34
Forearm and Wrist Fractures By Dr Fiona Hill HMO2
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | lewis-blankenship |
| View: | 245 times |
| Download: | 1 times |

Forearm and Wrist Fractures
By Dr Fiona Hill
HMO2
Key Learning Points
1. www.eorif.com
2. Always XR the joint above and below #.
3. # Ulnar = check the radial head # Radius= check the druj
4. GFR: Galeazzi = Fractured Radius BUM: Broken Ulnar = Monteggia
5. www.imagingpathways.health.wa.gov.au
Summary of Fractures
Galeazzi Monteggia Isolated Forearm
Fractures Colle’s Fracture Smith’s Fracture Fracture of Radial
Styloid
Forearm Fractures 101
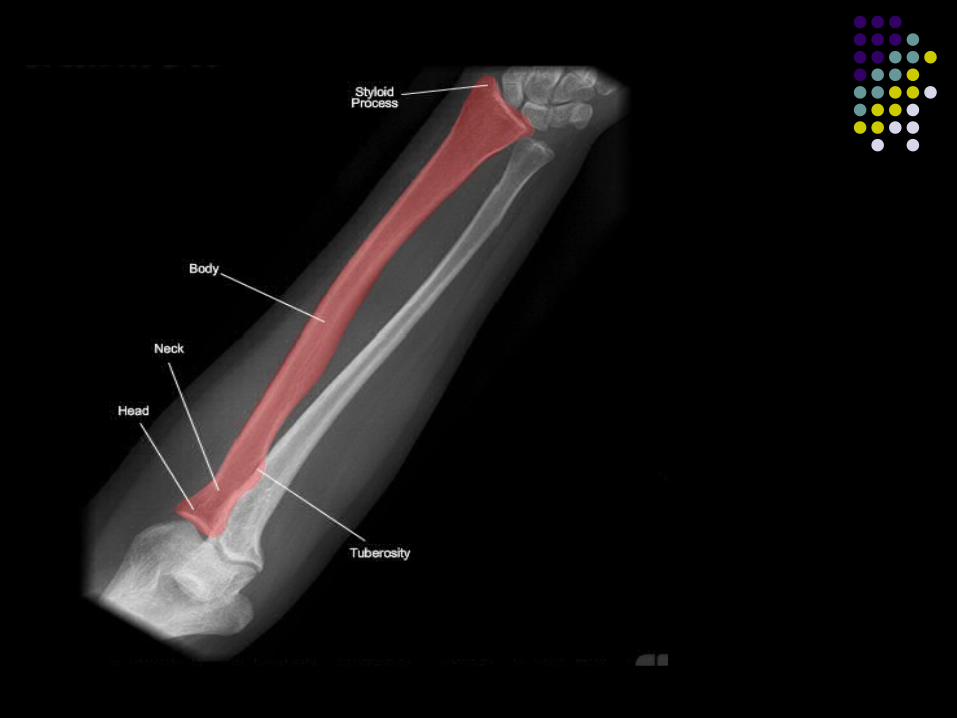
Radius and ulnar are bound together by: Annular ligament Interosseus membrane Radioulnar ligaments and triagular fibrocartilage.
With a direct blow you can break either isolated, however more likely w/ indirect (i.e. FOOSH) to damage both.

www.imagingpathways.health.wa.gov.au


www.imagingpathways.health.wa.gov.au


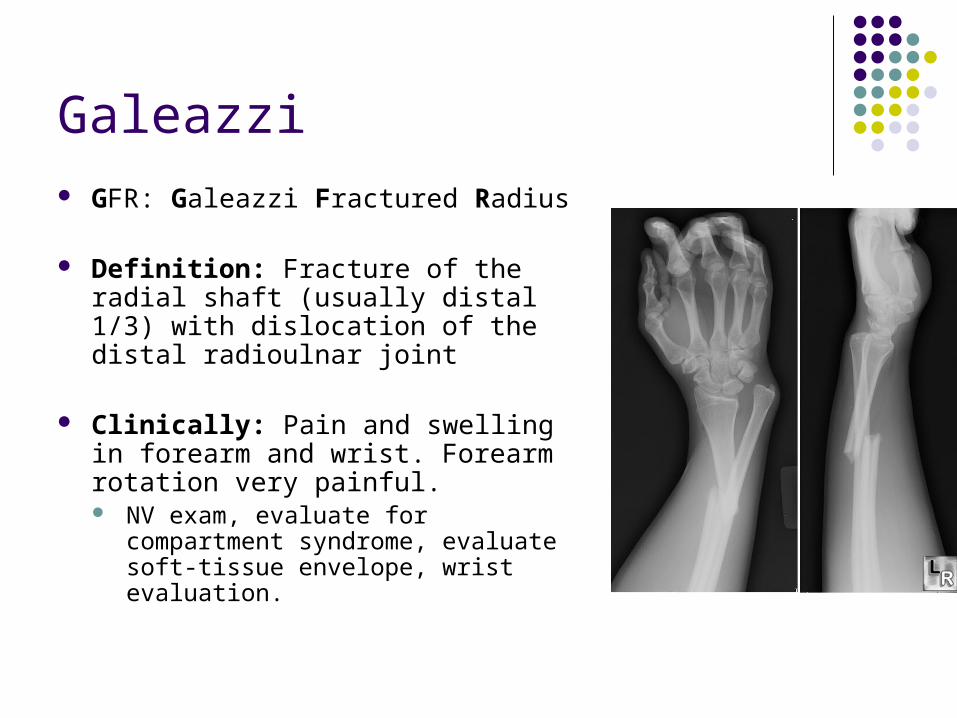
Galeazzi GFR: Galeazzi Fractured Radius
Definition: Fracture of the radial shaft (usually distal 1/3) with dislocation of the distal radioulnar joint
Clinically: Pain and swelling in forearm and wrist. Forearm rotation very painful. NV exam, evaluate for compartment
syndrome, evaluate soft-tissue envelope, wrist evaluation.

Galeazzi part 2 Radiologically: A/P and Lateral of
forearm +/- elbow, wrist.
Mx: ORIF of the radius is indicated in all cases. Further Mx depending on stability of
distal radioulnar joint.
Assoicated injuries/DDx: Ulnar Styloid Fracture TFCC Tear DRUJ Instability
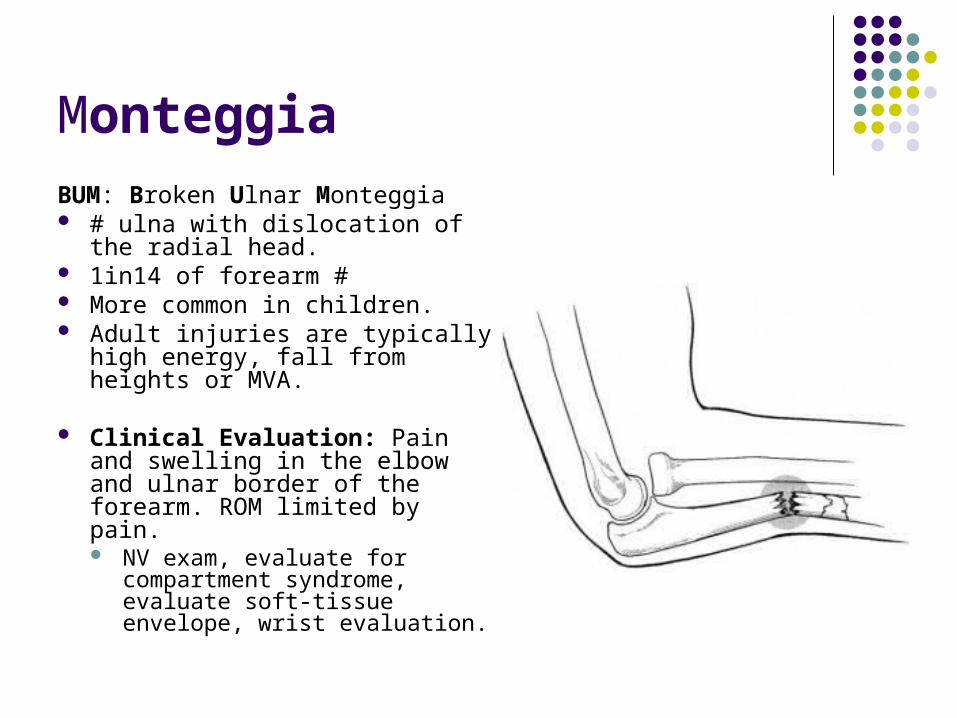
MonteggiaBUM: Broken Ulnar Monteggia # ulna with dislocation of the
radial head. 1in14 of forearm # More common in children. Adult injuries are typically high
energy, fall from heights or MVA.
Clinical Evaluation: Pain and swelling in the elbow and ulnar border of the forearm. ROM limited by pain. NV exam, evaluate for
compartment syndrome, evaluate soft-tissue envelope, wrist evaluation.

Monteggia Radiology: A/P and Lateral of
forearm +/- elbow, wrist. Always suspect a radial head
dislocation in an ulnar #.
A line drawn along the axis of the radius should pass through the capitellus on both lateral + AP views.
MX: ORIF generally.

Isolated Ulnar/Radius Most fractures of the
ulnar/radius shaft are caused by direct blows and result in minimal soft-tissue injury.
Generally obvious gross deformity NV exam, evaluate for
compartment syndrome, evaluate soft-tissue envelope, wrist evaluation.
A/P and Lateral of forearm +/- elbow, wrist.

Isolated Ulnar/Radius Ulnar Shaft Fracture Associated Injuries /
Differential Diagnosis Monteggia fracture-dislocation. Radius and ulna shaft fracture. Galeazzi Fracture
Mx: Depends on if it’s a distal, middle or proximal third. Plus if its displaced or not. Can be conservative or ORIF.
Fracture Complications a
Superficial wound infection Nonunion: (incidence is higher for comminuted or
displaced fx's) Hardware failure Malunion Painful hardware Ulnar nerve palsy Radial nerve palsy
Distal Radial Fracture (+ Colles Fracture)
Most commonly women age 60-70. 90% caused by compression on dorsiflexed
wrist. 90% of distal radius fractures are Colles
Fractures
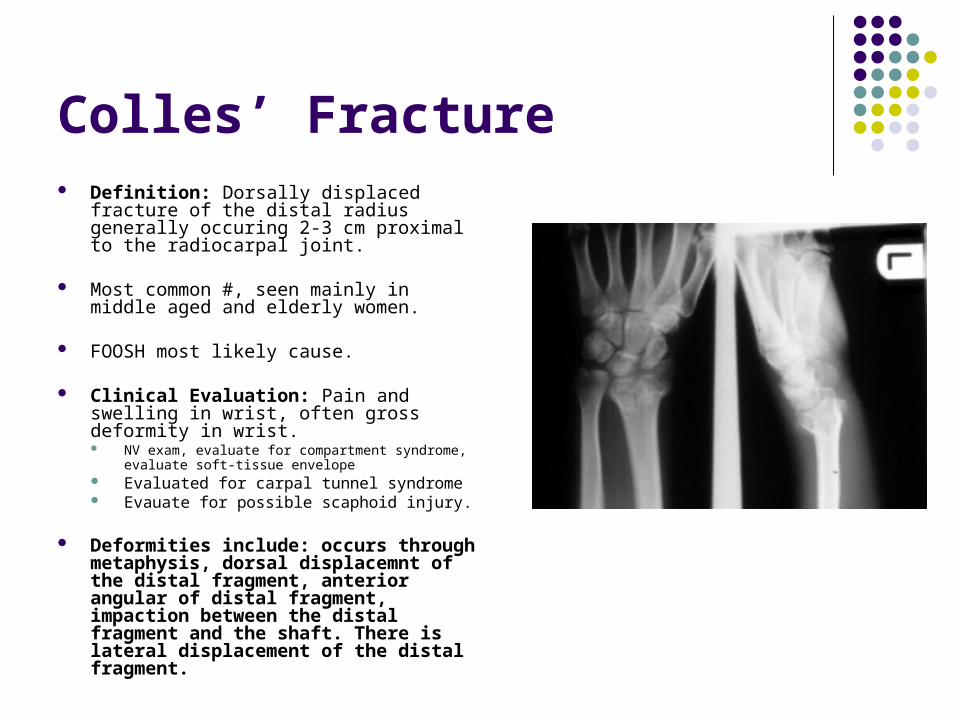
Colles’ Fracture Definition: Dorsally displaced fracture of
the distal radius generally occuring 2-3 cm proximal to the radiocarpal joint.
Most common #, seen mainly in middle aged and elderly women.
FOOSH most likely cause.
Clinical Evaluation: Pain and swelling in wrist, often gross deformity in wrist. NV exam, evaluate for compartment syndrome,
evaluate soft-tissue envelope Evaluated for carpal tunnel syndrome Evauate for possible scaphoid injury.
Deformities include: occurs through metaphysis, dorsal displacemnt of the distal fragment, anterior angular of distal fragment, impaction between the distal fragment and the shaft. There is lateral displacement of the distal fragment.
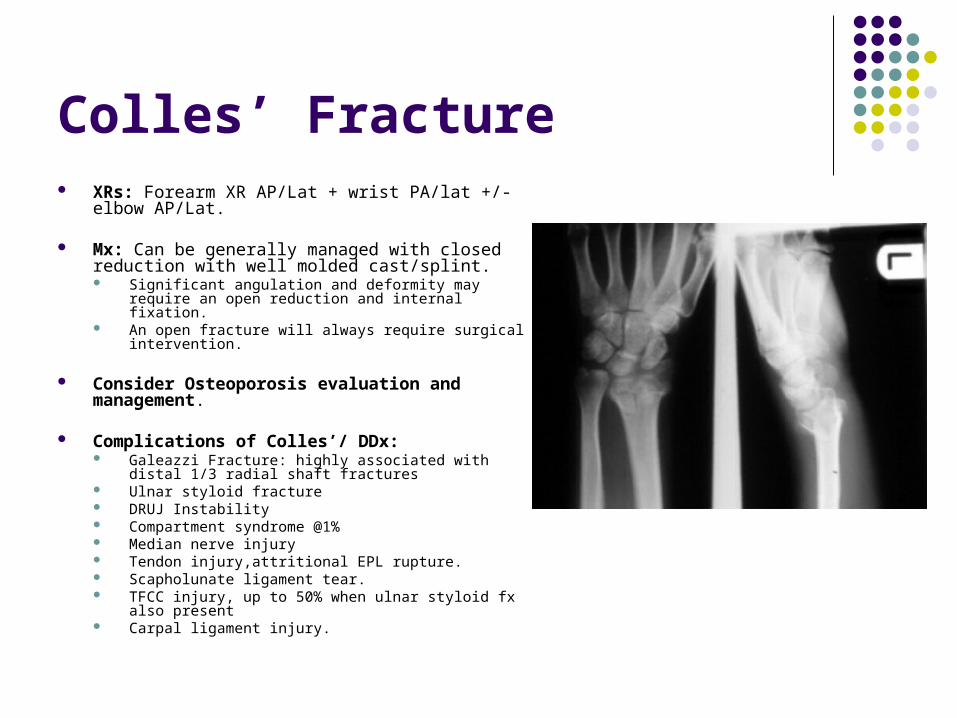
Colles’ Fracture XRs: Forearm XR AP/Lat + wrist PA/lat +/- elbow
AP/Lat.
Mx: Can be generally managed with closed reduction with well molded cast/splint. Significant angulation and deformity may require an open
reduction and internal fixation. An open fracture will always require surgical intervention.
Consider Osteoporosis evaluation and management.
Complications of Colles’/ DDx: Galeazzi Fracture: highly associated with distal 1/3 radial
shaft fractures Ulnar styloid fracture DRUJ Instability Compartment syndrome @1% Median nerve injury Tendon injury,attritional EPL rupture. Scapholunate ligament tear. TFCC injury, up to 50% when ulnar styloid fx also present Carpal ligament injury.
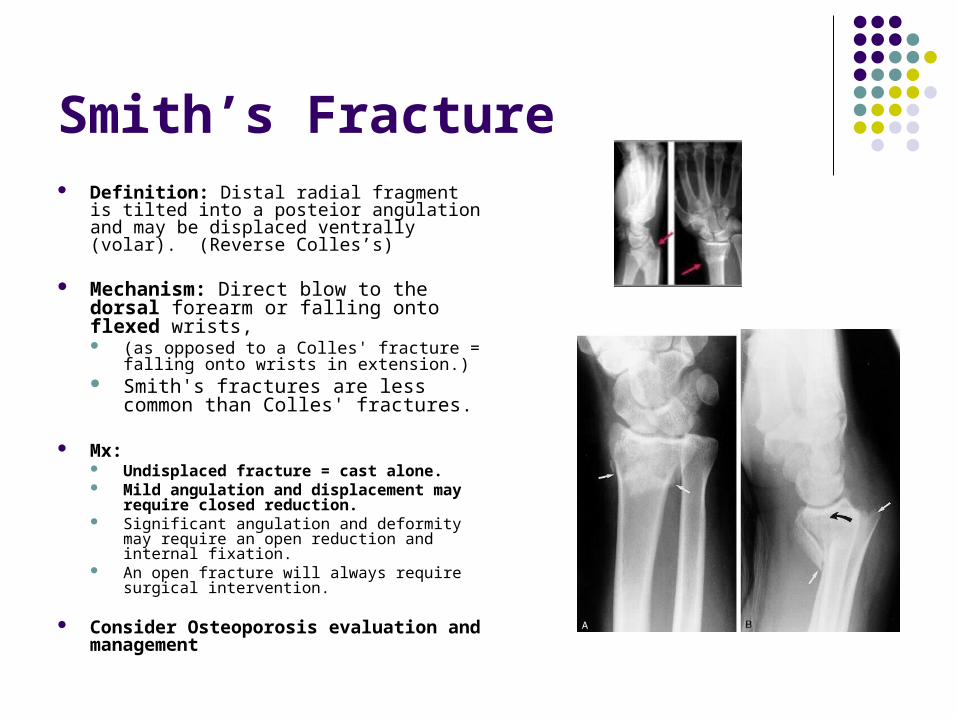
Smith’s Fracture Definition: Distal radial fragment is tilted
into a posteior angulation and may be displaced ventrally (volar). (Reverse Colles’s)
Mechanism: Direct blow to the dorsal forearm or falling onto flexed wrists, (as opposed to a Colles' fracture = falling
onto wrists in extension.) Smith's fractures are less common
than Colles' fractures.
Mx: Undisplaced fracture = cast alone. Mild angulation and displacement may
require closed reduction. Significant angulation and deformity may
require an open reduction and internal fixation.
An open fracture will always require surgical intervention.
Consider Osteoporosis evaluation and management
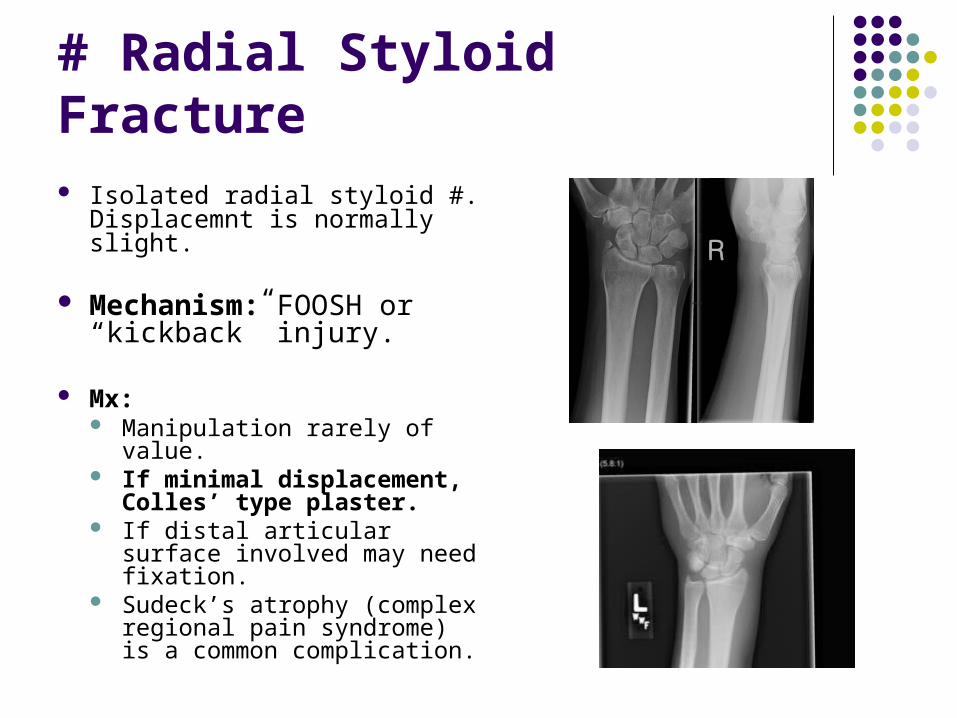
# Radial Styloid Fracture Isolated radial styloid #.
Displacemnt is normally slight.
Mechanism: FOOSH or “kickback” injury.
Mx: Manipulation rarely of value. If minimal displacement,
Colles’ type plaster. If distal articular surface
involved may need fixation. Sudeck’s atrophy (complex
regional pain syndrome) is a common complication.











Key Learning Points
1. www.eorif.com
2. Always XR the joint above and below #.
3. # Ulnar = check the radial head # Radius= check the druj
4. GFR: Galeazzi = Fractured Radius BUM: Broken Ulnar = Monteggia
5. www.imagingpathways.health.wa.gov.au
Thank you!

















