From Regulatory Compliance to Competence in Clinical Research The Joint Task Force for Clinical Research Competency Initiative Stephen A. Sonstein, PhD Director, Clinical Research Administration Eastern Michigan University Presented to: 11/17/2015 1
Transcript
From Regulatory Compliance to Competence in Clinical Research
The Joint Task Force for Clinical Research Competency Initiative
Stephen A. Sonstein, PhD
Director, Clinical Research Administration
Eastern Michigan University
Presented to:
11/17/2015
1
Expected Learning Outcomes
• Recognize the evolution of clinical research as an academic discipline
• Recognize the growing relevance of competency based education and training in career development
• Describe the outcomes of the Joint Task Force (JTF) initiative to define the Core Competencies in Clinical Research
• Describe the preliminary lessons learned from an international initiative to validate the JTF Core Competencies
2
Drug and device development is one of the most highly regulated activities globally
–Governmental regulatory authorities
•FDA
•OHRP
–ICH – GCPs
–IRB/IEC
–Pharmacovigilance
–Comparative efficacy vs cost
Personnel who conduct clinical trials
– Very general requirements
– In most countries, anyone with a medical license can conduct clinical trials….irrespective of their experience or education in clinical research
– Little detail in regulatory authority definitions of criteria required for responsible individuals
• ICH 4.1.1 The investigator(s) should be qualified by education, training, and experience to assume responsibility for the proper conduct of the trial, should meet all the qualifications specified by the applicable regulatory requirement(s), and should provide evidence of such qualifications through up-to-date curriculum vitae and/or other relevant documentation requested by the sponsor, the IRB/IEC, and/or the regulatory authority(ies)
Personnel who conduct clinical trials
– Declaration of Helsinki
• Previous – 3. Biomedical research involving human subjects should be conducted only by scientifically qualified persons and under the supervision of a clinically competent medical person. The responsibility for the human subject must always rest with a medically qualified person and never rest on the subject of the research, even though the subject has given his or her consent.
• Revised – (2014) 12. Medical research involving human subjects must be conducted only by individuals with the appropriate ethics and scientific education, training and qualifications. Research on patients or healthy volunteers requires the supervision of a competent and appropriately qualified physician or other health care professional.
The Harsh Reality of Clinical Research Sites Today
• 70% of clinical research sites never do more than one clinical trial
in the business lifetime
• Fewer than half of sites meet enrollment goals and 10% never
enroll a single subject
• Few sites have professionally trained and certified research
personnel
• Many sites are still using paper records without EDC/CTMS
• Monitoring accounts for nearly one-third of clinical trial budgets
• Redundancy, delays, non-compliance, and poor quality are the
norm rather than the exception
6
Clinical Investigator Deficiencies.
CDER Inspections 2004-2011
Enhancing the quality of clinical trials
Deficiencies and Opportunities
Khin NA et al. Clin Pharmacol Therap,2013; 94,2:230 Education and Training
7
• Improved trial design principles
• Defined personnel roles and responsibilities
• Improved policies and procedures
• Improved study start-up
• Quality assurance and auditing
• Document management
• Improved adverse event reporting
• Record retentionPerspect Clin Res.
2011 Oct-Dec; 2(4):
124–128.
What are we expecting when we hire a clinical research
professional?
• Principal investigator – Any licensed physician anywhere in the
world can serve as Principal Investigator
• CRC – there are no educational requirements
• CRA – there are no educational requirements
• Regulatory Affairs Professional – there are no educational
requirements
How do we differentiate between an entry level
and an advanced level professional?
What criteria do we use to justify promotion?
8
Activity
• Informal training: coaching, tutoring• Short term courses: how to do it!
• Professional bodies (training, support)
Discipline
• Academic involvement: Standards and competencies• Formal Curriculum: short and long term programs• National accreditation and certification
Profession
• International Standards/Harmonization of Training/mutual recognition
• International Certification/Specialization• Maintenance through CPD
Evolution of Education and Training in
Clinical Research
Honorio Silva MD, 2010
9
How to do it?
• Systematic harmonization and broad based acceptance
of job descriptions and performance outcomes for the
many roles that exist in the clinical research enterprise
• Standardization and Documentation of
education/ training and experience in clinical research
• Required personnel certification
• Accreditation of the sites which conduct clinical trials
Moving the clinical research enterprise from a focus on
regulatory compliance to professional competence
10
Traditional Vs Outcomes Based education
TRADITIONAL EDUCATION OUTCOMES BASED
EDUCATION
Based upon knowledge Based upon competencies
Time fixed; Time is variable
Learners grouped in classes and
move together
Learners advance in various
ways to achieve outcomes
Teachers are responsible for a
course
Teachers are responsible for a
set of outcomes
Learners accumulate courses
and grades lead ing to a
credential
Learners demonstrate
achievement of outcomes at
their own pace
Defined competencies are
important
Defined competencies are a
paradigm 11
Competency vs. Competence
Competencies encompass knowledge, skills, attitudes, and behaviors
necessary for a particular set of tasks or objectives in a specific
job/function
• Are usually organized in clusters (domains)
• Can be measured (assessed)
• Can be improved
A competent professional is one possessing the required abilities in all
domains in a certain context at a defined stage of education or practice.
(Frank J. Medical Teacher, 2010)
12
Use of competencies
• Competency profiles
• Competency-based education and training
• Job profiles – linked – personnel profiles
• Level of competency vs level of job
• Self-assessment & competence
• Competence & career development
• Gap analysis
• Training to fill gaps
• Continuous process (competence not static, jobs change,
gaps appear); lifelong learning
13
Competence: Self-Assessment
What learning opportunities can help
me?
How can I consolidate
the learning & become
competent?
What competencies
do I need for my work & what are
the gaps?
14
The Joint Task Force for Clinical Trial
Competency
• Organized under the sponsorship of MRCT and ACRES at Harvard University.
• Supported by MAGI, DIA and ACRP
• Included representatives from industry, academy and nonprofit organizations
• Agreed to work toward aligning and harmonizing the many more focused statements relating to core competencies for clinical research professionals into a single, high-level set of standards which could be adopted globally and serve as a framework for defining professional competence throughout the clinical research enterprise
15
16
Joint Task Force for Clinical Trial Competency
Contributors and Collaborators
Representatives met in person or via TC during the
period October 2013-June 2015
JTF Coordinators: S. Sonstein and R. Li
Outcomes of the JTF on Core Competencies in Clinical
Research
• 51 specific competencies within the 8 domains derived from the published and presented efforts of specific related groups
• Based upon cognitive parameters
• Not expected that each member of the clinical research enterprise is competent in all
• Still need to be leveled as Expert, Competent, Novice
• Hope is that Harmonized Core Competencies will be u tilized as a basic framework for job descriptions and job portfolios
Sonstein, S.A., Seltzer, J., Li, R., Jones, C.T., Silva, H., Daemen, E. (2014, June). Moving from compliance to competency: A harmonized core competency framework for the clinical research professional. Clinical Researcher. 28(3)17-23.
17
Harmonized Core Competency Domains for the Clinical
Research Professional
18
A cooperative multi-institutional effort
19
The JTF International Validation of
Core Competencies and Educational
Needs Assessment
Initiative in final stages
•Globally distributed questionnaire including demographics, domains and competencies.
• Respondents were asked to share their own perception of competence, role relevance and needs for training utilizing the JTF Core Competency Domains and statements
• Data to be used for:
• Needs assessment for training
• Standard ization of position descriptions
• Integration into personnel and site certification efforts
• Validation and identification of key competencies
• Standardization of curricula for academic programs
- complete statistical analysis currently ongoing….
20
Demographics by region and function
21
ONLY 366 CERTIFIED
Role #
Clinical Research
Coordinator/Research Nurse
338
Research Administrator/Project
Manager
229
Principal Investigator/Co-
investigator
228
Clinical Research
Associate/Monitor
129
Regulatory Affairs Professional 52
Educator/Trainer 50
Pharmaceutical Physician/Medical
Director
42
Data Management Professional 38
Others 107
Total 1213
Latin America41%
US/CAN35%
Europe20%
Scale of Self-Assessed Responses to Perception of
Competence and job relevance
Competency Key:
• 0 Never been exposed to this content
• 1= Aware of the content, but never needed to become further informed;
• 2= Exposed and sufficiently aware of content that I can look up what might be necessary for my
job;
• 3= Competent–Able to interpret or discuss concepts and use knowledge to solve simple
problems based on application concepts;
• 4 = Mastery–able to apply knowledge to complex problems, integrate information and create
solutions
Relevance Key:
•0 = unnecessary, no relevance to my role;
• 1 = has some relevance to my role, but not my responsibility;
• 2 = relevant to my role, but not a major component;
• 3 = significant to my role and part of my job responsibilities;
• 4 = major part of my responsibility or supervisory expectations
22
Criteria for Competency Relevance to Role
• Percentage of responses rated 3 or 4
• 1 – High Relevance - >80%
• 2- Significant Relevance – 60-79%
• 3- Intermediate Relevance– 40-59%
• 4- Low Relevance– 20-39%
• 5- No relevance - <20%
• Applied to both domains and specific competencies.
23
24
Self-assessment of Competence, Relevance and Training Needs - Overall
N=1213
Domain Self Assessment of Competence (%)
Relevance to the job (%)
Additional Training Needs (%)
Scientific Concepts
& research design
42 36 51
Ethics & Safety 67 61 43
Medicines Dev. &
regulations
46 40 50
Clin. Trials Ops 68 63 45
Study & Site Mgmt 57 57 55
Data Mgt & inform 59 55 47
Leadership &
professionalism
65 64 55
Communication &
Teamwork
62 57 50
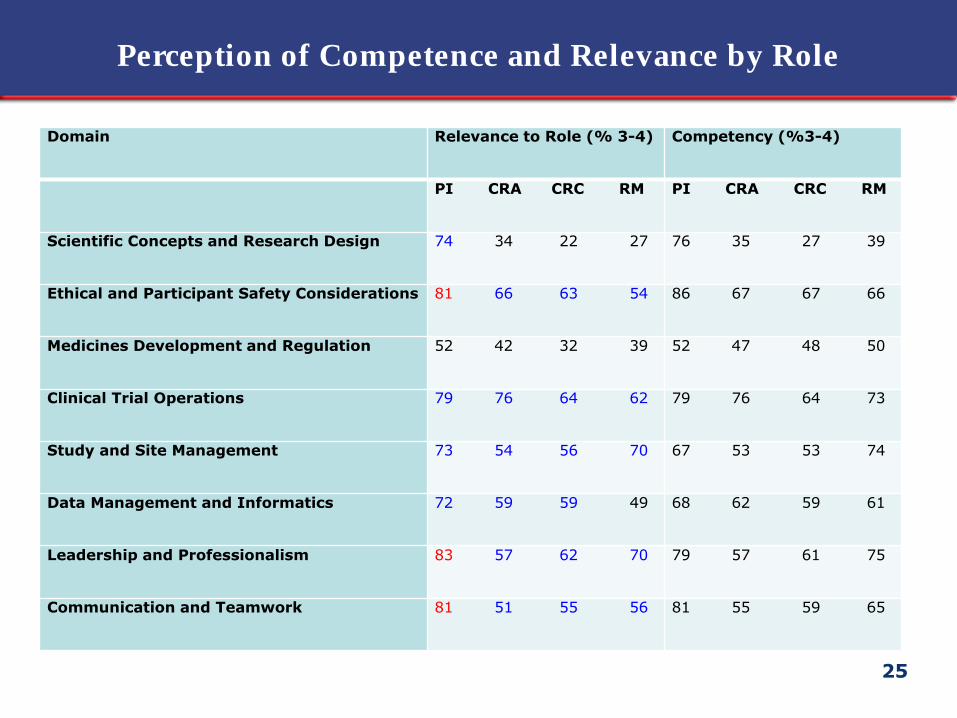
Perception of Competence and Relevance by Role
Domain Relevance to Role (% 3-4) Competency (%3-4)
PI CRA CRC RM PI CRA CRC RM
Scientific Concepts and Research Design 74 34 22 27 76 35 27 39
Communication and Teamwork 81 51 55 56 81 55 59 65
25
Perceived need for training by role
Domain Need for Training (%yes)
PI CRA CRC RM
Scientific Concepts and Research Design 61 57 48 44
Ethical and Participant Safety Considerations 51 52 48 44
Medicines Development and Regulation 58 58 50 38
Clinical Trial Operations 53 52 45 36
Study and Site Management 62 57 56 48
Data Management and Informatics 60 53 45 36
Leadership and Professionalism 62 62 55 52
Communication and Teamwork 57 57 48 45
26
27
Competency (% 3-4) Relevance (%3-4)
Years of Experience 2-5 6-10 10-19 20+ 2-5 6-10 10-19 20+
Ethical and Participant Safety Considerations
Compare and contrast clinical care and clinical management of research participants (317)
52 63 75 74 44 62 71 68
Define the concepts of “clinical equipoise” and “therapeutic misconception” as they relate to the conduct of a clinical trial (315)
25 39 43 57 21 40 39 55
Compare the requirements for human subject protection and privacy under different national and international regulations and ensures their implementation throughout all phases of a clinical study (315)
56 71 75 74 56 69 77 82
Explain the evolution of the requirement for informed consent from research participants and the principles and content of the key documents which ensure the protection of human participants in clinical research (313)
85 90 93 96 81 85 92 91
Describe the ethical issues involved when dealing with vulnerable populations and the need for additional safeguards (314)
81 88 87 100 74 80 85 86
Evaluate and apply an understanding of the past and current ethical issues, cultural variation and commercial aspects on the medicines development process (313)
39 59 64 82 36 46 59 68
Explain how inclusion and exclusion criteria are included in a clinical protocol to assure human subject protection (313)
84 85 90 95 80 78 83 100
Summarize the principles and methods of distributing balancing risk and benefit through selection and management of clinical trial subjects (313)
59 75 77 89 53 70 73 81
Specific Competency and Relevance to CRC’s by years
of experience
CRC - Perceived competence, relevance and
training need by location
28
Domain Location N Competence Relevance Training
% 3+4 % 3+4 % yes
Scientific Concepts and Research Design US/Can 123 31 27 43
LA 36 36 37 75
WE 122 20 16 45
AA 12 28 20 43
Ethical and Participant Safety Considerations US/Can 117 70 64 35
LA 36 59 62 64
WE 120 65 64 40
AA 12 56 59 33
Medicines Development and Regulations US/Can 114 41 41 41
LA 36 35 40 67
WE 118 36 34 53
AA 12 18 12 58
Clinical Trial Operations US/Can 114 68 64 40
LA 36 64 67 72
WE 117 63 63 42
AA 12 46 59 47
Study and Site Management US/Can 113 57 58 54
LA 36 50 59 75
WE 117 63 63 42
AA 12 43 43 51
Data Management and Informatics US/Can 115 64 60 41
LA 36 51 62 72
WE 114 55 57 41
AA 12 58 58 48
Leadership and Professionalism US/Can 116 62 63 49
LA 36 55 66 81
WE 114 61 66 53
AA 12 56 58 54
Communication and Teamwork US/Can 115 59 62 43
LA 36 55 63 68
WE 114 59 57 46
AA 12 64 56 44
29
Conclusions
1. Performance deficiencies in the clinical trial process are not only
costly, but contribute to delay and risk in the medicines
development process
2. Competency rather than compliance is the currency by which we
should be measuring the conduct of clinical research and medicines
development
3. Competency based education is emerging as a paradigm for
education and training in health professions
4. The JTF has developed a Harmonized Framework of Core
Competencies for the Clinical Research Professional and a global
survey aimed at validation, perception of competence, relevance to
the job and educational needs was recently completed . Final results
are expected soon.
5. Preliminary data show differences in the perception of competence,
relevance and need for training for the various functions and
competency domains. The significance of such d ifferences is to be
determined.
• Finalize analysis of collected data, and continue with
internal/ external d iscussions with stakeholders
• Ongoing validation and collaboration with the NIH CTSA
network
• Further regional/ country validation
• Formalize the ACRP role as “Custodian”
• Adoption of key competencies for accreditation of academic
programs
• Create global awareness for further adoption and adaptation