Issue Date 2019-10 See shaded sections: Updated information from 2019-04 version. Dimension ® clinical chemistry system A1C Flex ® reagent cartridge DF105B Hemoglobin A1C Assay Intended Use: The Dimension® Hemoglobin A1C assay is an in vitro diagnostic assay for the quantitative determination of %HbA1c (DCCT/NGSP) and mmol/mol HbA1c (IFCC) in human anticoagulated venous whole blood for use on the Dimension® clinical chemistry system. Measurement of Hemoglobin A1c is used as an aid in diagnosis and monitoring of long-term blood glucose control in patients with diabetes mellitus and as an aid in the identification of patients at risk for developing diabetes mellitus. Summary: HbA1c refers to the product of a non-enzymatic reaction between glucose and hemoglobin A1. The human erythrocyte is freely permeable to glucose, which can non-enzymatically combine with hemoglobin to form HbA1c. This non-enzymatic reaction between the alpha-amino group of the N-terminal valine of the hemoglobin beta-chain and glucose takes place to form an unstable aldimine or Schiff base intermediate (labile fraction). This reaction is slow and reversible and occurs at a rate that is proportional to the glucose concentration in the blood. The aldimine intermediate subsequently undergoes a non-reversible Amadori rearrangement to form the stable ketoamine 1-glucofrutovaline product. Since the reaction is driven by the concentration of reactants, the degree of glycosylation (reported as HbA1c relative to the total hemoglobin) is proportional to the average concentration of blood glucose over the circulating life span of hemoglobin in the red cell (approximately 120 days). 1,2 The utility of HbA1c measurements was demonstrated in the Diabetes Control and Complications Trial (DCCT). 3 A significant finding of this study was the direct correlation between glycemic control and patient outcome with respect to long-term complications. Patients with improved glycemic control (i.e., lower HbA1c) showed significantly improved prognosis with respect to micro-vascular complications including neuropathy, retinopathy, and nephropathy. 3 Principles of Procedure: The Dimension® Hemoglobin A1C assay measures both HbA1c and total hemoglobin. The HbA1c measurement is based on a turbidimetric inhibition immunoassay (TINIA) principle, and the measurement of total hemoglobin is based on a modification of the alkaline hematin reaction. Using the values obtained for each of these two analytes, the relative proportion of the total hemoglobin that is glycated is calculated and reported. Pre-treatment to remove the labile fraction is not necessary as only the Amadori rearranged form of HbA1c is detected. All hemoglobin variants that are glycated at the beta-chain N-terminus and have epitopes identical to that of HbA1c are measured by this assay. Total Hemoglobin Measurement: A sample of whole blood is added to the first cuvette containing lysing reagent. This reagent lyses the red blood cells and simultaneously converts the released hemoglobin to a derivative that has a characteristic absorbance spectrum. An aliquot of the lysed whole blood is transferred from the first cuvette to a second cuvette where total hemoglobin concentration is measured at 405 nm and 700 nm. 4 Whole blood + lysing agent Released hemoglobin hemoglobin derivative (measured at 405 nm) Hemoglobin A1c Measurement: The same aliquot of the lysed whole blood that is transferred from the first cuvette to the second cuvette for the Hb measurement is also used for the measurement of HbA1c. The second cuvette contains an anti-HbA1c antibody in a buffered reagent. Hemoglobin A1c in the sample reacts with anti-HbA1c antibody to form a soluble antigen-antibody complex. A polyhapten reagent containing multiple HbA1c epitopes is then added to this cuvette. The polyhapten reacts with excess (free) anti-HbA1c antibodies to form an insoluble antibody-polyhapten complex. The rate of this reaction is measured turbidimetrically at 340 nm and blanked at 700 nm and is inversely proportional to the concentration of HbA1c in the sample. hemoglobin A1c + anti-HbA1c antibody hemoglobin A1c-anti-HbA1c antibody complex anti-HbA1c antibody (excess) + polyhapten Ab/polyhapten complex (absorbs at 340 nm) A1C Kit Components Note: Each kit lot contains matched sets of A1C Flex® reagent cartridges and calibrators. These components are not interchangeable between kits with other lot numbers. Reagents Wells a Form Ingredient Concentration b Source 1–2 Liquid Antibody ≥0.5 mg/mL c Sheep, Polyclonal from ovine serum MES d Buffer 0.025 M TRIS e Buffer 0.015 M Stabilizers 3 Liquid Polyhapten Reagent ≥8 µg/mL MES d Buffer 0.025 M TRIS e Buffer 0.015 M Stabilizers 4 Empty 5–6 Liquid TTAB f <1% (hemolyzing reagent) a. Wells are numbered consecutively from the wide end of the cartridge. b. Nominal value per well in a cartridge. c. Antibody titer and conjugate activity (or particle reagent concentration) may vary from lot to lot. d. MES = 2-morpholinoethane sulfonic acid e. TRIS = tris(hydroxymethyl)-aminomethane f. TTAB = tetradecyl trimethyl ammonium bromide Risk and Safety: H412 P273, P501 Warning! Harmful to aquatic life with long lasting effects. Avoid release to the environment. Dispose of contents and container in accordance with all local, regional, and national regulations Contains: 2-methyl-H4-isothiazol-3-one Safety data sheets (MSDS/SDS) available on siemens.com/healthcare Precautions: Used cuvettes contain human body fluids; handle with appropriate care to avoid skin contact or ingestion. Caution: Federal (USA) law restricts this device to sale by or on the order of a licensed healthcare professional. For in vitro diagnostic use Note: The A1C Flex® reagents and calibrators are packaged in a kit. Each kit lot contains matched sets of A1C Flex® reagent cartridges and A1C Calibrators. Do not interchange reagents with different lot numbers. Reagent Preparation: All reagents are liquid and ready to use. Store at: 2–8°C Expiration: Refer to carton for expiration date of the kit. All kit components are stable until the expiration date when stored unopened at 2–8°C. Sealed cartridge wells on the instrument are stable for 30 days. Open Well Stability: 5 days for wells 1–2 and 5–6 10 days for well 3 Specimen Collection and Handling: Recommended specimen type: Anticoagulated venous whole blood (K 2 EDTA; K 3 EDTA; sodium fluoride/Na 2 EDTA; lithium heparin, or Na Fluoride/K-Oxalate). Specimens should be collected using recommended procedures for collection of diagnostic blood specimens by venipuncture. 5–7 Follow the instructions provided with your specimen collection device for use and processing. 6 • Samples for the A1C method can only be assayed from a sample cup or SSC. • Samples cannot be assayed directly from primary collection tubes. • Samples should be mixed gently by inversion (gently invert the tube ten times) or in a rocker mixer prior to pipetting into the sample cup or SSC in order to obtain uniform distribution of the erythrocytes prior to testing. Avoid the formation of foam. • Samples containing clots should not be used. • Pipette 200 µL of the whole blood sample into the sample cup or SSC. • Sample can sit in sample cup on instrument for up to one hour. Specimen Stability: Samples are stable when stored for no greater than: 8 3 days at 15–25°C 7 days at 2–8°C 4 months at -20°C (freeze only once) The purpose of this specimen storage information is to provide guidance to users; however, users may validate their own procedures for storing samples. Procedure Materials Provided A1C Kit, Cat. No. DF105B: Includes A1C Flex® reagent cartridges and A1C calibrator (5 levels) Materials Required But Not Provided Quality Control Materials Test Steps Sampling g , reagent delivery, mixing, and processing are automatically performed by the Dimension® clinical chemistry system. For details of this processing, refer to your Dimension® Operator’s Guide. g. The sample container must contain 200 μL whole blood to ensure proper re-mix. Test Conditions Cuvette 1 Cuvette 2 Sample Volume 3 µL (from sample cup) 19 µL (from cuvette 1) Hemolyzing Reagent Volume 300 µL 0 µL Antibody/Buffer Volume 0 µL 320 µL Polyhapten Volume 0 µL 52 µL Diluent Volume 147 µL 69 µL Temperature 37°C 37°C Test wavelength 340 and 700 nm for hemoglobin A1c 405 and 700 nm for hemoglobin Type of Measurement Turbidimetric for hemoglobin A1c Colorimetric for hemoglobin
Transcript
Issue Date 2019-10See shaded sections: Updated information from 2019-04 version.
Dimension® clinical chemistry system
A1CFlex® reagent cartridge
DF105B
Hemoglobin A1C AssayIntended Use: The Dimension® Hemoglobin A1C assay is an in vitro diagnostic assay for the quantitative determination of %HbA1c (DCCT/NGSP) and mmol/mol HbA1c (IFCC) in human anticoagulated venous whole blood for use on the Dimension® clinical chemistry system. Measurement of Hemoglobin A1c is used as an aid in diagnosis and monitoring of long-term blood glucose control in patients with diabetes mellitus and as an aid in the identification of patients at risk for developing diabetes mellitus.
Summary: HbA1c refers to the product of a non-enzymatic reaction between glucose and hemoglobin A1. The human erythrocyte is freely permeable to glucose, which can non-enzymatically combine with hemoglobin to form HbA1c. This non-enzymatic reaction between the alpha-amino group of the N-terminal valine of the hemoglobin beta-chain and glucose takes place to form an unstable aldimine or Schiff base intermediate (labile fraction). This reaction is slow and reversible and occurs at a rate that is proportional to the glucose concentration in the blood. The aldimine intermediate subsequently undergoes a non-reversible Amadori rearrangement to form the stable ketoamine 1-glucofrutovaline product. Since the reaction is driven by the concentration of reactants, the degree of glycosylation (reported as HbA1c relative to the total hemoglobin) is proportional to the average concentration of blood glucose over the circulating life span of hemoglobin in the red cell (approximately 120 days).1,2
The utility of HbA1c measurements was demonstrated in the Diabetes Control and Complications Trial (DCCT).3 A significant finding of this study was the direct correlation between glycemic control and patient outcome with respect to long-term complications. Patients with improved glycemic control (i.e., lower HbA1c) showed significantly improved prognosis with respect to micro-vascular complications including neuropathy, retinopathy, and nephropathy.3
Principles of Procedure: The Dimension® Hemoglobin A1C assay measures both HbA1c and total hemoglobin. The HbA1c measurement is based on a turbidimetric inhibition immunoassay (TINIA) principle, and the measurement of total hemoglobin is based on a modification of the alkaline hematin reaction. Using the values obtained for each of these two analytes, the relative proportion of the total hemoglobin that is glycated is calculated and reported. Pre-treatment to remove the labile fraction is not necessary as only the Amadori rearranged form of HbA1c is detected. All hemoglobin variants that are glycated at the beta-chain N-terminus and have epitopes identical to that of HbA1c are measured by this assay.
Total Hemoglobin Measurement: A sample of whole blood is added to the first cuvette containing lysing reagent. This reagent lyses the red blood cells and simultaneously converts the released hemoglobin to a derivative that has a characteristic absorbance spectrum. An aliquot of the lysed whole blood is transferred from the first cuvette to a second cuvette where total hemoglobin concentration is measured at 405 nm and 700 nm.4
Whole blood + lysing agent Released hemoglobin hemoglobin derivative (measured at 405 nm)
Hemoglobin A1c Measurement: The same aliquot of the lysed whole blood that is transferred from the first cuvette to the second cuvette for the Hb measurement is also used for the measurement of HbA1c. The second cuvette contains an anti-HbA1c antibody in a buffered reagent. Hemoglobin A1c in the sample reacts with anti-HbA1c antibody to form a soluble antigen-antibody complex. A polyhapten reagent containing multiple HbA1c epitopes is then added to this cuvette. The polyhapten reacts with excess (free) anti-HbA1c antibodies to form an insoluble antibody-polyhapten complex. The rate of this reaction is measured turbidimetrically at 340 nm and blanked at 700 nm and is inversely proportional to the concentration of HbA1c in the sample.
Note: Each kit lot contains matched sets of A1C Flex® reagent cartridges and calibrators. These components are not interchangeable between kits with other lot numbers.
Reagents
Wellsa Form Ingredient Concentrationb Source1–2 Liquid Antibody ≥0.5 mg/mLc Sheep, Polyclonal from ovine serum
a. Wells are numbered consecutively from the wide end of the cartridge.b. Nominal value per well in a cartridge.c. Antibody titer and conjugate activity (or particle reagent concentration) may vary from lot to lot.d. MES = 2-morpholinoethane sulfonic acide. TRIS = tris(hydroxymethyl)-aminomethanef. TTAB = tetradecyl trimethyl ammonium bromide
Risk and Safety:H412P273, P501
Warning!Harmful to aquatic life with long lasting effects.
Avoid release to the environment. Dispose of contents and container in accordance with all local, regional, and national regulations
Contains: 2-methyl-H4-isothiazol-3-one
Safety data sheets (MSDS/SDS) available on siemens.com/healthcare
Precautions: Used cuvettes contain human body fluids; handle with appropriate care to avoid skin contact or ingestion.
Caution: Federal (USA) law restricts this device to sale by or on the order of a licensed healthcare professional.
For in vitro diagnostic use
Note: The A1C Flex® reagents and calibrators are packaged in a kit. Each kit lot contains matched sets of A1C Flex® reagent cartridges and A1C Calibrators. Do not interchange reagents with different lot numbers.
Reagent Preparation: All reagents are liquid and ready to use.
Store at: 2–8°C
Expiration: Refer to carton for expiration date of the kit. All kit components are stable until the expiration date when stored unopened at 2–8°C. Sealed cartridge wells on the instrument are stable for 30 days.
Open Well Stability: 5 days for wells 1–2 and 5–6 10 days for well 3
Specimen Collection and Handling: Recommended specimen type: Anticoagulated venous whole blood (K2 EDTA; K3 EDTA; sodium fluoride/Na2 EDTA; lithium heparin, or Na Fluoride/K-Oxalate).
Specimens should be collected using recommended procedures for collection of diagnostic blood specimens by venipuncture.5–7 Follow the instructions provided with your specimen collection device for use and processing.6
• Samples for the A1C method can only be assayed from a sample cup or SSC. • Samples cannot be assayed directly from primary collection tubes. • Samples should be mixed gently by inversion (gently invert the tube ten times) or in a rocker mixer prior
to pipetting into the sample cup or SSC in order to obtain uniform distribution of the erythrocytes prior to testing. Avoid the formation of foam.
• Samples containing clots should not be used.• Pipette 200 µL of the whole blood sample into the sample cup or SSC.• Sample can sit in sample cup on instrument for up to one hour.
Specimen Stability: Samples are stable when stored for no greater than:8
3 days at 15–25°C 7 days at 2–8°C 4 months at -20°C (freeze only once)
The purpose of this specimen storage information is to provide guidance to users; however, users may validate their own procedures for storing samples.
Procedure
Materials ProvidedA1C Kit, Cat. No. DF105B: Includes A1C Flex® reagent cartridges and A1C calibrator (5 levels)
Materials Required But Not ProvidedQuality Control Materials
Test Steps
Samplingg, reagent delivery, mixing, and processing are automatically performed by the Dimension® clinical chemistry system. For details of this processing, refer to your Dimension® Operator’s Guide.
g. The sample container must contain 200 μL whole blood to ensure proper re-mix.
405 and 700 nm for hemoglobinType of Measurement Turbidimetric for hemoglobin A1c
Colorimetric for hemoglobin
CalibrationThe general calibration procedure is described in your Dimension® Operator’s Guide.
Note: The A1C Flex® reagents and calibrators are packaged in a kit. Each kit lot contains matched sets of A1C Flex® reagent cartridges and A1C Calibrators. Do not interchange reagents with different lot numbers.
The system automatically performs the calibration for both Hb and HbA1c.
The Dimension® Hemoglobin A1C assay requires lot-specific scalers which must be entered in the Calibration Set Up screen, prior to calibration. The scaler values are provided on the Flex® reagent cartridge carton. These scalers are applied to all QC and patient results to maintain accuracy. Failure to enter the lot-specific scalers will cause inaccurate results.
The A1C method offers two options for calibration and reporting of results.
Option 1:
• Results reported in %HbA1c using the following equation:
%HbA1c = 100 xHbA1c (g/dL)
Hb (g/dL)
• Calibrator values (g/dL) are required for hemoglobin A1c and total hemoglobin. These values are obtained from the Table of Assigned Values provided in the Dimension® Hemoglobin A1C Calibrator Instructions for Use (IFU).
• Subsequently the Dimension® clinical chemistry system calculates an NGSP standardized %HbA1c result based on the calculation shown below. This calculation provides a %HbA1c value that is standardized to the DCCT study result, which is printed on the Dimension® report slip. The values of the polynomial coefficients (b, c and d) may vary by Flex® reagent cartridge lot.
NGSP Standardized %HbA1c = (b x (%HbA1c)2) + (c x %HbA1c) + d
A1C lots are produced under controlled conditions to meet established product specifications. Annually, one lot is tested on each Dimension® model to confirm standardization to the National Glycohemoglobin Standardization Program (NGSP). Copies of certificates may be accessed at www.siemens.com/diagnostics. Additional information concerning NGSP certification may be obtained at www.ngsp.org.9
Option 2:
• Results reported in SI unit [mmol/mol]h using the following equation:
mmol/mol HbA1c = 1000 xHbA1c (mmol/L)
Hb (mmol/L)
• Calibrator values (mmol/L) are required for hemoglobin A1c and total hemoglobin. These values are obtained from the Table of Assigned Values provided in the Dimension® Hemoblobin A1C Calibrator IFU.
• Subsequently the Dimension® system calculates an IFCC standardized mmol/mol A1C result based on the calculation shown below. This calculation provides a mmol/mol HbA1c value that is standardized to the IFCC reference system9, which is printed on the Dimension® report slip. The values of the polynomial coefficients (b, c and d) may vary by Flex® reagent cartridge lot.
IFCC Standardized HbA1c (mmol/mol) = (b x (HbA1c mmol/mol)2) + (c x HbA1c mmol/mol) + d
h. Système International d’Unités [SI Units] are in brackets.
Calibration Material Secondary calibrators such as A1C calibratorsCalibration Scheme 2 levels, n=5 for Hbi
5 levels, n=5 for HbA1ci
Units % [mmol/mol]Typical Calibration Levels 5.0–25.0 g/dL [3.1–15.5 mmol/L] Hb
0.25–2.90 g/dL [0.16–1.80 mmol/L] HbA1cCalibration Frequency Every 30 days for any one lotA new calibration is required • For each new lot of Flex® reagent cartridges
• After major maintenance or service, if indicated by quality control results• As indicated in laboratory quality control procedures• When required by government regulations
Scalers See Flex® reagent cartridge carton for lot-specific scaler values.Calibration cups must be filled with 600 µL of calibrator.i. The calibration results for HbA1c are automatically displayed; refer to the Calibration report for calibration results
for Hb.
Calibration Acceptance Criteria
The Dimension® Hemoglobin A1C assay requires confirmation of additional calibration guidelines; after calibration is complete, ensure that the following criteria are met:
Data Acceptance Guideline Comments
Hemoglobin A1c (A1C) Slope (m) 0.95–1.05 N/A
Hemoglobin A1c (A1C) y-intercept (b) Close to 0 Not clinically significant
Hemoglobin (HB BV) Accuracy (g/dL [mmol/L])
Mean ± 10%Average the 5 report results and compare to HB BV data
A reflection of the precision of the individual total hemoglobin milliabsorbance values used for the calculation of the “EX” calibration coefficient.
Quality ControlFollow government regulations or accreditation requirements for quality control frequency. At least once each day of use, analyze two levels of a Quality Control (QC) material with known hemoglobin A1c concentrations. Follow your laboratory internal QC procedures if the results obtained are outside acceptable limits.
Note: It is important to consider the local, or regional medical usefulness requirements when establishing acceptable limits for quality control (for example, College of American Pathologists (CAP), Deutschen Gesellschaft für Klinische Chemie und Laboratoriumsmedizin (DGKL) and others).
Results: The Dimension® system automatically calculates concentrations of total A1c, Hb, and HbA1c using the calculation scheme illustrated in your Dimension® Operator’s Guide.
The system reports the results in a single unit (% or mmol/mol); to manually convert the reporting unit with either the IFCC NGSP “Master Equation” or the NGSP IFCC “Master Equation” recommended by the International Federation for Clinical Chemistry Subcommittee on Hemoglobin A1c standardization,10,11 use the equations shown below:
Calculated HbA1c Ratio (A1C): 3.8–14.0% [18–130 mmol/mol]
The Hb and HbA1c analyte values can be measured directly from the specimen without any dilution or pretreatment that is not part of the usual analytical process. Hb and HbA1c analyte values outside of the ranges above will trigger a test report message to appear with the Calculated HbA1c Ratio result.
The Calculated HbA1c Ratio range has been validated by Siemens using native whole blood samples. This range may be used for laboratory validation of AMR, if needed.
Samples with results in excess of 14.0% [130 mmol/mol], 25 g/dL [15.5 mmol/L] hemoglobin or 2.90 g/dL [1.80 mmol/L] HbA1c will be reported as “Above Assay Range” and should be repeated on dilution. If the message persists on the diluted sample, report the result as “greater than 14.0% [130 mmol/mol].”
Manual Dilution: Mix one part of clinical laboratory reagent water (CLRW) and one part of well mixed whole blood. Re-assay the dilution mixture to obtain results within the analytical measurement range.
Important
The resulting readout (%HbA1c [mmol/mol]) is the reportable result. The result must not be corrected for dilution as it is a calculated result based on the ratio between HbA1c and Hb. Therefore, a dilution factor must not be used in the Dimension® Hemoglobin A1C assay.
Autodilution (AD): Not available for this method.
Samples with results less than 3.8% [18 mmol/mol], hemoglobin less than 5.0 g/dL [3.1 mmol/L] or HbA1c less than 0.25 g/dL [0.16 mmol/L] will be reported as “Below Assay Range” by the instrument. Dispense a new 200 μL aliquot of whole blood and re-assay the sample. If the message persists, contact your local support provider for assistance.
The instrument reporting system contains flags and comments to provide the user with information regarding instrument processing errors, instrument status information and potential errors in A1C results. Refer to your Dimension® Operator’s Guide for the meaning of report flags and comments.
A system malfunction may exist if the following 5-test precision† is observed:
A1c Concentration % [mmol/mol]
SD % [mmol/mol]
5.5 [37] >0.2 [1.6]9.6 [81] >0.3 [4.3]
† Sample cup must be filled with 200 µL for the 5-test precision study.
Limitations of Procedure
WARNINGThe Dimension® Hemoglobin A1C assay has significant interference with fetal hemoglobin (HbF). Samples containing HbF may produce a negative bias (lower than actual results) with the Dimension® Hemoglobin A1C assay. Hemoglobin A1c results are invalid for patients with abnormal amounts of HbF, including those with known Hereditary Persistence of Fetal Hemoglobin. For additional information on the interference of the HbF variant, refer to Interfering Substances.
Do not use the Dimension® Hemoglobin A1C calibrators to test precision.
As with any other laboratory procedure, a large discrepancy between the clinical impression and test results usually warrants investigation. Some of the following test limitations should be considered:
The Dimension® Hemoglobin A1C assay is designed only for accurate and precise measurement of mmol/mol HbA1c (IFCC) and %HbA1c (DCCT/NGSP). The individual results for total Hb and HbA1c concentration are not reported.
Patients with hemoglobin concentrations outside of the acceptable range for the Dimension® Hemoglobin A1C assay should be assayed by a test employing a different assay principle.
The Dimension® Hemoglobin A1C assay should not be used to diagnose diabetes during pregnancy. Hemoglobin A1c reflects the average blood glucose levels over the preceding 3 months (the average life span of a red blood cell) and therefore may be falsely low during pregnancy or any other condition associated with recent onset of hyperglycemia and/or decreased red blood cell survival.
The Dimension® Hemoglobin A1C assay should not be used to diagnose or monitor diabetes in patients with the following conditions: hemoglobinopathies except as demonstrated to produce acceptable performance (such as, sickle cell trait), abnormal red blood cell turnover (such as, anemias from hemolysis and iron deficiency), malignancies, and severe chronic hepatic and renal disease.
In cases of rapidly evolving Type 1 diabetes, the increase of HbA1c values might be delayed compared to the acute increase in glucose concentrations. In these conditions, diabetes mellitus must be diagnosed based on plasma glucose concentrations and/or the typical clinical symptoms.
This test should not replace glucose testing for patients with Type 1 diabetes, pediatric patients or pregnant women.
Any cause of shortened red blood cell survival (for example, hemolytic anemia or other hemolytic diseases, pregnancy, or recent significant blood loss) will reduce the exposure of red blood cells to glucose with a consequent decrease in HbA1c values. Results of HbA1c are not reliable in patients with chronic blood loss and consequent variable erythrocyte lifespan.12–15
Expected Values:
The reference range for HbA1c is indicated in the table below.16
Hemoglobin A1c values in healthy individuals may vary across reference populations. Each laboratory should check the validity of the reference interval and establish, if necessary, its own reference interval.
The frequency of HbA1c testing should depend on the clinical situation, the treatment regimen, and the clinician’s judgment. The American Diabetes Association recommends a reasonable HbA1c goal for many nonpregnant adults is <7%. Less stringent HbA1c goals may be appropriate for some patients with diabetes and other risk factors, such as severe hypoglycemia or extensive comorbid conditions.17
Interfering Substances
Various substances other than sugars can form aggregates with hemoglobin and potentially interfere with the assay causing false results. Examples include individuals with opiate addiction,18 lead poisoning and alcoholism.12
The antibody reagent used in the Dimension® Hemoglobin A1C assay will measure any glycosylated hemoglobin variants that are glycated at the beta-chain N-terminus and have epitopes identical to that of HbA1c (amino acid sequence: VAL-HIS-LEU-THR). This includes HbS, HbC, HbD, and HbE. Other hemoglobinopathies may give incorrect results with this test. Care must be taken when interpreting any HbA1c result from patients with Hb variants. Abnormal hemoglobins might affect the half-life of the red cells or the in vivo glycation rates. In these cases, even analytically correct results do not reflect the same level of glycemic control that would be expected in patients with normal hemoglobin.14
Glycated HbF (Fetal Hemoglobin), consisting of two alpha and two gamma chains, is not recognized by the anti-HbA1c antibody. Individuals with elevated levels of HbF (>10%), most commonly found in infants and in patients with beta thalassemia, may produce lower than expected results with this assay. These samples must be assayed by an alternate method.
No cross-reaction was found for the anti-HbA1c antibodies used in this kit with HbA0, HbA1a, HbA1b, acetylated hemoglobin, carbamylated hemoglobin, and labile HbA1c.
Specific Performance Characteristics
The following data represent typical performance for the Dimension® system. Actual results obtained by individual laboratories may differ depending on the study design.
PrecisionPrecision testing was performed in accordance with CLSI document EP05-A3.19 Testing was performed over 20 testing days using 3 instruments and 3 reagent lots on each instrument. Each testing day, 2 runs were performed (with a minimum of 2 hours in between).
Method ComparisonMethod Comparison testing was performed in accordance with CLSI document EP09-A3.20 The results of the Dimension® Hemoglobin A1C assay (y) were compared with the results generated using a NGSP standardized test method (HPLC) (x).
Passing-Bablok Regression
Units N Sample Range Slope 95% Cl y-intercept 95% Cl%HbA1c 147 4.5–13.2 0.983 0.966–1.001 0.030 -0.095–0.144mmol/mol 147 26–121 0.973 0.955–0.992 0.437 -0.474–1.450
The method comparison data was evaluated using Bland-Altman analysis of bias,21 which is the approach employed by the NGSP. The mean difference between A1C and the NGSP network method (HPLC) and the 95% confidence intervals of the differences in the range of 4–10% HbA1c are provided. 95% of the differences between the values obtained for individual samples with both methods fall within the range defined by the lower and upper 95% confidence intervals of the differences.
95% ConfidenceIntervals
Lower UpperComparative Method Mean Difference Sample Range N
NGSP (HPLC) -0.10 -0.37 0.17 4.5–10.0% 132
IFCC (HPLC) -1.0 -4.0 1.9 26–86 mmol/mol 132
Anticoagulant ComparisonEquivalence testing for 5 anticoagulants was performed in accordance with CLSI document EP09-A3.20 Testing was performed using one lot of reagents and a single replicate from a matched set of each of 4 anticoagulants (K3 EDTA; sodium fluoride/Na2 EDTA; lithium heparin, and Na Fluoride/K-Oxalate) and K2 EDTA samples.
Na Fluoride/K-Oxalate K2 EDTA 1.007 0.989–1.025 -0.032 -1.22–1.16
Number of Samples (N) = 79Sample Range (mmol/mol) = 28–125
Siemens Healthcare Diagnostics Inc.500 GBC DriveNewark, DE 19714 USA
2019
-10
C P
N 11
2752
89 -
US
Specificity
Non-Interfering Substances
Interference testing was performed in accordance with CLSI document EP07-A2.22
The following substances do not interfere with the Dimension® Hemoglobin A1C assay when present in whole blood at the concentrations indicated. Inaccuracies (biases) due to these substances are less than or equal to 5% at Hemoglobin A1c concentrations of 6.5% ± 1.0% and 8.0% ± 1.0% (less than or equal to 8% at 48 mmol/mol ± 11 mmol/mol and 64 mmol/mol ± 11 mmol/mol).
Interferent Interferent Concentration Common Units
Hemoglobin VariantsInterference testing to determine the effect of hemoglobin variants on the Dimension® Hemoglobin A1C assay was performed in accordance with CLSI document EP07-A2.22 No significant interference bias was observed for HbC, HbD, HbE, HbS, and HbA2. Significant interference bias was observed for HbF.
NGSP
Relative % Bias(Range % Bias)
Relative % Bias(Range % Bias)
Hb Variant N Range (%Variant)
Range (%HbA1c) ~6% HbA1c ~9% HbA1c
HbC 37 26.1–40.0 4.4–15.7 -1.0% (-5.0–4.9%)
-0.9% (-4.6–4.4%)
HbD 20 24.8–38.4 5.0–13.0 -2.2% (-4.9–4.4%)
-2.5% (-4.4– -1.3%)
HbE 22 19.7–30.4 4.7–11.0 -2.1% (-4.9–3.1%)
-2.5% (-4.3– -1.0%)
HbS 22 27.5–36.3 5.3–14.0 -1.3% (-4.7–4.9%)
-2.0% (-4.9–3.5%)
HbA2 23 4.3–6.2 5.1–8.4 0.1% (-4.8–3.6%)
-2.0% (-3.0– -1.1%)
HbF 20 4.3–29.3 4.3–10.1 -23.2% (-30.3–1.2%)
-24.7% (-25.8– -23.3%)
IFCC
Relative % Bias(Range % Bias)
Relative % Bias(Range % Bias)
Hb Variant N Range (%Variant)
Range (mmol/mol
HbA1c)~42 mmol/mol ~75 mmol/mol
HbC 37 26.1–40.0 25–148 -1.4% (-8.2–8.2%)
-1.2% (-5.7–6.2%)
HbD 20 24.8–38.4 31–119 -3.5% (-8.1–7.1%)
-3.4% (-5.2– -1.8%)
HbE 22 19.7–30.4 28–97 -3.4% (-8.2–5.2%)
-3.3% (-6.2– -1.3%)
HbS 22 27.5–36.3 34–130 -2.0% (-7.6–7.6%)
-2.6% (-6.3–4.1%)
HbA2 23 4.3–6.2 32–68 0.2% (-8.3–6.1%)
-2.7% (-4.1– -1.6%)
HbF 20 4.3–29.3 23–87 -37.0% (-48.6–2.0%)
-32.7% (-36.3– -30.8%)
Hemoglobin DerivativesInterference testing to determine the effect of hemoglobin derivatives, including acetylated hemoglobin, carbamylated hemoglobin, labile hemoglobin, and hemoglobin fractions on the Dimension® Hemoglobin A1C assay was performed in accordance with CLSI document EP07-A2.22 Inaccuracies (biases) due to these substances are less than or equal to 5% at Hemoglobin A1c concentrations of 5.0% ± 1.0% , 6.5% ± 1.0%, and 8.0% ± 1.0% (less than or equal to 9% at 31 mmol/mol ± 11 mmol/mol, 48 mmol/mol ± 11 mmol/mol and 64 mmol/mol ± 11 mmol/mol). • Acetylated Hemoglobin with greater than or equal to 50 mg/dL (2.8 mmol/L) of acetylsalicylic acid • Carbamylated Hemoglobin with greater than or equal to 10 mmol/L of Cyanate • Labile Hemoglobin with greater than or equal to 1500 mg/dL (83.3 mmol/L) of Glucose
Limit of Detection and Limit of Blank
The Limit of Detection (LoD) and Limit of Blank (LoB) were determined in accordance with CLSI document EP17-A2.23
The LoB is the highest measurement result that is likely to be observed on a blank sample. The LoB was determined using 60 determinations with 5 blank samples each for tHb and 75 determinations with 5 blank samples each for %HbA1c/HbA1c.
The LoD corresponds to the lowest concentration of HbA1c or tHb that can be detected with a probability of 95%. The LoD was determined using 60 determinations, with 5 low level samples each for tHb and 75 determinations with 5 low samples each for %HbA1c/HbA1c.
The LoB and LoD for the Dimension® Hemoglobin A1C assay are shown below.
Siehe schraffierte Abschnitte: Aktualisierte Informationen gegenüber der Version 2019-04. Ausgabedatum 2019-10
Dimension® clinical chemistry system
A1CFlex® reagent cartridge
DF105B
Hämoglobin A1C-TestVerwendungszweck: Der Dimension® Hämoglobin A1C-Test ist ein In‑vitro-Diagnostikum zur quantitativen Bestimmung von %HbA1c (DCCT/NGSP) bzw. mmol/mol HbA1c (IFCC) im antikoagulierten menschlichen venösen Vollblut zur Verwendung auf dem klinisch-chemischen System Dimension®. Die Hämoglobin A1c-Messung unterstützt die Diagnose und Überwachung der Langzeit-Blutglukosekontrolle bei Patienten mit Diabetes mellitus und hilft bei der Erkennung von Patienten, die dem Risiko unterliegen, an Diabetes mellitus zu erkranken.
Zusammenfassung: HbA1c bezieht sich auf das Produkt einer nichtenzymatischen Reaktion zwischen Glukose und Hämoglobin A1. Menschliche Erythrozyten sind voll durchlässig für Glukose, die sich mit Hämoglobin nichtenzymatisch zu HbA1c verbinden kann. Bei dieser nichtenzymatischen Reaktion zwischen der Alpha-Aminogruppe des N-terminalen Valins der Hämoglobin-Beta-Kette und der Glukose wird ein instabiles Aldimin- oder Schiff-Basen-Zwischenprodukt (labile Fraktion) gebildet. Die Reaktion ist langsam und reversibel. Die Reaktionsgeschwindigkeit ist proportional zur Glukosekonzentration im Blut. Anschließend wird das Aldimin-Zwischenprodukt in einer irreversiblen Amadori-Umlagerung zu dem stabilen Ketoamin 1-Glukofrutovalin umgewandelt. Da die Reaktionsgeschwindigkeit von der Konzentration der Reaktionspartner abhängt, ist der Grad der Glykierung (gemessen als HbA1c relativ zum Gesamt-Hämoglobin) proportional zur durchschnittlichen Konzentration von Glukose im Blut während der Lebensdauer von Hämoglobin im roten Blutkörperchen (ungefähr 120 Tage).1,2
Der Nutzen von HbA1c-Messungen wurde in der DCCT-Studie (Diabetes Control and Complications Trial) belegt.3 Ein wichtiges Ergebnis dieser Studie war die direkte Korrelation zwischen der Blutzuckereinstellung bei den Patienten und dem Risiko von Langzeitkomplikationen. Patienten mit besserer Blutzuckereinstellung (d. h. niedrigerem HbA1c) wiesen wesentlich bessere Prognosen hinsichtlich mikrovaskulärer Komplikationen wie Neuropathien, Retinopathien und Nephropathien auf.3
Grundlagen des Verfahrens: Mit dem Dimension® Hämoglobin A1C-Test wird sowohl der HbA1c- als auch der Gesamt-Hämoglobinwert gemessen. Die HbA1c-Messung basiert auf dem Prinzip eines turbidimetrischen Hemmungs-Immunoassays (TINIA), und die Messung des Gesamt-Hämoglobins basiert auf einer Modifikation der alkalischen Hämatin-Reaktion. Aus den für diese beiden Analyten gemessenen Werten wird der relative Anteil glykierten Hämoglobins am Gesamt-Hämoglobin berechnet und angegeben. Eine Vorbehandlung zur Entfernung der labilen Fraktion ist nicht notwendig, da nur die umgebildete Form von HbA1c nach der Amadori-Umlagerung gemessen wird. Bei diesem Assay werden alle Hämoglobinvarianten, die an der N-terminalen Gruppe der Betakette glykiert sind und identische Epitope haben wie HbA1c, gemessen.
Messung des Gesamt-Hämoglobins: Eine Vollblutprobe wird in die erste Küvette gegeben, die ein lysierendes Reagenz enthält. Dieses Reagenz löst die roten Blutkörperchen auf und wandelt gleichzeitig das freigesetzte Hämoglobin in ein Derivat mit einem charakteristischen Absorptionsspektrum um. Ein Aliquot des lysierten Vollbluts wird aus der ersten Küvette in eine zweite Küvette übertragen, wo das Gesamt-Hämoglobin bei 405 nm und 700 nm gemessen wird.4
Messung des Hämoglobins A1c: Dasselbe Aliquot des lysierten Vollbluts, das zur Messung des Hb aus der ersten Küvette in die zweite Küvette übertragen wurde, wird auch für die Messung des HbA1c verwendet. Die zweite Küvette enthält einen Anti-HbA1c-Antikörper in einem gepufferten Reagenz. Das Hämoglobin A1c in der Probe reagiert mit dem Anti-HbA1c-Antikörper zu einem löslichen Antigen-Antikörper-Komplex. Dann wird ein Polyhapten-Reagenz mit mehreren HbA1c-Epitopen in die Küvette gegeben. Das Polyhapten reagiert mit überschüssigen (freien) Anti-HbA1c-Antikörpern zu einem unlöslichen Antikörper-Polyhapten-Komplex. Die Geschwindigkeit dieser Reaktion wird durch Trübungsmessung bei 340 nm und Leerwertermittlung bei 700 nm ermittelt und ist umgekehrt proportional zur Konzentration von HbA1c in der Probe.
Anti-HbA1c-Antikörper (überschüssig) + Polyhapten Ak/Polyhapten-Komplex(wird bei 340 nm absorbiert)
Komponenten des A1C-Kits
Hinweis: Jedes Set enthält zusammengehörige A1C Flex®-Reagenzkassetten und -Kalibratoren. Diese Komponenten dürfen nicht zusammen mit Komponenten aus Kits mit anderen Chargennummern verwendet werden.
Reagenzien
Zellena Form Inhaltsstoff Konzentrationb Ursprung1–2 Flüssig Antikörper ≥ 0,5 mg/mlc Schaf, polyklonal vom Schafserum
a. Die Zellen sind vom breiten Ende der Kassette aus durchgehend nummeriert.b. Nominalwert pro Zelle in einer Kassette.c. Der Antikörpertiter und die Konjugataktivität (oder die Partikelreagenzkonzentration) können von Charge zu
Charge schwanken.d. MES = 2-Morpholinoethan-Sulfonsäuree. TRIS = Tris(Hydroxymethyl-)Aminomethanf. TTAB = Tetradecyl-Trimethyl-Ammoniumbromid
Gefahrenhinweise und Sicherheitssätze:H412P273, P501
Warnung!Schädlich für Wasserorganismen, mit langfristiger Wirkung.
Freisetzung in die Umwelt vermeiden. Inhalt und Behälter sind in Übereinstimmung mit den gesetzlichen Bestimmungen zu entsorgen
Enthält: 2-Methyl-H4-isothiazol-3-on
Sicherheitsdatenblätter (MSDS/SDS) verfügbar auf siemens.com/healthcare
Vorsichtsmaßnahmen: Gebrauchte Küvetten enthalten menschliche Körperflüssigkeiten; mit entsprechender Vorsicht handhaben und Hautkontakt oder Verschlucken vermeiden.
Vorsicht: Das Bundesrecht der USA erlaubt den Verkauf dieses Medizinprodukts nur durch oder auf Anordnung einer staatlich anerkannten Fachkraft im Gesundheitswesen.
In‑vitro-Diagnostikum
Hinweis: Die A1C Flex®-Reagenzien und -Kalibratoren werden in einem Kit ausgeliefert. Jedes Kit enthält zusammengehörige A1C Flex®-Reagenzkassetten und A1C-Kalibratoren. Reagenzien mit unterschiedlichen Chargennummern dürfen nicht untereinander ausgetauscht werden.
Reagenzvorbereitung: Alle Reagenzien sind flüssig und gebrauchsfertig.
Aufbewahrung bei: 2–8°C
Verfalldatum: Verfalldatum des Kits siehe Umkarton. Alle Komponenten des Kits sind bis zum Verfalldatum bei ungeöffneter Lagerung bei 2–8°C stabil. Verschlossene Kassettenzellen sind im Gerät 30 Tage lang stabil.
Stabilität geöffneter Zellen: 5 Tage für Zellen 1–2 sowie 5–6 10 Tage für Zelle 3
Probenentnahme und -handhabung: Empfohlener Probentyp: Antikoaguliertes venöses Vollblut (K2 EDTA; K3 EDTA; Natriumfluorid/Na2 EDTA; Lithiumheparin oder Na-Fluorid/K-Oxalat).
Die Proben sollten mit empfohlenen Verfahren zur Entnahme diagnostischer Blutproben durch Venenpunktion gewonnen werden.5–7 Beachten Sie die Anweisungen zur Verwendung der Probenentnahmevorrichtung und zur Probenverarbeitung.6
• Proben für die A1C-Methode können nur aus einem Proben-Cup oder SSC getestet werden. • Die Proben können nicht direkt aus Primärröhrchen getestet werden. • Vor dem Pipettieren in das Proben-Cup oder SSC sollten die Proben durch Inversion (Röhrchen vorsichtig
zehnmal umdrehen) oder mit einem Rollenmischer vorsichtig gemischt werden, um eine gleichmäßige Verteilung der Erythrozyten vor dem Test zu erzielen. Schaumbildung vermeiden.
• Keine Proben mit Gerinnseln verwenden.• 200 µl der Vollblutprobe in das Proben-Cup oder SSC pipettieren.• Die Probe darf im Proben-Cup bis zu 1 Stunde lang im Gerät verbleiben.
Probenstabilität: Die Proben bleiben über den nachfolgenden Zeitraum stabil, wenn sie wie folgt gelagert werden:8
3 Tage bei 15–25°C 7 Tage bei 2–8°C 4 Monate bei -20°C (nur einmal einfrieren)
Die Hinweise über die Aufbewahrung dieser Proben sind allgemeine Empfehlungen. Anwender können Verfahren zur Aufbewahrung von Patientenproben auch selbst validieren.
Verfahren
Mitgelieferte MaterialienA1C-Kit, Art.- Nr. DF105B: Enthält A1C Flex®-Reagenzkassetten und A1C-Kalibrator (5 Level)
Erforderliche, aber nicht mitgelieferte MaterialienQualitätskontrollmaterialien
Testschritte
Probenentnahme,g Reagenzzugabe, Mischung und Bearbeitung werden vom klinisch-chemischen Analysensystem Dimension® automatisch durchgeführt. Weitere Informationen entnehmen Sie bitte dem Dimension®-Bedienungshandbuch.
g. Das Probengefäß muss 200 µl Vollblut enthalten, damit die Nachmischung ordnungsgemäß ausgeführt wird.
405 und 700 nm für HämoglobinMessverfahren Turbidimetrisch für Hämoglobin A1c
Kolorimetrisch für Hämoglobin
KalibrationDas allgemeine Kalibrationsverfahren wird im Dimension®-Bedienungshandbuch beschrieben.
Hinweis: Die A1C Flex®-Reagenzien und -Kalibratoren werden in einem Kit ausgeliefert. Jedes Kit enthält zusammengehörige A1C Flex®-Reagenzkassetten und A1C-Kalibratoren. Reagenzien mit unterschiedlichen Chargennummern dürfen nicht untereinander ausgetauscht werden.
Das System führt die Kalibrierung für Hb und HbA1c automatisch durch.
Für den Dimension® Hämoglobin A1C-Test müssen vor der Kalibration chargenspezifische Skaler-Werte in den Bildschirm Calibration Set Up (Kalibrations-Programm) eingegeben werden. Die Skaler-Werte sind auf der Verpackung der Flex®-Reagenzkassette angegeben. Diese Faktoren werden auf alle QK- und Patientenergebnisse angewendet, um die Genauigkeit zu gewährleisten. Werden die chargenspezifischen Faktoren nicht eingegeben, kommt es zu ungenauen Ergebnissen.
Bei der A1C-Methode stehen zwei Optionen für die Kalibrierung und die Ergebnisberichterstellung zur Verfügung.
Option 1:
• Die Ergebnisse werden in %HbA1c nach der folgenden Gleichung zusammengestellt:
%HbA1c = 100 xHbA1c (g/dl)
Hb (g/dl)
• Die Kalibratorwerte (g/dl) sind für Hämoglobin A1c und Gesamt-Hämoglobin erforderlich. Diese Werte werden aus der Nominalwerttabelle in der Gebrauchsanweisung für den Dimension® Hämoglobin A1C-Kalibrator ermittelt.
• Dann berechnet das klinisch-chemische Analysensystem Dimension® ein NGSP-standardisiertes %HbA1c-Ergebnis auf Basis der nachstehenden Formel. Diese Berechnung liefert einen nach dem Ergebnis der DCCT-Studie standardisierten %HbA1c-Wert, der auf dem Befundblatt des Dimension®-Systems ausgedruckt wird. Die Werte der Polynomkoeffizienten (b, c und d) können je nach Flex®-Reagenzkassetten-Charge variieren.
NGSP-standardisiertes %HbA1c = (b x (%HbA1c)2) + (c x %HbA1c) + d
A1C-Chargen werden unter kontrollierten Bedingungen hergestellt, damit sie den festgelegten Produktspezifikationen entsprechen. Jedes Jahr wird auf jedem Dimension®-Modell eine Charge getestet, um die Standardisierung nach dem US-National Glycohemoglobin Standardization Program (NGSP) zu bestätigen. Exemplare der Zertifikate können unter www.siemens.com/diagnostics abgerufen werden. Weitere Informationen zur NGSP-Zertifizierung sind einsehbar unter www.ngsp.org.9
Option 2:
• Die Ergebnisse werden in der SI-Einheit [mmol/mol]h nach der folgenden Gleichung zusammengestellt:
mmol/mol HbA1c = 1000 xHbA1c (mmol/l)
Hb (mmol/l)
• Die Kalibratorwerte (mmol/l) sind für Hämoglobin A1c und Gesamt-Hämoglobin erforderlich. Diese Werte werden aus der Nominalwerttabelle in der Gebrauchsanweisung für den Dimension® Hämoglobin A1C-Kalibrator ermittelt.
• Dann berechnet das Dimension®-System ein IFCC-standardisiertes A1C-Ergebnis in mmol/mol auf Basis der nachstehenden Formel. Diese Berechnung liefert einen nach dem IFCC-Referenzsystem9 standardisierten HbA1c-Wert in mmol/mol, der auf dem Befundblatt des Dimension®-Systems ausgedruckt wird. Die Werte der Polynomkoeffizienten (b, c und d) können je nach Flex®-Reagenzkassetten-Charge variieren.
IFCC-standardisiertes HbA1c (mmol/mol) = (b x (HbA1c mmol/mol)2) + (c x HbA1c mmol/mol) + d
h. SI-Einheiten sind in Klammern angegeben.
Kalibrationsmaterial Sekundäre Kalibratoren wie A1C-KalibratorenKalibrierschema 2 Level, n=5 für Hbi
0,25–2,90 g/dl [0,16–1,80 mmol/l] HbA1cKalibrationshäufigkeit Alle 30 Tage mit derselben ChargeEine neue Kalibration ist erforderlich • Für jede neue Charge von Flex®-Reagenzkassetten
• Nach größeren Wartungs- oder Servicemaßnahmen, falls die Ergebnisse der Qualitätskontrolle dies nahelegen
• Nach Maßgabe der Qualitätskontrollverfahren des Labors• Nach Maßgabe behördlicher Vorschriften
Skaler-Werte Die chargenspezifischen Skaler-Werte befinden sich auf der Verpackung der Flex®-Reagenzkassette.
Die Kalibrator-Cups müssen mit 600 µl Kalibrator gefüllt werden.i. Die Kalibrationsergebnisse für HbA1c werden automatisch angezeigt. Die entsprechenden Kalibrationsergebnisse für
Hb finden Sie im Kalibrations-Report
Kalibrationsakzeptanzkriterien
Für den Dimension® Hämoglobin A1C-Test ist eine Bestätigung der zusätzlichen Kalibrierungsrichtlinien erforderlich. Stellen Sie nach abgeschlossener Kalibrierung sicher, dass die folgenden Kriterien erfüllt sind:
Eine Reflektion der Genauigkeit der Gesamthämoglobin-Milliabsorptionswerte, die zur Berechnung des Kalibrierungskoeffizienten „EX“ verwendet werden.
QualitätskontrolleHalten Sie die behördlichen Vorschriften oder Akkreditierungsanforderungen für die Häufigkeit von Qualitätskontrollen ein. In der Praxis sollten mindestens einmal täglich zwei Konzentrationsstufen eines Qualitätskontroll (QK-)materials mit bekannten Hämoglobin-A1c-Konzentrationen analysiert werden. Bei Ergebnissen außerhalb der akzeptablen Grenzwerte nach laborinternen QK-Vorschriften vorgehen.
Hinweis: Es ist wichtig, die lokalen oder regionalen Richtlinien zur diagnostischen Qualität zu berücksichtigen, wenn akzeptierbare Grenzwerte für die Qualitätskontrolle festgelegt werden (z. B. des College of American Pathologists (CAP), der Deutschen Gesellschaft für Klinische Chemie und Laboratoriumsmedizin (DGKL) usw).
Ergebnisse: Das Dimension®-System berechnet die Konzentration des Gesamt-A1c, Hb und des HbA1c nach dem Berechnungsschema, das im Dimension®-Bedienungshandbuch dargestellt ist.
Das System berichtet die Ergebnisse als einzelne Einheit (% oder mmol/mol); um die Berichtseinheit entweder mit der IFCC NGSP „Master-Gleichung“ oder der NGSP IFCC „Master-Gleichung“, die das Unterkomitee der International Federation for Clinical Chemistry für die Hämoglobin-A1c-Standardisierung empfiehlt,10,11 umzuwandeln, verwenden Sie die folgenden Gleichungen:
Resultate dieses Tests sollten stets in Verbindung mit der Vorgeschichte des Patienten, dem klinischen Bild und anderen Untersuchungsergebnissen interpretiert werden.
Die Hb- und HbA1c-Analytwerte können ohne vorherige Verdünnung oder Vorbehandlung, die nicht Teil des üblichen Analysevorgangs ist, in der Probe direkt ermittelt werden. Hb- und HbA1c-Analytwerte außerhalb der oben aufgeführten Bereiche lösen eine Befundblattmeldung aus, die mit dem berechneten HBA1c-Verhältnis aufgeführt wird.
Der Bereich der berechneten HBA1c-Verhältnisse wurde von Siemens mithilfe von nativen Vollblutproben validiert. Dieser Bereich kann ggf. zur laborinternen Validierung des Messbereichs verwendet werden.
Für Proben mit Ergebnissen über 14,0 % [130 mmol/mol], 25 g/dl [15,5 mmol/l] Hämoglobin bzw. 2,90 g/dl [1,80 mmol/l] HbA1c wird „Oberhalb des Testbereichs“ ausgegeben. Nach Verdünnung erneut analysieren. Wenn die Meldung auch für die verdünnte Probe angezeigt wird, das Ergebnis als „größer als 14,0 % [130 mmol/mol]“ angeben.
Manuelle Verdünnung: Mischen Sie einen Teil CLRW (Clinical Laboratory Reagent Water) und einen Teil gut gemischten Vollbluts. Wiederholen Sie den Test für die verdünnte Mischung, um Ergebnisse innerhalb des Messbereichs zu erhalten.
Wichtig
Das angegebene Messergebnis (%HbA1c [mmol/mol]) wird im Ergebnisausdruck angegeben. Das Ergebnis darf nicht für eine Verdünnung korrigiert werden, da es sich um ein berechnetes Ergebnis basierend auf dem Verhältnis zwischen HbA1c und Hb handelt. Daher darf für den Dimension® Hämoglobin A1C-Test kein Verdünnungsfaktor verwendet werden.
Automatische Verdünnung (AD): Für diesen Test nicht verfügbar.
Proben mit Ergebnissen unter 3,8 % [18 mmol/mol], Hämoglobin unter 5,0 g/dl [3,1 mmol/l] oder HbA1c unter 0,25 g/dl [0,16 mmol/l] werden vom System als „Unterhalb des Messbereichs“ gemeldet. Setzen Sie ein neues Aliquot von 200 µl Vollblut ein und wiederholen Sie den Test für die Probe. Bleibt die Nachricht bestehen, wenden Sie sich an den lokalen Support.
Das integrierte Meldesystem des Geräts informiert den Nutzer durch Codes und Hinweise über Bearbeitungsfehler des Geräts, den Gerätestatus und mögliche Fehler bei den Ergebnissen der A1C-Tests. Informationen zur Bedeutung der Fehlercodes und Hinweise finden Sie im Dimension®-Bedienungshandbuch.
Treten die im Folgenden aufgeführten Präzisionswerte bei 5-fach-Bestimmung† auf, kann eine Fehlfunktion des Systems vorliegen:
A1c-Konzentration % [mmol/mol]
SA % [mmol/mol]
5,5 [37] > 0,2 [1,6]9,6 [81] > 0,3 [4,3]
† Für die Präzisionsstudie über 5 Tests muss das Proben-Cup mit 200 µl gefüllt werden.
Grenzen des Verfahrens
VORSICHTDer Dimension® Hämoglobin A1C-Test weist signifikante Interferenzen mit fetalem Hämoglobin (HbF) auf. Problen mit HbF können bei dem Dimension® Hämoglobin A1C-Test eine negative Abweichung (geringer als die tatsächlichen Ergebnisse) ergeben. Die Hämoglobin A1c-Ergebnisse sind für Patienten mit abnormalen HbF-Werten nicht gültig, einschließlich Patienten mit bekannter hereditärer Persistenz des fetalen Hämoglobins. Weitere Informationen zur Interferenz der HbF-Variante finden Sie unter „Störsubstanzen“.
Verwenden Sie die Dimension® Hämoglobin A1C-Kalibratoren nicht für Präzisionstests.
Wie bei allen Laborverfahren sollten bei großen Diskrepanzen zwischen klinischem Erscheinungsbild und Testergebnissen weitere Untersuchungen erfolgen. Dabei sollten folgende Grenzen des Verfahrens berücksichtigt werden:
Der Dimension® Hämoglobin A1C-Test ist nur auf die präzise Messung des HbA1c mmol/mol-Wertes (IFCC) und des %HbA1c-Wertes (DCCT/NGSP) ausgelegt. Die einzelnen Ergebnisse für die Gesamt-Hb- und HbA1c-Konzentration werden nicht berichtet.
Patienten, deren Hämoglobinkonzentration sich außerhalb des akzeptablen Bereichs für den Dimension® Hämoglobin A1C-Test befindet, sollten mit einem Test untersucht werden, der ein anderes Testprinzip nutzt.
Daher darf der Dimension® Hämoglobin A1C-Test nicht zur Diabetesdiagnose während der Schwangerschaft verwendet werden. Hämoglobin A1c spiegelt die durchschnittlichen Blutglukosewerte über die letzten 3 Monate wieder (die durchschnittliche Lebensdauer eines roten Blutkörperchens) und kann daher während der Schwangerschaft oder Erkrankungen, bei denen eine kurzfristige einsetzende Hyperglykämie und/oder eingeschränkte Überlebensfähigkeit der roten Blutkörperchen auftritt, falsch niedrig sein.
Der Dimension® Hämoglobin A1C-Test sollte nicht zur Diagnose oder Überwachung von Diabetes bei Patienten mit folgenden Erkrankungen genutzt werden: Hämoglobinstörungen, wenn hierbei keine akzeptable Leistung belegt ist (wie z. B. Auftreten von Sichelzellen im Blut), abnormale Erneuerung der roten Blutkörperchen (wie z. B. bei Anämien aufgrund von Hämolyse und Eisenmangel), Malignitäten sowie schwere chronische Leber- und Nierenerkrankungen.
Bei einem sich schnell entwickelnden Diabetes Typ 1 kann der Anstieg der HbA1c-Werte im Vergleich zum akuten Anstieg der Glukosekonzentrationen verzögert ablaufen. Unter diesen Umständen muss ein Diabetes mellitus auf Grundlage der Plasmaglukose-Konzentrationen und/oder den typischen klinischen Symptomen diagnostiziert werden.
Dieser Test dient nicht als Ersatz für Glukosetests bei Patienten mit Diabetes Typ 1, pädiatrischen Patienten oder schwangeren Frauen.
Ein durch hämolytische Anämie, andere hämolytische Erkrankungen, Schwangerschaft oder kürzlich erfolgten erheblichen Blutverlust oder sonstige Ursachen bedingtes eingeschränktes Überleben der roten Blutkörperchen führt zu einer geringeren Glukoseexposition der roten Blutkörperchen und dadurch bedingt zu niedrigeren HbA1c-Werten. Die HbA1c-Ergebnisse sind bei Patienten mit chronischem Blutverlust und der dadurch bedingten schwankenden Lebensdauer der Erythrozyten nicht zuverlässig.12–15
Erwartete Werte:
Der Referenzbereich für HbA1c ist in der folgenden Tabelle angegeben.16
Die Hämoglobin-A1c-Werte bei gesunden Personen können zwischen Referenzpopulationen schwanken. Jedes Labor sollte die Gültigkeit des Referenzbereichs überprüfen und, wenn nötig, einen eigenen Referenzbereich aufstellen.
Die Frequenz von HbA1c-Tests sollte je nach klinischer Situation, Behandlungsplan und Ermessen des Arztes festgelegt werden. Die American Diabetes Association empfiehlt als angemessenes HbA1c-Ziel für viele nicht schwangere Frauen < 7 %. Für Patienten mit Diabetes und anderen Risikofaktoren wie schwerer Hypoglykämie oder umfangreichen Begleiterkrankungen können weniger strikte HbA1c-Ziele angemessen sein.17
Störsubstanzen
Außer Zuckern können sich auch verschiedene andere Substanzen an Hämoglobin anlagern und so möglicherweise durch Störungen des Tests zu falschen Ergebnissen führen. Beispiele sind Patienten mit Opiatabhängigkeit,18 Bleivergiftung und Alkoholismus.12
Das Antikörper-Reagenz, das bei dem Dimension® Hämoglobin A1C-Test zum Einsatz kommt, misst alle glykierten Hämoglobinvarianten, die an der N-terminalen Gruppe der Betakette glykiert sind und identische Epitope haben wie HbA1c (Aminosäuresequenz: VAL-HIS-LEU-THR). Hierzu gehören HbS, HbC, HbD und HbE. Andere Hämoglobinstörungen könnten bei diesem Test zu fehlerhaften Ergebnissen führen. Die Interpretation der HbA1c-Ergebnisse von Patienten mit Hb-Varianten muss mit besonderer Sorgfalt erfolgen. Abnormale Hämoglobine können die Halbwertszeit der roten Blutkörperchen oder die In‑vivo-Glykierungsraten beeinträchtigen. In diesen Fällen zeigen selbst analytisch fehlerfreie Ergebnisse nicht den Grad der Blutzuckereinstellung, der bei Patienten mit normalem Hämoglobin zu erwarten wäre.14
Glykiertes HbF (Fötales Hämoglobin) besteht aus zwei Alpha- und zwei Gammaketten und wird vom Anti-HbA1c-Antikörper nicht erkannt. Bei Personen mit erhöhten HbF-Werten (> 10 %), meist Säuglinge und Patienten mit Beta-Thalassämie, sind die Ergebnisse aus diesem Assay unter Umständen niedriger als erwartet. Solche Proben müssen mit einer alternativen Methode analysiert werden.
Für die in diesem Kit verwendeten Anti-HbA1c-Antikörper wurde keine Kreuzreaktion mit HbA0, HbA1a, HbA1b, acetyliertem Hämoglobin, carbamyliertem Hämoglobin und labilem HbA1c festgestellt.
Spezifische Leistungsdaten
Die folgenden Daten stellen die typische Leistung für das Dimension®-System dar. Die tatsächlichen Ergebnisse der jeweiligen Laboratorien können je nach Studiendesign hiervon abweichen.
PräzisionPräzisionstests wurden gemäß CLSI-Dokument EP05-A3 durchgeführt.19 Die Tests wurden über 20 Testtage anhand von 3 Instrumenten und 3 Reagenzchargen pro Instrument vorgenommen. An jedem Testtag wurden 2 Läufe durchgeführt (mit mindestens 2 Stunden Abstand).
MethodenvergleichMethodenvergleichstests wurden gemäß CLSI-Richtlinie EP09-A3 durchgeführt.20 Die Ergebnisse des Dimension® Hämoglobin A1C-Tests (y) wurden mit den Ergebnissen verglichen, die anhand einer NGSP-standardisierten Testmethode (HPLC) (x) ermittelt wurden.
Passing-Bablok-Regression
Einheiten N Proben bereich Steigung 95 % KI Y-Achsab schnitt 95 % KI%HbA1c 147 4,5–13,2 0,983 0,966–1,001 0,030 -0,095–0,144mmol/mol 147 26–121 0,973 0,955–0,992 0,437 -0,474–1,450
Die Methodenvergleichsdaten wurden anhand der Bland-Altman-Abweichungsanalyse ausgewertet,21 also gemäß dem NGSP-Verfahren. Es werden die mittlere Differenz zwischen A1C und der NGSP-Netzwerkmethode (HPLC) sowie die 95 %-Konfidenzintervalle der Differenzen im Bereich von 4–10 % HbA1c angegeben. 95 % der Differenzen zwischen den Werten, die für einzelne Proben mit beiden Methoden ermittelt wurden, fallen in den Bereich, der durch das untere und obere 95 %-Konfidenzintervall der Differenzen definiert ist.
Siemens Healthcare Diagnostics Inc.500 GBC DriveNewark, DE 19714 USA
2019
-10
C P
N 11
2752
89 -
DE
Antikoagulanzien-VergleichÄquivalenztests mit 5 Gerinnungshemmern wurden gemäß CLSI-Richtlinie EP09-A3 durchgeführt.20 Die Tests wurden anhand einer Reagenziencharge und einem einzelnen Replikat eines abgestimmten Satzes mit je 4 Gerinnungshemmern (K3 EDTA; Natriumfluorid/Na2 EDTA; Lithiumheparin und Na-Fluorid/K-Oxalat) und K2 EDTA-Proben durchgeführt.
Passing-Bablok-Regression: NGSP (%)
Gerinnungs hemmer Vergleichs probe (x) Steigung 95 % KI Y-Achsab schnitt 95 % KI
Interferenztests wurden gemäß CLSI-Dokument EP07-A2 durchgeführt.22
Die folgenden Substanzen haben keinen Einfluss auf den Dimension® Hämoglobin A1C-Test, wenn sie in den genannten Konzentrationen im Vollblut enthalten sind. Abweichungen aufgrund dieser Substanzen belaufen sich bei Hämoglobin A1c-Konzentrationen von 6,5 % ± 1,0 % und 8,0 % ± 1,0 % auf höchstens 5 % (weniger oder gleich 8 % bei 48 mmol/mol ± 11 mmol/mol und 64 mmol/mol ± 11 mmol/mol).
Störsubstanz Konzentration der Störsubstanz Gängige Einheiten
HämoglobinvariantenInterferenztests zur Ermittlung der Auswirkungen von Hämoglobinvarianten auf den Dimension® Hämoglobin A1C-Test wurden gemäß CLSI-Richtlinie EP07-A2 durchgeführt.22 Bei HbC, HbD, HbE und HbA2 zeigte sich keine signifikante Interferenzabweichung. Bei HbF zeigte sich eine signifikante Interferenzabweichung.
NGSP
Relative Abweichung in %(Bereich der Abweichung in %)
Relative Abweichung in %(Bereich der Abweichung in %)
Hb-Variante N Bereich (% Variante)
Bereich (%HbA1c) ~6 % HbA1c ~9 % HbA1c
HbC 37 26,1–40,0 4,4–15,7 -1,0 % (-5,0–4,9 %)
-0,9 % (-4,6–4,4 %)
HbD 20 24,8–38,4 5,0–13,0 -2,2 % (-4,9–4,4 %)
-2,5 % (-4,4– -1,3 %)
HbE 22 19,7–30,4 4,7–11,0 -2,1 % (-4,9–3,1 %)
-2,5 % (-4,3– -1,0 %)
HbS 22 27,5–36,3 5,3–14,0 -1,3 % (-4,7–4,9 %)
-2,0 % (-4,9–3,5 %)
HbA2 23 4,3–6,2 5,1–8,4 0,1 % (-4,8–3,6 %)
-2,0 % (-3,0– -1,1 %)
HbF 20 4,3–29,3 4,3–10,1 -23,2 % (-30,3–1,2 %)
-24,7 % (-25,8– -23,3 %)
IFCC
Relative Abweichung in %(Bereich der Abweichung in %)
Relative Abweichung in %(Bereich der Abweichung in %)
Hb-Variante N Bereich (% Variante)
Bereich (mmol/mol
HbA1c)~42 mmol/mol ~75 mmol/mol
HbC 37 26,1–40,0 25–148 -1,4 % (-8,2–8,2 %)
-1,2 % (-5,7–6,2 %)
HbD 20 24,8–38,4 31–119 -3,5 % (-8,1–7,1 %)
-3,4 % (-5,2– -1,8 %)
HbE 22 19,7–30,4 28–97 -3,4 % (-8,2–5,2 %)
-3,3 % (-6,2– -1,3 %)
HbS 22 27,5–36,3 34–130 -2,0 % (-7,6–7,6 %)
-2,6 % (-6,3–4,1 %)
HbA2 23 4,3–6,2 32–68 0,2 % (-8,3–6,1 %)
-2,7 % (-4,1– -1,6 %)
HbF 20 4,3–29,3 23–87 -37,0 % (-48,6–2,0 %)
-32,7 % (-36,3– -30,8 %)
HämoglobinderivateInterferenztest zur Ermittlung der Auswirkungen von Hämoglobinderivaten, darunter acetyliertem Hämoglobin, carbamyliertem Hämoglobin, labilem Hämoglobin und Hämoglobinfraktionen auf den Dimension® Hämoglobin A1C-Test wurden gemäß CLSI-Richtlinie EP07-A2 durchgeführt.22 Abweichungen aufgrund dieser Substanzen belaufen sich bei Hämoglobin A1c-Konzentrationen von 5,0 % ± 1,0 %, 6,5 % ± 1,0 % und 8,0 % ± 1,0 % auf höchstens 5 % (weniger oder gleich 9 % bei 31 mmol/mol ± 11 mmol/mol, 48 mmol/mol ± 11 mmol/mol und 64 mmol/mol ± 11 mmol/mol). • Acetyliertes Hämoglobin mit mindestens 50 mg/dl (2,8 mmol/l) Acetylsalicylsäure • Carbamyliertes Hämoglobin mit mindestens 10 mmol/l Cyanat • Labiles Hämoglobin mit mindestens 1500 mg/dl (83,3 mmol/l) Glukose
Nachweisgrenze und LeerwertgrenzeDie Leerwertgrenze (LoB) und die Nachweisgrenze (LoD) wurden gemäß CLSI-Richtlinie EP17-A2 ermittelt.23
Die LoB ist das höchste Messergebnis, das bei einer Leerwertprobe beobachtet werden kann. Die LoB wurde anhand 60 Bestimmungen mit je 5 Leerproben für tHb und 75 Bestimmungen mit je 5 Leerproben für %HbA1c/HbA1c ermittelt.
Die LoD entspricht der niedrigsten HbA1c- oder tHb-Konzentration, die mit einer Wahrscheinlichkeit von 95 % nachgewiesen werden kann. Die LoD wurde anhand 60 Bestimmungen mit je 5 Untergrenzen-Proben für tHb und 75 Bestimmungen mit je 5 Untergrenzen-Proben für %HbA1c/HbA1c ermittelt.
Im Folgenden sehen Sie die LoD und LoB für den Dimension® Hämoglobin A1C-Test.
Voir les sections ombrées : Informations mises à jour à partir de la version 2019-04. Date d’édition 2019-10
Dimension® clinical chemistry system
A1CFlex® reagent cartridge
DF105B
Dosage hémoglobine A1CUtilisation : le dosage d’hemoglobine A1C Dimension® est un test de diagnostic in vitro pour la détermination quantitative de l’HbA1c exprimé en % (DCCT/NGSP) et en mmol/mol (IFCC) dans le sang total veineux anticoagulé humain à utiliser sur le système de chimie clinique Dimension®. La mesure de l’hémoglobine A1c est utilisée pour faciliter le diagnostic et la surveillance à long terme de la glycémie chez les patients atteints de diabète sucré et facilite l’identification des patients ayant un risque de développer un diabète sucré.
Résumé : l’HbA1c fait référence au produit d’une réaction non enzymatique entre le glucose et l’hémoglobine A1. L’érythrocyte humain laisse librement passer le glucose, qui peut s’associer de façon non enzymatique à l’hémoglobine pour former l’HbA1c. Cette réaction non enzymatique entre le groupe alpha-aminé de la valine N-terminale de la chaîne bêta de l’hémoglobine et le glucose entraîne la formation d’une aldimine instable ou d’un intermédiaire de type base de Schiff (fraction labile). Cette réaction est lente et réversible et se produit à une vitesse proportionnelle à la concentration de glucose dans le sang. L’aldimine intermédiaire subit ensuite un réarrangement d’Amadori non réversible qui forme un produit stable de kétoamine 1-glucofrutovaline. Comme la réaction dépend de la concentration des réactifs, le degré de glycosylation (indiqué par le ratio de l’HbA1c sur l’hémoglobine totale) est proportionnel à la concentration moyenne de glucose dans le sang sur une période équivalent à la durée de vie circulante de l’hémoglobine dans les globules rouges (environ 120 jours).1,2
L’utilité des mesures de HbA1c a été démontrée dans l’essai Diabetes Control and Complications Trial (DCCT).3 Une découverte importante de cette étude est la corrélation directe existant entre le contrôle glycémique et le résultat du patient en ce qui concerne les complications à long terme. Les patients montrant un meilleur contrôle glycémique (c’est-à-dire avec un taux d’HbA1c inférieur) ont présenté un bien meilleur pronostic concernant les complications micro-vasculaires, dont la neuropathie, la rétinopathie et la néphropathie.3
Principes de la méthode : Le dosage de l’hemoglobine A1C Dimension® mesure à la fois l’HbA1c et l’hémoglobine totale. La mesure de l’HbA1c se fonde sur un principe d’immunodosage par inhibition turbidimétrique (TINIA), tandis que la mesure de l’hémoglobine totale repose sur une modification de la réaction d’hématine alcaline. À l’aide des valeurs obtenues pour chacun de ces deux analytes, la proportion relative d’hémoglobine totale glyquée est alors calculée et communiquée. Il n’est pas nécessaire d’effectuer de prétraitement pour retirer la fraction labile car seule la forme d’Amadori réarrangée de l’HbA1c est détectée. Ce dosage mesure toutes les variantes d’hémoglobine glyquées à l’extrémité N-terminale de la chaîne bêta et dont les épitopes sont identiques à ceux de l’HbA1c.
Mesure de l’hémoglobine totale : un échantillon de sang total est ajouté à la première cuvette contenant le réactif lysant. Ce réactif lyse les globules rouges et convertit simultanément l’hémoglobine libérée en dérivé dont le spectre d’absorbance est caractéristique. On transfère une aliquote du sang total lysé de la première cuvette vers une deuxième, où la concentration d’hémoglobine totale est mesurée à 405 et 700 nm.4
Sang total + agent lysant Hémoglobine libérée dérivé d’hémoglobine (mesuré à 405 nm)
Mesure de l’hémoglobine A1c : pour la mesure de l’HbA1c, on utilise la même aliquote de sang total lysé qui est transférée de la première cuvette vers la deuxième pour la mesure de l’Hb. La deuxième cuvette contient un anticorps anti-HbA1c dans un réactif tamponné. L’hémoglobine A1c présente dans l’échantillon réagit avec l’anticorps anti-HbA1c pour former un complexe soluble antigène-anticorps. Un réactif polyhaptène contenant plusieurs épitopes d’HbA1c est ensuite ajouté à cette cuvette. Le polyhaptène réagit avec les anticorps anti-HbA1c en excès (libres) pour former un complexe anticorps-polyhaptène insoluble. La vitesse de cette réaction est mesurée de façon turbidimétrique à 340 nm et à blanc à 700 nm et est inversement proportionnelle à la concentration de HbA1c dans l’échantillon.
anticorps anti-HbA1c (excès) + polyhaptène complexe Ab/polyhaptène(absorption à 340 nm)
Composants du kit A1C
Remarque : chaque lot de kits contient des jeux correspondants de cartouches de réactifs A1C Flex® et de calibrateurs. Ces composants ne sont pas interchangeables entre des kits portant des numéros de lot différents.
Réactifs
Puitsa Forme Composant Concentrationb Origine1–2 Liquide Anticorps ≥ 0,5 mg/mlc Mouton, polyclonal de sérum ovin
a. Les puits sont numérotés consécutivement, depuis l’extrémité la plus large de la cartouche.b. Valeur nominale par puits dans une cartouche.c. Le titre de l’anticorps et l’activité du conjugué (ou la concentration du réactif des particules) sont susceptibles
de varier selon les lots.d. MES = acide 2-morpholinoéthane sulfoniquee. TRIS = tris(hydroxyméthyl)-aminométhanef. TTAB = tétradécyl triméthyl bromure d’ammonium
Risque et sécurité :H412P273, P501
AvertissementNocif pour les organismes aquatiques, entraîne des effets néfastes à long terme.
Éviter le rejet dans l’environnement. Éliminer les contenus et les contenants conformément à toutes les réglementations locales, régionales et nationales
Contient : 2-méthyl-H4-isothiazol-3-one
Les fiches de sécurité sont disponibles sur siemens.com/healthcare
Précautions : les cuvettes utilisées contiennent des liquides biologiques humains. Les manipuler avec soin pour éviter tout risque d’ingestion ou de contact avec la peau.
Attention : Aux États-Unis, la loi fédérale n’autorise la vente de ce dispositif que sur ordre ou par un professionnel de la santé agréé.
Pour diagnostic in vitro
Remarque : les réactifs et calibrateurs Flex® A1C sont présentés sous forme de kit. Chaque lot de kits contient des jeux correspondants de cartouches de réactifs A1C Flex® et de calibrateurs A1C. Ne pas interchanger des réactifs portant des numéros de lot différents
Préparation des réactifs : Tous les réactifs sont liquides et prêts à l’emploi.
Conserver entre : 2–8°C
Expiration : Voir la date d’expiration indiquée sur l’emballage du kit. Tous les composants du kit sont stables jusqu’à la date d’expiration lorsqu’ils sont conservés non ouverts entre 2–8°C. Les puits fermés des cartouches sont stables sur l’instrument pendant 30 jours.
Stabilité des puits ouverts : 5 jours pour les puits 1–2 et 5–6 10 jours pour le puits 3
Prélèvement et manipulation des échantillons : Type d’échantillons recommandé : sang total veineux anticoagulé (K2 EDTA ; K3 EDTA ; fluorure sodium/Na2 EDTA ; héparine lithium, ou fluorure de Na/oxalate de K).
Les échantillons doivent être prélevés au moyen des procédures recommandées de prélèvement d’échantillons sanguins pour diagnostic par ponction veineuse.5–7 Suivre les instructions d’utilisation et de traitement fournies avec le dispositif de collecte des échantillons.6
• Avec la méthode A1C, les échantillons ne peuvent être dosés qu’à partir d’une cupule d’échantillon ou d’un SSC.
• Les échantillons ne peuvent pas être dosés directement à partir des tubes de prélèvement primaires. • Les échantillons doivent être mélangés doucement par inversion (en retournant délicatement le tube dix
fois) ou dans un culbuteur avant d’être pipetés dans la cupule d’échantillon ou le SSC afin de garantir la distribution uniforme des érythrocytes avant le test. Éviter la formation de mousse.
• Les échantillons coagulés ne doivent pas être utilisés.• Pipeter 200 µl d’échantillon de sang total dans la cupule d’échantillon ou le SSC.• L’échantillon peut rester jusqu’à une heure dans la cupule d’échantillon sur l’instrument.
Stabilité des échantillons : Les échantillons sont stables lorsqu’ils sont stockés pendant un maximum de :8
3 jours à 15–25°C 7 jours à 2–8°C 4 mois à -20°C (ne congeler qu’une seule fois)
Les informations de stockage des échantillons sont destinées à servir de référence aux utilisateurs ; ceux-ci peuvent toutefois valider leurs propres procédures de conservation des échantillons.
Procédure
Matériel fourniA1C Kit, Réf. catalogue DF105B : inclut des cartouches de réactifs A1C Flex® et le calibrateur A1C (5 niveaux)
Matériel requis mais non fourniMatériel de contrôle de qualité
Étapes du test
L’échantillonnage,g la distribution des réactifs, le mélange et le traitement sont automatiquement réalisés par le système de chimie clinique Dimension®. Pour les détails du traitement, voir le guide de l’opérateur du système Dimension®.
g. Le conteneur d’échantillons doit contenir 200 μl de sang total pour que le nouveau mélange se déroule correctement.
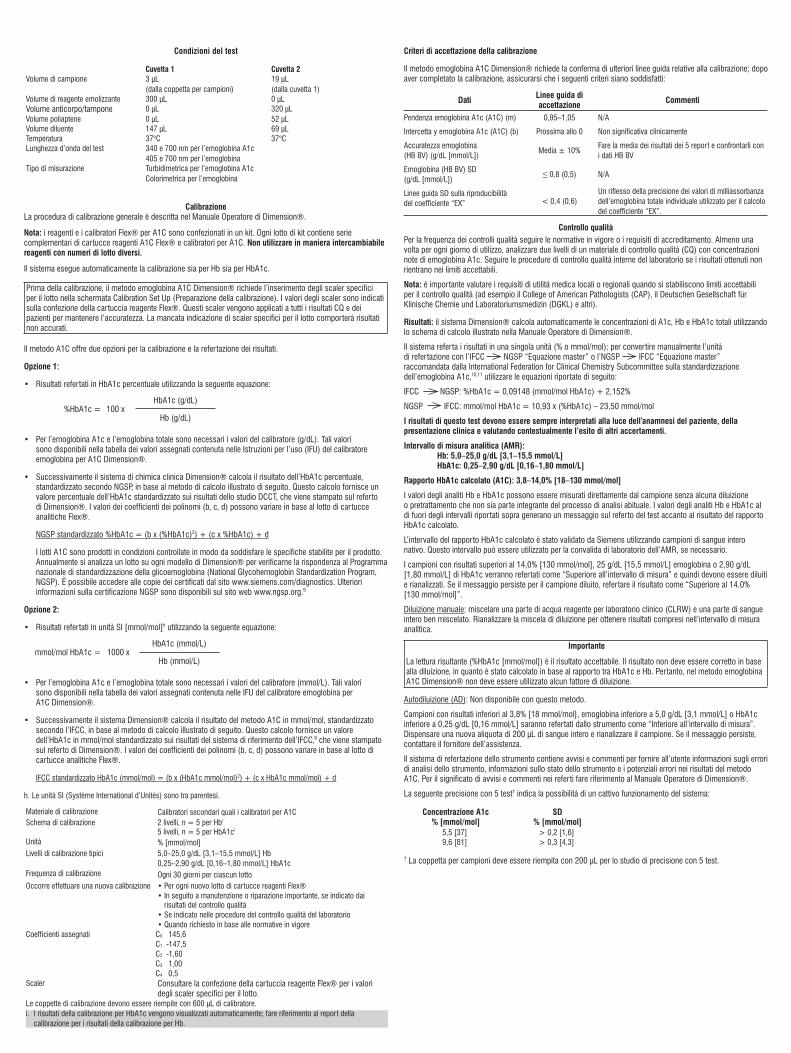
Conditions du test
Cuvette 1 Cuvette 2Volume d’échantillon 3 µl
(depuis la cupule d’échantillon)19 µl(depuis la cuvette 1)
Volume de réactif hémolysant 300 µl 0 µlVolume d’anticorps/tampon 0 µl 320 µlVolume de polyhaptène 0 µl 52 µlVolume de diluant 147 µl 69 µlTempérature 37°C 37°CLongueur d’onde du test 340 et 700 nm pour l’hémoglobine A1c
405 et 700 nm pour l’hémoglobineType de mesure Turbidimétrique pour l’hémoglobine A1c
Colorimétrique pour l’hémoglobine
CalibrationLa procédure de calibration générale est décrite dans le guide de l’opérateur du système Dimension®.
Remarque : les réactifs et calibrateurs Flex® A1C sont présentés sous forme de kit. Chaque lot de kits contient des jeux correspondants de cartouches de réactifs A1C Flex® et de calibrateurs A1C. Ne pas interchanger des réactifs portant des numéros de lot différents.
Le système effectue automatiquement la calibration pour Hb et HbA1c.
Le dosage d’hémoglobine A1C Dimension® nécessite des échelles spécifiques au lot qui doivent être saisies sur l’écran Calibration Set Up (Préparation de la calibration), et ce, avant la calibration. Les valeurs d’échelle sont fournies sur l’emballage de la cartouche de réactifs Flex®. Ces échelles s’appliquent à tous résultats de CQ et des patients pour maintenir la précision. Les résultats seront erronés si ces échelles spécifiques au lot ne sont pas saisies.
La méthode A1C propose deux options de calibration et de communication des résultats.
Option 1 :
• Résultats communiqués en %HbA1c à l’aide de l’équation suivante :
%HbA1c = 100 xHbA1c (g/dl)
Hb (g/dl)
• Les valeurs du calibrateur (g/dl) sont requises pour l’hémoglobine A1c et l’hémoglobine totale. Ces valeurs peuvent être trouvées dans le tableau des valeurs assignées fourni dans le mode d’emploi du calibrateur d’hémoglobine A1C Dimension®.
• Le système de chimie clinique Dimension® calcule ensuite un résultat %HbA1c normalisé selon le NGSP sur la base du calcul présenté ci-dessous. Ce calcul fournit une valeur %HbA1c normalisée selon le résultat de l’étude DCCT, imprimé sur le rapport Dimension®. Les valeurs des coefficients polynomiaux (b, c et d) peuvent varier en fonction du lot de cartouches de réactifs Flex®.
%HbA1c normalisé selon le NGSP = (b x (%HbA1c)2) + (c x %HbA1c) + d
Les lots d’A1C sont produits sous contrôle afin de satisfaire les spécifications établies pour le produit. Une fois par an, un lot est testé sur chaque modèle Dimension® afin de confirmer la normalisation selon le National Glycohemoglobin Standardization Program (NGSP). Des copies des certificats sont disponibles sur le site www.siemens.com/diagnostics. Des informations supplémentaires sur la certification NGSP sont disponibles sur le site www.ngsp.org.9
Option 2 :
• Résultats communiqués en unités SI [mmol/mol]h à l’aide de l’équation suivante :
mmol/mol HbA1c = 1000 xHbA1c (mmol/l)
Hb (mmol/l)
• Les valeurs du calibrateur (mmol/l) sont requises pour l’hémoglobine A1c et l’hémoglobine totale. Ces valeurs peuvent être trouvées dans le tableau des valeurs assignées fourni dans le mode d’emploi du calibrateur d’hémoglobine A1C Dimension®.
• Le système Dimension® calcule ensuite un résultat d’A1C en mmol/mol normalisé selon l’IFCC sur la base du calcul présenté ci-dessous. Ce calcul fournit une valeur d’HbA1c en mmol/mol normalisée selon le système de référence IFCC,9 imprimé sur le rapport Dimension®. Les valeurs des coefficients polynomiaux (b, c et d) peuvent varier en fonction du lot de cartouches de réactifs Flex®.
HbA1c normalisée selon l’IFCC (mmol/mol) = (b x (HbA1c mmol/mol)2) + (c x HbA1c mmol/mol) + d
h. Les unités SI [Système International d’Unités] sont indiquées entre crochets.
Matériel de calibration Calibrateurs secondaires tels que des calibrateurs A1CSchéma de calibration 2 niveaux, n = 5 pour Hbi
0,25–2,90 g/dl [0,16–1,80 mmol/l] HbA1cFréquence de calibration Tous les 30 jours pour chaque lotUne nouvelle calibration est requise • Pour chaque nouveau lot de cartouches de réactifs Flex®
• Après une maintenance ou une réparation majeure, en fonction des résultats du contrôle de qualité
• Comme indiqué dans les procédures de contrôle de qualité du laboratoire• Selon les réglementations nationales en vigueur
Facteurs d’échelle Voir l’emballage de la cartouche de réactifs Flex® pour obtenir les valeurs d’échelles spécifiques au lot.
Les cupules de calibration doivent être remplies avec 600 µl de calibrateur.i. Les résultats de calibration pour l’HbA1c s’affichent automatiquement ; se référer au rapport de calibration pour les
résultats d’Hb.
Critères d’acceptation de la calibration
Le dosage d’hémoglobine A1C Dimension® nécessite la confirmation de recommandations supplémentaires pour la calibration ; une fois la calibration terminée, vérifier que les critères suivants sont remplis :
Données Recommandation d’acceptation Commentaires
Hémoglobine A1c (A1C) Pente (m) 0,95–1,05 S/O
Hémoglobine A1c (A1C) Ordonnée à l’origine y (b)
Proche de 0 Aucun intérêt clinique
Hémoglobine (HB BV) Exactitude (g/dl [mmol/l])
Moyenne ± 10 %Moyenne des résultats des 5 rapports et comparaison avec les données HB BV
Hémoglobine (HB BV) ET (g/dl [mmol/l])
≤ 0,8 (0,5) S/O
Recommandation concernant l’écart-type de reproductibilité du coefficient « EX » < 0,4 (0,6)
Une réflexion de la précision des valeurs de milliabsorbance individuelles de l’hémoglobine totale utilisée pour le calcul du coefficient de calibration « EX ».
Contrôle de qualitéSe conformer aux réglementations ou exigences d’accréditation réglementaires pour la fréquence de passage du contrôle de qualité. Analyser au moins une fois par jour d’utilisation deux niveaux d’un matériel de contrôle de qualité aux concentrations connues d’hémoglobine A1c. Si les résultats obtenus ne sont pas compris dans les limites acceptables, suivre les procédures de contrôle de qualité internes du laboratoire.
Remarque : il est important de tenir compte des exigences locales ou régionales en matière d’utilité médicale lors de la définition des limites acceptables pour le contrôle de qualité (par exemple College of American Pathologists (CAP), Deutsche Gesellschaft für Klinische Chemie und Laboratoriumsmedizin (DGKL) et autres).
Résultats : le système Dimension® calcule automatiquement les concentrations d’A1c totale, d’Hb et d’HbA1c grâce au schéma de calcul illustré dans le guide de l’opérateur du système Dimension®.
Le système indique les résultats dans une seule unité (% ou mmol/mol) ; pour convertir manuellement l’unité de rapport avec l’« équation maîtresse » IFCC NGSP ou l’« équation maîtresse » NGSP IFCC recommandée par l’International Federation for Clinical Chemistry Subcommittee on Hemoglobin A1c standardization,10,11 utilisez les équations ci-dessous :
Les résultats de ce test doivent toujours être interprétés en rapport avec les antécédents médicaux du patient, les signes cliniques et autres constatations.
Rapport HbA1c calculé (A1C) : 3,8–14,0 % [18–130 mmol/mol]
Les valeurs d’analyte Hb et HbA1c peuvent être mesurées directement dans l’échantillon sans dilution ni traitement préalable qui ne fasse pas partie de la méthode d’analyse usuelle. Les valeurs d’analyte Hb et HbA1c situées hors des domaines ci-dessus déclenchent un message de rapport de test qui apparaît avec le résultat du ratio HbA1c calculé.
Le domaine du ratio d’HbA1c calculé a été validé par Siemens à l’aide d’échantillons de sang total natifs. Il peut être utilisé pour la validation du domaine de mesure analytique (AMR) en laboratoire, si nécessaire.
Les échantillons dont les résultats sont supérieurs à 14,0 % [130 mmol/mol], 25 g/dl [15,5 mmol/l] pour l’hémoglobine ou à 2,90 g/dl [1,80 mmol/l] pour l’HbA1c seront signalés comme étant « Supérieurs au domaine de mesure » et devront être répétés après dilution. Si le message persiste sur l’échantillon dilué, communiquer le résultat comme étant « Supérieur à 14,0 % [130 mmol/mol] ».
Dilution manuelle : mélanger un volume d’eau de qualité réactif laboratoire clinique à un volume de sang total bien mélangé. Redoser le mélange de dilution afin d’obtenir des résultats compris dans le domaine de mesure analytique.
Important
La valeur obtenue (%HbA1c [mmol/mol]) est le résultat à communiquer. Le résultat ne doit pas être corrigé pour tenir compte de la dilution car il s’agit d’un résultat calculé en fonction d’un ratio entre HbA1c et Hb. Il ne faut donc pas utiliser de facteur de dilution avec le dosage d’hémoglobine A1C Dimension®.
Dilution automatique (DA) : non disponible avec cette méthode.
Les échantillons ayant des résultats inférieurs à 3,8 % [18 mmol/mol], une hémoglobine inférieure à 5,0 g/dl [3,1 mmol/l] ou un HbA1c inférieur à 0,25 g/dl [0,16 mmol/l] seront signalés comme étant « Inférieur au domaine de mesure » par l’instrument. Distribuer une nouvelle aliquote de 200 µl de sang total et redoser l’échantillon. Si le message persiste, contacter votre technicien local pour obtenir de l’aide.
Le système de rapport de l’instrument renvoie des indicateurs et des commentaires qui fournissent à l’opérateur des informations concernant les erreurs de traitement de l’instrument, les informations d’état de l’instrument et les erreurs potentielles dans les résultats d’A1C. Pour connaître la signification de ces indicateurs et commentaires, voir le manuel de l’opérateur du système Dimension®.
Il peut y avoir un dysfonctionnement du système si la précision suivante est observée lors de 5 tests consécutifs† :
Concentration d’A1c % [mmol/mol]
ET % [mmol/mol]
5,5 [37] > 0,2 [1,6]9,6 [81] > 0,3 [4,3]
† La cupule d’échantillons doit être remplie avec 200 µl pour l’étude de précision sur 5 tests.
Limites de la procédure
AVERTISSEMENTLe dosage d’hemoglobine A1C Dimension® présente une interférence significative avec l’hémoglobine fœtale (HbF). Les échantillons contenant de la HbF peuvent produire un biais négatif (inférieur aux résultats réels) avec le dosage d’hémoglobine A1C Dimension®. Les résultats de l’hémoglobine A1c sont invalides pour les patients ayant des quantités anormales d’HbF, y compris ceux ayant une persistance héréditaire connue de l’hémoglobine fœtale. Pour plus d’informations sur l’interférence de la variante HbF, consultez Substances interférentes.
Ne pas utiliser les calibrateurs d’hémoglobine A1C Dimension® pour tester la précision.
Comme pour toute autre procédure de laboratoire, un écart important entre l’impression clinique et les résultats du test nécessite en général de plus amples investigations. Certaines des limites suivantes sont à prendre en considération pour le test :
Le dosage d’hémoglobine A1C Dimension® est conçu uniquement pour la mesure exacte et précise de mmol/mol HbA1c (IFCC) et %HbA1c (DCCT/NGSP). Les résultats individuels de concentration totale de Hb et HbA1c ne sont pas signalés.
Les patients ayant des concentrations d’hémoglobine en dehors de la plage acceptable pour le dosage d’hémoglobine A1C Dimension® doivent être dosés par un test utilisant un principe de test différent.
Le dosage d’hémoglobine A1C Dimension® ne doit pas être utilisé pour diagnostiquer le diabète pendant la grossesse. L’hémoglobine A1c reflète la glycémie moyenne sur les 3 mois précédents (la durée de vie moyenne d’un globule rouge) et peut donc être faussement basse pendant la grossesse ou tout autre état associé à un début récent d’hyperglycémie et/ou une baisse de la survie des globules rouges.
Le dosage d’hémoglobine A1C Dimension® ne doit pas être utilisé pour diagnostiquer ou surveiller le diabète chez les patients ayant les pathologies suivantes : hémoglobinopathies, sauf si une performance acceptable est avérée (par exemple drépanocytose), cycle de gobules rouges anormal (par exemple anémies d’hémolyses et carence en fer), tumeurs et maladie hépatique et rénale chronique grave.
Dans les cas de diabète de type 1 à évolution rapide, l’augmentation des valeurs d’HbA1c peut être retardée par rapport à l’augmentation aiguë de la glycémie. Dans ces conditions, le diabète sucré doit être diagnostiqué d’après les concentrations de glucose dans le plasma et/ou les symptômes cliniques typiques.
Ce test ne doit pas remplacer le test du glucose chez les patients atteints de diabète de type 1, les patients pédiatriques ou les femmes enceintes.
Toute cause de survie réduite des globules rouges (par exemple anémie hémolytique ou autre maladie hémolytique, grossesse ou perte de sang importante récente) réduit l’exposition des globules rouges au glucose avec une baisse constante des valeurs d’HbA1c. Les résultats HbA1c ne sont pas fiables chez les patients souffrant de pertes de sang chroniques et dont la durée de vie des érythrocytes est donc variable.12–15
Valeurs attendues :
La plage de référence pour l’HbA1c figure dans le tableau ci-dessous.16
Les valeurs de l’hémoglobine A1c sur des individus en bonne santé peuvent varier selon les populations de référence. Chaque laboratoire doit vérifier la validité de l’intervalle de référence et définir, si nécessaire, son propre intervalle de référence.
La fréquence du test d’HbA1c doit dépendre de la situation clinique, du régime de traitement et du jugement du clinicien. L’American Diabetes Association recommande un objectif d’HbA1c raisonnable pour de nombreux adultes non enceintes < 7 %. Des objectifs d’HbA1c moins stricts peuvent convenir à certains patients avec un diabète et d’autres facteurs de risque, tels qu’une hypoglycémie grave ou des conditions comorbides extensives.17
Substances interférentes
Différentes substances autres que les sucres sont susceptibles de former des agrégats avec l’hémoglobine et éventuellement d’interférer avec le dosage en générant de faux résultats. Ceci peut se produire chez les individus souffrant d’addiction aux opiacés,18 d’empoisonnement au plomb et d’alcoolisme.12
Le réactif de l’anticorps utilisé dans le dosage de l’hémoglobine A1C Dimension® mesure toutes les variantes d’hémoglobine glycosylée qui sont glyquées à l’extrémité N-terminale de la chaîne bêta et dont les épitopes sont identiques à ceux de l’HbA1c (séquence d’acides aminés : VAL-HIS-LEU-THR). Cela inclut HbS, HbC, HbD et HbE. D’autres hémoglobinopathies sont susceptibles de donner des résultats erronés avec ce test. Les résultats HbA1c de patients présentant des variantes d’Hb doivent être interprétés avec prudence. Des hémoglobines anormales peuvent affecter la demi-vie des globules rouges ou les taux de glycation in vivo. Dans ces cas, même des résultats corrects d’un point de vue analytique ne reflètent pas le même niveau de contrôle glycémique que celui attendu chez les patients présentant une hémoglobine normale.14
L’HbF (hémoglobine fœtale) glyquée, qui est constituée de deux chaînes alpha et de deux chaînes gamma, n’est pas reconnue par l’anticorps anti-HbA1c. Les personnes affichant des niveaux élevés d’HbF (> 10 %), principalement des nourrissons et des patients atteints de bêta-thalassémie, peuvent produire des résultats inférieurs aux attentes avec ce dosage. Ces échantillons doivent être dosés selon une autre méthode.
Aucune réactivité croisée n’a été observée pour les anticorps anti HbA1c utilisés dans ce kit avec HbA0, HbA1a, HbA1b, l’hémoglobine acétylée, l’hémoglobine carbamylée et l’HbA1c labile.
Caractéristiques spécifiques de performance
Les données suivantes représentent les performances types du système Dimension®. Les résultats réels obtenus par chaque laboratoire peuvent différer en fonction de la conception de l’étude.
PrécisionLe test de précision a été effectué conformément au document EP05-A3 du CLSI.19 Le test a été effectué sur 20 jours de test avec 3 instruments et 3 lots de réactifs sur chaque instrument. Chaque jour de test, 2 séries ont été effectuées (avec un intervalle minimum de 2 heures).
NGSP (%HbA1c)
Répétabilité (Intra-séries)
Intra-laboratoire (Total)
Type d’échantillon N Moyenne ETj CV (%)k ETj CV (%)k
Contrôle 1 720 5,2 0,05 1,0 0,13 2,6Contrôle 2 720 9,5 0,08 0,8 0,16 1,7Pool 1 de sang total 720 5,3 0,05 0,9 0,13 2,4Pool 2 de sang total 720 6,4 0,05 0,7 0,11 1,7Pool 3 de sang total 720 7,8 0,06 0,8 0,13 1,6Pool 4 de sang total 720 11,9 0,09 0,8 0,22 1,8
IFCC (mmol/mol)Répétabilité (Intra-séries)
Intra-laboratoire (Total)
Type d’échantillon N Moyenne ETj CV (%)k ETj CV (%)k
Contrôle 1 720 34 0,56 1,7 1,47 4,4Contrôle 2 720 81 0,87 1,1 1,73 2,2Pool 1 de sang total 720 35 0,54 1,5 1,42 4,1Pool 2 de sang total 720 47 0,52 1,1 1,17 2,5Pool 3 de sang total 720 62 0,68 1,1 1,41 2,3Pool 4 de sang total 720 107 0,99 0,9 2,41 2,3
j. Écart-typek. Coefficient de variation
Comparaison de méthodeLe test de comparaison de méthode a été effectué conformément au document EP09-A3 du CLSI.20 Les résultats du dosage d’hémoglobine A1C Dimension® (y) ont été comparés aux résultats obtenus avec une méthode de test standardisée du NGSP (HPLC) (x).
Régression de Passing-Bablok
Unités N Plage d’échantillons Pente IC 95 % Ordonnée
Les données de comparaison de méthode ont été évaluées à l’aide de l’analyse de biais de Bland-Altman,21 qui est l’approche utilisée par le NGSP. La différence moyenne entre l’A1C et la méthode du réseau du NGSP (HPLC) et les intervalles de confiance à 95 % des différences dans le domaine de 4–10 % d’HbA1c sont fournis. 95 % des différences entre les valeurs obtenues pour des échantillons individuels à l’aide des deux méthodes sont comprises dans le domaine défini par les intervalles de confiance à 95 % inférieur et supérieur des différences.
Siemens Healthcare Diagnostics Inc.500 GBC DriveNewark, DE 19714 USA
2019
-10
C P
N 11
2752
89 -
FR
Comparaison d’anticoagulantUn test d’équivalence pour 5 anticoagulants a été effectué conformément au document EP09-A3 du CLSI.20 Le test a été réalisé avec un lot de réactifs et un seul réplicat d’un jeu correspondant de chacun des 4 anticoagulants (K3 EDTA ; fluorure de sodium/Na2 EDTA ; héparine-lithium et fluorure de Na/oxalate de K) et des échantillons de K2 EDTA.
Régression de Passing-Bablok : NGSP (%)
Anticoagulant Échantillon de comparaison (x) Pente IC 95 % Ordonnée à l’origine y IC 95 %
Fluorure de Na/oxalate de K K2 EDTA 1,007 0,989–1,025 -0,032 -1,22–1,16
Nombre d’échantillons (N) = 79Plage d’échantillons (mmol/mol) = 28–125
Spécificité
Substances non interférentes
Le test d’interférence a été effectué conformément au document EP07-A2 du CLSI.22
Les substances suivantes n’interfèrent pas avec le dosage d’hémoglobine A1C Dimension® lorsqu’elles sont présentes dans le sang total aux concentrations indiquées. Les imprécisions (biais) dues à ces substances sont inférieures ou égales à 5 % à des concentrations d’hémoglobine A1c de 6,5 % ± 1,0 % et 8,0 % ± 1,0 % (inférieur ou égal à 8 % à 48 mmol/mol ± 11 mmol/mol et 64 mmol/mol ± 11 mmol/mol).
Substance interférente Concentration de substance interférente
Variantes de l’hémoglobineUn test d’interférence pour déterminer l’effet des variantes de l’hémoglobine sur le dosage d’hémoglobine A1C Dimension® a été effectué conformément au document EP07-A2 du CLSI.22 Aucun biais d’interférence significatif n’a été observé pour l’HbC, HbD, HbE et HbA2. Un biais d’interférence significatif a été observé pour l’HbF.
NGSP
Biais relatif %(Biais en % de plage)
Biais relatif %(Biais en % de plage)
Variante d’Hb N Plage (% variante)
Plage (%HbA1c) ~6 % HbA1c ~9 % HbA1c
HbC 37 26,1–40,0 4,4–15,7 -1,0 % (-5,0–4,9 %)
-0,9 % (-4,6–4,4 %)
HbD 20 24,8–38,4 5,0–13,0 -2,2 % (-4,9–4,4 %)
-2,5 % (-4,4– -1,3 %)
HbE 22 19,7–30,4 4,7–11,0 -2,1 % (-4,9–3,1 %)
-2,5 % (-4,3– -1,0 %)
HbS 22 27,5–36,3 5,3–14,0 -1,3 % (-4,7–4,9 %)
-2,0 % (-4,9–3,5 %)
HbA2 23 4,3–6,2 5,1–8,4 0,1 % (-4,8–3,6 %)
-2,0 % (-3,0– -1,1 %)
HbF 20 4,3–29,3 4,3–10,1 -23,2 % (-30,3–1,2 %)
-24,7 % (-25,8– -23,3 %)
IFCC
Biais relatif %(Biais en % de plage)
Biais relatif %(Biais en % de plage)
Variante d'Hb N Plage (% variante)
Plage (mmol/mol HbA1c) ~42 mmol/mol ~75 mmol/mol
HbC 37 26,1–40,0 25–148 -1,4 % (-8,2–8,2 %)
-1,2 % (-5,7–6,2 %)
HbD 20 24,8–38,4 31–119 -3,5 % (-8,1–7,1 %)
-3,4 % (-5,2– -1,8 %)
HbE 22 19,7–30,4 28–97 -3,4 % (-8,2–5,2 %)
-3,3 % (-6,2– -1,3 %)
HbS 22 27,5–36,3 34–130 -2,0 % (-7,6–7,6 %)
-2,6 % (-6,3–4,1 %)
HbA2 23 4,3–6,2 32–68 0,2 % (-8,3–6,1 %)
-2,7 % (-4,1– -1,6 %)
HbF 20 4,3–29,3 23–87 -37,0 % (-48,6–2,0 %)
-32,7 % (-36,3– -30,8 %)
Dérivés d’hémoglobineUn test d’interférence destiné à déterminer l’effet des dérivés de l’hémoglobine, y compris l’hémoglobine acétylée, l’hémoglobine carbamylée, l’hémoglobine labile et les fractions d’hémoglobine sur le dosage d’hémoglobine A1C Dimension® a été effectué conformément au document EP07-A2 du CLSI.22 Les imprécisions (biais) dues à ces substances sont inférieures ou égales à 5 % à des concentrations d’hémoglobine A1c de 5,0 % ± 1,0 %, 6,5 % ± 1,0 % et 8,0 % ± 1,0 % (inférieur ou égal à 9 % à 31 mmol/mol ± 11 mmol/mol, 48 mmol/mol ± 11 mmol/mol et 64 mmol/mol ± 11 mmol/mol). • L’hémoglobine acétylée avec 50 mg/dl (2,8 mmol/l) ou plus d’acide acétylsalicylique • L’hémoglobine carbamylée avec 10 mmol/l ou plus de cyanate • L’hémoglobine labile avec 1500 mg/dl (83,3 mmol/l) ou plus de glucose
Limite de détection et limite du blancLa limite de détection (LdD) et la limite du blanc (LdB) ont été déterminées conformément au document EP17-A2 du CLSI.23
La LdB est le résultat de mesure le plus élevé susceptible d’être observé dans un échantillon blanc. La LdB a été déterminée à l’aide de 60 déterminations avec 5 échantillons blancs chacun pour la tHb et 75 déterminations avec 5 échantillons blancs chacun pour %HbA1c/HbA1c.
La LdD correspond à la concentration minimale de HbA1c ou de tHb pouvant être détectée avec une probabilité de 95 %. La LdD a été déterminée à l’aide de 60 déterminations avec 5 échantillons à faible niveau chacun pour la tHb et 75 déterminations avec 5 échantillons faibles chacun pour %HbA1c/HbA1c.
La LdB et LdD pour le dosage de l’hémoglobine A1C Dimension® figurent ci-dessous.
Vedere le sezioni ombreggiate: informazioni aggiornate dalla versione 2019-04. Data di edizione 2019-10
Dimension® clinical chemistry system
A1CFlex® reagent cartridge
DF105B
Test emoglobina A1CUso previsto: il metodo emoglobina A1C Dimension® è un test diagnostico in vitro per la determinazione quantitativa di %HbA1c (DCCT/NGSP) e HbA1c in mmol/mol (IFCC) in sangue intero venoso anticoagulato umano da utilizzare sul sistema di chimica clinica Dimension®. La misurazione dell’emoglobina A1c è utilizzata come ausilio nella diagnosi e nel monitoraggio del controllo glicemico a lungo termine in pazienti affetti da diabete mellito e come ausilio nell’identificazione di pazienti a rischio di sviluppare il diabete mellito.
Riassunto: HbA1c si riferisce al prodotto di una reazione non enzimatica tra glucosio ed emoglobina A1. Gli eritrociti umani sono facilmente permeabili da parte del glucosio, il quale è in grado di combinarsi con l’emoglobina in maniera non enzimatica, formando HbA1c. Da questa reazione non enzimatica fra il gruppo alfa-amminico della valina N-terminale della catena beta dell’emoglobina e il glucosio si forma una aldimina instabile o base di Schiff intermedia (frazione labile). Questa reazione, lenta e reversibile, avviene a un tasso proporzionale alla concentrazione di glucosio nel sangue. L’aldimina intermedia viene in seguito sottoposta a un riarrangiamento di Amadori non reversibile e forma una ketamina stabile, la 1-glucofrutovalina. Poiché la reazione è determinata dalla concentrazione dei reagenti, il grado di glicosilazione (refertato come HbA1c relativo all’emoglobina totale) è proporzionale alla concentrazione media del glucosio nel sangue durante il periodo di sopravvivenza in circolo dell’emoglobina nei globuli rossi (circa 120 giorni).1,2
L’utilità delle misurazioni dell’HbA1c è stata dimostrata nello studio sperimentale DCCT (Diabetes Control and Complications Trial).3 Un risultato significativo di questo studio è stata la correlazione diretta fra il controllo glicemico e la prognosi del paziente rispetto alle complicanze a lungo termine. I pazienti con un miglior controllo glicemico, ossia con valori minori dell’HbA1c, hanno evidenziato una prognosi significativamente migliore rispetto alle complicanze microvascolari, fra cui neuropatia, retinopatia e nefropatia.3
Principi del metodo: Il metodo emoglobina A1C Dimension® misura sia l’HbA1c sia l’emoglobina totale. La misurazione dell’HbA1c si basa su un principio di immunoinibizione turbidimetrica (TINIA), mentre la misurazione dell’emoglobina totale si basa su una modifica della reazione dell’ematina alcalina. Utilizzando i valori ottenuti da ciascuno di questi due analiti, viene calcolata e refertata la proporzione relativa di emoglobina totale glicata. Non è necessario un pretrattamento per rimuovere la frazione labile in quanto viene rilevata soltanto la forma dell’HbA1c che ha subito il riarrangiamento di Amadori. Il test misura tutte le varianti dell’emoglobina glicate in corrispondenza dell’N-terminale della catena beta e con epitopi identici a quelli dell’HbA1c.
Misurazione dell’emoglobina totale: Un campione di sangue intero viene aggiunto alla prima cuvetta contenente il reagente lisante. Il reagente lisa i globuli rossi e contemporaneamente trasforma l’emoglobina rilasciata in un derivato con uno spettro di assorbanza caratteristico. Un’aliquota del sangue intero lisato viene trasferita dalla prima alla seconda cuvetta, nella quale viene misurata la concentrazione di emoglobina totale a 405 nm e 700 nm4.
Misurazione dell’emoglobina A1c: La stessa aliquota di sangue intero lisato che viene trasferita dalla prima alla seconda cuvetta per la misurazione dell’Hb viene utilizzata anche per la misurazione dell’HbA1c. La seconda cuvetta contiene un anticorpo anti-HbA1c in un reagente tamponato. L’emoglobina A1c presente nel campione reagisce con l’anticorpo anti-HbA1c a formare un complesso antigene-anticorpo solubile. In questa cuvetta viene quindi aggiunto un reagente poliaptenico contenente vari epitopi dell’HbA1c. Il poliaptene reagisce con gli anticorpi anti-HbA1c in eccesso (liberi) a formare un complesso anticorpo-poliaptene insolubile. Il tasso di questa reazione viene misurato turbidimetricamente a 340 nm, con bianco a 700 nm, ed è inversamente proporzionale alla concentrazione di HbA1c nel campione.
anticorpo anti-HbA1c (in eccesso) + poliaptene Complesso Ab/poliaptene(assorbe a 340 nm)
Componenti del kit A1C
Nota: ogni lotto di kit contiene serie complementari di cartucce reagenti A1C Flex® e calibratori per A1C. Questi componenti non sono intercambiabili fra kit con numeri di lotto diversi.
Reagenti
Pozzettia Forma Componente Concentrazioneb Origine1–2 Liquida Anticorpo ≥ 0,5 mg/mLc Ovina, policlonale da siero ovino
a. I pozzetti sono numerati in sequenza a partire dall’estremità larga della cartuccia.b. Valore nominale per pozzetto in una cartuccia.c. La titolazione dell’anticorpo e l’attività del coniugato (o concentrazione del reagente con particelle) possono
variare da un lotto all’altro.d. MES = acido 2-morfolinoetansulfonicoe. TRIS = tris(idrossimetil)-amminometanof. TTAB = tetradecil trimetil ammonio bromuro
Rischio e sicurezza:H412P273, P501
Avvertenza!Nocivo per gli organismi acquatici con effetti di lunga durata.
Non disperdere nell’ambiente. Smaltire il prodotto e il contenitore in conformità con tutte le disposizioni locali, regionali e nazionali
Contiene: 2-metil-H4-isotiazol-3-one
Le schede di sicurezza sono disponibili sul sito siemens.com/healthcare
Precauzioni: Le cuvette usate contengono liquidi di origine umana; maneggiare con cura per evitarne il contatto con la pelle o l’ingestione.
Attenzione: la legge federale statunitense limita la vendita di questo dispositivo solo su ordine di operatori sanitari abilitati.
Per uso diagnostico in vitro
Nota: i reagenti e i calibratori Flex® per A1C sono confezionati in un kit. Ogni lotto di kit contiene serie complementari di cartucce reagenti A1C Flex® e calibratori per A1C. Non utilizzare in maniera intercambiabile reagenti con numeri di lotto diversi
Preparazione del reagente: Tutti i reagenti sono liquidi e pronti per l’uso.
Conservare a: 2–8°C
Scadenza: Vedere la data di scadenza sulla confezione del kit. Tutti i componenti del kit sono stabili fino alla data di scadenza se conservati chiusi a 2–8°C. I pozzetti delle cartucce sigillate sullo strumento sono stabili per 30 giorni.
Stabilità pozzetto aperto: 5 giorni per pozzetti 1–2 e 5–6 10 giorni per il pozzetto 3
Raccolta e manipolazione dei campioni: Tipo di campione consigliato: sangue intero venoso anticoagulato umano (K2 EDTA; K3 EDTA; fluoruro di sodio/Na2 EDTA; litio eparina o Na fluoruro/K-ossalato).
I campioni devono essere prelevati utilizzando le procedure raccomandate per il prelievo di campioni di sangue per diagnostica mediante venipuntura.5–7 Per l’uso del dispositivo di raccolta dei campioni e l’analisi, seguire le istruzioni fornite con il dispositivo.6
• I campioni da utilizzare con il metodo A1C possono essere analizzati soltanto dalle coppette per campioni o contenitori SSC.
• Non è possibile effettuare l’analisi direttamente dalle provette di raccolta primarie. • Miscelare delicatamente i campioni mediante capovolgimento (capovolgere la provetta delicatamente per
dieci volte) oppure con un agitatore prima di pipettare nella coppetta per campioni o contenitore SSC, in modo da ottenere una distribuzione uniforme degli eritrociti prima del test. Evitare la formazione di schiuma.
• Non utilizzare campioni contenenti coaguli.• Pipettare 200 µL di campione di sangue intero nella coppetta per campioni o contenitore SSC.• Il campione può rimanere nella coppetta sullo strumento per un’ora al massimo.
Stabilità dei campioni: I campioni sono stabili se conservati per un periodo non superiore a:8
3 giorni a 15–25°C 7 giorni a 2–8°C 4 mesi a -20°C (congelare una sola volta)
Lo scopo delle presenti informazioni sulla conservazione dei campioni è di fornire una guida agli utenti; tuttavia gli utenti possono applicare le proprie procedure per la conservazione dei campioni.
Procedura
Materiali fornitiKit A1C, Num. cat. DF105B: include cartucce reagenti Flex® per A1C e il calibratore per A1C (5 livelli)
Materiali necessari ma non fornitiMateriali di controllo qualità
Fasi del test
Il sistema di chimica clinica Dimension® effettua automaticamente il campionamento,g l’erogazione del reagente, la miscelazione e il processo di analisi. Per ulteriori informazioni, fare riferimento al Manuale Operatore di Dimension®.
g. Il contenitore del campione deve contenere 200 μL di sangue intero per garantire un’adeguata rimiscelazione.
Condizioni del test
Cuvetta 1 Cuvetta 2Volume di campione 3 µL
(dalla coppetta per campioni)19 µL(dalla cuvetta 1)
Volume di reagente emolizzante 300 µL 0 µLVolume anticorpo/tampone 0 µL 320 µLVolume poliaptene 0 µL 52 µLVolume diluente 147 µL 69 µLTemperatura 37°C 37°CLunghezza d’onda del test 340 e 700 nm per l’emoglobina A1c
405 e 700 nm per l’emoglobinaTipo di misurazione Turbidimetrica per l’emoglobina A1c
Colorimetrica per l’emoglobina
CalibrazioneLa procedura di calibrazione generale è descritta nel Manuale Operatore di Dimension®.
Nota: i reagenti e i calibratori Flex® per A1C sono confezionati in un kit. Ogni lotto di kit contiene serie complementari di cartucce reagenti A1C Flex® e calibratori per A1C. Non utilizzare in maniera intercambiabile reagenti con numeri di lotto diversi.
Il sistema esegue automaticamente la calibrazione sia per Hb sia per HbA1c.
Prima della calibrazione, il metodo emoglobina A1C Dimension® richiede l’inserimento degli scaler specifici per il lotto nella schermata Calibration Set Up (Preparazione della calibrazione). I valori degli scaler sono indicati sulla confezione della cartuccia reagente Flex®. Questi scaler vengono applicati a tutti i risultati CQ e dei pazienti per mantenere l’accuratezza. La mancata indicazione di scaler specifici per il lotto comporterà risultati non accurati.
Il metodo A1C offre due opzioni per la calibrazione e la refertazione dei risultati.
Opzione 1:
• Risultati refertati in HbA1c percentuale utilizzando la seguente equazione:
%HbA1c = 100 xHbA1c (g/dL)
Hb (g/dL)
• Per l’emoglobina A1c e l’emoglobina totale sono necessari i valori del calibratore (g/dL). Tali valori sono disponibili nella tabella dei valori assegnati contenuta nelle Istruzioni per l’uso (IFU) del calibratore emoglobina per A1C Dimension®.
• Successivamente il sistema di chimica clinica Dimension® calcola il risultato dell’HbA1c percentuale, standardizzato secondo NGSP, in base al metodo di calcolo illustrato di seguito. Questo calcolo fornisce un valore percentuale dell’HbA1c standardizzato sui risultati dello studio DCCT, che viene stampato sul referto di Dimension®. I valori dei coefficienti dei polinomi (b, c, d) possono variare in base al lotto di cartucce analitiche Flex®.
NGSP standardizzato %HbA1c = (b x (%HbA1c)2) + (c x %HbA1c) + d
I lotti A1C sono prodotti in condizioni controllate in modo da soddisfare le specifiche stabilite per il prodotto. Annualmente si analizza un lotto su ogni modello di Dimension® per verificarne la rispondenza al Programma nazionale di standardizzazione della glicoemoglobina (National Glycohemoglobin Standardization Program, NGSP). È possibile accedere alle copie dei certificati dal sito www.siemens.com/diagnostics. Ulteriori informazioni sulla certificazione NGSP sono disponibili sul sito web www.ngsp.org.9
Opzione 2:
• Risultati refertati in unità SI [mmol/mol]h utilizzando la seguente equazione:
mmol/mol HbA1c = 1000 xHbA1c (mmol/L)
Hb (mmol/L)
• Per l’emoglobina A1c e l’emoglobina totale sono necessari i valori del calibratore (mmol/L). Tali valori sono disponibili nella tabella dei valori assegnati contenuta nelle IFU del calibratore emoglobina per A1C Dimension®.
• Successivamente il sistema Dimension® calcola il risultato del metodo A1C in mmol/mol, standardizzato secondo l’IFCC, in base al metodo di calcolo illustrato di seguito. Questo calcolo fornisce un valore dell’HbA1c in mmol/mol standardizzato sui risultati del sistema di riferimento dell’IFCC,9 che viene stampato sul referto di Dimension®. I valori dei coefficienti dei polinomi (b, c, d) possono variare in base al lotto di cartucce analitiche Flex®.
IFCC standardizzato HbA1c (mmol/mol) = (b x (HbA1c mmol/mol)2) + (c x HbA1c mmol/mol) + d
h. Le unità SI (Système International d’Unités) sono tra parentesi.
Materiale di calibrazione Calibratori secondari quali i calibratori per A1CSchema di calibrazione 2 livelli, n = 5 per Hbi
0,25–2,90 g/dL [0,16–1,80 mmol/L] HbA1cFrequenza di calibrazione Ogni 30 giorni per ciascun lottoOccorre effettuare una nuova calibrazione • Per ogni nuovo lotto di cartucce reagenti Flex®
• In seguito a manutenzione o riparazione importante, se indicato dai risultati del controllo qualità
• Se indicato nelle procedure del controllo qualità del laboratorio• Quando richiesto in base alle normative in vigore
Scaler Consultare la confezione della cartuccia reagente Flex® per i valori degli scaler specifici per il lotto.
Le coppette di calibrazione devono essere riempite con 600 µL di calibratore.i. I risultati della calibrazione per HbA1c vengono visualizzati automaticamente; fare riferimento al report della
calibrazione per i risultati della calibrazione per Hb.
Criteri di accettazione della calibrazione
Il metodo emoglobina A1C Dimension® richiede la conferma di ulteriori linee guida relative alla calibrazione; dopo aver completato la calibrazione, assicurarsi che i seguenti criteri siano soddisfatti:
Dati Linee guida di accettazione Commenti
Pendenza emoglobina A1c (A1C) (m) 0,95–1,05 N/A
Intercetta y emoglobina A1c (A1C) (b) Prossima allo 0 Non significativa clinicamente
Accuratezza emoglobina (HB BV) (g/dL [mmol/L])
Media ± 10%Fare la media dei risultati dei 5 report e confrontarli con i dati HB BV
Emoglobina (HB BV) SD (g/dL [mmol/L])
≤ 0,8 (0,5) N/A
Linee guida SD sulla riproducibilità del coefficiente “EX” < 0,4 (0,6)
Un riflesso della precisione dei valori di milliassorbanza dell’emoglobina totale individuale utilizzato per il calcolo del coefficiente “EX”.
Controllo qualitàPer la frequenza dei controlli qualità seguire le normative in vigore o i requisiti di accreditamento. Almeno una volta per ogni giorno di utilizzo, analizzare due livelli di un materiale di controllo qualità (CQ) con concentrazioni note di emoglobina A1c. Seguire le procedure di controllo qualità interne del laboratorio se i risultati ottenuti non rientrano nei limiti accettabili.
Nota: è importante valutare i requisiti di utilità medica locali o regionali quando si stabiliscono limiti accettabili per il controllo qualità (ad esempio il College of American Pathologists (CAP), il Deutschen Gesellschaft für Klinische Chemie und Laboratoriumsmedizin (DGKL) e altri).
Risultati: il sistema Dimension® calcola automaticamente le concentrazioni di A1c, Hb e HbA1c totali utilizzando lo schema di calcolo illustrato nella Manuale Operatore di Dimension®.
Il sistema referta i risultati in una singola unità (% o mmol/mol); per convertire manualmente l’unità di refertazione con l’IFCC NGSP “Equazione master” o l’NGSP IFCC “Equazione master” raccomandata dalla International Federation for Clinical Chemistry Subcommittee sulla standardizzazione dell’emoglobina A1c,10,11 utilizzare le equazioni riportate di seguito:
I risultati di questo test devono essere sempre interpretati alla luce dell’anamnesi del paziente, della presentazione clinica e valutando contestualmente l’esito di altri accertamenti.
I valori degli analiti Hb e HbA1c possono essere misurati direttamente dal campione senza alcuna diluizione o pretrattamento che non sia parte integrante del processo di analisi abituale. I valori degli analiti Hb e HbA1c al di fuori degli intervalli riportati sopra generano un messaggio sul referto del test accanto al risultato del rapporto HbA1c calcolato.
L’intervallo del rapporto HbA1c calcolato è stato validato da Siemens utilizzando campioni di sangue intero nativo. Questo intervallo può essere utilizzato per la convalida di laboratorio dell’AMR, se necessario.
I campioni con risultati superiori al 14,0% [130 mmol/mol], 25 g/dL [15,5 mmol/L] emoglobina o 2,90 g/dL [1,80 mmol/L] di HbA1c verranno refertati come “Superiore all’intervallo di misura” e quindi devono essere diluiti e rianalizzati. Se il messaggio persiste per il campione diluito, refertare il risultato come “Superiore al 14,0% [130 mmol/mol]”.
Diluizione manuale: miscelare una parte di acqua reagente per laboratorio clinico (CLRW) e una parte di sangue intero ben miscelato. Rianalizzare la miscela di diluizione per ottenere risultati compresi nell’intervallo di misura analitica.
Importante
La lettura risultante (%HbA1c [mmol/mol]) è il risultato accettabile. Il risultato non deve essere corretto in base alla diluizione, in quanto è stato calcolato in base al rapporto tra HbA1c e Hb. Pertanto, nel metodo emoglobina A1C Dimension® non deve essere utilizzato alcun fattore di diluizione.
Autodiluizione (AD): Non disponibile con questo metodo.
Campioni con risultati inferiori al 3,8% [18 mmol/mol], emoglobina inferiore a 5,0 g/dL [3,1 mmol/L] o HbA1c inferiore a 0,25 g/dL [0,16 mmol/L] saranno refertati dallo strumento come “Inferiore all’intervallo di misura”. Dispensare una nuova aliquota di 200 µL di sangue intero e rianalizzare il campione. Se il messaggio persiste, contattare il fornitore dell’assistenza.
Il sistema di refertazione dello strumento contiene avvisi e commenti per fornire all’utente informazioni sugli errori di analisi dello strumento, informazioni sullo stato dello strumento e i potenziali errori nei risultati del metodo A1C. Per il significato di avvisi e commenti nei referti fare riferimento al Manuale Operatore di Dimension®.
La seguente precisione con 5 test† indica la possibilità di un cattivo funzionamento del sistema:
Concentrazione A1c % [mmol/mol]
SD % [mmol/mol]
5,5 [37] > 0,2 [1,6]9,6 [81] > 0,3 [4,3]
† La coppetta per campioni deve essere riempita con 200 µL per lo studio di precisione con 5 test.
Limiti della procedura
AVVERTENZAIl metodo emoglobina A1C Dimension® presenta una significativa interferenza con l’emoglobina fetale (HbF). I campioni contenenti HbF possono produrre un bias negativo (inferiore ai risultati effettivi) con il metodo emoglobina A1C Dimension®. I risultati dell’emoglobina A1c non sono validi per i pazienti con quantità anomale di HbF, compresi quelli con nota persistenza ereditaria di emoglobina fetale. Per ulteriori informazioni sull’intereferenza della variante dell’HbF, fare riferimento alle Sostanze interferenti.
Non utilizzare i calibratori emoglobina per A1C Dimension® per testare la precisione.
Come per qualunque altra procedura di laboratorio, grandi discordanze fra l’impressione clinica e i risultati del test di solito rendono necessari ulteriori approfondimenti. Tenere in considerazione alcune delle seguenti limitazioni del test:
Il metodo emoglobina A1C Dimension® è progettato esclusivamente per la misurazione accurata e precisa di HbA1c in mmol/mol (IFCC) e %HbA1c (DCCT/NGSP). I singoli risultati per la concentrazione totale di Hb e HbA1c non vengono refertati.
I pazienti con concentrazioni di emoglobina non comprese nell’intervallo accettabile per il metodo emoglobina A1C Dimension® devono essere analizzati con un metodo che impiega un principio di test diverso.
Il metodo emoglobina A1C Dimension® non deve essere utilizzato per diagnosticare il diabete durante la gravidanza. L’emoglobina A1c riflette i livelli medi di glucosio nel sangue nei 3 mesi precedenti (la durata media di un globulo rosso) e pertanto può essere falsamente bassa durante la gravidanza o qualsiasi altra condizione associata a insorgenza di iperglicemia e/o a riduzione della sopravvivenza dei globuli rossi.
Il metodo emoglobina A1C Dimension® non deve essere utilizzato per diagnosticare o monitorare il diabete in pazienti affetti dalle seguenti condizioni: emoglobinopatie, ad eccezione di quanto dimostrato di produrre prestazioni accettabili (come il tratto falciforme), turnover anomalo dei globuli rossi nel sangue (come, anemie da emolisi e carenza di ferro), neoplasie e malattia epatica e renale cronica grave.
Nei casi di diabete di tipo 1 in rapida evoluzione, l’aumento dei valori dell’HbA1c potrebbe essere ritardato rispetto all’aumento acuto delle concentrazioni di glucosio. In tali condizioni, il diabete mellito deve essere diagnosticato sulla base delle concentrazioni di glucosio nel plasma e/o dei sintomi clinici tipici.
Per i pazienti affetti da diabete di tipo 1, i pazienti pediatrici o le donne in gravidanza, questo test non deve sostituire il test del glucosio.
Qualunque causa di riduzione della sopravvivenza dei globuli rossi nel sangue (ad esempio, anemia emolitica o altre malattie emolitiche, gravidanza o recente significativa perdita di sangue) ridurrà l’esposizione dei globuli rossi al glucosio con una conseguente diminuzione dei valori di HbA1c. I risultati dell’HbA1c non sono affidabili in pazienti che presentano perdite di sangue croniche e una conseguente variabilità del periodo di vita degli eritrociti.12–15
Valori attesi:
L’intervallo di riferimento relativo all’HbA1c è indicato nella seguente tabella.16
I valori di emoglobina A1c in soggetti sani possono variare a seconda delle diverse popolazioni di riferimento. Ogni laboratorio deve verificare la validità dell’intervallo di riferimento e stabilire, se necessario, un intervallo proprio.
La frequenza del test dell’HbA1c deve dipendere dalla situazione clinica, dal regime di trattamento e dal parere medico. L’American Diabetes Association raccomanda che un obiettivo ragionevole relativo all’HbA1c per molte pazienti adulte non incinte è < 7%. Obiettivi meno rigidi relativi all’HbA1c possono essere appropriati per alcuni pazienti affetti da diabete ed esposti ad altri fattori di rischio, quali ipoglicemia grave o diffuse condizioni di comorbilità.17
Sostanze interferenti
Varie sostanze oltre agli zuccheri possono formare aggregati con l’emoglobina e potenzialmente interferire con il test dando luogo a falsi risultati. Ciò avviene ad esempio negli individui con dipendenza dagli oppiacei,18 avvelenamento da piombo e alcolismo.12
Il reagente anticorpo utilizzato nel metodo emoglobina A1C Dimension® misura le varianti dell’emoglobina glicosilata che vengono glicate in corrispondenza dell’N terminale della catena beta con epitopi identici a quelli dell’HbA1c (sequenza di amminoacidi: VAL-HIS-LEU-THR). Fra questi figurano HbS, HbC, HbD e HbE. Altre emoglobinopatie possono dare luogo a risultati errati con questo test. È necessario interpretare con cautela qualsiasi risultato dell’HbA1c in pazienti con varianti dell’Hb. Valori anomali delle emoglobine possono influire sull’emivita dei globuli rossi o sulle percentuali di glicazione in vivo. In questi casi, seppure corretti da un punto di vista analitico, i risultati non rappresentano lo stesso livello di controllo glicemico che ci si aspetterebbe in pazienti con emoglobina normale.14
L’HbF (emoglobina fetale) glicata, costituita da due catene alfa e due catene gamma, non viene riconosciuta dall’anticorpo anti-HbA1c. I soggetti con livelli elevati di HbF (> 10%), riscontrati comunemente nei neonati e nei pazienti con beta talassemia, possono produrre risultati inferiori al previsto con questo test. Tali campioni devono essere rianalizzati con un metodo alternativo.
Non sono state osservate cross-reazioni fra gli anticorpi anti-HbA1c utilizzati in questo kit e HbA0, HbA1a, HbA1b, emoglobina acetilata, emoglobina carbamilata e HbA1c labile.
Caratteristiche specifiche di prestazione
I seguenti dati rappresentano le prestazioni tipiche del sistema Dimension®. I risultati effettivi ottenuti dai singoli laboratori possono differire in base al disegno dello studio.
PrecisioneIl test di precisione è stato eseguito in conformità al documento CLSI EP05-A3.19 Il test è stato condotto nel corso di un periodo di 20 giorni utilizzando 3 strumenti e 3 lotti di reagente su ogni strumento. Durante ogni giorno di esecuzione del test, sono state eseguite 2 analisi (con un lasso di tempo di 2 ore tra un test e l’altro).
j. Deviazione standardk. Coefficiente di variazione
Confronto dei metodiIl test di confronto dei metodi è stato eseguito in conformità al documento CLSI EP09-A3.20 I risultati del metodo emoglobina A1C Dimension® (y) sono stati confrontati con i risultati ottenuti utilizzando un metodo di test standardizzato NGSP (HPLC) (x).
Regressione Passing-Bablok
Unità N Intervallo campione Pendenza IC al 95% Intercetta y IC al 95%%HbA1c 147 4,5–13,2 0,983 0,966–1,001 0,030 -0,095–0,144mmol/mol 147 26–121 0,973 0,955–0,992 0,437 -0,474–1,450
Unità N Intervallo campione Pendenza IC al 95% Intercetta y IC al 95%%HbA1c 147 4,5–13,2 0,978 0,957–1,000 0,052 -0,094–0,198mmol/mol 147 26–121 0,970 0,948–0,992 0,532 -0,603–1,666
I dati del confronto dei metodi sono stati valutati utilizzando l’analisi Bland-Altman del bias,21 che rappresenta l’approccio impiegato dall’NGSP. Vengono forniti la differenza media tra il metodo A1C e il metodo di rete NGSP (HPLC) e gli intervalli di confidenza al 95% delle differenze nell’intervallo dal 4 al 10% di HbA1c. Il 95% delle differenze tra i valori ottenuti per i singoli campioni con entrambi i metodi rientra nell’intervallo definito dall’intervallo di confidenza al 95% inferiore e da quello superiore delle differenze
Siemens Healthcare Diagnostics Inc.500 GBC DriveNewark, DE 19714 USA
2019
-10
C P
N 11
2752
89 -
IT
Confronto anticoagulantiIl test di equivalenza per 5 anticoagulanti è stato eseguito in conformità al documento CLSI EP09-A3.20 Il test è stato eseguito utilizzando un lotto di reagenti e una singola ripetizione da una serie complementare di ciascuno dei 4 anticoagulanti (K3 EDTA; fluoruro di sodio/Na2 EDTA; litio eparina e Na fluoruro/K-ossalato) e campioni di EDTA K2.
Regressione Passing-Bablok: NGSP (%)
Anticoagulante Campioni di confronto (x) Pendenza IC al 95% Intercetta y IC al 95%
Na floruro/K-ossalato K2 EDTA 1,007 0,989–1,025 -0,032 -1,22–1,16
Numero di campioni (N) = 79Intervallo campione (mmol/mol) = 28–125
Specificità
Sostanze non interferenti
I test di interferenza sono stati eseguiti in conformità al documento CLSI EP07-A2.22
Le seguenti sostanze non interferiscono con il metodo emoglobina A1C Dimension® se presenti nel sangue intero alle concentrazioni indicate. Le imprecisioni sistematiche (bias) dovute a queste sostanze sono inferiori o pari al 5% a concentrazioni di emoglobina A1c del 6,5% ± 1,0% e dell’8,0% ± 1,0% (inferiori o uguali all’8% a 48 mmol/mol ± 11 mmol/mol e 64 mmol/mol ± 11 mmol/mol).
Interferente Concentrazione interferente Unità comuni
Varianti emoglobinaI test di interferenza per determinare l’effetto delle varianti di emoglobina sul metodo emoglobina A1C Dimension® sono stati eseguiti in conformità al documento CLSI EP07-A2.22 Non sono stati osservati bias significativi di interferenza per HbC, HbD, HbE e HbA2. Sono stati osservati bias di interferenza significativi per HbF.
Emoglobine derivateI test di interferenza per determinare l’effetto dei derivati dell’emoglobina, inclusi l’emoglobina acetilata, l’emoglobina carbamilata, l’emoglobina labile e le frazioni di emoglobina sul metodo emoglobina A1C Dimension® sono stati eseguiti in conformità al documento CLSI EP07-A2.22 Le imprecisioni (bias) dovute a queste sostanze sono inferiori o uguali al 5% a concentrazioni di emoglobina A1c del 5,0% ± 1,0%, 6,5% ± 1,0% e 8,0% ± 1,0% (inferiori o uguali al 9% a 31 mmol/mol ± 11 mmol/mol, 48 mmol/mol ± 11 mmol/mol e 64 mmol/mol ± 11 mmol/mol). • Emoglobina acetilata con una quantità maggiore o uguale a 50 mg/dL (2,8 mmol/L) di acido acetilsalicilico • Emoglobina carbamilata con una quantità maggiore o uguale a 10 mmol/L di cianato • Emoglobina labile con una quantità maggiore o uguale a 1500 mg/dL (83,3 mmol/L) di glucosio
Limite di rilevazione e limite del biancoIl limite di rilevazione (LoD) e il limite del bianco (LoB) sono stati determinati secondo quanto descritto nel documento CLSI EP17-A2.23
Il LoB è il risultato della misurazione massima che è possibile osservare su un campione bianco. Il LoB è stato determinato utilizzando 60 determinazioni con 5 campioni bianchi ciascuno per tHb e 75 determinazioni con 5 campioni bianchi ciascuno per %HbA1c/HbA1c.
Il LoD corrisponde alla concentrazione più bassa di HbA1c o tHb che può essere rilevata con una probabilità del 95%. Il LoD è stato determinato utilizzando 60 determinazioni, con 5 campioni di livello basso ciascuno per tHb e 75 determinazioni con 5 campioni bassi ciascuno per %HbA1c/HbA1c.
Di seguito vengono mostrati LoB e LoD per il metodo emoglobina A1C Dimension®.
Consulte las secciones sombreadas: Información actualizada desde la versión de 2019-04. Fecha de la edición 2019-10
Dimension® clinical chemistry system
A1CFlex® reagent cartridge
DF105B
Ensayo de hemoglobina A1CUso previsto: El ensayo de hemoglobina A1C Dimension® es un ensayo de diagnóstico in vitro para la determinación cuantitativa del %HbA1c (DCCT/NGSP) y mmol/mol de HbA1c (IFCC) en sangre total venosa anticoagulada humana para uso con el sistema de química clínica Dimension®. La medición de la hemoglobina A1c se utiliza como ayuda en el diagnóstico y la monitorización del control de la glucosa en sangre a largo plazo en pacientes con diabetes mellitus y como ayuda para la identificación de pacientes en riesgo de padecer diabetes mellitus.
Resumen: HbA1c se refiere al producto de una reacción no enzimática entre la glucosa y la hemoglobina A1. El eritrocito humano es totalmente permeable a la glucosa, que se puede combinar de manera no enzimática con la hemoglobina para formar HbA1c. Esta reacción no enzimática entre el grupo alfa-amino de la valina N-terminal de la cadena beta de la hemoglobina y la glucosa forma una aldimina inestable o producto intermedio de base de Schiff (fracción lábil). Esta reacción es lenta y reversible y se produce a una velocidad proporcional a la concentración de glucosa en sangre. El producto intermedio de aldimina sufre posteriormente una reordenación irreversible de Amadori para formar el producto cetoamina 1-glucofrutovalina. Dado que la reacción depende de la concentración de los reactantes, el grado de glucosilación (registrado como HbA1c con respecto al total de hemoglobina) es proporcional a la concentración media de glucosa en sangre respecto al intervalo de vida circulante de la hemoglobina en el glóbulo rojo (aproximadamente 120 días)1,2.
La utilidad de las medidas de HbA1c se demostró en el Ensayo de control y complicaciones de la diabetes (DCCT)3. Un importante descubrimiento de este estudio fue la correlación directa que existe entre el control glucémico y la respuesta del paciente con respecto a las complicaciones a largo plazo sufridas por el paciente. Los pacientes con un mejor control glucémico (es decir, una menor HbA1c) mostraron un pronóstico considerablemente mejor con respecto a las complicaciones microvasculares, incluida la neuropatía, la retinopatía y la nefropatía3.
Principios del procedimiento: El ensayo de hemoglobina A1C Dimension® mide la hemoglobina total y HbA1c. La medición de HbA1c se basa en el principio del inmunoensayo de inhibición turbidimétrico (TINIA) y la medición de la hemoglobina total se basa en una modificación de la reacción de hematina alcalina. A partir de los valores obtenidos para cada uno de estos dos analitos, se calcula y registra la proporción relativa de glucohemoglobina respecto a la hemoglobina total. No es necesario realizar un pretratamiento para retirar la fracción lábil, ya que únicamente se detecta la forma de HbA1c que ha sufrido la reordenación de Amadori. Este análisis mide todas las variantes de la hemoglobina que están glicadas en el N-terminal de la cadena beta y tienen epítopos idénticos al de la HbA1c.
Medición de la hemoglobina total: Se añade una muestra de sangre total a la primera cubeta, que contiene el reactivo lisante. Este reactivo lisa los glóbulos rojos y convierte simultáneamente la hemoglobina liberada en un derivado que tiene un espectro de absorbancia característico. A continuación, una alícuota de la sangre total lisada se transfiere de la primera cubeta a una segunda cubeta donde se mide la concentración de hemoglobina total a 405 nm y 700 nm4.
sangre total + agente lisante Hemoglobina liberada derivado de la hemoglobina (medido a 405 nm)
Medición de hemoglobina A1c: La misma alícuota de sangre total lisada que se ha transferido de la primera cubeta a la segunda cubeta para la medición de Hb también se utiliza para la medición de HbA1c. La segunda cubeta contiene un anticuerpo anti-HbA1c en un reactivo tamponado. La hemoglobina A1c de la muestra reacciona con el anticuerpo anti-HbA1c para formar un complejo soluble antígeno-anticuerpo. A continuación, se añade a esta cubeta un reactivo polihapteno que contiene varios epítopos HbA1c. El polihapteno reacciona con el exceso de anticuerpos (libres) anti-HbA1c y forma un complejo insoluble anticuerpo-polihapteno. La velocidad de esta reacción se mide por turbidimetría a 340 nm y en blanco a 700 nm, y es inversamente proporcional a la concentración de HbA1c en la muestra.
anticuerpo anti-HbA1c (exceso) + polihapteno Complejo Ab/polihapteno(absorbe a 340 nm)
Componentes del kit de A1C
Nota: Cada lote del kit contiene juegos emparejados de cartuchos de reactivos A1C Flex® y calibradores. Estos componentes no son intercambiables entre kits con números de lote diferentes.
Reactivos
Pocillosa Forma Ingrediente Concentraciónb Origen1–2 Líquido Anticuerpo ≥ 0,5 mg/mlc Carnero, policlonal de suero ovino
a. Los pocillos están numerados consecutivamente desde el extremo ancho del cartucho.b. Valor nominal por pocillo en un cartucho.c. El título de anticuerpos y la actividad del conjugado (o la concentración de reactivo de partículas) pueden variar
de un lote a otro.d. MES = ácido sulfónico 2-morfolinoetanoe. TRIS = tris(hidroximetil)-aminometanof. TTAB = bromuro de tetradeciltrimetilamonio
Riesgos y seguridad:H412P273, P501
¡Advertencia!Nocivo para los organismos acuáticos, con efectos nocivos duraderos.
Evitar su liberación al medio ambiente. Eliminar el contenido y el recipiente de acuerdo con las normativas locales, regionales y nacionales
Contiene: 2-metil-H4-isotiazol-3-ona
Las fichas de datos de seguridad (MSDS/SDS) están disponibles en siemens.com/healthcare
Precauciones: Las cubetas usadas contienen fluidos corporales humanos, por lo que deben manipularse con cuidado para evitar la ingestión o el contacto con la piel.
Precaución: La legislación federal de EE. UU. restringe la venta de este dispositivo a profesionales sanitarios o bajo orden de los mismos.
Para uso diagnóstico in vitro
Nota: Los calibradores y cartuchos de reactivos A1C Flex® se envasan juntos en un kit. Cada lote del kit contiene juegos emparejados de cartuchos de reactivos A1C Flex® y calibradores A1C. No intercambie reactivos con diferentes números de lote.
Preparación del reactivo: Todos los reactivos son líquidos y están listos para su uso.
Conservar a: 2–8°C
Caducidad: Consulte la fecha de caducidad del kit en el envase. Todos los componentes de kit son estables hasta la fecha de caducidad si se conservan sin abrir a 2–8°C. En el instrumento, los pocillos sellados del cartucho son estables durante 30 días.
Estabilidad de los pocillos abiertos: 5 días para los pocillos 1–2 y 5–6 10 días para el pocillo 3
Recogida de muestras y manipulación: Tipo de muestra recomendado: Sangre total venosa anticoagulada (K2 EDTA; K3 EDTA; fluoruro sódico/Na2 EDTA; heparina de litio o fluoruro sódico/oxalato de potasio).
Las muestras deben obtenerse utilizando los procedimientos recomendados para la obtención de muestras de sangre para diagnóstico mediante venopunción5–7. Siga las instrucciones de uso y procesamiento suministradas con el dispositivo de recogida de muestras6.
• Las muestras para el método A1C solo pueden analizarse desde una copa de muestra o SSC. • No se pueden analizar las muestras directamente desde los tubos de recogida principales. • Las muestras deben mezclarse suavemente mediante inversión (invierta el tubo con cuidado diez veces)
o en un agitador antes de pipetearlas en la copa de muestra o en un SSC para obtener una distribución uniforme de los eritrocitos antes del análisis. Evite que se forme espuma.
• No se deben utilizar muestras que contengan coágulos.• Pipetee 200 µl de la muestra de sangre total en la copa de muestra o SSC.• La muestra puede permanecer en una copa de muestra en el instrumento durante un máximo de
una hora.
Estabilidad de las muestras: Las muestras son estables cuando se almacenan durante un periodo que no supere8:
3 días a 15–25°C 7 días a 2–8°C 4 meses a -20°C (congelar una única vez)
Esta información sobre el almacenamiento de muestras se proporciona con fines orientativos; sin embargo, los usuarios pueden validar sus propios procedimientos para almacenar muestras.
Procedimiento
Materiales suministradosKit de A1C, ref. DF105B: incluye cartuchos de reactivos A1C Flex® y un calibrador de A1C (5 niveles)
Materiales necesarios pero no suministradosMateriales de control de calidad
Proceso del análisis
El sistema de química clínica Dimension® realiza de manera automática el muestreog, la dispensación de reactivos, la mezcla y el procesamiento. Para más detalles sobre este proceso, consulte el Manual del usuario del sistema Dimension®.
g. El cubilete de la muestra debe contener de 200 μl de sangre total para garantizar una mezcla adecuada.
Condiciones del análisis
Cubeta 1 Cubeta 2Volumen de la muestra 3 µl
(de la copa de muestra)19 µl(de la cubeta 1)
Volumen de reactivo hemolizante 300 µl 0 µlVolumen de anticuerpo/tampón 0 µl 320 µlVolumen de polihapteno 0 µl 52 µlVolumen de diluyente 147 µl 69 µlTemperatura 37°C 37°CLongitud de onda de análisis 340 y 700 nm para la hemoglobina A1c
405 y 700 nm para la hemoglobinaTipo de medición Turbidimétrica para la hemoglobina A1c
Colorimétrica para la hemoglobina
CalibraciónEn el Manual del usuario del sistema Dimension® se describe el procedimiento general de calibración.
Nota: Los calibradores y cartuchos de reactivos A1C Flex® se envasan juntos en un kit. Cada lote del kit contiene juegos emparejados de cartuchos de reactivos A1C Flex® y calibradores A1C. No intercambie reactivos con diferentes números de lote.
El sistema realiza automáticamente la calibración de Hb y HbA1c.
El ensayo de hemoglobina A1C Dimension® requiere ajustes de escala específicos para cada lote que deben introducirse en la pantalla Calibration Set Up (Configuración calibración) antes de la calibración. Los valores de los ajustes de escala están indicados en el envase del cartucho de reactivo Flex®. Dichos ajustes de escala se aplican a todos los resultados de paciente y de control de calidad para mantener la precisión. Si no se introducen los ajustes de escala específicos para cada lote, los resultados serán inexactos.
El método A1C ofrece dos opciones para realizar la calibración y registrar los resultados.
Opción 1:
• Los resultados pueden registrarse como %HbA1c utilizando la siguiente ecuación:
%HbA1c = 100 xHbA1c (g/dl)
Hb (g/dl)
• Son necesarios los valores del calibrador (g/dl) correspondientes a la hemoglobina A1c y la hemoglobina total. Estos valores pueden consultarse en la tabla de valores asignados que se incluye junto con las instrucciones de uso (IFU) del calibrador de hemoglobina A1C para el sistema Dimension®.
• A continuación, el sistema de química clínica Dimension® calcula un resultado estandarizado de %HbA1c según el NGSP basado en el cálculo que se indica a continuación. Este cálculo proporciona un valor de %HbA1c que se estandariza según el resultado del estudio DCCT, que es el que se imprime en el informe de Dimension®. Los valores de los coeficientes polinómicos (b, c y d) pueden variar según el lote de cartuchos de reactivos Flex®.
%HbA1c estandarizado según NGSP = (b x (%HbA1c)2) + (c x %HbA1c) + d
Los lotes de A1C se fabrican en condiciones controladas para cumplir las especificaciones del producto establecidas. Todos los años, se analiza un lote en cada modelo de Dimension® para confirmar la estandarización con el National Glycohemoglobin Standardization Program (NGSP). Puede consultar las copias de los certificados en www.siemens.com/diagnostics. Se puede obtener información adicional acerca de la certificación NGSP en www.ngsp.org9.
Opción 2:
• Los resultados pueden registrarse en unidades del SI [mmol/mol]h utilizando la siguiente ecuación:
mmol/mol HbA1c = 1000 xHbA1c (mmol/l)
Hb (mmol/l)
• Son necesarios los valores del calibrador (mmol/l) correspondientes a la hemoglobina A1c y la hemoglobina total. Estos valores pueden consultarse en la tabla de valores asignados que se incluye junto con las instrucciones de uso (IFU) del calibrador de hemoglobina A1C para el sistema Dimension®.
• A continuación, el sistema Dimension® calcula un resultado de A1C en mmol/mol estandarizado según la IFCC basado en el cálculo que se indica a continuación. Este cálculo proporciona un valor de HbA1c en mmol/mol que está estandarizado según el sistema de referencia de la IFCC9, que es el que se imprime en el informe de Dimension®. Los valores de los coeficientes polinómicos (b, c y d) pueden variar según el lote de cartuchos de reactivos Flex®.
HbA1c estandarizado según IFCC (mmol/mol) = (b x (HbA1c mmol/mol)2) + (c x HbA1c mmol/mol) + d
h. Las unidades del Sistema Internacional de Unidades [unidades SI] se indican entre corchetes.
Material de calibración Calibradores secundarios como calibradores de A1CEsquema de calibración 2 niveles, n = 5 para Hbi
0,25–2,90 g/dl [0,16–1,80 mmol/l] HbA1cFrecuencia de calibración Cada 30 días para cualquier loteSe requiere una nueva calibración • Para cada lote nuevo de cartuchos de reactivos Flex®
• Después de la realización de importantes tareas de mantenimiento o servicio, si los resultados de control de calidad así lo indican
• Tal como se indica en los procedimientos de control de calidad del laboratorio• Cuando es obligatorio según las reglamentaciones gubernamentales
Ajustes de escala Ver envase del cartucho de reactivo Flex® para conocer los valores de ajuste de escala específicos para el lote.
Las copas de calibración deben llenarse con 600 µl de calibrador.i. Los resultados de calibración para HbA1c se muestran automáticamente, consulte el informe de calibración para ver
los resultados de la calibración de Hb
Criterios de aceptación de la calibración
El ensayo de hemoglobina A1C Dimension® requiere la confirmación de pautas para la calibración adicionales. Una vez realizada la calibración, compruebe que se cumplen los siguientes criterios:
Datos Pauta de aceptación ObservacionesPendiente de hemoglobina A1c (A1C) (m) 0,95–1,05 N/A
Intersección Y de hemoglobina A1c (A1C) (b)
Cerca de 0 No significativo clínicamente
Precisión de hemoglobina (HB BV) (g/dl [mmol/l])
Media ± 10%Obtenga un promedio de los 5 resultados del informe y compárelo con los datos de HB BV
DE de hemoglobina (HB BV) (g/dl [mmol/l])
≤ 0,8 (0,5) N/A
Pautas de desviación estándar de reproducibilidad del coeficiente “EX” < 0,4 (0,6)
Reflejo de la precisión de los valores de miliabsorbancia de hemoglobina total individual para el cálculo del coeficiente de calibración “EX”.
Control de calidadSiga las reglamentaciones gubernamentales o los requisitos de acreditación relativos a la frecuencia de control de calidad. Al menos una vez por día de uso, analice dos niveles de un material de control de calidad (CC) con concentraciones conocidas de hemoglobina A1c. Siga los procedimientos internos de CC de su laboratorio si los resultados obtenidos no se encuentran dentro de los límites aceptables.
Nota: Es importante tener en cuenta los requisitos de utilidad médica locales o regionales a la hora de establecer límites aceptables del control (por ejemplo, College of American Pathologists (CAP), Deutschen Gesellschaft für Klinische Chemie und Laboratoriumsmedizin (DGKL) y otros).
Resultados: El sistema Dimension® calcula automáticamente las concentraciones de A1c, Hb y HbA1c total según el esquema de cálculo ilustrado en el Manual del usuario del sistema Dimension®.
El sistema registra los resultados en una sola unidad (% o mmol/mol). Para convertir manualmente esta unidad de registro con la “ecuación maestra” de IFCC NGSP o la “ecuación maestra” de NGSP IFCC recomendada por el subcomité sobre estandarización de la hemoglobina A1c de la Federación internacional de química clínica10,11, utilice las ecuaciones que se indican a continuación:
IFCC NGSP: %HbA1c = 0,09148 (mmol/mol de HbA1c) + 2,152%
Los resultados de esta prueba deberán interpretarse siempre de acuerdo con la historia clínica del paciente, la sintomatología clínica y otras observaciones.
Rango de medición analítico (AMR): Hb: 5,0–25,0 g/dl [3,1–15,5 mmol/l] HbA1c: 0,25–2,90 g/dl [0,16–1,80 mmol/l]
Proporción calculada de HbA1c (A1C): 3,8–14,0% [18–130 mmol/mol]
Los valores de los analitos Hb y HbA1c pueden medirse directamente a partir de la muestra sin dilución o tratamiento previo que no forme parte del proceso analítico normal. Los valores de los analitos Hb y HbA1c que estén fuera de los rangos anteriores generarán un mensaje de informe de prueba para que aparezca con el resultado de proporción calculada de HbA1c.
Siemens ha validado el rango de proporción calculada de HbA1c utilizando muestras de sangre total nativas. Este rango se puede usar para la validación en laboratorio del AMR, si fuera necesario.
Las muestras con resultados que superen el 14,0% [130 mmol/mol], 25 g/dl [15,5 mmol/l] de hemoglobina o 2,90 g/dl [1,80 mmol/l] de HbA1c se registrarán como “superiores al intervalo del ensayo” y deberán repetirse con dilución. Si el mensaje vuelve a aparecer con la muestra diluida, registre el resultado como “superior a 14,0% [130 mmol/mol]”.
Dilución manual: Mezcle una parte de agua para reactivos para laboratorios clínicos (CLRW) y una parte de sangre total bien mezclada. Vuelva a analizar la mezcla diluida para obtener resultados dentro del rango de medición analítico.
Importante
La lectura resultante (%HbA1c [mmol/mol]) es el resultado que se incluye en el informe. No hay que introducir una corrección por la dilución en el resultado, ya que este resultado se calcula sobre la base de la relación entre HbA1c y Hb. Por tanto, no debe utilizarse un factor de dilución en el ensayo de hemoglobina A1C Dimension®.
Autodilución (AD): No disponible para este método.
El intervalo registrará las muestras con resultados inferiores a 3,8% [18 mmol/mol], hemoglobina inferior a 5,0 g/dl [3,1 mmol/l] o HbA1c inferior a 0,25 g/dl [0,16 mmol/l] “Inferior al intervalo del ensayo”. Dispense una nueva alícuota de 200 μl de sangre total y vuelva a analizar la muestra. Si el mensaje persiste, póngase en contacto con el proveedor local de asistencia técnica para recibir ayuda.
El sistema de generación de informes del instrumento incluye alarmas y comentarios que proporcionan al usuario información relativa a los errores de procesamiento del instrumento, información del estado de este y posibles errores en los resultados del A1C. Consulte el Manual del usuario del sistema Dimension® para conocer el significado de las alarmas y los comentarios de los informes.
Existe la posibilidad de un funcionamiento incorrecto del sistema si se obtiene la siguiente precisión en 5 pruebas† consecutivas:
Concentración de A1c % [mmol/mol]
DE % [mmol/mol]
5,5 [37] > 0,2 [1,6]9,6 [81] > 0,3 [4,3]
† La copa de muestra debe llenarse con 200 µl para el estudio de precisión en 5 pruebas.
Limitaciones del procedimiento
ADVERTENCIAEl ensayo de hemoglobina A1C Dimension® tiene interferencia significativa con la hemoglobina fetal (HbF). Las muestras que contengan HbF pueden producir una deriva negativa (inferior a los resultados reales) con el ensayo de hemoglobina A1C Dimension®. Los resultados de hemoglobina A1c no son válidos para pacientes con cantidades anómalas de HbF, incluidos aquellos con persistencia hereditaria de hemoglobina fetal diagnosticada. Si desea información adicional sobre la interferencia de la variante de HbF, consulte Sustancias que causan interferencia.
No utilice los calibradores de hemoglobina A1C Dimension® para probar la precisión.
Al igual que ocurre con todos los procedimientos de laboratorio, si existe una importante discrepancia entre la impresión clínica y los resultados del análisis, deberá realizarse la investigación pertinente. Deben tenerse en cuenta algunas de las siguientes limitaciones de análisis:
El ensayo de hemoglobina A1C Dimension® solamente está diseñado para la medición exacta y precisa de mmol/mol de HbA1c (IFCC) y %HbA1c (DCCT/NGSP). Los resultados individuales de la concentración de Hb y HbA1c total no se registran.
Los pacientes con concentraciones de hemoglobina fuera del intervalo aceptable para el ensayo de hemoglobina A1C Dimension® se deben analizar mediante una prueba que emplee un principio de ensayo diferente.
El ensayo de hemoglobina A1C Dimension® no se debe utilizar para diagnosticar diabetes durante el embarazo. La hemoglobina A1c refleja los niveles medios de glucosa en sangre en los 3 meses anteriores (el intervalo de vida medio de un glóbulo rojo), por lo que puede mostrar valores bajos falsos durante el embarazo o cualquier otra afección asociada con la aparición reciente de hiperglucemia o una menor supervivencia de los glóbulos rojos.
El ensayo de hemoglobina A1C Dimension® no se debe emplear para diagnosticar o controlar la diabetes en pacientes con las siguientes afecciones: hemoglobinopatías excepto si se ha demostrado producir un rendimiento aceptable (como rasgo drepanocítico), renovación anómala de los glóbulos rojos (como anemias producidas por hemólisis y deficiencia de hierro), tumores malignos e insuficiencia hepática o renal crónica grave.
En casos de diabetes Tipo 1 de evolución rápida, el aumento de los valores de HbA1c puede demorarse en comparación con el aumento agudo de las concentraciones de glucosa. En estas circunstancias, la diabetes mellitus se debe diagnosticar conforme a las concentraciones de glucosa en plasma o los síntomas clínicos habituales.
Esta prueba no sustituye las pruebas de glucosa para pacientes con diabetes Tipo 1, pacientes pediátricos ni mujeres embarazadas.
Cualquier causa de una menor supervivencia de los glóbulos rojos (por ejemplo, anemia hemolítica u otras enfermedades hemolíticas, embarazo o pérdidas recientes de sangre) reducirán la exposición de los glóbulos rojos a la glucosa, con la consecuente reducción en los valores de HbA1c. Los resultados de HbA1c no son fiables en pacientes con pérdidas crónicas de sangre, debido a la consiguiente variabilidad del intervalo de vida de los eritrocitos12–15.
Valores esperados:
El intervalo de referencia para HbA1c está indicado en la tabla a continuación16.
Los valores de hemoglobina A1c en los individuos sanos pueden variar en función de las poblaciones de referencia. Cada laboratorio debe comprobar la validez del intervalo de referencia y establecer, si es necesario, su propio intervalo de referencia.
La frecuencia de las pruebas HbA1c debería depender de la situación clínica, el régimen de tratamiento y el juicio del médico. La American Diabetes Association recomienda el objetivo razonable de HbA1c del < 7% para adultos no embarazados. Otros objetivos menos estrictos de HbA1c pueden ser adecuados para algunos pacientes con diabetes y otros factores de riesgo, como hipoglucemia grave o numerosas comorbilidades17.
Sustancias que causan interferencia
Hay otras sustancias aparte de los azúcares que pueden formar agregados con la hemoglobina e interferir potencialmente con el análisis produciendo resultados erróneos. Entre los ejemplos, se incluyen los individuos adictos al opio18, saturnismo y alcoholismo12.
El reactivo de anticuerpo utilizado en el ensayo de hemoglobina A1C Dimension® medirá todas las variantes de la glucohemoglobina que estén glicadas en el N-terminal de la cadena beta y que tengan epítopos idénticos a los de la HbA1c (secuencia de aminoácidos: VAL-HIS-LEU-THR). Incluye HbS, HbC, HbD y HbE. Otras hemoglobinopatías pueden producir resultados incorrectos con este análisis. Debe tenerse cuidado al interpretar cualquier resultado de HbA1c procedente de pacientes con variantes de Hb. Una hemoglobina anómala puede afectar a la vida media de los glóbulos rojos o las tasas de glucación in vivo. En estos casos, incluso los resultados que sean analíticamente correctos no reflejarán el mismo nivel de control glucémico que sería de esperar en pacientes con hemoglobina normal14.
El anticuerpo anti-HbA1c no reconoce la HbF glicada (hemoglobina fetal), que consta de dos cadenas alfa y dos cadenas gamma. Los individuos con niveles elevados de HbF (> 10%), que se encuentra sobre todo en niños y pacientes con talasemia beta, pueden producir con este análisis resultados más bajos de lo esperado. Estas muestras deberán analizarse utilizando un método alternativo.
No se ha detectado ninguna reacción cruzada para los anticuerpos anti-HbA1c utilizados en este kit con HbA0, HbA1a, HbA1b, hemoglobina acetilada, hemoglobina carbamilada y HbA1c lábil.
Características específicas de funcionamiento
Los siguientes datos representan el rendimiento típico del sistema Dimension®. Los resultados reales obtenidos por cada laboratorio pueden diferir según el diseño del estudio.
PrecisiónLas pruebas de precisión se realizaron conforme a la directriz del CLSI EP05-A319. Las pruebas se realizaron en 20 días con 3 instrumentos y 3 lotes de reactivos en cada instrumento. Cada día de análisis se realizaron 2 ensayos (con una separación mínima de 2 horas entre ellos).
NGSP (%HbA1c)
Repetibilidad (Intra-ensayo)
Intralaboratorio (Total)
Tipo de muestra N Media DEj CV (%)k DEj CV (%)k
Control 1 720 5,2 0,05 1,0 0,13 2,6Control 2 720 9,5 0,08 0,8 0,16 1,7Mezcla de sangre total 1 720 5,3 0,05 0,9 0,13 2,4Mezcla de sangre total 2 720 6,4 0,05 0,7 0,11 1,7Mezcla de sangre total 3 720 7,8 0,06 0,8 0,13 1,6Mezcla de sangre total 4 720 11,9 0,09 0,8 0,22 1,8
IFCC (mmol/mol)Repetibilidad (Intra-ensayo)
Intralaboratorio (Total)
Tipo de muestra N Media DEj CV (%)k DEj CV (%)k
Control 1 720 34 0,56 1,7 1,47 4,4Control 2 720 81 0,87 1,1 1,73 2,2Mezcla de sangre total 1 720 35 0,54 1,5 1,42 4,1Mezcla de sangre total 2 720 47 0,52 1,1 1,17 2,5Mezcla de sangre total 3 720 62 0,68 1,1 1,41 2,3Mezcla de sangre total 4 720 107 0,99 0,9 2,41 2,3
j. Desviación estándark. Coeficiente de variación
Comparación de métodosLas pruebas de la comparación de métodos se realizaron conforme a la directriz del CLSI EP09-A320. Los resultados del ensayo de hemoglobina A1C Dimension® (y) se compararon con los resultados generados con un método de prueba NGSP estandarizado (HPLC) (x).
Regresión de Passing-BablokUnidades N Intervalo de muestra Pendiente IC del 95% Intersección Y IC del 95%%HbA1c 147 4,5–13,2 0,983 0,966–1,001 0,030 -0,095–0,144mmol/mol 147 26–121 0,973 0,955–0,992 0,437 -0,474–1,450
Estimación de la regresión de Passing-Bablok%HbA1c Deriva % deriva5,00 -0,05 -1,106,50 -0,08 -1,248,00 -0,11 -1,3312,00 -0,17 -1,45
Resumen de errores totales de Passing-Bablok
%HbA1c % deriva %CV % total de error5,0 -1,10 2,4 5,86,5 -1,24 1,7 4,58,0 -1,33 1,6 4,412,0 -1,45 1,8 4,9
Regresión de Deming
Unidades N Intervalo de muestra Pendiente IC del 95% Intersección Y IC del 95%%HbA1c 147 4,5–13,2 0,978 0,957–1,000 0,052 -0,094–0,198mmol/mol 147 26–121 0,970 0,948–0,992 0,532 -0,603–1,666
%HbA1c % deriva %CV % total de error5,0 -1,16 2,4 5,86,5 -1,40 1,7 4,78,0 -1,55 1,6 4,612,0 -1,77 1,8 5,2
La comparación de métodos se evaluó utilizando el análisis de Bland-Altman de la deriva21, que es el método empleado por el NGSP. Se indican la diferencia media entre A1C y el método de red del NGSP (HPLC) y los intervalos de confianza del 95% de las diferencias en el rango de 4–10% de HbA1c. El 95% de las diferencias entre los valores obtenidos para las muestras individuales con ambos métodos están comprendidos dentro del rango definido por los intervalos de confianza del 95% inferior y superior de las diferencias.
Siemens Healthcare Diagnostics Inc.500 GBC DriveNewark, DE 19714 USA
2019
-10
C P
N 11
2752
89 -
ES
Comparación de anticoagulantesSe realizó la prueba de equivalencia para 5 anticoagulantes conforme a la directriz del CLSI EP09-A320. Las pruebas se realizaron utilizando un lote de reactivos y un solo duplicado de un juego emparejado de 4 anticoagulantes (K3 EDTA; fluoruro sódico/Na2 EDTA; heparina de litio y fluoruro sódico/oxalato de potasio) y muestras de K2 EDTA.
Regresión de Passing-Bablok: NGSP (%)
Anticoagulante Muestra de comparación (x) Pendiente IC del 95% Intersección Y IC del 95%
Heparina de litio K2 EDTA 1,008 0,990–1,027 -0,271 -1,47–0,93
Fluoruro sódico/oxalato de potasio K2 EDTA 1,007 0,989–1,025 -0,032 -1,22–1,16
Número de pruebas analizadas (N) = 79Intervalo de muestra (mmol/mol) = 28–125
Especificidad
Sustancias que no causan interferencia
Las pruebas de interferencia se realizaron conforme a la directriz del CLSI EP07-A222.
Las siguientes sustancias no interfieren con el ensayo de hemoglobina A1C Dimension® si están presentes en la sangre total en las concentraciones indicadas. Las inexactitudes (derivas) debidas a estas sustancias son inferiores o iguales al 5% para concentraciones de hemoglobina A1c del 6,5% ± 1,0% y 8,0% ± 1,0% (inferiores o iguales al 8% para 48 mmol/mol ± 11 mmol/mol y 64 mmol/mol ± 11 mmol/mol).
Interferente Concentración de interferente Unidades comunes
Variantes de hemoglobinaLas pruebas de interferencia para determinar las variantes de hemoglobina en el ensayo de hemoglobina A1C Dimension® se realizaron conforme a la directriz del CLSI EP07-A222. No se observó ninguna deriva de interferencia para HbC, HbD, HbE y HbA2. Se observó una deriva de interferencia significativa para HbF.
Derivados de la hemoglobinaSe realizaron pruebas de interferencia para determinar el efecto de los derivados de la hemoglobina, entre los que se incluyó hemoglobina acetilada, hemoglobina carbamilada, hemoglobina lábil y fracciones de hemoglobina en el ensayo de hemoglobina A1C Dimension® conforme a la directriz del CLSI EP07-A222. Las inexactitudes (derivas) debidas a estas sustancias son inferiores o iguales al 5% para concentraciones de hemoglobina A1c del 5,0% ± 1,0%, 6,5% ± 1,0% y 8,0% ± 1,0% (inferiores o iguales al 9% para 31 mmol/mol ± 11 mmol/mol, 48 mmol/mol ± 11 mmol/mol y 64 mmol/mol ± 11 mmol/mol). • La hemoglobina acetilada fue superior o igual a 50 mg/dl (2,8 mmol/l) de ácido acetilsalicílico • La hemoglobina carbamilada fue superior o igual a 10 mmol/l de cianato • La hemoglobina lábil fue superior o igual a 1500 mg/dl (83,3 mmol/l) de glucosa
Límite de detección y límite del blancoEl límite de detección (LoD) y el límite del blanco (LoB) se determinaron como se describe en la directriz del CLSI EP17-A223.
El LoB es el resultado de la medición más alto que es probable que se observa en una muestra en blanco. El LoB se halló utilizando 60 determinaciones con 5 muestras en blanco para tHb y 75 determinaciones con 5 muestras en blanco para %HbA1c/HbA1c.
El LoD corresponde a la concentración más baja de HbA1c o tHb que se puede detectar con una probabilidad del 95%. El LoD se halló utilizando 60 determinaciones con cinco muestras de bajo nivel para tHb y 75 determinaciones con cinco muestras bajas para %HbA1c/HbA1c.
A continuación se muestran el LoB y el LoD del ensayo de hemoglobina A1C Dimension®.
1. Bunn HF, Gabbay KH, and Gallop PM. The glycosylation of hemoglobin: relevance to diabetes mellitus. Science 200: 21-27, 1978.
2. Nathan DM. Labile glycosylated hemoglobin contributes to hemoglobin A1 as measured by liquid chromatography or electrophoresis. Clin Chem. 27:1261-1263, 1981.
3. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 329:977-986, 1993.
4. King EJ. Alkaline hematin method for haemoglobin determination. Br Med J. 2(1):349-350, 1947.5. Clinical and Laboratory Standards Institute/NCCLS. Procedures for the Collection of Diagnostic Blood
Specimens by Venipuncture; Approved Standard—Fifth Edition. CLSI/NCCLS document H3-A5 [ISBN 1-56238-515-1]. CLSI, 940 West Valley Road, Suite 1400, Wayne, PA 19087-1898 USA, 2003.
6. Clinical and Laboratory Standards Institute/NCCLS. Tubes and Additives for Venous Blood Specimen Collection; Approved Standard—Fifth Edition. CLSI/NCCLS document H1-A5 [ISBN 1-56238-519-4]. CLSI, 940 West Valley Road, Suite 1400, Wayne, PA 19087-1898 USA, 2003.
7. Clinical and Laboratory Standards Institute/NCCLS. Procedures for the Handling and Processing of Blood Specimens; Approved Guideline—Third Edition. CLSI/NCCLS document H18-A3 [ISBN 1- 56238-555-0]. CLSI, 940 West Valley Road, Suite 1400, Wayne, PA 19087-1898 USA, 2004.
8. Data on file.9. National Glycohemoglobin Standardization Program (NGSP) website: www.ngsp.org accessed
November 3, 2017. 10. Hoelzel W, Weykamp C, Jeppsson J, Miedema K, et al. IFCC Reference System for Measurement of
Hemoglobin A1c in Human Blood and the National Standardization Schemes in the United States, Japan, and Sweden; A Method-Comparison Study. Clin. Chem. 50:1, 166-174, 2004.
11. International Federation of Clinical Chemistry, Working Group on Standardization of Hemoglobin A1c website: http://www.ifcchba1c.net accessed June 5, 2018
12. Goldstein DE, Wiedmeyer HM, England JD, Little RR, Parker KM. Recent advances in glycosylated hemoglobin measurements. Crit Rev Clin Lab Sci 1984; 21:187-228.
13. Peacock I. Glycosylated haemoglobin: measurement and clinical use. J Clin Pathol 1984; 37:841- 851.14. Miedema K. Influence of hemoglobin variants on the determination of glycated hemoglobin. Klin Lab 1993;
39:1029-1032. 15. Lind T, Cheyne GA. Effect of normal pregnancy upon the glycosylated haemoglobins. Br J Obstet Gyn 1979;
86:210-213.16. American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2017;
40 (Supplement 1): S11-S24.17. American Diabetes Association. Standards of Medical Care in Diabetes—2017. Diabetes Care. 2017;
40(Suppl. 1): S1–S13518. Ceriello A, Giulgliano D, Dello Russo P, Sgambato S, D’Onofrio F. Increased glycosylated hemoglobin A1 in
opiate addicts. Evidence for hyperglycemic effect of morphine. Diabetologia 1962; 22:379.19. Clinical and Laboratory Standards Institute (formerly NCCLS). Evaluation of Precision Performance of