40
Prof. Utham Murali. M.S.,M.B.A .
| Date post: | 22-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | uthamalingam-murali |
| View: | 71 times |
| Download: | 3 times |

Prof. Utham Murali. M.S.,M.B.A .

Page 2
Fluids – Importance & Composition.
Fluid – Types of Transport.
Fluid Imbalances – You See & You Do.

Page 3
Between 50% and 60% of the human body by weight is water.
Water provides a medium for transporting nutrients to cells and wastes from cells and for transporting substances such as hormones, enzymes, platelets, RBC’s & WBC’s.
Helps maintain normal body temperature Facilitates digestion and promotes elimination Acts as a tissue lubricant
Page 4
Because fat cells contain little water and lean tissue is rich in water, the more obese the person, the smaller the percentage of total body water compared with body weight.
This is also true between sexes because females tend to have proportionally more body fat than males.

Page 5AGEAGE

Page 6
Page 7
Page 8

Page 9
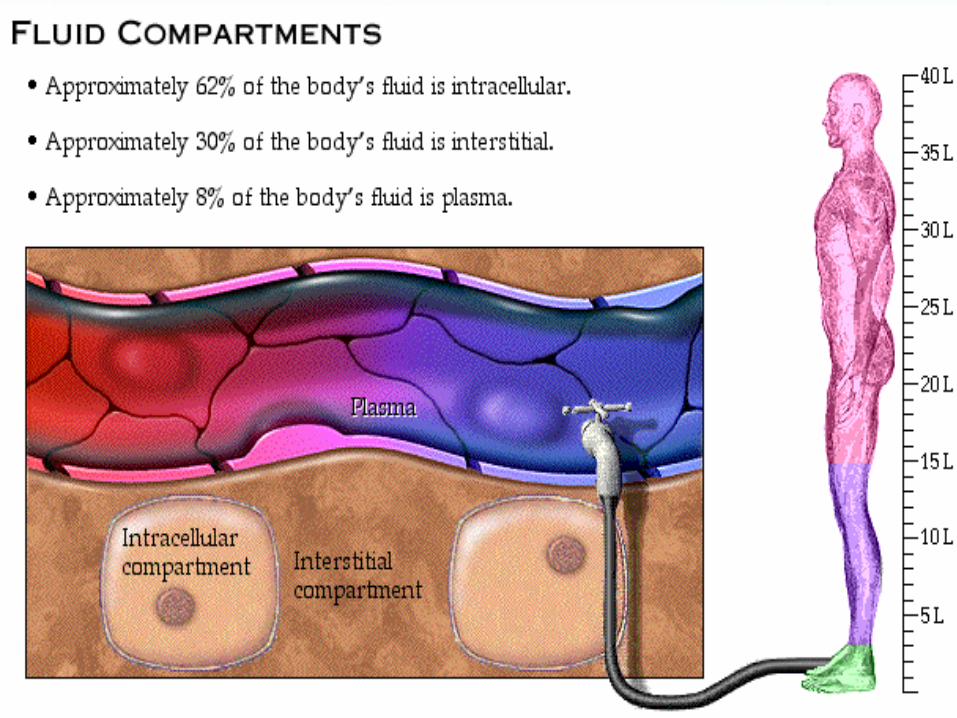
60% composed of water70 kg person= 42 L2/3 ICF = 28L1/3 ECF = 14L
TBW= ECF + ICF

Page 10
Fluids and solutes constantly move within the body, which allows the body to maintain homeostasis.
Fluids along with nutrients and waste products constantly shift within the body’s compartments from the cell to the interstitial spaces, to the blood vessels and back again.
Page 11
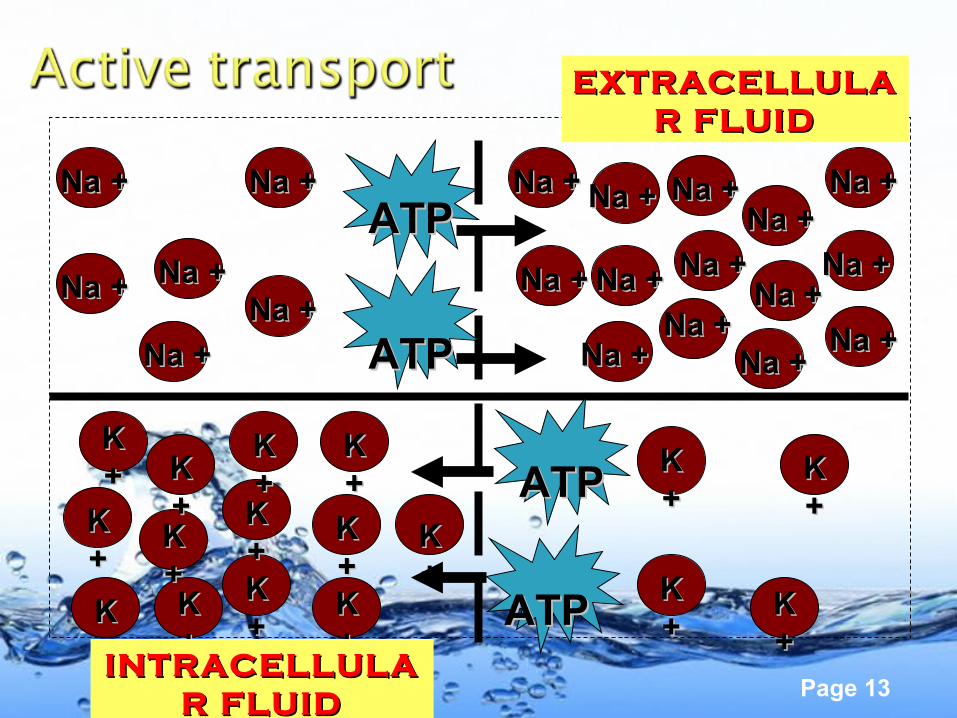
A. Active transport
B. Passive transport
- Diffusion
- Osmosis
- Filtration
Page 12
Solutes / Molecules can be moved against a concentration gradient as they move from an area of lower concentration to an area of higher concentration and requires an energy.
Also called “pumping” Dependent on the presence of ATP
Page 13
K K ++
K K ++
K K ++
K K ++
K K ++
K K ++
K K ++K K
++K K ++
K K ++
K K ++
K K ++K K
++
K K ++
K K ++
K K ++
K K ++
ATPATP
ATPATP
ATPATP
ATPATP Na +Na +
Na +Na +Na +Na +
Na +Na + Na +Na +Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +
Na +Na +Na +Na +
INTRACELLULAINTRACELLULAR FLUIDR FLUID
EXTRACELLULAEXTRACELLULAR FLUIDR FLUID
Page 14
Molecules move across a biological membrane from an area of higher to an area of lower concentration
Membrane types◦ Permeable◦ Semi-permeable◦ Impermeable
Page 15
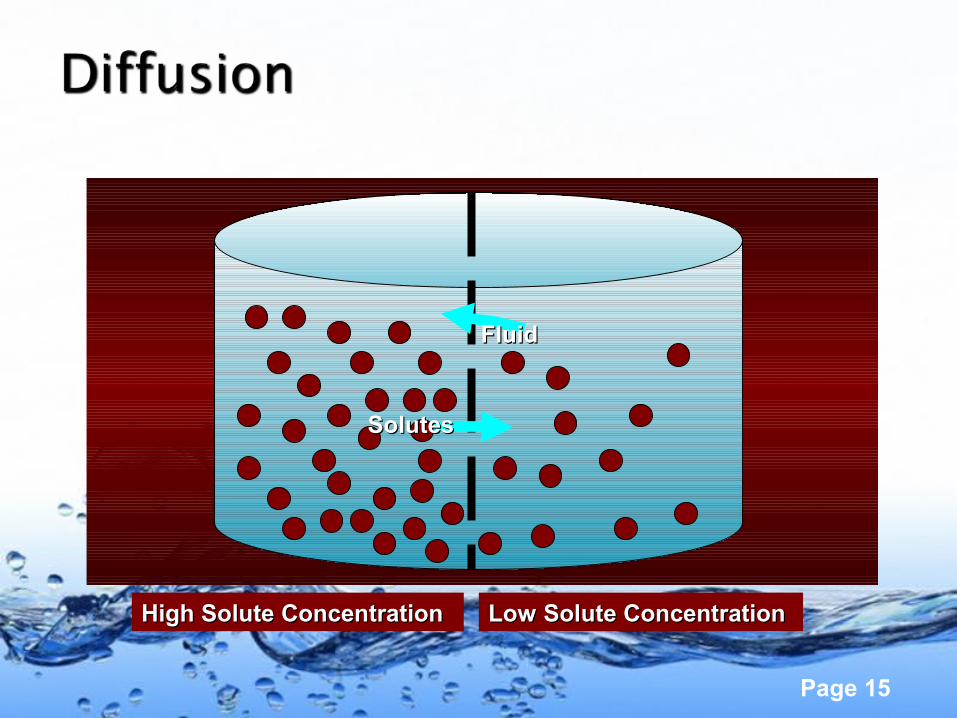
High Solute ConcentrationHigh Solute Concentration Low Solute ConcentrationLow Solute Concentration
FluidFluid
SolutesSolutes
Page 16
Movement of solute and solvent across a membrane caused by hydrostatic (water pushing) pressure
Occurs at the capillary level If normal pressure gradient changes (as occurs
with right-sided heart failure) edema results from “third spacing”

Page 17
Page 18
Movement of solvent from an area of lower solute concentration to one of higher concentration
Occurs through a semipermeable membrane using osmotic (water pulling) pressure

Page 19
FluidFluid
High Solution High Solution Concentration, Concentration,
Low Fluid Low Fluid ConcentrationConcentration
Low Solute Low Solute Concentration, Concentration,
High Fluid High Fluid ConcentrationConcentration

Page 20
Fluids in the body generally aren’t found in pure forms.
Isotonic, hypotonic, and hypertonic types.
Defined in terms of the amount of solute or dissolve substances in the solution.
Balancing these fluids involves the shifting of fluid not the solute involved.
Page 21
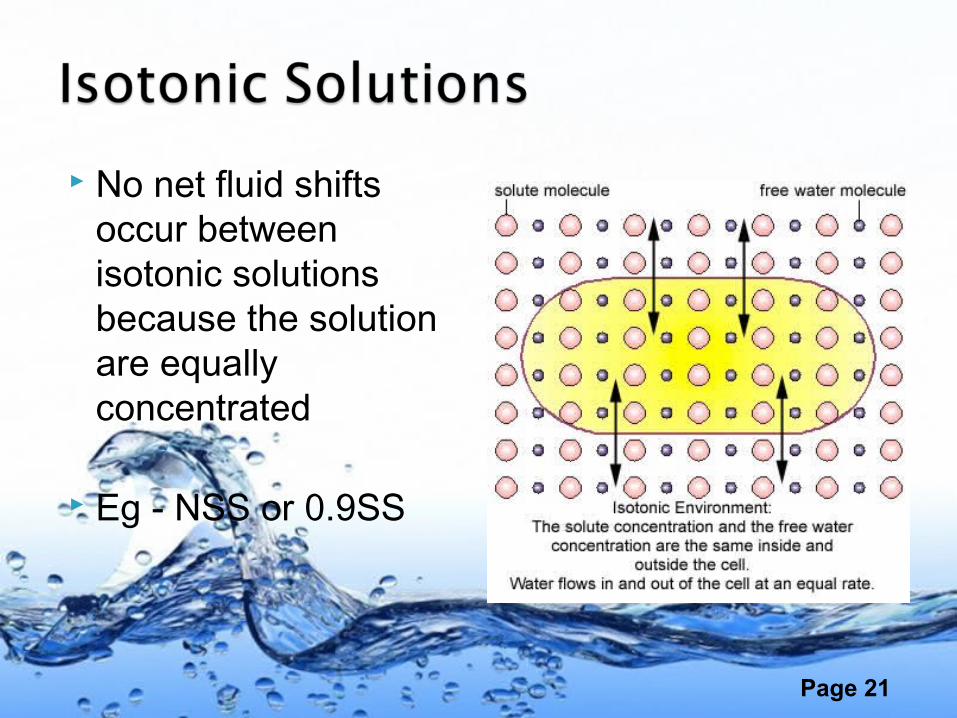
No net fluid shifts occur between isotonic solutions because the solution are equally concentrated
Eg - NSS or 0.9SS

Page 22
Has a lower solute concentration than another solution
Fluid from the hypotonic solution would shift into the second solution until the two solutions had equal concentrations
Eg - Half normal or 0.45%SS
Page 23
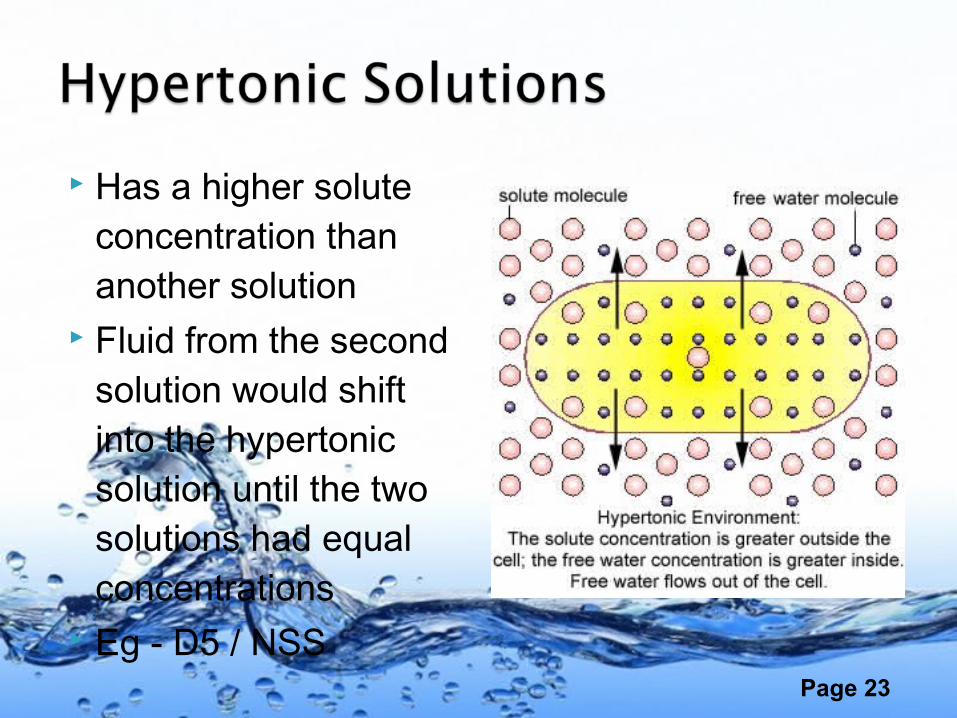
Has a higher solute concentration than another solution
Fluid from the second solution would shift into the hypertonic solution until the two solutions had equal concentrations
Eg - D5 / NSS
Page 24
Isotonic loss of water and electrolytes (fluid volume deficit) – “Hypovolaemia”
Isotonic gain of water and electrolytes (fluid volume excess) – “Hypervolaemia / Edema”
Hyperosmolar loss of only water (Dehydration) Hypo-osmolar gain of only water (Overhydration) –
“Water Intoxication”
Page 25
Loss of body fluids ⇒ increased concentration of solutes in the blood and a rise in serum Na+ levels.
Fluid shifts out of cells into the blood to restore balance.
Cells shrink from fluid loss and can no longer function properly.
Page 26
Mild = Weight loss – 5%
Moderate = Weight loss – 10%
Severe = Weight loss – 15%

Page 27
IrritabilityConfusionDizzinessWeaknessExtreme thirst⇓ urine output
FeverDry skin/mucous
membranesSunken eyesPoor skin turgorTachycardia
Page 28
Fluid Replacement - Oral or IV over 48 hrs. Monitor symptoms and vital signs Maintain I & O Maintain IV access Daily weights Skin and mouth care
Page 29
Isotonic fluid loss from the extracellular space
Can progress to hypovolemic shock
Caused by:◦ Excessive fluid loss
(hemorrhage)◦Decreased fluid
intake◦ Third space fluid
shifting

Page 30
Mild = < 2 L fluid loss
Moderate = 2 – 3 L fluid loss
Severe = > 3 L fluid loss

Page 31
Mental status deterioration
Thirst Tachycardia Delayed capillary
refill
Orthostatic hypotension
Urine output < 30 ml/hr
Cool, pale extremities
Weight loss
Page 32
Fluid replacement Albumin
replacement Blood transfusions
for hemorrhage
Dopamine to maintain BP
Assess for fluid overload with treatment
Page 33
Excess fluid in the extracellular compartment as a result of fluid or sodium retention, excessive intake, or renal failure.
Occurs when compensatory mechanisms fail to restore fluid balance.
Leads to CHF and pulmonary edema.
Page 34
Tachypnea Dyspnea Crackles Rapid, bounding pulse Hypertension S3 gallop
Increased CVP, pulmonary artery pressure and pulmonary artery wedge pressure
Acute weight gain Edema
Page 35
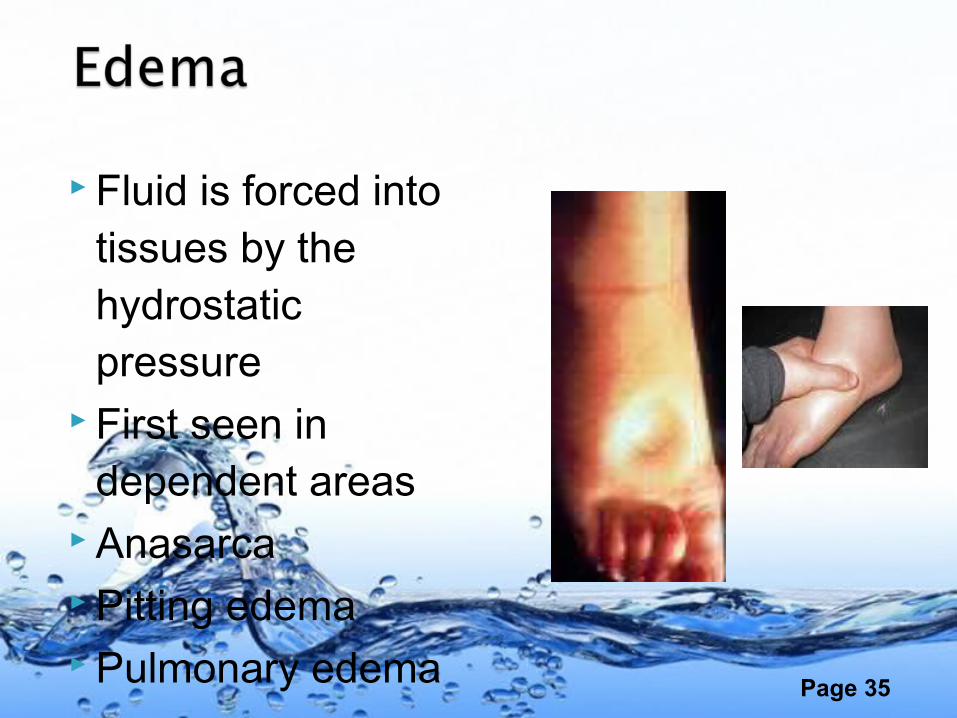
Fluid is forced into tissues by the hydrostatic pressure
First seen in dependent areas
Anasarca Pitting edema Pulmonary edema

Page 36
Fluid and Na+ restriction
Diuretics Monitor vital signs Hourly I&O Breath sounds
Monitor ABGs and labs
Elevate HOB and give O2 as ordered
Maintain IV access Skin & mouth care Daily weights
Page 37
Hypotonic extracellular fluid shifts into cells to attempt to restore balance
Cells swell
Causes:◦ SIADH◦ Rapid infusion of
hypotonic solution◦ Excessive tap water NG
irrigation or enemas◦ Psychogenic polydipsia◦ TURP
Page 38
Signs and symptoms of increased intracranial pressure◦ Early: change in LOC, N/V, muscle weakness,
twitching, cramping
◦ Late: bradycardia, widened pulse pressure, seizures, coma
Page 39
Prevention is the best treatment
Assess neuro status Monitor I&O and vital
signs - ICU Fluid restrictions
IV access Daily weights Monitor serum Na+ Seizure precautions

Page 40







![L-14 Fluids [3] Fluids at rest Fluid Statics Fluids at rest Fluid Statics Why things float Archimedes’ Principle Fluids in Motion Fluid Dynamics.](https://static.documents.pub/doc/80x56/56649ced5503460f949ba1d5/l-14-fluids-3-fluids-at-rest-fluid-statics-fluids-at-rest-fluid-statics.jpg)




![L 13 Fluids [2]: Statics fluids at rest](https://static.documents.pub/doc/80x56/56815fcc550346895dcec7e6/l-13-fluids-2-statics-fluids-at-rest-56c761b351f15.jpg)




