46
1 www.aap.org/oralhealth/ pact Protecting All Children’s Teeth Fluorid e

1 www.aap.org/oralhealth/pact
Protecting All Children’s Teeth
Fluoride

2 www.aap.org/oralhealth/pact
Introduction
Fluoride plays an important role in the prevention of dental caries.
The primary mechanism of action of fluoride in preventing dental caries is topical. Fluoride acts in the following ways to prevent dental caries:
1. It enhances remineralization of the tooth enamel. This is the most important effect of fluoride in caries prevention.
2. It inhibits demineralization of the tooth enamel.
3. It makes cariogenic bacteria less able to produce acid from carbohydrates.
Used with permission from Lisa Rodriguez

3 www.aap.org/oralhealth/pact
Learner Objectives
Upon completion of this presentation, participants will be able to:
State the 3 mechanisms of action of fluoride in dental caries prevention
Summarize the available sources of fluoride and their relative benefits
List strategies to minimize the development of fluorosis Discuss the fluoride supplementation guidelines Recognize the various forms of fluorosis and recall their
prevalence
Used with permission from Lisa Rodriguez

4 www.aap.org/oralhealth/pact
Fluoride Facts
Fluoride has been available in the United States since the mid 1940’s. In 2008, 64.3% of the population served by public water systems received optimally fluoridated water. Public water fluoridation practice varies by city and state. Water fluoridation was recognized by the Centers for Disease
Control and Prevention (CDC) as one of the 10 greatest public
health achievements of the 20th century.

5 www.aap.org/oralhealth/pact
Fluoride Facts, continued
There is strong evidence* that community water fluoridation is
effective in preventing dental caries.
In 2011, the U.S Dept of Health and Human Services proposed that
community water systems adjust the concentration of fluoride in
drinking water to 0.7 mg/L ppm (change from 0.7-1.2 mg/L). This proposal has not been finalized.
Water filters may alter the fluoride content of community water. Activated charcoal filters and cellulose filters have a negligible effect
Reverse osmosis filters and water distillation remove almost all fluoride from water
6 www.aap.org/oralhealth/pact
Sources of Systemic Fluoride Exposure
Fluoride can be ingested through:
Drinking water (naturally occurring or water system additive) Other beverages Foods Toothpaste Fluoride dietary supplements

7 www.aap.org/oralhealth/pact
Bottled Water
No one source exists to tell consumers the fluoride content in bottled waters.
The US Food and Drug Administration (FDA) does not require that fluoride content be listed on the labels of bottled waters.
It is reasonable to assume that children whose only source of water is bottled are not receiving optimal amounts of fluoride from that source.

8 www.aap.org/oralhealth/pact
Commercial Beverages and Foods
Many foods and beverages are made with community fluoridated water, so may contain fluoride.
Foods such as seafood and certain teas can also have a naturally high fluoride content.
This must all be taken into account when determining daily fluoride intake.

9 www.aap.org/oralhealth/pact
Infant Nutrition
Human breast milk contains almost no fluoride, even when the nursing mother drinks fluoridated water.
Powdered infant formula contains little or no fluoride, unless mixed with fluoridated water. The amount of fluoride ingested will depend on the volume of fluoridated water mixed with the formula.
Used with permission from Kathleen Marinelli, MD

10 www.aap.org/oralhealth/pact
Toothpaste
Toothpaste’s effects are mainly topical, but some toothpaste is swallowed by children and results in systemic fluoride exposure.
Strategies to Minimize Toothpaste Ingestion Limit the amount of toothpaste on the toothbrush Discourage children from swallowing toothpaste Encourage spitting of toothpaste Supervise brushing until spitting can be ensured
Used with permission from Norman Tinanoff, DDS

11www.aap.org/oralhealth/pact
Topical Sources of Fluoride
Following are the most common forms of topical fluoride:
Toothpaste Fluoride mouthrinses Fluoride gels Fluoride varnish

12 www.aap.org/oralhealth/pact
Toothpaste
Toothpaste is the most recognizable source of topical fluoride.
The addition of fluoride to toothpaste began in the 1950s.
Brushing with fluoridated toothpaste is associated with a 24% reduction in decayed, missing, and filled tooth surfaces.
The CDC concluded that the quality of evidence for fluoridated toothpaste in reduction of caries is grade 1. Strength of recommendation is A for use in all persons.
Used with permission from Rocio B. Quinonez, DMD, MS, MPH; Associate Professor Department of Pediatric Dentistry, School
of Dentistry University of North Carolina

13 www.aap.org/oralhealth/pact
Fluoride Mouthrinses
Mouthrinses containing fluoride are recommended in a “swish and spit” manner for children at least age 6.
Mouthrinses are available over the counter. • Daily use of a 0.05% sodium fluoride rinse may benefit children over 6
years who are at high risk for dental caries• No additional benefit shown beyond daily fluoridated toothpaste use for
children at low risk for caries
The CDC concluded that quality of evidence for fluoride mouthrinses is Grade 1. Strength of recommendation is A with targeted effort atpopulations at high risk for dental caries.

14 www.aap.org/oralhealth/pact
Fluoride Gels
Fluoride gels are professionally applied or prescribed for home use under professional supervision. They are typically recommended for use twice per year.
The CDC concluded that the quality of evidence for using fluoride gel to prevent and control dental caries in children is Grade 1. Strength of recommendation is A, with targeted effort at populations at high risk for caries.

15 www.aap.org/oralhealth/pact
Fluoride Varnish
Varnish is a professionally applied, sticky resin of highly concentrated fluoride (up to 22,600 ppm).
In the United States, fluoride varnishhas been approved by the FDA for use as a cavity liner and root desensitizer, but not specifically as an anti-caries agent.
For caries prevention, fluoride varnish is an “off label” product.
Used with permission from Suzanne Boulter, MD

16
Fluoride Varnish
Application frequency for fluoride varnish ranges from 2 to 6 times per year.
The use of fluoride varnish leads to a 33% reduction in decayed, missing, and filled tooth surfaces in the primary teeth and a 46% reduction in the permanent teeth.
The CDC concluded that the quality of evidence for using fluoride varnish to prevent and control dental caries in children is Grade 1. Strength of recommendation is A, with targeted effort at populations at high risk for dental caries.
Used with permission from Ian VanDinther

17 www.aap.org/oralhealth/pact
Community Water Fluoridation
The goal of community water fluoridation is to maximize dental caries prevention while minimizing the frequency of enamel fluorosis.
In January 2011, the US Department of Health and Human Servicesproposed 0.7 ppm be considered the optimal fluoride concentrationin drinking water.
Because there is geographic variability in community waterfluoridation, it is important to know fluoride content of the water children consume.

18 www.aap.org/oralhealth/pact
Water Fluoridation
The US Environmental Protection Agency requires that all community water supply systems provide customers an annual report on the quality of water, including fluoride concentration. Families or providers can contact the local water authority for this information.
Fluoride content of a town’s water can also be determined byaccessing CDC’s My Water's Fluoride Web site.
Used with permission from iSTOCK

19 www.aap.org/oralhealth/pact
Well Water
Wide variations in the natural fluoride concentration of well water sources exist.
Private wells should be tested for fluoride concentration before prescribing supplements.
Testing can be done through local and state public health departments or through private laboratories.

20 www.aap.org/oralhealth/pact
Fluoride Dietary Supplementation
When access to community water fluoridation is limited, fluoride can be supplemented in liquid, tablet, or lozenge form.
Fluoride supplements require a prescription. A 2010 ADA guideline* recommends fluoride supplements be prescribed only to children determined to be at high risk for the development of caries whose community water source is suboptimal.

21
Supplementation Dosing Schedule
The AAP, ADA, and AAPD have developed the following recommendations regarding fluoride supplementation:
1. All sources of fluoride must be considered, including primary drinking water, other sources of water, prescriptions from the dentist, fluoride mouthrinse in school, and fluoride varnish. 2. Supplementation should be provided to high-risk children if fluoride access is limited. 3. Children younger than 6 months and older than 16 years should NOT be supplemented. 4. Children who have adequate access to (and are drinking) appropriately fluoridated community water should not be supplemented.

22 www.aap.org/oralhealth/pact
Fluoride Supplements, continued
CDC Quality of Evidence to Support the Use of Fluoride Supplements
Children 6 years and younger: Grade II-3. Strength of recommendation of C with targeted effort at populations at high risk for dental caries. Children 6-16 years: Grade 1. Strength of recommendation of A with targeted effort at populations at high risk for dental caries. Pregnant women: Quality of evidence against providing fluoride supplementation to pregnant women to benefit their children is Grade 1. Strength of recommendation of E (good evidence to reject the use of the modality).

23
Fluoride Supplements, continued
The 2010 ADA guideline* recommends
fluoride supplements be prescribed only
to children at high risk for caries.
Strength of recommendation: B
The United States Preventive Services
Task Force recommends fluoride
supplementation be prescribed at
recommended doses to children older
than 6 months whose primary water
source is deficient in fluoride. Strength of recommendation: BUsed with permission from Content Visionary
24 www.aap.org/oralhealth/pact
Fluorosis
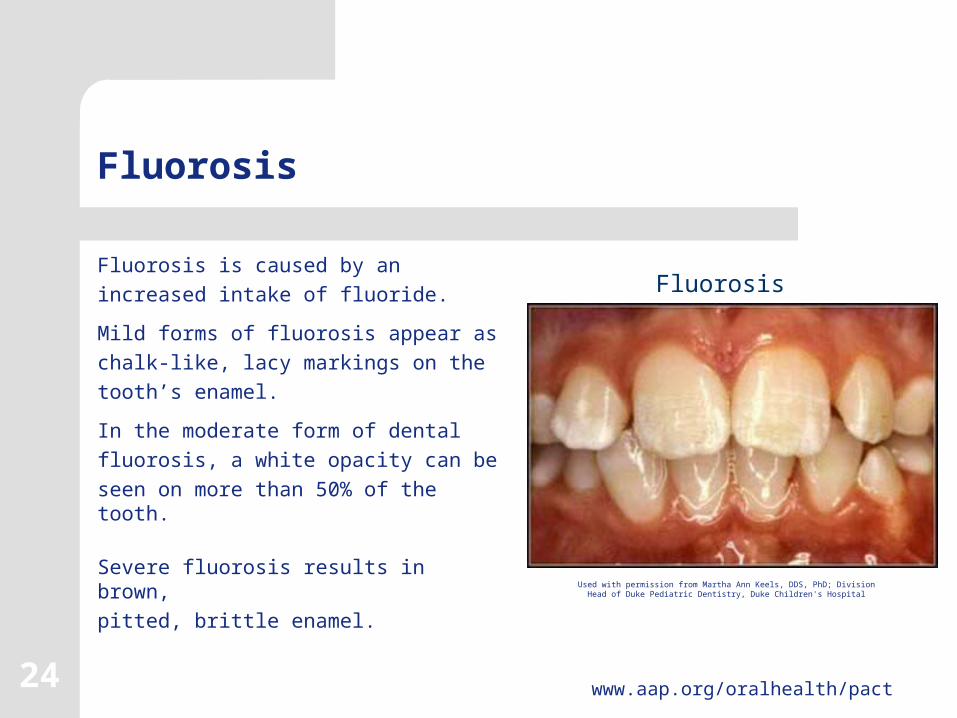
Fluorosis is caused by an increased intake of fluoride.
Mild forms of fluorosis appear as chalk-like, lacy markings on the tooth’s enamel.
In the moderate form of dental fluorosis, a white opacity can be seen on more than 50% of the tooth.
Severe fluorosis results in brown, pitted, brittle enamel.
Used with permission from Martha Ann Keels, DDS, PhD; Division Head of Duke Pediatric Dentistry, Duke Children's Hospital
Fluorosis

25
Fluorosis
Dental fluorosis occurs during tooth
development.
Permanent teeth are more susceptible to
fluorosis than primary teeth.
Most critical ages of susceptibility are
0 to 6 years, especially between the ages
of 15 and 30 months.
After 7 or 8 years of age, dental fluorosis cannot
occur because the permanent teeth are fully
developed, although not erupted.Used with permission from Content Visionary

26 www.aap.org/oralhealth/pact
Prevalence of Fluorosis
The prevalence of dental fluorosis has increased in the United States from 22.8% in 1986-1987 to 32% in 1999-2002.
This can be attributed to the increased availability and ingestion of multiple sources of fluoride by young children, including:
Foods Beverages Toothpaste Other oral care products Dietary fluoride supplements

27 www.aap.org/oralhealth/pact
Prevalence of Fluorosis, continued
Some form of dental fluorosis is found in the following age groups*: 40% of US children ages 6-11 years 48% of 12- to 15-year-olds 42% of 16- to 19-year-olds
Most of this fluorosis is mild and barely noticeable by non-dental health professionals.

28 www.aap.org/oralhealth/pact
Prevalence of Fluorosis, continued
Although the effects of dental fluorosis are mainly aesthetic, the increased prevalence mandates that health professionals be aware of all possible sources of fluoride before considering supplementation.

29 www.aap.org/oralhealth/pact
Fluorosis and Toothpaste
Ingestion of toothpaste increasesthe risk of enamel fluorosis.
If fluoridated toothpaste is used,strategies to limit the amountswallowed include limiting theamount placed on the brush andobserving the child as they brush.
Used with permission from Rocio B. Quinonez, DMD, MS, MPH; Associate Professor Department of Pediatric Dentistry, School of Dentistry University of North Carolina

30 www.aap.org/oralhealth/pact
Fluorosis and Toothpaste
According to the AAPD, the best way to minimize a child's risk for fluorosis is to limit the amount of toothpaste on the toothbrush.
The AAPD suggests a “smear” of toothpaste for children younger than 2 years of age and a "pea-sized" amount for children ages 2 to 5.
Used with permission from Michael SanFilippo

31 www.aap.org/oralhealth/pact
Fluorosis and Toothpaste
For children younger than 2, the CDC suggests the pediatrician consider fluoride levels in the community drinking water, other sources of fluoride, and factors likely to affect susceptibility to dental caries when weighing the risk and benefits of fluoride toothpaste. For children younger than 6, the CDC recommends that parents:
1. Limit tooth brushing to 2 times a day. 2. Apply less than a pea-sized amount of toothpaste to the brush. 3. Supervise tooth brushing and encourage children to spit out excess toothpaste.4. Keep toothpaste out of the reach of young children to avoid accidental ingestion.

32 www.aap.org/oralhealth/pact
Fluorosis and Toothpaste
A 2007 Maternal and Child Health Bureau expert panel recommended: All children at high risk for dental caries use fluoride toothpaste Children younger than age 2 use a “smear” of fluoride toothpaste Children aged 2-6 years use a slightly larger, “pea-sized” amount The AAP endorses this recommendation.
When deciding whether to use fluoridated toothpaste in children younger than 2, the panel recommends considering: The child's risk of dental caries The risk of dental fluorosis The benefit of the topical application in the form of fluoridated toothpaste

33 www.aap.org/oralhealth/pact
Question #1
What is the most critical age of susceptibility to fluorosis of
the permanent teeth?
A. Between 0 and 15 months of ageB. Between 15 and 30 months of ageC. Between 30 and 45 months of ageD. The risk of fluorosis in the permanent teeth is equal
across all agesE. None of the above

34 www.aap.org/oralhealth/pact
Answer
What is the most critical age of susceptibility to fluorosis of
the permanent teeth?
A. Between 0 and 15 months of ageB. Between 15 and 30 months of age C. Between 30 and 45 months of ageD. The risk of fluorosis in the permanent teeth is equal
across all agesE. None of the above

35 www.aap.org/oralhealth/pact
Question #2
True or False? The most important mechanism of action of fluoride is a systemic effect.
A. True B. False
36 www.aap.org/oralhealth/pact
Answer
True or False? The most important mechanism of action of fluoride is a systemic effect.
A. TrueB. False

37 www.aap.org/oralhealth/pact
Question #3
Which of the following is the most important function of
fluoride in caries prevention?
A. Fluoride enhances remineralization of tooth enamelB. Fluoride inhibits demineralization of tooth enamelC. Fluoride negatively affects the acid producing capabilities
of cariogenic bacteriaD. Fluoride displaces sugars from the surface of the teethE. All of the above are equally important

38 www.aap.org/oralhealth/pact
Answer
Which of the following is the most important function of
fluoride in caries prevention?
A. Fluoride enhances remineralization of tooth enamel. B. Fluoride inhibits demineralization of tooth enamel.C. Fluoride negatively affects the acid producing capabilities
of cariogenic bacteria.D. Fluoride displaces sugars from the surface of the teeth.E. All of the above are equally important.

39 www.aap.org/oralhealth/pact
Question #4
True or False? Fluoride supplements should be prescribed for high-risk children whose community water source is optimal.
A. TrueB. False

40 www.aap.org/oralhealth/pact
Answer
True or False? Fluoride supplements should be prescribed for high-risk children whose community water source is optimal.
A. True
B. False

41 www.aap.org/oralhealth/pact
Question #5
Which of the following is a symptom of mild fluorosis?
A. A white opacity on more than 50% of the toothB. Dark spots on the teethC. Brown, pitted, brittle enamelD. Chalk-like, lacy markings on the enamelE. None of the above

42 www.aap.org/oralhealth/pact
Answer
Which of the following is a symptom of mild fluorosis?
A. A white opacity on more than 50% of the toothB. Dark spots on the teethC. Brown, pitted, brittle enamelD. Chalk-like, lacy markings on the enamelE. None of the above

43 www.aap.org/oralhealth/pact
References
1. American Academy of Pediatric Dentistry. Guideline on Infant Oral Health Care. Council on Clinical Affairs. Reference Manual 2011. 33(6): 124-128. 2. American Academy of Pediatric Dentistry. Policy on Early Childhood Caries (ECC): Classifications, Consequences, and Preventive Strategies. Pediatr Dent 2011, 33(6): 47-49.3. American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride. Evidence-based clinical recommendations. JADA. August 1, 2006. 137(8): 1151-1159. 4. Berg J, Gerweck C, Hujoel PP, et al. Evidence-Based Clinical Recommendations Regarding Fluoride Intake from Reconstituted Infant Formula and Enamel Fluorosis. A Report of the American Dental Association Council on Scientific Affairs. JAMA. January 2011 vol. 142(1): 79-87. 5. Centers for Disease Control and Prevention. Recommendations for using fluoride to prevent and control dental caries in the United States. MMWR. 2001; 50(RR-14): 1-42. Available online at: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5014a1.htm. Accessed November 20, 2006.

44 www.aap.org/oralhealth/pact
References, continued
6. Centers for Disease Control and Prevention. Surveillance for Dental caries, Dental sealants, Tooth Retention, Edentulism, and Enamel Fluorosis-United States, 1988-1994 and 1999-2002. MMWR Surveillance Summaries. 2005. 54(03);1-44. Available online at: http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5403a1.htm. Accessed November 20, 2006. 7. Centers for Disease Control and Prevention. Using Fluoride to Prevent and Control Tooth Decay in the United States Fact Sheet, updated Jan 2011. www.cdc.gov/fluoridation/fact_sheets/fl_caries.htm8. Department of Health and Human Services. HHS Recommendation for Fluoride Concentration in Drinking Water for Prevention of Dental Caries. Federal Register. Vol. 76(9): January 13, 2011. 9. Krol DM. Dental caries, oral health, and pediatricians. Curr Probl Pediatr Adolesc Health Care. 2003; 33(8):253-270.10. Lewis CW, Milgrom P. Fluoride. Pediatr Rev. 2003; 24(10):327-336.11. Lewis DW, Ismail AI. Periodic health examination: 1995 update: 2. Prevention of dental caries. The Canadian Task Force on the Periodic Health Examination. Can Med Assoc J. 1995; 152(6): 836-46.

45 www.aap.org/oralhealth/pact
References, continued
12. Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride varnishes for preventing dental caries in children and adolescents. The Cochrane Database of Systematic Reviews 2002, Issue 1. Art. No.: CD002279. DOI: 10.1002/14651858.CD002279. This version first published online: 21 January 2002 in Issue 1, 2002. 13. Marinho VCC, Higgins JPT, Logan S, Sheiham A. Topical fluoride (toothpastes, mouthrinses, gels, or varnishes) for preventing dental caries in children and adolescents. The Cochrane Database of Systematic Reviews 2003, Issue 1. Art. No.: CD002782. DOI: 10.1002/14651858.CD002782. This version first published online: 20 January 2003 in Issue 1, 2003. 14. Oral health in America: A Report of the Surgeon General. Rockville MD: US Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health; 2000. Available online at: http://www.nidcr.nih.gov/DataStatistics/SurgeonGeneral. Accessed November 20, 2006. 15. Rozier RG, Adair S, Graham F, et al. Evidence-Based Clinical Recommendations on the Prescription of Dietary Fluoride Supplements for Caries Prevention. A Report of the American Dental Association Council on Scientific Affairs. JADA. December 2010 vol. 141(12): 1480-1489.

46 www.aap.org/oralhealth/pact
References, continued
16. US Environmental Protection Agency. 40 CFR Part 141.62. Maximum contaminant levels for inorganic contaminants. Code of Federal Regulations 2002:428-9. 17. US Environmental Protection Agency. 40 CFR Part 143.3 National secondary drinking water regulations. Code of Federal Regulations 2002; 614. 18. United States Preventive Services Task Force. Guide to clinical preventive services, 2010-2011. Available online at: http://www.ahrq.gov/clinic/pocketgd.htm. Accessed January 28, 2011.















![Fluoride toothpastes for preventing dental caries in ...neuron.mefst.hr/docs/katedre/znanstvena_metodologija/Fluoride... · [Intervention Review] Fluoride toothpastes for preventing](https://static.documents.pub/doc/80x56/5ac7a33f7f8b9aa3298b67ff/fluoride-toothpastes-for-preventing-dental-caries-in-intervention-review-fluoride.jpg)

