Freeport Physicians’ C.M.E. Day Waterloo – May 6, 2009 Antithrombotic Therapy in the Elderly Bill Geerts, MD, FRCPC Thromboembolism Specialist Sunnybrook Health Sciences Centre Professor of Medicine, U. of Toronto National Lead, VTE Prevention, Safer Healthcare Now!
Transcript
Freeport Physicians’ C.M.E. DayWaterloo – May 6, 2009
Antithrombotic Therapy in the
ElderlyBill Geerts, MD, FRCPC
Thromboembolism Specialist Sunnybrook Health Sciences CentreProfessor of Medicine, U. of Toronto
National Lead, VTE Prevention, Safer Healthcare Now!
Disclosures
Personal/family none investments
Grants/program Bayer, Boehringer Ingelheim, support Pfizer, Sanofi Aventis
Now: increased swelling and discomfort Lt calf and thigh
Case: Mrs. LK
Doppler ultrasound:
DVT in the popliteal and femoral veins
Case: Mrs. LK (popliteal-femoral DVT)
Which ONE of the following management options would you select?
A. Transfer to hospital for IV heparin warfarin
B. Transfer to hospital for SC LMWH
warfarin
C. LTC treatment with LMWH warfarin
D. LTC treatment with warfarin alone
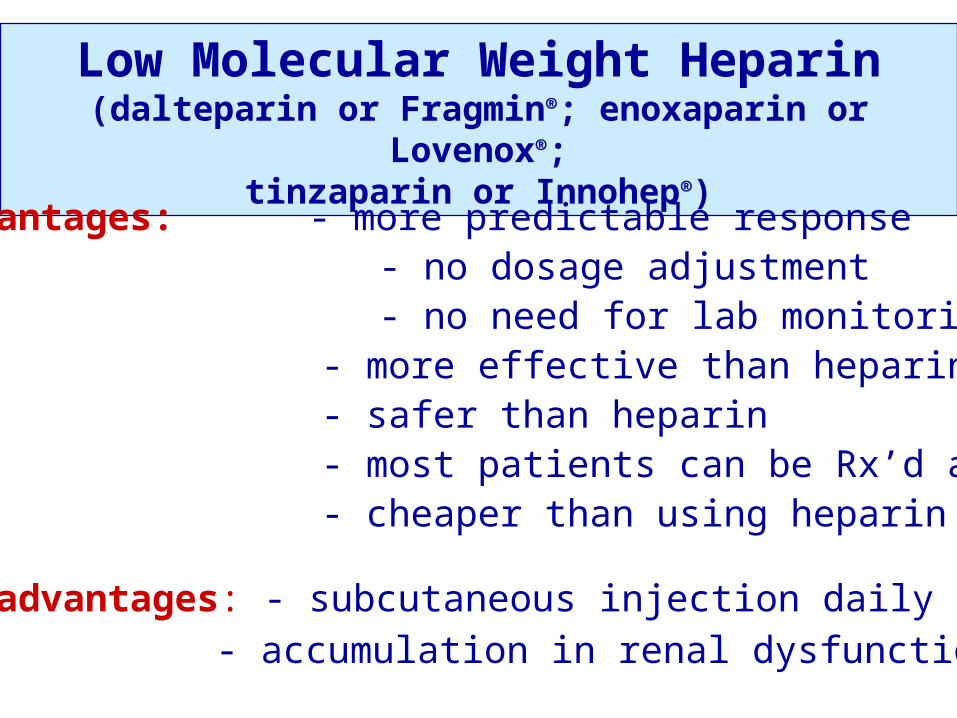
Low Molecular Weight Heparin(dalteparin or Fragmin®; enoxaparin or Lovenox®;
tinzaparin or Innohep®)
Advantages: - more predictable response - no dosage adjustment - no need for lab monitoring - more effective than heparin - safer than heparin - most patients can be Rx’d as OP - cheaper than using heparin
Disadvantages: - subcutaneous injection daily- accumulation in renal dysfunction
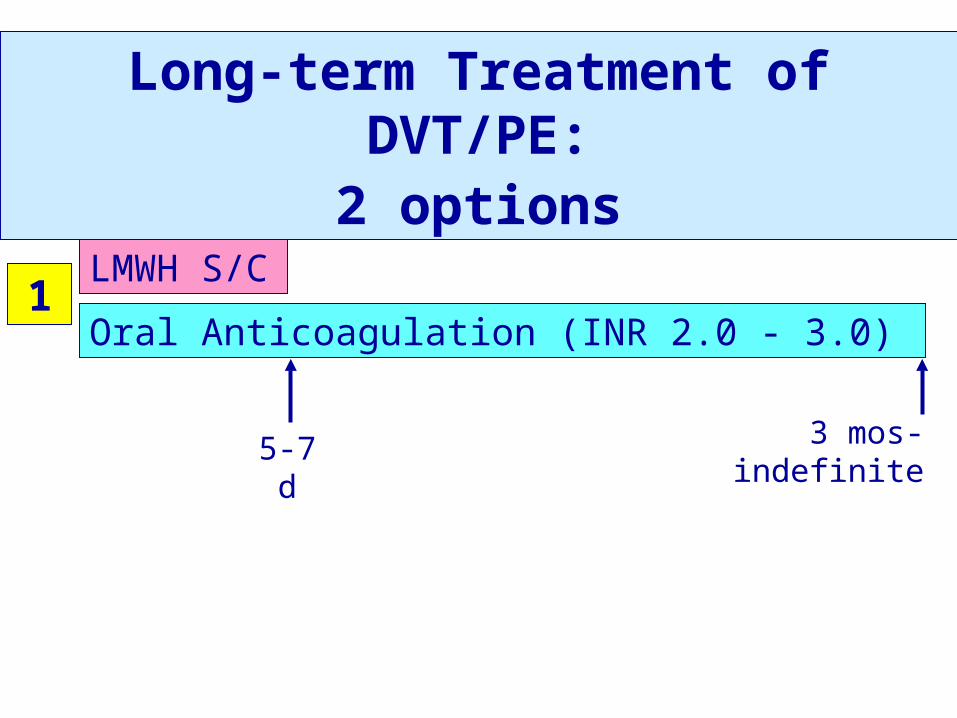
Long-term Treatment of DVT/PE:
2 optionsLMWH S/C
Oral Anticoagulation (INR 2.0 - 3.0)
5-7 d 3 mos-indefinite
1
Case: Mrs. LK (popliteal-femoral DVT)
Which of the following management options would you select?
A. Transfer to hospital for IV heparin warfarin No reason to admit or to use heparin
B. Transfer to hospital for SC LMWH warfarin No reason to admit to hospital
C. LTC treatment with LMWH warfarin YES = treatment of choice
D. LTC treatment with warfarin alone Never for proximal DVT
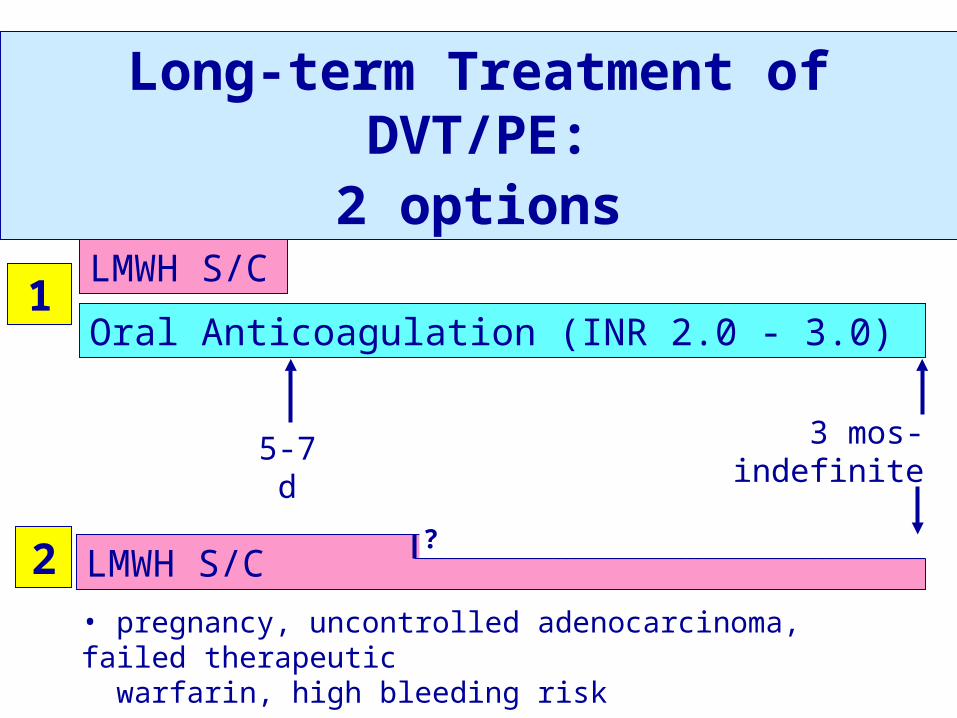
Long-term Treatment of DVT/PE:
2 optionsLMWH S/C
Oral Anticoagulation (INR 2.0 - 3.0)
5-7 d 3 mos-indefinite
LMWH S/C?
1
2• pregnancy, uncontrolled adenocarcinoma, failed therapeutic warfarin, high bleeding risk
Case: Mrs. LK (popliteal-femoral DVT)
What else would you do?
A. Bedrest until pain & swelling decreases
B. Do hypercoagulability testing
C. Look for occult cancer
D. Repeat the Doppler US at 3 months to look for resolution of the DVT
Case: Mrs. LK (popliteal-femoral DVT)
What else would you do?
A. Bedrest until pain & swelling decreases No
B. Do hypercoagulability testing No
C. Look for occult cancer No
D. Repeat the Doppler US at 3 months to look for resolution of the DVT No
2. Treatment of VTE
• Acute treatment of VTE: LMWH (most as OPs)
• Long-term treatment of VTE:
1) warfarin INR 2-3
2) LMWH – active adenocarcinoma, high bleeding risk, pregnancy
• Encourage patients to remain active (do not restrict mobility)
1. The Problem: thrombosis and anticoagulants in the elderly
2. Treatment of VTE
3. Starting and maintaining oral anticoagulation
4. Thromboprophylaxis: implications for geriatric patients / long-term care
Antithrombotic Therapy in the Elderly: Objectives
There is a 50-fold variation in
warfarin maintenance
dose!
(0.5 mg/day – 25 mg/day)
• 100 Sunnybrook Anticoagulation Clinic Patients
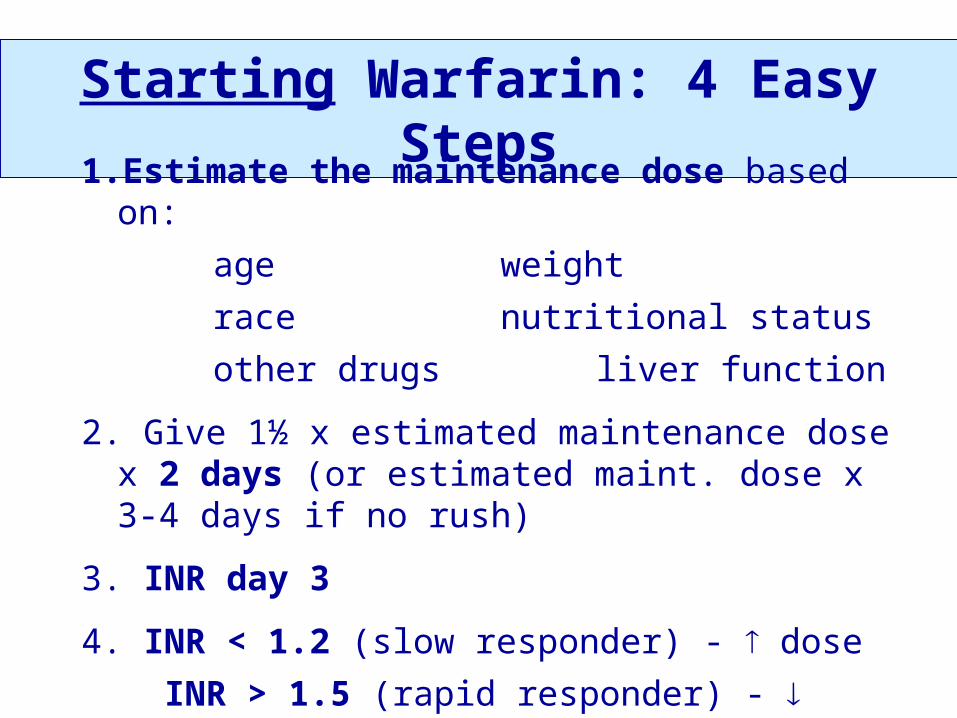
Starting Warfarin: 4 Easy Steps
1. Estimate the maintenance dose based on:
age weight
race nutritional status
other drugs liver function
2. Give 1½ x estimated maintenance dose x 2 days (or estimated maint. dose x 3-4 days if no rush)
3. INR day 3
4. INR < 1.2 (slow responder) - dose
INR > 1.5 (rapid responder) - dose
INR 1.2-1.5 – continue estimated maint. dose
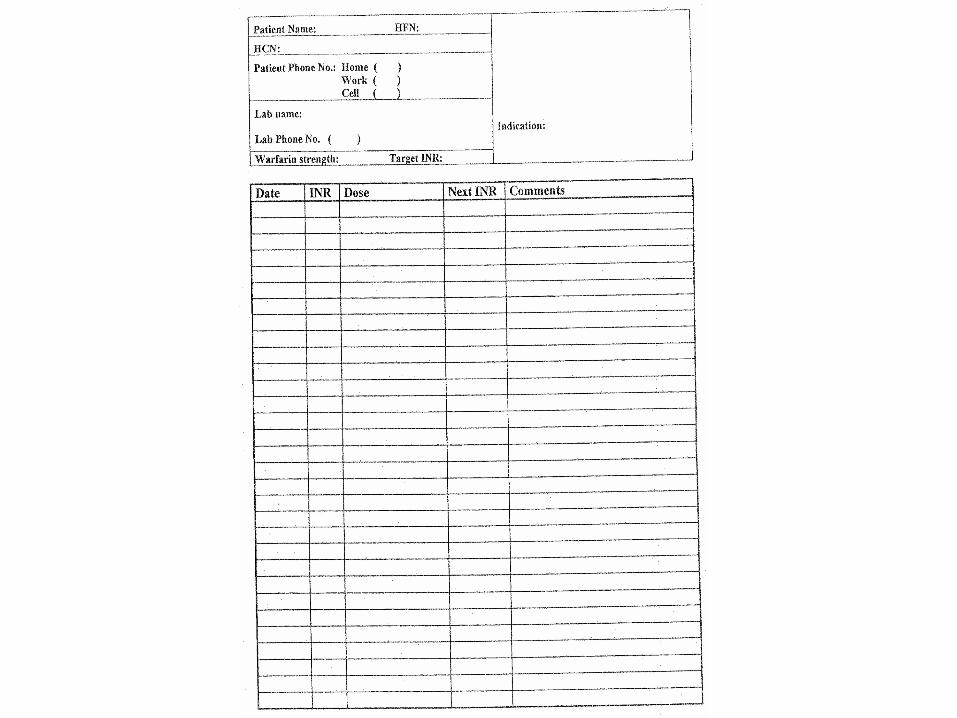
Maintaining Warfarin in Elderly• Obsessive longitudinal record of doses, INR
results using a warfarin dosing sheet
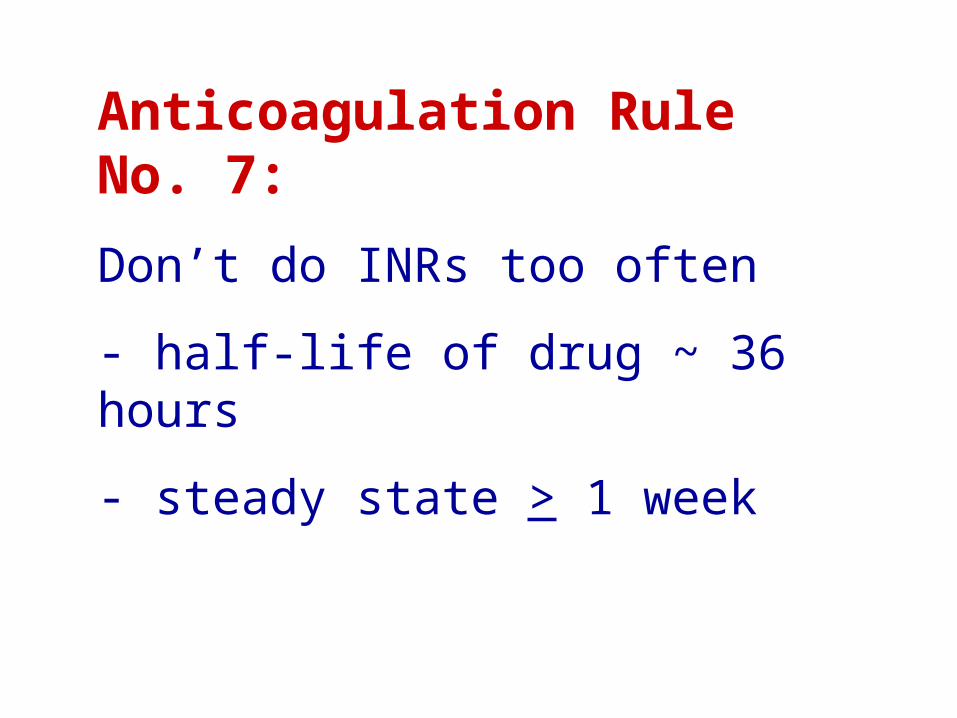
• INR at least once a month
• Automatic alerts for missed INRs
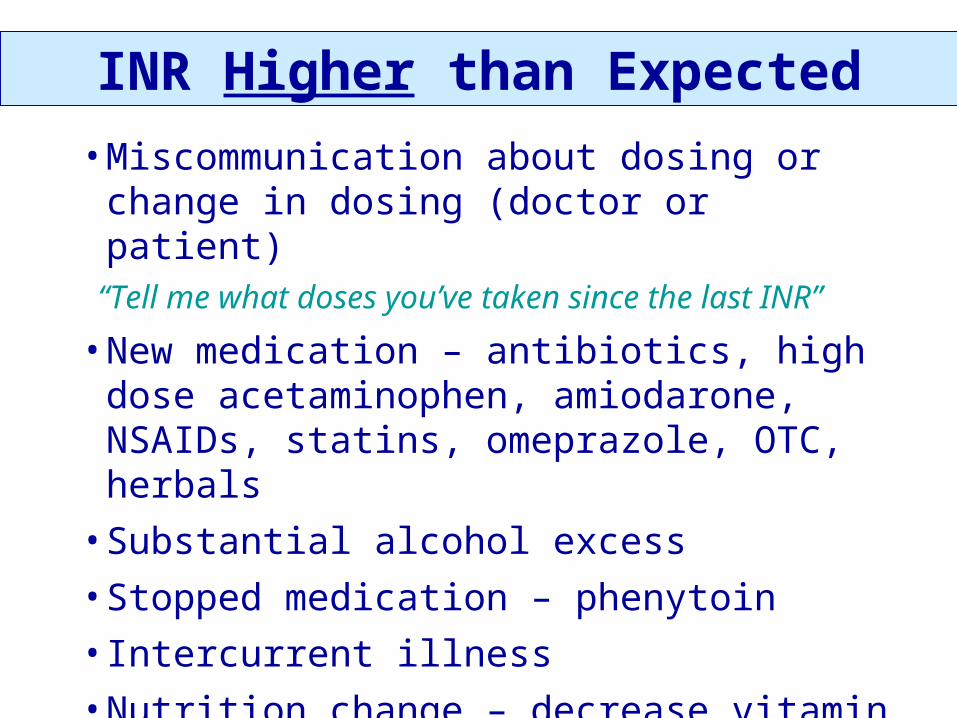
• Instruct patients/staff to report meds, acute illness, bleeding
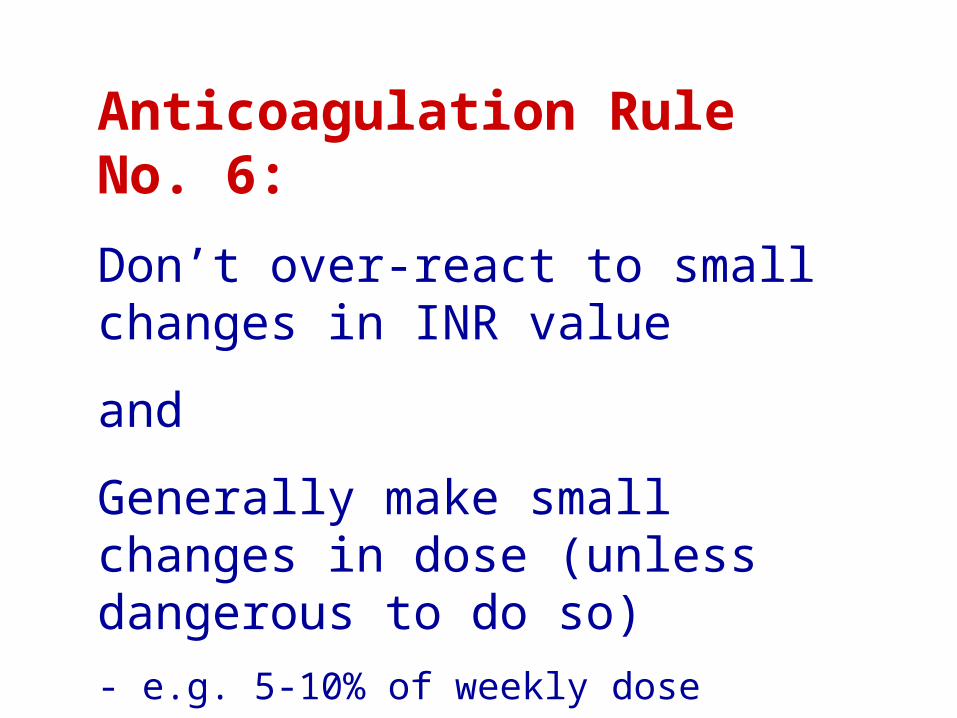
• Don’t over-react to single INR value - use long-term trends
• Use an anticoagulation clinic, if possible, or pharmacist-run management, or obsessive care
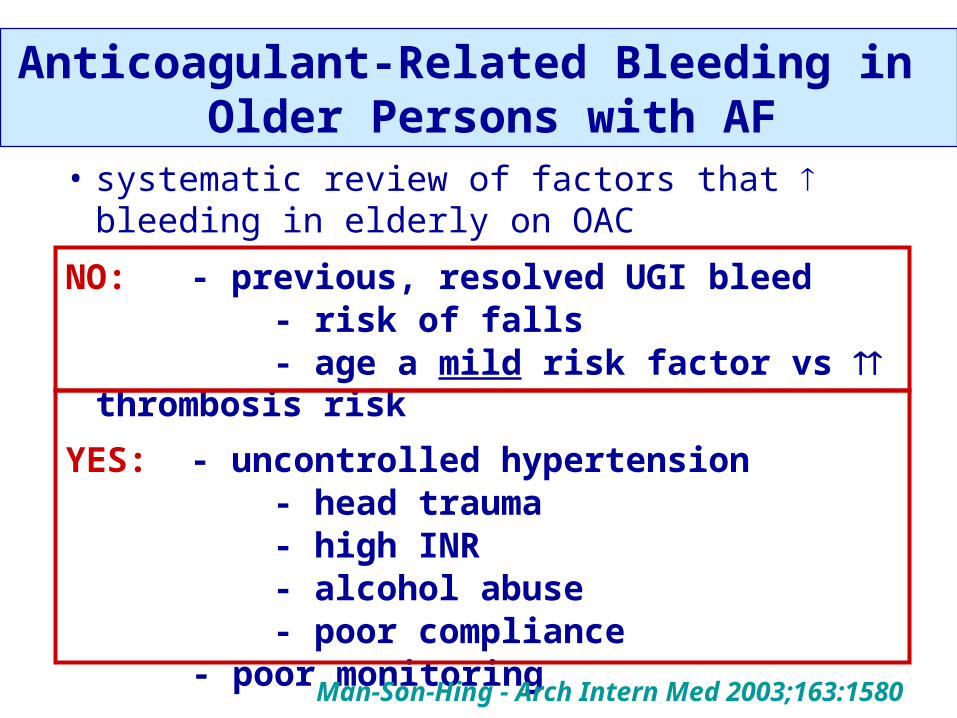
Bleeding and Risk of Falls
decision analysis in elderly with atrial fibrillation
Risk of falling is not an important factor in
decision re antithrombotic therapy
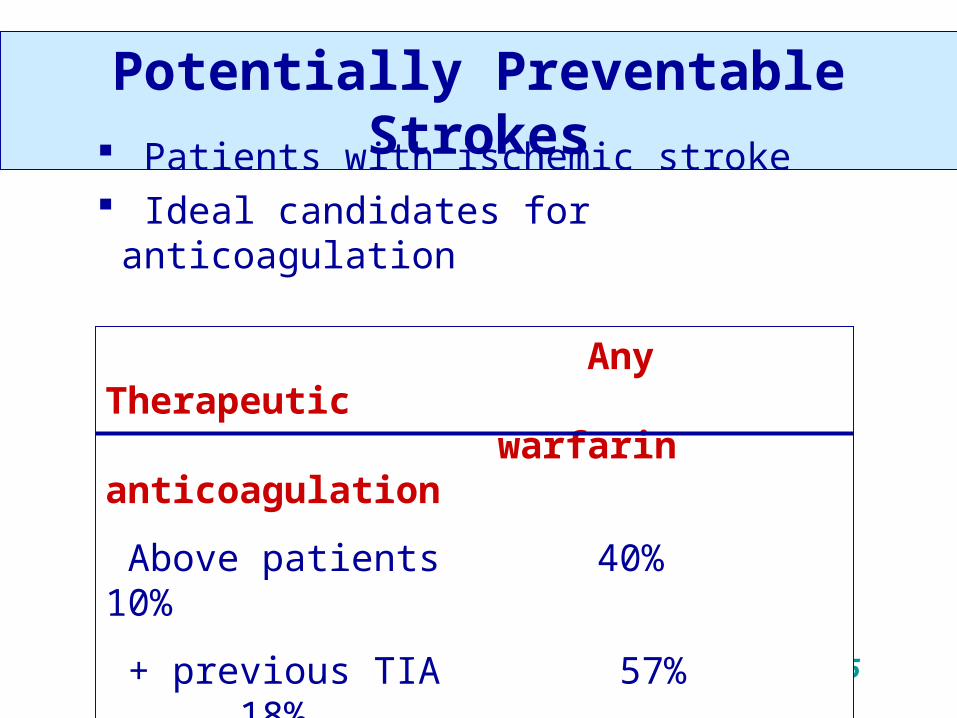
With an average risk of stroke from AF
(5%/yr), benefit:risk favors anticoagulation
unless the person falls > 300 times/yr!
Man-Son-Hing - Arch Intern Med 1999;159:677
Hypertension and Intracranial Bleeding
• BP > 160/95 7 x risk of ICBBrott - Stroke 1986;17:1078Saloheimo - Stroke 2001;32:399Qureshi - NEJM 2001;344:1450
• Hypertension risk of intracerebral bleed in patients taking oral anticoagulants
Hylek - Ann Intern Med 1994;120:897
SPAF - Arch Intern Med 1996;156:409
Diet and Warfarin Use
Do NOT advise restriction of vitamin K-containing food = associated with less stable INR values
Encourage foods high in vitamin K (broccoli, spinach, brussels sprouts)
“Let me know if you plan a major change in your usual diet.”
ASA and Warfarin Use
• Generally AVOID
• No additional benefit for most patients
• Definite increase in bleeding risk
• There must be a good reason for the ASA e.g. coronary artery stent; high-risk mechanical heart valve; TIA despite INR >2
• Therefore, the combination of an antiplatelet agent and warfarin must be an ACTIVE decision
Case: Mrs. LK (popliteal-femoral DVT)
What duration of anticoagulation would you provide?
A. 3 months
B. 6 months
C. 12 months
D. Until the DVT resolves
E. Indefinite
Recurrent
VTE
Anticoagulation
Time
Treatment Duration for VTE
0
• secondary
• idiopathic• active cancer• some thrombophilia (APLAS, AT def)• big residual clot
Duration of Treatment for VTE
Recurrent Episodes: indefinite*
1st Episode:
Transient, reversed risk 3 - 6 mos
Idiopathic 12 mos indefinite*
Continuing risk (unresolved cancer, AT deficiency, APLA) indefinite*
Duration of Treatment for VTE
Recurrent Episodes: indefinite*
1st Episode:
Transient, reversed risk 3 - 6 mos
Idiopathic 12 mos indefinite*
Continuing risk (unresolved cancer, AT deficiency, APLA) indefinite*
*Periodic reassessment re:
1) New patient risk factors for bleeding, thrombosis
2) New knowledge
3) Patient preference
Case: Ms. LK (popliteal-femoral DVT)
What duration of anticoagulation would you provide?
A. 3 months
B. 6 months
C. 12 months
D. Until the DVT resolves
E. Indefinite – unless important bleeding risk
> recurrent thrombosis risk
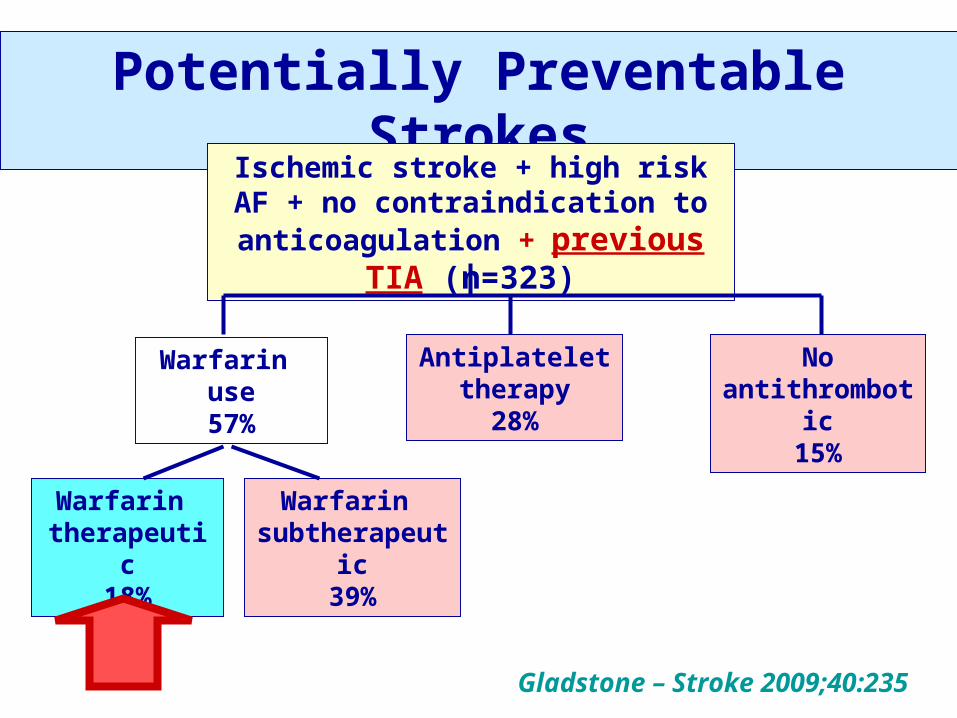
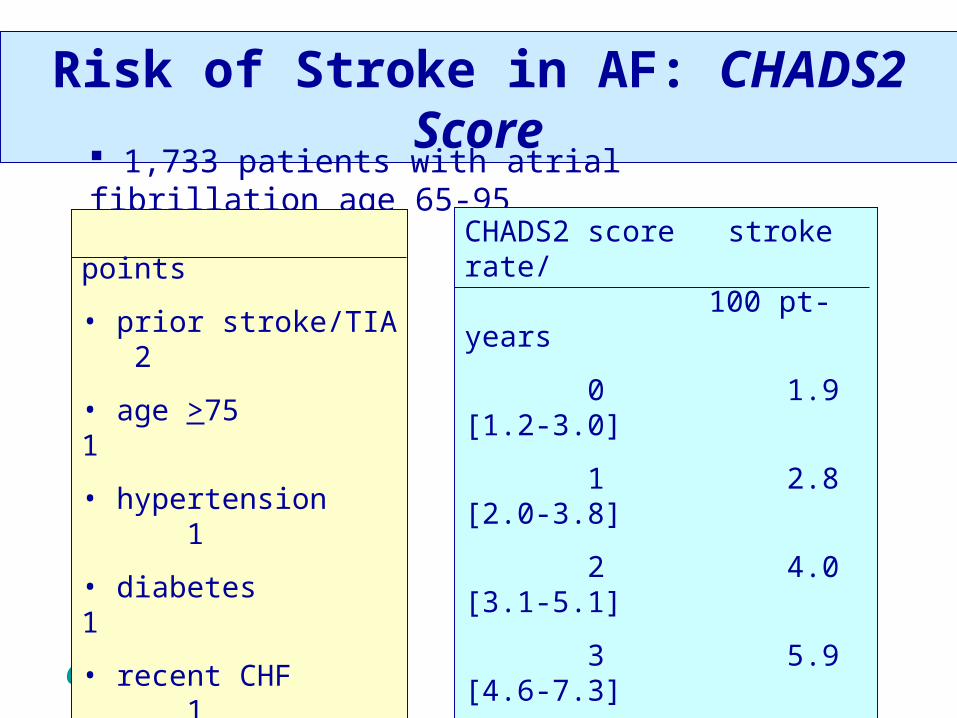
1. Most patients with AF should be on warfarin
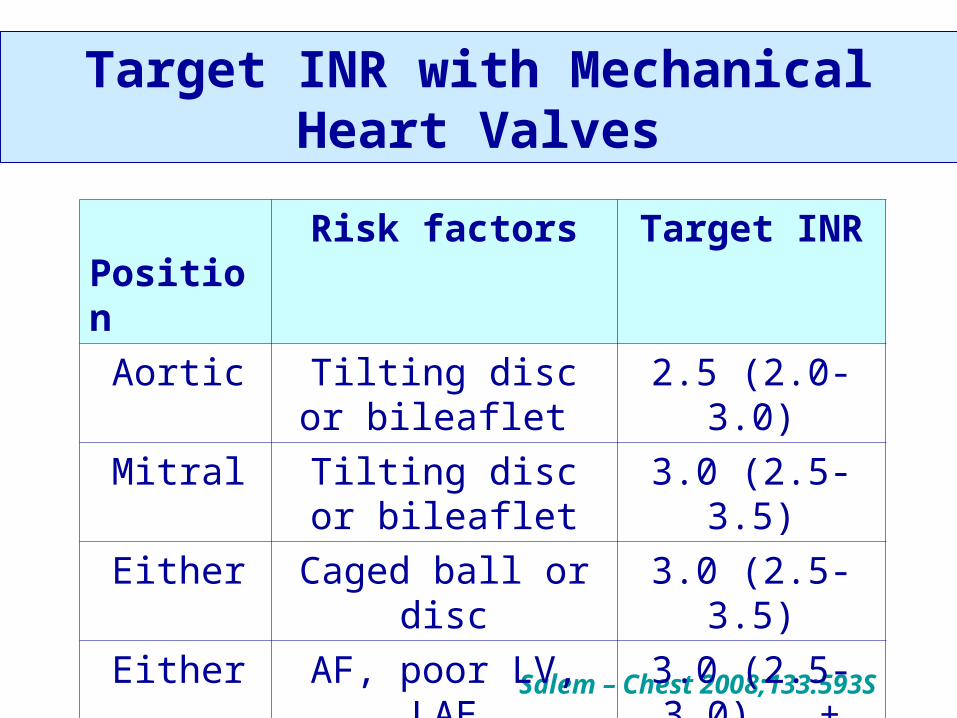
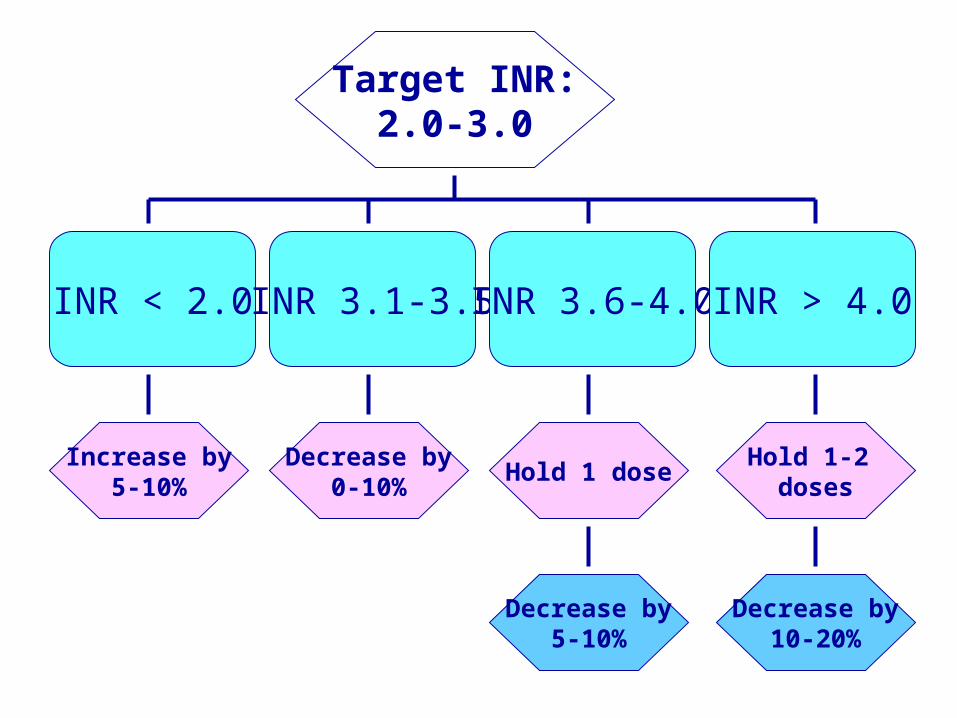
2. INR 2.0-3.0 (2.5-3.5 for high risk mechanical heart valve)
3. Need an obsessive system to monitor OAC – it makes a difference to outcomes (+ remember CMPA)
4. Avoid combined antiplatelet agent and warfarin unless a very good reason
5. Manage hypertension well
6. Encourage vitamin K intake
3. Starting and maintaining oral anticoagulation
1. The Problem: thrombosis and anticoagulants in the elderly
2. Treatment of VTE
3. Starting and maintaining oral anticoagulation
4. Thromboprophylaxis: implications for geriatric patients / long-term care
Antithrombotic Therapy in the Elderly: Objectives
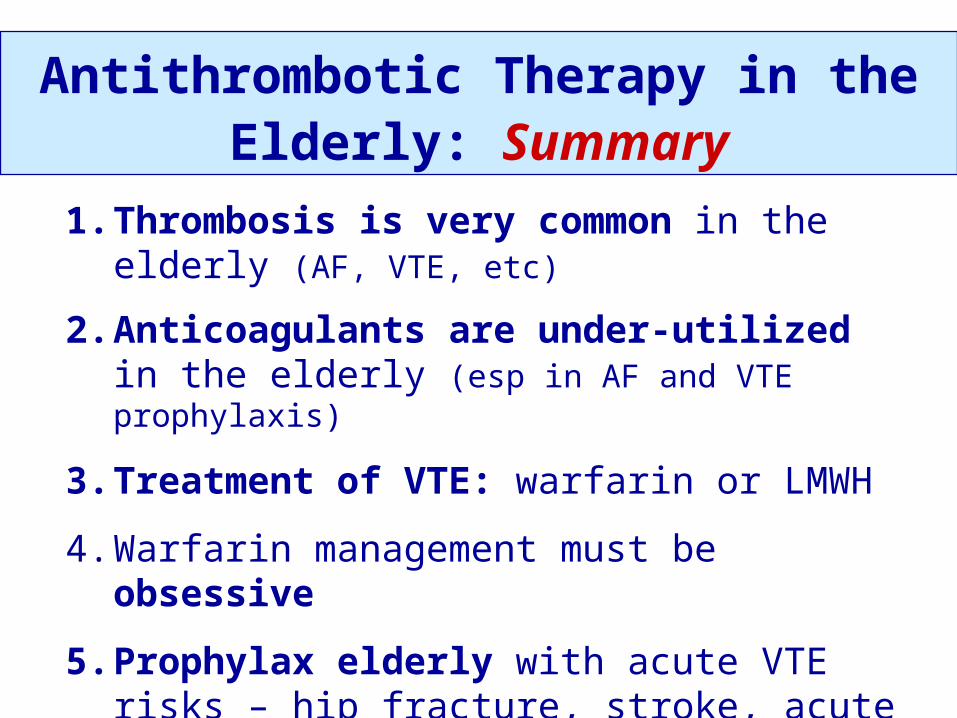
Thromboprophylaxis Summary
Patient Group
Options Duration
Medical illness • Low Mol Wt Heparin• Low dose heparin
1. The Problem: thrombosis and anticoagulants in the elderly
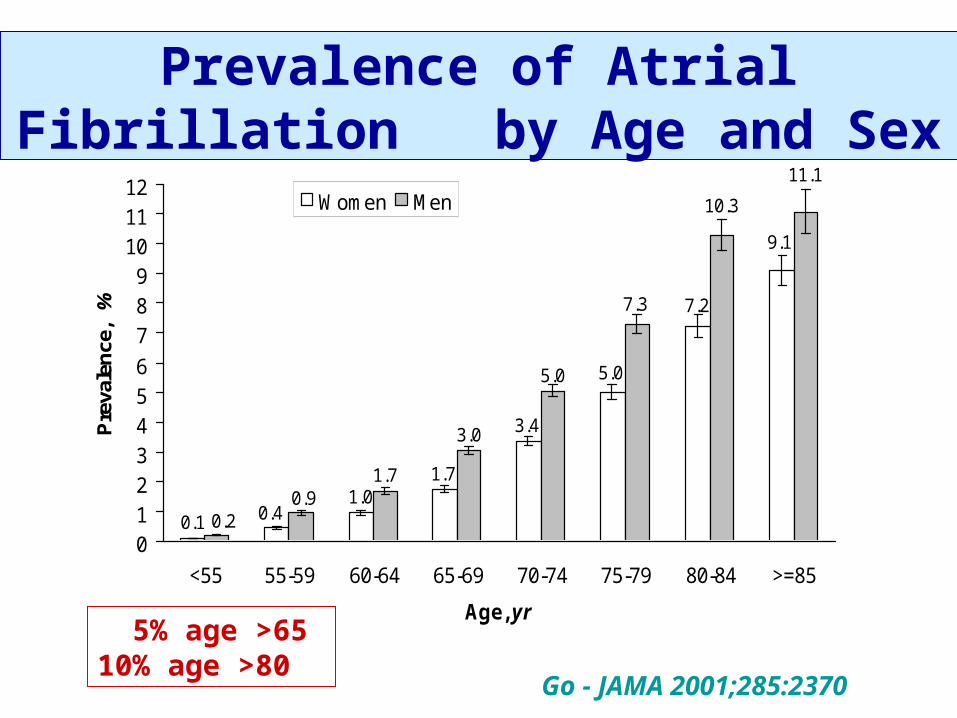
In the elderly:
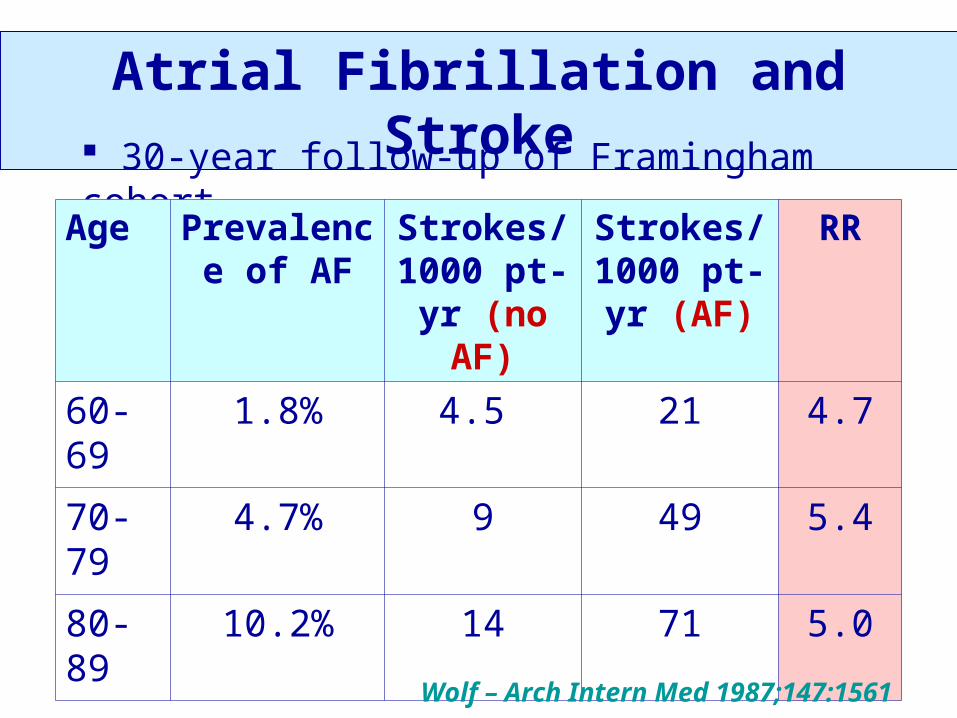
• Thromboembolism (AF, stroke, VTE, cardiomyopathy, etc) is very common
• Anticoagulants are very effective in preventing thrombosis
• Physicians tend to underuse anticoagulants
• Bleeding risk increased
• Anticoagulants can be dangerous
Prophylactic and treatment doses of LMWHs are NOT the
same• For a 75 kg patient with normal renal function
LMWH Prophylaxis dose
Treatment dose
dalteparin
(Fragmin®)
5,000 U QD 15,000 U QD
(200 U/kg QD*)
enoxaparin
(Lovenox®)
30 mg bid or
40 mg QD
120 mg QD
(1.5 mg/kg QD*)
tinzaparin
(Innohep®)
4,500 U QD 13,125 U QD
(175 U/kg QD*)*no maximum
8th ACCP Guidelines on Antithrombotic Therapy
2008;133:67S-968S
8th ACCP Guidelines on Antithrombotic Therapy
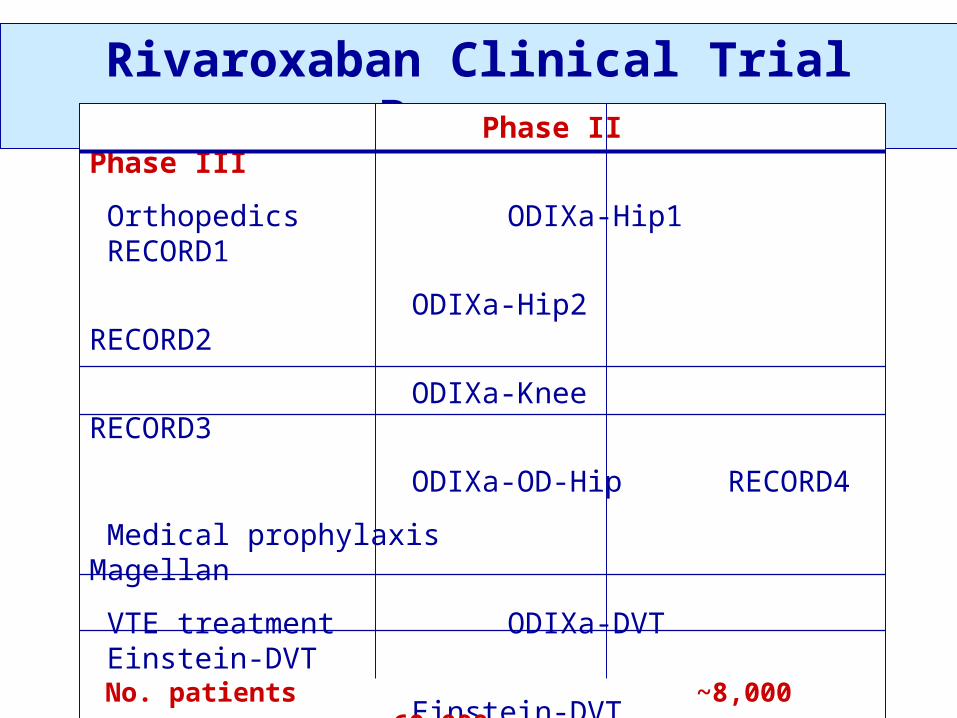
• Anticoagulants: heparin, LMWH, warfarin
• Antiplatelet agents
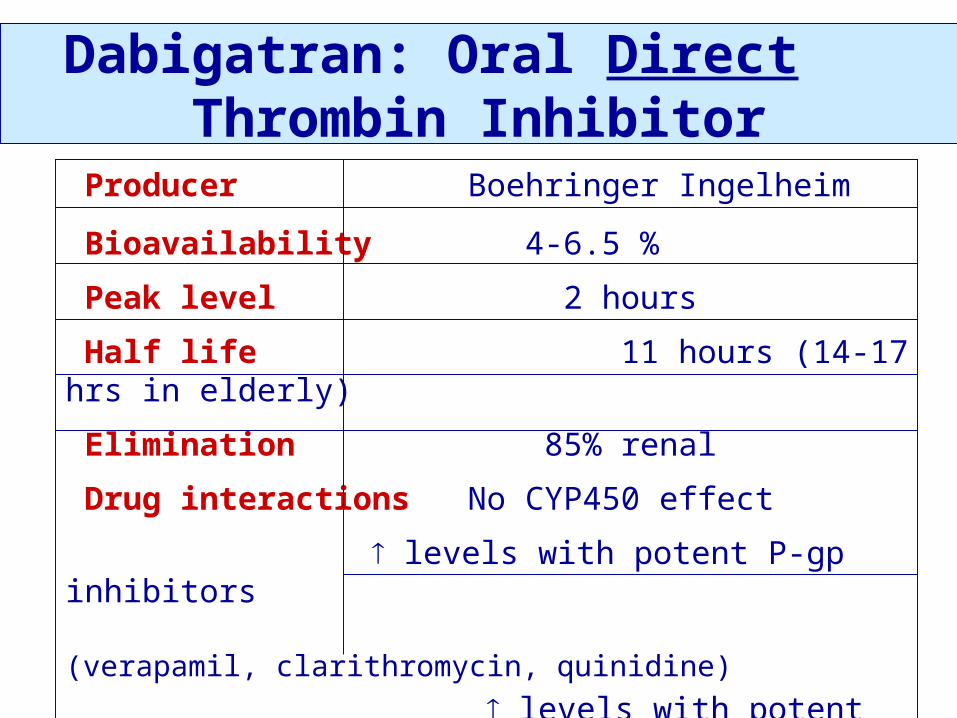
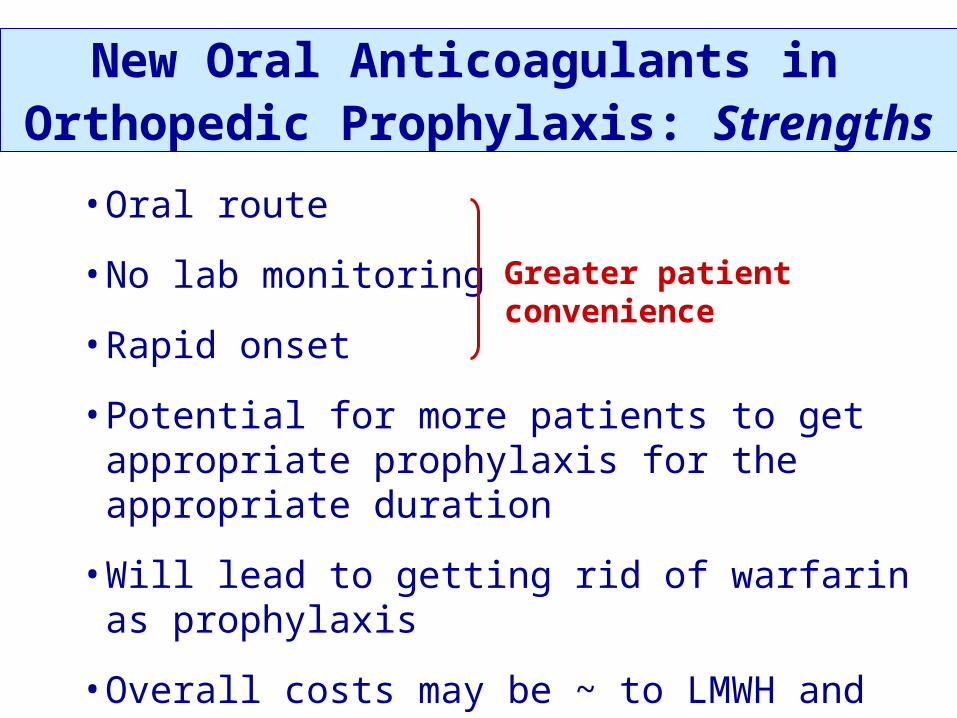
• New antithrombotic drugs
• Complications of antithrombotic therapy: bleeding, HIT
• Prevention of venous thromboembolism
• Treatment of venous thromboembolism
• Peri-procedure management
• Arterial disease: AF, CAD, stroke, PAD, valvular disease
• Pregnancy and pediatric thrombotic issues
Thromboembolism Risk Groups8th ACCP Guidelines on the Prevention of VTE (2008)
• General surgery• Vascular surgery• Gynecologic surgery• Urologic surgery• Thoracic surgery• Bariatric surgery• Laparoscopic surgery• Cor. bypass surgery• Hip arthroplasty• Knee arthroplasty• Knee arthroscopy• Hip fracture surgery
• Spine surgery• Lower extremity injuries• Neurosurgery• Major trauma• Spinal cord injuries• Burn patients• Medical patients• Cancer patients • Central venous catheters• Critical care patients• Long distance travel
Geerts – Chest 2008;133:381S
ACCP Guidelines on Thromboprophylaxis
For each patient group:
1. risks of VTE
2. prophylaxis evidence
3. graded recommendations
1. Graduated compression stockings
(TEDS™, elastic stockings)
2. Intermittent pneumatic compression
devices (SCDs™, leg squeezers)
3. Foot pumps
Mechanical Methods of Prophylaxis
1. Graduated compression stockings
(TEDS™, elastic stockings)
2. Intermittent pneumatic compression
devices (SCDs™, leg squeezers)
3. Foot pumps
• If used properly, these methods work in some patients, but
• They generally don’t work as well as anticoagulants, and
• They require a big effort to work at all.
Mechanical Methods of Prophylaxis
Using Mechanical Prophylaxis:
1. Ensure they fit properly
2. Start ASAP
3. Have on ~24 hours/day – only remove
- for leg washing
- when patient actually walking
4. Don’t stop when patient starts to walk
Mechanical Methods of Prophylaxis
1.4.3 Mechanical prophylaxis used primarily:
- in patients at high risk of bleeding
[Grade 1A],
- or possibly in addition to anticoagulant
prophylaxis [Grade 2A]
Recommend careful attention to proper use of
and optimal compliance with mechanical
prophylaxis [Grade 1A]
8th ACCP Conference on Antithrombotic Therapy
Geerts – Chest 2008;133:381S
1. Low dose heparin / minidose heparin heparin 5,000 U SC Q12H or Q8H