40
Flaps in otolaryngology BALASUBRAMANIAN THIAGARAJAN
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | shivjee-prashant |
| View: | 184 times |
| Download: | 3 times |

Flaps in
otolaryngologyBALASUBRAMANIAN THIAGARAJAN

Ideal flap
"when a part of one's person is lost, it
should be replaced in kind, bone for
bone, muscle for muscle, hairless skin
for hairless skin, an eye for an eye, a tooth for a tooth."
Ralph Millard

Introduction
The term "flap" first originated during the 16th century from the Dutch
word "flappe" meaning a structure that hung broad and loose,
fastened only on one side.
Flaps are usually used to repair structural defects following surgery i.e.
for malignant conditions of head and neck.

History
600 B.C. Susrutha performed nasal reconstruction using cheek flap
1440 A.D. Forehead rhinoplasty (India).
Pivotal flaps was preferred during early days. This involves rotation
of the flap around its vascular pedicle.
Advancement flap (French surgeons). This involves transfer of skin
from adjacent area without rotation.
History (contd)
McGregor - Who introduced the forehead flap during 1963
Bakamjian - Who introduced the deltopectoral flap during 1965
Ariyan - Who pioneered the Pectoralis major myocutaneous flap in
1979
Daniel & Taylor - Who pioneered the free flap in 1973
Flap surgery - Principles
Principle I : Replace like with like. This will go a long way in Camouflaging the surgical defect.
Principle II: Reconstruction should be thought in terms of units. It was Millard who divided the human body into 7 main parts (head, neck, body and extremities). He subdivided each of these parts into units. Each unit is further divided into subunits. These units and subunits should be considered and studied before the process of reconstruction is begun.
The most important aspect of these units are their borders. These borders include creases, margins and hair lines. Adherence to these borders during reconstruction is very important. It is always better to convert a partial unit defect into a whole unit defect before grafting. This will enable better consmesis.
Principle III: There should be a pattern and a fall back option always at hand.
Principle IV: The graft should be sutured without any tension. The donor area should not suffer excessive tissue loss.

Definition of flap / graft
Flap is a unit of tissue that can be transferred from one site (donor) to another (recipient site) while maintaining its own blood supply. Flap is transferred with its
blood supply intact, whereas a graft is a transfer of tissue without its own blood
supply. Survival of graft depends entirely on the blood supply from the recipient
site.

Facial incision
Classification of flap
Flaps may be classified according to their:
1. Blood supply
2. Tissue to be transferred
3. Location of donor site
Blood supply
For any graft tissue to survive blood supply is a must. If the
blood supply is derived from unnamed blood vessels then it is
termed as "Random flap". Many local skin flaps fall in this
category. If blood supply to the flap is derived from named
vessel / vessels it is referred to as "Axial flap". Most muscle flaps
fall in this category

Types of axial flaps
Type I Axial flap: Has only one vascular pedicle e.g. Facia lata
Type II Axial flap: Has blood supply served by dominant and Minor
pedicles e.g. Gracilis flap
Type III Axial flap: Has blood supply served by two dominant
pedicles e.g. Gluteus maximus flap
Type IV Axial flap: Has blood supply via segmental blood vessels
e.g. Sartorious flap
Type V Axial flap: Derives blood supply from one dominant pedicle
and many segmental blood vessels e.g. Latissmus dorsi flap

Axial flaps (contd)

Classification – according to tissue
to be transferred
Skin
Fascia
Muscle
Bone
Viscera (colon, small intestine, omentum)
Composite – Fasciocutaneous, myocutaneous, Tendocutaneous
and osseocutaneous flaps

Classification - Location
Tissue could be transferred from an area adjacent to the defect. This
type of flap is known as local flap. They may be further subclassified
depending on its geometric design.
Pivotal flaps: are also known as geometric flaps. They include
rotation, transposition, and interpolation types.
Advancement flaps: This type include single pedicle / Bipedicle / V-
Y flaps
Tissue transferred from non contiguous site i.e. distant flaps. These
flaps could either be pedicled or free flaps. The pedicled flaps are
still attached to their blood supply, while free flaps are totally severed from their blood supply and are reattached to vessels at
the recipient site (microanastomosis).

Advancement flap (History)
Celsus of ancient Rome as the first to perform advancement flap
French surgeons in 1800 popularized this flap as sliding flaps
Used to cover skin defects close to an area of skin laxity
Initially it was commonly used in forehead, scalp, eyelid and upper
lip areas

Vascularity of advancement flaps
Critical blood supply – 1-2 ml / min / 100g of tissue is adequate.
Advancement flaps depend on random blood supply arising from
anastomoses within subdermal / dermal plexus
Flap length : width ratio in head and neck region is 4:1

Types of advancement flaps
Monopedicled flap
Bipedicled flap
V – Y flaps
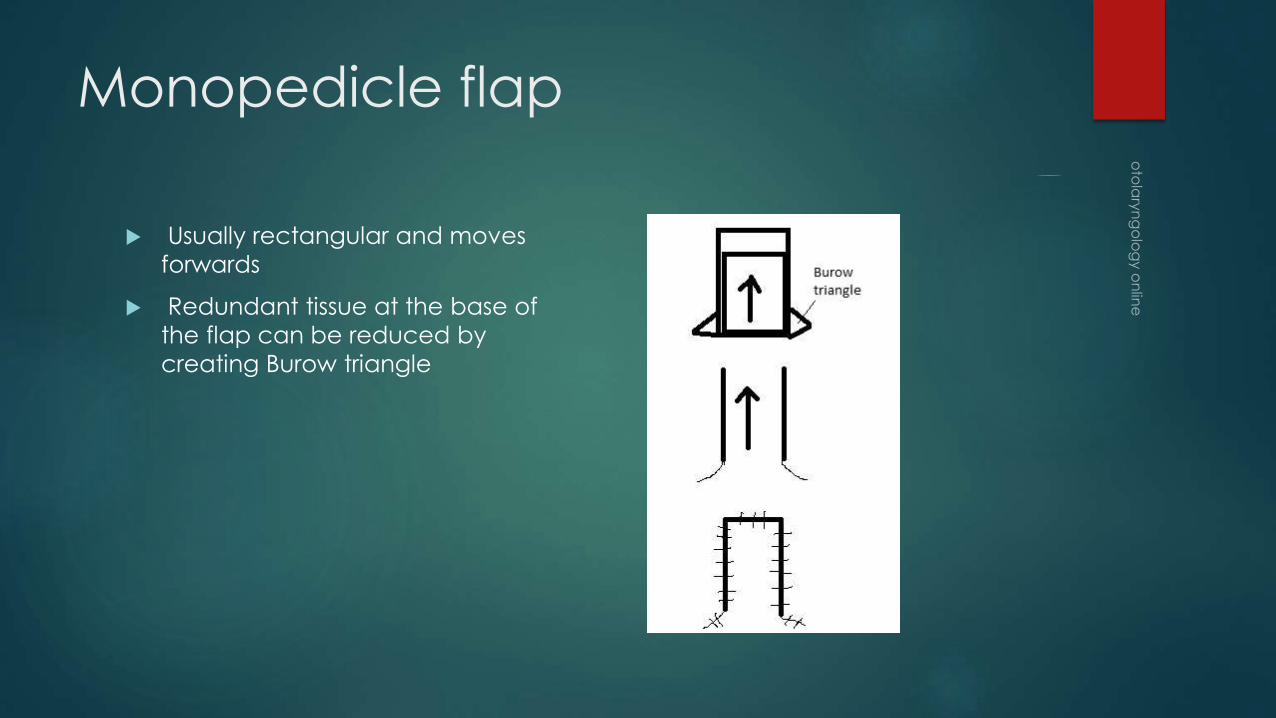
Monopedicle flap
Usually rectangular and moves
forwards
Redundant tissue at the base of
the flap can be reduced by
creating Burow triangle

Bipedicle flap
Incisions are made on each side
of flap
These are random flaps (obtain
blood supply from capillaries
rather than named arteries
Commonly these flaps are
generally skin

V – Y Flap
V – shaped incision
Broad base of V is advanced into
the defect
Resultant defect is closed (Y
shaped closure)
If long flaps are needed delay
phenomenon can be made use
of. After raising the flap 1-3 weeks
time is given before advancing it.
Delay phenomenon works
because the choked blood vessels
open up if time is given.

Glabellar flap
Best suited for reconstruction of
defects involving the bridge or
upper half of the nose.
Axial flap
Blood supply – supratrochlear
artery / dorsal nasal branches
Upper portion of incision should be
carried up to the periosteum
Mobilisation around naso frontal
angle should be carried out by
blunt dissection. Supra trochlear
vessels should be preserved

Sliding rotation degloving nasal
flap
Helps to cover the lower half of
the front of the nasal cavity
The degloving flap is outlined in
such a fashion that the incision to
mobilize the flap is on the right-
hand side along the nasolabial
fold going up to the glabellar
region.
The apex of the flap is in the
midline, with symmetrical right and
left limbs
Blood supply is from the nasolabial
artery

Nasolabial flap
Axial flap
Blood supply – Nasolabial artery
Width to length ratio – 1:5
Useful in covering defects over
lower portion of nose and ala of
the nose
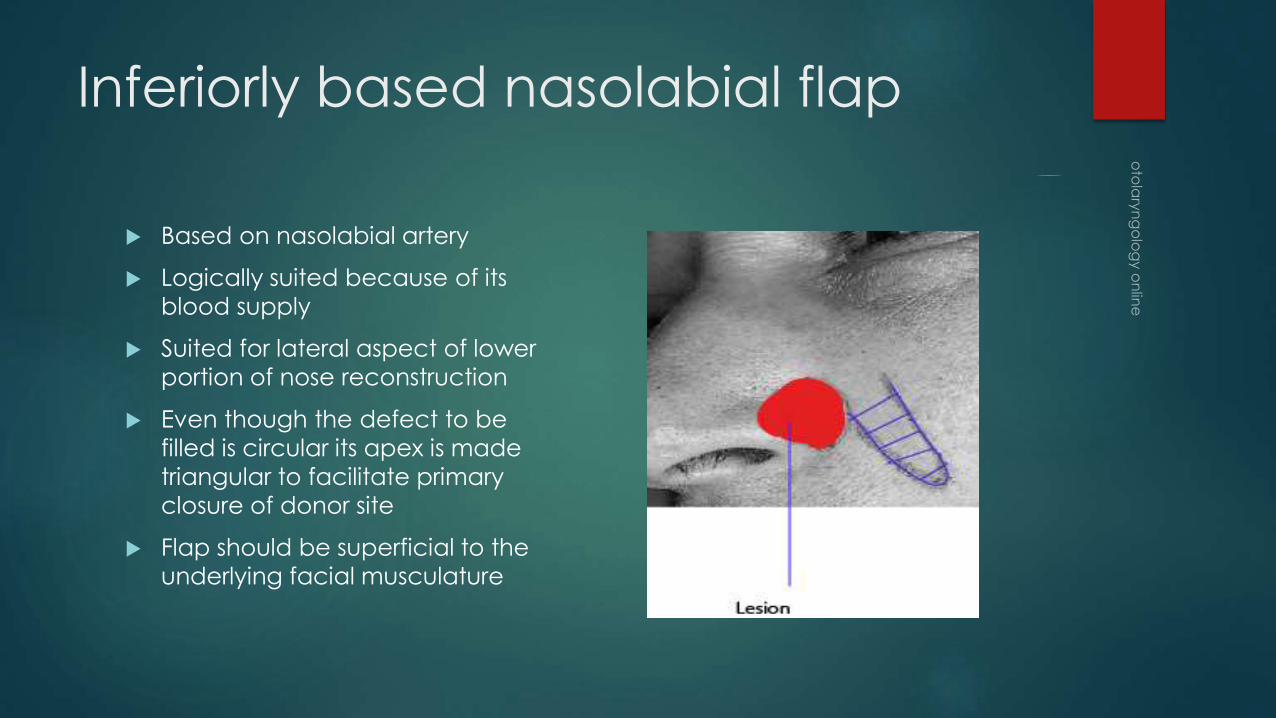
Inferiorly based nasolabial flap
Based on nasolabial artery
Logically suited because of its
blood supply
Suited for lateral aspect of lower
portion of nose reconstruction
Even though the defect to be
filled is circular its apex is made
triangular to facilitate primary
closure of donor site
Flap should be superficial to the
underlying facial musculature
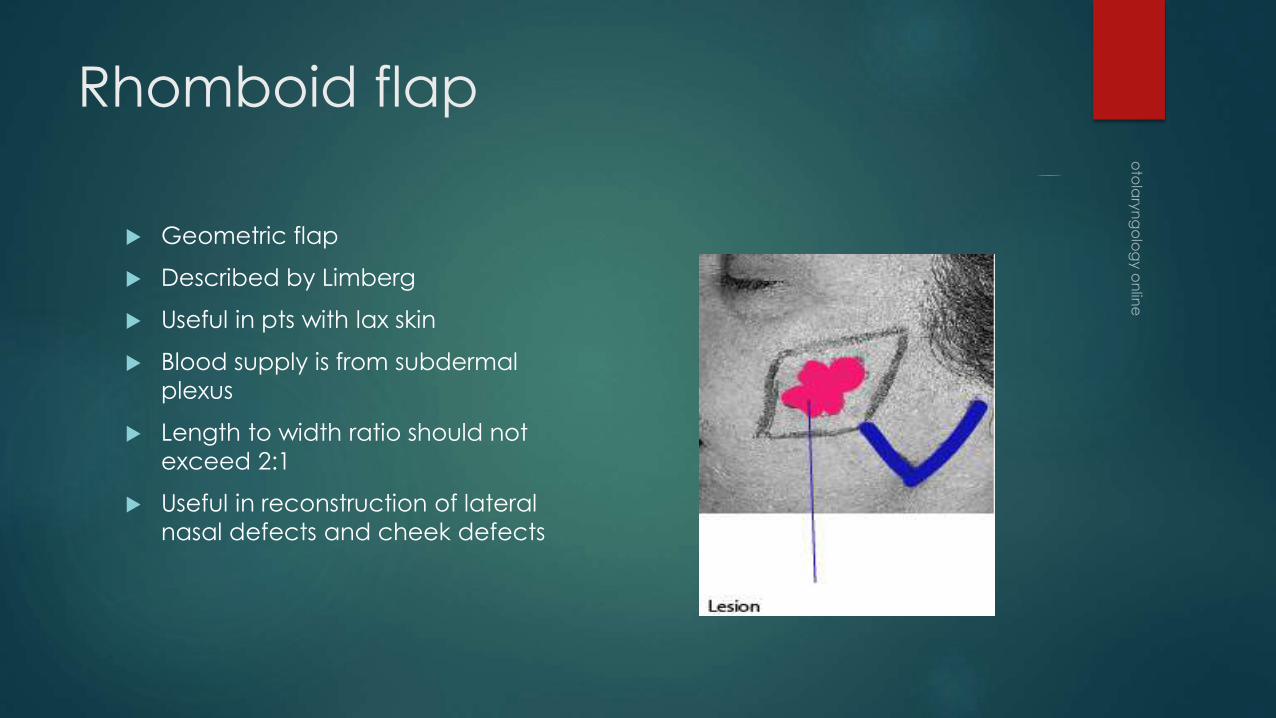
Rhomboid flap
Geometric flap
Described by Limberg
Useful in pts with lax skin
Blood supply is from subdermal
plexus
Length to width ratio should not
exceed 2:1
Useful in reconstruction of lateral
nasal defects and cheek defects

Mustardé Advancement Rotation
Cheek Flap
1. Defects of infraorbital region / medial
part of cheek can be closed using
this cheek flap
2. Blood supply is from the terminal
branches of facial artery
3. Flap should be mobilized up to the
angle of the mandible to avoid
unnecessary tension to the flap
4. Superior aspect of incision is towards
the temple – prevents drooping of
lateral canthus of eye
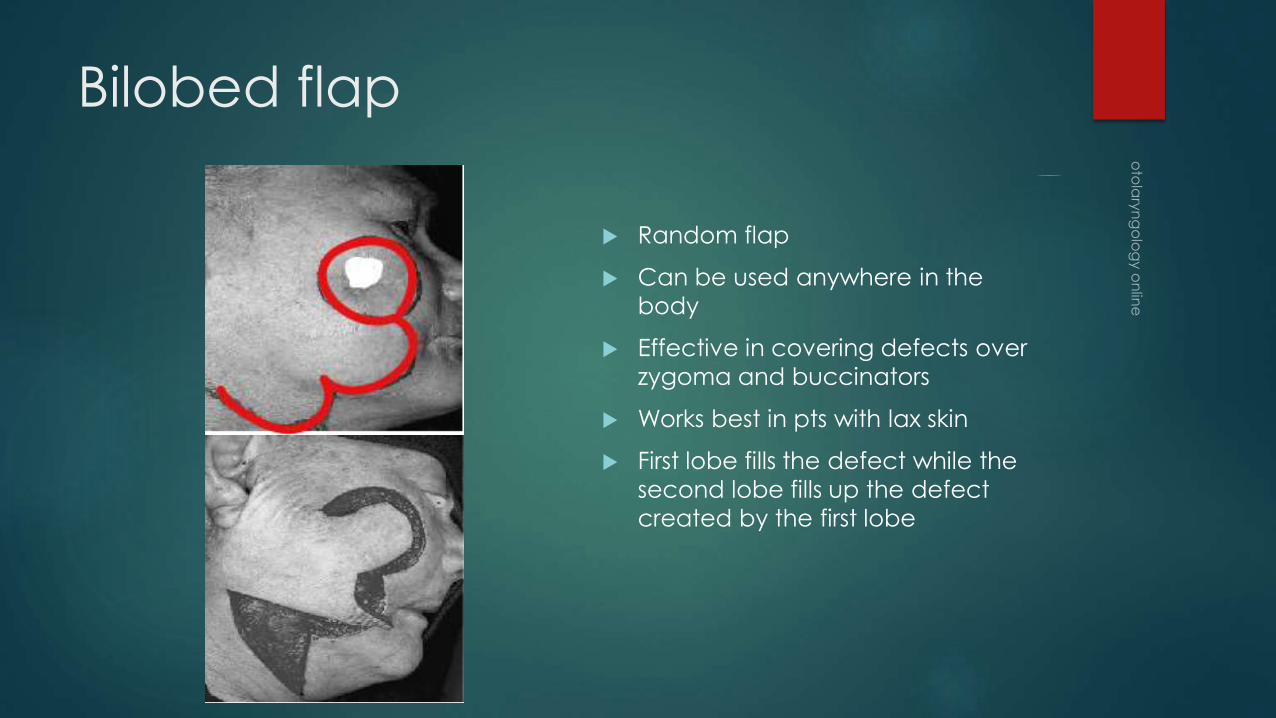
Bilobed flap
Random flap
Can be used anywhere in the
body
Effective in covering defects over
zygoma and buccinators
Works best in pts with lax skin
First lobe fills the defect while the
second lobe fills up the defect
created by the first lobe

Cervical flap
Regional cutaneous flap
Useful to cover lower half of the
face and upper neck
Vascularity from subdermal
arterical plexus
Length to width ratio not to
exceed 3:1
Neck dissection if need be can be
performed via the same incision
Flap is to be elevated superficial to
platysma

Myocutaneous flaps
Includes skin, subcutaneous tissues
and muscles
Useful in sealing large defects
Classified according to their
vascular patterns and locations
1. Pectoralis major myocutaneous
flap
2. Deltopectoral flap
3. Radial forearm free flap
4. Temporalis flap

Pectoralis major myocutaneous
flap
Myocutaneous flap
Pectoral branch of
acromiothoracic artery
Enters the muscle just below
clavicle at the junction of middle
and outer thirds
Useful in reconstruction of oral
cavity, oropharynx, hypopharynx
and larynx
Pectoralis major myocutaneous
flap – elevation tips
1. The incision should be made above the nipple in male and below
the breast in the female patient.
2. Pedicle should be identified carefully to preserve the vascularity
of the flap
3. After repair of the defect rubber drains should be placed
Deltopectoral flap
Bakamjian in 1965
Axial flap
Supplied by perforating branches
of internal mammary artery
Can cover any site of the neck up
to the level of zygoma.
Advantage – Flap retraction
occurs from side to side and not
from end to end.

Deltopectoral flap (contd)
Flap is outlined in the anterior chest wall and shoulder
Dissection plane – deep to pectoral and deltoid muscle fascia
Muscle fibres should be seen as the flap is being elevated
Elevation of this flap should only be done up to 2cms lateral to the
sternal border taking care to avoid injury to perforating arteries
Donor site should be covered with split thickness skin graft

Radial forearm flap
Faciocutaneous flap based on
radial artery
Venous outflow is from the
superficial veins of forearm
Used to reconstruct oral cavity,
oropharynx and hypopharyx
This flap includes skin from the
anterior cubital fossa to the flexor
crease at the wrist. Skin should not
be elevated over the ulnar artery

Abbe Estlander flap
This flap is commonly used to
reconstruct defects involving lips
and commissures
Full thickness flap with skin /
muscle / mucous membrane are
used
The flap can be marked, rotated
and sutured leading to the
formation of new commissure

Temporoparietal flap
Based on superficial temporal
artery
Both anterior and posterior
branches of superficial temporal
artery should be included
Size of the flap should be the size
of temporalis muscle
The arch of the zygoma should be
fractured to deliver the flap into
the oral cavity
Donor site should be closed
primarily

Hadad Flap
Used for skull base reconstruction
Mucoperichondrial/periosteal flap
Based on nasoseptal artery
Commonly used for anterior skull
base reconstruction

Hadad flap - Indications
Skull base reconstruction after endonasal surgery
To prevent communication between brain and sinuses
To repair anterior skull base leak

Hadad flap - advantages
Robust blood supply
Superior arc of rotation
Provides enough area to cover entire anterior skull base
Can be safely stored in nasopharynx if the procedure needs to be
staged
Can be taken down and reused in revision cases


















