41
FRACTURES SURGERY DEPARTMENT MEDICAL FACULTY YARSI UNIVERSITY JAKARTA 2008
| Date post: | 13-Dec-2015 |
| Category: |
Documents |
| Upload: | afnan-alkaff |
| View: | 213 times |
| Download: | 1 times |
FRACTURES
SURGERY DEPARTMENTMEDICAL FACULTY YARSI UNIVERSITY
JAKARTA2008

Loss of bony continuity
Bony disruption

Compound fractures
Simple fractures

Direct violence
Indirect violence

Pathological fracture
Osteoporosis
Secondary metastases

Hair line fracture
Greenstick fracture
Greenstick fracture
March fracture
Fracture type
Depends on Anatomic location Region (diaphysis , metaphysis,
epiphysis, intra/extra articular) Fracture lines (transverse, oblique,
spiral) Condition of bone (comminuting,
pathologic, incomplete, segmental)

Bone loss Butterfly fragment Stress fracture Avulsion and impacted fracture Deformities (length discrepancy,
angulations, rotation, translation) Alignment
Diagnosis
1. AnamnesisMechanism of injury, history
A fracture is suspected from history and clinical examination, and confirmed by radiography
2. Physical examination
Look Asymmetry of contour
Comparing one side with the otherDisplaced, angledLocal bruising, swelling, laceration
Asymmetry of postureFemoral neck fracture with external rotationAngulations, shortening

FeelCrepitus, tenderness
Movementfalse moving/ pseudoarthrosis
Assess NVD and compartment syndrome!
Neurovascular disturbance
Neurologic Sensor and motor fx distal to fracture
site
Vascular Pulse palpation Capillary refill Warm or cold skin Color of skin

Compartment syndrome Pain Pale Parestesia Paralysis Pulseless
Pain on passive stretching of the muscle intracompartment

3. Radiological examination Two projection
Standard projections AP and lateral Two articulation
Above and below , dislocation? Two extremity
Comparison, especially in child Two times
Hair line, callus formation
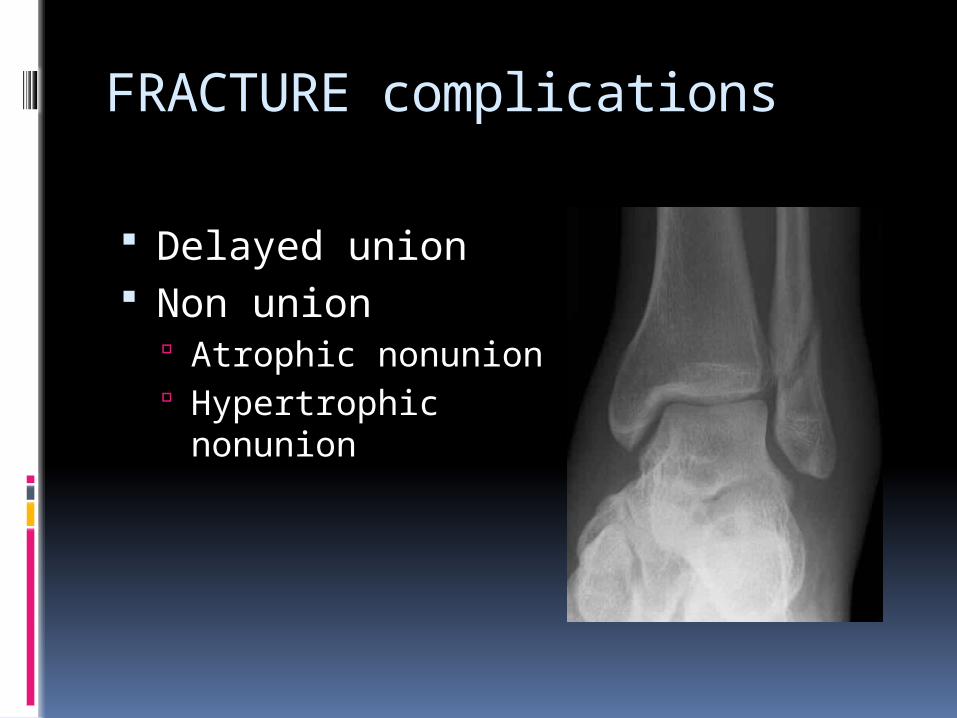
FRACTURE complications
Delayed union Non union
Atrophic nonunion Hypertrophic nonunion

Med malleolar nonunion

Diabetic nonunion

Diabetic nonunion

Pseudoarthrosis nonunion

Mal union
Colles malunion

Bone infection, osteomyelitis
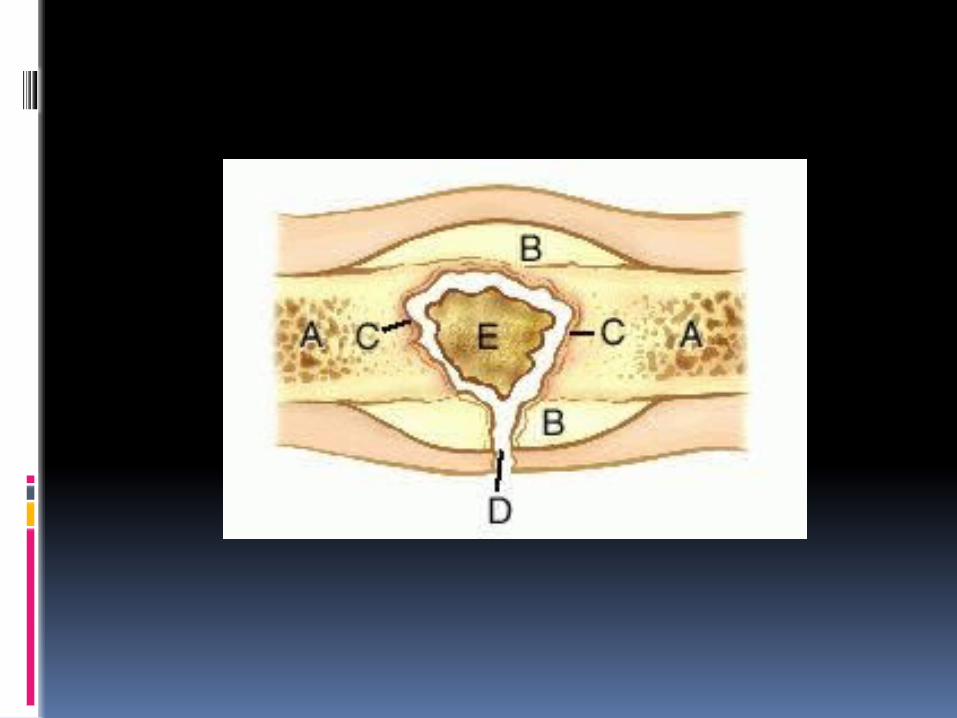

Bone infection, osteomyelitis
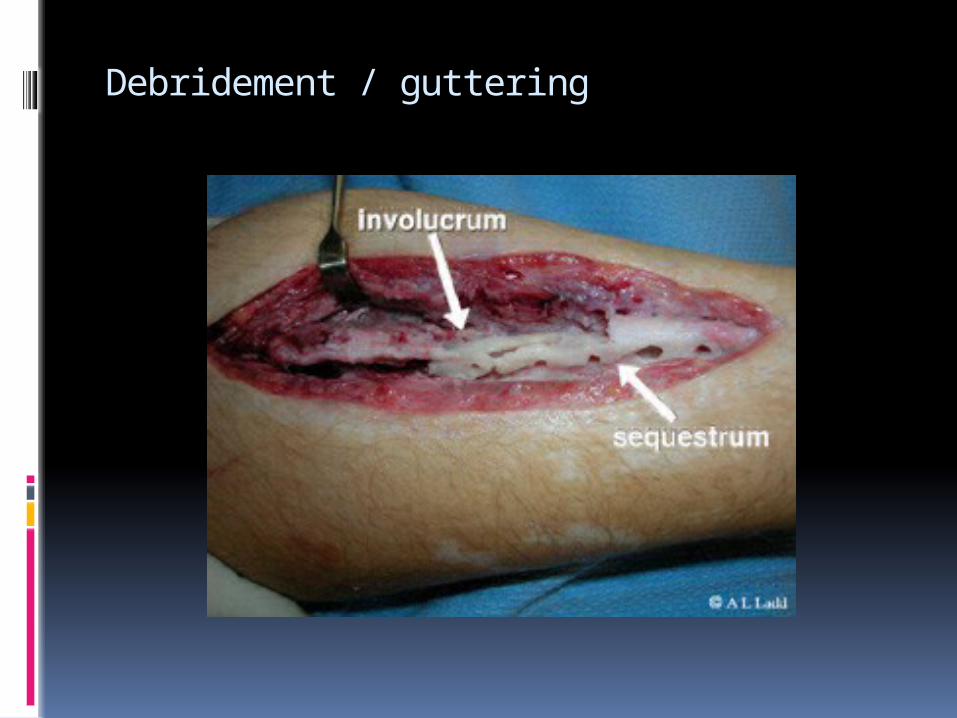
Debridement / guttering


Joint contracture, stiffness Limb shortening Compartment syndrome NVD Avascular necrosis Heterotrophic ossification

Management
Closed reduction
Splinting Casting Traction technique
Skin traction Skeletal traction
Steinmann’s pin

Open reduction

Splintage Allows sliding between implant and bone
Bridging To bridge an area of comminution

Kirschner wire Lag screw

Kirschner wire

Kirschner wire
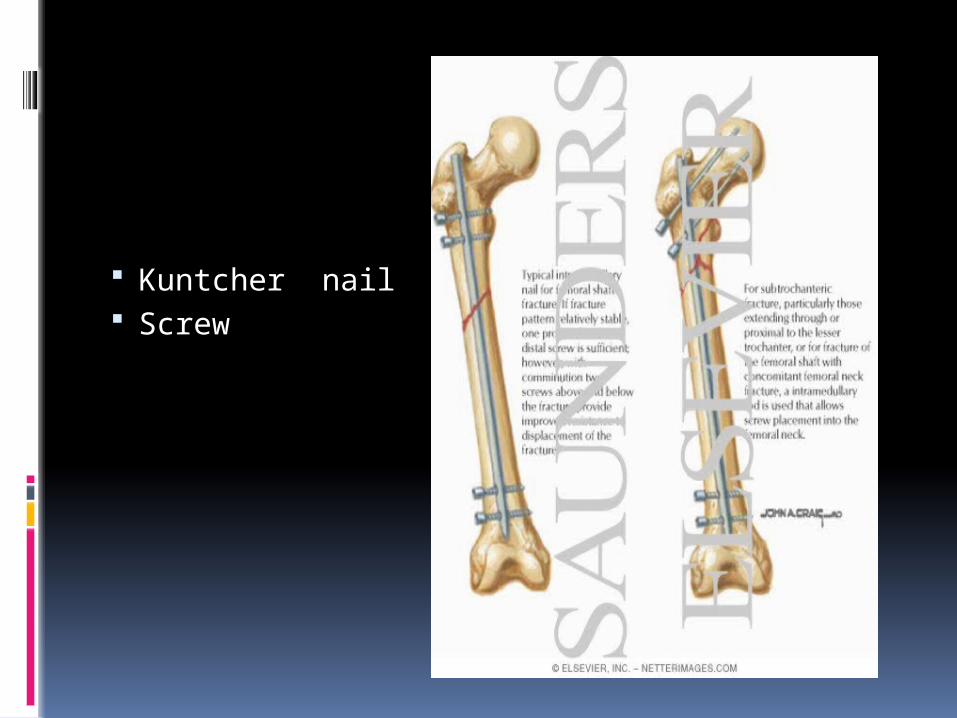
Kuntcher nail Screw

Plate and screw

External fixator
Rehabilitation
Extremely important Part of fracture management Regain optimal function asap Arrangements
Restoring ROM Stretching Strengthening
decrease pain and swelling

Lower extremity Cane Crutch walker
Fracture healing
Inflammation stageBleeding at fracture site Source of hemopoetic cells
ProliferationFibrovascular tissue developedOsteoblast, fibroblast proliferate
Repair stage Primary callus or bridging callus occur 2wks Fibrocartilage developed Soft callus to hard callus (woven bone) by ossification Medullary callus can supplements the bridging callus

Remodeling stage From midpoint repair until the fractures
heal clinically (up 7 yrs) Woven bone replaced by lamellar bone Bone assume its normal configuration
If there is anomaly in biological bone formation in healing process, there will be disturbance in the union of fractures, ex delayed or nonunion.

Factors affecting fracture healing
Type of bonecancellous bonecortical bone
Patient’s ageMobility fracture siteSeparation bone endsInfectionJoint involvementBone pathologyDisturbance of blood supply

Thank you
















