Page 1
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 1/33
From Pain to Sleep: Listening to
Patient‐Reported
Outcomes
Pediatric Trends 2009
Pamela S. Hinds, PhD, RN, FAAN
Director, Nursing Research
Children’s National Medical Center
Washington, D.C.
Objectives:
• describe the role of nurses in generating clinical
research questions as influenced by patient‐reports.
• analyze the evolution of a research program
centered around nurses’ responses to patient‐
reported outcomes
Page 2
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 2/33
Amazing Collaborators
• Marilyn Hockenberry, PhD, RN, PNP,FAAN
• Heather Jones, MN
• Sue Zupanec, MN
• Ching‐Hon Pui, M.D.
• Mary Relling, PharmD
• Deo Kumar
Srivastava,
PhD
• Susan Clifton, RN
Amazing Collaborators
• Nancy K. West, BSN, CRA
• Michele Pritchard, PhD, PNP
• Kelly Vallance, M.D.
• Jami Gattuso, MSN
• Jia Yang,
PhD
• Brett Loechelt, MD
• Jane Sande, MD
Page 3
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 3/33
Patient‐Reported Outcomes
• What are they?
‘a measurement of any aspect of patient’s health
status that comes directly from the patient (i.e.,
without the interpretation of the patient’s
responses by physician or others)’
– FDA, 2006
PROs: why
such
interest?
• Provide clinically valuable information about
the patient’s experience with treatment or
disease‐related care
• Symptoms
• Toxicities
• Burden
• Benefits
Page 4
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 4/33
PROs: Why such Interest?
• FDA Preference
– Guidance for Industry: Patient‐Reported Outcome
Measures, 2006
• NIH Involvement
– Instrumentation Funding Opportunities
• AHRQ Report
– Lorenz, Lynn,
Hughes
et
al.,
2006
PROs in
Pediatrics
• Not always possible
– Disease or treatment factors
– Developmental status
– Family culture
• Reasonable reliance upon proxy reports
– Early
involvement
of
proxies
–not
just
at
end
of
life
Page 5
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 5/33
PROs at End of Life
0
1
2
3
4
5
6
7
8
In eligible Patien t Pare nt Staff R ecord Oth er
PROs Require
• Respect for the child’s voice
• Standardized ways to invite the child’s voice
• Action on behalf of the child’s report
Page 6
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 6/33
From Pain to Sleep:
• Initial study in the pediatric intensive care unit
to study instruments by patient‐reported pain
• Compared scores and acceptability of
instruments to children ages 4 and older
• Faces Scale, Hester Poker Chips, VAS
• Cultural aspects for parents
• Child report:
‘you
think
pain
is
the
worst… it’s
not.’
Fatigue
Page 7
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 7/33
Distinguishing Fatigue in its Age‐
Related forms
• One of 10 monitored symptoms: Fatigue was rated
as most prevalent and distressing
• Two‐site Fatigue Scholars’ Program (Oncology
Nursing Society)
– Conceptual Definitions
– Instruments
What is
fatigue?
• Cancer‐related fatigue (focus groups,
individual interviews, concept analysis)‐ – In 7 to 12 year olds: a profound sense of being weak or
tired, or of having difficulty with movement such as
arms or legs too heavy to life and eyes to heavy to open.
» Hinds, Hockenberry ‐Eaton, Gilger et al., 1999
– In 13 to 18 year olds: a changing state of
exhaustion that is a physical condition, at other
times a mental
state,
and
at
other
times
a
combination of physical, emotional and mental
tiredness» Hinds, Hockenberry ‐Eaton, Gilger et al.,1999
Page 8
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 8/33
Method Differences with
Adolescents
• Individual Interviews: Code for Sadness
• Focus groups: Code for Anger
– implications for measurement and clinical
assessment identified
– Education sheets created
CONTRIBUTING FACTORS
Environmental Personal/Behavioral Cultural/Family/Other Treatment-Related
• Lacking a schedule• Interruptions in ahospital environment
Environmental Personal/Behavioral Cultural/Family/Other Treatment-Related
FATIGUE
ALLEVIATING FACTORS
• Protected rest time
• Controlled or reducedinterruptions• Being quiet
++ + +
_ _ _ _
Page 9
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 9/33
Measuring Fatigue and the
Derivation of Screening Items
• Instruments:
– Fatigue Scale – Child (10‐item; 7 day and 24‐hour versions; cut
score)
– Fatigue Scale – Adolescent (14‐item; 7 day and 24‐hour
versions)
– Fatigue Scale – Parent (17‐item; 7 day and 24‐hour versions)
– Fatigue
Scale
– Staff
(9‐
item;
7
day
and
24‐
hour
versions)
– Symptom Distress Scale – Patient (10‐item; ‘this day’)
InstrumentationInstrument Internal
Consistency
Construct Validity‐
Factor Analysis
Construct
Validity ‐
Correlations
FS‐Child 0.84 Lack of energy
Can’t function
Altered mood
0.35/FS‐Parent
0.16/FS‐Staff
0.45/
Depression
FS‐Adolescent 0.95 Lack of energy
Can’t function
Altered mood
Can’t engage
0.76/FS‐Parent
0.27/FS‐Staff
0.87/
Depression
FS‐Parent 0.88 Lack of energy
Can’t function
Altered Sleep
Altered Mood
0.43/Staff
Page 10
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 10/33
Instrumentation
• Child and Adolescent versions distinguished between
those experiencing anemia and those who were not.
• Gender differences: females reporting more
symptoms of fatigue and higher intensity
• Age: adolescents
reported
more
symptoms
of
fatigue
and higher intensity than did children
Clinical Screen
Item:
• ‘Tired’ Item from the SDS:
Please put a circle around the number that most closely
measures how tired you are feeling today.
Could not feel I am not
more
tired
5 4
3
2
1 tired
at
all
(score of 3 or higher invites a full fatigue assessment)
Page 11
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 11/33
Clinical Screen Item
• NCCN Guidelines
Research Instruments to Measure Cancer‐related Fatigue
in Children and Adolescents
• Child Fatigue Scale (7‐to 12‐year olds) – Hockenberry et al., 2003
• Adolescent Fatigue Scale (13‐to18‐ year olds) – Hinds et al., 2007
• The Revised Memorial Symptom Assessment Scale (7‐to 12‐year olds) – Collins et al., 2002
• The Pediatric FACT Scale
– Lai et
al.,
2007
• The Symptom Distress Scale (8‐ to 18‐ year olds) – Hinds, et al., 2000; Hinds et al., 2002
• PedsQL Fatigue Scale (8 to 12; 13 to 18 year olds) – Varni et al., 2004
Page 12
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 12/33
Incidence of Fatigue in Children and Adolescents
with Cancer “nearly universal”
• Distressing levels reported at:
– time of diagnosis (fatigue at diagnosis is predictive of fatigue during
treatment)
– Collins et al., 2002; Hinds et al., 1999
– During treatment (significantly increased during reinduction for ALL and
during hospitalizations)
– Hockenberry et al., 2003; Hinds et al., 1990; Hinds et al, 2007
– Up to 23 years following treatment (most distressing)
– Crom et
al.,
200x;
Meeske
et
al.,
2005
– During the last 30 days of life – Wolfe et al., 2000
CONTRIBUTING FACTORS
Environmental Personal/Behavioral Cultural/Family/Other Treatment-Related
• Lacking a schedule• Interruptions in a
hospital environment
Environmental Personal/Behavioral Cultural/Family/Other Treatment-Related
FATIGUE
ALLEVIATING FACTORS
• Protected rest time
• Controlled or reducedinterruptions
• Being quiet
++ + +
_ _ _ _
Page 13
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 13/33
Actigraph• Sleep Parameters
– Sleep duration
– Sleep efficiency
– Nocturnal
awakenings
– Actual sleep minutes
– Total daily sleep
minutes
– Total daily nap
minutes
– Total nocturnal sleep
minutes
– Sleep latency
– Wake after sleep
onset
https://reader010.{domain}/reader010/html5/0627/5b3378f5a84ba/5b3378fc51b3e.jpg
Page 14
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 14/33
Benefits of Actigraphy
• Small and innocuous
• Able to attach to wrist or ankle for prolonged periods of
time- able to assess motion and thus sleep patterns
overtime
• Provides continuous activity data with little interference
or limitations imposed on the subject
• Can be used in the home environment
• Does not require ongoing monitoring by professionals• Cost effective
American Academy of Sleep Medicine
Recommendations
• Actigraphy has proven useful for
delineating sleep patterns and
documenting treatment response in
normal children, as well as in special
populations
Morgenthaler et al(2007)
Page 15
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 15/33
The first
Intervention
• Enhanced Activity in Hospitalized Children
with Cancer
• 2‐site, randomized pilot study
• 27 patients with a solid tumor or AML
diagnosis admitted for chemotherapy
• Peddling twice daily for 20 minutes
• Intervention successfully delivered 85.4% of
scheduled times
Page 16
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 16/33
The first Intervention
• Trend towards the activity arm having better quality
sleep (more efficient) (F=4.17, p=0.053)
• Children experiencing 19 or more nocturnal
awakenings were significantly more fatigued the
next day
• Children with higher nocturnal awakenings had
longer
sleep
duration
(F=6.35,
p=0.0007)
Dexamethasone (DEX), Sleep and
Fatigue
• Examining treatment influences on fatigue
and sleep in children with ALL
• Study purpose:
– To assess the relationship between systemic
exposure to DEX and sleep quality and fatigue in
patients with ALL during continuation
Page 17
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 17/33
DEX, Sleep and Fatigue
• Two hypotheses:
– 1. DEX contributes to changes in sleep efficiency,
actual sleep minutes, sleep duration, nocturnal
awakenings, total daily sleep minutes, and daily
nap minutes and to increased fatigue
– 2. patient age, sex and ALL risk category influence
the extent
of
change
in
sleep
and
fatigue
observed during DEX treatment
Study Design
Days: 1 2 3 4 5 6 7 8 9 10
No DEX DEX
Actigraph worn
•Sleep Diary•Fatigue Scale(parent and patient)
•Sleep Diary•Fatigue Scale(parent and patient)
Blood SamplesPre-DEX, 1,2,4,8 h
10 Continuous
Page 18
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 18/33
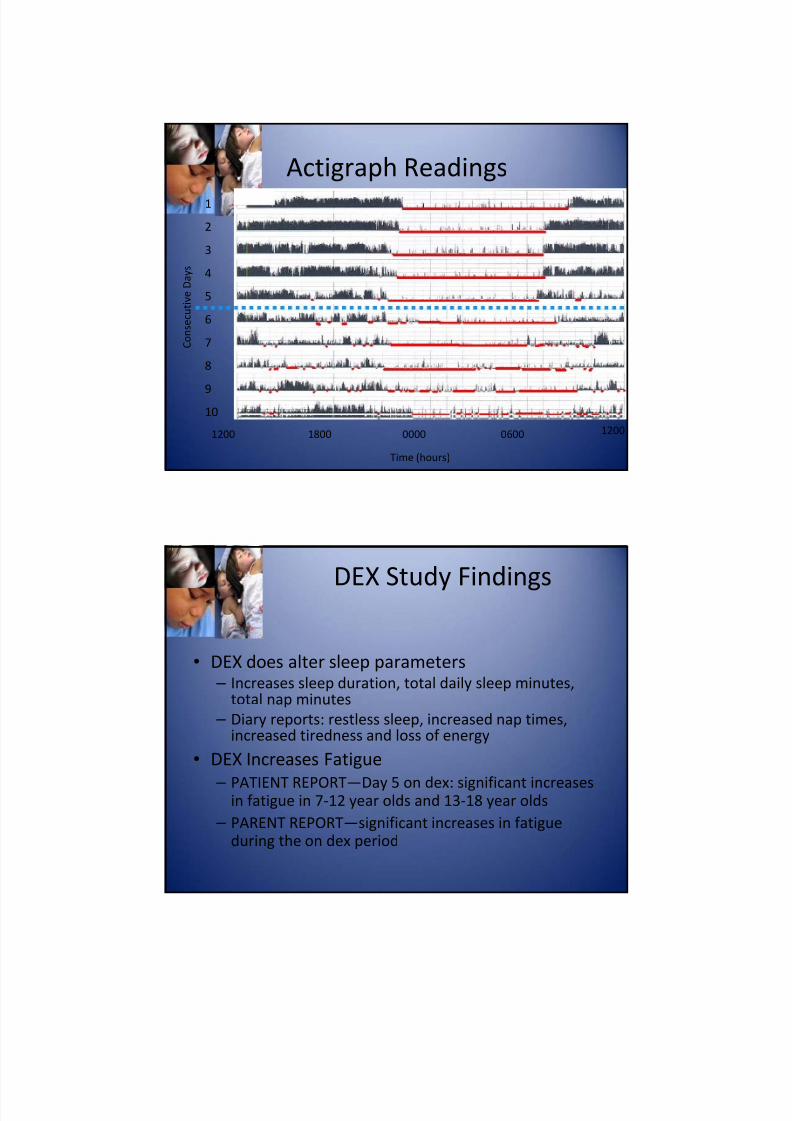
Actigraph Readings
1200 06001800 0000 1200
Time (hours)
1
2
3
4
5
6
7
8
910
C o n s e c u t i v e
D a y s
DEX
Study
Findings
• DEX does alter sleep parameters – Increases sleep duration, total daily sleep minutes,
total nap minutes
– Diary reports: restless sleep, increased nap times, increased tiredness and loss of energy
• DEX Increases Fatigue
– PATIENT REPORT—Day
5 on
dex:
significant
increases
in fatigue in 7‐12 year olds and 13‐18 year olds
– PARENT REPORT—significant increases in fatigue
during the on dex period
Page 19
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 19/33
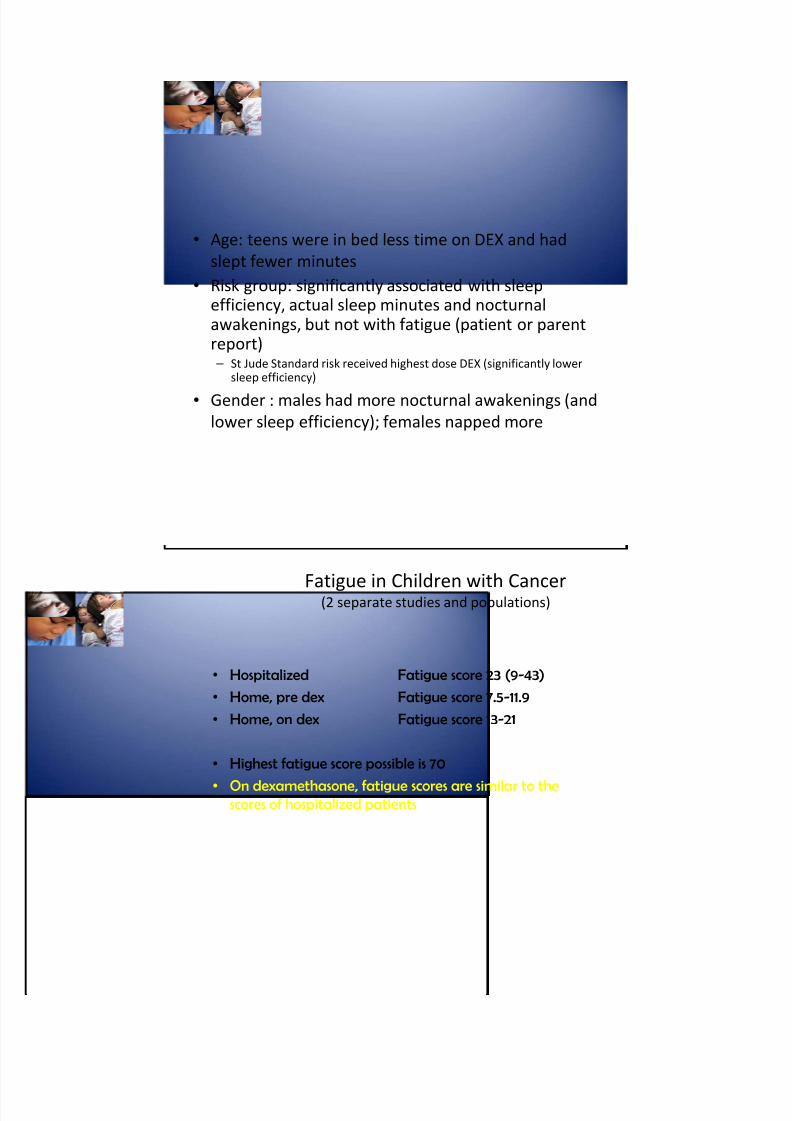
• Age: teens were in bed less time on DEX and had
slept fewer minutes
• Risk group: significantly associated with sleep
efficiency, actual sleep minutes and nocturnal awakenings, but not with fatigue (patient or parent report) – St Jude Standard risk received highest dose DEX (significantly lower
sleep efficiency)
• Gender : males
had
more
nocturnal
awakenings
(and
lower sleep efficiency); females napped more
Fatigue
in
Children
with
Cancer(2 separate studies and populations)
• Hospitalized Fatigue score 23 (9-43)
• Home, pre dex Fatigue score 7.5-11.9
• Home, on dex Fatigue score 13-21
• Highest fatigue score possible is 70
• On dexamethasone, fatigue scores are similar to thescores of hospitalized patients
Page 20
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 20/33
Fatigue in Adolescents with Cancer(2 separate studies and populations)
• Hospitalized Fatigue score 32
• Home, pre dex Fatigue score 23-29
• Home, on dex Fatigue score 32-33
• On dexamethasone, fatigue is the same as whenhospitalized
• Adolescents report higher fatigue scores than do children
Daily Parent
Report
Diary
• 15 item parent report scale
• Reports parents perceptions of child’s sleep and nap
patterns during the previous 24 hours
• Additional items relate to naps, tiredness,
consumption of selected food items and perceived
energy levels
• Items strongly correlated with actigraph findings(r=0.89;p=0.001) (Sadeh, 1994)
• Completed 4 times during 10 day study period
Page 21
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 21/33
Page 22
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 22/33
Consistency of wake time by
gender, weekday vs weekend,
and DEX
vs.
No
Dex
•Girls did not have significant differences in wake time consistency
weekday versus weekend
•Boys had more consistent wake time on weekdays compared to
weekends
•Boys had more consistent wake times compared to girls
•Dexamethasone (week 2) did not significantly alter wake time
consistency
Association of fatigue with consistent
wake time
• Multiple regression analysis: younger boys
with more consistent wake times had
lower fatigue scores
• May suggest that consistent morning wake times
for the
younger
child
on
ALL
maintenance
therapy
can help to minimize fatigue
Page 23
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 23/33
Potential Biological Mechanisms of
Sleep Disturbance and of Fatigue
• What are the potential biological mechanisms? – Steroids?
– PK, PGN
– Albumin?
– Cytokines?
– Neuroanatomy or Neurophysiology?
– Neurochemicals?
Potential Biological Mechanisms of
Sleep Disturbance and of Fatigue
• Steroids contribute to altered sleep
disturbances and fatigue
– How?
• Pharmacokinetics
– Exposure to dexamethasone (AUC) increases with age and is higher
in standard care ALL risk compared to low risk groups
– Wake after
sleep
onset
increases
as
AUC
increases
– A decrease in time to attain threshold of 100 nM is significantly
associated with increased sleep efficiency
– No PK association with fatigue
– No association with clearance and sleep or fatigue
Page 24
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 24/33
Potential Biological Mechanisms of
Sleep Disturbance and of Fatigue
• Steroids contribute to altered sleep
disturbances and fatigue
– How?
• Pharmacogenomics: SNP genotype and sleep and
fatigue
– AHSG/C>G exon 7 (sleep efficiency)
– CYP11B2/K1733R (sleep duration)
– IL6/IL6_C‐634‐G (sleep duration)
Potential Biological Mechanisms of
Sleep Disturbance and of Fatigue
• Albumin and dexamethasone – Low albumin likely leads to higher and longer exposure to dexamethasone
– Relationship between albumin and fatigue established in adults (direct
relationship not mediated by a steroid)
• Wang et al., 2002, JCO
– albumin and
dexamethasone
associated
during
reinduction
• Yang, et al., 2008, JCO
– No relationship between albumin and dexamethasone PK during
continuation
Page 25
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 25/33
Can we improve sleep and fatigue in
children with cancer?
• Increase daytime physical activity
• Modify the hospital sleep environment
• Use relaxation interventions
• Administer pharmacologic interventions
• Consider complimentary therapies
• Implement Educational interventions:
‐ preparing families for likely and fatigue changes
‐ share with families sleep hygiene principles and hours
of sleep needed for their child
Sleep Hygiene
Principles
• consistent bed times and wake times
• making sure that your child receives enough sleep every
day to feel alert and well rested
• naps based on developmental age and stage
• limiting caffeine before bedtime
• child's bedroom at a comfortable temperature
• Child not
going
to
bed
hungry
• child's bed and bedroom are inviting and comfortable
• a regular bedtime ritual to help child prepare for nighttime
sleep
Page 26
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 26/33
Page 27
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 27/33
What will happen to me in this study?
You will have to wear the Actigraph all the time you are in the hospital.The Actigraph looks like a watch. It is a little computer.It will tell us how well you sleep.
You will answer questions one time a day.We will ask you about your sleep and how you feel.
Page 28
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 28/33
You will choose special things to do before you go to bed.These are things to help you sleep. We will visit you and help you.
You will choose some soothing sounds to listen to at night.
Page 29
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 29/33
You will choose your “lights out” and “lights on” time
You will let us draw a little bit of extra blood for special tests.This would be with morning labs.
Page 30
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 30/33
What will we do?
The staff will try hard to go in and out of your room less at night.They will come in if you want them to.
We will put up an extra window cover to keep light out of your roomwhen you are sleeping.
Page 31
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 31/33
From Pain to Sleep: PROs
• Asking and then Listening to our patients
• Having a standardized way of asking
• Acting on patients’ reports
Page 32
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 32/33
Reference List
Carskadon MA. Patterns of sleep and sleepiness in adolescents. Pediatrician. 1990;17:5‐12.
Cleeland CS, Bennett GJ, Dantzer R et al. Are the symptoms of cancer and cancer treatment due to a shared biologic mechanism? A cytokine‐
immunologic model of cancer symptoms. Cancer 2003;97:2919‐2925.
Hinds PS, Hockenberry‐Eaton M, Gilger E et al. Comparing patient, parent, and staff descriptions of fatigue in pediatric oncology patients. Cancer Nurs. 1999;22:277‐288.
Hinds PS, Schum L, Srivastava DK. Is clinical relevance sometimes lost in summative scores? West J.Nurs.Res. 2002;24:345‐353.
Hinds P, Scholes S, Gattuso J, Riggins M, Heffner B. Adaptation to illness in adolescents with cancer. J.Pediatr.Oncol.Nurs. 1990;7:64‐65.
Hinds PS, Hockenberry MJ, Gattuso JS et al. Dexamethasone alters sleep and fatigue in pediatric patients with acute lymphoblastic leukemia. Cancer 2007;110:2321‐2330.
Hart CN, Palermo TM, Rosen CL. Health‐related quality of life among children presenting to a pediatric sleep disorders clinic. Behav.Sleep
Med. 2005;3:4‐17. K
Kurzrock R. Cytokine deregulation in hematological malignancies: clinical and biological implications. Clin.Cancer Res. 1997;3:2581‐2584.
Kurzrock R. The role of cytokines in cancer‐related fatigue. Cancer 2001;92:1684‐1688.
Lee BN, Dantzer R, Langley KE et al. A cytokine‐based neuroimmunologic mechanism of cancer‐related symptoms. Neuroimmunomodulation.
2004;11:279‐292.
Meeske KA, Siegel SE, Globe DR, Mack WJ, Bernstein L. Prevalence and correlates of fatigue in long‐term survivors of childhood leukemia. J.Clin.Oncol. 2005;23:5501‐5510.
Mindell, J. A. and Owens, J. A. Lee BN, Dantzer R, Langley KE et al. A cytokine‐based neuroimmunologic mechanism of cancer‐related
symptoms. Neuroimmunomodulation. 2004;11:279‐292.
Vardy J, Chiew KS, Galica J, Pond GR, Tannock IF. Side effects associated with the use of dexamethasone for prophylaxis of delayed emesis after moderately emetogenic chemotherapy. Br.J.Cancer 2006;94:1011‐1015.
Wood LJ, Nail LM, Gilster A, Winters KA, Elsea CR. Cancer chemotherapy ‐related symptoms: evidence to suggest a role for proinflammatorycytokines. Oncol.Nurs.Forum 2006;33:535‐542.
References II
Belluco C, Olivieri F, Bonafe M et al. ‐174 G>C polymorphism of interleukin 6 gene promoter affects interleukin 6 serum level in
patients with colorectal cancer. Clin.Cancer Res. 2003;9:2173‐2176.
Fayad L, Cabanillas F, Talpaz M, McLaughlin P, Kurzrock R. High serum interleukin‐6 levels correlate with a shorter failure‐free
survival in indolent lymphoma. Leuk.Lymphoma 1998;30:563‐571.
Hong S, Mills PJ, Loredo JS, Adler KA, Dimsdale JE. The association between interleukin‐6, sleep, and demographic characteristics.
Brain Behav.Immun. 2005;19:165‐172.
Rich T, Innominato PF, Boerner J et al. Elevated serum cytokines correlated with altered behavior, serum cortisol rhythm, and
dampened 24‐hour rest‐activity patterns in patients with metastatic colorectal cancer. Clin.Cancer Res. 2005;11:1757‐1764.
Schiller JH, Storer BE, Witt PL et al. Biological and clinical effects of intravenous tumor necrosis factor‐alpha administered three
times weekly. Cancer Res. 1991;51:1651‐1658.
Vgontzas AN, Bixler EO, Lin HM et al. IL‐6 and its circadian secretion in humans. Neuroimmunomodulation. 2005;12:131‐140.
Vgontzas AN, Zoumakis E, Bixler EO et al. Adverse effects of modest sleep restriction on sleepiness, performance, and
inflammatory cytokines. J.Clin.Endocrinol.Metab 2004;89:2119‐2126.
Vgontzas AN,
Zoumakis
E,
Lin
HM
et
al.
Marked
decrease
in
sleepiness
in
patients
with
sleep
apnea
by
etanercept,
a tumor
necrosis factor‐alpha antagonist. J.Clin.Endocrinol.Metab 2004;89:4409‐4413.
Page 33
8/14/2019 From Pain to Sleep: Listening to Patient-reported Outcomes
http://slidepdf.com/reader/full/from-pain-to-sleep-listening-to-patient-reported-outcomes 33/33
References
Kurzrock R. The role of cytokines in cancer‐related fatigue. Cancer 2001;92:1684‐1688.
Fayad L, Cabanillas F, Talpaz M, McLaughlin P, Kurzrock R. High serum interleukin‐6 levels correlate with a shorter failure‐free
survival in indolent lymphoma. Leuk.Lymphoma 1998;30:563‐571.
Rich T, Innominato PF, Boerner J et al. Elevated serum cytokines correlated with altered behavior, serum cortisol rhythm, and
dampened 24‐hour rest‐activity patterns in patients with metastatic colorectal cancer. Clin.Cancer Res. 2005;11:1757‐1764.
Belluco C, Olivieri F, Bonafe M et al. ‐174 G>C polymorphism of interleukin 6 gene promoter affects interleukin 6 serum level in
patients with colorectal cancer. Clin.Cancer Res. 2003;9:2173‐2176.
Vgontzas AN, Bixler EO, Lin HM et al. IL‐6 and its circadian secretion in humans. Neuroimmunomodulation. 2005;12:131‐140.
Vgontzas AN, Zoumakis E, Bixler EO et al. Adverse effects of modest sleep restriction on sleepiness, performance, and
inflammatory cytokines. J.Clin.Endocrinol.Metab 2004;89:2119‐2126.
Hong S, Mills PJ, Loredo JS, Adler KA, Dimsdale JE. The association between interleukin‐6, sleep, and demographic characteristics.
Brain Behav.Immun. 2005;19:165‐172.
Vgontzas AN, Zoumakis E, Lin HM et al. Marked decrease in sleepiness in patients with sleep apnea by etanercept, a tumor
necrosis factor‐alpha antagonist. J.Clin.Endocrinol.Metab 2004;89:4409‐4413.
Schiller JH, Storer BE, Witt PL et al. Biological and clinical effects of intravenous tumor necrosis factor‐alpha administered three
times weekly. Cancer Res. 1991;51:1651‐1658.