36
FINAL REPORT FEBRUARY 2018

FINAL REPORT
FEBRUARY 2018

FINAL REPORT FEBRUARY 2018
2
1 Introduction 31.1 Background and rationale for programme 31.2 Programme aims 31.3 Programme Model 41.4 Profile of projects 41.4.1 Belfast Community Sports Development
Network, Belfast, Northern Ireland 41.4.2 Food Academy, East Ham, London 51.4.3 Lanarkshire Community Food and Health
Partnership, North Lanarkshire, Scotland 51.4.4 Nottingham CityCare, Nottingham,
East Midlands 51.4.5 Valley Kids, Rhondda Cynon Taf, Wales 61.4.6 Accord Group, Sandwell, West Midlands 61.5 Evaluation approach and methodology 61.6 Data limitations 81.6.1 Self-report surveys 81.6.2 Measuring levels of physical activity 81.6.3 Evidencing sustainability of change 91.6.4 Contribution not attribution 9
2 Who did the clubs reach? 102.1 Demographic profile 102.2 Families facing challenges 112.3 Baseline health behaviours 112.4 Motivation 12
3 What difference did the clubs make? 133.1 Summary of outcomes 133.2 Eat a little better 133.2.1 Choosing healthy options 133.2.2 Knowing about food and nutrition 153.2.3 Cooking from scratch 163.3 Helping with the budget 173.4 Move a little more 183.5 Sustainability of behavioural changes 193.5.1 Healthy eating 193.5.2 Physical activity 213.6 Social and community outcomes 213.7 Organisational changes/development 22
4 What made the difference? 234.1 Realistic ambition 234.2 Finding a route to the target audience 234.3 Clear and consistent messages 234.4 Practical ways to make healthy changes 244.5 Family focus 244.5.1 Helping to remove barriers 244.5.2 Learning as a family 244.6 The learning environment 254.6.1 Accessibility and familiarity 254.6.2 A relaxed learning space 254.7 Learning together 254.8 Building rapport and trust 254.9 Innovation and adaptability 254.10 Incentives 25
5 What have we learned? 265.1 Development of the model 265.2 Lessons learned 265.2.1 Recruitment and retention 265.2.2 Relationships 275.2.3 The family approach 275.2.4 Delivering the message 275.2.5 Physical activity 275.2.6 Duration and timing 275.2.7 Acknowledgeculturaldifferences 275.3 Strategic added value 285.4 Financial analysis 285.4.1 Cost of pilot programme delivery 285.4.2 Model costs for future delivery 295.5 Sustainability 32 6 Conclusions 336.1 Programme effectiveness 336.2 Critical success factors 336.3 Building a legacy 34
7 Appendix 1: Make, Move & Munch Logic Model 35
Contents

FINAL REPORT FEBRUARY 2018
3
1 Introduction
1.1 Background and rationale for programmeIntheUKtoday,therearearound4millionpeoplewhohaveType 2diabetesandaround7millionliving with heart and circulatory disease. These can be serious life-threatening conditions. This is why Diabetes UK, the British Heart Foundation (BHF) and Tesco came together to form the National Charity Partnership (NCP) in order to inspire millions of people to eat better, get active and reduce their risk of developing these two conditions, both of which are largely preventable.
The NCP was established as a three-year collaboration, to raise vital funds for the two charities as well as delivering programmes across the UK that supported people to live healthier lifestyles. After extensive research, the partnership chose to target their prevention activities towards mums aged 25-40 years who lived in areas of high deprivation, with a secondary audience of children and other family members. The prevention strategy was spread across three key strands of work:
Reach
Engage Support
Let’s Do This
A UK wide social marketing campaign delivering supportive and motivational health messages
Signposting to and delivering local healthy lifestyle programmes in nine areas across the UK, with online support from the Let’s Do This website and 8 Week Challenge
Intensive community programmes Make, Move & Munch Clubs and Beat the Street delivering in six areas of high need across the UK
1.2 Programme aimsThe aim of Make, Move and Munch Clubs (MMMCs formally Holiday Lunch Clubs) was to provide a platform to motivate and incentivise participants to make small and sustainable behavioural changes and achieve a healthier lifestyle. The focus was on eating more healthily and becoming more physically activebymakingsimple,practicalandcost-effectivelifestylechanges.Thekeyplannedoutcomes,forpeople and most at risk communities, included:
Healthy eating
• Eating a more balanced diet• Being able to cook a healthy meal• Having basic knowledge of food labels
Physical activity
• Being more physically active• Feelingconfidenttojoinlocalphysicalactivities• Knowing how to incorporate physical activity into daily life
Social outcomes
• Having increased social and peer support to be more physically active and to eat socially
A full list of the planned outcomes is provided in the programme logic model shown at Appendix 1.
FINAL REPORT FEBRUARY 2018
4
Potentialparticipantswereprofiledasthosewhowantedtoimprovetheirlifestylesbutneededsupport and motivation alongside increased knowledge to be able to improve their own health and thatoftheirfamiliesThemainbarrierstomakingandsustainingchangewereidentifiedascost,timeand childcare commitments. To help overcome these barriers, the MMMCs were delivered at no cost to the participants, with children also being able to attend and take part in activities.
1.3 Programme ModelMake, Move and Munch Clubs were developed to support women and children living in areas of deprivation to live healthier lifestyles in relation to healthy eating and physical activity. The NCP identifiedsixareaswhereincidenceofType 2diabetes,prematuredeathsfromheartandcirculatorydisease and obesity levels were high, particularly among women with young families living in areas of deprivation. The six chosen areas were Belfast, East London, North Lanarkshire, Nottingham, RhonddaCynonTafandSandwell.
Early engagement with local stakeholders resulted in six providers being chosen to deliver MMMC in their respective localities. Each provider was asked to deliver MMMC according the format described below, however local variations did occur and can be read in the relevant regional report.
Each MMMC consisted of eight sessions that families could attend over a period of up to six to twelve months, although a course of eight consecutive weeks was often used. Clubs were delivered during the term time and school holidays at any time of day and at any suitable community locations, with schools becoming the most preferred venue. Sessions of around 1½ to 2½ hours were to include:
• activities that enabled food-based learning, with key messaging about salt, sugar and fat intake as well as portion sizes, delivered through cookery demonstrations, cook-alongs where possible and informal facilitated peer to peer discussions
• entry level and sustainable physical activity for adults • a nutritious meal at each session, to be shared by adults and children • behavioural change techniques to help motivate sustained change in health behaviours
Participants were recruited through a variety of channels including local press articles and advertising, social media and posters placed in community venues. Targeted recruitment, through schools, community-based organisations and exploitation of existing networks were used widely, particularly in the second year. To support retention, participants received a ‘Meal-in-a-Bag’ at least once during the 8 weeks. These were bags of dry ingredients such as herbs or tinned tomatoes, provided by Tesco, whichcouldhelpmaketryingoutnewrecipesathomemoreaffordable.
1.4 Profile of projects Theprogrammemodelasdescribedwasdeliveredbydifferentorganisationsineachofthesixselected areas of the UK. Whilst the core elements of the model remained the same, there were localvariationsinthewayitwasdeliveredtoreflectboththeneedsoflocalcommunitiesandthe infrastructure in each area. This section provides a brief overview of the providers and their approaches to delivering Make, Move and Munch Clubs.
1.4.1 Belfast Community Sports Development Network, Belfast, Northern Ireland
Belfast Community Sports Development Network (BCSDN) delivered MMMCs in Belfast. This organisation uses sport and physical activity to support people and communities across Northern Ireland. They work with numerous partners to deliver programmes in areas of high social deprivation and across community divides, using sport as a vehicle to bring communities together, improve health, increase employability and build capacity.

FINAL REPORT FEBRUARY 2018
5
BCSDN’sapproachtoMMMCwastotraintheirexistingstafftobeabletodelivernutritionalmessagesand basic cooking skills. The team undertook training over a six week period to upskill. As experienced coaches and sports development facilitators, the physical activity element was straightforward, and their knowledge and experience of working in communities enabled them to establish good relationships with participants. They used their existing network of contacts with community groups, schools and other initiatives to recruit participants, and in most instances delivered the intervention to existing groups in a variety of community settings during both term and holiday times.
1.4.2 Food Academy, East Ham, LondonMMMCs were delivered in East London by Food Academy, an organisation supporting better lives throughchangesindietandphysicalactivity.FoodAcademyinitiallysetupandranthefirstJamieOliver’s Ministry of Food programme in London, but now works with other partners to deliver initiatives aimedatbringingaboutsustainedbehaviouralchangetotackleobesityandType 2diabetes.FoodAcademywasinvolvedfromtheoutsetofthisprogramme,pilotingthefirstversionoftheMMMCs.
Food Academy works from the East Ham Leisure Centre, and delivered all MMMCs in these premises which include a fully equipped teaching kitchen and a sports hall. The organisation is well-established inthelocalarea,andassuchwasabletorecruitthroughexistingnetworksandcontacts.Staffdelivering the MMMCs already had extensive experience in delivering cooking courses and healthy eating messages. They delivered MMMCs which remained closely aligned to the original model and, unlike other providers, delivered the clubs almost exclusively during school holidays.
1.4.3 Lanarkshire Community Food and Health Partnership, North Lanarkshire, Scotland
In North Lanarkshire, MMMCs were delivered by Lanarkshire Community Food and Health Partnership (LCFHP). LCFHP is a long-established charity that has worked throughout North Lanarkshire for the past 23 years, supporting local communities to improve their health through better diet. The organisation is supported by North Lanarkshire Partnership, North Lanarkshire Council, NHS Lanarkshire and the Scottish Government’s Enterprise Growth Fund to tackle health inequalities related to food access and healthy eating.
MMMCsevolvedovertheperiod,withthefirstyearfocussedondeliveryincommunitycentreswithsessionsdeliveredbynutritionists,leisurecentrestaffandfreelancefitnesstrainers.Thisprovedtobecostly,andlesseffectivethanhopedatreachingpotentialparticipants.InyeartwotheyworkedmorecloselywithschoolsandCommunityLearningandDevelopmentofficerstorecruitfamilies.Thecouncil’s Active Schools team supported the delivery of physical activity, and healthy eating sessions were delivered by community workers rather than nutritionists. As the programme approached its end, the model shifted to being schools-based, but operated in both term-time and holidays.
1.4.4 Nottingham CityCare, Nottingham, East MidlandsMMMCs in Nottingham were delivered by Nottingham CityCare Partnership – a social enterprise that provides community health services, including services for the NHS. The team leading the MMMCs were highly skilled and experienced in delivering programmes and working in dietary and nutrition interventions.
NottinghamCityCarePartnershipstaffdeliveredthehealthyeatingactivitiesoftheclubs,andthephysical activity aspect and children’s creche were subcontracted to other organisations or freelance professionals.Respondingtothelearningfromthefirstyearofdelivery,mostclubsweredeliveredatschools during school term time in the second year. This led to improved retention levels. They also focused on working with adults and children separately during both the healthy eating and physical activity sessions, where possible, in order to minimise distractions and pass the message across to mumsmoreeffectively.
FINAL REPORT FEBRUARY 2018
6
1.4.5 Valley Kids, Rhondda Cynon Taf, WalesMMMCs were delivered in Rhondda Cynon Taf by Valley Kids, a charity focussed on supporting young people, families and communities. The charity is well-established locally and has been working in these deprivedareasforover30years.Theco-foundersarestilldirectorsoftheorganisation,andthestaffofover50,supportedby100plusvolunteers,deliverarangeofprojectsandinitiativesacrossRhonddaCynonTaf.Theyofferplayschemes,providesupporttoyoungpeople,developparentingskillstosupport families and deliver community development activities.
Thefamily-focusoftheMMMCfeltlikeagoodfitfortheorganisation.Theyharnessedtheirexistingnetwork of groups and contacts to deliver MMMCs, but also used the intervention to start reaching intonewcommunities.Additionalstaff,includingsomeoftheirexistingvolunteers,wererecruitedtodeliverMMMCsincommunitycentresandschools,aswellasinsomeoftheirownvenues.Staff,though having a broad skillset amongst them, underwent training to be able to deliver the sessions including the key the nutritional messages. Whilst physical activity of various types was delivered, this provider focussed more on active play and walking as it was felt this was a more realistic goal for participants.
1.4.6 Accord Group, Sandwell, West MidlandsAccord, one of the largest housing associations and social care providers working in the Midlands, developedandco-ordinatedthedeliveryofMMMCsinSandwell.Accordcommissionedandproject-managedfivelocalcommunitypartnerstodelivertheprogramme:MyTimeActive,CompleteKidz,Ideal for All, Kaleidoscope Plus Group and, latterly, Groundwork West Midlands. Each of these providers had local relationships within the community, and also brought their own expertise and experience, which collectively included health and wellbeing, physical activity, working with children and engaging communities. Accord appointed them following a competitive tendering process, due to their shared valuesandstrongreputationindeliveringprojectsaimedatsupportingcommunities.
This model of delivery, with one organisation coordinating and supporting delivery of MMMCs through partner organisations, was unique in the programme. Accord provided practical support, ongoing communications and social media, and managed the local logistics of the programme. The organisation also provided training workshops to their delivery partners related to the programme toolkit, to share learning and help them to adapt delivery of the clubs where needed. In the second year, MMMCs were delivered in schools during school term time, or venues where the providers were already highly engaged with the community. This resulted in improved recruitment and retention rates.
1.5 Evaluation approach and methodology Theevaluationwasdesignedtofulfiltwopurposes:
1. evidenceparticipantoutcomes–whatdifference,ifany,MMMCsmadetoparticipants
2. gather process learning to inform programme development and future delivery – what worked well, what could work better, how have outcomes been achieved
The evaluation approach was designed to ensure participants and providers were not overburdened by the evaluation processes, whilst ensuring that the data collected was robust and reliable. This meant, for example, using self-report surveys for participant outcomes, and only selecting a small number of key indicators to evidence overall behavioural change, rather than attempting to measure everything.
The following methods were used to gather the data presented within this report:
FINAL REPORT FEBRUARY 2018
7
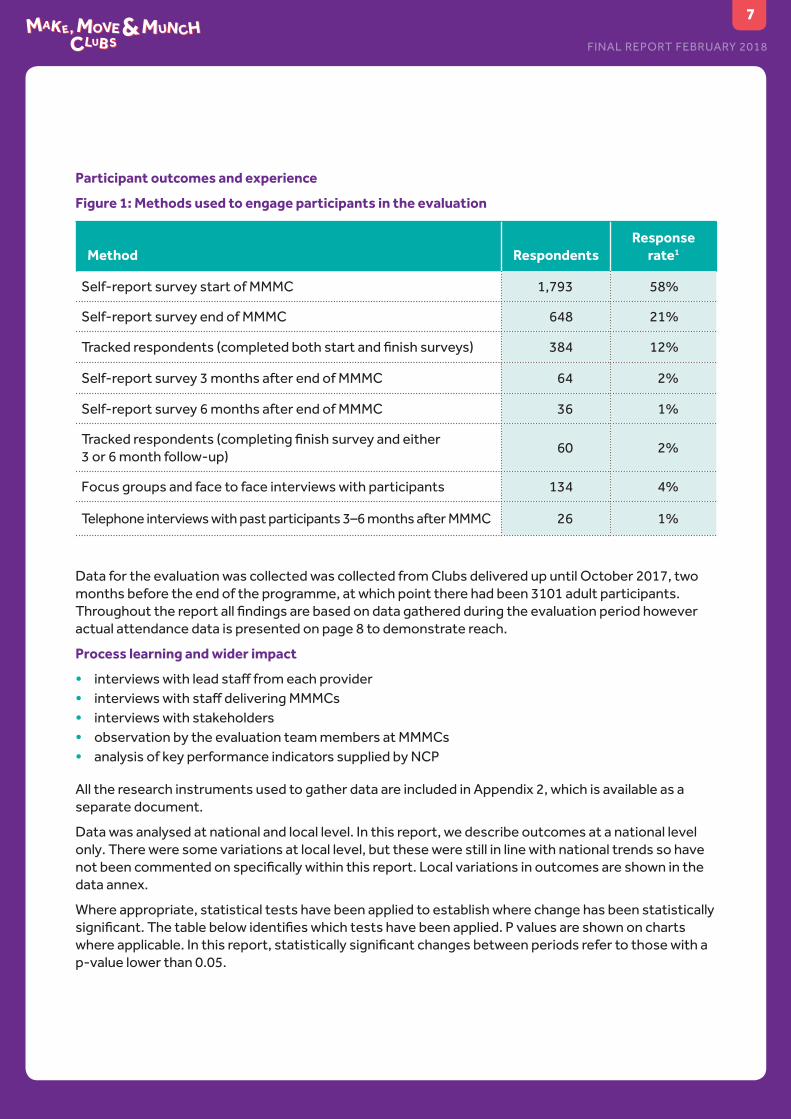
Participant outcomes and experience
Figure 1: Methods used to engage participants in the evaluation
Method RespondentsResponse
rate1
Self-report survey start of MMMC 1,793 58%
Self-report survey end of MMMC 648 21%
Trackedrespondents(completedbothstartandfinishsurveys) 384 12%
Self-report survey 3 months after end of MMMC 64 2%
Self-report survey 6 months after end of MMMC 36 1%
Trackedrespondents(completingfinishsurveyandeither 3 or 6 month follow-up)
60 2%
Focus groups and face to face interviews with participants 134 4%
Telephone interviews with past participants 3–6 months after MMMC 26 1%
Data for the evaluation was collected was collected from Clubs delivered up until October 2017, two months before the end of the programme, at which point there had been 3101 adult participants. Throughoutthereportallfindingsarebasedondatagatheredduringtheevaluationperiodhoweveractual attendance data is presented on page 8 to demonstrate reach.
Process learning and wider impact
• interviewswithleadstafffromeachprovider• interviewswithstaffdeliveringMMMCs• interviews with stakeholders• observation by the evaluation team members at MMMCs• analysis of key performance indicators supplied by NCP
All the research instruments used to gather data are included in Appendix 2, which is available as a separate document.
Data was analysed at national and local level. In this report, we describe outcomes at a national level only. There were some variations at local level, but these were still in line with national trends so have notbeencommentedonspecificallywithinthisreport.Localvariationsinoutcomesareshowninthedata annex.
Where appropriate, statistical tests have been applied to establish where change has been statistically significant.Thetablebelowidentifieswhichtestshavebeenapplied.Pvaluesareshownonchartswhereapplicable.Inthisreport,statisticallysignificantchangesbetweenperiodsrefertothosewithap-value lower than 0.05.

FINAL REPORT FEBRUARY 2018
8
1 Based on a total number of adult programme participants of 3101.
Figure 2: Statistical tests applied during quantitative analysis
Indicator Measure Statistical test
Eating≥3vegetablesorsalad, or fruit
Change in proportion of respondents. McNemar’s Test
Cooking main meal from the scratch
Change in average number of times per week.
T-test (Paired)
Looking at the nutritional information
Change in proportion of respondents looking always or nearly always.
McNemar’s Test
Being physically active Average change of number of days per week.
T-test (Paired)
Sustainability of behavioural changes
Eating≥3vegetablesorsalad, or fruit
Change in proportion of respondents. Two-proportion z-test
Cooking main meal from the scratch
Change in average number of times per week.
T-test (two-sample)
Looking at the nutritional information
Change in proportion of respondents looking always or nearly always.
Two-proportion z-test
Being physically active Change in proportion of respondents being inactive, moderately active, and active.
Two-proportion z-test
1.6 Data limitationsWhilst we collated a large number of surveys over the period of the evaluation, and carried out extensive qualitative work, we do recognise some limitations to the data. These are outlined below and should be borne in mind when reading the report.
1.6.1 Self-report surveysSelf-reporting of behaviours is not ideal, as people tend to underestimate unhealthy habits and overstate healthier ones. However, we agreed with the NCP that, within the constraints of the evaluation, it was the only realistic method for gathering participant behaviours. Recognising the likelihoodofbias,findingsshouldbeinterpretedwithadegreeofcaution.However,whilstoverallself-reportedlevelsmaybesubjecttothisbias,thetrendsinchangedbehaviourshouldstillbevalid.Tomakethefindingsasrobustaspossible,weusedsurveysfromatrackedsampleofparticipants(thatis, participants that completed a both baseline survey at the start and a survey on completion), when presenting change over time.
1.6.2 Measuring levels of physical activityLevels of physical activity were measured by asking respondents how many days per week they were active for 30 minutes or more, in blocks of at least 10 minutes. Activities they could count included walking, cycling gardening and exercise or sport. This approach was used to align the measure with the government’s recommended levels of activity of 150 minutes per week. In the second year a
FINAL REPORT FEBRUARY 2018
9
supplementary question was added, to be able to capture those respondents who were active for 150minutesbutdidtheiractivityoverfewerthanfivedays.
During the analysis process we found that this additional question did not aid our understanding of the changes that were seen amongst participants. As we only had this data for the second year, we have not presented this additional data, and have focussed on the number of days respondents told us they were active per week before and after the intervention.
Wehaveusedasimplifiedindustry-standarddefinitionofactivitylevelstocategoriserespondents:
• active for 0–1 days – inactive • active for 2– 4 days – moderately active• active for 5 days or more – active
1.6.3 Evidencing sustainability of changeTo understand the extent to which participants sustained their health behavioural changes after the end of the MMMC, we used follow-up surveys at three and six months after completion. Responses to these follow-up surveys were lower than responses to the end of programme surveys, as they were notcompletedintheClub(seefigure1).
In addition to lower numbers in this group, we must also be aware of selection bias. We assume that those who consented to be followed-up and then completed a follow-up survey are likely to be those most engaged with the intervention, and potentially those that have had greater success in making lifestyle changes. It is generally less common to receive returns from those that feel they have been less successful.
Insection3.5weincludeabaselinefigurealongsidetrackedfollow-upresponses,toshowdistancetravelled. However, this is the baseline calculated from all pre-MMMC survey responses, not only thosewhowereinthetrackedfollow-upsample.Wehaveusedthisbaselineastherewereinsufficientnumbers of respondents that submitted a pre-, end and follow-up survey to produce a robust sample. We have therefore, been able to draw some inferences about sustainability of behavioural change, but the evidence is less robust and should be read with a degree of caution, in particular bearing in mind thedifferentsampleusedtocalculatethebaseline.
1.6.4 Contribution not attributionManyfactorsinfluencehealthbehaviouralchange,bothduringandbeyondanintervention.Weusedqualitative methods to explore these factors and the extent to which the intervention itself led to behavioural change. However, we must state that behavioural change, where seen, cannot be directly attributed solely to the intervention; rather we must focus on the contribution made.
FINAL REPORT FEBRUARY 2018
10
2 Who did the clubs reach?At the time the evaluation concluded in October 2017, 3101 adults and 4603 children had attended Make, Move & Munch clubs. This increased to 3235 and 4775 respectively by the end of the programme in December. All data presented hereafter is based on that gathered during the evaluation period.
58% of participants completed at least four sessions, 38% completed six, and 20% completed eight sessions. The average attendance was 4.7 sessions.
Using attendance data from the Clubs, and the baseline survey responses (completed by 1,618 participants), we can describe the people attending MMMCs in further detail – their demographic profile,theirexistinghabitsandlifestylechoices,andthechallengestheyarefacing.Thischapteraims to paint a picture of the kind of people attending MMMCs, rather than provide a detailed baseline. Further data on their initial behaviours and how these have changed over time are presented in Chapter 3.
2.1 Demographic profileThe target audience for MMMCs was mums between the ages of 25 and 40. Attendance data shows that96%ofparticipantswerefemale,andthisisalsoreflectedinthesurveydata.
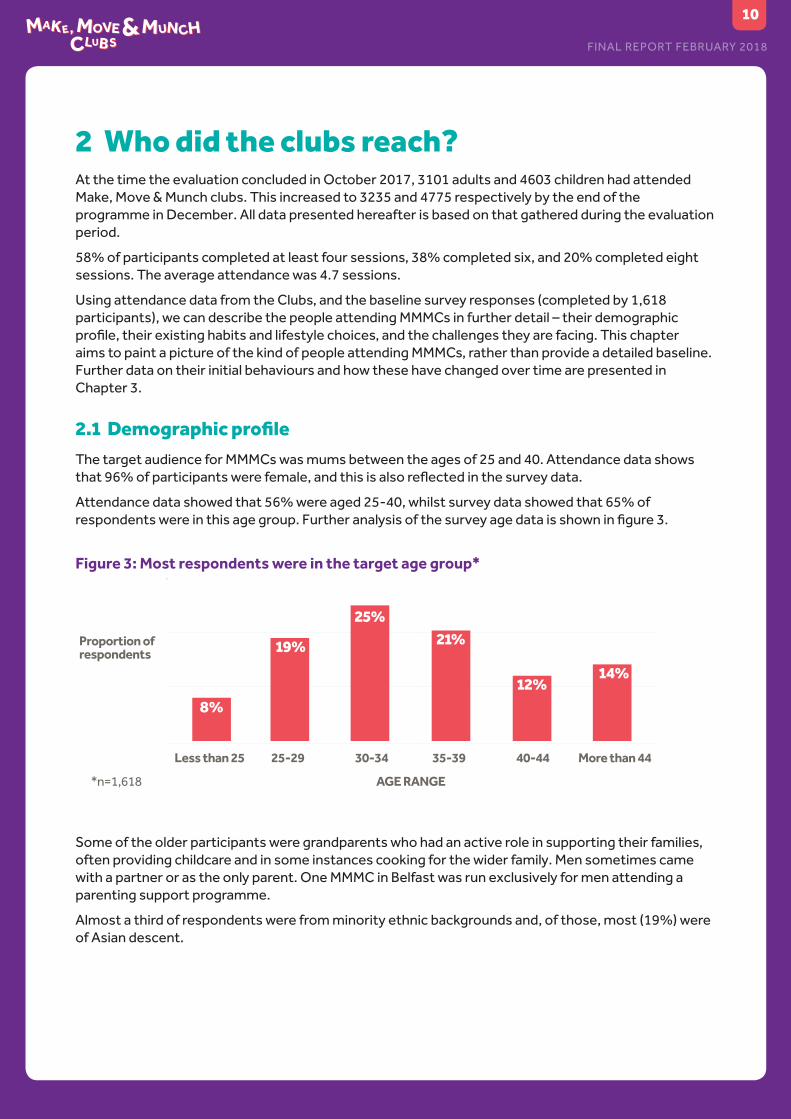
Attendance data showed that 56% were aged 25-40, whilst survey data showed that 65% of respondentswereinthisagegroup.Furtheranalysisofthesurveyagedataisshowninfigure3.
Figure 3: Most respondents were in the target age group*
8%
Less than 25 25-29 30-34 35-39 40-44 More than 44
AGE RANGE
Proportion of respondents
*n=1,618
19%
25%21%
12%14%
Some of the older participants were grandparents who had an active role in supporting their families, often providing childcare and in some instances cooking for the wider family. Men sometimes came with a partner or as the only parent. One MMMC in Belfast was run exclusively for men attending a parenting support programme.
Almost a third of respondents were from minority ethnic backgrounds and, of those, most (19%) were of Asian descent.

FINAL REPORT FEBRUARY 2018
11
2.2 Families facing challengesFigure 4: Most respondents were from the 20% most deprived areas within their nation2*
*n=1,585
9
32%26%
17%11%
5%3%
1 2 3 4 5 6 7 8 10
Index Multiple Deprivation decile
1.8% 2.3% 0.8% 0.7%
Proportion of respondents
Overonethird(38%)oftherespondentsstatedhavingdifficultiesmakingtheirfoodbudgetlasttheweek.
As well as locating MMMCs in deprived areas, providers also targeted families to identify those that theyfeltwouldbenefitmostfromtheintervention.Thisincludedfamiliesnewtothearea,familiesinwhichEnglishwasnotafirstlanguage,familieswithdifficultrelationships,childrenwithchallengingbehaviour, and parents undertaking parenting skills programmes.
2.3 Baseline health behaviours
Figure 5: Most respondents were eating 1 or 2 portions of vegetables/salad and fruit per day
5%
26%32%
21%
7% 4% 4% 8%
27%30%
19%
8% 6%3%
Proportion of respondents
Proportion of respondents
VEGETABLES OR SALAD* FRUIT*
0 1 2 3 4 5 >5Number of portions of vegetables or salad Number of portions of fruit
*n=1,667 *n=1,651
0 1 2 3 4 5 >5
Figure 6: More than half of respondents were physically active fewer than the recommended five days per week*
14% of respondents were inactive
*n=1,576
Proportion of respondents
6% 8%13%
16%13% 14%
6%
23%
Days a week physically active0 1 2 3 4 5 6 7
Inactive Moderately active Active
2 Based on the Indices of Multiple Deprivation for England, Wales and Scotland and the Northern Ireland Multiple Deprivation Measure.

FINAL REPORT FEBRUARY 2018
12
2.4 MotivationInthefirstsurvey,respondentswereaskedwhytheydecidedtocomealongtoMMMC.Mostcommonresponses referred to learning about healthy eating cooking/nutrition. The next most common reason was activities for the children or as a family. Far fewer responses (8%) mentioned the physical activity aspectsoftheofferasbeinginfluential.
Figure 7: Respondents were keen to learn about healthy eating and cooking*
Activities for the family were also important
Learn about healthy eating and cooking/nutrition
Activities for/with children/family
Like cooking/want to learn/improve
Get advice/learn new things
Recommended to join/joined because of friends
Try new things/socialise
Exercise/get fit
Fun
Others
40%
35%28%
17%
11%
10%8%7%
9%
Proportion of respondents
*n=1,541
Note that percentages add up to over 100% because respondents could provide multiple responses
Participantswespoketoalsoreflectedthesereasonsforcoming.
“I wasn’t a very good cook and it sounded like something that would help me do better.”
Parentscommentedthat,particularlyduringschoolholidays,havingsomethingnewanddifferenttodowashelpfulinkeepingthechildrenoccupied.Theyalsohighlightedthatitwashardtofindactivitiesto do together as a family. Some also commented that MMMC being free was a plus, and a charge for attending would almost certainly have been a barrier.
“It sounded like something different, interesting, and something that the children could take part in. It can be hard
to find different things to do in the holidays.”

FINAL REPORT FEBRUARY 2018
13
3 What difference did the clubs make?
3.1 Summary of outcomesThis chapter describes the range of outcomes achieved through MMMCs, and explores the reasons behind the outcomes. For simplicity, the key outcomes are summarised below, comparing survey responsesfromthestartandfinishofMMMCs:
Eat a little better
• 51%ofrespondentswereeatingmoreportionsofvegetables/saladwithasignificantincreaseinthose eating three or more portions a day
• 46%ofrespondentswereeatingmorefruitwithasignificantincreaseinthoseeatingthreeormoreportions per day
• respondents were eating unhealthy snacks less often• 47% of respondents always or nearly always looked at nutritional information when buying a new
product, compared with 26% at the start• respondents were cooking from scratch more often• MMMCs had helped 93% of respondents make their weekly food budget go further
Move a little more
• the percentage of respondents that were physically inactive3 fell from 15% to 1%• respondents that were previously inactive were, on average, active 3.9 days per week• the proportion of active respondents had increased by 25%, to 54% • Participants in the tracked sample from which these outcomes are derived attended, on average,
6.4 sessions.
Sustaining the change
• Analysis of follow up surveys revealed that respondents were maintaining their positive cooking and shopping habits. Other positive behaviours also still remained at a higher level than when they had started MMMCs, even though some had dipped a little since the end of the programme.
3.2 Eat a little better
3.2.1 Choosing healthy optionsWeaskedparticipantsabouttheirfoodintakeintwodifferentways:
• asking them to detail their weekly intake of certain foods (fruits, vegetables, snacks, drinks) – reported intake
• asking them their perception of whether their intake had increased, decreased or remained unchanged – perceived intake
At the end of the programme, 73% of respondents reported a perception that they were eating more vegetables and fruit, and 67% that they were eating more salad. Their reported intake also indicated an improvement, albeit not quite as much: 51% of respondents were eating more portions of vegetables/salad after MMMC and 46% were eating more fruit.
Therewasalsoasignificantincreaseinthenumberofrespondentseatingthreeormoreportionsofvegetables/salad and fruit. 3 Inactive is defined as being active for 0-1 days per week, moderately active 2–4 days per week and active 5 days or more

FINAL REPORT FEBRUARY 2018
14
Figure 8: On completion more than half of respondents were eating at least three portions a day each of fruit and vegetables/salad *
37%
59%52%
34%
Vegetables or salad Fruit
% respondents eating >3 portions/day
Pre-MMMC
End of MMMC
*nv=348, nf=346 p < 0.01 for both
In addition to encouraging participants to eat more fruit and vegetables, the MMMCs provided the opportunity to try new ones, thereby increasing the range of foods families were exposed to. Vegetarian recipes gave participants more scope to incorporate vegetables, and some participants reported eating vegetarian at least once per week. Parents we spoke to often said children would try food at the Club that they wouldn’t try at home, and this opened up opportunities to increase their intake of healthier options. Some adults too were introduced to vegetables and fruit they hadn’t tried before, often because unusual fruits and vegetables were quite expensive, and parents didn’t want to waste money on something they might not like.
“I knew I wasn’t using enough vegetables in my cooking but this has shown me different ways of including them in meals. I even try to make vegetarian meals during the week now and I never done that before.”
Responses also showed some small improvements in snacking habits, with healthy snacks such as fruit and vegetables being eaten more often and less healthy snacks (biscuits, cake, crisps, sweets and chocolate) less often.
Figure 9: The average number of days per week that respondents ate various snacks shows improved habits
Snack Pre-MMMC End of MMMC ChangeFruit 3.7 4.2
Vegetables 3.1 3.8
Unsalted nuts 0.6 0.7
Plain Yogurt 1.0 1.0
Biscuits 2.6 2.0
Cake 1.4 1.0
Crisps 2.4 1.7
Sweets 1.5 1.1
Chocolate 2.3 1.6

FINAL REPORT FEBRUARY 2018
15
Wealsoaskedaboutdrinksconsumedbyadultparticipants.Overallfluidintakewasgenerallyatquite a good level already, but there were still positive changes in drinking habits such as reduced consumptionoffull-sugarfizzydrinks,andofteaandcoffeewithsugar.Wedidnotcapturedataaboutchildren’s drinking habits, but we heard anecdotally that participants had been shocked by the sugar contentoffruitjuicesandjuicedrinks,whichtheyperceivedtobehealthy,andwerereducingtheamountofthesetypesofdrinkstheygavetotheirchildrenaswellasreducingfull-sugarfizzydrinks.
“I was horrified! I really thought I’d been giving them a healthy option with Ribena, but then we did the sugar activity and I couldn’t believe how
much was in those little cartons. Not any more – I give them no added sugar squash now, and I make it pretty weak too. ”
3.2.2 Knowing about food and nutritionThe key messages about reducing salt, sugar and fat really hit home. Nearly all of those we spoke to referred to one or more of these lessons, and how they made them change the way they cooked and chose foods for their families. Whilst they didn’t always make a direct connection between diet andconditionssuchasType 2diabetesandcardiovasculardisease,somereferredmoreindirectlytotheimportanceofeatinghealthilytoreduceriskofdisease.Afewintervieweesdidmakespecificreference to conditions they or their family members had, and that they were using what they had learnedtoeffectpositivechange.
Susan’s dad has high cholesterol and high blood pressure. At MMMC she learned that changing his diet could improve his symptoms, so she has changed the way she cooks at home, including reducing the amount of salt she puts in and using the measuring spoons to make sure she uses less oil when cooking. Susan said her dad was bit hesitant about having healthier meals, but once he tried he was more open to change. She says she knows she needs to do more but feels at least it’s a step in the right direction.
Some already knew these things were bad for them, but they didn’t realise how much they were consuming. They sometimes thought they had been making healthy choices but, having become better informed, they were able to take easy, practical steps to cut back. Simple changes such as measuringtheamountofoilbeingusedforcooking,switchingfromfruitjuicetosugar-freeflavouredwaterandusingherbsandspicestoflavourinsteadofsalt,werecommonlyadoptedbyfamilies.
Participantsalsoappliedtheirknowledgewhilstshoppingtoinfluencetheirchoices.Theyreportedbeingmoreawarethatpre-preparedfood,suchasjarsofsauces,oftencontainedhighlevelsofsaltand sugars and so bought them less frequently. They also reported using the labels on foods to avoid thosewithpoorernutritionalvalues.Thedescribedthetrafficlightsystemasuseful,asbothadultsand children found it easy to understand and it provided a point of discussion for families shopping together.
Survey responses also demonstrated how this knowledge was changing habits with respondents looking at food labels more frequently.
FINAL REPORT FEBRUARY 2018
16
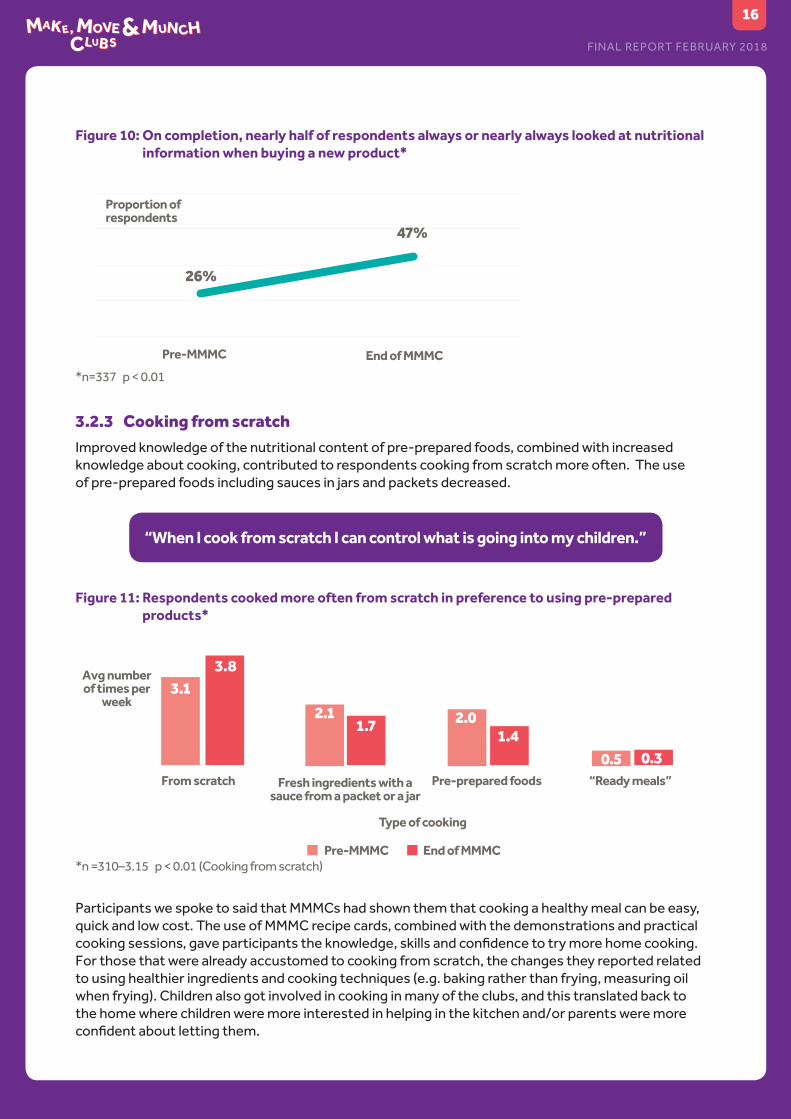
Figure 10: On completion, nearly half of respondents always or nearly always looked at nutritional information when buying a new product*
Pre-MMMC End of MMMC
Proportion of respondents
*n=337 p < 0.01
26%
47%
3.2.3 Cooking from scratchImproved knowledge of the nutritional content of pre-prepared foods, combined with increased knowledge about cooking, contributed to respondents cooking from scratch more often. The use ofpre-preparedfoodsincludingsaucesinjarsandpacketsdecreased.
“When I cook from scratch I can control what is going into my children.”
Figure 11: Respondents cooked more often from scratch in preference to using pre-prepared products*
3.83.1
2.11.7
1.40.5 0.3
2.0
From scratch Pre-prepared foods “Ready meals”Fresh ingredients with a sauce from a packet or a jar
Avg number of times per
week
Type of cooking
End of MMMCPre-MMMC*n =310–3.15 p < 0.01 (Cooking from scratch)
Participants we spoke to said that MMMCs had shown them that cooking a healthy meal can be easy, quick and low cost. The use of MMMC recipe cards, combined with the demonstrations and practical cookingsessions,gaveparticipantstheknowledge,skillsandconfidencetotrymorehomecooking.For those that were already accustomed to cooking from scratch, the changes they reported related to using healthier ingredients and cooking techniques (e.g. baking rather than frying, measuring oil when frying). Children also got involved in cooking in many of the clubs, and this translated back to the home where children were more interested in helping in the kitchen and/or parents were more confidentaboutlettingthem.
FINAL REPORT FEBRUARY 2018
17
“I never used to let them get involved with cooking, but it has let me see that they can do more than you think they can. ”
Before MMMC, Jane often used jars of sauce as it made preparing family meals quick and easy. Since she and her son have attended MMMC, she has bought far fewer and now makes sauces from scratch. It’s not complicated. When they go shopping they check labels, especially for fat content. Jane said if her son brings her something not so healthy, she tells him this has a lot of fat let’s get something with less.
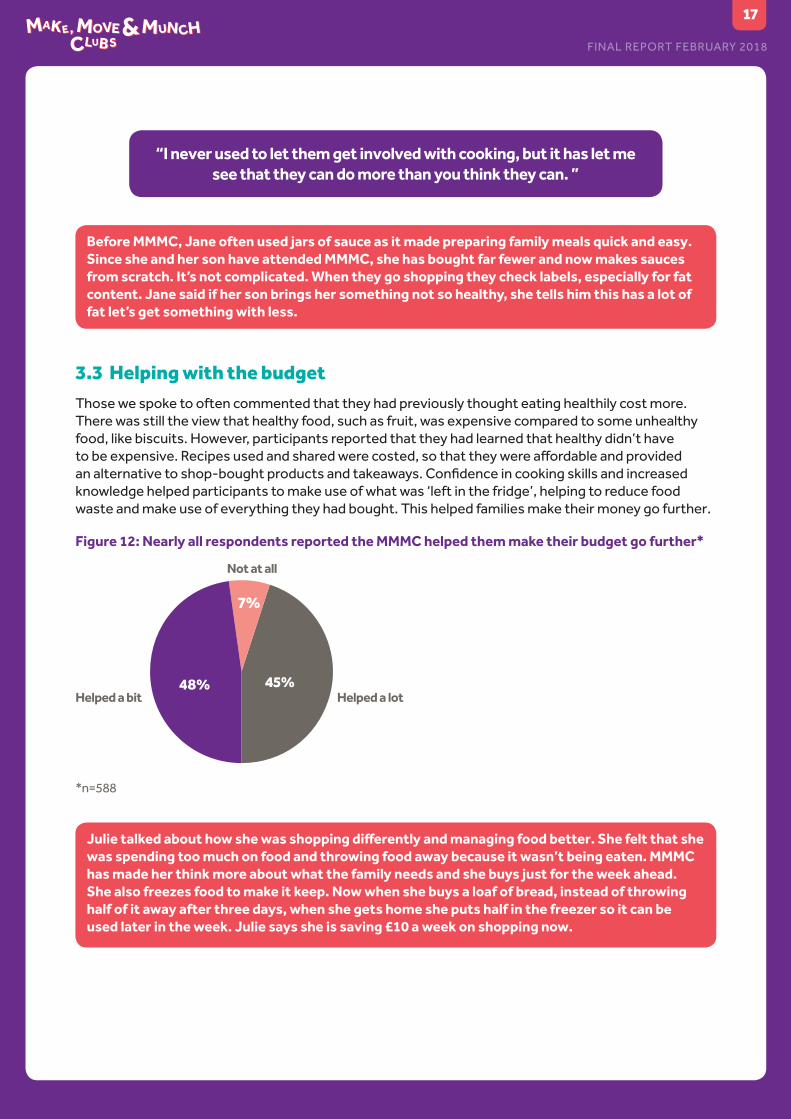
3.3 Helping with the budgetThose we spoke to often commented that they had previously thought eating healthily cost more. There was still the view that healthy food, such as fruit, was expensive compared to some unhealthy food, like biscuits. However, participants reported that they had learned that healthy didn’t have tobeexpensive.Recipesusedandsharedwerecosted,sothattheywereaffordableandprovidedanalternativetoshop-boughtproductsandtakeaways.Confidenceincookingskillsandincreasedknowledge helped participants to make use of what was ‘left in the fridge’, helping to reduce food waste and make use of everything they had bought. This helped families make their money go further.
Figure 12: Nearly all respondents reported the MMMC helped them make their budget go further*
48% 45%
7%
*n=588
Helped a lotHelped a bit
Not at all
Julie talked about how she was shopping differently and managing food better. She felt that she was spending too much on food and throwing food away because it wasn’t being eaten. MMMC has made her think more about what the family needs and she buys just for the week ahead. She also freezes food to make it keep. Now when she buys a loaf of bread, instead of throwing half of it away after three days, when she gets home she puts half in the freezer so it can be used later in the week. Julie says she is saving £10 a week on shopping now.

FINAL REPORT FEBRUARY 2018
18
3.4 Move a little morePeople we spoke to, who had felt they were previously fairly inactive, said that they got more exercise. Somesaidtheystilldidn’tdoasmuchastheyfelttheyshould,becauseitwasdifficulttofitexerciseinto their daily routine. Cost and accessibility also remained as barriers for some.
“With cooking you are making changes to something that you are doing anyhow, with exercise it is something new that you have to fit into your day.”
WhilstsomecommentedthattheyhadenjoyedthemoreformalexerciseofferedatsomeoftheClubs, like Zumba, Yoga and boxercise, they often felt unable to continue with this form of exercise outside of the Clubs. Walking and active play were the most common ways people found to get a bit more exercise. Walking to school, exercising at home or dancing with the children provided more practical ways to make small changes.
Despite these challenges there have been notable improvements in the activity levels of participants. Thesurveyshowedthat,onjoiningMMMCs,15%ofrespondentswerephysicallyinactive.Attheendof the programme only 1% were. The proportion of active respondents had also increased from 43% to 54%.
Figure 13: After MMMC only 1% of respondents were inactive and the proportion of active respondents also increased*
7% 8%
14%
19%16% 16% 16%
5%
10%
22%
28%
10%
20%
8%
0% 1%
Proportion of respondents
Days a week physically active0 1 2 3 4 5 6 7
Inactive Moderately active Active*n=332
(Light = Pre-MMMC Dark = End of MMMC)
At the start of MMMCs the average number of days that respondents were physically active was 3.9 per week. This rose to 4.8 by the end. Obviously, this average includes a wide spread of activity levels, from inactive to active every day.
Thesubsetwhowereinactivesignificantlyincreasedtheaveragenumberofdaystheywereactive,from0.5to3.9daysperweek.ThisindicatesthattheMMMCwasespeciallyeffectiveatenablingbehaviour change amongst the least active.

FINAL REPORT FEBRUARY 2018
19
Figure 14: Levels of activity increased most in those that were inactive at the start*
Average days being physically active
Pre-MMMC
All respondents
Inactive
End of MMMC
*n=332, Inactive = 49 P <0.01
3.9 3.9
4.8
0.5
Mary thought MMMC would help keep her grandchildren occupied and provide an opportunity to learn more about healthy eating, as she was already trying to lose weight. She told us that, before going to MMMC, she wouldn’t have entertained the idea of physical activity. Having tried yoga at the MMMC, she thought ‘this is something I can do’ and so started sessions at the local leisure centre. She also swims once a week. Mary used to walk with a stick and found doing the housework tiring. Since going to MMMCs she has lost 4 stone, no longer uses her stick and finds she is no longer breathless when playing with the grandchildren. She found making the changes ‘quite painless’ and now she feels 10 years younger!
3.5 Sustainability of behavioural changesEvidence of sustainability of change described in this section is based on the analysis of tracked respondents who completed an end-of-MMMC survey and a follow-up survey. There are therefore somedifferencesintheend-of-MMMCrespondentnumberscomparedwiththoseintheprevioussection, which is based on tracked respondents that completed a pre-MMMC survey and end survey. The baseline is derived from all pre-MMMC survey responses. The limitations of the data for this sectionhavebeendiscussedinmoredetailinsection1.5.3.Seefigure1fordetailsofnumbersofsurvey respondents and telephone interviewees.
3.5.1 Healthy eatingThe key to a successful behavioural change programme is that positive changes ‘stick’. Participants we spoke to via telephone, three to six months after they had attended MMMCs, still reported eating healthier food and making good choices about their diet. Messages were still clear in their minds, and they said eating healthily now felt like the norm for them. They reported that the approach of making a few small but important changes had made it easier to stick to those changes. They also described howwhattheyhadlearnedwasnowbenefitingthewiderfamily,intheircookingandshoppinghabits.
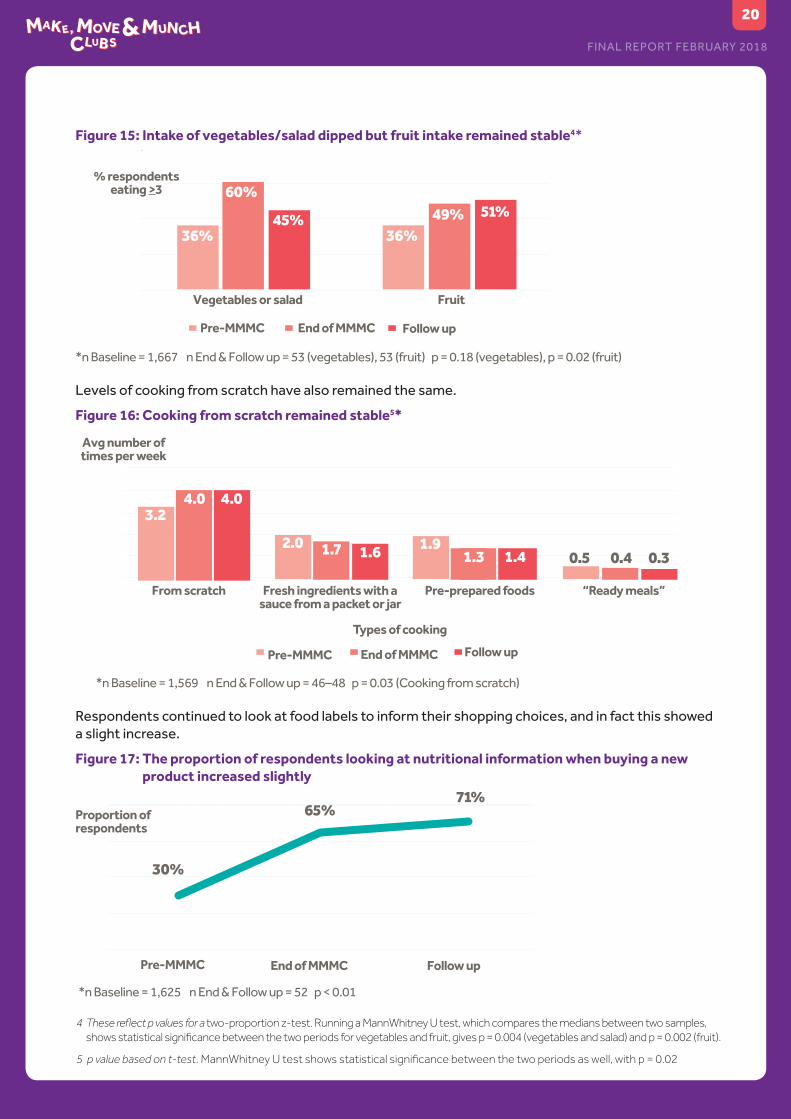
Whilstintakeofvegetables/saladhaddroppedofffromthepointoffinishingtheClub,itwasstillata higher level than the start. Intake of fruit had remained stable. Both results were still higher than baseline showing a sustained change in some.
FINAL REPORT FEBRUARY 2018
20
Figure 15: Intake of vegetables/salad dipped but fruit intake remained stable4*
36%
60%
45% 49% 51%
36%
Follow upEnd of MMMCPre-MMMC
Vegetables or salad
% respondents eating >3
Fruit
*n Baseline = 1,667 n End & Follow up = 53 (vegetables), 53 (fruit) p = 0.18 (vegetables), p = 0.02 (fruit)
Levels of cooking from scratch have also remained the same.
Figure 16: Cooking from scratch remained stable5*
3.24.0 4.0
2.0 1.7 1.6 1.91.3 1.4 0.5 0.4 0.3
From scratch Pre-prepared foods
Types of cooking
“Ready meals”Fresh ingredients with a sauce from a packet or jar
Pre-MMMC End of MMMC Follow up
*n Baseline = 1,569 n End & Follow up = 46–48 p = 0.03 (Cooking from scratch)
Avg number of times per week
Respondents continued to look at food labels to inform their shopping choices, and in fact this showed a slight increase.
Figure 17: The proportion of respondents looking at nutritional information when buying a new product increased slightly
Pre-MMMC End of MMMC
Proportion of respondents
*n Baseline = 1,625 n End & Follow up = 52 p < 0.01
30%
65%
Follow up
71%
4 These reflect p values for a two-proportion z-test. Running a MannWhitney U test, which compares the medians between two samples, shows statistical significance between the two periods for vegetables and fruit, gives p = 0.004 (vegetables and salad) and p = 0.002 (fruit).
5 p value based on t-test. MannWhitney U test shows statistical significance between the two periods as well, with p = 0.02

FINAL REPORT FEBRUARY 2018
21
3.5.2 Physical activitySpeaking to past participants revealed that barriers to physical activity, principally cost and time, continuedtomakeitdifficulttoestablishanexercisehabitevenwhentheywantedto.Despitethis,the proportion of inactive respondents remained low at 6%, and the proportion of active respondents increased from 48% to 58%.
Figure 18: Overall respondents became more active and levels of inactivity have remained low6*
Proportion of respondents
Days a week physically active
0-1 (Inactive) 5-7 Active)2-4 (Moderately active)
Lightest colour = Pre-MMMC Darkest colour = Follow up
*n Baseline = 1,576 n End & Follow up = 50 p = 0.04 (active), 0.08 (inactive)
15%
42%48%
36%44% 48%
58%
4% 6%
Respondents’ levels of activity, based on average days per week, have been sustained.
Figure 19: Respondents have sustained their levels of physical activity after MMMCs*
Pre-MMMC End of MMMC
Avg days per week being active
*n Baseline = 1,567 n End & Follow up = 50 p = 0.047
4.04.7
Follow up
4.6
3.6 Social and community outcomesMMMCs provided learning in a social environment, and many we spoke to commented on the social aspects of the Clubs. Some attended with friends, but many came alone and made new friends and social contacts. Whilst these did not always continue beyond the duration of the programme, some newfriendshipgroupsformed.Participantsenjoyedtheopportunityforsomeadultcompanyandconversation, and for a few it reduced social isolation.
Childrentoobenefittedfrommeetingotherchildren,makingnewfriendsandbuildingconfidence.Families within communities that had not met were brought together and could at least stop for a chat at the school gates or whilst out shopping.
FINAL REPORT FEBRUARY 2018
22
ParentswhobroughtchildrenwithchallengingbehavioursandlearningdifficultiestotheClubsreported that they provided a helpful opportunity for further socialisation, and that the children enjoyedtheClub.Familieswhowerenewtoanareaandstrugglingtosettleintotheirnewcommunityalso found the Club helped their children integrate and make new friends.
One mum dealing with anxiety, and her daughter who also had additional needs, found the MMMC a safe and welcoming place. It felt different to other courses she had been on when she found it difficult to keep focus. Having her daughter close at hand and knowing she was happy meant she could focus on the cooking and other learning. She felt there were people around that would help her and she really enjoyed her time at the Club. She said it has helped her outside as well and she has started a computer course again because she feels more able to focus.
3.7 Organisational changes/developmentFor some of the organisations, providing MMMCs gave them an opportunity to develop and explore new ways of working, including:
• trainingstaffincookingskillsandfoodhygiene• trainingstafftodeliverphysicalactivity• using food/cooking as a ‘hook’ for other interventions they deliver• incorporatingphysicalactivityintotheirinterventionsratherthanjustfocussingsolelyonhealthyeating
MMMCs also enabled providers to:
• extend their reach into new areas• develop relationships with other community based organisations• strengthen relationships with local schools
A number of the providers have integrated the key messages and skillsets from MMMC into their wider suite of interventions, and this also informed an evolution of their organisational strategy in at least one case.
6 These reflect p values for a two-proportion z-test. Running a MannWhitney U test, which compares the medians between two samples, shows statistical significance between the two periods of = 0.047.

FINAL REPORT FEBRUARY 2018
23
4 What made the difference?The previous chapter explores the outcomes achieved by participants as a result of MMMCs. The evaluation also sought to understand the factors that contributed to the achievement of these outcomes. This chapter describes the ‘key ingredients’ of the programme, which enabled the programme’s success.
4.1 Realistic ambitionMMMCs recognised that change would be best achieved through small steps over time, resulting in smallimprovementsthatcouldbebuiltupon.Theoutcomesinthelogicmodelreflectthisethos;itincluded a holistic range of lifestyle choices which contribute to improved wellbeing, but with a goal of someimprovementratherthanafixedquantitativegoal.
Participants were encouraged to make real changes, with goals that were achievable for them. It wasn’t about setting a big, potentially intimidating, goal, it was simply about doing a little better. Most that attended came with the intent to learn and make positive change, so were at the contemplative stage of the transtheoretical model of behaviour change. Some were ready to change, having already taken small steps. MMMCs have enabled and supported participants to get to the next stages preparation and action.
Many behaviour change programmes fail because they demand too much and/or the messaging is accurate but dry. The philosophy behind MMMCs was that a positive change, no matter how small, was a success and was more likely to stick. Participant feedback suggests this approach was key to their own success, as they were encouraged to make small but achievable changes and thus were able to keep up their good habits.
4.2 Finding a route to the target audienceProvidersthatutilisedtheirexistingcontactswithincommunitiesgotofftoafasterstartinthefirstyear, compared to those that tried to recruit through more general promotional methods such as posters and local press. This was an important piece of learning, and in year two providers that had beenlesssuccessfulrecruitingandretainingparticipantsinthefirstyeartookadifferentapproach.This involved working predominantly with schools to promote the Clubs and refer families to it.
Working with schools proved particularly successful, as they provided both a channel to reach participants and a venue that was familiar to parents and children. There was a trusted relationship thattheMMMCteamcouldbuildon,byinvolvingschoolstaffasapointofcontactorfamiliarfaceinthe room. Clubs were also extended to term-time making them more accessible.
Providing MMMCs to existing groups also proved successful for some providers. Established groups already had a pre-existing bond, a familiar venue and regular meeting time.
4.3 Clear and consistent messages The core messages delivered by MMMCs were well-known messages about reducing the risk of cardiovasculardiseaseandType 2diabetes:reducesalt,sugarandfatintake,increasefruitandvegetable intake. The use of visualisation, to demonstrate how much fat, sugar and salt were in food, was powerful and stayed with participants for many weeks. Messaging was also consistent and repeated throughout the sessions, which reinforced learning.

FINAL REPORT FEBRUARY 2018
24
4.4 Practical ways to make healthy changesAswellashelpingparticipantsunderstandwhatbehaviourstochange,importantlyMMMCsofferedpractical advice on how to make the change. Clubs provided alternative suggestions, such as adding flavourwithherbsandspicesinsteadofsalt,andswitchingbrandstoreducesugarintake,whichmadeapplying what they were learning much easier for participants.
Similarlywithphysicalactivity,theygaveparticipantstastersessionsforavarietyofdifferenttypesofexercise,andsomefoundthatenjoyable.However,formany,attendingexerciseclassesatthelocalleisure centre remains a challenge. Active play sessions and encouraging participants to walk more providedlowcost,enjoyablewaystoexercise,andspendmoretimewiththefamily.
4.5 Family focus
4.5.1 Helping to remove barriersThe family approach was instrumental in both facilitating access to Clubs and in landing messages. Childcarewasidentifiedasabarriertoparticipation,sotheprovisionofcrechefacilitiesandactivitiesfor older children enabled access. Including children also assisted with retention, as the participants toldusthechildrenenjoyedtheClubsandwantedtogoback.
Having children present also removed some of the barriers around taking part in physical activity, as ‘joininginwiththekids’wasalessdauntingprospectthantakingpartinaZumbaclass.Childrenalsopicked up on the health messages and helped reinforce these outside the Clubs; some participants reported that children were now involved in shopping decisions and menu planning using what they had learned at the Clubs.
NearlyallClubsfinishedwiththegroupsittingtogetherforamealcookedduringthesession or provided for them. Bringing the family together for the meal was important for bonding and re-establishing family habits.
4.5.2 Learning as a familyProvidersdeliveredsessionsdifferently,withsomehavingseparateactivitiesforchildrenandadults,whilst others were mixed. Most had a blend of the two, with some activities being adult-only and othersjointactivities.Foradult-onlyactivities,havingthechildrennearbymeantparentsweren’tworried about them and could focus on what they were doing. Some participants also said they liked havingabitofadulttime,whilstotherswantedmoretimewiththechildreninvolvedasjointactivitiesgave the opportunity for family learning and bonding. In some Clubs, the presence of children in some of the activities, either intentionally or otherwise, was sometimes a distraction, but without that elementmanyparentswouldn’thavebeenabletoattendinthefirstplace.
There did not appear to be an ideal formula, and there were pros and cons to both approaches. However,havingtheflexibilitytomeettheneedsofthegroupwasessential.

FINAL REPORT FEBRUARY 2018
25
4.6 The learning environment
4.6.1 Accessibility and familiarityThe use of schools and community venues meant participants could access them easily and they were in familiar surroundings. Though facilities were not always ideal, innovations such as ‘pop up’ kitchens enabled the Clubs to be brought to the participants. Some venues had limited space, but providers made the best use of what they had.
4.6.2 A relaxed learning spaceProviders were able to create environments conducive to learning. They were relaxed and informal, and whilst the messages were serious the learning was fun. Participants said they and their children reallyenjoyedtheClubsandwecertainlyobservedlotsoflaughter.Thefunfactorkeptparticipantscoming back and kept them engaged in what they were learning.
4.7 Learning togetherStaffwerekeentodelivermessageswithoutpreachingorpatronising,andpromotedanethosoflearningtogether.Whenthecookingdemonstrationdidn’tgotoplan,theymadeajokeaboutitandrecoveredasbesttheycould.Thismadeitacceptableforeveryonetogetitwrongsometimes.Stafffollowed up on the structured sessions with more informal chats, as a gentler way of getting messages over.Thisapproachwaswell-receivedbyparticipants,whofrequentlycommentedthatstaffwerevery friendly and approachable. They didn’t feel as if they were being told what to do.
4.8 Building rapport and trustStaffworkedhardtoestablishrapportwiththeirgroups,todevelopatrustedrelationship.Insomeinstances, providers had a head start because they had already worked with the families, but for others the relationships were new. However, time taken at the start to build relationships was essential. Whilst there were structured sessions, much of the messaging was reinforced through informal discussion. Groups were involved in the decision-making about the types of activities they wanted to do or the recipes they wanted to cook. Giving ownership to the groups helped keep them engaged.
4.9 Innovation and adaptability Providersandstaffwereempoweredtoadaptthemodeltosuittheircommunity,theirvenuesandthegroup in front of them, without losing core content. Only one provider had the ’ideal’ venue, others have hadtocreate‘popup’kitchens,findspacetodophysicalactivity,andadaptactivitiestofitthevenue.Providersalsotrieddifferenttimesandpatternsofdeliverytomeetdifferingneeds.Atasessionlevel,staffdemonstratedtheabilitytothinkontheirfeetandadaptasession,ratherthanstickdoggedlytoa plan, to ensure participants remained engaged and without losing the essence of the learning. Our research suggests that, because of the adaptability demonstrated by providers, there was no impact on outcomesfromusingavarietyofvenueswithdifferentfacilities.
4.10 IncentivesThroughout the programme, participants were given ‘freebies’ such as measuring spoons, pasta measures, bats, balls, frisbees and aprons. The incentives provided by NCP went down well with participants and probably helped with both retention and sustainability of changes. Participants wespoketoenjoyedgettingsomethinganditmaintainedtheirinterest,keepingthemcomingback. In terms of sustaining change, measuring spoons and spaghetti measurers were given out so participants could put into practice what they had learned, and toys encouraged continued family play. The meals in a bag were nearly always used, and also provided store cupboard ingredients, like herbs and spices, which participants were able to continue using.

FINAL REPORT FEBRUARY 2018
26
5 What have we learned?5.1 Development of the modelAs is often the case with innovative interventions, the original design for MMMCs needed some adaptationonceitwasbeingimplementedinavarietyofdifferentsettings.Thechallengesthatemerged during early implementation were:
• Excluding pre-school children meant even mums with older children couldn’t attend because they couldn’t get child care.
• Running Clubs over a number of weeks and allowing participants to drop in and out presented a logistical challenge that most providers immediately shied away from, concerned about retention and the ability to manage numbers on an ad hoc basis.
• Providingphysicalactivitywassometimesdifficulteitherbecauseofvenueorparticipantresistance. This was compounded by the fact that the original name for the Clubs made no mention of physical activity, so participants didn’t expect it.
• Recipesdevisedinitially(bothbylocalprovidersandtheNCP)didn’treflectthelifestyleorcultureofthe participants. They were unfamiliar and therefore didn’t immediately appeal to participants.
• RunningClubsonlyinschoolholidaysmadeitdifficulttorecruitandretainparticipants,andmadeitdifficulttomaintainmomentumforthedeliveryteams,aswellaspracticalissuesoftemporarystaffingforshortperiods.
As providers fed back their concerns, the programme team had a choice to make – adhere to the original modelorallowadegreeofflexibility.Remainingtruetothemodelriskedfailuretomeettargetnumbers,butallowingflexibilityriskedlosingfidelitytowhatwasawell-researchedandplannedapproach.Italsomeantthatitcouldbegintolooklikesixdifferentprojects,insteadofacoherentprogramme.
Theprogrammeteamchosetoallowflexibility,whilstretainingfidelitytocoremessagesandcomponents. This was not an easy decision as, apart from anything else, it required a rebranding to take place ahead of year two. Make, Move and Munch Clubs was the result of the evolution from initial concepttopracticalapplication,enablingClubstorunatalltimesofyear,atdifferenttimesofthedayand to be moulded to suit the communities in which they were being delivered.
Certain elements had to remain true, with the provision of a nutritious meal remaining at the core. Learning about food and nutrition through cooking and information-giving remained, though the style and formality varied and was probably more informal than originally anticipated. Physical activity was included, but often as active play and walking rather than more structured exercise. Providers and the NCPworkedtogethertodevelopavarietyofrecipes,reflectingparticipants’culturesandlifestyleswhilst also being nutritionally balanced. These have been well-received, especially healthy versions of favouritefamilymealsand‘fakeaways’.Providershavegrowninconfidenceindevelopingrecipesandmeal makeovers, and successful recipes have been shared with other providers through the NCP.
5.2 Lessons learnedGivingprovidersflexibilityandallowingthemodeltoevolveasdescribedabovehasbeenkey.Themainlessonslearnedoverthepasttwoyearswhichhaveinfluencedthisevolutionaresummarisedbelow. We recommend that organisations planning to deliver MMMC or similar take these lessons into account when planning their intervention, as they proved crucial in the pilot phase.
5.2.1 Recruitment and retentionTapping into existing networks and working with other local organisations to recruit participants wasmoreeffectivethangeneralmarketing.Recruitmentwasresource-intensiveandpotential

FINAL REPORT FEBRUARY 2018
27
providers should not underestimate the time needed to recruit and retain participants. Use of social mediahelpedboostinterestandkeptparticipantsengaged.Wordofmouthwasalsoaneffectiverecruitment method once the Clubs were up and running.
5.2.2 RelationshipsHaving a trusted relationship with participants was essential. Whilst pre-existing relationships accelerated this, they were not essential. Taking time at the start and working through contacts known to participants helped develop these relationships. Keeping Clubs relaxed, informal, fun and social also helped develop relationships and the group dynamic.
5.2.3 The family approachIncluding children removed some of the barriers to accessing health interventions and acted as additionalmotivationforattendingandjoininginactivities.Childrenlearnedalongsidetheadultsandthis enabled reinforcement of learning at home, as they have a shared experience.
5.2.4 Delivering the messageHealthy eating messages did not have to be delivered by experts, but they needed to be clear, simple, and consistent. Use of visual aids to demonstrate salt, fat and sugar content were highly impactful, but more subtle approaches, such as informal chats, also helped reinforce messages. Practicality was essential: understanding how to make a change was as important as becoming convinced that change was needed.
5.2.5 Physical activityFormingaregularhabitaroundphysicalactivityisdifficultformanypeople,notonlyMMMCparticipants. Ensuring physical activity was pitched at the right level was important, so that participantswerenotfurtherputoffbysomethingthatwastoophysicallychallengingordifficulttofitin with their lifestyle. Some providers found pitching it right to be challenging. Activities that could be incorporated into daily life and existing routines, such as walking, active play and home exercise, were originallyconsideredmorelikelytobemoresustainable,andourfindingssupportthis.Toembedmorestructured exercise would require further support to remove barriers and help sustain any change.
5.2.6 Duration and timingRetainingparticipantsforeightweeksproveddifficult,asitrepresentedquiteacommitmentforparticipants. The dropout rates suggested that anything more than six sessions was challenging unless working with an existing group. The length of school holidays and school terms also tend to be closer to six weeks.
Most providers felt it would be possible to gain similar outcomes with slightly fewer sessions, and some thought a post intervention drop-in or some form of follow-up could help with sustaining change.However,theevidencecollectedduringthisevaluationdoesnotenableustoconfirmorchallenge this perception.
Deliveringatdifferenttimesofthedaymaximisedopportunitiesforallfamilies.Forexample,offeringaClub during the evening enabled parents that work to attend.
5.2.7 Acknowledge cultural differencesTailoringrecipesandmessagingtofittheculturalpreferencesoftheparticipantspromotedacceptabilityand uptake. It was far easier to elicit change when the familiarity of food was retained. For some cultures, participatinginphysicalactivityrequiresspecificcriteriatobeputinplace,forexamplefemaleinstructorsforMuslimwomen.Providersneededtobesensitivetothedifferentculturesofandwithingroups.
FINAL REPORT FEBRUARY 2018
28
5.3 Strategic added valueAswellasdeliveringpositiveoutcomesforprogrammeparticipants,ourfindingsindicatethatMMMCsalso delivered important Strategic Added Value (SAV)7.SAVwasfirstintroducedasameanstoevaluateRegionalDevelopmentAgencies’impactthatcamenotfromprogrammeandprojectspend,butontheirinfluenceonstakeholders’andpartners’behavioursandperformance.SAVhassincebeenadopted throughout numerous charitable and public agencies, and provides a very helpful lens through which to view the additional indirect impact of MMMC.
SAVincludesanumberofdifferentcategoriesofimpact,andfromourfindingsweconcludethatMMMC delivered in the following categories:
• strategic leadership & catalyst: articulating and communicating evidence-based approaches to delivering nutrition and physical activity messages in communities; supporting partners to increasetheircapacity,capabilityandconfidencetodeliverthesemessagesandactivitiesintheircommunities
• strategicinfluence:influencingpartnerstoincorporateMMMCmessagesintotheirfuturedeliverymodels; enabling and encouraging partners to build stronger local partnerships which will in turn lead to more widespread incorporation of MMMC messages into local health and wellbeing delivery
These are important outcomes – without MMMC, a number of partners would not have developed these new capabilities and partnerships, which have the potential to continue the legacy of MMMC beyond the programme’s lifetime.
5.4 Financial analysisThe pilot programme involved a combination of local delivery costs and national programme infrastructure costs, some of which related to being a pilot and would therefore not be required if MMMCsweretobereplicatedinfutureatalocallevel.Forthefinancialandeconomicaspectoftheprogramme evaluation we have considered the following:
• cost of pilot programme delivery – what it cost to deliver the programme in its pilot form, including the leadership and learning provided by the national programme team
• model costs for future local delivery, based on the learning and performance from the pilot programme – start-up year costs and annual ongoing delivery costs
• cost-consequenceanalysis–thefuturemodeldeliverycostsandthebenefitslikelytobegenerated
5.4.1 Cost of pilot programme deliveryEachlocaldeliveryprojectwasfundedfortwoyears,alongsidenationalleadership,supportandinfrastructureprovidedbytheprogrammeteam.Eachlocalprojectreceivedfundingrangingfrom£200,000 to £220,831 for the local delivery, and the programme team had a budget of £140,490 for nationalprogrammesupportcosts(excludingprogrammestaffingcosts),thereforethetotalcostofthe programme was £1,400,951.
7,700 individuals participated in the MMMCs across the two years, of whom 3,101 were adults.
The average local delivery cost per person7variedconsiderablybetweenprojects,rangingfrom£111.02to£173.33overtheprogrammeperiod.Furthermore,mostprojectshadnotablevariationsincostperpersonbetweenyearoneandyeartwo,reflectingthefactthatthiswasanewserviceforthem and recruitment was challenging. The table below shows the range of costs per person in years one and two.
7 Excluding programme level costs

FINAL REPORT FEBRUARY 2018
29
Figure 20: Cost per person for programme delivery
Average cost per person
Lowest cost per person
Highest cost per person
Year 1 £192.56 £86.93 £310.84
Year 2 £122.92 £66.35 £174.41
Average across both years £133.03 £111.02 £173.33
5.4.2 Model costs for future deliveryThevariationsintotalcostsandcostperpersonarosefromdifferentmanagementanddeliverymodels, and from the extent to which local deliverers were already experienced in designing and delivering similar interventions to a similar target group. In addition, the availability of venues and equipment contributed to varying costs.
Assumptions
In order to develop a model for how much future delivery might cost, if a new provider were to take on the MMMC concept, we made a number of assumptions:
• the provider would need to upskill their delivery team in order to be able to provide MMMCs – whether it involved learning the food and cooking aspects or the physical activity aspects, the most cost-effectivenewdeliverersinthepilotretaineddeliverywithintheirin-houseteamratherthansubcontracting to specialists
• the provider would need to invest in some equipment to enable delivery of MMMCs – this may include cooking equipment, physical activity equipment and learning resources
• duringthefirstyear,fewerparticipantsarelikelytobesupportedthaninfutureyears,duetothetime taken to establish and recruit to the programme (we calculated costs for a range between 500and800attendeesinthefirstyear)
• oncetheserviceisestablished(i.e.afterthefirstyear)costsarebasedon1000participantsperyear
• 40% of participants would be adults, with the remainder children• food costs per participant per session would be £2.70 at 2017 prices• each MMMC runs for eight sessions with an average of eight adult participants per session9
• deliverers would need to invest in printing and incentives for MMMCs, as these have been important aspects of the programme’s success – these have been included in the delivery costs at a rate of £2,500 per year
Weusedcostsfromthreeofthesixprojectstodevelopourmodelcosts.AllwerenewtotheconceptofMMMCandbroughtsomebutnotalloftherequiredskillsandexperience.Alltrainedtheirstaff,andorrecruitedadditionalstaff,toupskilltheirteams.Weexcludedthreeprojectsfromthemodellingastheywereconsideredatypical:onehadaparticularlychallengingfirstyearwhichmeanttheirnumbersand costs were not as expected; one was considerably more expensive than the others; and one had longstanding experience of delivering similar interventions in purpose-built facilities.
8 It would be possible to accommodate a larger group size with the same fixed costs. The variable costs (meal in a bag and per session food costs) would obviously increase, but the overall cost per person would decrease.

FINAL REPORT FEBRUARY 2018
30
Costs
Ourcostcalculationstookintoaccountfourdifferentcategoriesofcost:
• upfrontset-upcosts–stafftrainingandpurchaseofequipmentandresources• fixeddeliverycosts–staffsalaries,venuehire,printingandincentives• fixedmanagementcosts–recruitmentofparticipants,marketing,administrationandproject
management• variable delivery costs – food costs for one meal per person per session
The table below sets out the costs in the start-up year and future years. We have assumed all costs will bebornebythefunderoftheproject,withparticipantsreceivingtheservicewithoutcharge.
Figure 21: model costs to deliver a local MMMC from scratch over two years
Year 1Future years
(at 2017 prices)Set up costs
– Training £8,000 -
– Equipment/resources £14,000 -
Fixed delivery costs £60,000 £60,000
Fixed management costs £15,000 £15,000
Variable delivery costs (food per-person) £2.70 £2.70
Total participants 500 - 800 1000
Total adult participants 200 - 320 400
Total delivery cost £98,350 - £99,160 £77,700
Cost per person £123.95 - £196.70 £77.70
Cost per family (assume average 1 adult and 2 children) £309.88 - £491.75 £194.25
ItwasnotpossibletofindadirectcomparatorforMMMC,todeterminewhethertherelativevalueformoneyof MMMC was better or worse than other interventions. However, the NICE Physical Activity Return on Investment Tool cites the cost of an adult physical activity multi-component intervention at approximately £155 per person. Given the twin focus on healthy eating and physical activity, a per-family cost of £194.25 does not seem unreasonable. At a per person cost of £77.70, MMMC appears to have been good value formoney,especiallygiventhatourfindingsindicatetheprogrammeislayingafoundationforchildrentodevelop healthier eating and activity habits through their parents’ changes in behaviour.
9 It would be possible to accommodate a larger group size with the same fixed costs. The variable costs (meal in a bag and per session food costs) would obviously increase, but the overall cost per person would decrease.

FINAL REPORT FEBRUARY 2018
31
Cost-consequence analysis
Figure 22: Cost-consequence analysis based on local delivery to 250 individuals (100 adults) in year 1 and 1000 individuals (400 adults) in subsequent years)
Measures in the analysis Potential impact of MMMC on these measures
COSTS
Intervention cost to provider/commissioner – year 1
£98,350 - £99,160
Intervention cost to provider/commissioner – steady state (annual cost)
£77,700
BENEFITS10
Eating habits 51% of adults eating more vegetable portions
46% of adults eating more fruit portions
88 more adults eating more than 3 portions of vegetables
72 more adults eating more than 3 portions of fruit per day
Adults eating fewer snacks with high salt/sugar/fat
Children consuming fewer high sugar drinks
Adults now cooking one more main family meal from scratch per week
Adults now cooking more than half of main family meals from scratch using low sugar/fat/salt ingredients
Adults preparing fewer processed foods for themselves and the family
84 more adults referring to nutritional information when shopping, in order to choose lower sugar/fat/salt option
Physical activity 56 inactive adults becoming physically active
50% of adults increasing their levels of physical activity
72 more adults achieving government recommended physical activity levels
44 more adults being physically active 6 or 7 days per week
Adults participating in active play with their children
Family Parents involving children in cooking
Families eating together more often
Families spending more time playing together
93% more able to make their food budget last the week
Social Increasedsocialisation,integrationandconfidenceforchildren,includingthose at risk of social exclusion
Increased socialisation and reduced isolation for parents
10 Where absolute numbers (instead of percentages) are cited, these apply to steady state delivery (year 2 onwards)
FINAL REPORT FEBRUARY 2018
32
5.5 SustainabilityAs the NCP concluded at the end of 2017, funding for MMMCs stopped at that time. They agreed to leave as a legacy the MMMC name and branding, the learning resources and the tools to deliver MMMCs. The two charities involved will hold the resources and the evidence from MMMCs, to make available to interested partners. The NCP also presented the evaluation evidence at national and international public health conferences, to generate interest in the model. Whilst this activity and the remaining suite of resources are valuable, alone they will not ensure the sustainability of the intervention. Providers have taken steps, supported by the programme team, to engage local stakeholders that may be able to support MMMCs or something very similar going forward. This was followed by some initial planning by providers about how they could take MMMCs forward in their own areas.
Providers told us that MMMC aligns with a number of high priority agendas – health and wellbeing, family support, parenting programmes, obesity and community development, to name a few. Their experience has shown that it can be used as a programme to deliver health messages that also has socialbenefits;oritcanbeaninitiativethatusesfoodasthe‘hook’forrelationshipbuildingandothersocial outcomes that also delivers health messages. They believed this broad appeal meant it had the potential to be pitched to and funded by a range of organisations and public bodies.
WeheardfromlocalstakeholdersinthedifferentprojectareasabouthowsuccessfultheyfeltMMMCshadbeen,andthedifferencestheyhadseenintheirschoolsandcommunities.Headteachers,healthimprovementworkers,parentsupportofficers,communitylearninganddevelopmentworkersandpublic health representatives spoke favourably about their experience of MMMCs. Though they recognised the challenges of getting funding for such initiatives, they commented that, having seen thedifferencesMMMCshavedelivered,theywereadvocatingstronglyforcontinuation.Aswellasthe better eating and cooking habits delivered by MMMCs, they highlighted improved behaviour in children, healthier lunch boxes and quality family time as important outcomes that were priorities for their organisations.
Stakeholders also felt that integration of MMMCs with other initiatives was important; using MMMCs as an intervention to contribute to the broader agenda of reducing health inequalities and supporting families. No single intervention provided the solution but, linked with other interventions, they felt the style and ambition of MMMCs aligned well within a holistic approach to improving community and family wellbeing.
Some of the providers were already planning to draw elements of MMMC into their other initiatives, others were actively seeking funding or commissioning. Whilst they said the model may need to evolve and develop in response to local commissioning priorities, they intended to retain the core principles.
Most of the providers reported that they developed new skills and insights as a result of being part of MMMC – they learned more about how to deliver healthy eating and physical activity messages, and became convinced of the value of combining these messages with other community development work. They told us that this cultural and attitudinal shift, combined with their upskilling, meant that even where MMMC was not sustained in its current form, there were several providers out there now who would continue to live the principles of MMMC in all of their work.
Beyond the MMMC pilot areas, the challenge will be spreading the MMMC concept to new geographies. Theremaybeopportunitiesinsomeareasforthepilotprojectstospreadtheirpracticetoalargerpatch, but there are large areas of the UK that would not be reached through this approach. Therefore influencinguptakemorewidelywouldbeneeded.TheNCP’spromotionalactivityatconferenceshasgenerated interest, and thought needs to be given to how this can be continued after the end of the NCP. The dissemination of this evaluation may be instrumental in broadening interest and BHF and Diabetes UKwillbothhavearoletoplayinsharingthelearningtoencouragewideradoption.
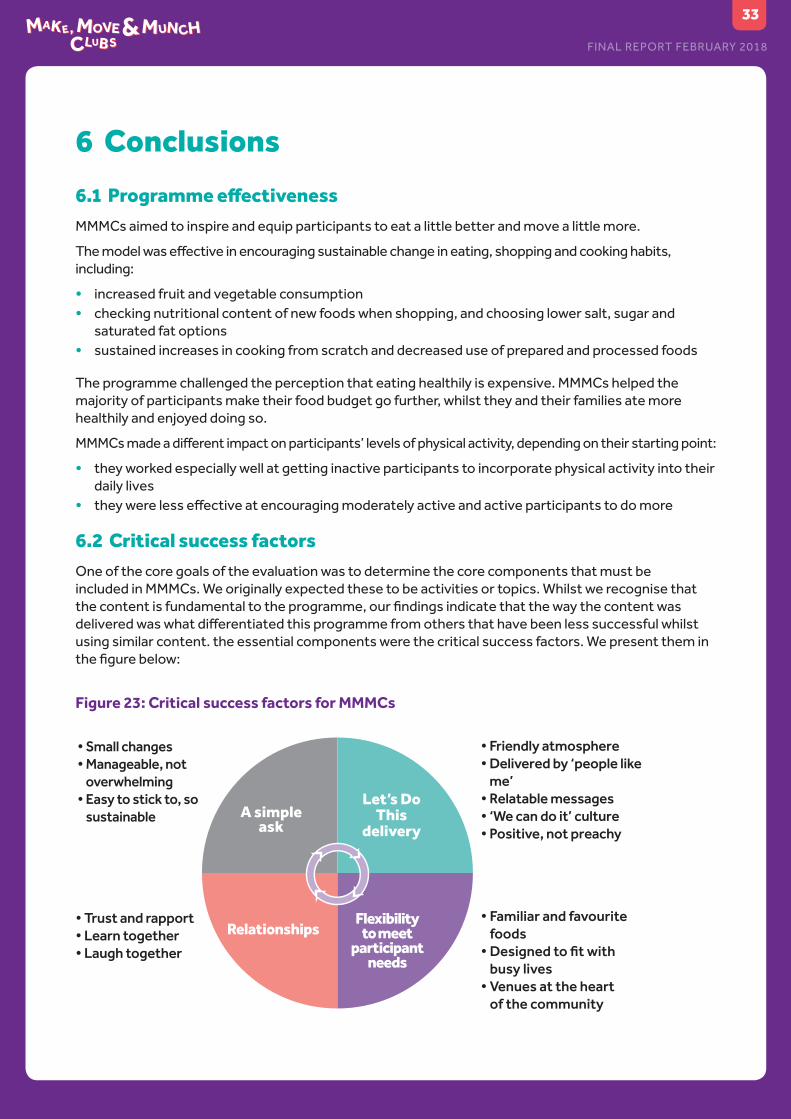
FINAL REPORT FEBRUARY 2018
33
6 Conclusions
6.1 Programme effectivenessMMMCs aimed to inspire and equip participants to eat a little better and move a little more.
Themodelwaseffectiveinencouragingsustainablechangeineating,shoppingandcookinghabits,including:
• increased fruit and vegetable consumption • checking nutritional content of new foods when shopping, and choosing lower salt, sugar and
saturated fat options• sustained increases in cooking from scratch and decreased use of prepared and processed foods
The programme challenged the perception that eating healthily is expensive. MMMCs helped the majorityofparticipantsmaketheirfoodbudgetgofurther,whilsttheyandtheirfamiliesatemorehealthilyandenjoyeddoingso.
MMMCsmadeadifferentimpactonparticipants’levelsofphysicalactivity,dependingontheirstartingpoint:
• they worked especially well at getting inactive participants to incorporate physical activity into their daily lives
• theywerelesseffectiveatencouragingmoderatelyactiveandactiveparticipantstodomore
6.2 Critical success factorsOne of the core goals of the evaluation was to determine the core components that must be included in MMMCs. We originally expected these to be activities or topics. Whilst we recognise that thecontentisfundamentaltotheprogramme,ourfindingsindicatethatthewaythecontentwasdeliveredwaswhatdifferentiatedthisprogrammefromothersthathavebeenlesssuccessfulwhilstusing similar content. the essential components were the critical success factors. We present them in thefigurebelow:
Figure 23: Critical success factors for MMMCs
A simple ask
RelationshipsFlexibility
to meet participant
needs
Let’s Do This
delivery
• Familiar and favourite foods
• Designed to fit with busy lives
• Venues at the heart of the community
• Trust and rapport• Learn together• Laugh together
• Small changes• Manageable, not
overwhelming• Easy to stick to, so
sustainable
• Friendly atmosphere• Delivered by ‘people like
me’• Relatable messages• ‘We can do it’ culture• Positive, not preachy
FINAL REPORT FEBRUARY 2018
“I know how to make healthy things much more quickly, I don’t feel we need to resort to a quick
takeaway option so much.”Manaza, London
34
These factors suggest important learning for the charities involved in the NCP, in terms of how they present prevention messages to local communities. Getting alongside people, encouraging them to make small changes in their daily lives, and supporting them with information and tools about how to do so, appears to lead to behavioural change that can be sustained and built upon.
6.3 Building a legacyAs well as delivering outcomes for participants, MMMCs made an impact on the organisations delivering the Clubs:
• increasedcapabilityandconfidencetodeliverevidence-basedhealthyeatingandphysicalactivitymessages to their communities (in some cases to the extent that it has changed the strategic direction of the organisation)
• intention to incorporate the key MMMC messages into future delivery • new and strengthened relationships with other local partners in community development, health,
wellbeing and education, which will lead to future collaborative opportunities as well as having supported MMMC delivery
These should lead to a legacy from MMMC, which extends beyond the programme’s lifetime.

FINAL REPORT FEBRUARY 2018
35
7 Appendix 1: Make, Move & Munch Logic Model
Rationale: There are 3.5 million people in the UK who have Type 2 diabetes and |7 million living with cardiovascular disease. These can be serious life-threatening conditions
Long term aim: Tesco, Diabetes UK and the British Heart Foundation will reduce the number of people at risk of Type 2 Diabetes and CVD
Objective 1: People and most at risk communities (potential risk of Type 2 Diabetes and CVD) will increase their physical activity, eat more healthily and know more about the conditions
INPUTS ACTIVITIES OUTPUTS OUTCOMES Behaviour (B), Attitude (A), Skills (S), Knowledge (K)
IMPACTS
£ raised in partnership with Tesco
In-kind contributions from BHF, DUK and Tesco
Support from local partners
Support from BHF, DUK and Tesco
Partnership Team resource
A meal (not breakfast)
Meal planning, recipes and cooking tips
Food labels and product swapping
Shopping on a budget
£10 of fruit and vegetables per family
Key messaging on healthy eating (lower salt, lower sugar, smaller portions)
CVD and T2 Diabetes awareness
CPR
Food Tasting sessions for adults
Self-esteem/self-worth building
Myth busting
Fun physical activities (for children and adults
No. of MMMCs
No. of participants, meals, people taking part in physical activities
No. of people trained in CPR
No. of fruit & vegetables handed out and eaten
No. of people taking part in tasting session
No. of resources created
HEALTHY EATINGPeople and most at risk communities (MARCS):• Buy healthier products (B)• Eat a more balanced diet (B)• Set goals for themselves to improve healthy eating (B)• Want to set goals for themselves to improve healthy eating (A)• Speak or write positively about healthy eating (A)• Encourage others to eat healthily (A)• Are able to cook a healthy meal (S)• Are able to budget to cook a healthy meal (S)• Are able to set realistic goals for themselves to improve healthy
eating (S)• Know the appropriate meal sizes for family members (K)• Have basic knowledge about food labels (K)• Know that health eating can reduce the risk of developing heart
disease and Type 2 Diabetes (K) PHYSICAL ACTIVITY People and most at risk communities (MARCS):• Are more physically active (B)• Participate in free local physical activities (B)• Set goals for themselves to improve physical activity (B)• Want to set goals for themselves to improve physical activity (A)•Feelconfidenttojoininlocalphysicalactivities(A)• Are able to set realistic goal for themselves to improve physical
activity (S)• Are able to plan walking/cycling routes to and from regular
destinations (S)• Are able to use tools to record their physical activity (S)• Know how to incorporate physical activity into their daily life (K)•Knowhowtofindoutaboutfreelocalphysicalactivities(K)• Know that regular physical activity can reduce the risk of developing heart disease and physical activity (K) SOCIAL OUTCOMESPeople and most at risk communities (MARCS):• Have increased social and peer support to be more physically
active and to eat socially (B)• View healthy eating and being physically active as a social norm
(A)• Are able to advocate for themselves and their community to improve local support for physical activity and healthy eating (S)•Knowwhotheleadersandcommunityinfluencersaretoimprove physical activity and healthy eating in the community (K)
People value health and wellbeing
People lead heathier lifestyles
Fewer people die from CVD and Type 2Diabetesprematurely
Reduction in heath inequalities
Brought to you by the National Charity Partnership – a partnership between Tesco and registered charities Diabetes UK and the British Heart Foundation

CONTACT
Brought to you by the National Charity Partnership – a partnership between Tesco and registered charities Diabetes UK and the British Heart Foundation
Independent evaluation of the Make, Move & Munch Club programme was undertaken by Brightpurpose

















