:ment iiiii!ii~ persistent "cessful use of a chicken-based diet for the of severely malnourished children with diarrhea: A prospective, randomized study Samuel Nur/co, AID, dosdAlberto Garchz-Aranda, AID,Euyenia Fiahbein, RN, and AIartha In& Pdrez-Ztiffiya, RD Objective: To evaluate the efficacy of a chicken-based diet for the treatment of persis- tent diarrhea in severely malnourished children. Stud}" design: Prospective, randomized, double-blind study that compared a chicken- based diet with elemental (Vivonex) and soy (Nursoy) diets. Hospitalized children with third-degree malnutrition and persistent diarrhea, aged 3 to 36 months, were included. Diets were isocaloric and given nasogastrically at 150 ml/kg per day in progressively increasing concentrations. Results: Fifty-six children were included (18 received Vivonex, 19 Nursoy, 19 chick- en). They had a mean age of 6.4 _+ 4.4 months, a mean weight of 3604 _+1232 gm, and a mean weight-for-age percentage of 51.4% _+ 7.2%. Sixty-four percent had associated conditions on admission to the hospital. Forty-one children (73.2%) were successfully treated (13 Vivonex, 13 Nursoy, 15 chicken). There were no differences in diarrheal outcomes, and all groups had significant weight gain. Failure was independent of the diet and was associated with the presence of infection on admission. There was a signif- icantly higher nitrogen balance in the children from the chicken group (358.2 _+13 mg/kg per day) than in those receiving Vivonex (226.6 +_ 61) or Nursoy (291.4 _+111.6; p < 0.05) groups. Conclusions: The chicken-based diet was as effective as Vivonex or Nursoy. It is well tolerated, inexpensive, and widely available and thus represents an effective and inex- pensive alternative to the treatment of severely malnourished children with persistent diarrhea. (J Pediatr 1997;131:405-12) Persistent diarrhea confnues to be a major health problem in developing countries 1"3 and is often associated with a deterioration in nutritional state. 1'3'4The nutritional reha- bilitation of children with PD and severe malnutrition is difficult and usually requires hospitalization 4 and specialized care. l's Initially the introduction of parenteral nutri- tion improved the outcome of PD in these children. 6'7 Recent studies have shown that specialized enteral feeding during the diar- rhea] episode results in improved nutrition- al outcomes. 1'4'8 Therefore the enteral ad- ministration of elemental and semielementat diets, with supplementation with parenteral nutrition when needed, has become the standard therapy. 5-z'9 These specialized en- teral feedings, however, are very expensive, usually unpalatable, and not readily avail- able in many areas of the world. 1,4,8 From the Departnwat of Pediatric GaaO'oenterology and Nutrition Hospital l@mtil de Mdrico Federico Gdme;4Mexico CitN d/fexico. Supported in part b2- the Applied Diarrheal Disease Research Project at Harvard University, by means of a cooperative agreement with the U.S. Agency for International Development, and in part by National Institutes of Health grant T32-DK 07703. Submitted for publication April 3, 1996; accepted Dec. 17, 1996. Reprint requests: Samuel Nurko, MD, Pediatric Gastroenterology, Children's Hospital, 300 Longwood Ave., Boston, MA 02115. ~Dr. Nurko is now in the Combined Program in Pediatric Gastroenterology and Nutrifon, Children's Hospital, Boston, Mass. Copyright 1997 by Mosby-Year Book, Inc. 0022-3476/97/$5.00 + 0 9/21/79985 Recent work suggests that malnour- ished patients with PD may be capable of tolerating more complex diets, 1'4'8 so ef- forts are being undertaken to find inex- pensive, available, and culturally accept- able diets.l'8' 10,11 Because milk is not well tolerated by children with PD when given as a full diet, 1'4'12 alternatives have been suggested. 1"4'8"10'1I Soy-based formulas are still used extensively, but their effica- cy continues to be controversial. 4'8 Chicken-based diets have been empirical- 405
Transcript
: m e n t iiiii!ii~
persistent
"cessful use of a chicken-based diet for the of severely malnourished children with diarrhea: A prospective, randomized study
Samuel Nur/co, AID, dosd Alberto Garchz-Aranda, AID, Euyenia Fiahbein, RN, and AIartha In& Pdrez-Ztiffiya, RD
Objective: To evaluate the efficacy of a chicken-based diet for the treatment of persis-
tent diarrhea in severely malnourished children.
Stud}" design: Prospective, randomized, double-blind study that compared a chicken-
based diet with elemental (Vivonex) and soy (Nursoy) diets. Hospitalized children with
third-degree malnutrition and persistent diarrhea, aged 3 to 36 months, were included.
Diets were isocaloric and given nasogastrically at 150 ml/kg per day in progressively
increasing concentrations.
Results: Fifty-six children were included (18 received Vivonex, 19 Nursoy, 19 chick-
en). They had a mean age of 6.4 _+ 4.4 months, a mean weight of 3604 _+ 1232 gm, and a
mean weight-for-age percentage of 51.4% _+ 7.2%. Sixty-four percent had associated
conditions on admission to the hospital. Forty-one children (73.2%) were successfully
treated (13 Vivonex, 13 Nursoy, 15 chicken). There were no differences in diarrheal
outcomes, and all groups had significant weight gain. Failure was independent of the
diet and was associated with the presence of infection on admission. There was a signif-
icantly higher nitrogen balance in the children from the chicken group (358.2 _+ 13
mg/kg per day) than in those receiving Vivonex (226.6 +_ 61) or Nursoy (291.4 _+ 111.6;
p < 0.05) groups.
Conclus ions : The chicken-based diet was as effective as Vivonex or Nursoy. It is well
tolerated, inexpensive, and widely available and thus represents an effective and inex-
pensive alternative to the treatment of severely malnourished children with persistent
diarrhea. (J Pediatr 1997;131:405-12)
Persistent diarrhea confnues to be a major health problem in developing countries 1"3 and is often associated with a deterioration in nutritional state. 1'3'4 The nutritional reha- bilitation of children with PD and severe malnutrition is difficult and usually requires hospitalization 4 and specialized care. l's Initially the introduction of parenteral nutri- tion improved the outcome of PD in these children. 6'7 Recent studies have shown that specialized enteral feeding during the diar- rhea] episode results in improved nutrition- al outcomes. 1'4'8 Therefore the enteral ad- ministration of elemental and semielementat diets, with supplementation with parenteral nutrition when needed, has become the standard therapy. 5-z'9 These specialized en- teral feedings, however, are very expensive, usually unpalatable, and not readily avail- able in many areas of the world. 1,4,8
From the Departnwat of Pediatric GaaO'oenterology and Nutrition Hospital l@mtil de Mdrico Federico Gdme;4 Mexico CitN d/fexico.
Supported in part b 2- the Applied Diarrheal Disease Research Project at Harvard University, by means of a cooperative agreement with the U.S. Agency for International Development, and in part by National Institutes of Health grant T32-DK 07703.
Submitted for publication April 3, 1996; accepted Dec. 17, 1996.
Reprint requests: Samuel Nurko, MD, Pediatric Gastroenterology, Children's Hospital, 300 Longwood Ave., Boston, MA 02115.
~Dr. Nurko is now in the Combined Program in Pediatric Gastroenterology and Nutrifon, Children's Hospital, Boston, Mass.
Copyright �9 1997 by Mosby-Year Book, Inc.
0022-3476/97/$5.00 + 0 9/21/79985
Recent work suggests that malnour- ished patients with PD may be capable of tolerating more complex diets, 1'4'8 so ef- forts are being undertaken to find inex- pensive, available, and culturally accept- able diets.l'8' 10,11 Because milk is not well tolerated by children with PD when given as a full diet, 1'4'12 alternatives have been sugges ted . 1"4'8"10'1I Soy-based formulas
are still used extensively, but their effica- cy continues to be controversial. 4'8 Chicken-based diets have been empirical-
405
NURKO ET AL. THE JOURNAL OF PEDIATRICS SEPTEMBER 1997
Table I. Composition of the diets at the maximum concentration
ly and successfully used for the treatment of malnourished infants with PD when el- emental or soy diets have not been avail- able. 4'13-1s Chicken has the advantage of being considered by mothers and health personnel in Mexico 16'17 and other areas of the world as a safe food for children with diarrhea or malnutrition. 4'1a'14
Because the optimal nutritional therapy for severely malnourished patients with PD is still controversial, 1'4 we evaluated the efficacy of a chicken-based diet for the treatment of PD in severely malnourished children.
M E T H O D S
Patients In this prospective, randomized, dou-
ble-blind study a local chicken-based diet was compared with both an elemental diet (Vivonex Standard; Norwich Eaton) and a soy-based formula (Nursoy; Wyeth Laboratories) in the treatment of severely malnourished hospitalized children with PD.
The study was performed at the Hospital Infantil de 1Vidxico Federico Gdmez in Mexico City. Patients between 3 and 36 months of age hospitalized with third-degree malnutrition of the maras- matic type with PD were included. Third- degree malnutrition was defined by using the Gdmez criteria for weight for age (<60% of the National Center for Health Statistics 50th percenfle), is PD was de- fined as three or more loose stools for 14 days or longer. 2
Patients with the following characteris- tics were excluded: exclusively breast fed, chronic illness (e.g., acquired im- munodeficieney syndrome, tuberculo- sis), congenital malformation, an abdom- inal condition that would preclude enteral feedings, a severe condition re- quiring intensive care, or lack of parental consent.
The protocol was approved by the local ethical review committee and by the Harvard School of Public Health Com- mittee on the Use of Human Subjects in Research. Informed consent was obtained from all parents.
Study Design
DIETS
The mainstay of therapy for PD and se- vere malnutrition at the Hospital Infantil de Mgxico has been the elemental diet Vivonex Standard. 5 Vivonex contains crystalline amino acids, glucose and glu- cose oligosaccharides, a small amount of highly purified safflower oil, electrolytes, minerals, micronutrients, and vitamins, s'9 For use in children with PD, we and oth- ers have shown that Vivonex is effective if it is given in progressively increasing con- centrations, starting at 150 ml/kg per day in a concentration that provides 47.8 kcal/dl (12.5% weight/volume) and ad- vancing slowly by 2.5% per day to a max- imum concentration of 85.6 kcal/dl (22.5% weight/volume) s'9 (Table I). Sodium chloride and potassium chloride were also added to the formula to ensure administration of sodium, 4 mEq/kg per day, and potassium, 3 mEq/kg per day. 5
The chicken-based diet was designed with the use of tables of food composition 19'20 and consists of easily available and simple ingredients: cooking oil, boiled chicken breast, table sugar, and minerals. To pre- pare the chicken-based diet, we calculated the total volume needed per day (150 ml/kg). At the maximum concentration (Table I) the following ingredients per deciliter of diet were used: 8 gm boiled, comminuted chicken breast; 3 ml veg- etable cooking oil; and 10.5 gm table sugar. After these components were blended together, the following minerals were added: 5 ml calcium gluconate (10% solution, PISA), 2.7 ml of dibasic sodium phosphate (PISA, dibasic sodium phos- phate), and 1.7 ml of magnesium sulfate (10% solution, PISA). Sodium chloride (0.gN solution) to achieve 4 mEq of sodi- um per kilogram of body weight per day and potassium chloride to achieve 3 mEq/kg/day were also added. Finally, boiled water was added to achieve the total volume required.
The soy formula used was Nursoy, which contains soy protein, coconut, safflower and soy oils, sucrose, minerals, and vita- mins. All diets were prepared in the pedi-
406
THE JOURNAL OF PEDIATRICS Volume 13 I, Number 3
NURKO ET AL.
atric nutrition kitchen of the hospital under the supervision of a trained nutri- tionist.
The study was designed to use Vivonex as the standard against which the other formulas were compared, so all three diets were given nasogastrically at progressive isocalorie concentrations. The maximum concentration of the diets is shown in Table I. Because of intrinsic differences in diet composition, the percentage of total calories provided as protein, carbohy- drate, or fat varied (Table I).
PROTOCOL
Patients were randomly assigned to treatment by using a table of random numbers. Only the nutritionist who pre- pared the formula was aware of group as- signment. The investigators, nurses, and
residents remained masked to the type of diet because aluminum foil was used to cover the formula bag and tubing.
On admission to the hospital, patients were hydrated according to World Health Organiza t ion /UNICEF guidelines with the use of a standard glucose-electrolyte solution. 21 Patients were then fasted overnight. Hydrat ion was maintained during that time with intravenously ad- ministered fluids. The next morning the assigned diet was started if the patient was well hydrated and there were no other contraindications to feeding. The nasogastric tube was inserted by trained nursing staff. The diet was started at the lowest concentration at a volume of 150 ml/kg per day, and concentrations were advanced every 48 hours. If no intoler- ance occurred, full concentration was achieved by the ninth day (Table I). If there was evidence of intolerance, the diet concentration was either maintained or decreased as follows: (1) It was kept un-
changed if there was evidence of 2% or 3% positive reducing substances (before or after hydrolysis) or if there was an in-
crease in stool output of more than 50% (>20 ml/kg). (2) It was reduced if Clini- test results showed 4% or if there was an increase of 75% or more in the stool out- put (>20 m]/kg).
When full concentration of the diet was
achieved, it was maintained for an addi- tional 7 days. Daily supplementation with
1 mg folie acid, 1 ml multivitamin (Poly- Vi-Sol), and elemental iron, 6 mg/kg, was begun when the maximum concentration was achieved. After 7 days of the maxi- mum diet concentration, patients under- went a challenge with whole cow milk: we
administered half-strength whole cow milk, 10 ml/kg, and advanced to full-
strength milk if tolerated. Milk-tolerant patients continued their rehabilitation with lactose-contalning formula or whole milk, depending on the age. If patients showed evidence of lactose malabsorp- tion, as manifested by return of liquid stools, with p H less than 5 and greater than 2% reducing substances in the stool, a milk-flee diet was instituted. After the milk challenge, all patients restarted a
complete age-appropriate, complex-bal- anced diet, which was continued until dis-
charge. Cessation of diarrhea was defined as the
passage of formed stool not followed by liquid stools for at least 24 hours. Successful treatment was declared if the for- mula could be advanced to the highest concentration and there was cessation of the diarrhea at the end of the study. The onset of nutritional recovery was considered to be when the diarrhea ceased and there
was consistent weight gain for at least 48 hours. Treatmentfai[are was declared if the patient had 5% or more dehydration dur-
ing the administration of the diet, if there was clinical deterioration that precluded further enteral therapy, if diarrhea persist- ed at the end of the study, or if the formu- la could not be advanced to full concen- tration.
When treatment was declared a failure, the code was broken. If patients had been receiving Nursoy or chicken, they were started on a regimen of Vivonex. If the pa- tients with treatment failure had original- ly been receiving Vivonex or were unable to continue with enteral feedings, total parenteral nutrition alone was initiated and was then continued un t l the patient was stabilized and gaining weight. Con- tinuous enteral feedings with Vivonex were then added to the total parenteral
nutrition and advanced every 24 hours as tolerated. Once patients achieved full en- teral feedings, they continued to receive Vivonex for another 2 weeks and nutri- tional rehabilitation continued as outlined previously.
CLINICAL PROCEDURES
Nude weight was obtained on admis- sion and daily thereafter. The posthydra-
tion weight, obtained on the morning of the start of the feedings, was considered the baseline weight. Weights were ob- tained at the same time every morning with an electronic scale (ScalesTronLx, Wheaton, Ill.) and were accurate to at least 10 gm. Recumbent length was ob- tained with a specially designed board on admission, at the end of 2 weeks, and be- fore discharge. All measurements were
obtained by trained nutritionists, and their accuracy was validated before the beginning of the study.
All patients had baseline laboratory val- ues obtained at admission; laboratory studies included complete blood cell count, electrolyte concentrations, D-xy- lose concentration, stool and urine cul- tures, and stool tests for ova and parasites. Blood culture specimens were obtained only if indicated.
All intake and output were recorded.
Patients, both male and female, were placed on metabolic beds or cots for sep- aration of stool from urine. 5 To confirm Successful separation of stool and urine in girls, we performed a separate analysis for all the variables associated with the stool collection at the end of the study. No differences between sexes were found (data not shown), so all data were pooled. A 72-hour nitrogen balance test was per- formed at the end of the second week, starting 4 days after the maximum diet concentration had been achieved. The beginning and end of the stool collection time were marked by the fecal excretion
of orally administered activated char- coal. s The nitrogen balance was mea- sured by the micro Kjeldahl method. 22 Tests for pH and reducing and nonreduc- ing substances in stool were performed daily.
407
NURKO ET AL.
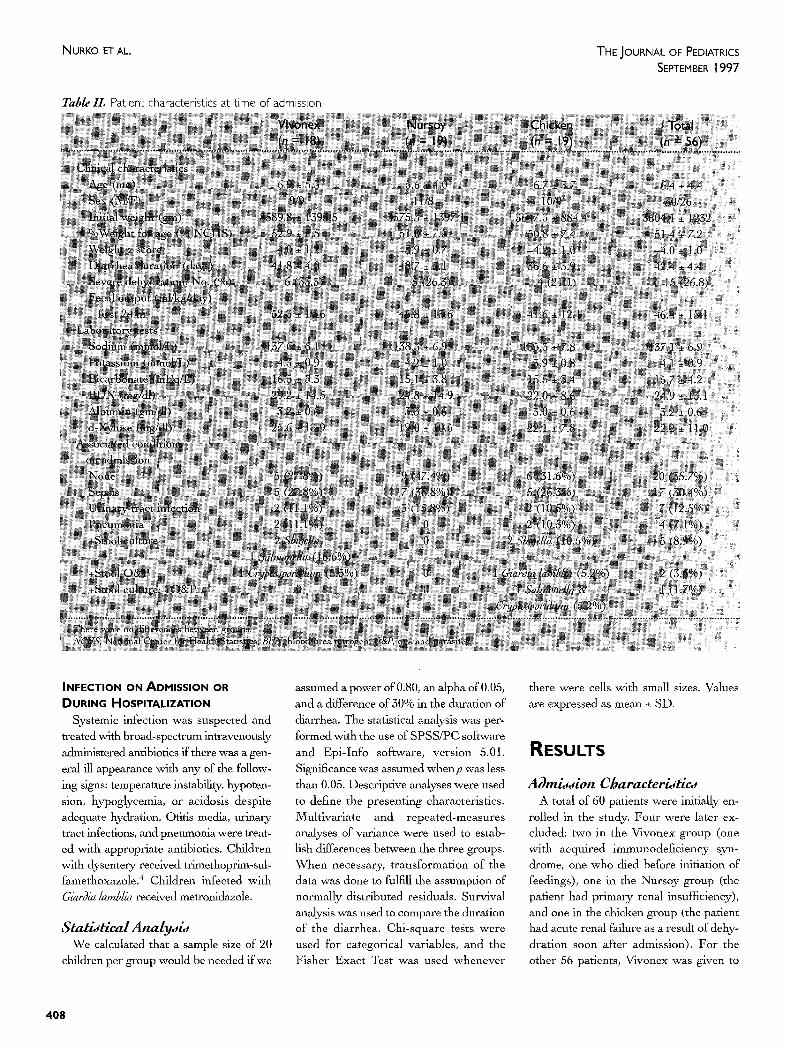
Table II. Patient characteristics at time of admission
THE JOURNAL OF PEDIATRICS SEPTEMBER 1997
INFECTION ON ADMISSION OR DURING HOSPITALIZATION
Systemic infection was suspected and treated with broad-spectrum intravenously
administered antibiotics if there was a gen- eral ill appearance with any of the follow- ing signs: temperature instability, hypoten- sion, hypoglycemia, or acidosis despite adequate hydration. Otitis media, urinary tract infections, and pneumonia were treat- ed with appropriate antibiotics. Children with dysentery received trimethoprim-sul- famethoxazole. 4 Children infected with Giardia larr~lia received metronidazole.
Statistical analysis We calculated that a sample size of 20
children per group would be needed if we
assumed a power of 0.80, an alpha of 0.05, and a difference of 30% in the duration of diarrhea. The statistical analysis was per- formed with the use of SPSS/PC software
and Epi-Info software, version 5.01. Significance was assumed when p was less than 0.05. Descriptive analyses were used to define the presenting characteristics. Multivariate and repeated-measures analyses of variance were used to estab- lish differences between the three groups. When necessary, transformation of the data was done to fulfill the assumption of normally distributed residuals. Survival analysis was used to compare the duration of the diarrhea. Chi-square tests were used for categorical variables, and the Fisher Exact Test was used whenever
there were cells with small sizes. VaLues are expressed as mean _+ SD.
RESULTS
Admission Characteristics A total of 60 patients were initially en-
rolled in the study. Four were later ex- cluded: two in the Vivonex group (one with acquired immunodeficiency syn- drome, one who died before initiation of feedings), one in the Nursoy group (the patient had primary renal insufficiency), and one in the chicken group (the patient had acute renal failure as a result of dehy- dration soon after admission). For the other 56 patients, Vivonex was given to
408
THE JOURNAL OF PEDIATRICS Volume 13 I, Number 3
18, Nursoy to 19, and chicken to 19. Their initial clinical and laboratory characteris- tics are Shown :in Table II. Sixty-four per- cent of the patients had associated condi- tions at the time of admission (Table II). Fifty percent had a nongastrointestinal in- fection, and 14.3% had a gastrointestinal infection.
There were no significant differences between the three groups.
Outcome A successful outcome was seen in 41 pa-
tients (73.2%): 13 (72.2%) with Vivonex, 13 (68.4%) with Nursoy, and 15 (78.9%) with chicken (not significant). During the study, 34 (60.7%) of the 56 patients had some evidence of formula intolerance: 14 (77.8%) of the patients receiving Vivonex, 11 (57.9%) Nursoy, and 9 (47.4%) chick- en (NS). The intolerance was transient in 19 (56%) of 34 patients. The other 15 (44%) (5 receiving Vivonex, 6 Nursoy, and 4 chicken) had treatment failure. The mean time from initiation of the diet to failure was 85.6 • 72 hours (60.6 • 45.7 hours with Vivonex, 98.5 • 99.9 with Nursoy, and 97.5 • 99.9 with chicken) (NS). Intestinal pneumatosis developed in 7.14% of the patients (2 patients re- ceiving Vivonex, 1 Nursoy, and 1 chick- en). One of the failures in the Nursoy group was shown to be a result of allergy to the formula.
Five patients (8.9%) died: two who had been receiving Vivonex, 1 Nursoy, and 2 chicken (NS). The patients died of intesti- nal pneumatosis (2), central line-associat- ed sepsis (2), and bacterial sepsis (K[ebsfe/[apneanwn/ae) early in the hospital course (1).
The other 10 patients with treatment failure were successfully managed, and their mean stay was 50 • 30 days. Total parenteral nutrition was required in 7 of the 10 patients, and 9 were eventually dis- charged home on a milk-containing diet regimen. The other was discharged on a soy- and milk-free diet regimen because of allergy.
Diarrhea The mean fecal output per kilogram of
body weight and the number of bowel
NURKO ET AL.
Table I IL Main outcome characteristics for the 41 patients who successfully completed the stud;/
movements per kilogram per day in the first 24 hours were similar in all groups (Table II). There were also no differences in the mean stool output per kilogram per day or in the day of cessation of diarrhea in comparison with the 41 patients who successfully completed the study (Table III).
The Figure shows the results of the sur- vival analysis done to compare the daily probability of continuing with diarrhea among the three groups. There were no differences between groups, and the me- dian duration of diarrhea, estimated by the analysis, was 8.8 days for Vivonex, 5.67 days for Nursoy, and 7.3 days for chicken.
Nutritional Outcome The mean number of total calories per
kilogram of body weight per day ingested by each group after the full diet was toler- ated was similar: 115.2 • 8.3, 111.3 • 9.1, and 116.0 • 9.6 for the Vivonex, Nursoy, and chicken groups, respectively. There was a significant difference in the amount
of protein per kilogram per clay ingested after the full diet was tolerated: 2.4 • 0.2 gm/kg per day, 3.4 • 0.3 gm/kg, and 3.5 _+ 0.4 gm/kg with Vivonex, Nursoy, and chicken, respectively (p < 0.05).
Table III shows the outcome character- istics of those patients successfully treat- ed. There was a significant weight gain in all groups and no differences between groups.
All patients in each group had an ap- parent positive nitrogen balance and a similar percentage of absorption, percent- age of retention, and biologic values. There was a statistically significant higher nitrogen balance (p < 0.02) and a tenden- cy toward a higher number of children with nutritional recovery in the chicken group (NS).
Laboratory Tests The serum albumin concentration de-
creased significantly in the Nursoy group (from 3.5 • 0.6 to 3,l • grrdcll; p < 0.05), whereas it did not change significantly in the other groups: 3.3 • 0.6 to 3.2 • 0.5
409
NURKO ET AL. THE JOURNAL OF PEDIATRICS SEPTEMBER 1997
o
"0
o e - 4
1.0
O.B
0.6
0.4
0.2
0.0
"'. \ \
- \
. \ \
- \
I a I �9
\
\ \ ~
\
o , ~ ~
VIVONEX
NUNSOY
CHICKEN
m
I I I I I "" I
0 2 4 6 B 10 12
I
14 16
Days since admiss ion F~ure. Probability of continuing diarrhea since admission: a comparison between the diets.
gngdl with Vivonex, and 3.0 + 0.7 to 3.3 + 0.3 gm/dl with chicken. There were no electrolyte abnormalities noted in children of either group, and there were .no other significant differences in laborato W val- ues between formulas (data not shown).
At the end of the study, children receiv- ing Vivonex had a significantly higher D- xNlose concentration (34.6 _+ 13.7 mg/dl) than those receiving Nursoy (23.8 _+ 10.1 mg/dl) or chicken (23.1 _+ 11.5 mg/dl) (0 <
0.05)
Milk Tolerance Test Intolerance was present in 7 patients
(17%): in none of the 13 patients in the Vivonex group, in 3 (23.07%) of 13 in the Nursoy group, and in 4 (21.1%) of 15 in the chicken group. Those with milk intol- erance had a lower admission weight (2900.83 _+ 289.24 vs 3659.28 _+ 1258.91 gm; p < 0.004), a tendency to be younger (3.91 +- 2.80 vs 6.64 + 4.1 months; p <
0.07), and a lower D-xylose concentration at baseline (17.00 ~_ 2.09 vs 23.28 • 10.6 mg/dl; p < 0.004) than those who tolerated milk. There was no difference in the D-xy- lose level at the end of the study when both groups were compared (20.66 _+ 8.61
vs 27.89 +_ 13.2 mg/dl).
Risk Factors There were significant differences (o <
0.05) between patients with treatment success and those with treatment failure with regard to the following admission characteristics: albumin concentration (3.2 _+ 0.6 vs 2.9 _+ 0,4 gm/dl), sodium con- centration (138.4 _+ 6.2 vs 133.5 _+ 7.9 mmol/L), and the incidence of associated infections (56.1% vs 86.7%). There were also differences in stool output on the sec- ond (20.9 _+ 19.8 vs 47.4 +_ 33.9 ml/kg) and third (16.7 +_ 16.5 vs 54.0 _+ 40.3 ml/kg) days. No other significant differences were found.
A sodium concentration less than 130 mmol/L (relative risk, 3.07; 95% confi- dence limits, 1.41 to 6.65) and the pres- ence of associated infections (RR, 3.61; 95% CL, 1.1 to 14.42), particularly infec- tion with Cryptospor~ium (RR, 4.15; 95% CL, 1.58 to 6.67) or pneumonia (RR, 3.25; 95% CL, 1.53 to 6.9), were identified as important factors associated with treat- ment failure.
DISCUSSION
We have shown in this study that the use of a locally available chicken-based diet is at least as effective as elemental and soy-based diets in the hospital treatment of severely malnourished children with PD. The main components of the chick- en-based diet are easily available, are cul- turally acceptable, and are inexpen- sive. 16'17 Chicken-based diets were also
previously used as an alternative for the treatment and rehabilitation of children with malnutrition 1'10'13'14 and acute diar-
rhea. 15'16 However, use of this diet in chil- dren with PD has been limited. 1'11
This study included a difficult popula- tion that is frequently excluded from other clinical trials. 1'8'13 Severely mal-
nourished children with PD usually have a high mortality rate and high treatment failure rates. There can be up to a 17-fold increase in the mortality rate, l'a'la'ya and it
has been suggested that approximately 49% (range, 23% to 62%) of diarrhea-as- sociated deaths result from PD and mal- nutrition. 1'a'13 The mortality rate found in this study (8.9%) compares favorably with rates previously reported in the liter- ature, la'93 We also did not find any differ-
ences in outcome when comparing the treatment failure rates of those children ha~ng the most extreme levels of malnu- trition (weight-for-age percentage, <40%) with the rates of less malnourished chil- dren. We confirmed that children with su- perimposed infections are at a higher risk of treatment failure, which emphasizes the need to look for and control superim- posed infections at the time of admission and nutritional rehabilitation. 13'25
As in previous studies, the diets were
4 1 0
THE JOURNAL OF PEDIATRICS Volume 13 I, Number 3
NURKO ET AL.
given at a fixed volume and the caloric density was advanced slowly. 5'6'9'2a'24
Sixty percent of children acquired some signs of intolerance while the diet regi- mens were being advanced. These signs were most likely related to carbohydrate malabsorption, 12 and a good correlation between fecal carbohydrates and total fecal output has been shown. 25 Of the three diets tested, Vivonex has a much higher carbohydrate concentration (Table I), mainly of oligosaecharides, which probably accounts for the higher inci- dence of transient intolerance seen in those patients. &25 Transient intolerance was also seen in children receiving chick- en or soy, which suggests that malnour- ished infants with PD frequently have transient intolerance to other sugars. 25 Caution should be exercised in the treat- ment of those patients in whom increasing stool outputs appear in the first and sec- ond day, because they may be at risk of failure. In those children, a slower ad- vancement of the dietary regimen may be necessary.
A potential shortcoming of this study is the difference in the macronutrient compo- sition of the diets (Table I). In Vivonex, the majority of the calories are provided by carbohydrate and the protein content is lower, &26"27 providing only about 8% of total calories. Previous studies confirm that children receiving 6.70/0 of energy as pro- tein achieved a slow compensatory growth, 24"27 and it has been shown recent- ly that, in recovering malnourished infants, there were no differences in growth when formulas with 5.5%, 6.70/0, and 8.0% pro- tein calories were compared. 28 Further- more other studies have documented the adequacy of Vivonex for growth and for treatment of PD. 5'9 It is then possible that the hydrolyzed amino acids are better ab- sorbed. 5'9 This difference in protein con- tent may partially explain why children on the chicken-based diet regimen had a sig- nificantly higher nitrogen balance than those receiving Vivonex.
The protein and caloric intakes were similar in children receiving chicken or soy feedings. The higher nitrogen balance in those receiving chicken indicates that chicken protein has a higher biologic
value than soy. Chicken has a low osmo- larity, a better amino acid score, and a higher degree of digestibility and bioavail- ability. 11'14'24 We also found a significant
decrease in the serum albumin concentra- tion in patients who received Nursoy de- spite a positive nitrogen balance. These data suggest that the protein status and lean body mass of malnourished patients fed soy formulas may be deteriorating slowly despite apparently adequate nitro- gen retention. 29 It is therefore possible that protein intake with Nursoy was inad- equate to allow more rapid accretion of ni- trogen at higher energy intakes. 29 Other problems have also been associated with the use of soy formulas in these patients. Some authors have found that nearly 50% of hospital-referred patients with PD do not recover from diarrhea a week after the introduction of a soy formula. 8 It has also been suggested that soy-containing diets may produce transient sensitivity and subtle mucosal abnormalities in the in- testinal mucosa of children with diarrhea, with the potential for increasing the sever- ity of their illness.16
Like Vivonex, 5 the chicken diet re- quires the addition of minerals. These mineral additions make preparation suit- able only in health care facilities, a factor that does not represent a major obstacle for severely malnourished children with PD, who usually require hospitalization. 4 In the community the treatment of chil- dren with PD needs to include continued feeding with locally available, inexpen- sive, and effective nutrients. I It is possible that the chicken-based diet may be anoth- er alternative once the usual therapies have failed.
All diets were administered continuous- ly via nasogastric infusion, a method of feeding that has been shown to have a beneficial effect in control of diarrhea, nu- trient absorption, nitrogen balance, and weight gain in children with PD. <8'11'1a Two main limitations of the nasogastric route need to be mentioned. The technical aspects of the placement and management of the feedings requires specialized per- sonnel and equipment, s More important- ly the child has no control over the amount of food that is being ingested,
which increases the risk of overzealous refeeding or intolerance 27 and, later, the risk of limiting the amount of nutrients in comparison with ad lib oral intake.
Although the use of milk as the sole nu- trient for children with PD has been shown to be deleterious, 12 the question that remains unanswered is when milk can safely be reintroduced into the diet of these children. We found that 83% of pa- tients who successfully finished the study were able to tolerate a full milk load at least after 2 weeks of nutritional rehabili- tation. Those children who were milk in- tolerant at the end of the study had an ini- tial lower admission weight, were younger, and had a lower D-xylose con- centration, which suggests that their ini- tial mueosal damage was greater. 6 Most likely the intolerance was related to lac- tose malabsorption, although we cannot exclude the possibility of intolerance to milk protein.
In summary, severely malnourished children with PD can be successfully managed with a chicken-based diet. These children were able to tolerate a complex diet, achieve positive nitrogen balance, and show weight gain. There was no advantage to the use of an elemental or a soy-based diet. Clear benefits of the chicken-based diet include good toler- ance, low cost, availability, and cultural acceptance. Therefore the chicken-based diet represents a good alternative for the treatment of hospitalized children with se- vere malnutrition and PD.
We express special thanks to the nurses~ resi- dents, and laboratmy personnel of the nutrition ~vard at the Hospital lnfantil de ~Ilxico for their help in the pe,formanee o/this study, in p~rtieu- la6 we thank Gina Toussaint, Dr. Liliana Worona, Dr. Alejandra Consnelo, Rosaura P~'ez, Sarah Arvizu, and Aloniea Covarrubias. We are indebted to all the personnel of the Applied Dialv'heal Disease Research Project for rhea" support during the poformance of the study. We also thank DI: Laurie Fishman and DI: Alan Leiehtner for their o'itical review of the manuscript and for lheir helpful su~gestions.
REFERENCES 1. Bhutta ZA, Hendricks KM. Nutritional
management of persistent diarrhea in child-
411
NURKO ET AL. THE JOURNAL OF PEDIATRICS SIFPTEI"IBI:R 1997
hood: a perspective from the developing world, d Pediatr Gastroenterol Nutr 1996; 22:17-37.
2. Persistent diarrhea in children in develop- ing countries. Memorandum from a World Health Organization meeting. Bull WHO 1988;66:707-17.
3. Fauvean V, Henry FJ, Briend A, Yunus M, Charkraborty d. Persistent diarrhea as a cause of childhood mortality in rural Bangladesh. Acta Pediatr 1992;381 (Suppl): 12~4.
4. Bhan MK, Arora NK, Singh KD. Manage- ment of persistent diarrhea during infancy in clinical practice. Indian d Pediatr 1991; 58:769-74.
5. Vega Franco L, Carbajal-Ouzmgm A, Garcfa-Aranda JA. Alimentacidn enteral continua en nifios lactantes empleando una dicta elemental. Bol Med Hosp Infant Mex 1982;39:651-8.
6. Orenstein S. Enteral vs parenteral therapy for intractable diarrhea of infancy: a prospective randomized trial. J Pediatr 1986; 109:277-86.
7. Kleinman RE, Galeano NE Ghishan E Lebenthal E, Sutphen J, Ulshen MH. Nutritional management of chronic diar- rhea and/or malabsorption. J Pediatr Gastroenterol Nutr 1989;9:407-15.
8. Bhutta ZA, Molla AM, Issani Z, Badruddin S, Hendrieks K, Snyder JD. Dietary management of persistent diarrhea and malnutrition: comparison of a tradition- al rice-lentil-based diet with soy formula. Pediatrics 1991;88:1010-8.
9. Sherman ,JO, Hamty CA, Khachadurian AK. Use of an oral elemental diet in infants with severe intractable diarrhea. J Pediatr 1975;86:518-23.
10. Roy SK, Haider R, Akbar MS, Alam AN, Khatum M, Eeckels R. Persistent diarrhea: clinical efficacy and nutrient absorption with a rice-based diet. Arch Dis Child 1990; 65:294-7,
11. Godard C, Bustos M, Mufioz M, Nussle D. Value of a chicken-based formula for refeeding of children with protracted diar- rhea and malnutrition in a developing coun- try. J Pediatr Gastroenterol Nutr 1989;9: 473-90.
12. Penny ME, Paredes E Brown KH. Clinical and nutritional consequences of lactose feeding during persistent postenterifis diar- rhea. Pediatrics 1989;84:835-44.
13. Maffei HV, Padula NN, Annicchino GP, Ferrari GF, Goldberg TB. Nutritional man- agement and weight changes during hospi- talization of Brazilian infants with diarrhea: primary reliance on oral feeding or continu- ous nasogastrie drip with locally made, modulated minced chicken formula, d Trop Pediatr 1990;56:240-6.
14. Larcher E Shepherd R, Francis DEM, Harries JT. Protracted diarrhea in infancy. Arch Dis Child 1977;52:597-605.
15. Romer H, Guerra M, Pina ,JM, Urrestarazu MI, Garcia D, Blanco ME. Realimentafion of dehydrated children with acute diarrhea: comparison of cow's milk to a chicken-based formula, d Pediatr Gastro- enterol Nutr 1991;13:46-51.
16. Maulrn-Radovgm I, Brown KH, Acosta MA, Fern~indez-Varela H. Comparison of a rice-based, mixed diet versus a lactose-free, soy-protein isolate formula for young chil- dren with acute diarrhea. ,J Pediatr 1994; 125:699-706.
17. Martfnez-Salgado H, Saueedo G. Mothers' perceptions about childhood diarrhea in rural Mexico. d Diarrheal Dis Res 1991;9:235-43.
18. Gomez E Ramos Galvan R, Cravioto J, Frenk S. Malnutrition in infancy and child- hood, with special reference to kwash- iorkor. Adv Pediatr 1955;7:131-55.
19. Chavez M, Hernandez M, Roldan S. Tablas de valor nutritivo de los alimentos de mayor consumo en Mexico. In: Comision National de Alimentaeion, edi-
tors. Institnto Nacinnal de la Nutricion; 1992.
20. Composition of Foods [Agricultural Handbook 8]. Washington (DC): U.S. Department of Agriculture; Oct 1975.
21. The management of diarrhea and use of oral rehydration therapy. Geneva: World Health Organization; 1985.
22. Henry RJ. Clinical chemistry principles and techniques. New York: Harper & Row; 1964.
25. MaeLean WC, Romafia GL, Massa E, Graham GG. Nutritional management of chronic diarrhea and malnutrition: primary reliance on oral feeding. J Pediatr 1980; 97:316-23.
24. Brown KH. Appropriate diets for the reha- bilitation of malnourished children in the community setting. Acta Pediatr Scand 1991;374(Suppl):151-9.
25. Lifschitz C, Carrazza F. Effect of formula carbohydrate concentration on tolerance and maeronutrient absorption in infants with severe chronic diarrhea. J Pediatr 1990; 117:578-85.
26. Field CR, Schoeller DA, Brown KH. Body composition of children recovering from se- vere protein-energy malnutrition at two rates of catch-up growth. Am ,J Clin Nntr 1989;50:1266-75.
27. Whitehead RG. Protein and energy re- quirements of young children living in the developing countries to allow for catch-up growth after infections. Am J Ctin Nutr 1977;50:1645-7.
28. Graham GG, MacLean WC, Brown KH, Morales E, Lembcke ,J, Gastanaduy A. Protein requirement of infants and chil- dren: growth during recovery from malnu- trition. Pediatrics 1996;97:499-505.
29. MacLean WC, Graham GG. The effect of energy intake on nitrogen content of weight gained by recovering malnour- ished infants. Am J Clin Nutr 1980;55: 905-9.