“Focus on” : Linfedema e Lipedema Full Professor of General Surgery, Director Section & Research Center of Lymphatic Surgery, Lymphology, and Microsurgery. Operative Unit of General Surgery and Lymphatic Surgery. Postgraduate School of Alimentary Tract Surgery (Confederated with Pisa, Florence and Siena) University Polyclinic Hospital San Martino National Institute for Cancer Research, Genoa, Italy [email protected]www.lymphaticsurgery.org Corradino Campisi, MD, PhD, FACS
Transcript
“Focus on”: Linfedema e Lipedema
Full Professor of General Surgery, Director Section & Research Center of Lymphatic Surgery, Lymphology, and Microsurgery.
Operative Unit of General Surgery and Lymphatic Surgery.Postgraduate School of Alimentary Tract Surgery
(Confederated with Pisa, Florence and Siena) University Polyclinic Hospital San MartinoNational Institute for Cancer Research,
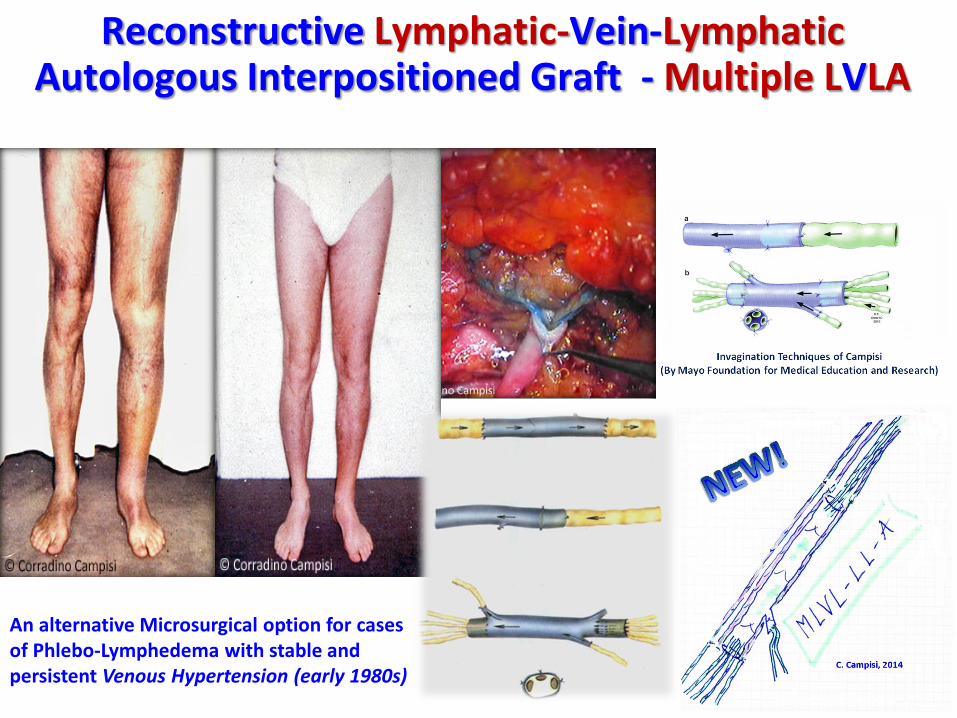
An alternative Microsurgical option for casesof Phlebo-Lymphedema with stable and persistent Venous Hypertension (early 1980s)
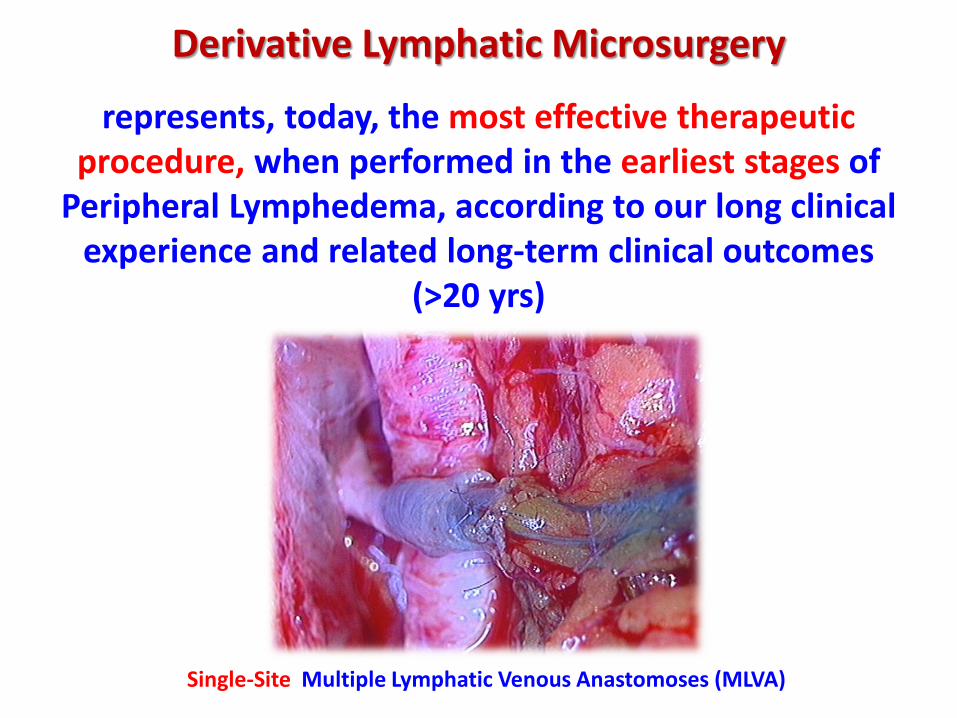
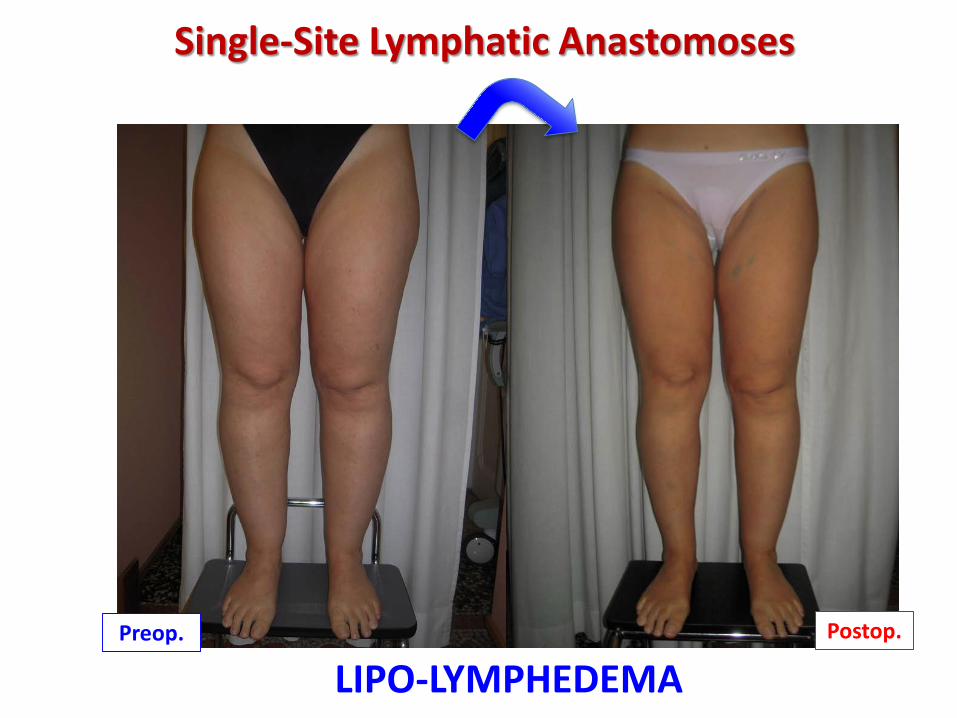
Single-Site Lymphatic Anastomoses
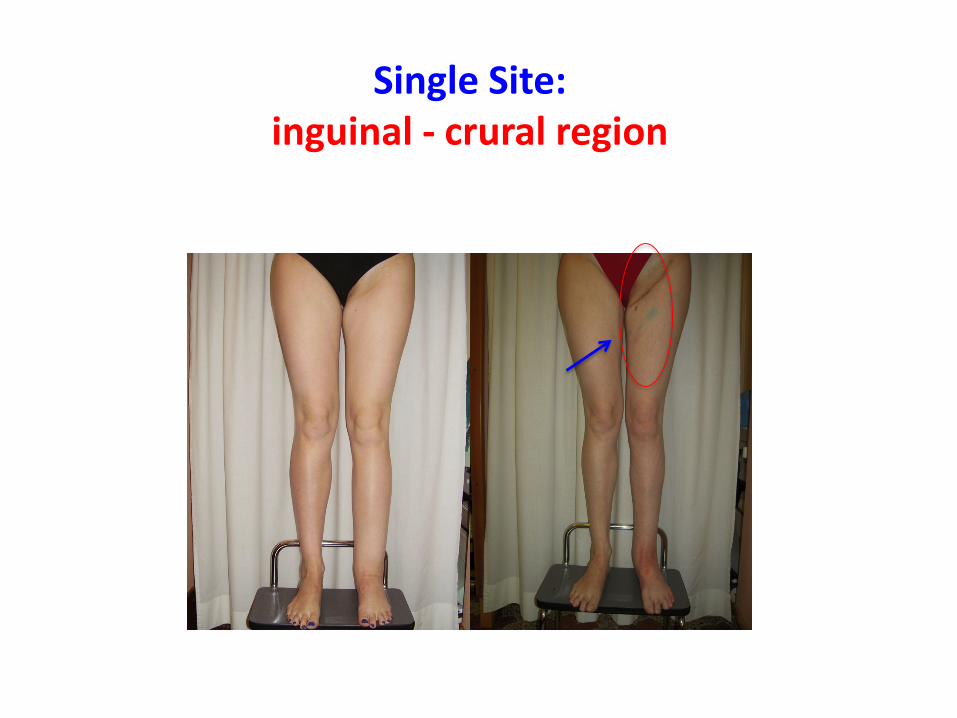
• MLVA or MLVLA are performed at a single adaptable incision (inguinal-crural region or upper- middle third of the volar surface of the arm ) using both superficial and deep lymphatic vessels, previously stained with blue dye
Campisi CC, Ryan M, Boccardo F, Campisi C. A single-site technique of multiple lymphatic venous anastomoses for the treatment of peripheral lymphedema: Long term clinical outcomes. J. Reconstr Microsurg, 2016 Jan;32(1):42-9.
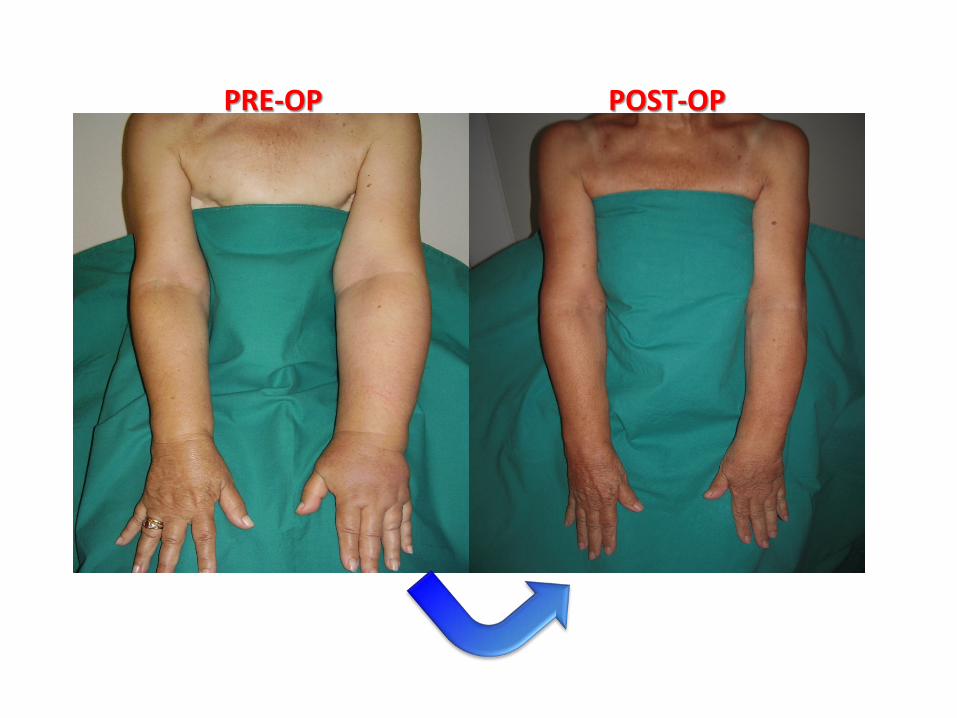
Single Site:upper-middle third of the volar surface
of the upper arm
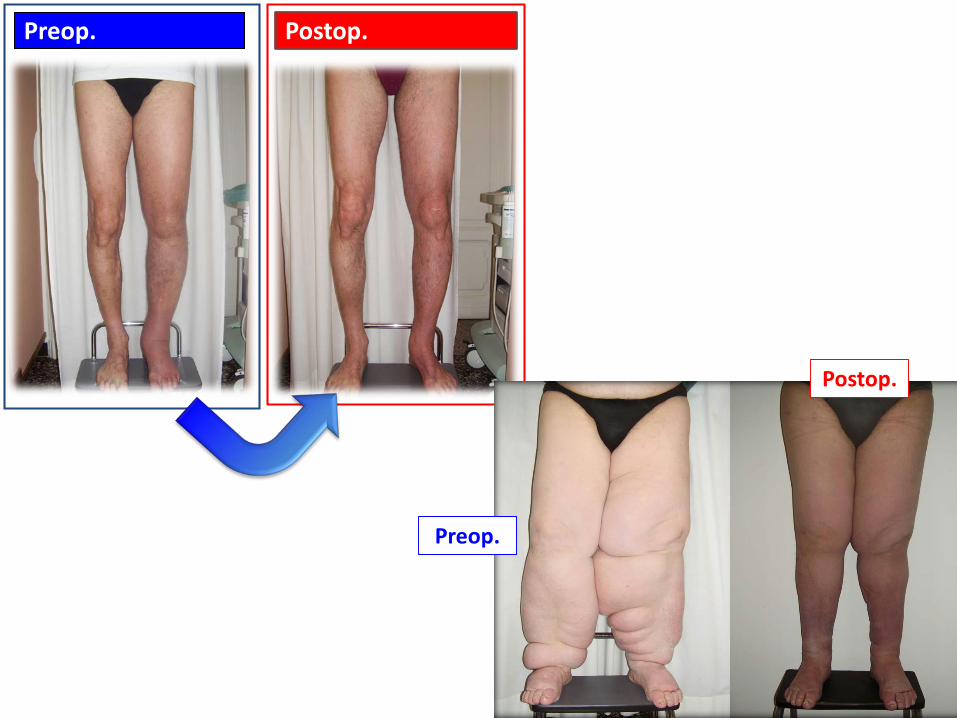
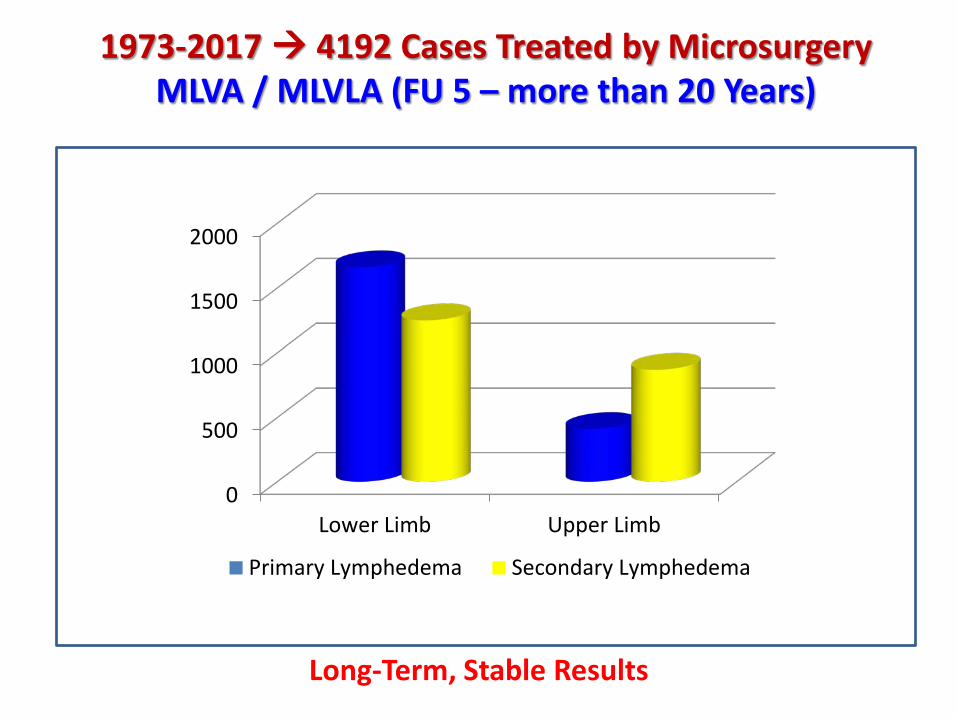
Long-Term StableResults
PRE-OP POST-OP
PRE-OP POST-OP
Single Site:inguinal - crural region
Long-TermStableResults
Preop.
Postop.
Preop. Postop.
Preop.
Postop.
The rationale behind the single-site approach is twofold …
Single-Site Lymphatic Anastomoses
Campisi CC, Ryan M, Boccardo F, Campisi C. A single-site technique of multiple lymphatic venous anastomoses for the treatment of peripheral lymphedema: Long term clinical outcomes. J. Reconstr Microsurg. 2016 Jan;32(1):42-9.
Single-Site Lymphatic Anastomoses
1) Lowered Infection Risk:
- A single incision means less surface area exposed to microbes
- The incision is made proximally:
In our experience, infections are more likely to occur distally, starting in the hands and feet. This is most likely due to the poor mobilization of immune cells to lymph nodes due to chronic lymph stasis
Campisi CC, Ryan M, Boccardo F, Campisi C. A single-site technique of multiple lymphatic venous anastomoses for the treatment of peripheral lymphedema: Long term clinical outcomes. J. Reconstr Microsurg. 2016 Jan;32(1):42-9.
Single-Site Lymphatic Anastomoses
2) Increased Vessel Caliber
- Larger Lymphatic vessels are easier to use for anastomoses
Campisi CC, Ryan M, Boccardo F, Campisi C. A single-site technique of multiple lymphatic venous anastomoses for the treatment of peripheral lymphedema: Long term clinical outcomes. J. Reconstr Microsurg. 2016 Jan;32(1):42-9.
2) Increased Vessel Caliber
- Larger Lymphatic vessels allow a greater flow of lymph through each anastomosis
- Multiple LVA are created in close proximity to vein valves; thus the suction induced by these valves is sufficient to overcome the differential pressure
- Lymph is immediately pulled into the vein, preventing thrombosis of the anastomoses
Single-Site Lymphatic Anastomoses
Campisi CC, Ryan M, Boccardo F, Campisi C. A single-site technique of multiple lymphatic venous anastomoses for the treatment of peripheral lymphedema: Long term clinical outcomes. J. Reconstr Microsurg. 2016 Jan;32(1):42-9.
Single Incision
Single Operating Microscope
Multiple Anastomoses(Superficial & Deep)
Multiple Long-Term Effectiveness
Single-Site Multiple LVA
Corradino Campisi & Coll., Genoa, Italy 2017
‘TIMING’: EARLYApplication = LONG-TERM
results!
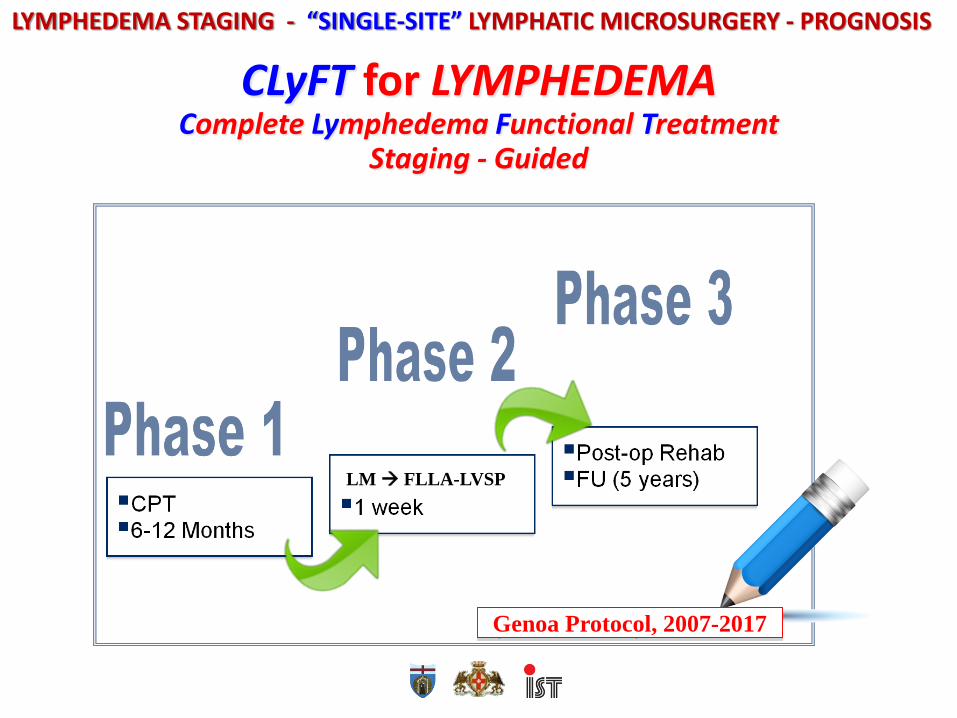
Genoa Protocol, 2007-2017
CLyFT for LYMPHEDEMAComplete Lymphedema Functional Treatment
F = Fast (Length of Surgery: 15’-20’ / Anastomosis – 60’-150’ / in total)I = Increasing (both Lymph TransportCapacity & Patient Turnover)E = Effective (Significant Edema Volume Reduction in the Long-Term)R = Recovering (High-Grade Clinical & QoL Restoration)A = Aesthetic (Remarkable & StableCosmetic Results) E = Economic (Low-Cost Surgeryrequiring only 1 OpMi & 2 Surgeons, according to the available budget in everyhospital, in every area of the world!)
MLVA / MLVLA Microsurgery
=F.I.E.R.A.E.Microsurgery
NEW ADVANCES
For Advanced Stages of Lymphedema (IIB-III) LM is able to give onlypartial results.
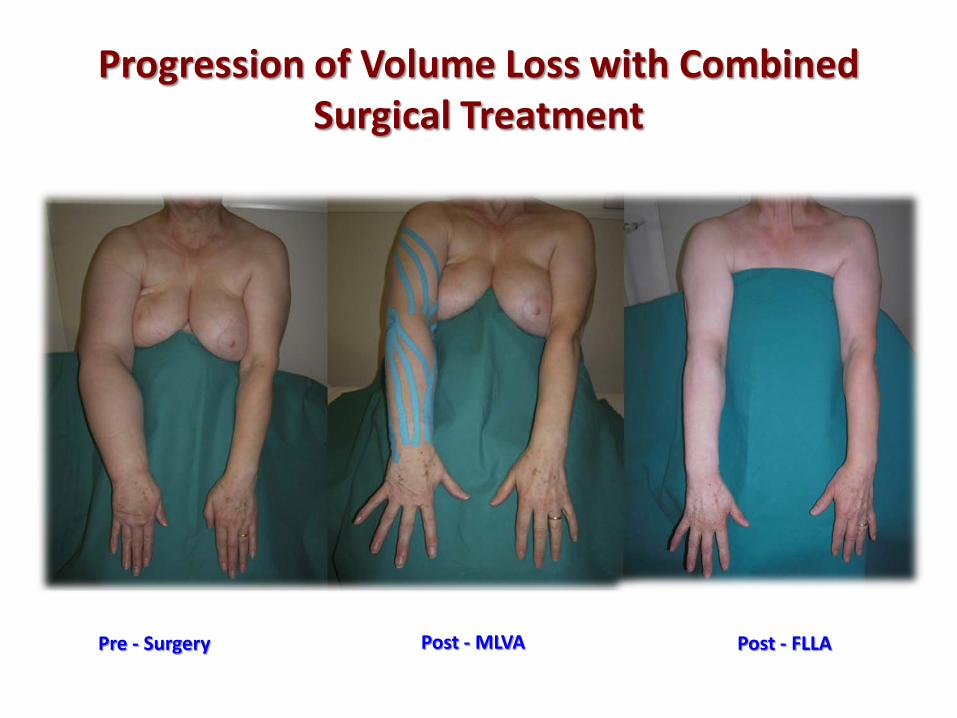
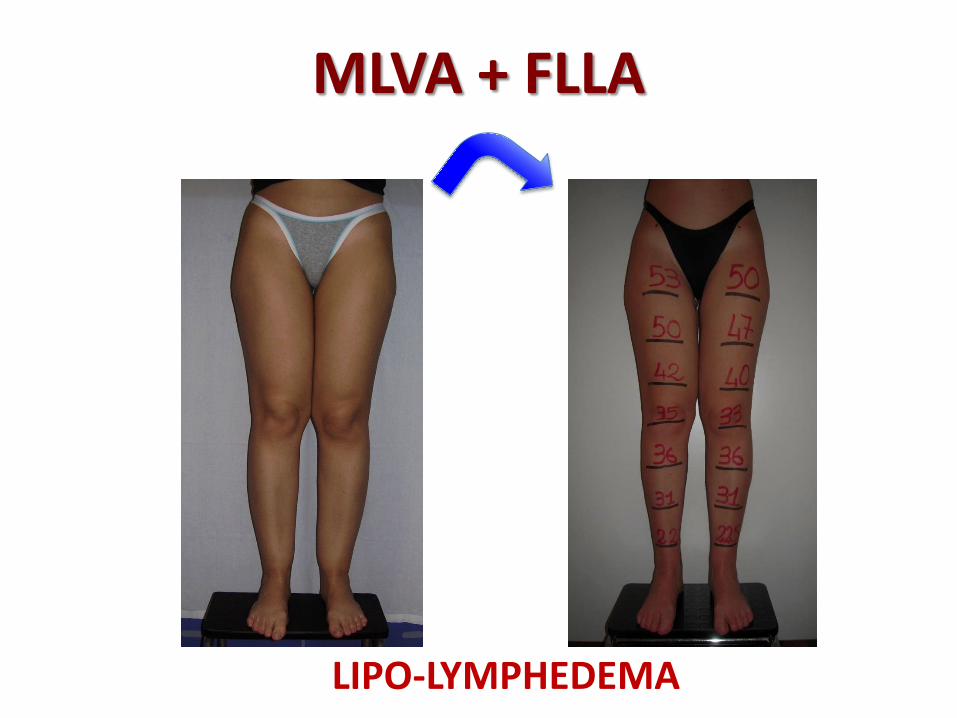
That is why we developed a “Lymph Vessel Sparing Procedure (2012)”, with Liposuction-Like technique (i.e. Selective Liposuction) that is called:
FIBRO-LIPO-LYMPH-ASPIRATION (FLLA-LVSP)
The aim of the new FLLA-LVSP procedure is to remove the remaining excess fibro-adipose tissue of the lymphedematous limb
previously treated by MLVA.
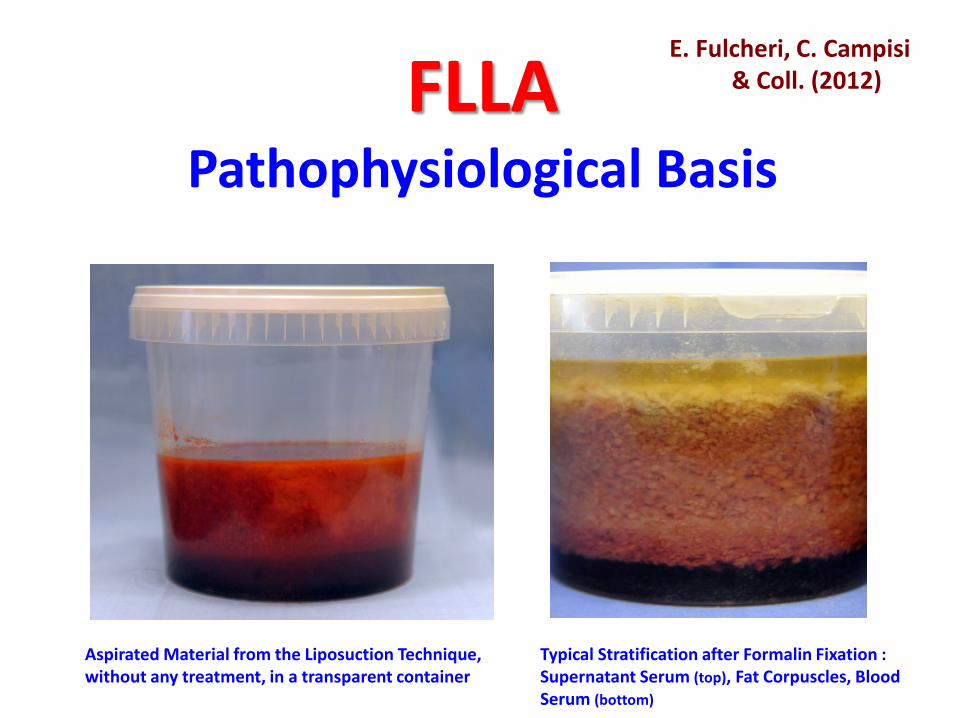
FLLAPathophysiological Basis
Aspirated Material from the Liposuction Technique, without any treatment, in a transparent container
Thickened and Fibrous Connective Tissue with small Blood and Lymphatic Vessels E.E. 10 - 20x
CD 31 CD 34
Lymphatic Vessels and Walls with Markedly thickened Peri-Adventitial MatrixThe endothelium of the vessel is clearly positive to immunohistochemical staining with antibodies to CD31. IIC - CD31, 10x and to antibodies
EARLY ‘Single-Site’ MLVA Application Avoids LATER Surgery !‘TIMING’!
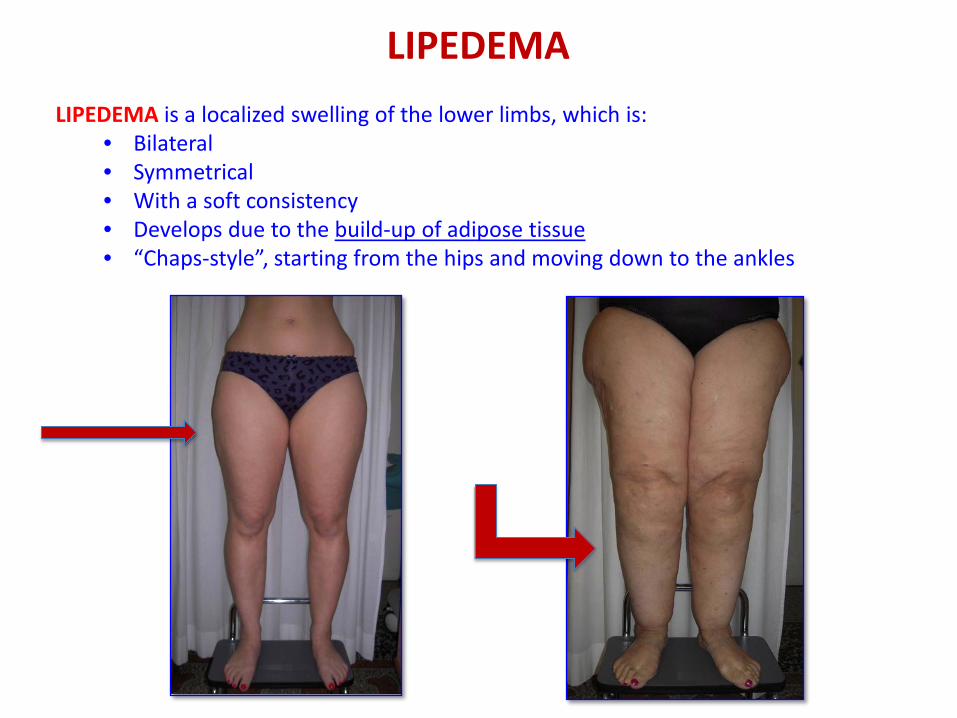
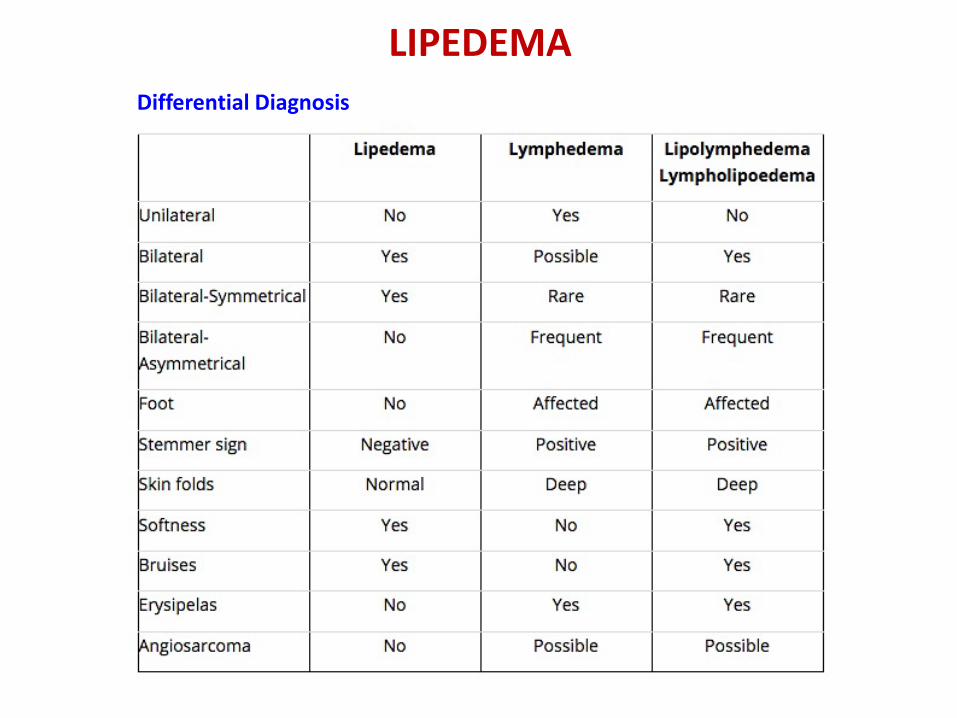
LIPEDEMALIPEDEMA is a localized swelling of the lower limbs, which is:
• Bilateral• Symmetrical• With a soft consistency• Develops due to the build-up of adipose tissue• “Chaps-style”, starting from the hips and moving down to the ankles
LIPEDEMAPATHOPHYSIOLOGY
Trigger Mechanism: Micro-angiopathy takes place in the adipose tissue leading to higher protein permeability and, at the same time, more fragile capillaries.
As a consequence of higher permeability, high-protein content fluid builds up in the surrounding cell area.
The skin bruises easily due to higher capillary fragility.
Skin resiliency is severely decreased, while skin compliance (skin stiffness, expressed in mmHg, measured with a special device) is increased: The skin loses its helping role as a venous pump in the lower extremities Macrophages, which can scavenge plasma proteins outside lymphatic vessels, are
rarely present in adipose tissues
The lymphatic system eventually becomes overloaded, leading to the onset of lipo-lymphedema in the later stages of disease
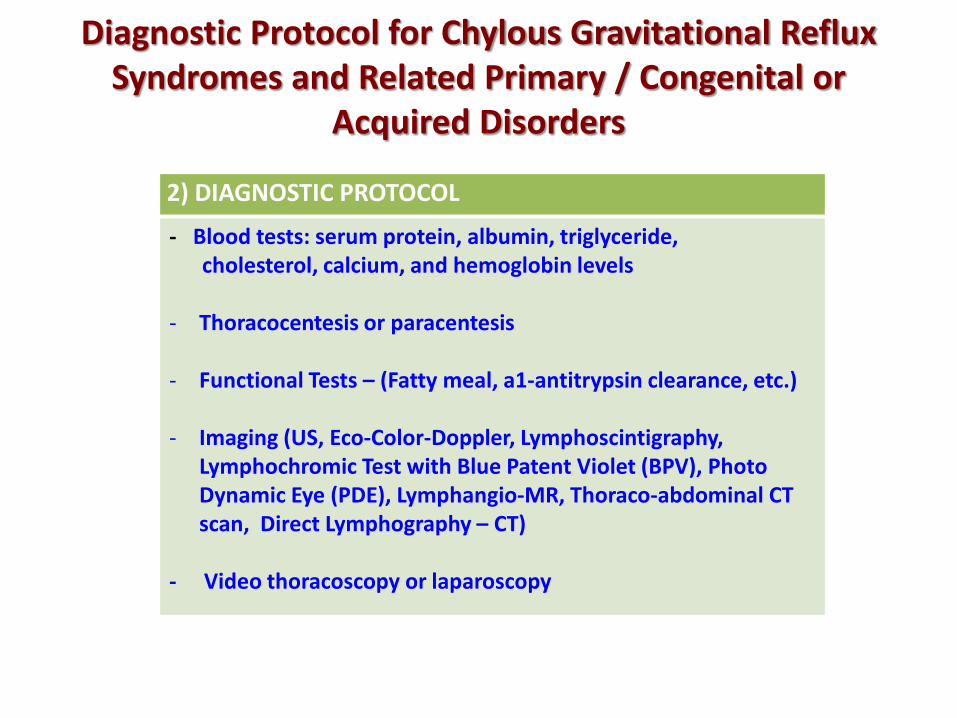
- Imaging (US, Eco-Color-Doppler, Lymphoscintigraphy, Lymphochromic Test with Blue Patent Violet (BPV), Photo Dynamic Eye (PDE), Lymphangio-MR, Thoraco-abdominal CT scan, Direct Lymphography – CT)
- Video thoracoscopy or laparoscopy
Angio - CT
MRI
Lymphography
Lymphangio - MR
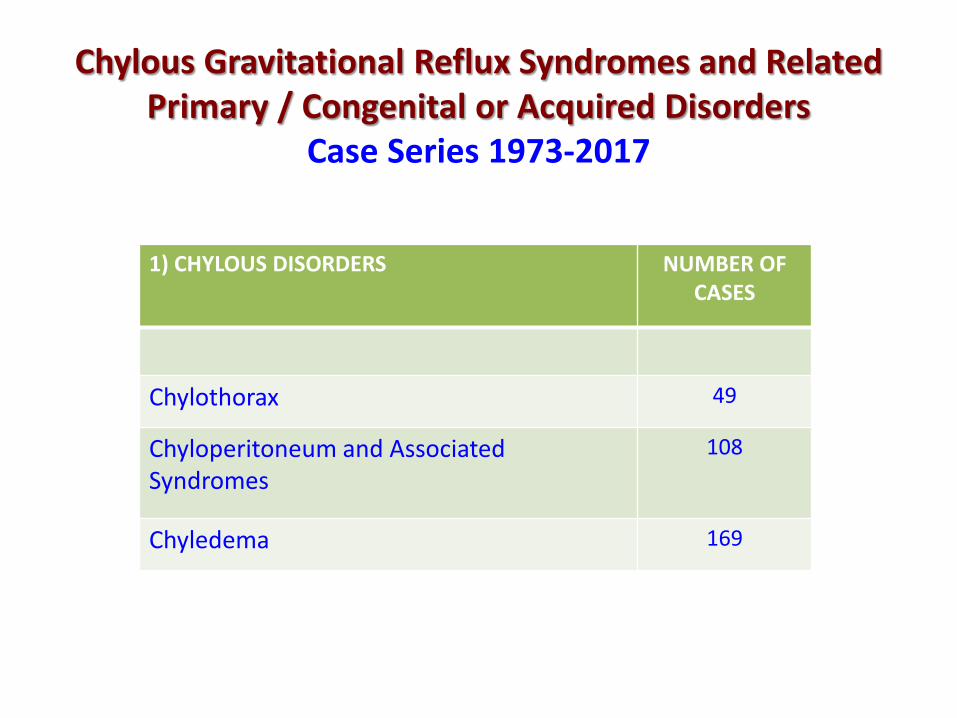
Treatment Protocol for Chylous Gravitational Reflux Syndromes and Related Primary / Congenital or
Acquired Disorders
3) BASIC MEDICAL TREATMENT PROTOCOL • Nutritional Management
Total Parenteral Nutrition – Hypo-alipid and Hyper-proteic Diet(Medium Chain Triglycerides - MCT) / Chiloil*
• Drug Management
Somatostatin Analogs / Octreotide
Antiobiotics
• Drainage of the Effusion (Thoracocentesis / Paracentesis)
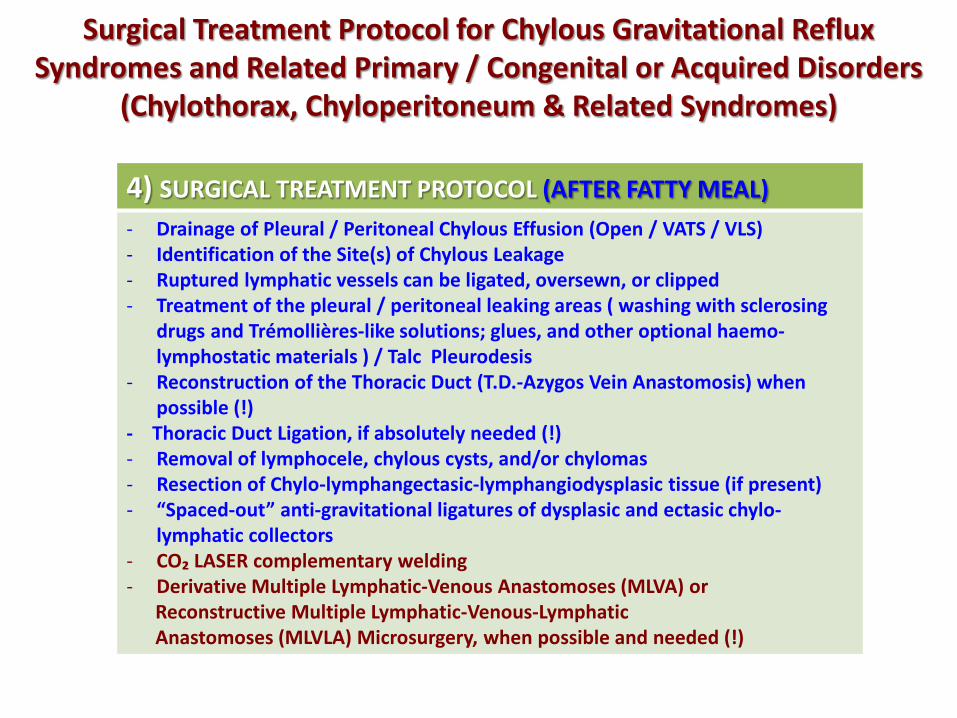
Surgical Treatment Protocol for Chylous Gravitational Reflux Syndromes and Related Primary / Congenital or Acquired Disorders
(Chylothorax, Chyloperitoneum & Related Syndromes)
4) SURGICAL TREATMENT PROTOCOL (AFTER FATTY MEAL)- Drainage of Pleural / Peritoneal Chylous Effusion (Open / VATS / VLS)- Identification of the Site(s) of Chylous Leakage- Ruptured lymphatic vessels can be ligated, oversewn, or clipped- Treatment of the pleural / peritoneal leaking areas ( washing with sclerosing
drugs and Trémollières-like solutions; glues, and other optional haemo-lymphostatic materials ) / Talc Pleurodesis
- Reconstruction of the Thoracic Duct (T.D.-Azygos Vein Anastomosis) when possible (!)
- Thoracic Duct Ligation, if absolutely needed (!)- Removal of lymphocele, chylous cysts, and/or chylomas- Resection of Chylo-lymphangectasic-lymphangiodysplasic tissue (if present)- “Spaced-out” anti-gravitational ligatures of dysplasic and ectasic chylo-
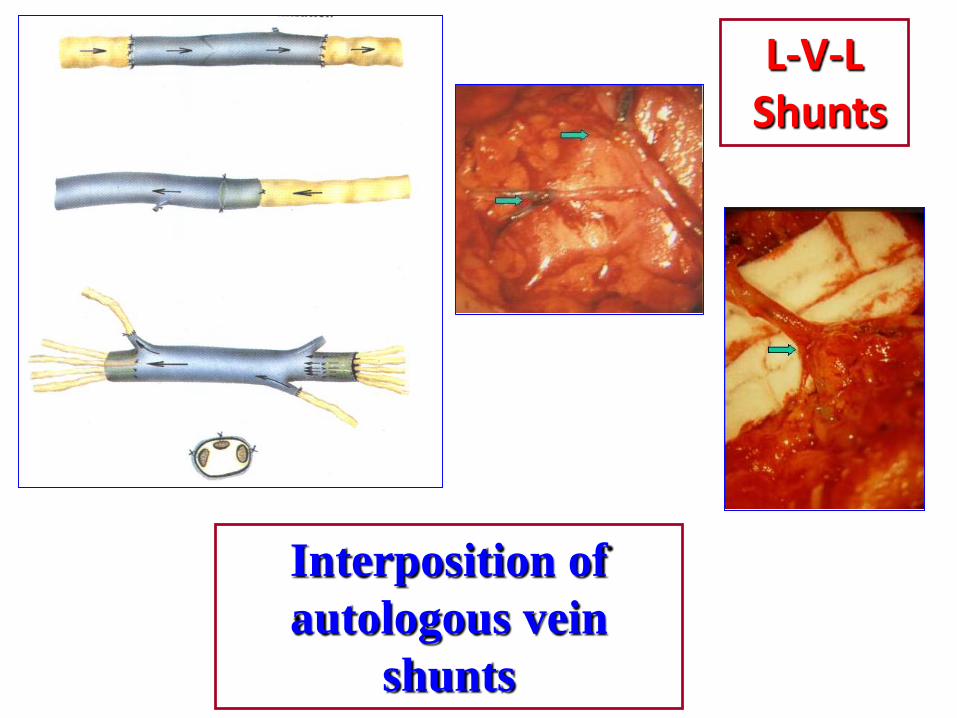
Reconstructive Multiple Lymphatic-Venous-LymphaticAnastomoses (MLVLA) Microsurgery, when possible and needed (!)
L-V-LShunts
Interposition of autologous vein
shunts
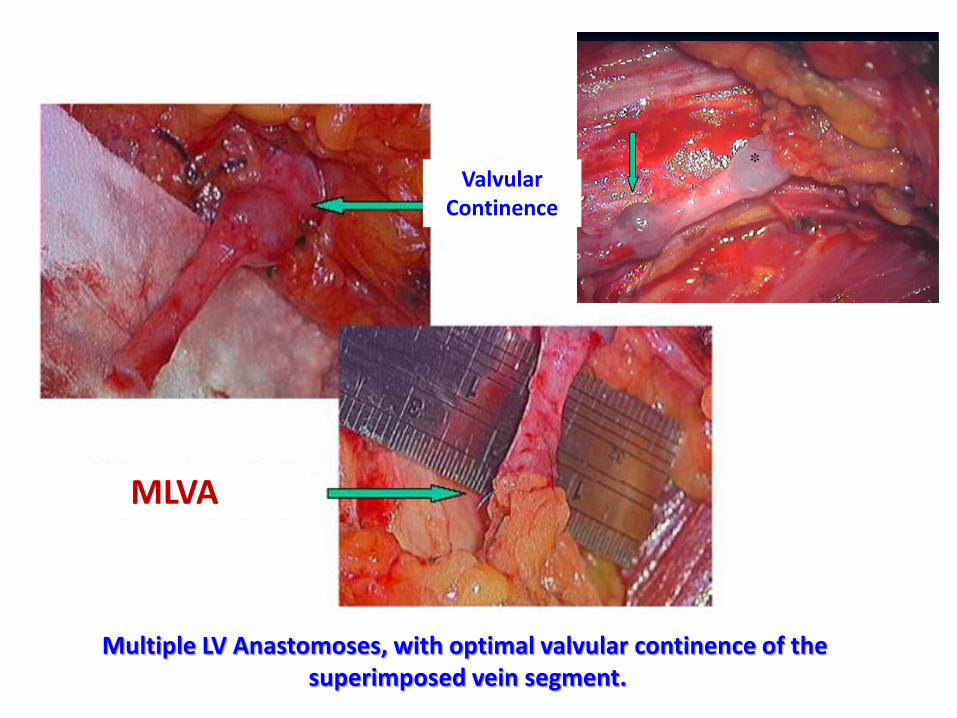
Valvular Continence
MLVA
Multiple LV Anastomoses, with optimal valvular continence of the superimposed vein segment.
A B
C D
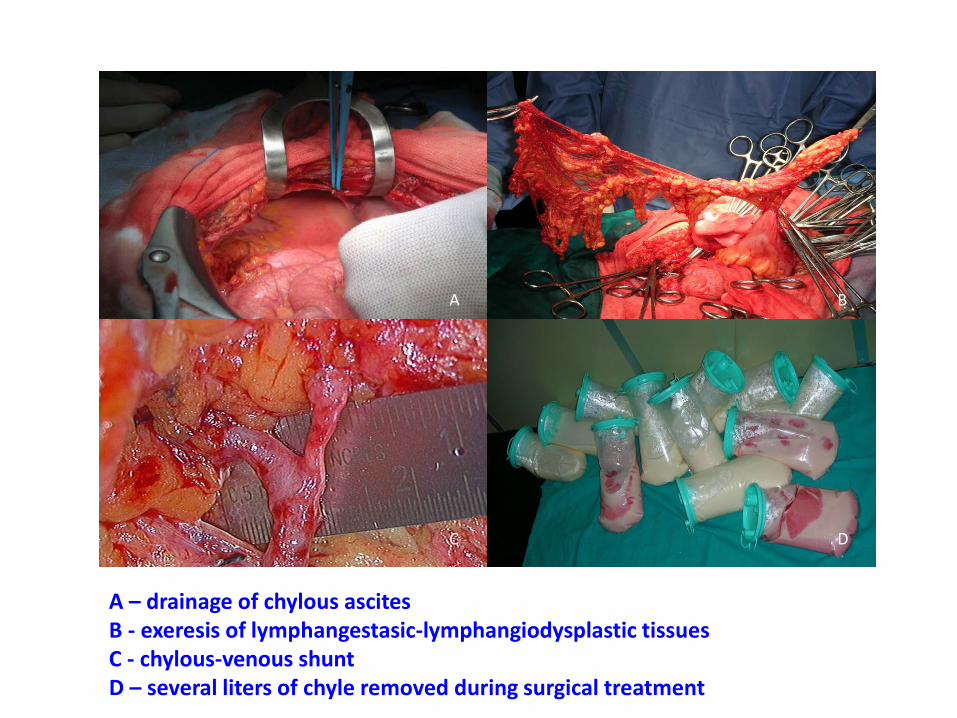
A – drainage of chylous ascitesB - exeresis of lymphangestasic-lymphangiodysplastic tissuesC - chylous-venous shuntD – several liters of chyle removed during surgical treatment
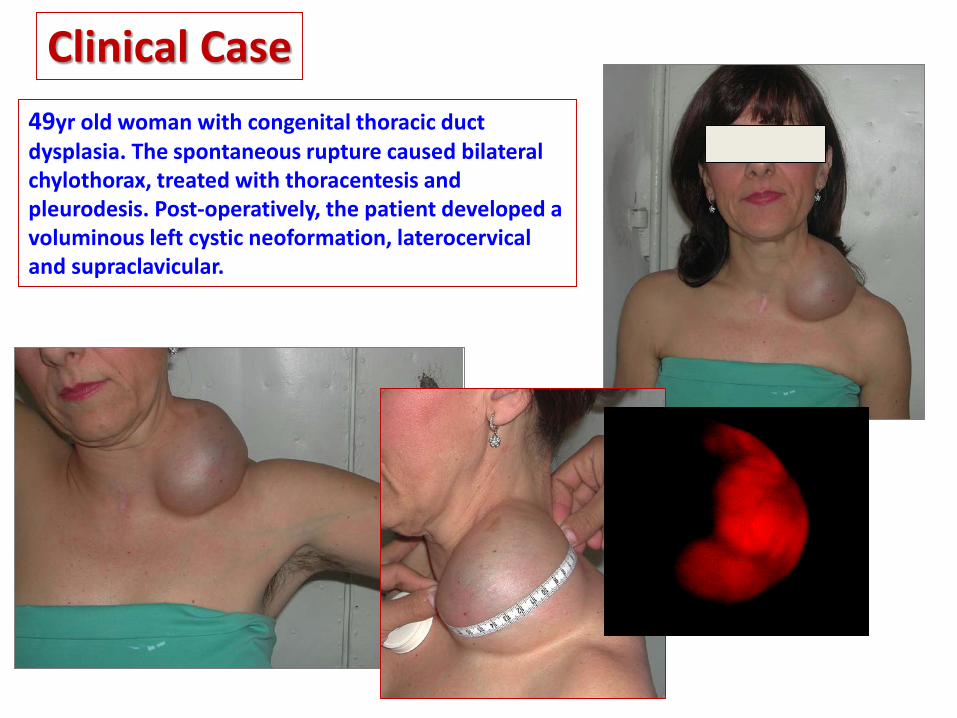
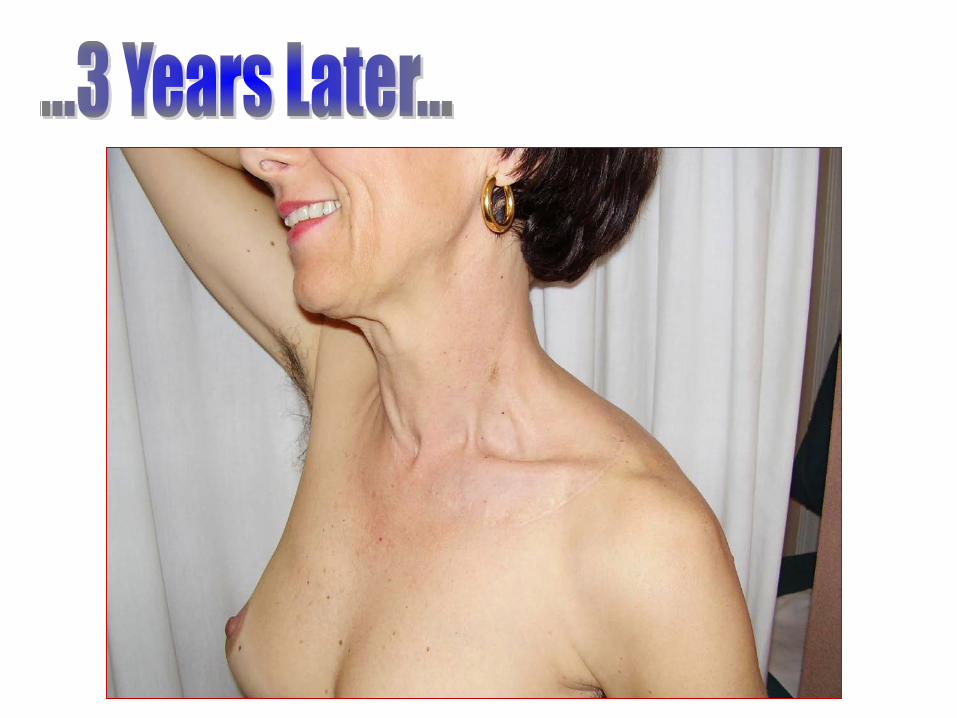
Clinical Case49yr old woman with congenital thoracic ductdysplasia. The spontaneous rupture caused bilateralchylothorax, treated with thoracentesis and pleurodesis. Post-operatively, the patient developed a voluminous left cystic neoformation, laterocervicaland supraclavicular.
Some more of our clinical casuistry…
•Surgical excision of the elephantasictissue with assiociated derivative/ reconstructive lymphatic-venousmicrosurgery of the left thigh, and CO2
LASER Treatment of the lymphostaticpapillomatosis
•Congenital Chyledema with gravitationalreflux due to chylo-lymphangio-adeno-dysplasia of the left leg.•Saccular deformation of the medial surface of the left thigh with lymphostaticverrucae papillomatosis
After
Before
Before After
Spontaneous, recurrent, Chyloperitoneum related to Chylous-Lymphangio-Dysplasia.Reactive Chylous Peritonitis, Acute Appedicitis, and right Hydrocele
- Resection of chylous-lymphangio--dysplastic omentum. - Closure of multiple chylous-peritoneal fistulas with anti-gravitational ligatures-Appendectomy, cholecystectomy-Eversion/resection of tunica vaginalisof right testis
TAKE HOME MESSAGELymphatic Disorders Surgical Management
The Best Practice: State of the Art
Corradino Campisi & Coll., Genoa, Italy 2017
Modern Surgical Treatment of Lymphatic DisordersEBM Latest Main References 2000-2017
1. Dellachà A, Boccardo F, Zilli A, Napoli F, Fulcheri E, Campisi C. Unexpected Histopathological Findings in Peripheral Lymphedema. Lymphology 2000;33(Suppl):62-64.
2. Campisi C, Boccardo F. Vein graft interposition in treating peripheral lymphoedemas. Handchir Mikrochir Plast Chir. 2003 Jul;35(4):221-4.
3. Campisi C, Boccardo F. Microsurgical techniques for lymphedema treatment: derivative lymphatic-venous microsurgery. World J Surg. 2004 Jun;28(6):609-13.
4. Campisi C, Bellini C,Eretta C, Zilli A, Da Rin E, Davini, Bonioli E, Boccardo F. Diagnosis and management of primary chylous ascites. J VascSurg. 2006 Jun;43(6):1244-8.
5. Campisi C, Eretta C, Pertile D, Da Rin E, Campisi C, Macciò A, Campisi M, Accogli S, Bellini C, Bonioli E, Boccardo F. Microsurgery for treatment of peripheral lymphedema: long-term outcome and future perspectives. Microsurgery 2007;27(4):333-8;
6. Boccardo F, Bellini C, Eretta C, Pertile D, Da Rin E, Benatti E, Campisi M, Talamo G, Macciò A, Campisi C, Bonioli E, Campisi C. The lymphatics in the pathophysiology of thoracic and abdominal surgical pathology: immunological consequences and the unexpected role of microsurgery. Microsurgery 2007;27(4):339-45.
7. Pardini M, Bonzano L, Roccatagliata L, Boccardo F, Mancardi G, Campisi C. Functional magnetic resonance evidence of cortical alterations in a case of reversible congenital lymphedema of the lower limb: a pilot study. Lymphology 2007 Mar;40(1):19-25.
8. Bellini C, Boccardo F, Campisi C, Villa G, Taddei G, Traggiai C, Bonioli E. Lymphatic dysplasias in newborns and children: the role of lymphoscintigraphy. J Pediatr. 2008 Apr;152(4):587-9.
9. Campisi C, Da Rin E, Bellini C, Bonioli E, Boccardo F. Pediatric lymphedema and correlated syndromes: role of microsurgery. Microsurgery 2008;28(2):138-42.
10. Gloviczki P. Handbook of Venous Disorders. Third Edition. Guidelines of the American Venous Forum. Edward Arnold Publ. 2009;658-672.
11. Boccardo F, Casabona F, De Cian F, Friedman D, Villa G, Bogliolo S, Ferrero S, Murelli F, Campisi C. Lymphedema microsurgical preventive healing approach: a new technique for primary prevention of arm lymphedema after mastectomy. Ann Surg Oncol 2009: 16(3):703-8
12. Campisi C, Boccardo F. Sistema Linfatico. In: R. Bellantone, G. De Toma, M. Montorsi (eds.). Chirurgia Generale (Metodologia, Patologia, Clinica Chirurgica). Torino: Edizioni Minerva Medica; 2009:54.
13. Boccardo F, Bellini C, Girino M, Campisi C, Vidali F, Corazza GR, Campisi C. Diagnostic assessment and therapeutic approach for immunodeficiency due to chylous dysplasia: a case report. Microsurgery 2010 Jul;30(5):401-4.
14. Boccardo F, Campisi C, Murdaca G, Benatti E, Boccardo C, Puppo F, Campisi C. Prevention of lymphatic injuries in surgery.Microsurgery 2010 May;30(4):261-5.
15. Campisi C, Bellini C, Campisi C, Accogli S, Bonioli E, Boccardo F. Microsurgery for lymphedema: clinical research and long-term results. Microsurgery 2010 May;30(4):256-60.
16. Suami H, Chang DW. Overview of surgical treatments for breast cancer-related lymphedema. Plastic and Reconstructive Surgery Journal 2010 Dec;126(6):1853-63.
17. Lee B, Andrade M, Bergan J, et al. Diagnosis and treatment of primary lymphedema. Consensus document of the International Union of Phlebology (IUP)-2009. Int. Angiol 2010;29(5):454-70.
18. Boccardo F, Casabona F, Friedman D, Puglisi M, De Cian F, Ansaldi F, Campisi C. Surgical prevention of arm lymphedema after breast cancer treatment. Ann Surg Oncol 2011: 18(9):2500-5.
20. Campisi C, Boccardo F, Witte M, Bernas M. Lymphatic Surgery and Surgery of Lymphatic Disorders. In: Dieter R, Dieter Jr. RA, Dieter IIIRA (eds.). Venous and Lymphatic Diseases. New York, USA: Eds. The Mc Graw Hill Companies, Inc.; 2011 Chapter 42.
21. Campisi C, Campisi C, Boccardo F. Topics in cancer survivorship. Chapter 4 (pp. 43-52), Surgical prevention of arm lymphedema inbreast cancer treatment. InTech Publisher, January 2012.
Modern Surgical Treatment of Lymphatic DisordersEBM Latest Main References 2000-2017
22. Campisi CC, Spinaci S, Lavagno R, Larcher L, Boccardo F, Santi PL, Campisi C. Immunodeficiency due to chylous dysplasia: diagnostic andtherapeutic considerations. Lymphology 2012 Jun; 45(2):58-62.
23. Boccardo F, Campisi CC, Molinari L, Dessalvi S, Santi PL, Campisi C. Lymphatic complications in surgery: possibility of prevention andtherapeutic options. Updates Surg. 2012 Sep.;64(3):211-6. Epub 2012 Jul. 21.
24. Campisi CC, Larcher L, Lavagno R, Spinaci S, Adami M, Boccardo F, Santi PL, Campisi C. Microsurgical primary prevention of lymphaticinjuries following breast cancer treatment. Plast Reconstr Surg 2012 Nov;130(5):749-750.
25. Boccardo F, Fulcheri E, Villa G, Molinari L, Campisi C, Dessalvi S, Murdaca G, Campisi C, Santi PL, Parodi A, Puppo F, Campisi C.Lymphatic microsurgery to treat lymphedema: techniques and indications for better results. Ann Plast Surg 2012; 71:191-195
26. Campisi C, Boccardo F, Campisi C.C. Patologia dei Linfatici. In: Carlo Setacci (ed.). Chirurgia Vascolare. Turin:Italy. Edizione MinervaMedica;2012:Chapter18.
27. Campisi CC, Larcher L, Lavagno R, Spinaci S, Adami M, Boccardo F, Santi P, Campisi C. Microsurgical primary prevention of lymphaticinjuries following breast cancer treatment. Plast Reconstr Surg. 2012 ;130:749-750
28. Campisi CC, Boccardo F, Piazza C, Campisi C. Evolution of chylous fistula management after neck dissection. Curr Opin OtolaryngolHead Neck Surg. 2013 ;21: 150-156
29. Campisi C, Boccardo F, Campisi CC, Ryan M. Reconstructive microsurgery for lymphedema: while the early bird catches the worm, thelate riser still benefits. J Am Coll Surg. 2013;216:506-7
30. Ryan M, Campisi CC, Boccardo F, Campisi C. Surgical treatment for lymphedema: optimal timing and optimal techniques. J Am CollSurg. 2013;216:1221-3.
31. Morotti M, Menada MV, Boccardo F, Ferrero S, Casabona F, Villa G, Campisi C, Papadia A. Lymphedema microsurgical preventivehealing approach for primary prevention of lower limb lymphedema after inguinofemoral lymphadenectomy for vulvar cancer. Int JGynecol Cancer. 2013 May;23(4):769-74.
Modern Surgical Treatment of Lymphatic DisordersEBM Latest Main References 2000-2017
32. Boccardo F, De Cian F, Campisi CC, Molinari L, Spinaci S, Dessalvi S, Talamo G, Campisi CS, Villa G, Bellini C, Parodi A, Santi PL, Campisi C.Surgical prevention and treatment of lymphedema after lymph node dissection in patients with cutaneous melanoma. Lymphology. 2013Mar;46(1):20-6.
33. Bellini C, Ergaz Z, Boccardo F, Bellini T, Campisi CC, Bonioli E, Ramenghi LA. Dynamics of pleural fluid effusion and chylothorax in the fetusand newborn: Role of the Lymphatic System. Lymphology. 2013;46:75-84.
34. Campisi CC, Ryan M, Boccardo F, Campisi C. Ly.M.P.H.A. and the prevention of lymphatic injuries: A rationale for early microsurgicalintervention. J Reconstr Microsurg. 2014 Jan;30(1):71-2.
35. Boccardo F, Dessalvi S, Campisi CC, Molinari L, Spinaci S, Talamo G, Campisi C. Microsurgery for groin lymphocele and lymphedema afteroncologic surgery. Microsurgery. 2014 Jan;34(1):10-3.
36. Campisi C, Ryan M, Campisi CS, Boccardo F, Campisi CC. (2015). Lymphatic Truncular Malformations of the Limbs: Surgical Treatment. In:R. Mattassi et al. (eds.). Hemangiomas and Vascular Malformations: An Atlas of Diagnosis and Treatment (pp. 451-461). Springer –VerlagItalia 2009, 2015
37. Campisi C, Ryan M, Campisi CS, Boccardo F, Campisi CC. (2015). Thoracic Duct Dysplasias and Chylous Reflux. In: R. Mattassi et al. (eds.).Hemangiomas and Vascular Malformations: An Atlas of Diagnosis and Treatment (pp. 463-473). Springer-Verlag Italia 2009, 2015
38. C.C. Campisi, M. Ryan, C.S. Campisi, P. Di Summa, F. Boccardo, C. Campisi. Intermittent negative pressure therapy in the combined treatment of peripheral lymphedema. Lymphology 2015; 48:197-204
39. Campisi CC, Ryan M, Campisi C. (2015-2016). Multiple Lymphaticovenous Anastomoses and Multiple Lymphatic-Venous-Lymphatic Anastomose / Fibro-Lipo-Lympho-Aspiration with the Lymph Vessel-Sparing Procedure. In: PC Neligan, J Masia, NB Piller (eds.). Lymphedema: Complete Medical and Surgical Management (Chapter 33 pp. 447-462). CRC Press Taylor & Francis Group, Boca Raton, FL, USA
40. Campisi CC, Ryan M, Boccardo F, Campisi C. A single-site technique of multiple lymphatic venous anastomoses for the treatment of peripheral lymphedema: Long term clinical outcomes. J. Reconstr Microsurg. 2016 Jan;32(1):42-9.
41. Campisi CC, Ryan M, Boccardo F, Campisi C Fibro-Lipo-Lymph-Aspiration with a Lymph Vessel Sparing Procedure (FLLA-LVSP) to Treat Advanced Lymphedema after Multiple Lymphatic-Venous Anastomoses (MLVA): the Complete Treatment Protocol. Annals of Plastic Surgery. 2017 Feb;78(2):184-190
Modern Surgical Treatment of Lymphatic DisordersEBM Latest Main References 2000-2017