49
Focus on Central Line Bloodstream Infection Reduction Expanding Prevention Hospital Wide Ghinwa Dumyati, MD, FSHEA Associate Professor of Medicine University of Rochester Medical Center
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | jonas-casey |
| View: | 216 times |
| Download: | 3 times |
Focus on Central Line Bloodstream Infection Reduction
Expanding Prevention Hospital Wide
Ghinwa Dumyati, MD, FSHEAAssociate Professor of Medicine
University of Rochester Medical Center
Agenda
• Review the burden of central line associated bloodstream infections (CLABSI) outside the ICU
• Describe the components of a central line maintenance bundle
• Review the methods for implementing and sustaining CLABSI prevention hospital wide
• Questions
Why Expand CLABSI Prevention Hospital Wide?
• CLABSI rates outside the ICU are similar or higher than
the ICU
Range: 0.9-5.2 per 1,000 line days
• Excess variable cost ~ $ 33,000
• Crude in-hospital mortality: up to 28%
after controlling for confounders: CLABSI is associated with
2.27-fold (95% CI 1.15–4.46) increased risk of mortalityClimo M, et al. ICHE 2003; 24:942-945 Marshalls J, et al ICHE 2007;28: 905-909Son CH, et al. ICHE 2012:33; 869-874 Stevens V, et al. CMI 2013;20: O319-O324
CLABSI Outside the ICU• Device utilization ratio varies
In ICU: 0.52-0.77
Non-ICU: Medical-surgical: 0.08-0.27
Specialties: 0.25-0.53
Step down: 0.26-0.73
• Length of catheterization prior to infection
Median 10-17 days
• Type of central lines differ
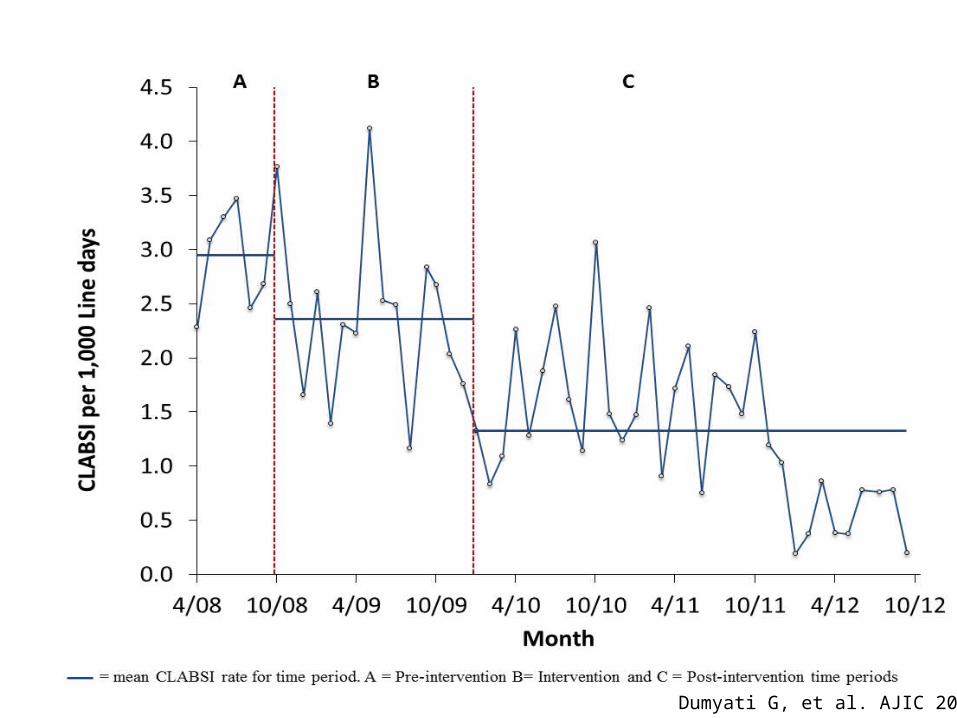
Dumyati G, et al. AJIC 2014; 42:723-30 Tedja R, et al. ICHE 2014; 35: 164-168Rhee Y, et al ICHE 2015; 36:424–430 Son CH, et al. ICHE 2012:33; 869-874
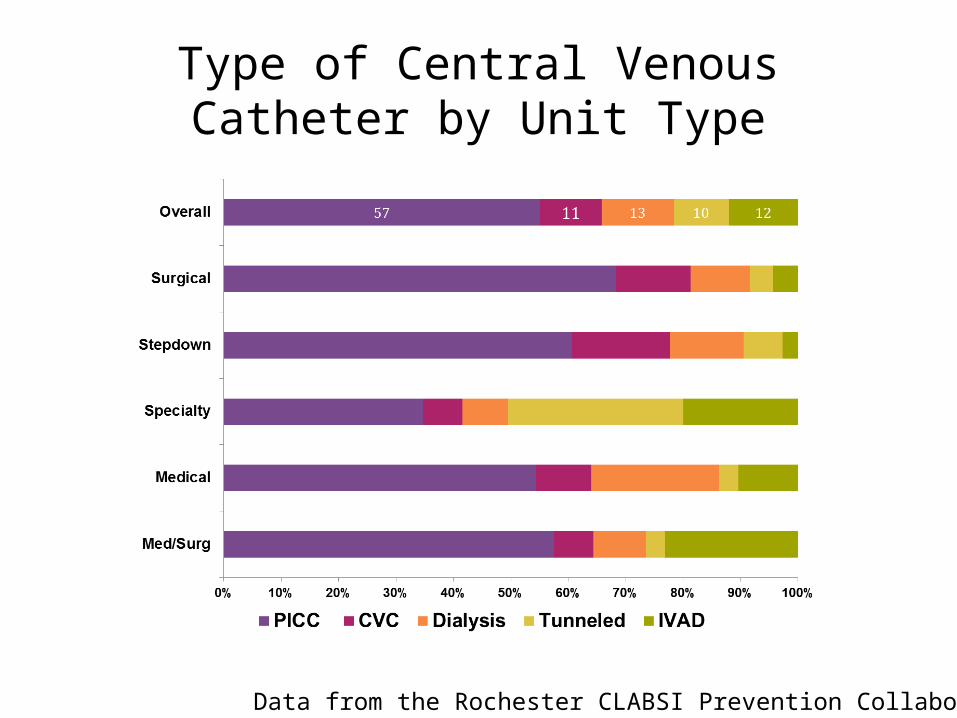
Type of Central Venous Catheter by Unit Type
Data from the Rochester CLABSI Prevention Collaborative
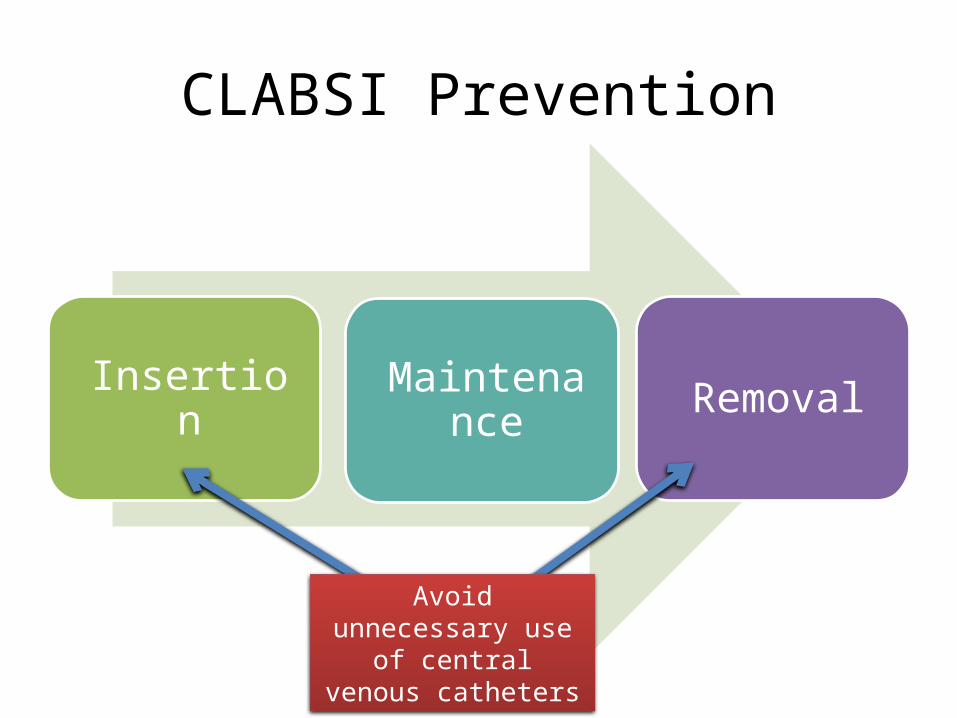
CLABSI Prevention
Insertion Maintenance Removal
Avoid unnecessary use of central venous
catheters
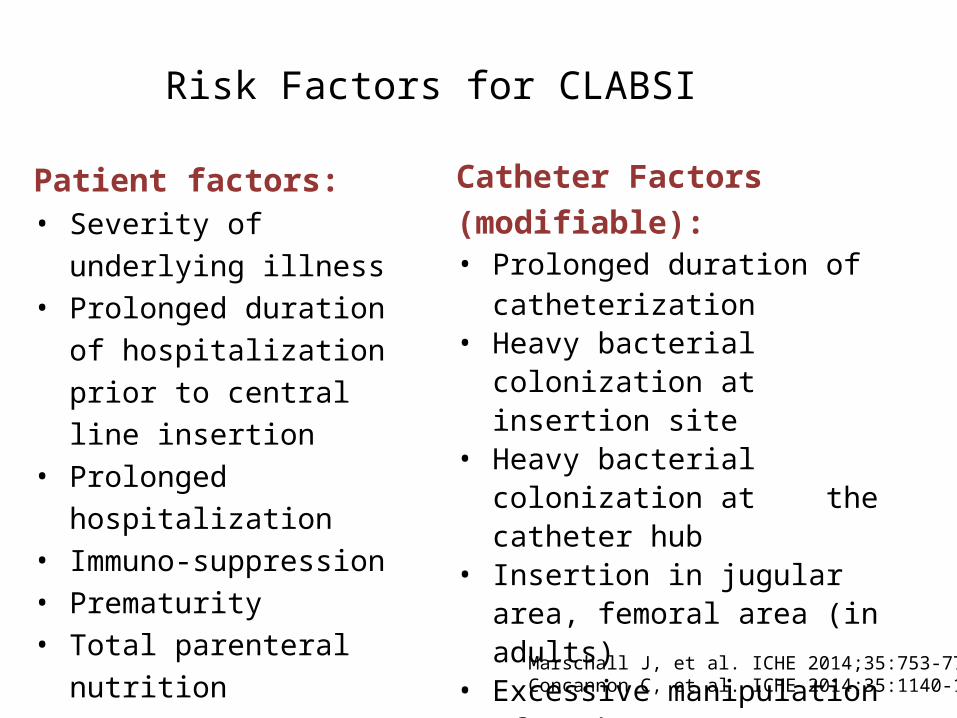
Risk Factors for CLABSI
Patient factors: • Severity of underlying illness• Prolonged duration of
hospitalization prior to central line insertion
• Prolonged hospitalization• Immuno-suppression• Prematurity• Total parenteral nutrition
Catheter Factors (modifiable):• Prolonged duration of
catheterization• Heavy bacterial colonization at
insertion site • Heavy bacterial colonization at the
catheter hub• Insertion in jugular area, femoral
area (in adults)• Excessive manipulation of catheter• Presence of multiple catheters
Marschall J, et al. ICHE 2014;35:753-771Concannon C, et al. ICHE 2014;35:1140-1146
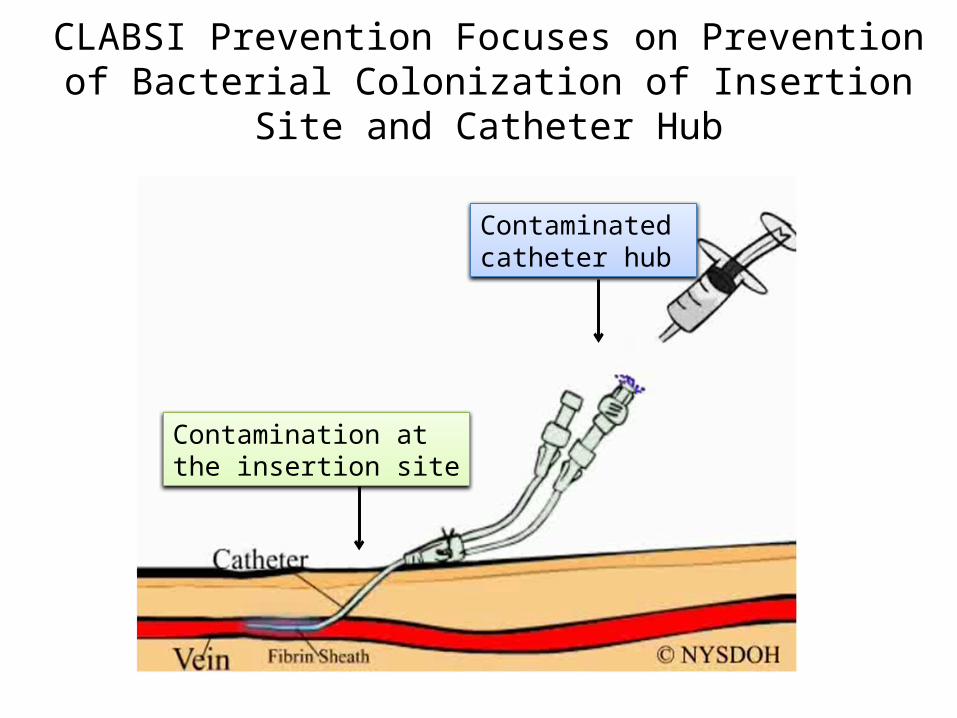
CLABSI Prevention Focuses on Prevention of Bacterial Colonization of Insertion Site and Catheter Hub
Contaminated catheter hub
Contamination at the insertion site

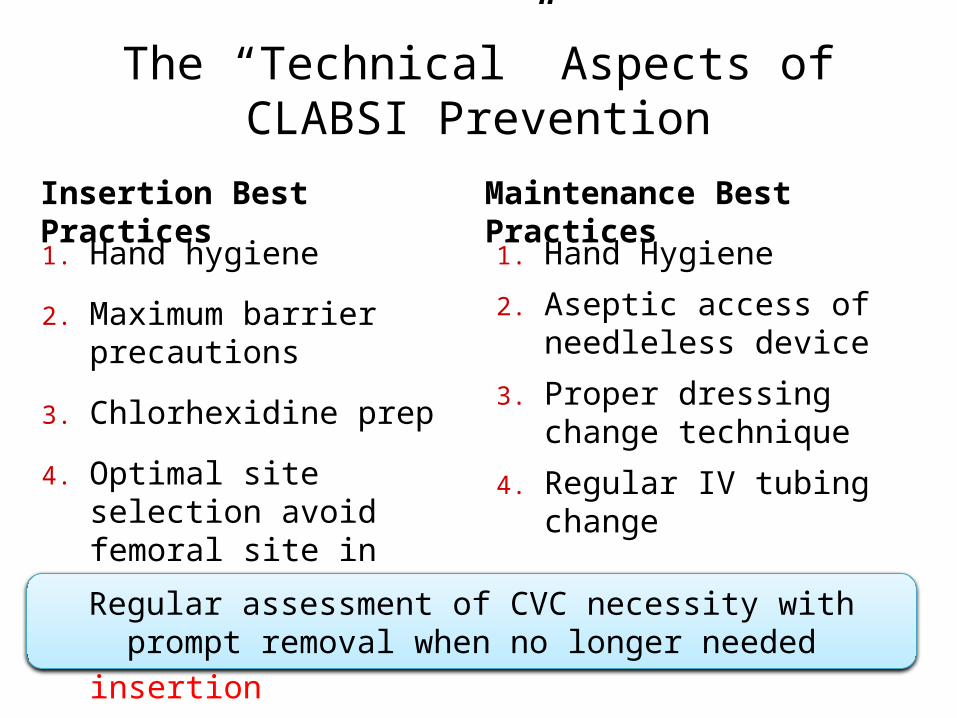
The “Technical” Aspects of CLABSI Prevention
Insertion Best Practices
1. Hand hygiene
2. Maximum barrier precautions
3. Chlorhexidine prep
4. Optimal site selection avoid femoral site in obese patients
5. Ultrasound guided insertion
Maintenance Best Practices
1. Hand Hygiene
2. Aseptic access of needleless device
3. Proper dressing change technique
4. Regular IV tubing change
Regular assessment of CVC necessity with prompt removal when no longer needed
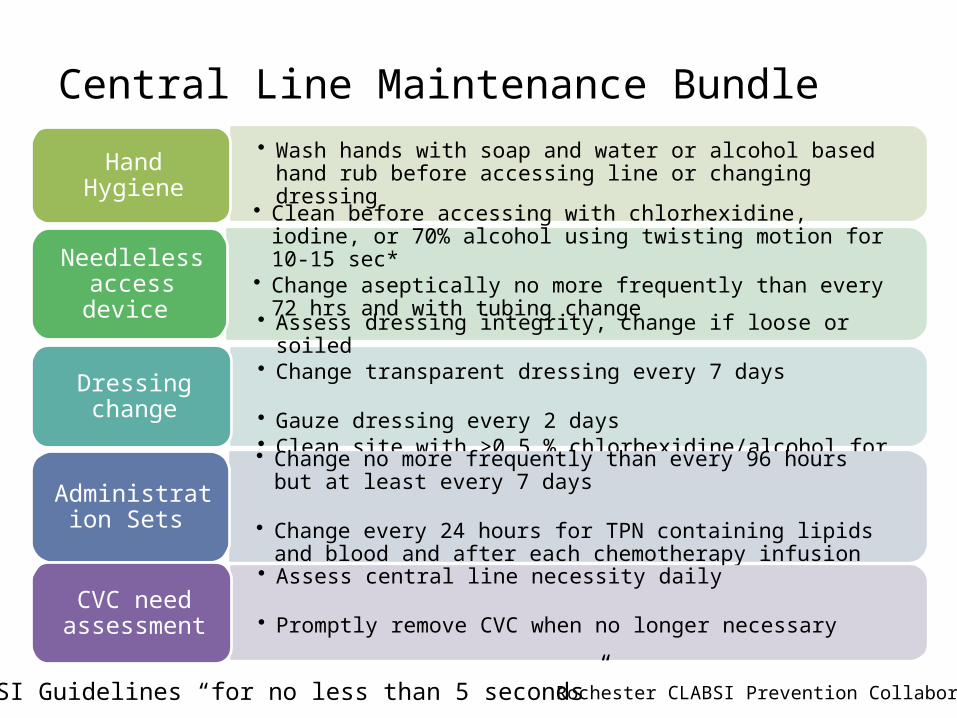
Central Line Maintenance Bundle• Wash hands with soap and water or alcohol based hand rub before
accessing line or changing dressing Hand Hygiene
• Clean before accessing with chlorhexidine, iodine, or 70% alcohol using twisting motion for 10-15 sec*
• Change aseptically no more frequently than every 72 hrs and with tubing change
Needleless access device
• Assess dressing integrity, change if loose or soiled • Change transparent dressing every 7 days • Gauze dressing every 2 days • Clean site with >0.5 % chlorhexidine/alcohol for 30 sec
Dressing change
• Change no more frequently than every 96 hours but at least every 7 days
• Change every 24 hours for TPN containing lipids and blood and after each chemotherapy infusion
Administration Sets
• Assess central line necessity daily• Promptly remove CVC when no longer necessary
CVC need assessment
* CLABSI Guidelines “for no less than 5 seconds” Rochester CLABSI Prevention Collaborative
Examples of Central Line Maintenance Bundles
• The joint Commission. Preventing Central Line-Associated Bloodstream Infection: Useful tools. An International Perspective, Nov 20,2013. Accessed June 17, 2015. http://www.joint comission.org/CLABSI toolkit
• Wheeler DS, et al. A Hospital-wide Quality-Improvement Collaborative to Reduce Catheter-Associated Bloodstream Infections. PEDIATRICS 2011; 128:e995-e997
• Bundy DG, et al. Preventing CLABSI among pediatric hematology/oncology inpatients: National collaborative results. PEDIATRICS 2014; 134: e1678-1685
Special “Technical” Approaches for Preventing CLABSI
1. Antiseptic or antimicrobial-impregnated catheters
2. Use chlorhexidine-impregnated sponge
3. Use an antiseptic-containing hub/connector protector to cover needleless access device
4. Use antibiotic locks
5. Chlorhexidine Bathing
To be used if “basic” prevention unsuccessful in reducing CLABSI rate
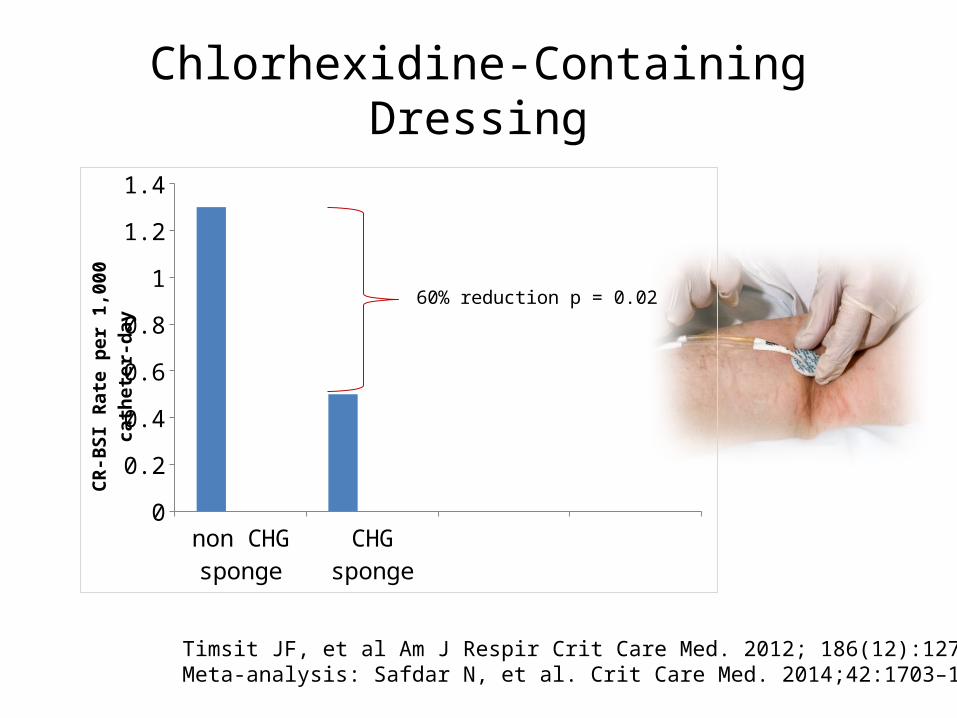
Chlorhexidine-Containing Dressing
non CHG sponge
CHG sponge0
0.2
0.4
0.6
0.8
1
1.2
1.4
CR-B
SI R
ate
per 1
,000
cat
hete
r-da
y
60% reduction p = 0.02
Timsit JF, et al Am J Respir Crit Care Med. 2012; 186(12):1272-1278Meta-analysis: Safdar N, et al. Crit Care Med. 2014;42:1703–1713
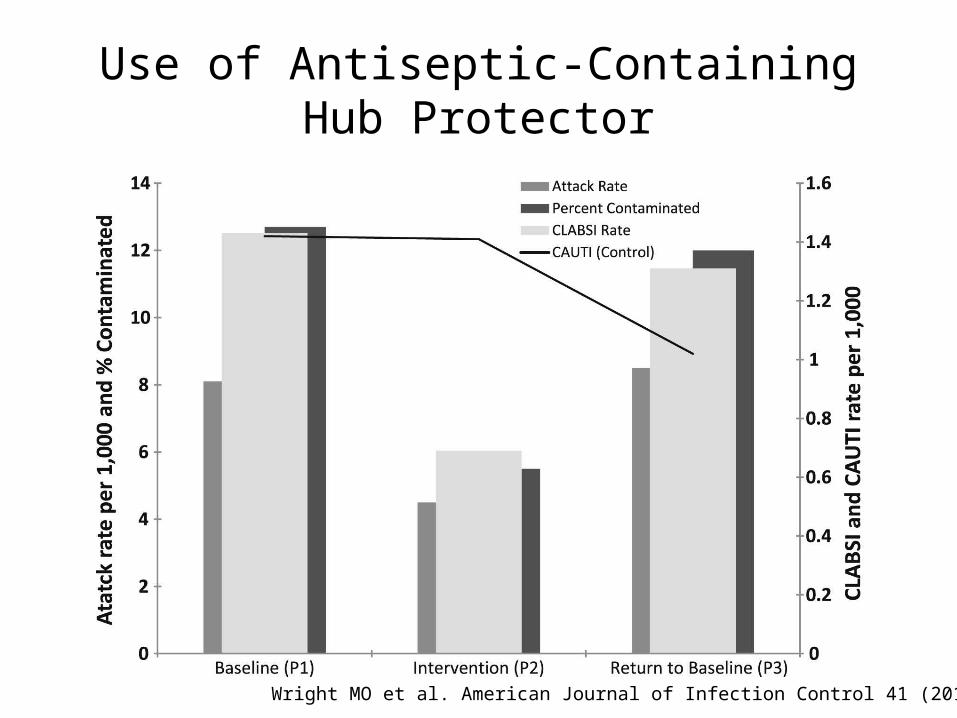
Use of Antiseptic-Containing Hub Protector
Wright MO et al. American Journal of Infection Control 41 (2013) 33-8
Chlorhexidine Bathing
• Most study support bathing in ICU– Meta-analysis of 12 ICU studies:
• Pooled odds ratio: 0.44 (95%CI 0.33-0.59; p<0.0001)
– 2 large multicenter studies showed reduction of bloodstream infections
• 1 single center study showed no benefit
O’horo JC, et al. ICHE 2012;33:257-267Climo MW, et al. N. Engl J Med 2013;368:533-42 Huang SS, et al. NEJM 2013;368:2255-2265Noto MJ, et al. JAMA 2015; 313:369-78
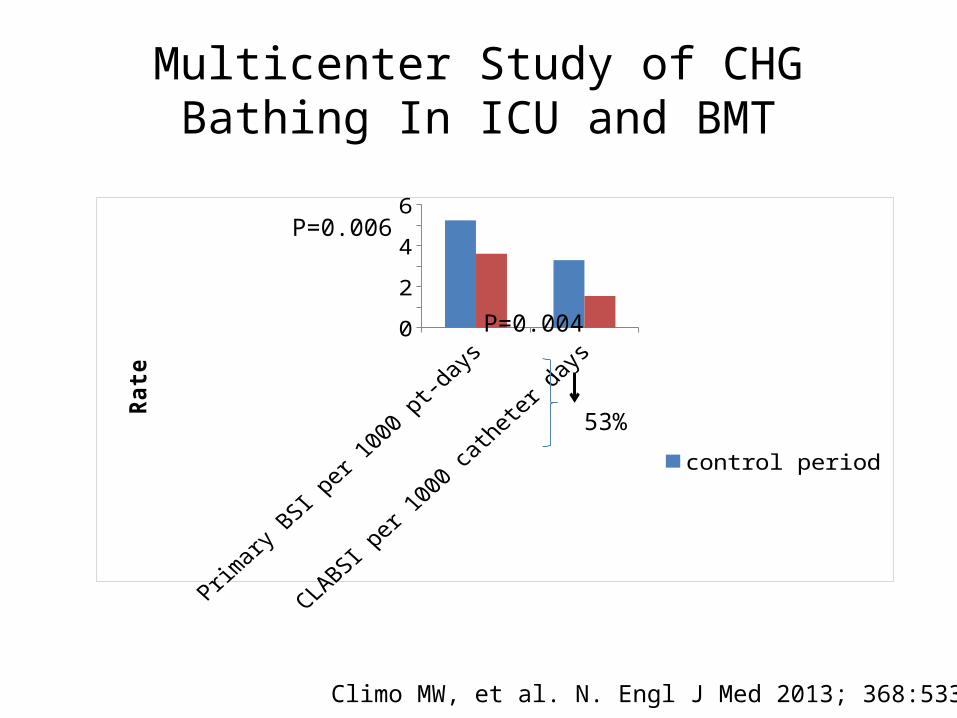
Multicenter Study of CHG Bathing In ICU and BMT
Climo MW, et al. N. Engl J Med 2013; 368:533-42
Primary BSI per 1000 pt-days
CLABSI per 1000 catheter days
0
1
2
3
4
5
6
control periodIntervention period
Rate
P=0.006
P=0.004
53%
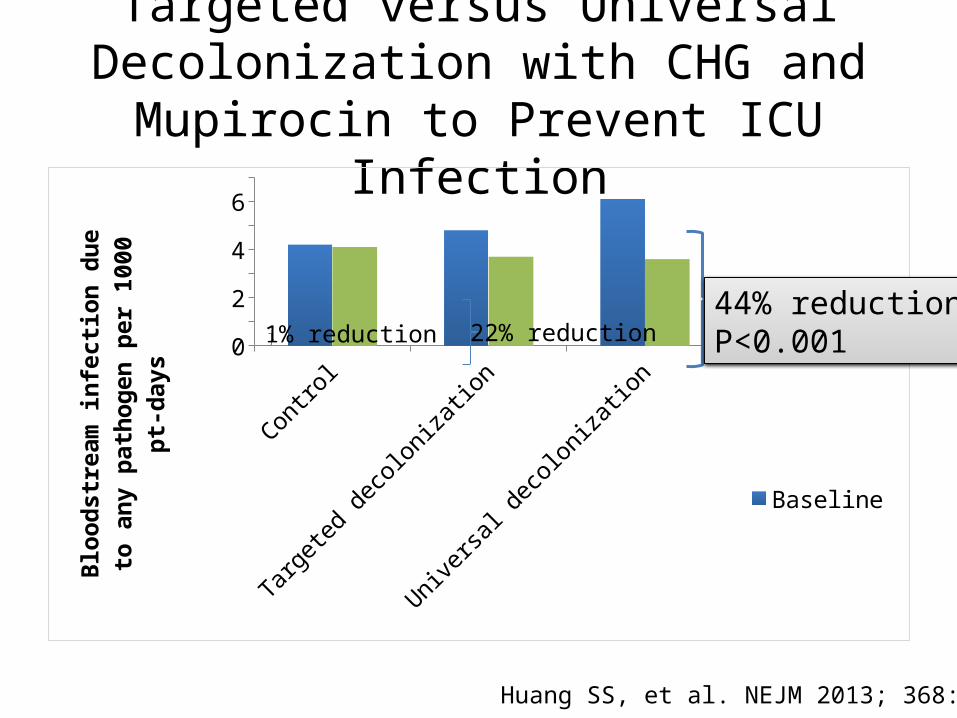
Targeted versus Universal Decolonization with CHG and Mupirocin to Prevent ICU
Infection
Control
Targeted deco
lonization
Universa
l deco
lonization
01234567
BaselineIntervention
Bloo
dstr
eam
infe
ction
due
to a
ny
path
ogen
per
100
0 pt
-day
s
Huang SS, et al. NEJM 2013; 368:2255
44% reductionP<0.00122% reduction1% reduction
CHG Bathing Hospital-Wide• Compliance with bathing:
– 90% in ICU – 58% in non-ICU
• Effect on CLABSI rates could not be demonstrated possibly due to – Low baseline rates– Enforcement of the CL insertion and maintenance
bundles
Rupp ME, et al. Infect Control and Hosp Epidemio 2102;33(11):1094-1100
CHG Bathing Outside the ICU• Active Bathing to Eliminate Infection (ABATE
Infection) – Cluster randomized trial to reduce multidrug
resistance organisms and healthcare associated infections in non-ICU
– Decolonization with CHG bathing and nasal mupirocin for MRSA +
– Results pending
https://clinicaltrials.gov/ct2/show/NCT02063867
WHERE TO START?
IMPLEMENTATION CLABSI PREVENTION HOSPITAL WIDE
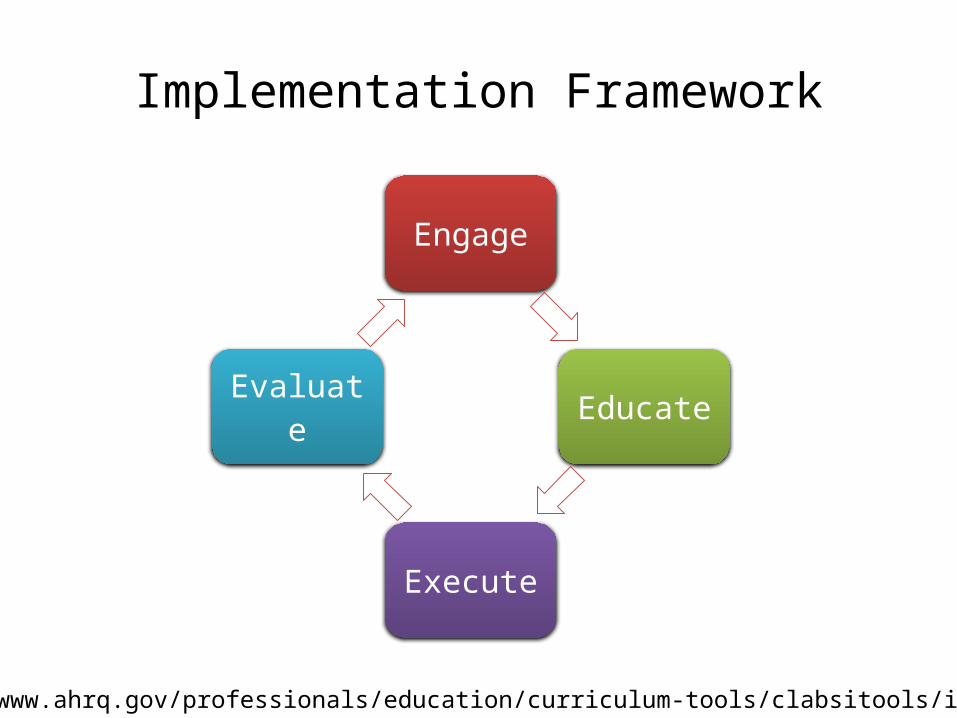
Implementation Framework
Engage
Educate
Execute
Evaluate
http://www.ahrq.gov/professionals/education/curriculum-tools/clabsitools/index.html
Implementing CLABSI Prevention Hospital WideWhere to Start?
• Obtain senior and nursing leadership support and buy-in– Approve time for oversight of the intervention– Approve cost for additional products– Provide accountability– Demonstrate that CLABSI prevention is a priority
Engage
• Identify one or two non-ICU wards with– High central venous catheter use– High CLABSI rate
• Identify and engage local champions on the ward– Front line nursing staff that can partner with infection
preventionist and/or IV access team– The champion will educate others, perform
observations, assess all nursing staff competency • Establish a CLABSI prevention multidisciplinary
team (or expand the ICU team)
Engage
Implementing CLABSI Prevention Hospital Wide
Assessment:• Current policies for catheter insertion and
maintenance hospital wideConsolidate if multiple policies exist
• The knowledge of front line staff of the CLABSI prevention policies
• Compliance with the current policiesPoint prevalence of CVC dressing observationsDocumentation of CVC insertion and maintenance
procedures/checklist
Educate
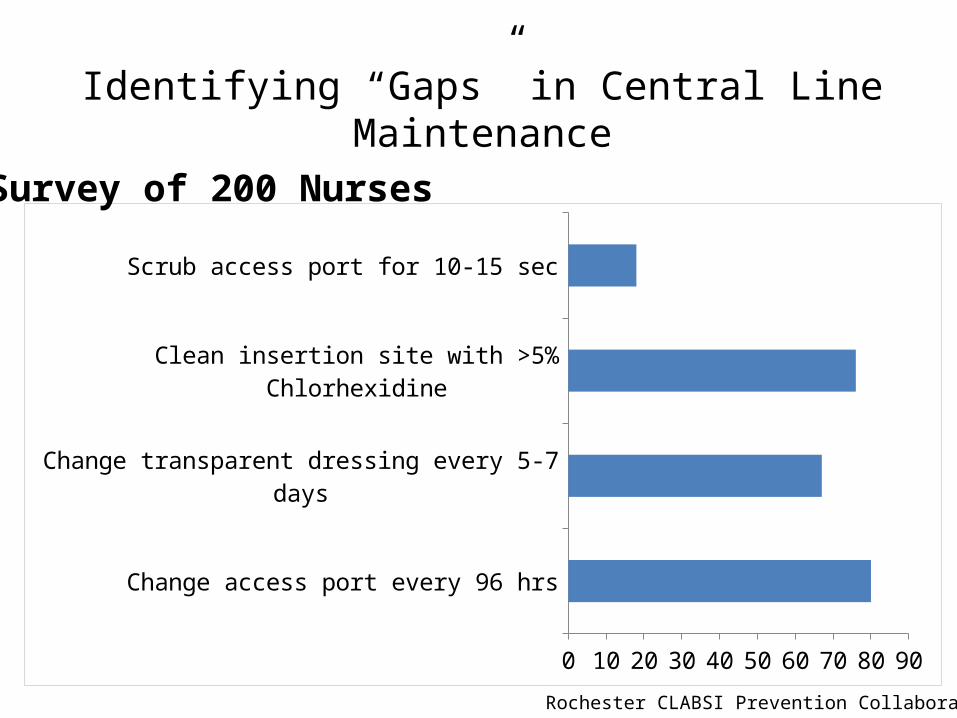
Identifying “Gaps” in Central Line Maintenance
Change access port every 96 hrs
Change transparent dressing every 5-7 days
Clean insertion site with >5% Chlorhexidine
Scrub access port for 10-15 sec
0 10 20 30 40 50 60 70 80 90
Survey of 200 Nurses
Rochester CLABSI Prevention Collaborative
Implementing CLABSI Prevention Hospital Wide
• Use multiple approaches for education:– Lectures– On-line course– One on one education– Assessment of staff competency
• Repeat education regularly and with any new products or change in policies
Educate
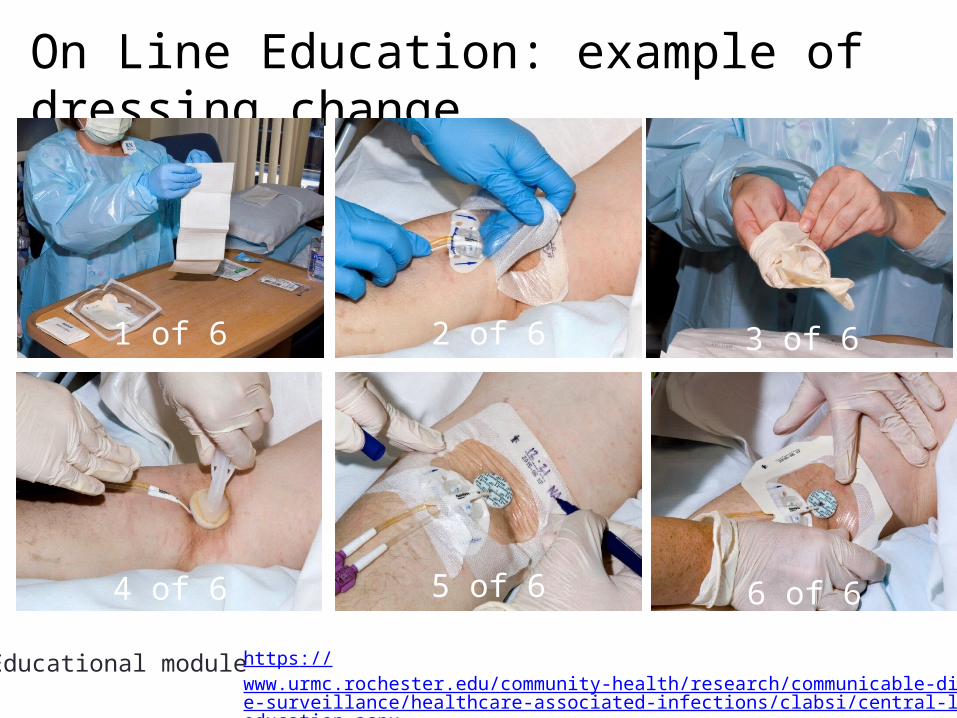
On Line Education: example of dressing change
1 of 6 2 of 6 3 of 6
4 of 6 5 of 6 6 of 6
Educational module https://www.urmc.rochester.edu/community-health/research/communicable-disease-surveillance/healthcare-associated-infections/clabsi/central-line-education.aspx
Implementing CLABSI Prevention Hospital Wide
• Identify your target goals:– CLABSI rate or SIR (unit level and hospital wide)
– Percent compliance with insertion and maintenance bundles
• Make your hospital wide CLABSI rate information a part of the organization score card
• Share at executive and board meetings
Execute
Be aggressive with your target goals
• Assess location and services inserting CVC in non ICU patientsEnsure that all staff inserting CVC are educated
Insertion checklist implemented outside the ICU setting, e.g. radiology, ED
• Assess the availability of supplies Insertion cart Supplies for dressing change (bundle into one package)Chlorhexidine sponge, securement device, alcohol caps (if used)
Implementing CLABSI Prevention Hospital Wide
Execute
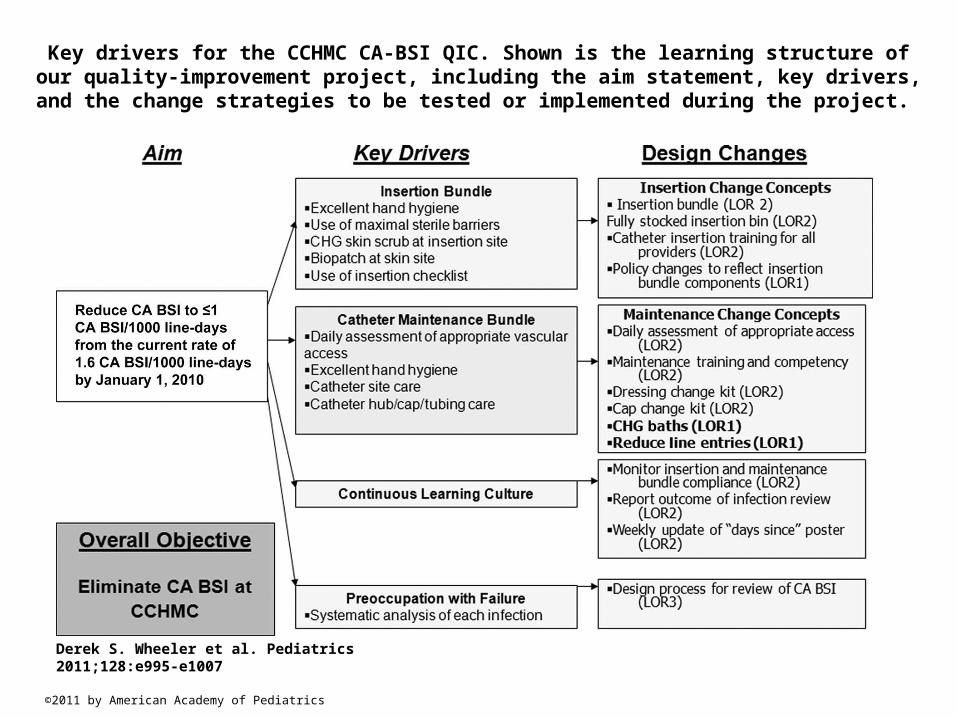
Key drivers for the CCHMC CA-BSI QIC. Shown is the learning structure of our quality-improvement project, including the aim statement, key drivers, and the change strategies to
be tested or implemented during the project.
Derek S. Wheeler et al. Pediatrics 2011;128:e995-e1007
©2011 by American Academy of Pediatrics
• Evaluate Process– Compliance with the insertion bundle– Compliance with the maintenance bundle
• Evaluate outcome– CLABSI rate– Number of patients affected each month– Days since last infection
Implementing CLABSI Prevention Hospital Wide
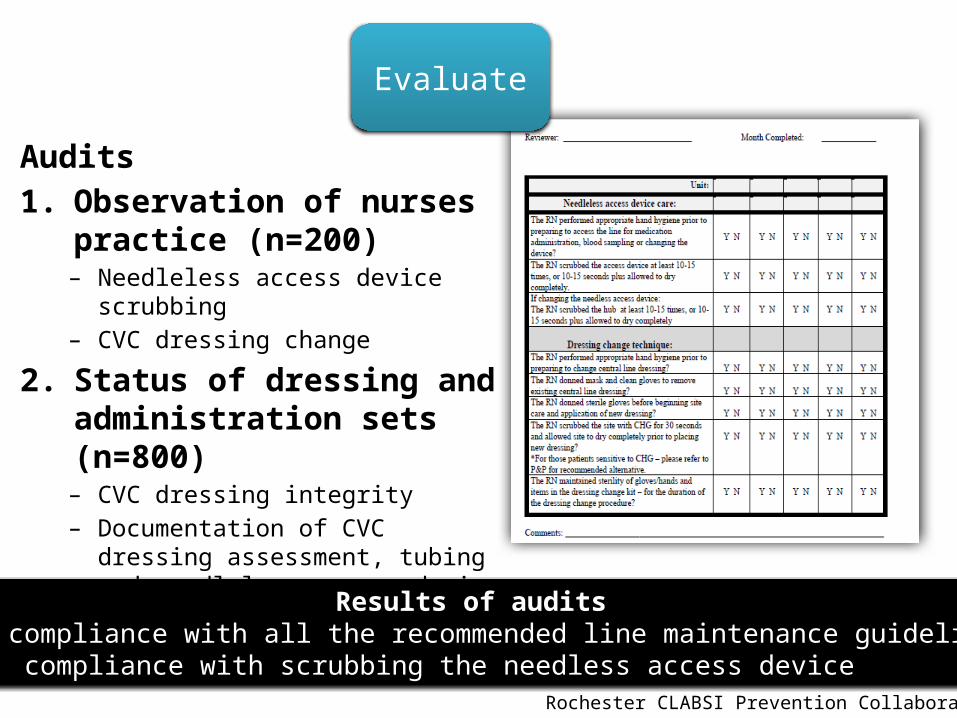
Audits1. Observation of nurses practice
(n=200)– Needleless access device scrubbing– CVC dressing change
2. Status of dressing and administration sets (n=800)– CVC dressing integrity– Documentation of CVC dressing
assessment, tubing and needleless access device date change
Results of audits>90% compliance with all the recommended line maintenance guidelines82% compliance with scrubbing the needless access device
Evaluate
Rochester CLABSI Prevention Collaborative
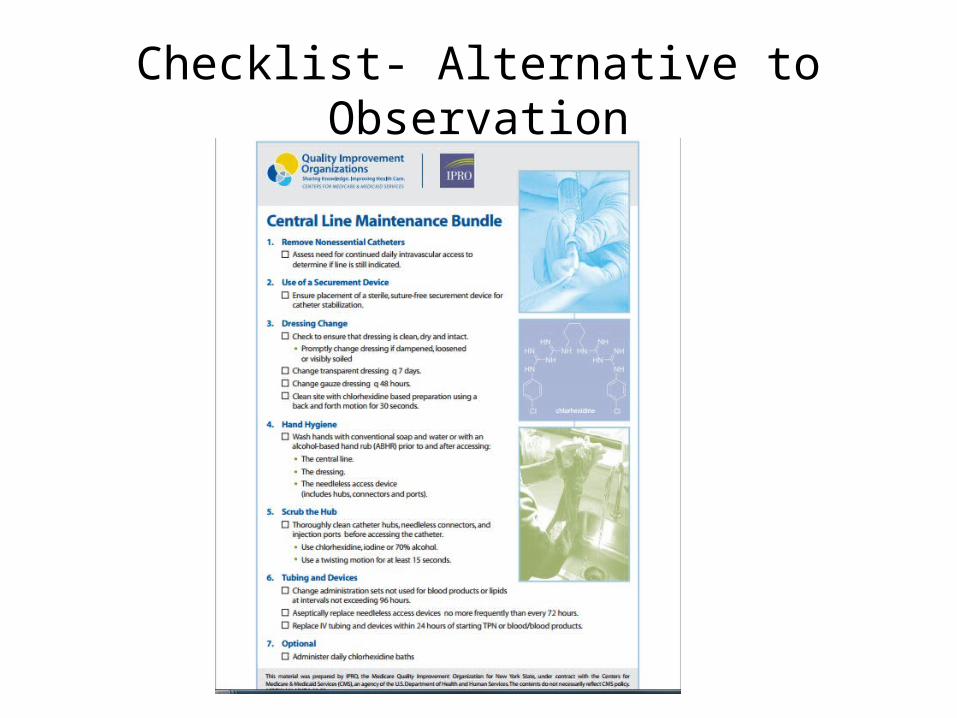
Checklist- Alternative to Observation
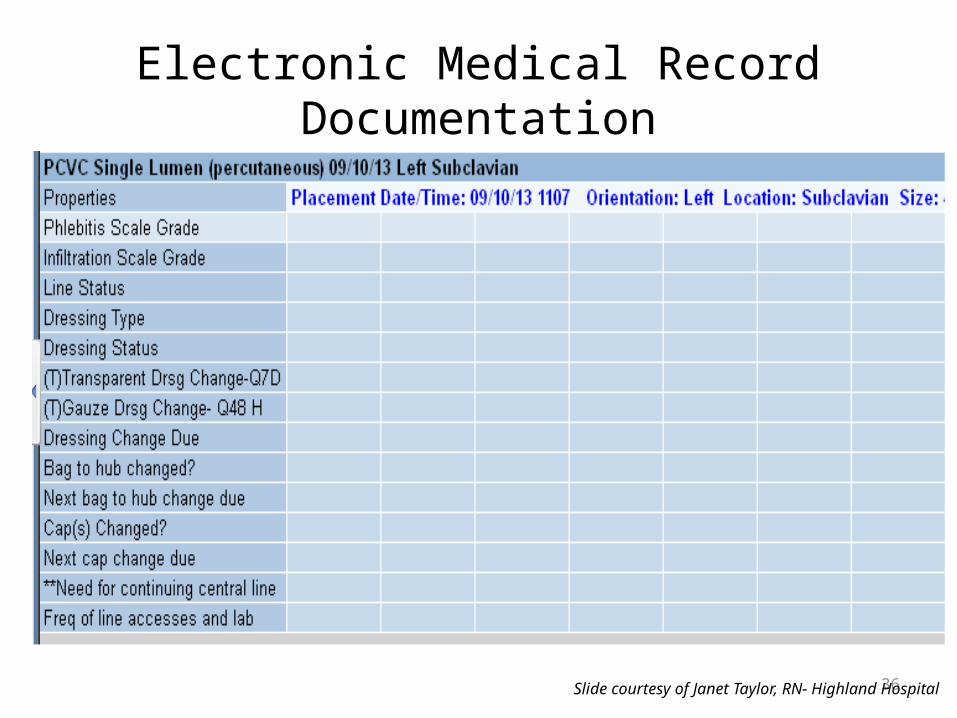
Electronic Medical Record Documentation
36Slide courtesy of Janet Taylor, RN- Highland Hospital
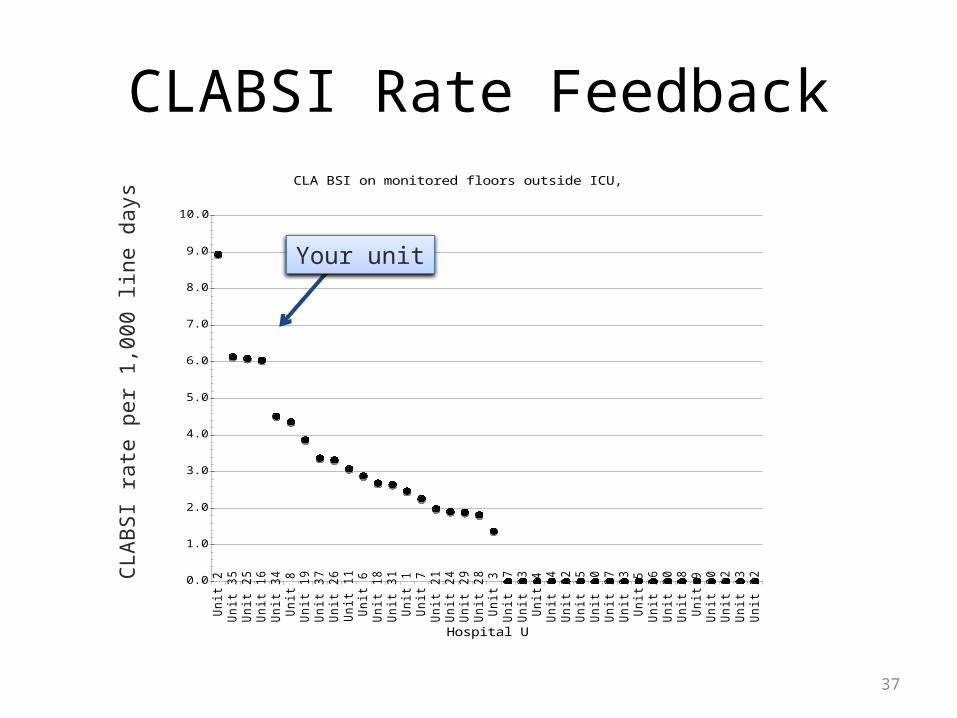
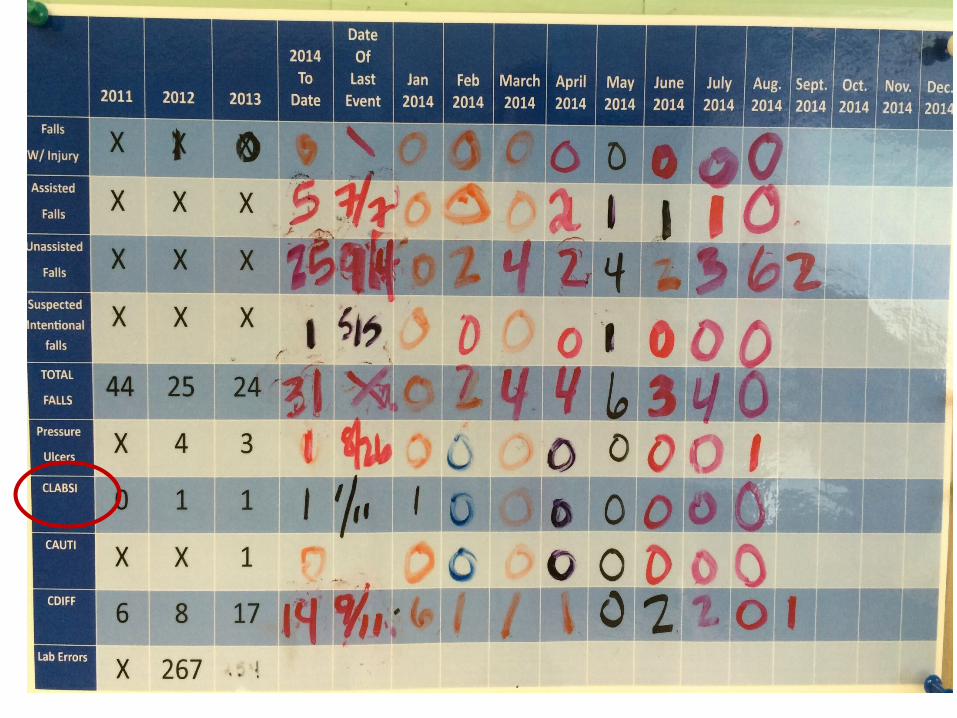
CLABSI Rate Feedback
37
CLA BSI on monitored floors outside ICU, April-June
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0U
nit 2
Unit 3
5U
nit 2
5U
nit 1
6U
nit 3
4U
nit 8
Unit 1
9U
nit 3
7U
nit 2
6U
nit 1
1U
nit 6
Unit 1
8U
nit 3
1U
nit 1
Unit 7
Unit 2
1U
nit 2
4U
nit 2
9U
nit 2
8U
nit 3
Unit 1
7U
nit 3
3U
nit 4
Unit 1
4U
nit 2
2U
nit 1
5U
nit 1
0U
nit 2
7U
nit 2
3U
nit 5
Unit 3
6U
nit 3
0U
nit 3
8U
nit 9
Unit 2
0U
nit 1
2U
nit 1
3U
nit 3
2
Hospital Unit
CL
A-B
SI p
er
10
00
Lin
e-D
ays
Your unit
CLAB
SI ra
te p
er 1
,000
line
day
s
Feedback
Bringing Prevention to the Patient Level
• Establish a Team to Brainstorm about each CLABSI case:– Nurses– Infection Preventionist– Intravenous access team– Unit nurse manager– Physicians
• Review:• WHY did it happen?
• WHAT can be done to prevent harm to the next patient?
39

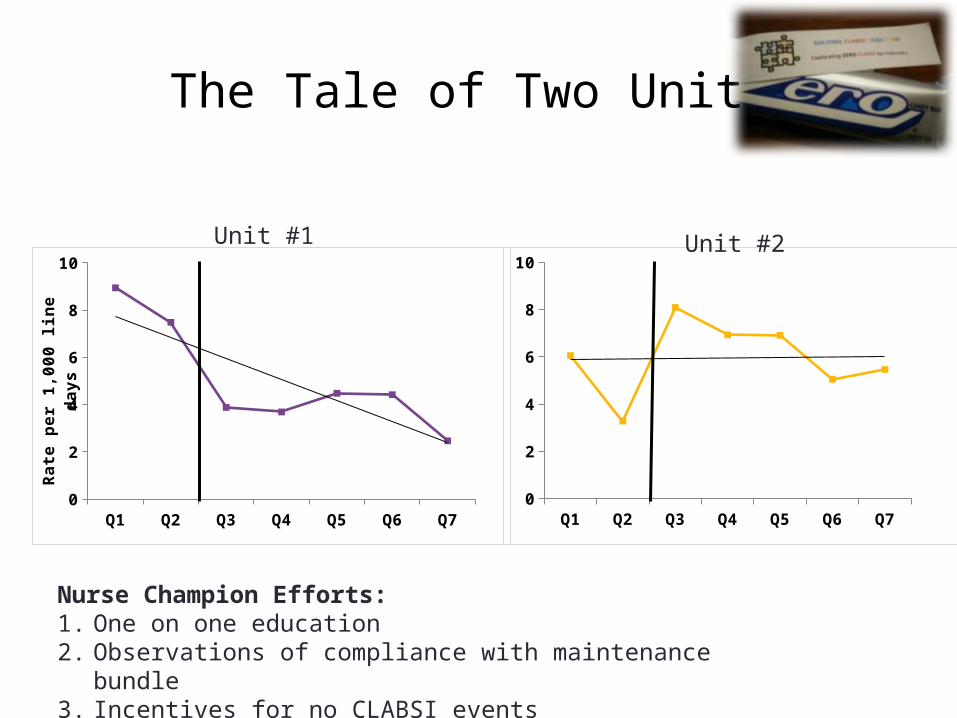
The Tale of Two Units
Q1 Q2 Q3 Q4 Q5 Q6 Q70
2
4
6
8
10
Q1 Q2 Q3 Q4 Q5 Q6 Q70
2
4
6
8
10
Rat
e p
er 1
,000
lin
e d
ays
Nurse Champion Efforts:1. One on one education2. Observations of compliance with maintenance bundle3. Incentives for no CLABSI events
Unit #1 Unit #2
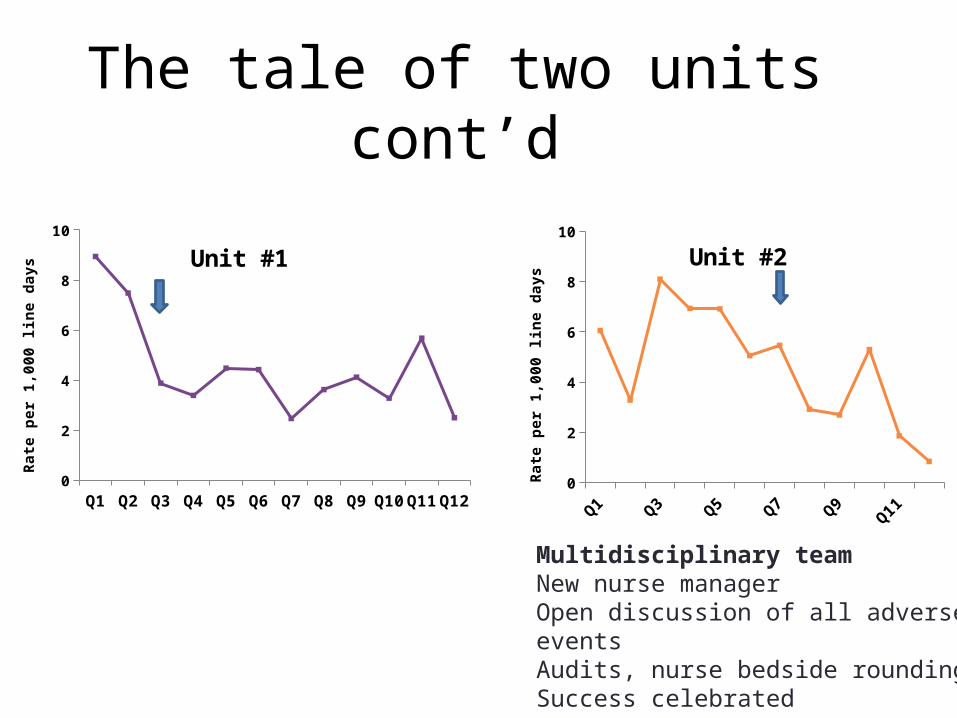
The tale of two units cont’d
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q120
2
4
6
8
10
Unit #2
Rate
per
1,0
00 li
ne d
ays
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q120
2
4
6
8
10
Unit #1
Rate
per
1,0
00 li
ne d
ays
Multidisciplinary teamNew nurse managerOpen discussion of all adverse events Audits, nurse bedside roundingSuccess celebrated
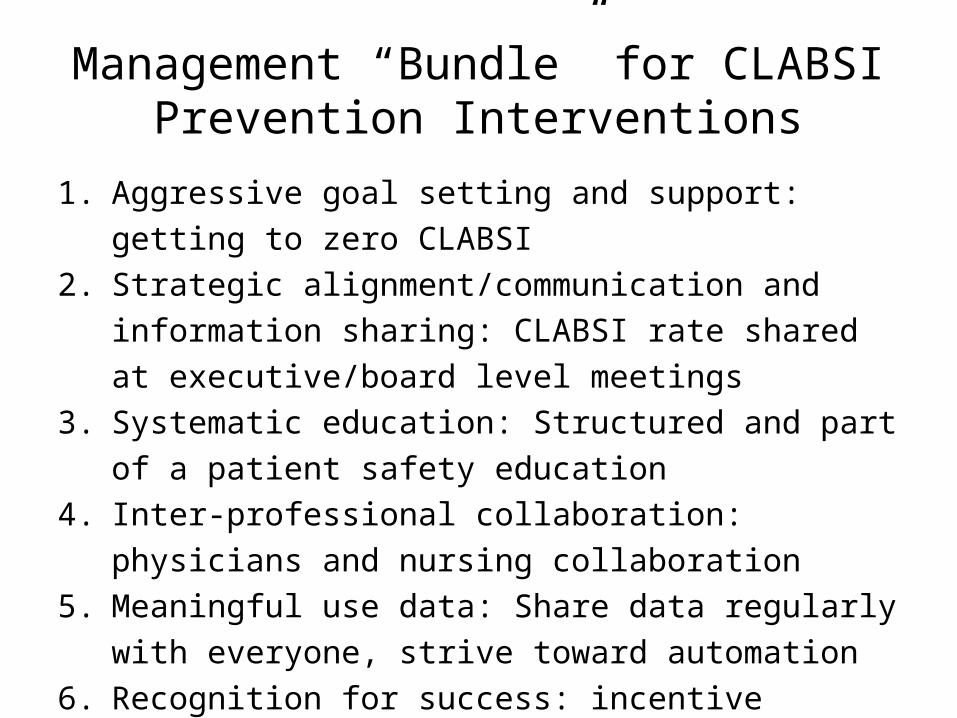
Management “Bundle” for CLABSI Prevention Interventions
1. Aggressive goal setting and support: getting to zero CLABSI2. Strategic alignment/communication and information
sharing: CLABSI rate shared at executive/board level meetings
3. Systematic education: Structured and part of a patient safety education
4. Inter-professional collaboration: physicians and nursing collaboration
5. Meaningful use data: Share data regularly with everyone, strive toward automation
6. Recognition for success: incentive compensation linked to the CLABSI prevention goals
Dumyati G, et al. AJIC 2014; 42:723-710
SUSTAINABILITY
Sustainability
• Improvement in safety culture• Ensure that all changes are included in policies and daily
work flow• Continue to repeat education due to staff turn over• Continue feedback of CLABSI data• Continued involvement of senior leadership
– Review of infection data and
– provide teams with the resources needed
• Alignment of the prevention project with the organizational goals
• Continue to support local champions and celebrate successPronovost PJ, et al.; BMJ, 2010; 340:c309
QUESTIONS?







![Business Case for ASP.pptx [Read-Only] · MAKING THE BUSINESS CASE FOR ASP: TAKING IT TO THE C-SUITE Gary R Kravitz MD FACP FIDSA FSHEA St. Paul Infectious Disease …](https://static.documents.pub/doc/80x56/5ac65e007f8b9aa0518e85cc/business-case-for-asppptx-read-only-the-business-case-for-asp-taking-it-to-the.jpg)









