ROLE FOR CD1C IN MULTIPLE SCLEROSISLyons J,Yeager M, Luecking L,Wang Q, Porcelli S,Trotter J
P98 MOLECULAR TRACKING OF MYELIN BASICPROTEIN-SPECIFIC T CELL EXPANSION IN MULTIPLESCLEROSIS Muraro PA,Wandinger K, Bielekova B,McFarland HF, Martin R
P99 NITRIC OXIDE AS AN ACTIVITY MARKER INMULTIPLE SCLEROSIS Demir Acar G, Ydiman F, Ydiman E,K’rkal’ G, Çakmakç’ H, Özakbas S
P100 LONGITUDINAL CYTOKINE RESPONSES TOMYELIN PEPTIDES IN MS: PERSISTENCE AND SPREAD-ING OF IMMUNE RESPONSES Pelfrey CM, Moldovan IR,Cotleur AC, Born SE, Karafa M, Lee J, Fisher E, Rudick RA
P101 FATIGUE AND INFLAMMATION IN PATIENTSWITH OPTIC NEURITIS Roed H, Olsen D, Langkilde A,Frederiksen J, Sellebjerg F
P102 DISEASE ACTIVITY IN MULTIPLE SCLEROSISCORRELATES WITH ALTERED EXPRESSION RATIOS OF THE BCL-2 FAMILY PROTEINS IN PERIPHERAL T LYMPHOCYTES Sharief MK, Noori MA
P103 THE EXPRESSION OF APOPTOSIS REGULA-TORY PROTEINS IN B LYMPHOCYTES FROM PATIENTSWITH MULTIPLE SCLEROSIS Sharief MK, Seidi OA
P104 INTERFERON-BETA THERAPY IN MULTIPLESCLEROSIS DOWNREGULATES SURVIVIN EXPRESSIONIN T LYMPHOCYTES Sharief MK, Zoukos Y
P105 CHEMOKINE RECEPTOR EXPRESSION ONCEREBROSPINAL FLUID T-CELLS IN PATIENTS WITHRELAPSING REMITTING MULTIPLE SCLEROSISSindern E, Patzold T, Ossege LM, Gisevius A, Malin JP
P106 DETECTION OF OLIGOCLONAL FREE KAPPACHAINS IN ABSENCE OF OLIGOCLONAL IGG IN THECSF OF CLINICALLY SUSPECTED MS PATIENTSSophie G, Christian S, Myriam S,Thierry D, H. H
P107 FUNCTIONAL CHARACTERIZATION OF THECD28-RELATED MOLECULE ICOS IN MULTIPLE SCLE-ROSIS:A POSSIBLE TARGET FOR SELECTIVE IMMUNEINTERVENTION? Wiendl H, Neuhaus O, Mehling M,Wintterle S, Schreiner B,Weissert R,Weller M, Hartung H,Tolosa E, Melms A
P108 MODULATION OF NEURONAL ACTIVITYAND MOG-INDUCED EAE BY THE ENDOGENOUSPENTAPEPTIDE QYNAD,A PUTATIVE MEDIATOR OFNEUROLOGICAL DYSFUNCTION IN HUMANDEMYELINATING DISEASES Wiendl H, Meuth S,Duyar H, Elbs M, Landgraf P,Weller M,Weissert R, Budde T
Experimental Allergic Encephalomyelitis (Part 1)
P109 �-LIPOIC AND DIHYDROPLIPOIC ACID SUP-PRESS EAE IN SJL MICE AND INHIBIT MMP-9 ACTIVITYIN VITRO Marracci G, Jones R, McKeon G,Winter R, Riscoe M,Bourdette D
P110 NEUROPROTECTIVE EFFECTS OF GLATI-RAMER ACETATE IN A MICE MODEL OF CHRONICEXPERIMENTAL AUTOIMMUNE ENCEPHALOMYELITISOffen DY, Gilgun-sherki Y, Hodengreber V, Panet H, Melamed E
P111 ROLE OF ALPHA(1,3)FUCOSYTRANSPHERASESIN LYMPHOCYTE RECRUITMENT IN BRAIN VENULESAND EXPERIMENTAL AUTOIMMUNEENCEPHALOMYELITIS Piccio L, Scarpini E, Rossi B,Ciabini D, D’Ambrosio D, Ottoboni L, Go A, Homeister JW,Lowe JB, Constantin G
P112 TYPE IV PHOSPHODIESTERASE INHIBITIONREDUCES MATRIX METALLOPROTEINASE 9 EXPRES-SION AND IMPAIRS NUCLEAR FACTOR-KAPPA BTRANSLOCATION IN EXPERIMENTAL ALLERGICENCEPHALOMYELITIS Puerta C, Sánchez A, Baranda P,Ortiz P, Garcia-Merino A
P113 DISEASE SIGNS IN GENE KNOCKOUT MOD-ELS OF MULTIPLE SCLEROSIS DIRECTLY CORRELATEWITH BLOOD-BRAIN BARRIER PERMEABILITYScott GS, Brimer CM, Kean RB, Hooper D
P114 IL-12 DEPENDENT/IFN GAMMA INDEPEN-DENT EXPRESSION OF CCR5 BY MYELIN-REACTIVECD4+ T CELLS CORRELATES WITH ENCEPHALITO-GENICITY Bagaeva L, Williams LP, Segal BM
P115 ENGAGEMENT OF TOLL LIKE RECEPTOR(TLR) 9 OR CD40 REVERSES TOLERANCE AGAINSTMYELIN ANTIGENS AND PRECIPITATES AUTOIMMUNEDEMYELINATION Segal BM, Ichikawa HT
P116 DIFFERENTIAL ANTIGEN-SPECIFIC PREVEN-TION OF EXPERIMENTAL AUTOIMMUNEENCEPHALOMYELITIS WITH NAKED DNA Walczak A,Szymanska B, Selmaj K
P117 PROFILES OF MATRIX METALLOPROTEINASES(MMPS) IN EXPERIMENTAL AUTOIMMUNE ENCEPH-ALOMYELITIS:A SIGNIFICANT ELEVATION OF MMP-12Weaver A, Pennington CJ, Nuttall R, Hogan A, Edwards DR,Yong VW
Neurobiology/Neurophysiology
P118 CEREBROSPINAL FLUID ISOELECTROFOCUS-ING IN A LARGE COHORT OF MULTIPLE SCLEROSISAND OTHERS NEUROLOGICAL DISEASES Amina B,J. D, R. G, B. O, B. H,T. S, D. F, P.V
P119 PERIPHERAL SENSORY AND MOTOR ABNOR-MALITIES IN PATIENTS WITH MULTIPLE SCLEROSISAnlar O,Tombul T, Kisli M
P120 ABSTRACT NOT AVAILABLE FOR PUBLICA-TION
P121 OLIGODENDROGLIAL EXPRESSION OF EDG-2RECEPTOR: DEVELOPMENTAL ANALYSIS AND PHAR-MACOLOGICAL RESPONSES TO LYSOPHOSPHATIDICACID Bruno S, Sonia B, Julien A, Celine J, Gilles B, Marie-Stephane A, Pierre S, Bernard Z, Catherine L
P122 SLEEP DISORDERS IN MULTIPLE SCLEROSISPATIENTS. CLINICAL CORRELATIONS de Andres deFrutos C, Lopez Esteban P, Peraita Adrados R
P123 ELECTRONYSTAGMOGRAPHY FINDINGS INPATIENTS WITH MULTIPLE SCLEROSIS Kylynç M, Can U,Benli S, Özlüolu L, Akkuzu B
P124 BRAINSTEM AUDITORY EVOKED RESPONSEWITH HIGH CLICK STIMULUS REPETITION RATE INMULTIPLE SCLEROSIS Lana-Peixoto MA, Santos MA,Munhoz MS
P125 NEUROPHYSIOLOGICAL EVALUATION OFEXECUTIVE FUNCTIONS IN MULTIPLE SCLEROSIS:A FOLLOW-UP STUDY Leocani L, Martinelli V,Annovazzi P,Tickonova I, Possa F, Comi G
P126 PRESENCE OF HERPES SIMPLEX VIRUS 1 INSAMPLES FROM PATIENTS WITH OPTIC NEURITIS ANDMULTIPLE SCLEROSIS Christodoulou C, Constantinou A,Koptides D, Paschalidou M, Georgiadis N, Chatzisotiriou A,Milonas I
P127 HHV-6A ACTIVE INFECTION IN MULTIPLESCLEROSIS PATIENTS Roberto Á,Virginia D, Eduardo V,Juan José P, Rafael A
P128 HOW DOES BETA INTERFERON TREATMENTAFFECT TO HHV-6 VIRAL LOAD IN MULTIPLE SCLERO-SIS PATIENTS? Virginia D, Roberto Á, Eduardo V, Juan José P,Rafael A
P129 DIFFERENT NON-RADIOACTIVE PERMEABIL-ITY ASSAYS IN AN IN VITRO MODEL OF THE BLOOD-BRAIN-BARRIER Voigt KE, Kraus JR, Oschmann P, Engel-hardt B
New Clinical Trials (Part 1)
P130 THE USE OF PHARMACOKINETIC (PK)MODELING AND EFFICACY DATA TO ESTABLISHOPTIMAL DOSING OF NATALIZUMAB (ANTEGRENTM)Bennett D, Ludden T, Shah J, Floren L, Beckman E
P131 SAFETY AND TOLERABILITY DOSE COMPARI-SON OF INTERFERON BETA-1A IN RELAPSING-REMIT-TING MULTIPLE SCLEROSIS:THE EVIDENCE STUDYBever CT, for the EVIDENCE Study Group
P132 THE REGISTRY TO EVALUATE NOVANTRONE®
(MITOXANTRONE FOR CONCENTRATE INJECTION)EFFECTS IN WORSENING MS (RENEW): STATUSREPORT SEPTEMBER 2002 Goodkin DE, Flanders K, Leung J, Butine M, Stead R
P133 THE EFFECT OF INTERFERON B-1B ONQUANTITIES DERIVED FROM MT MRI IN SECONDARYPROGRESSIVE MS Inglese M, vanWaesberghe J, Rovaris M,Beckmann K, Barkhof F, Hahn D, Kappos L, Miller D, Polman C,Pozzilli C,Thompson A,Yousry T,Wagner K, Comi G, Filippi M
P134 SINGLE CENTRE, DBPC, RANDOMISED TRIALOF INTERFERON BETA 1B IN PRIMARY PROGRESSIVEAND TRANSITIONAL PROGRESSIVE MULTIPLE SCLERO-SIS:AN EXPLORATORY PHASE II STUDY Montalban X,Brieva L,Tintore M, Borras C, Rio J, Nos C,Aymerich X, Alonso J,Horno R,Vicente M, Rovira A
P135 IFN BETA CHRONIC TREATMENT: HOW TOMANAGE THE DOSE AND THE FREQUENCY OFADMINISTRATION IN PATIENTS WITH ABSENCE OFDISEASE ACTIVITY Pipieri A, Barbero P, Bergui M,Verdun E,Clerico M, Durelli L
Poster Session I: Thursday, September 19
43
New Clinical Trials (Part 1) (continued)
P136 3 TESLA MAGNETIC RESONANCE IMAGINGCOMPARISON OF INTERFERON BETA-1B AND GLATI-RAMER ACETATE—A RANDOMIZED, SINGLE-BLINDSTUDY IN RELAPSING-REMITTING MULTIPLE SCLERO-SIS Wolansky LJ, Cadavid D, Cook SD, Skurnick J, Biswal B,Pachner A, Hill J
Genetics (Part 1)
P137 A SCANDINAVIAN GENOME-WIDE LINKAGEDISEQUILIBRIUM SCREEN IN MULTIPLE SCLEROSISPATIENTS INDICATES ASSOCIATION AT 1Q (D1S1601)AND 11Q (D11S1986) Datta P, Harboe H, Spurkland A,Ryder L, Sawcer S, Åkesson E, Celilus E, Modin H, Sandberg-Wollheim M, Myhr K,Andersen O, Hillert J, Solberg Sorensen P,Svejgaard A, Compston A,Vartdal F, Oturai A
P138 -384 INTERLEUKIN-2 POLYMORPHISMS INMULTIPLE SCLEROSIS FernándezV, Leyva L, Mayorga C,Matesanz F, Fedetz M,Alcina A, Guerrero M, León A, Luque G,Fernández O
P139 CTLA-4 GENE POLYMORPHISMS AND THEIRINFLUENCE ON SUSCEPTIBILITY TO MULTIPLE SCLE-ROSIS IN N. IRELAND Heggarty SV, Silversides J, Vanden-broeck K, McDonnell G, Hawkins S, Graham C
P140 ASSOCIATION STUDY OFFAS ANDFASL POLY-MORPHISMS WITH MULTIPLE SCLEROSIS Kantarci OH,Hebrink DD, Achenbach SJ, Elizabeth AJ, McMurray CT, Wein-shenker BG
P141 ANALYSIS OF A NOVEL INTRAGENIC SINGLE-NUCLEOTIDE POLYMORPHISM OF THE FAS GENE INRELAPSING MULTIPLE SCLEROSIS Lucas M, Zayas MD,Costa AF, Solano F, Durán E, Izquierdo G
P142 GENOMIC SCREENING IN SPANISH PATIENTSWITH MULTIPLE SCLEROSIS Goertsches R,Villoslada P,Comabella M, Montalban X, Gomez-de-la-Concha E,Arroyo R,Lopez de Munain A, Otaegui D, Palacios R, Spanish M
P143 RANTES AND CHEMOKINE RECEPTOR 5POLYMORPHISMS: SUSCEPTIBILITY TO AND OUTCOMEIN MULTIPLE SCLEROSIS Partridge JM, Fryer A, Ollier W,Boggild M, Strange R, Hawkins C
P144 POLYMORPHISM IN THE GLUTATHIONE S-TRANSFERASES, GSTA1 AND GSTA2, IN MULTIPLESCLEROSIS Partridge JM, Fryer A, Boggild M, Strange R,Hawkins C
P145 MMP-9 MICROSATELLITE POLYMORPHISMINCREASES THE RISK OF MULTIPLE SCLEROSIS Fiotti N,Zivadinov R, Altamura N, Nasuelli D, Bratina A,Tommasi MA,Bosco A, Locatelli L, Grop A, Cazzato G, Giansante C, Zorzon M
P146 HLA TYPING IN MULTIPLE SCLEROSIS. RELA-TION TO MAGNETIC RESONANCE IMAGING FIND-INGS Zivadinov R, Uxa L, Zacchi T, Nasuelli D, Ukmar M,Furlan C, Pozzi-Mucelli RS,Tommasi MA, Locatelli L, Ulivi S,Bratina A, Bosco A, Grop A, Cazzato G, Zorzon M
P147 APOE GENOTYPE IS NOT ASSOCIATED WITHCLINICAL DISEASE CHARACTERISTICS AND MRI FIND-INGS IN MULTIPLE SCLEROSIS Zwemmer J, van Veen T,van Winsen L, van Kamp G, Barkhof F, Polman C, Uitdehaag B
Immunotherapy (Part 1)
P148 MITOXANTRONE THERAPY IN PROGRESSIVEMULTIPLE SCLEROSIS A∂�a∂�lu J, Emir C, Gur M, Morali S,Tanik O
P149 IMMUNE REGULATORY EFFECTS OF GLATI-RAMER ACETATE (GA) ON HUMAN MONOCYTES:BYSTANDER SUPPRESSION REVISITED? Kim H,Duddy M, Bar-Or A
P150 BIOAVAILABILITY OF THREE INTERFERON�PREPARATIONS: A 96 HOURS TIME-COURSE STUDYBertolotto A, Capobianco M, Di Sapio A, Gilli F, Sala A,Malucchi S, Milano E, Melis F, Bottero R
P151 USE OF INTERFERON BETA 1B IN SEC-ONDARY PROGRESSIVE MULTIPLE SCLEROSIS INARGENTINA Carra AJ, Sinay V, Onaha P,Alvarez F, Ballario C,Caceres F, Cristiano E, Deri N, F. Liguori N, Luetic G, Garcea O,Palacio S, Patrucco L, Reich E, R. Escalante R, Sotelo H,Tarulla A,Vetere S
P152 RELAPSING REMITTING MULTIPLE SCLEROSISTHERAPY EXPERIENCE IN ARGENTINA Carra AJ,Onaha P, Sinay V,Alvarez F, Luetic G, Bettinelli R, Sanpedro E,Rodriguez L
P153 BBR2778,A NEW NON-CARDIOTOXIC DRUGSTRUCTURALLY RELATED TO MITOXANTRONE,REDUCES THE SEVERITY OF RAT ACUTE ANDCHRONIC EXPERIMENTAL ALLERGIC ENCEPHALO-MYELITIS Cavaletti G, Frigo M, Rota S, Stanzani L,Tredici G,Dassi M, Perseghin P, Lolli F, Mazzanti B, Biagioli T, Ballerini C,Cavalletti E, Pezzoni G, Sala F, Crippa L, Di Luccio E, Sala V,Oggioni N, Riccio P
P154 MITOXANTRONE-INDUCED IMMUNOLOGI-CAL CHANGES IN PERIPHERAL BLOOD LEUKOCYTESOF MS-PATIENTS Chan A,Weilbach FX,Toyka KV, Gold R
P155 EPITOPE SPECIFICITY OF NEUTRALIZINGANTIBODIES AGAINST INTERFERON-BETA Gneiss C,Reindl M, Berger T, Deisenhammer F
P156 IMMUNOMODULATORY THERAPIES IN FAMIL-IAL MULTIPLE SCLEROSIS Eraksoy M,Turan N, Kurtuncu M,Kyyat A,Yapici Z,Akman-Demir G
P157 CAMPATH-1H IN THE TREATMENT OF MULTI-PLE SCLEROSIS PATIENTS Le Page E,Amanda Louise C,Coles A, Denys V, Miller D, Hale G,Waldmann H, Compston A
P158 INTERFERON BETA INHIBITS MONOCYTE-DERIVED DENDRITIC CELL MATURATION McClurg AE,Fleming EM, Hawkins SA, Duddy ME, McQuaid S, Johnston JA,Armstrong MA
P159 INTERFERON BETA-1A VERSUS INTERFERONBETA-1B IN RELAPSING MS: 4-YEAR CLINICAL EFFI-CACY RESULTS Patti F, Fiorilla T, Florio C,Vivo P, Reggio A
P160 SAFETY AND TOLERABILITY OF CYCLOPHOS-PHAMIDE PULSES IN MULTIPLE SCLEROSIS Portaccio E,Zipoli V, Siracusa G, Piacentini S, Sorbi S, Ponziani G,Amato M
P161 EXPERIENCES WITH MITOXANTRONE TREAT-MENT—SIDE EFFECTS IN SECONDARY CHRONICPROGRESSIVE MULTIPLE SCLEROSIS PATIENTS Rajda C,Bencsik K,Török M,Vécsei L
P162 INTERFERON BETA DOSE REDUCTION INMULTIPLE SCLEROSIS PATIENTS: IMMUNOLOGICALPROFILE Ricci A,Verdun E, Oggero A, Barbero P, Cucci A,Clerico M, Pipieri A, Bosio A, Durelli L
P163 A PHASE IIB STUDY OF ORAL INTERFERONBETA-1A AT TWO DOSES IN RELAPSING REMITTINGMULTIPLE SCLEROSIS USING MRI, CLINICAL ANDIMMUNOLOGIC MEASURES VollmerTL, Preiningerova J,Markovic-Plese S, Rizzo M, Cutter G
P165 SERUM PARAOXONASE ACTIVITY INUNTREATED AND IFN-BETA TREATED MS PATIENTSDanni M,Viti B, Bacchetti T, Ferretti G, Splendiani G, Fiè A,Angeleri V, Ceravolo M, Provinciali L
P166 METALLOTHIONEIN EXPRESSION IN THECENTRAL NERVOUS SYSTEM OF MULTIPLE SCLEROSISPATIENTS Espejo C, Martinez-Caceres EM, Penkowa M,Ortega A, Hidalgo J, Montalban X
P167 ALPHA-SYNUCLEIN IMMUNOREACTIVEDEPOSITS IN MULTIPLE SCLEROSIS LESIONS Paramo D,Izquierdo G, Seilhean D
Poster Session I: Thursday, September 19
44
Rehabilitation and Quality of Life
P168 PRESSURE PAIN IN MULTIPLE SCLEROSISPATIENTS Armutlu K, Kerem M, Bumin G,Akbayrak T,Yigiter K, Keser I, Karabudak R
P169 ASSESSMENT OF RELATION BETWEEN HAND-ICAP STATUS AND QUALITY OF LIFE IN AMBULATORYMULTIPLE SCLEROSIS PATIENTS IN TURKEY Armutlu K,Guclu A, Cetisli N, Bosnak M, Karabudak R
P170 QUALITY OF LIFE, DISABILITY AND DEPRES-SION IN EARLY MS Deloire-Grassin M, Ouallet J, Salort E,Barroso B, Brochet B
P171 AEROBIC TRAINING IN MULTIPLE SCLERO-SIS—INFLUENCE ON METABOLIC, ENDOCRINE ANDQUALITY OF LIFE PARAMETERS Heesen C, Gold SM,Mladek M, Bartsch K, Hartmann S, Ludwig A,Witte J, Reer R,Braumann K, Schulz K
P172 ONE-YEAR CHANGES ON THE MS FUNC-TIONAL COMPOSITE AND PATIENT-PERCEIVED DIS-ABILITY Hoogervorst E, Kalkers N, Uitdehaag B, Polman C
P173 HIGH LEVELS OF ANXIETY AND DISTRESS IN MS PATIENTS AND THEIR PARTNERS IN THE FIRSTYEARS AFTER DIAGNOSIS Janssens C, van Doorn P,de Boer J, van der Meche F, Passchier J, Hintzen R
P174 THE MULTIPLE SCLEROSIS QUALITY OF LIFEINVENTORY AND DISABILITY AS MEASURED BY THEEDSS: EXPERIENCE IN A BRAZILIAN MULTIPLE SCLERO-SIS SAMPLE Lana-Peixoto MA,Araujo CR, Haase VG,Lacerda SS, Lima EP
P175 PREVIOUS HISTORY OF OPTIC NEURITIS AS AFACTOR FOR DECREASED VISION-SPECIFIC QUALITYOF LIFE IN MULTIPLE SCLEROSIS Lana-Peixoto MA, Mar-tins R, Haase VG, Lacerda SS
P176 ASSESSING THE VALIDITY OF THE MULTIPLESCLEROSIS IMPACT SCALE IN A COMMUNITY BASEDPOPULATION McGuigan C, McCarthy A, Hutchinson M
P177 THE RELATION OF HEALTH RELATED QUAL-ITY OF LIFE AND SUBJECT DISCONTINUATION IN APHASE 3 CLINICAL TRIAL Miller DM, Cohen JA,Tsao EC,Kooijmans MF
P178 AN OBJECTIVE FOLLOW-UP OF UPPER LIMBFUNCTION IN MULTIPLE SCLEROSIS Nisipeanu P,Hocherman S, Hardan Y, Inzelberg R
P179 THE RELATION BETWEEN DECONDITION,RESPIRATORY MUSCLE WEAKNESS AND FATIGUE INMULTIPLE SCLEROSIS Øasová K, Havrdová E, Brandejsky P,Rùûièka J
P180 CORRELATION BETWEEN “FUNCTIONALSYSTEMS” OF EXPANDED DISABILITY STATUS SCALEAND HEALTH RELATED QUALITY OF LIFE:ANALYSISOF 184 MULTIPLE SCLEROSIS PATIENTS Idiman E, Özak-bas S,Yozbatiran N, Uzunel F, Oguz M, Kürsad F
P181 CROSS-CULTURAL ADAPTATION AND VALI-DATION OF MULTIPLE SCLEROSIS QUALITY OF LIFEQUESTIONNAIRE (MSQOL-54) IN TURKISH MULTIPLESCLEROSIS POPULATION Idiman E, Uzunel F, Özakbas S,Yozbatiran N, Oguz M, Callioglu B, Gökce N, Bahar Z
P182 QUALITY OF LIFE FOR MS PATIENTS: REFER-ENCE STANDARDS FROM A LARGE PANEL OFPATIENTS Pierre C, DIDIER V, Laurent G, Maryline L,Dominique A,Aurélien M
P183 FRONTAL SYNDROME AND QUALITY OF LIFEIN MS PATIENTS Pierre C, Didier D, Delphine L, Céline T,Florence B, Laurent G
P184 PREDICTION OF QUALITY OF LIFE INSEVERELY DISABLED MS-PATIENTS Ritter SB, Ladurner G,Wranek U
P185 QUALITY OF LIFE AND COST OF ILLNESS INMITOXANTRONE TREATED MULTIPLE SCLEROSISPATIENTS VollmerTL, Hadjimichael O, Buenconsejo J
P186 EVOLUTION OVER A 3 MONTH PERIOD OFGLOBAL, PSYCHOLOGICAL,AND SOCIO-PROFES-SIONAL FUNCTIONING IN PATIENTS WITH RELAPS-ING REMITTING MULTIPLE SCLEROSIS, DURINGAVONEX® TREATMENT INITIATION Warter J, Gentin M
P187 SITUATION OF MEDICAL CARE OF PATIENTSWITH MULTIPLE SCLEROSIS IN NORTH-EASTERNGERMANY Zettl UU, KrügerT
Symptomatic Management
P188 GLATIRAMER ACETATE [GA] TREATMENTSHAVE SIGNIFICANT EFFECTS ON CONTROLLINGFATIGUE-INDUCED TREMOR AMPLITUDE IN MULTIPLESCLEROSIS PATIENTS Dogan S, Konopacki R, Brooks BR
P189 OSTEOPOROSIS IN MULTIPLE SCLEROSISPATIENTS TREATED WITH CORTICOSTEROIDSHavrdova E,Tyblova M, Stepan J, Zikan V, Horakova D,Ticha V,Novakova I
P190 BOTULINUM TOXIN IN THE TREATMENT OFDETRUSOR HYPERREFLEXIA IN MULTIPLE SCLEROSIS:CASE REPORT Hradilek P, Krhut J, Zapletalova O, Mainer K
P191 SPASTICITY IN MS PATIENTS IN THE NAR-COMS REGISTRY: PREVALENCE, SEVERITY AND TREAT-MENT PATTERNS USING ORAL AGENTS AND/ORINTRATHECAL BACLOFEN Rizzo M, Hadjimichael O,Buenconsejo J, Preiningerova J,Vollmer T
P192 VARIABILITY IN THE QUALITIES OF CHRONICNEUROPATHIC PAIN IN MULTIPLE SCLEROSIS ASSESSEDBY THE NEUROPATHIC PAIN SCALE (NPS) Rog DJ,Young CA
P193 BURDEN OF NEUROPATHIC PAIN IN MSRog DJ,Young CA
P194 FATIGUE ASSESSMENT BY MECHANICAL ANDMYOELECTRICAL OUTPUT DURING SUSTAINED MAX-IMAL ISOMETRIC VOLUNTARY CONTRACTION INMULTIPLE SCLEROSIS Sanjak M, Belden D, Konapacki R,Waclawik AJ, Brooks BR
P195 GLATIRAMER ACETATE TREATMENT EFFECTON MUSCLE STRENGTH IN MULTIPLE SCLEROSISPATIENTS.A PROSPECTIVE LONGITUDINAL MS CLINIC-BASED STUDY Sanjak M, Belden D, Konapacki R, Brooks BR
Clinical Aspects of MS (Part II)
P196 PREDICTIVE FACTORS TO SECONDARY PRO-GRESSIVE MULTIPLE SCLEROSIS POINT OUT THEPOTENTIAL IMPORTANCE OF THE INFLAMMATORYPROCESS Coustans M, Le Duff F,Taurin G, Le Page E, Leray E,Edan G
P197 MULTIPLE SCLEROSIS ASSOCIATED WITH SYS-TEMIC MASTOCYTOSIS:A SINGLE CASE REPORTCristina Z, Carlo F
P198 PREDICTIVE VALUE OF THE ONE-YEAR CLINI-CAL RESPONSE TO BETA-INTERFERON IN RELAPSING-REMITTING MULTIPLE SCLEROSIS Etienne R, Iliu-Florin T,Dominique P, Jean-Christophe O, Claire G, Olivier H
P199 EFFICACY OF MS THERAPY IS KEY DRIVER INTHERAPY CHOICE Eyring S,Wood C, Sherman S, Simone M
P200 CORRELATION BETWEEN VISUAL EVOKEDPOTENTIALS ABNORMALITIES AND PHYSICAL HANDI-CAP PROGRESSION IN MULTIPLE SCLEROSIS: PROSPEC-TIVE FOLLOW-UP OF 65 PATIENTS Ferriby D,Ardnt C,de seze j, Stojkovic t, Hache J,Vermersch P
P201 IMPAIRED SYMPATHETIC ACTIVITY INPATIENTS WITH MULTIPLE SCLEROSIS AND FATIGUEFlachenecker PM, Rufer A, Bihler I, v. Hippel C, Reiners K,Toyka KV, Kesselring J
P202 MEASURING THE OUTCOME OF INTERFERONTHERAPY FROM THE PATIENTS’ PERSPECTIVE Ford HL,Johnson MH, Denton S
P203 COAGULATION ABNORMALITIES IN MULTI-PLE SCLEROSIS AND POSSIBLE MULTIPLE SCLEROSISGalgani S, Corsi F, Corpetti M, Pingi A, Manni M, Gasperini C
P204 THE RANGE OF INFLAMMATORY MYEL-OPATHIES. CLINICAL, MRI,CEREBROSPINAL FLUID ANDIMMUNOLOGICAL FINDINGS IN 35 CONSECUTIVECASES Perini P, Calabrese M,Tiberio M,Tzintzeva E,Ranzato F, Gallo P
P205 FATIGUE AND AXONAL LOSS IN CORPUSCALLOSUM IN MULTIPLE SCLEROSIS Greg C, Minier D,Walker P, Brunotte F, Giroud M, Moreau T
P206 CLOMIPHENE CITRATE CAN INCREASERELAPSE RATE IN MULTIPLE SCLEROSIS Moreau T,Gere J, Greg C,Vernay D, Clavelou P, Giroud M
P207 ACUTE DISSEMINATED ENCEPHALO-MYELOPATHY AND PERIPHERAL NEUROPATHYASSOCIATED WITH CHRONIC HCV INFECTIONGiannesini C, Schelp C, Heinzlef O, Roullet E
P208 SAPHO SYNDROME ASSOCIATED WITH MUL-TIPLE SCLEROSIS Giannesini C, Mahfoud A, Heinzlef O,Aouba A, Roullet E
P209 MITOXANDRONE FOR PROGRESSIVE TYPE OFMULTIPLE SCLEROSIS TREATMENT Giannoulis C, Sarafia-nos A, Hatzidaki G, Kargadou A, Stavropoulos D, Karageorgiou KE
P210 ACTIVE HUMAN HERPESVIRUS SIX (HHV-6)INFECTIONS AND MS Knox K, Carrigan D
P211 CLINICAL, DEMOGRAPHIC,AND COGNITIVEFEATURES OF CHILDHOOD ONSET MULTIPLE SCLE-ROSIS Krupp LB, Belman AL, Cianciulli C, Milazzo M, Blitz K,Morgan T, Melville P
P212 CORRELATION OF THE GUYS NEUROLOGI-CAL DISABILITY SCALE WITH THE EDSS IN A SAMPLEOF BRAZILIAN MULTIPLE SCLEROSIS PATIENTS Lana-Peixoto MA,Araújo CR, Haase VG, Lacerda S, Lima EP
P213 ACUTE DEAFNESS REVEALING MULTIPLESCLEROSIS Lebrun C, de Seze J, Bourg V, Soriani M,Vermersh P, Chatel M
P214 MULTIPLE SCLEROSIS WITH HYPERSIGNAL-FREE T2-WEIGHTED MRI Lebrun C, Bourg V, Chanalet S,Soriani M, Chatel M
P215 PROGNOSIS IN RELAPSING-REMITTING MUL-TIPLE SCLEROSIS.A HIERARCHICAL MODEL Martínez-Yélamos S, Casado V, Carmona O, Martínez-Yélamos A,Ramón JM, Arbizu T
Poster Session II: Friday, September 20
45
Clinical Aspects of MS (Part II) (continued)
P216 CLINICAL ISOLATED MYELITIS: EARLY PREDIC-TION OF MULTIPLE SCLEROSIS BASED ON MAGNETICRESONANCE IMAGING AND CEREBROSPINAL FLUIDFINDINGS Meluzinova E, Bojar M, Houzvickova E, Glosova L,Belsan T
P217 COLLABORATIVE STUDY ON CHILDHOODONSET MULTIPLE SCLEROSIS IN FRANCE (KIDMUS):ABOUT A COHORT OF 495 PATIENTS Mikaeloff Y, Tar-dieu M, Catherine L, Edan G, Vallee L, Ponsot G, Confavreux C
P218 PATTERNS OF MS TREATMENT WITH DISEASEMODIFYING THERAPIES BEFORE ENTRY INTO ANOPEN-LABEL CLINICAL TRIAL OF REBIF® INJECTIONSMikol D, Burns T, Bennett S, Lopez-Bresnahan M
P219 FATIGUE IN MULTIPLE SCLEROSIS.A LONGI-TUDINAL STUDY Tellez N, Rio J,Tintore M, Sastre-Garriga J,Pericot I, Nos C, Montalban X
P220 RELAPSING MYELITIS:A DEMYELINATINGSYNDROME DISTINCT FROM MULTIPLE SCLEROSISNicholas R, Fletcher N, Boggild M
P221 HAEMATOLOGICAL ABNORMALITIES RELATEDTO INTERFERON BETA-1A THERAPY O’Connor P,O’Brien F,Alsop J, Chang P, Grumser Y, and Abdalla J
P222 OPTIC NEURITIS: CORRELATION OF CLINI-CAL,VISUAL FIELD AND NEUROIMAGING FINDINGSAND THEIR PROGNOSTIC ROLE Paschalidou M, Geor-giadis N, Haritanti A, Doskas T, Parissis D, Poulios G, Halvatzis N,Xinou E, Drevelegas A, Dimitriadis AS, Milonas I
P223 ASSOCIATION OF UVEITIS AND MULTIPLESCLEROSIS COULD INFLUENCE THE CLINICALCOURSE OF MULTIPLE SCLEROSIS PatrickV, Jean-yves G,Pierre L, Didier F, Tanya S, Albert V, Jérôme D
P224 THE EFFECT OF CORTICOSTEROID ON CON-DUCTION IN THE VISUAL PATHWAYS.A SERIAL STUDYUSING VISUAL PSYCHOPHYSICS Pye EM,Weatherby SJ,Kesson D, Foster DH, Hawkins CP
P225 A COMPARISON OF BILATERAL SIMULTANE-OUS AND BILATERAL SEQUENTIAL OPTIC NEURITISUSING VISUAL PSYCHOPHYSICS Pye EM,Weatherby SJ,Kesson D, Foster DH, Hawkins CP
P226 PHYSICAL ACTIVITY AND FATIGUE IN MULTI-PLE SCLEROSIS PATIENTS INITIATING INTERFERONBETA-1A THERAPY Riskind P, Brown V, Kevin K
P227 COURSE AND PROGNOSIS IN EARLY ONSETMULTIPLE SCLEROSIS Simone IL, Carrara D,Tortorella C,Liguori M, Lepore V, Pelligrini F, Bellacosa A, Ceccarelli A, Pavone I,Girolamo F, Livrea P
P228 MS PHENOTYPE:AN AGE-DRIVEN DISEASE?Vukusic S,Adeleine P, Gignoux L, Durand-Dubief F, Renoux C,Achiti I, Blanc S, Confavreux C
P229 NEUROGENIC SYNCOPE IN MULTIPLE SCLERO-SIS PATIENTS Zapletalova O, Dolezil D, Hradilek P, Stipal R
Imaging (Part II)
P230 CORRELATION BETWEEN BRAIN ATROPHYAND APOLIPOPROTEIN E GENOTYPES IN PATIENTSWITH EARLY RELAPSING-REMITTING MULTIPLE SCLE-ROSIS Amato M, Mortilla M, Bartolozzi M, Nacmias B, ZipoliV, Siracusa G, Cellini E, Bagnoli S, Guidi L, Lambruschini P, Sorbi S,Federico A, De Stefano N
P231 THE RELATION BETWEEN BRAIN MRILESIONS AND DEPRESSIVE SYMPTOMS IN MULTIPLESCLEROSIS BeneöováY, Niedermayerová I, Mechl M
P232 DISABILITY AND AXONAL LOSS IN EARLYRELAPSING AND REMITTING MULTIPLE SCLEROSIS.ASSESSMENT WITH MSFC AND H1-MRS Casanova B,Martinez C,Valero C, Celda B, Matí-Bonmatí L, Pascual A, Coret F
P233 EARLY CORTICAL ATROPHY IN RELAPSINGREMITTING AND PRIMARY PROGRESSIVE MULTIPLESCLEROSIS AND ITS RELEVANCE TO OTHER MR ANDCLINICAL MEASURES De Stefano N, Matthews PM,Filippi M, Iannucci G, De Luca M, Bartolozzi ML, Guidi L,Ghezzi A, Montanari E, Federico A, Smith S
P234 1H-MAGNETIC RESONANCE SPECTROSCOPYIN CORTICAL GREY MATTER, HIPPOCAMPUS ANDTHALAMUS OF HEALTHY SUBJECTS AT 1.5 T—A REPRO-DUCIBILITY STUDY Geurts JJ, Barkhof F, Castelijns JA, Pol-man CH, Pouwels PJ
P235 INCREASED GLUTAMATE/GLUTAMINE LEVELSMEASURED BY 1H-MRS IN MULTIPLE SCLEROSIS BRAINGreenstein JI, Luo J, Kanamalla US, Smith SA, Niman D, Boyko OB
P236 GLOBAL MAGNETIC RESONANCE SPEC-TROSCOPY METABOLIC VARIATIONS AS INDICATORSOF DISEASE ACTIVITY IN RELAPSING REMITTINGMULTIPLE SCLEROSIS Inglese M, Rusinek H, Babb JS,Grossman RI, Gonen O
P237 PROTON MAGNETIC RESONANCE SPEC-TROSCOPY EVIDENCE FOR EARLY GRAY MATTERINVOLVEMENT IN RELAPSING REMITTING MSInglese M, Ge Y, Filippi M, Falini A, Grossman RI, Gonen O
P238 BRAIN VOLUME CHANGES AFTER SUPPRES-SION OF MRI-VISIBLE INFLAMMATION IN PATIENTSWITH SECONDARY PROGRESSIVE MS TREATED WITHAUTOLOGOUS STEM CELL TRANSPLANTATIONInglese M, Mancardi G, Murialdo A, Marrosu M, Meucci G, Mas-saccesi L, Lugaresi A, Pagliai F, De Stefano N, Saccardi R, Filippi M
P239 COGNITIVE AND EMOTIONAL STATUS IN APOPULATION OF PATIENTS PRESENTED WITH CLINI-CALLY ISOLATED SYNDROMES SUGGESTIVE OF MULTI-PLE SCLEROSIS Jean P,Virginie L, Florence R, Bertrand A, JeanPhilippe R, Sylviane C,Andre A, Patrick C
P240 NEURAL SUBSTRATES UNDERLYING PERFOR-MANCE OF A CONTROLLED MOTOR TASK INPATIENTS WITH MULTIPLE SCLEROSIS Kadom N, Mor-gen K, Sawaki L,Tessitore A, Ohayon J, Frank J, McFarland H,Martin R, Cohen LG
P241 INTERCAUDATE NUCLEUS RATIO (ICR) IN MSPATIENTS AS A LINEAR MEASURE OF BRAIN ATROPHYKhan O, Zvartau-Hind M, Caon C, Ching W, Lisak R,Tselis A
P242 CEREBRAL ATROPHY IN SECONDARY PRO-GRESSIVE MULTIPLE SCLEROSIS: EFFECT OF INTRA-VENOUS IMMUNOGLOBULINS Lin X,Turner B, Constan-tinescu C, Blumhardt LD, Fazekas F, Filippi M, Hommes OR
P243 CORRELATES OF MAGNETIZATION TRANS-FER IMAGING METRICS IN PRIMARY PROGRESSIVEMULTIPLE SCLEROSIS Rovira A, Brieva L,Aymerich X,Borras C,Tintore M,Alonso J, Montalban X
P244 DISSEMINATION IN SPACE IN BRAINSTEMSYNDROMES Sastre-Garriga J,Tintore M, Rovira A, Nos C,Pericot I, Rio J,Thompson AJ, Montalban X
P245 COMPUTER ASSISTED VOLUMETRIC ANALYSISOF GADOLINIUM ENHANCEMENT IN MULTIPLE SCLE-ROSIS Preiningerova J, Ding Z, Cannistraci C, Sun H, Vollmer T,Anderson A
P246 COMPARISON OF CEREBRAL PERFUSION INMULTIPLE SCLEROSIS USING A NOVEL TECHNIQUERashidW, Parkes L, Ingle G, Chard D, Symms M, Miller D
P247 FUNCTIONAL CORTICAL CHANGES INPATIENTS WITH MULTIPLE SCLEROSIS AND NON-SPECIFIC CONVENTIONAL MAGNETIC RESONANCEIMAGING SCANS OF THE BRAIN Rocca MA, Pagani E,Ghezzi A, Falini A, Zaffaroni M, Colombo B, Scotti G, Comi G,Filippi M
P248 THE ROLE OF SPINAL CORD DAMAGE ONBRAIN CORTICAL PLASTICITY:A FUNCTIONAL MAG-NETIC RESONANCE IMAGING STUDY Filippi M,Rocca MA, Mezzapesa DM, Ghezzi A, Falini A, Martinelli V,Poggi A, Scotti G, Comi G
P249 SHORT-TERM CORRELATIONS BETWEENCLINICAL AND MRI FINDINGS IN RELAPSING-REMIT-TING MULTIPLE SCLEROSIS Filippi M, Rovaris M,Rocca MA, Ladkani D, Shifroni G,Wolinsky JS, Comi G
P250 PROTON MAGNETIC RESONANCE SPEC-TROSCOPY IN FAMILIAL AND SPORADIC MS Siger-Zajdel M, Selmaj K
P251 A COMPARISON OF DIFFERENT QUANTITA-TIVE MRI TECHNIQUES TO MEASURE WHOLE BRAINATROPHY IN RELAPSING-REMITTING MULTIPLE SCLE-ROSIS Zivadinov R, Bakshi R, Grop A, Sharma J, Bratina A,Kuwata JM, Nasuelli D,Tjoa CW, Zorzon M
P252 REGIONAL BRAIN PARENCHYMAL ATROPHYMEASURES IN MULTIPLE SCLEROSIS Locatelli L,Zivadinov R, Bratina A, Nasuelli D, Grop A, Zorzon M
P253 SHORT-TERM BRAIN ATROPHY CHANGES INRELAPSING-REMITTING MULTIPLE SCLEROSIS Zivadi-nov R, Bagnato F, Nasuelli D, Bastianello S, Bratina A, Finamore L,Locatelli L, Catalan M, Clemenzi A, Grop A, Millefiorini E, Zorzon M
P254 MRI MEASURES IN RELAPSING-REMITTINGMULTIPLE SCLEROSIS.A SHORT-TERM OBSERVATIONSTUDY Nasuelli D, Bagnato F, Zivadinov R, Bratina A, Bastia-nello S, Finamore L, Locatelli L, Grop A, Di Pofi B, Millefiorini E,Zorzon M
Immunology (Part II)
P255 NEW CANDIDATES IN MULTIPLE SCLEROSISIDENTIFY BY AN ANALYSIS OF IGG REPERTOIRE COU-PLED WITH A PROTEOMIC APPROACH ALMERAS L,Lefranc D, Drobecq H, de Seze J, Dubucquoi S,Vermersch P, Prin L
P256 IMMUNOPATHOGENIC AND CLINICAL RELE-VANCE OF ANTIBODIES AGAINST MOG IN MULTIPLESCLEROSIS BergerT, Egg R, Rubner P, Hochfilzer A,Lutterotti A, Schanda K, Deisenhammer F, Reindl M
P257 DECRYPTING THE SPECIFICITY OF THEINTRATHECAL IGG RESPONSE IN PATIENTS WITHMULTIPLE SCLEROSIS BY PROTEIN ARRAY TECHNOL-OGY Cepok S, Stei S, Sommer N, Hemmer B
P258 PREVALENCE OF HERPESVIRUS DNA IN MSPATIENTS DaskalovskaVA, Daskalovski ZV, Petkova-Boskovska T
P259 SEQUENTIAL STUDY OF SERUM SEX HOR-MONES AND TH1/TH2 CYTOKINE BALANCE DURINGAND AFTER RELAPSE OF MULTIPLE SCLEROSIS San-chez-Ramon S, Rodriguez-Saiz C, Lozano N, Resino S, Munoz C,Rodriguez-Mahou M, Muñoz-Fernández M, de Andrés C
P260 CHEMOKINE RECEPTOR EXPRESSION ON TCELLS IS RELATED TO NEW LESION DEVELOPMENT INMULTIPLE SCLEROSIS Eikelenboom MJ, Killestein J, Izeboud T,Kalkers NF, van Lier RA, Barkhof F, Uitdehaag BM, Polman CH
Poster Session II: Friday, September 20
46
Immunology (Part II) (continued)
P261 SEVERE URTICARIA AS REACTION TO INTER-FERON-�-1A ADMINISTRATION Fazio MC, Mazzeo L,Buccafusca M, Dattola V, Scalfari A, Ferlazzo E, Girlanda P,Messina C
P262 A 4-MONTH LONGITUDINAL STUDY ON THERELATIONSHIP BETWEEN CLINICAL ACTIVITY ANDBETA2-MICROGLOBULIN EXPRESSION IN MULTIPLESCLEROSIS Finamore L, Zivadinov R, Cecchinelli D, Pichi A,Nasuelli D, Pierallini A, Bratina A, Locatelli L, Grop A, Reale M,Zorzon M, Millefiorini E
P263 LONGITUDINAL STUDY OF SPONTANEOUSAND INDUCED APOPTOSIS IN LYMPHOCYTES OFPATIENTS WITH RELAPSING-REMITTING AND SEC-ONDARY-PROGRESSIVE MS TREATED WITH INTER-FERON BETA-1B Garcia-Merino A, Diaz D, Bacenilla H,Prieto A,Alvarez-Mon M
P264 SPONTANEOUS EX-VIVO AND MITOGEN-INDUCED APOPTOSIS ARE INCREASED IN SEVERALLYMPHOCYTE SUBSETS OF PATIENTS WITH RELAPS-ING-REMITTING AND SECONDARY-PROGRESSIVE MSGarcia-Merino A, Diaz D, Barcenilla H, Prieto A,Alvarez-Mon M
P265 INTERFERON BETA-1A REGULATES G PRO-TEIN COUPLED RECEPTORS IN MONONUCLEARCELLS FROM HEALTHY DONORS AND MULTIPLE SCLE-ROSIS PATIENTS Giorelli M, Livrea P, Defazio G, Ricchiuti F,Mola A, Di Monte E,Trojano M
P267 CROSS-REACTIVE ANTIBODIES AGAINSTMYELIN BASIC PROTEIN, ACINETOBACTER SP. ANDPSEUDOMONAS AERUGINOSA IN MULTIPLE SCLERO-SIS Hughes LE, Bonell S,Wilson C, Smith P,Amor S, Ebringer A
P268 THE PLASMA LEVELS OF ALPHA-2-MACROGLOBULIN AND THE TRANSFORMED FORMARE SIGNIFICANTLY DIFFERENT BETWEEN PATIENTSWITH MULTIPLE SCLEROSIS AND CONTROLSJensen PH, Datta P, Jorgensen S, Oturai AB, Sorensen PS
P269 LOW MOLECULAR WEIGHT GLYCOCONJU-GATES IN BRAIN HAVE IMMUNOREGULATORY ACTIV-ITY Lindsey JW,Waxham MN, Stephens NE,Weiser S
P270 LEVELS OF SAPO-1/FAS IN THE SERUM OFMULTIPLE SCLEROSIS PATIENTS BEFORE AND AFTERSTEROID TREATMENT Mitosek-Szewczyk K, Bartosik-Psujek H, Belniak E, Dobosz B, Stelmasiak Z
P271 UPREGULATED SURVIVIN EXPRESSION INACTIVATED T LYMPHOCYTES CORRELATES WITHDISEASE ACTIVITY IN MULTIPLE SCLEROSIS Noori M,Sharief MK
P272 DYSREGULATION OF PROGAMMED CELLDEATH ACTIVATION IN MULTIPLE SCLEROSIS PATIENTSSaresella M, Clerici M,Trabattoni D, Speciale L, Piacentini L,Caputo D, Ferrante P
P273 THE EXPRESSION OF CD5 ON PERIPHERAL BLYMPHOCYTES CORRELATES WITH DISEASE ACTIVITYIN PATIENTS WITH MULTIPLE SCLEROSIS Seidi OA,Sharief MK
P274 GLUCOCORTICOID SENSITIVITY IN PATIENTSWITH MULTIPLE SCLEROSIS Winsen Lv, Muris D, Dijkstra C,Polman C, van den Berg T, Uitdehaag B
Neuropsychology
P275 SCREENING FOR EARLY COGNITIVE IMPAIR-MENT IN MULTIPLE SCLEROSIS PATIENTS USING THECLOCK DRAWING TEST BarakY,Achiron A
P276 QUANTITATIVE MRI AND NEUROPSYCHO-LOGICAL ASSESSMENT IN 48 RR-MS PATIENTS BresciaMorraV, Lanzillo R, Brunetti A, Salvatore E, Schiavone V, Quaran-telli M, Coppola G, Orefice G
P277 COGNITIVE PERFORMANCES ARE ALTERED INEARLY MULTIPLE SCLEROSIS Salort E, Deloire-Grassin M,Boudineau M, Ouallet J, Barroso B,Arese P,Verley C, Fabrigoule C,Leteneur L, Brochet B
P278 PACED AUDITORY SERIAL ADDITION TESTAND MAGNETIC RESONANCE IMAGING FINDINGS IN MULTIPLE SCLEROSIS PATIENTS. PRELIMINARYSTUDY Callegaro D, Fuso S, Otaduy M, Costa M, Lacerda M,Bacheschi L, Leite C, Bueno O
P279 COGNITIVE SCREENING OF MS PATIENTSRECRUITED FOR A CLINICAL TRIAL Christodoulou C,Krupp LB, Melville P, Scherl W, Morgan T, McIlree C
P280 COGNITIVE FUNCTIONS IN MULTIPLE SCLE-ROSIS PATIENTS TREATED WITH INTERFERON-BETA:A CONTROLLED TWO YEAR FOLLOW-UP STUDYDanni M,Viti B, Splendiani G, Giambartolomei S,Arabi S, Pro-vinciali L, Ceravolo G
P281 COGNITIVE IMPAIRMENT IN ACTIVE MULTIPLESCLEROSIS de Seze J, Bouillaguet S, Dubois G, Cabaret M,Ferriby D, Dujardin K,Vermersch P
P282 EMOTIONAL ADJUSTMENT IN PATIENTSWITH MULTIPLE SCLEROSIS Pires-Barata S, Henriques I
P283 SUCCESSFUL ADULT DEVELOPMENT AS AFRAMEWORK FOR NEUROPSYCHOLOGICAL COUN-SELING IN MULTIPLE SCLEROSIS Lana-Peixoto MA,Haase VG, Lacerda SS, Lima EP
P284 DEVELOPMENT OF THE BRAZILIAN VERSIONOF THE MULTIPLE SCLEROSIS FUNCTIONAL COMPOS-ITE MEASURE: RESULTS FROM A PILOT STUDY Lana-Peixoto MA, Haase VG, Lacerda S, Lima EP
P285 BECK DEPRESSION INVENTORY AND GEN-ERAL HEALTH QUESTIONNAIRE: RESULTS OF A COM-PARISON BETWEEN MULTIPLE SCLEROSIS PATIENTSAND CONTROLS Lana-Peixoto MA, Haase VG, Lacerda SS,Lima EP
P286 PSYCHOSOCIAL FUNCTIONING IN MS:PSYCHOMETRIC CHARACTERISTICS OF SELF-REPORTED MEASURES EMPLOYED IN BRAZILLana-Peixoto MA, Haase VG, Lacerda SS, Lima EP
P287 PSYCHOSIS IN MULTIPLE SCLEROSIS Nieder-mayerová I, Beneöová Y, Mechl M
P288 THE EFFECT OF INTERFERON BETA ON THE COGNITIVE DYSFUNCTION OF 100 IRANIANPATIENTS WITH MULTIPLE SCLEROSIS (MS) Pak-daman H, Pakdaman R
P289 HOPELESSNESS IN MULTIPLE SCLEROSISPatten SB, Metz LM
P290 COGNITIVE DYSFUNCTION IN MULTIPLESCLEROSIS Petkovska-BoskovaT, Daskalovska V, Bojkovski V
P291 A CROSS-SECTIONAL STUDY OF 21 NEWLYDIAGNOSED, RELAPSE-REMITTING MULTIPLE SCLERO-SIS PATIENTS WITH PET, MRI AND TESTS OF COGNI-TIVE FUNCTIONS TscherningT, Mathiesen HK, Jonsson A,Blinkenberg M, Rostrup E, Larsson HB, Paulson OB, SoelbergSorensen P
Experimental Allergic Encephalomyelitis (Part II)
P292 DETECTION OF MAGNETICALLY LABELEDENCEPHALITOGENIC T-CELLS IN EXPERIMENTALAUTOIMMUNE ENCEPHALOMYELITIS (EAE) BY CELLU-LAR MAGNETIC RESONANCE IMAGING Anderson SA,Shukaliak-Quandt J,Arbab SA, Jordan EK, Martin R, McFarland HF,Frank JA
P293 EXPRESSION OF THE ACTIVATION MARKERUROKINASE PLASMINOGEN ACTIVATOR IN CNSMICROVASCULAR PERICYTES IN EXPERIMENTALAUTOIMMUNE ENCEPHALOMYELITIS Dore-Duffy P,Balabanov R,Wagnerova J,Washington R
P294 TREATMENT OF EXPERIMENTAL AUTOIM-MUNE ENCEPHALOMYELITIS WITH INTRAVENOUSIMMUNOGLOBULIN Humle Jørgensen S, Laursen H,Soelberg Sørensen P
P295 SUSCEPTIBILITY TO T CELL-MEDIATED CEN-TRAL NERVOUS SYSTEM INFLAMMATION MODU-LATED BY NON-MYELIN-SPECIFIC T CELLS Jones RE,Kay T,Wilkins D,Tsaknaridis L, Bourdette D
P296 AXONAL PROTECTION BY FLECAINIDETHERAPY IN EAE Bechtold DA, Kapoor R, Smith K J
P297 A SYNTHETIC ANDROSTENE DERIVATIVEWITHOUT GENDER-RELATED SIDE EFFECTS INHIBITSEAE. CANDIDATE FOR CLINICAL TRIALS IN MS?Offner H, Zamora A, Matejuk A,Auci D, Morgan E, Reading C
P298 THE ROLE OF THE MHC CLASS II TRANSACTI-VATOR (CIITA) IN CLASS II EXPRESSION AND ANTIGENPRESENTATION BY ASTROCYTES AND IN SUSCEPTIBIL-ITY TO CNS AUTOIMMUNE DISEASE Stuve O,Youssef S,King CL, Patarroyo JC, Brickey JW, Piskurich JF, Chapman HA,Zamvil SS
P299 TREOSULFAN IN MYELIN-OLIGODENDRO-CYTE-GLYCOPROTEIN-INDUCED EXPERIMENTALAUTOIMMUNE ENCEPHALOMYELITIS: POTENTIALNEW TREATMENT FOR MULTIPLE SCLEROSIS Weissert R,Pfrommer H,Wiendl H, Baumgart J, Melms A, Sass G,Weller M
Healthcare Systems
P300 COST-BENEFIT AND COST-EFFECTIVENESSANALYSIS OF INTERFERON BETA-1A 44MCG TIW,VER-SUS INTERFERON BETA-1A 30MCG QW, IN RELAPSING-REMITTING MULTIPLE SCLEROSIS (RRMS) Beresniak A,Martin M
P301 A RELAPSE OF MULTIPLE SCLEROSIS: HOWMUCH DOES IT COST IN CATALONIA? CasadoV, Mar-tinez-Yelamos S, Martinez-Yelamos A, Carmona O, Hernandez J J,Arbizu T
P302 AN AUDIT OF HEALTH SCREENING ISSUES INMS PATIENTS IN GENERAL PRACTICE Hawkins SA,Maclurg K,Whittington D, Evason E, Reilly PM
P303 THE ECONOMIC BURDEN OF RELAPSE INMULTIPLE SCLEROSIS: DIRECT MEDICAL COSTS PEREPISODE IN THE UNITED STATES O’Brien J, Patrick A,Duran P, Caro J
P304 BURDEN OF NURSING CARE FOR HOSPITAL-IZED PATIENTS WITH MULTIPLE SCLEROSIS Tissot E,Rumbach L, Limat S, Berger E, Monnin C, Lavier A,Woronoff-Lemsi M
Poster Session II: Friday, September 20
47
Healthcare Systems (continued)
P305 THE NEW ZEALAND BETA-INTERFERON PRO-GRAM. AN APPROACH TO EQUITABLE PROVISION OFTREATMENT FOR MS WHERE FUNDING IS RESTRICTEDWilloughby EW,Abernethy DA,Wright AR,Anderson NE
New Clinical Trials (Part II)
P306 THE INDEPENDENT COMPARISON OF INTER-FERON (INCOMIN) TRIAL: MRI ANALYSIS OF THE NEWPROTON DENSITY/T2 LESIONS Durelli L, Pipieri A,VerdunE, Barbero P, Incomin G
P307 BETAFERON®/BETASERON® (INTERFERONBETA-1B) IN EARLY TREATMENT OF MULTIPLE SCLERO-SIS:THE BENEFIT STUDY Freedman M, Edan G, Hartung H,Kappos L, Miller D, Montalban X, Polman C, Bauer L, Ghazi M,Sandbrink R
P308 PLACEBO-CONTROLLED DOUBLE-BLINDEDDOSE RANGING STUDY OF FAMPRIDINE-SR IN MULTI-PLE SCLEROSIS Goodman AD, Blight A, Cohen JA, Cross AH,Katz M, Rizzo MA,Vollmer T
P309 DISABILITY AND QUALITY OF LIFE (FLAIRSTUDY) AND NEUROPSYCHOLOGY (COBRA STUDY)IN RELAPSING MS PATIENTS Jongen P, Carton H, Sindic C,Tinbergen J,Wesnes K, FLAIR S
P310 TREATMENT OF EAE AND MS BY RAISINGSERUM URATE LEVELS THROUGH ADMINISTRATIONOF INOSINE Spitsin S, Hooper D, Scott GS, Koprowski H
P311 INTERFERON-� TREATMENT IN RELAPSING-REMITTING MULTIPLE SCLEROSIS: RESULTS OF ANOBSERVATIONAL STUDY IN SOUTHERN ITALY Tro-jano M, Paolicelli D, Liguori M, Zimatore G,Avolio C, Lavolpe V,Ruggieri M, Livrea P
P312 A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED STUDY OF INTRAVENOUS IMMUNEGLOBULINS (IVIG) IN COMBINATION WITH INTRA-VENOUS METHYLPREDNISOLONE (MP) IN THE TREAT-MENT OF RELAPSES IN PATIENTS WITH MULTIPLESCLEROSIS (MS) Visser LH, Beekman R,Tijssen CC, Uitde-haag BM, Movig C, Lenderink B
P313 EFFECTS OF INTERFERON BETA-1B DOSETITRATION ON EFFICACY AND TOLERABILITYWroe S
Genetics (Part II)
P314 TUMOR NECROSIS FACTOR RECEPTOR IIPOLYMORPHISM IN PATIENTS WITH MULTIPLE SCLE-ROSIS Ehling R, Gassner C, Fazekas F, Kollegger H, Kristo-feritsch W, Reindl M, Berger T
P315 ANTIBODY RESPONSE TO MYELIN OLIGO-DENDROCYTE GLYCOPROTEIN AND MYELIN BASICPROTEIN DEPEND ON FAMILIAL BACKGROUND ANDARE PARTIALLY ASSOCIATED WITH HUMAN LEUKO-CYTE ANTIGEN ALLELES IN MULTIPLEX FAMILIES ANDSPORADIC MULTIPLE SCLEROSIS Lutterotti A, Reindl M,Gassner C, Poustka K, Schanda K, Deisenhammer F, BergerT
P316 LACK OF ASSOCIATION BETWEEN CTLA-4GENE POLYMORPHISMS AND MULTIPLE SCLEROSIS INSARDINIAN PATIENTS Cocco EE, Fadda EE, Rolesu MM,Melis CC, Solla EE, Schirru LL, Costa GG, Murru MM, Murru RR,Marrosu MM
P317 A49G CTLA-4 GENE POLYMORPHISM IN SAR-DINIAN PATIENTS WITH MULTIPLE SCLEROSIS ANDTYPE 1 DIABETES Cocco EE, Fadda EE, Rolesu MM, Melis CC,Solla EE, Schirru LL, Fadda LL, Sanna S, Marrosu MM
P318 INFLUENCE OF MHC/HLA ALLELES IN MULTI-PLE SCLEROSIS CLINICAL VARIABLES Cocco EE, Fadda E,Rolesu M, Melis C, Solla E, Costa G, Murru M, Murru R, Fadda L,Marrosu MM
P319 A GENOME-WIDE LINKAGE SCREEN IN TURK-ISH MULTIPLEX FAMILIES WITH MULTIPLE SCLEROSISEraksoy M, Kurtuncu M, Sawcer SJ,Akesson E,Akman-Demir G,Compston AD,Turkish Multiple Sclerosis Genetics Study Group
P320 MOLECULAR ANTHROPOLOGICAL VIEW IN APOPULATION ANALYSIS OF BRAZILIAN INDIVIDUALSDURING A MULTIPLE SCLEROSIS GENETIC STUDY OFHLA DRB1-DQB1-DQA1 Leon SV, Alvarenga RP, Caballero A,Alonso A, Fernandez O
P321 HISTOCOMPATIBILITY CLASS II DR*, DQ*, DP*ANTIGENS ASSOCIATION WITH MULTIPLE SCLEROSISIN A POPULATION OF THE RIO DE JANEIRO CITY,BRAZIL Santos CC, Emmerick M, Liem AM, Frugulhetti I,Leon SV, Quirico-Santos T
P322 PRIMARY ASSOCIATION OF A TUMORNECROSIS FACTOR GENE POLYMORPHISM WITH MSSUSCEPTIBILITY Rafael A,Virginia D,Alfonso M,Ana R,Miguel F, Xavier M, Emilio G
P323 MHC GENE MODULATING MS SUSCEPTIBILITYCONFERRED BY HLA-DRB1*1501 Rafael A, Virginia D,Alfonso M, Ana R, Xavier M, Emilio G
P324 IL10 GENE AND RESPONSE TO IFN BETA IN MSde las Heras V, Rafael A, Martínez A, Rubio A, G de la Concha E
P325 ASSOCIATION OF APOLIPOPROTEIN E ANDMYELOPEROXIDASE GENOTYPES WITH THE CLINICALCOURSE OF FAMILIAL AND SPORADIC MULTIPLE SCLE-ROSIS Zakrzewska-Pniewska B, Podlecka A, Styczynska M,Samocka R, Peplonska B, Barcikowska M, Kwiecinski H
Immunotherapy (Part II)
P326 RAPID ONSET MITOXANTRONE-INDUCEDCARDIO TOXICITY IN SECONDARY PROGRESSIVEMULTIPLE SCLEROSIS Avasarala JR, Cross AH, Clifford DB,Siegel B,Abbey EE
P327 ANTI MOG AND ANTI MBP ANTIBODY SUB-CLASSES IN MULTIPLE SCLEROSIS PATIENTS DURINGINTERFERON BETA THERAPY Khalil M, Reindl M, Lutte-rotti A, Egg R, Schanda K, Deisenhammer F, BergerT
P328 GLATIRAMER ACETATE (GA)-REACTIVE T-CELLS PRODUCE BRAIN DERIVED NEUROTROPHICFACTOR (BDNF) Chen M, Dhib-Jalbut S
P329 IMPORTANCE OF CONTINUOUS IMMUNO-MODULATORY TREATMENT IN MULTIPLE SCLEROSISCsépányT, Csiba L
P330 EFFECT OF ORAL GLATIRAMER ACETATE(COPAXONE) IN MULTIPLE SCLEROSIS: REDUCTIONOF INTERFERON GAMMA PRODUCTION de Seze J,Dubucquoi S, Lefranc D, Almeiras L, Dutoit V, Clavelou P, Edan G,Hautecoeur P, Prin L, Vermersch P
P331 A RETROSPECTIVE COMPARATIVE ANALYSISON THE EFFICACY OF THREE INTERFERON BETATREATMENTS IN MULTIPLE SCLEROSIS Giray S, Demir-kiran M, Sarica Y
P332 CLINICAL AND MRI IMPACT OF MITOX-ANTRONE IN 111 SECONDARY PROGRESSIVE MULTI-PLE SCLEROSIS PATIENTS GregoryT, Emmanuelle L,Emmanuelle L, Eric S, Marc C, Gilles E
P333 NEUTRALIZING ANTIBODIES TO INTER-FERON BETA-1B AND THERAPEUTIC RESPONSE INMULTIPLE SCLEROSIS PATIENTS Hernández-Regadera J J,Bas-Minguet J,Arbizu-Urdiain T
P334 LONG-TERM TOLERABILITY OF INTERFERONBETA-1A IN RELAPSING-REMITTING MULTIPLE SCLE-ROSIS: 6-YEAR SAFETY FOLLOW-UP OF THE PRISMSSTUDY Kappos L, Stam Moraga M
P335 ALGORITHM FOR LONG-TERM TREATMENTOF EARLY MULTIPLE SCLEROSIS Koehler J,Wicht S,Hey W, Holger S
P336 THE BRAZILIAN EXPANDED CONSENSUS ONTREATMENT OF MULTIPLE SCLEROSIS Lana-Peixoto MA,Callegaro D, Moreira MA, Marchiori PE, Lino A, Gabbai AA,Souza AM, Campos GB, Rocha FC, Gama PD, tosta E,Ataide L,Brito L, Bacheschi LA
P337 INDUCTION TREATMENT WITH MITOX-ANTRONE DURING 6 MONTHS IN WORSENINGRELAPSING REMITTING MULTIPLE SCLEROSIS:A RES-CUE THERAPY FOR SUB-OPTIMAL RESPONDERS TOINTERFERON BETA? A PILOT STUDY Le Page E, Leray E,Coustans M,Taurin G, Chaperon J, Edan G
P338 IN VIVO EFFECT OF INTERFERON-�1A ONINTERLEUKIN-12 AND TRANSFORMING GROWTHFACTOR-�1 CYTOKINES IN PATIENTS WITH RELAPS-ING-REMITTING MULTIPLE SCLEROSIS Losy JJ,Michalowska-Wender G
P339 INTERLEUKIN 18 IS MODIFIED DURING THER-APY WITH GLATIRAMER ACETATE (COPAXONE) INPATIENTS WITH RELAPSING-REMITTING MULTIPLESCLEROSIS Losy JJ, Michalowska-Wender G,Wender M
P341 EXPRESSION OF CHEMOKINES AND CHEMO-KINE RECEPTORS BY GLATIRAMER ACETATE-REACTIVET-CELL LINES Neuhaus O, Bartosik-Psujek H, Kieseier BC,Wiendl H, Hartung H
P342 ACUTE MYELOID LEUKAEMIA (AML) INDUCEDBY MITOXANTRONE RaduTD, Marc D, Herve V
P343 GLATIRAMER ACETATE AS AN IN VITRO TOOLTO FOLLOW THE LONG-TERM EFFECT OF IMMUNO-MODULATORY THERAPIES ON T CELL RESPONSES INPATIENTS WITH MULTIPLE SCLEROSIS Schmied M,Reindl M,Auff E,Vass K
P344 REDUCED EXPRESSION OF THE INHIBITOROF APOPTOSIS PROTEINS IN T CELLS FROM PATIENTSWITH MULTIPLE SCLEROSIS FOLLOWING INTER-FERON-BETA THERAPY SemraYK, Sharief MK
P345 THE EFFECT OF LIVER TRANSPLANT COMBI-NATION IMMUNOSUPPRESSION ON MULTIPLE SCLERO-SIS AFTER 18 MONTHS Vorobeychik G,Yoshida E, Prout A
Giorelli M, P265Giovannoni G, 48, P11, P12Giray S, P331Girlanda P, P31, P261Girolamo F, P227Giroud M, P205, P206Gisevius A, P105Giuliani F, 17Glosova L, P216Gneiss C, P155Go A, P111Gober H, P164Goebels N, 16Goertsches R, P142Gökce N, P181Gold L, P52Gold R, 41, P154Gold SM, P34, P171, P266Gomez-de-la-Concha E, P142,
P324Gonen O, P7, P236, P237Goodkin DE, P132Goodman A, P5, P14, P15, P86,
P308Graham C, P139Greene C, 60Greenstein JI, P235Greg C, P205, P206Gregora E, 43Gregory T, P332Grekova M, 60Griffin C, P73, P85, P12Grive E, 51Grop A, P6, P145, P146, P251,
P252, P253, P254, P262Grossman R, 29Grossman RI, P7, P236, P237Grumser Y, P221Guclu A, P169Guerrero A, P35Guerrero M, P138Guerrero R, P54Guglielmo A, P13Guidi L, P230, P233Guillet M, 2Gur M, P148Gutierrez A, P26
Powell AW, P340Pozzilli C, P133Pozzi-Mucelli RS, P146Prakhova L, P88Prat A, 33Prat E, 1Preiningerova J, P163, P191, P245Prieto A, P263, P264Prin L, P255, P330Prout A, P345Provinciali L, P165, P280Prucha M, P1Pruvo J, P25Pryce G, 48Puerta C, P112Pujol-Borrell R, 1Pye EM, P224, P225
Quarantelli M, P276Quirico-Santos T, P95, P321
Radü E, 9Radu TD, P42, P342Rafael A, P127, P128, P322, P323,
P324Raine CS, 14, 38Rajda C, P161Ramo C, P82Ramón JM, P215Ranjeva J, P69Ransohoff RM, 34Ranzato F, P13, P204Rashid W, P12, P73, P246Rausch M, 9Ravid R, 15Reading C, P297Reale M, P6, P262Redekop G, P80Redmond it, P83Reer R, P171Reggio A, P159Reich E, P151Reichert-Scrivner S, 10Reilly PM, P302Reindl M, P4, P155, P256, P314,
P315, P327, P343Reiners K, P201Rejdak K, P12Rene A, P42Renoux C, 64, P68, P74, P228Resino S, P259Revenco E, P43Ricchiuti F, P265Ricci A, P162Riccio P, P153Richard P, P23Richert JR, 60Richert N, 8, 10Rieckmann P, P78Rinaldi L, P13Rio J, 51, P65, P134, P219, P244Risch N, 56Riscoe M, P109Riskind P, P226Ritter SB, P184
Rivera V, P52Rizzo M, P163, P191Rizzo MA, P308Roberto Á, P127, P128Rocca MA, 7, P247, P248, P249Rocha FC, P67, P336Rodegher M, 7Rodriguez L, P152Rodriguez-Mahou M, P259Rodriguez-Saiz C, P259Roed H, P101Roelke K, P20Rog DJ, P192, P193Rolesu MM, P316, P317, P318Ropele S, 6Ross C, 24, 60Rossi B, P111Rossi P, 62Rostrup E, P79, P291Rota S, P153Rotondi M, P3Roullet E, P207, P208Rovaris M, P133, P249Rovira À, 51, P10, P134, P243,
P244Rubio A, P324Rubner P, P256Rudick R, 12, 66, P100Rufer A, P201Ruggieri M, P311Ruiz C, 2Ruiz-Peña J, P56Rumbach L, P23, P43, P304Rus H, 39Rusinek H, P236Rùûièka J, P179Ryder L, P137
Sá PN, P59Saccardi R, P238Sadovnick D, 56Sala A, P150Sala F, P153Sala V, P153Salort E, P170, P277Salvatore E, P276Samocka R, P325Sánchez A, P112Sanchez E, 51Sanchez-Ramon S, P259Sandberg-Wollheim M, P137Sandbrink R, P307Sandoval G, P66Sandrock A, 66, P5, P86Sanjak M, P20, P194, P195Sanna S, P24, P317Sanpedro E, P152Sant’Anna G, P95Santos CC, P95, P321Santos MA, P124Sarafianos A, P209Saresella M, P272Sarica Y, P331Sartori E, P49Sass G, P299
Wilson C, P267Wilt S, 42Winsen Lv, P274Winter R, P109Wintterle S, P107Witte J, P171Witte T, P28Wolansky LJ, P136Wolinsky JS, 50, P249Wood C, P199Work Group on Standardized
MRI Protocol P81Woronoff-Lemsi M, P304Wranek U, P184Wright AR, P305Wroe S, P313Wuerfel J, 10Wullf H, 49
Xavier M, P322, P323Xinou E, P222
Yapici Z, P30, P156Yayla V, P18, P48Ydiman E, P99Ydiman F, P99Yeager M, P97Yigiter K, P168Yong V, 17, 35, P117Yoshida E, P345Young CA, P192, P193Yousry T, P133Youssef S, P298Yozbatiran N, P180, P181Yun S, 49
Zacchi T, P146Zaffaroni M, P32, P33, P247Zakrzewska-Pniewska B, P325Zamora A, P297Zamvil SS, P298Zapletalova O, P96
LB1
VALIDATION OF DIAGNOSTIC MRI CRITERIA FOR MS AND RESPONSETO TREATMENT WITH INTERFERON-BETA-1A
Barkhof Fb, Rocca Mc, Francis Gd, van Waesberghe Jb, Uitdehaag Bb, Hommes Oe, Hartung Hf,Durelli Lg, Edan Gh, Fernández Oa, Seeldrayers Pi, Sorenson Pj, Margrie Sk, Comi Gc, Filippi Mc,b
aMS-MRI centre,VU medical centre, Amsterdam, Europe, Netherlands; bIRCCS San Raffaele,Milan, Italy; cSerono Laboratories, Rockland, Massachusetts, USA; dEuropean Charcot Founda-tion, Nijmegen, Netherlands; eKarl-Franzens Universität, Graz, Austria; fUniversity of Turin,Turin,Italy; gUniversité de Rennes, Rennes, France; hHospital Carlos Haya, Malaga, Spain; iC.H.U. deCharleroi, and Hôpital Erasme, Brussels, Belgium; jRigshospitalet, Copenhagen, Denmark;kQuintiles Pty Limited, Sydney, Australia
Background: In the recently adopted diagnostic criteria for MS by McDonald, the modifiedcriteria of Barkhof have been adopted.Objectives:To prospectively test the validity of the modified Barkhof criteria and their pre-dictive value for IFN-beta-1a treatment response in the ETOMS studyMethods: The ETOMS study was a randomised, double-blind, placebo-controlled study ofIFN-beta-1a (i.m.) once weekly in 309 patients with a first episode consistent with demyeli-nating disease. Baseline MRI was assessed for the presence of gadolinium-enhancement (or9 T2 lesions), juxtacortical, infratentorial, and 3 periventricular lesions. Conversion to CDMSwas used as the outcome parameter.Results: Conversion to CDMS occurred in 41% of patients with gadolinium-enhancementor 9 T2 lesions versus 11% of those without (p�0.017); similar comparisons were 44% vs.31% for infratentorial (p�0.026), 40% vs. 35% for juxtacortical (p�0.413), and 41% vs. 17% formore than 3 periventricular lesions (p�0.034). For the cumulative number of modified Bark-hof criteria, the rate of conversion to CDMS was 25% for 1 abnormal criterion, rising to 47%with 4 abnormal criteria. For a cut-off of 3 positive criteria, the hazard ratio for time to CDMSwas 2.3 (95% CI 1.17-4.56, p�0.016).While the effect of treatment seemed most evident inpatients with 4 abnormal criteria, statistically significant treatment by variable interactioncould not be detected. However, the number of patients needed to treat decreases from 50with 2 or less criteria to 5.6 with 4 positive criteria.Conclusions:This study confirms the validity of the modified Barkhof criteria for conversionto CDMS, and suggests that treatment with IFN-beta-1a is more cost-effective in patientswith more abnormal criteria.
Disclosure: Most authors were consultants to SeronoFunding: Supported by the European Charcot Foundation and Serono
LB2
ANTI-MOG ANTIBODIES PREDICT EARLY CONVERSION TO CLINICALLYDEFINITE MS IN PATIENTS WITH A FIRST DEMYELINATING EVENT.
Berger Ta, Rubner Pa, Schautzer Fb, Egg Ra, Ulmer Hc, Mayringer Ia, Dilitz Ea, DeisenhammerFa, Reindl Ma
aNeurology, University of Innsbruck, Innsbruck,Austria; bNeurology, County Hospital,Villach,Austria;cBiostatistics, University of Innsbruck, Innsbruck,Austria
Background: 90% of MS patients present at onset with a clinically isolated syndrome (CIS).Although up to 80% of these patients will convert to clinically definite MS (CDMS), the fur-ther MS disease course is unpredictable at onset for individual patients.Objectives: New neuropathological findings, e.g. antibody-mediated demyelination, and theconcept of epitope spreading in the early disease phase, prompted us to investigate whetherthe presence of serum anti-MOG and anti-MBP antibodies (abs) in patients with CIS predictsthe further disease course.Methods: 103 consecutive patients with a CIS, confirmed by MRI and positive oligoclonalbands in CSF, were included and followed for at least 12 months.Anti-MOG and anti-MBPabs were measured as previously described (Reindl et al, 1999).Results: 73 females and 30 males (mean age at disease onset: 32.0 years; mean disease dura-tion: 50.9 months, range 12–96 months). 22 patients (21%) had serum abs against MOG andMBP, 42 (41%) were seropositive for anti-MOG abs only, and 39 (38%) were seronegative.Relapses occurred in only 9 (23%) seronegative patients, but in 95% of patients with absagainst MOG and MBP. Seronegative patients had their first relapse after a mean relapse freeinterval of 45.1 months (range 25–83 months). In contrast, patients with initial seropositiv-ity for anti-MOG and anti-MBP abs developed their first relapse after only 7.5 months (range1–18 months, P<0.001). Quantitation of MRI showed higher mean numbers of T2 and Gd-enhancing T1 lesions in patients with anti-MOG and anti-MBP abs compared to seronegativepatients. However, the number of MRI lesions varied in individual patients, irrespective of theirantibody status, from 2 to >9 T2 lesions and 0 to 4 Gd-enhancing T1 lesions.Conclusions: Analysis of antibodies against MOG and MBP in patients with CIS representa rapid, unexpensive and precise method to identify patients with either a high or low riskfor early conversion to CDMS.This may have implications for counseling and management inpatients with a first demyelinating event suggestive of MS.
Disclosure:T Berger has nothing to disclose.Funding:This work was supported by a grant of the Austrian Federal Ministry of Science (Nr. GZ70.059/2-Pr/4/99).
LB3
NEUROREHABILITATION IN MULTIPLE SCLEROSIS CONTRIBUTES TOFUNCTIONAL RECOVERY ACCOMPANIED BY CHANGES OF BRAINACTIVITY ON FMRI—PRELIMINARY RESULTS.
Rasova K, Krasensky J, Havrdova E, Obenberger J, Zalisova M, Seidl ZDepartment of Neurology, Charles University
Background: Although MS is an inflammatory demyelinating disease, which can lead to theaxonal injury and loss, neurorehabilitation may contribute to functional recovery accompa-nied by the changes in brain activity.Objectives: To show changes in brain activity on fMRI and their correlation with functionalrecovery.Methods: 18 outpatients with MS were evaluated before and after individualized neurore-habilitation treatment (two sessions per week, 30 weeks) for impairment (EDSS), disability(BI), handicap (ESS), quality of life (MSQoL) and amplitude of signal in the primary sensori-motor cortex (ASPSMC) using serial fMRI during the performance repetitive index-thumbopposition.Results:There were 6 men and 12 women, EDSS was 4.19, age 41.11 yrs and illness duration11.5 yrs. 8 patients had relapsing-remitting, 4 primary progressive and 6 secondary progres-sive MS.The therapy led to functional recovery and positively influenced the impairment (EDSSfrom 4.19 to 3.63: p<0,1), the disability (BI from 94.16 to 98.05: p<0.05), the handicap (ESSfrom 7.30 to 4.25: p<0.05) and quality of life (MSQoL from 152.6 to 161.13: trend shown).The functional recovery was accompanied by changes in ASPSMC.There was a trend towardsdecreased ASPSMC after therapy (ASPSMC for right hand from 7.82 to 7.20%, for left handfrom 8.61 to 7.71%).We found two different responses to therapy: in two thirds of patientsthe ASPSMC decreased, while in one third of patients it increased.We have found no rela-tionship between functional recovery and changes in the brain activity. It was shown thatwhen ASPSMC in left hand changed, it changed in right hand as well during the performanceof paradigm (correlation coefficient 0.56).The therapy was not aimed at improving functionof the hands, but control of the whole body. Nevertheless, the function of the hands andASPSMC during the performance of the paradigm changed. It seems that neurorehabilitationinfluences the function of the whole brain.Conclusions:There is very little scientific basis for the therapy that is designed to help dam-aged brain circuits recover.These preliminary results show that neuorehabilitation in MS con-tributes to functional recovery and can be accompanied by changes of brain activity.
Disclosure: K Rasova has nothing to disclose.
LB4
TIGHT JUNCTION ABNORMALITY IN MS AFFECTS ALL CALIBRES OFVESSEL AND CORRELATES WITH LESION ACTIVITY.
Kirk Ja, Plumb Jb, Mirakhur Mb, McQuaid Sb
aPathology, Queen’s University, Belfast, Northern Ireland, United Kingdom; bNeuropathology, RoyalVictoria Hospital, Belfast, Northern Ireland, United Kingdom
Background: Increased blood-brain barrier (BBB) permeability observed in MS has beenlinked to pathological change in the tight junctions (TJ) and vesicular transport of vascularendothelium.Objectives: This study quantifies the pathological changes in TJs which we have recentlyreported in MS, including their uneven distribution and the relation between abnormal TJ andBBB leakage.Methods: Frozen sections from plaque and normal appearing white matter (NAWM) in 14post-mortem(PM) cases of MS were studied together with white matter from 6 neurologicaland 5 normal controls. Using single and double immunofluorescence and confocal microscopythe TJ-associated proteins zonula occludens-1 (ZO-1) and occludin were examined acrosslesion types and tissue categories, and in relation to fibrinogen leakage. Confocal image datasetswere analysed for 2198 MS and 1062 control vessels.Results: Significant differences in the extent of TJ abnormalities (i.e. beading, interruption,absence or redistribution of fluorescence signal, separation or opening of junctions) weredetected between the different lesional types in MS and between MS and control white mat-ter.They were frequent in oil-red O(ORO) + ‘active’ plaques, affecting 42.5% of vessels, butless frequent in ORO- ‘inactive’ plaques (22.8%) or NAWM (13.1%) and in both normal (3.9%)and neurological controls (9.5%).A similar pattern was found irrespective of the size of ves-sels examined. In both NAWM and inactive lesions, dual-labelling showed that those with themost TJ abnormality had the greatest fibrinogen leakage.This was most apparent in activelesions where 41% of vessels showed severe leakage.Conclusions: TJ abnormality affects vessels of all sizes, suggesting a diffusable chemical(?cytokine) cause. It occurs in lesional and non-lesional white matter, being most severe wherethere is evidence of active demyelination. Disruption of TJs, affecting both paracellular andtranscellular pathways probably contributes to the BBB leakage detected in this study.Thefinding of TJ abnormality and BBB leakage in ‘inactive’ lesions points to a failure of effectiveand complete TJ repair or to the continuation of a pathological process. In NAWM it sug-gests either pre-lesional change or white matter damage secondary to remote lesions.
Disclosure: J Kirk has nothing to disclose.Funding: JP is supported by The Irish Brain Research Foundation. Pilot studies were supported bythe MS Society of GB & NI.
56
LATE BREAKING NEWS ABSTRACTS
LB5
SINGLE CENTRE, DBPC, RANDOMISED TRIAL OF INTERFERON� 1B INPRIMARY PROGRESSIVE AND TRANSITIONAL PROGRESSIVE MULTIPLESCLEROSIS:AN EXPLORATORY PHASE II STUDY.
Montalban Xa, Brieva La,Tintore Ma, Borras Ca, Rio Ja, Nos Ca,Aymerich Xb,Alonso Jb,Horno Ra,Vicente Ma, Rovira Ab
Background: Beneficial effects of interferon� have been shown only for patients in therelapsing phase of MS as its role in the treatment of SPMS patients still remains controver-sial.The single phase II randomized controlled trial on PPMS using IFN� 1a(IM) shows no sig-nificant treatment effect on EDSS though some effect on T2 lesion load.Objectives: To investigate safety and efficacy hints of interferon� 1b given to patients withprimary and transitionalprogressive multiple sclerosis (PPMS and TPMS).Methods: 73 patients (49 PPMS, 24 TPMS) with EDSS scores of 3.0 to 7.0, were random-ized to receive 8 million IU of IFN� 1b or placebo every other day, subcutaneously for 2years. Safety parameters including the Ashworth spasticity, Krupp fatigue and DepressionInventory scales and blood tests were performed three monthly. Clinical outcomes (EDSSand MS Functional Composite—MSFC) were also performed three monthly and the Sick-ness Impact Profile six monthly. MRI measures (T2 and T1-weighted brain lesion load, brainparenchymal fraction, active lesions, spinal cord atrophy, MTR and spectroscopy) and neuro-psychological assessment (BRNB) were done annually.Results: Adverse events significantly associated with IFN� included injection-site reaction,flu-like symptoms and lymphopenia. One patient on placebo died of pulmonary infection. In all,96% of the patients reached study end and 93% completed the treatment period.Treatmentgroups were comparable on all baseline variables.The proportion of patients with confirmedprogression measured by EDSS at 3 months was 27.8% in the IFN arm and 37.8% in theplacebo arm (p�0.3135). Statistically significant differences were found for MSFC (PASAT 3”,9-HPT and AI (p�0,03),T2 (p�0.006) and T1 (p�0.001) lesion load and number of activelesions (p�0.005) in favor of the IFN-treated group.Conclusions: IFN� 1b is safe in treating patients with PPMS and TPMS. Our study seems tobe the first indicating a beneficial effect of IFN� in these patients.
Disclosure: X Montalban has nothing to disclose.Funding:Trial supported by Schering España SA (of Schering AG, Germany)
LB6
SUCCESSFUL TREATMENT WITH IFN-�1B IN RR MS PATIENTS IS ASSOCI-ATED WITH AN INCREASE IN THE NUMBER OF IL-10 PRODUCING (REG-ULATORY) CD4 +T CELLS.
van Boxel-Dezaire Aa,b, Smits Ma, Uitdehaag Bb, Polman Cb, Nagelkerken La
aDivision of Immunological and Infectious Diseases,TNO Prevention and Health, Leiden, Nether-lands; bDepartment of Neurology,Vrije Universiteit Medical Center,Amsterdam, Netherlands
Background: Although IFN-� is now widely used for treatment of MS, its mode of actionstill remains unclear; recent studies do not support a shift in the Th1/Th2 balance. In vitrostudies show that type I interferons induce the differentiation of Tregulatory-1 (Tr1) cells andthe survival of CD4+CD25+ T cells, which are both recently described suppressor T cells ableto produce IL-10.Objectives:The aim of the present study was to investigate whether IFN-�1b therapy inducesIL-10 in a general fashion or in a specific (regulatory) T-cell subset only. In addition, it was eval-uated whether differential effects on IL-10 production by peripheral blood monocytes, CD4+
or CD8+ T cells could be correlated with clinical efficacy of IFN-�1b treatment.Methods: Based on EDSS-progression and the number of relapses and steroid interventionsin the 2 years before initiation of IFN-�1b treatment compared with those in the 2 yearsafter initiation of treatment, 24 RR MS patients were classified as responders (15) and non-responders (9). Using intracellular cytokine staining techniques, the effect of IFN-�1b after0, 3 and 6 months of treatment was studied on the number of IL-10 producing CD8+ T cells,CD4+ (CD25+) T cells and monocytes.Results: Numbers of IL-10 producing CD4+ T cells were significantly decreased prior totreatment. Remarkably, after 3 and 6 months of treatment a significant increase in the num-ber of such T cells could be found in the clinical responders only. In contrast, treatmentdecreased numbers of IL-10 producing monocytes in both responders and nonrespondersand did not affect numbers of CD8+ T cells that produced IL-10. In a subgroup of the respon-ders (7 out of 15), the effect of IFN-�1b treatment was also studied on CD4+CD25+ T cells.Notably, a significant increase in the number of IL-10 producing CD4+CD25+ T cells could beobserved after 6 months of treatment.Conclusions: Enhancement of the number of CD4+CD25+ T cells that produce IL-10 may bean important mechanism in the therapeutic effect of IFN-� in RR MS.
Disclosure:A van Boxel-Dezaire has nothing to disclose.Funding: Supported by the Dutch Foundation for the support of MS Research, grant 94-175 MS;The Multiple Sclerosis Center for Research and Care,Amsterdam,The Netherlands
Background:The long and variable course of MS, as well as the individual and unpredictableresponse to currently available immune-modifying treatments require a detailed and stan-dardized patient record. Furthermore, the systematic collection of data on large cohorts ofconsecutive patients may help to correlate clinical information with basic research.Althoughthe development of database programs to monitor MS patients started almost thirty yearsago, no single application has gained widespread use so far.Objectives: To develop a modular electronic patient record supporting both the daily careof patients and the collection of specific information on MS.Methods: MSDS is a SQL (structured query language) database.A multilingual (German, Eng-lish; Italian and Spanish in preparation), graphical user interface allows easy data input andoutput. Client-server architecture optimizes MSDS for using it in local area networks.Results: Since its introduction in 12/2001, MSDS has been distributed to 25 hospitals (16universities).Through MSDS users recorded and managed visiting dates, patient history (com-plaints, relapses), physical examination findings, and results of blood and CSF chemistry, evokedpotentials and MRI. MS diagnosis can be specified according to criteria by Poser (applied auto-matically), by McDonald and by Lublin/Reingold. Clinical scores calculated by MSDS comprisethe EDSS, the MSFC, and the Scripps NRS. In general, data input is standardized (pull-downmenus).Whenever required, specific details can be added as free text. Data consistency iscontrolled by internal check mechanisms. Multiple reports describe the individual diseasecourse, as well as the local patient population. In addition to these built-in features, individ-ual queries can be designed to retrieve specific information. Correspondence to practition-ers is supported by MSDS.Additional features include a pedigree generator, a bio-sample data-base and a study-protocol editor.To support the building of a national MS registry, the presentversion of MSDS automatically keeps a consensus minimal data set of each patient up-to-date. Current users have found MSDS user-friendly and well suited to accurately describe theclinical aspects of MS.Conclusions: MSDS may provide an improved platform for clinical documentation of MSand facilitate international standardization.
Disclosure: M Pette has nothing to disclose.Funding: Supported by Gemeinnuetzige Hertie-Stiftung
Welcome Reception at the Baltimore Marriott Waterfront Hotel700 Aliceanna Street, Phone: 410-385-3000Wednesday, September 18th7:00 pm–9:00 pm
On opening day, the Steering Committee invites allconference delegates to an informal “WelcomeReception” at the Baltimore Marriott WaterfrontHotel. Meet new friends, renew acquaintances, andcongratulate the fine young investigators who pre-sented their research that afternoon.
National Aquarium of BaltimorePier 3 at 501 E. Pratt Street, Phone: 410-576-3800Reception and Buffet DinnerThursday, September 19th7:30 pm–10:30 pm
Begin your evening with a leisurely stroll through the aquariumexhibits, enjoying a glass of wine and selections of hors d’oeuvresalong the way. Dazzling tropical fish, a giant Pacific octopus, electriceels, graceful stingrays, playful puffins, two-toed sloths, red-belliedpiranhas, poison dart frogs and a giant anaconda are among the morethan 10,000 marine and freshwater animals waiting to say hello. Theself-guided tour ends with a candlelight dinner buffet.
B&O Railroad Museum901 W. Pratt Street at Poppleton Street, Phone: 410-752-2490
Reception and Buffet DinnerFriday, September 20th
7:30 pm–10:00 pm
Affiliated with the Smithsonian Institution, the B&O Railroad Museum isdedicated to the preservation and interpretation of American railroading—especially the historic Baltimore and Ohio (B&O) line. You’ll enter themuseum through Mt. Clare Station, built in 1851, and proceed to the 1884Baldwin Roundhouse—a 22-sided room with a 136-foot high ceiling!Dinner and dancing are the order of the evening with the opportunity tostroll through some of the locomotive and artifacts exhibits.
Complimentary round-trip transportation will be available for all social events.
59
Committee Reception and Dinner (by invitation)Baltimore Museum of Industry1415 Key Highway at Lawrence StreetPhone: 410-727-4808Saturday, September 21st7:00 pm–10:00 pm
Next Year’s MeetingsACTRIMS 2003
October 19 San Francisco
8th Annual Meeting of the Americas Committee for Treatment and Research in Multiple Schlerosis
ECTRIMS 2003September 17–20
Milan19th Congress of the European Committee
for Treatment and Research in Multiple Schlerosis
60
An expert source ofMS information for
healthcare professionals
The National MS Society has long been a resource for health professionals providing care to peoplewith multiple sclerosis.The new Professional Resource Center,which houses the most comprehensivelibrary of MS information in the world, offers multidisciplinary expertise on MS disease process andmanagement, opportunities for clinial affiliation, and a range of educational programs and materials.
Physicians are invited to consult via email with MS specialist colleagueswho serve on our Medical Advisory Board:
Allied health professionals are invited to consult via email with MS specialist colleagues:[email protected]
Questions are also welcome at our toll-free number:1-866-MS-TREAT (678-7328)
Visit our website: nationalmssociety.org/PRC.asp
The National Multiple Sclerosis Society proudly introduces the
61
Travel InformationReservation AssistanceTarga Tours can offer discounts with American Airlinesand US Airways, and will also search for the lowest avail-able fare on ANY airline serving Baltimore. A US$20service fee applies.Call toll-free: 1-800-756-7957 (From outside the USAor within the Chicago metro area, call 312-541-0780)Fax: 312-541-0783E-mail: [email protected]: targatours.com
Airport/AirlinesBaltimore/Washington 410-859-7111
International AirportRonald Reagan Washington 703-417-8000
National AirportWashington Dulles International Airport 703-572-2700American Airlines 800-433-7300Frontier Airlines 410-694-6220Southwest Airlines 410-290-7001US Airways 800-428-4322
To the AirportThe Airport Shuttle, Inc. 410-381-2772Baltimore Airport Shuttle 410-821-5387Butler Transportation 410-732-5098BWI Airport Shuttle 800-258-3826
Taxi and Limousine ServicesYellow Transportation 410-727-7300American Limousines, Inc 410-522-0400Carey Limousine/Baltimore 410-880-0999Prime Time Sedan and Limo Service 443-562-0067














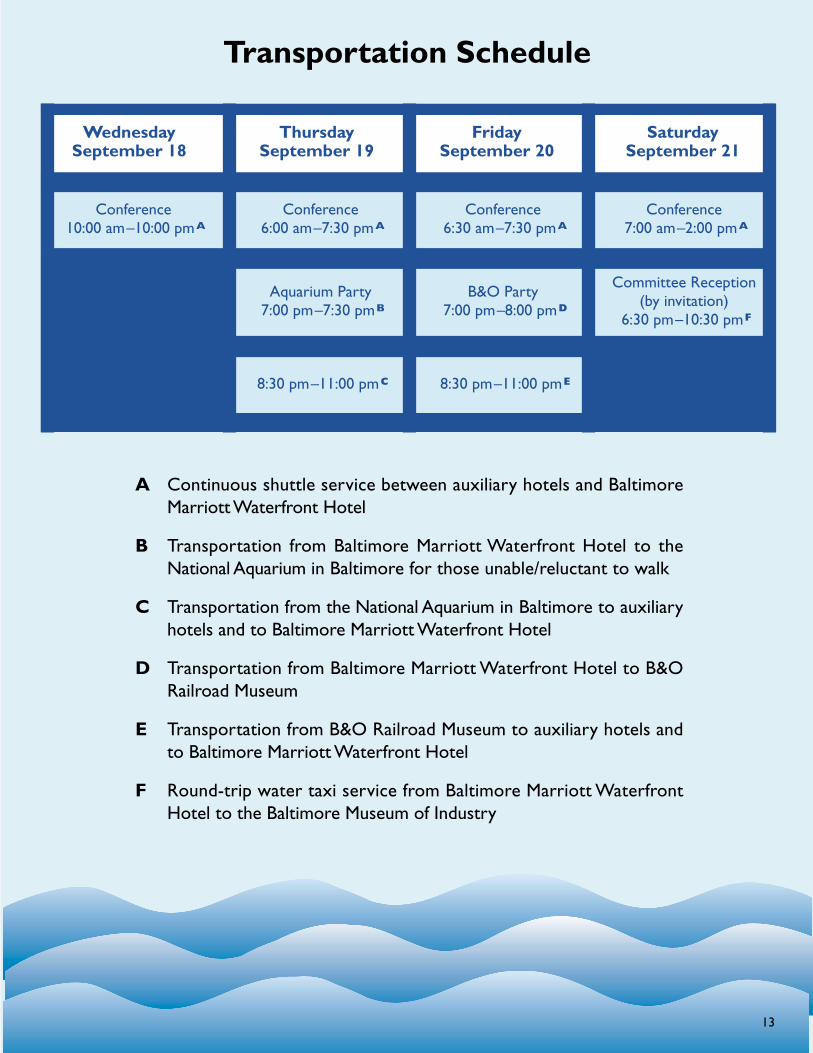
























































![201704 KanuchaResort map · Nov. to March. Beach Counter Beach Volley Court & Beach Futsal [Hours]8:00 am-6:00 pm (Reception close at 5:00 pm) D-4 35 Ext.785 Ext.86 ※ Reception](https://static.documents.pub/doc/80x56/5f5525e090c29f060f113d0d/201704-kanucharesort-map-nov-to-march-beach-counter-beach-volley-court-beach.jpg)





