29
F. Schlachetzki Klinik für Neurologie, Universität Regensburg und Bezirksklinikum Regensburg, [email protected] Jubiläumssymposium Berlin, 8.November, 2014 30 Jahre Notarzt Berlin e.V.

F. Schlachetzki Klinik für Neurologie, Universität Regensburg und Bezirksklinikum Regensburg,
Jubiläumssymposium Berlin, 8.November, 2014 30 Jahre Notarzt Berlin e.V.

das sollte vermieden werden
Stroke unit/ CT
Prähospital Schlaganfallversorgung ...
Ziele von Prähospitalprojekten: • Gezielter Transport in ein Schlaganfallzentrum
• Verkürzung innerhospitaler Abläufe (DTN !) • ? Unterstützung nicht-‐ärztlichen ReJungspersonals? • ? Prähospitale Schlaganfalltherapie ?
Sonothrombolyse – Rekanalisation durch Ultraschall
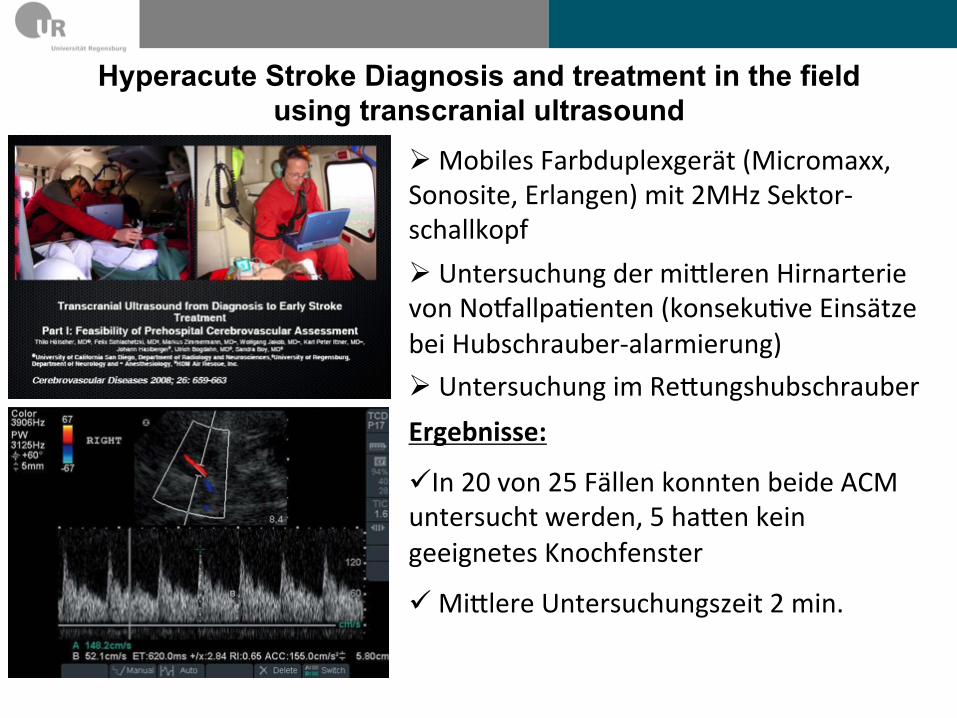
Hyperacute Stroke Diagnosis and treatment in the field using transcranial ultrasound
Ø Mobiles Farbduplexgerät (Micromaxx, Sonosite, Erlangen) mit 2MHz Sektor-‐schallkopf Ø Untersuchung der miNleren Hirnarterie von NoOallpaPenten (konsekuPve Einsätze bei Hubschrauber-‐alarmierung) Ø Untersuchung im ReNungshubschrauber Ergebnisse:
ü In 20 von 25 Fällen konnten beide ACM untersucht werden, 5 haNen kein geeignetes Knochfenster
ü MiNlere Untersuchungszeit 2 min.
Christoph Regensburg
Einsatzauswertung Medat 2012 Version 01 vom 22. April 2012 Seite 69 von 94
Christoph Regensburg
Einsatzauswertung Medat 2012 Version 01 vom 22. April 2012 Seite 63 von 94
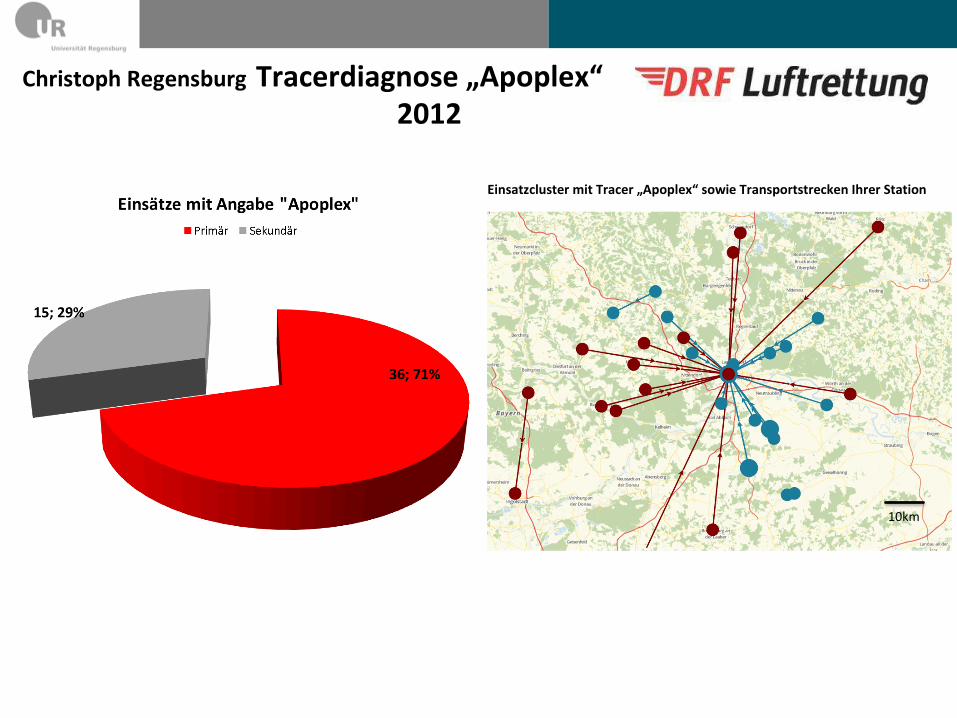
Einsatzcluster mit Tracer „Apoplex“ sowie Transportstrecken Ihrer Station
10km
Christoph Regensburg
Einsatzauswertung Medat 2012 Version 01 vom 22. April 2012 Seite 62 von 94
5 „Apoplex“ Tracerdiagnose – betrachtet werden nur Primäreinsätze; alle NACA.
Christoph Regensburg
Einsatzauswertung Medat 2012 Version 01 vom 22. April 2012 Seite 62 von 94
5 „Apoplex“ Tracerdiagnose – betrachtet werden nur Primäreinsätze; alle NACA.
Tracerdiagnose „Apoplex“ 2012

Regensburger Schlaganfallmobil - praktischer Ablauf
112
Untersuchung auf dem Weg zur STROKE UNIT

Einsatzgebiet des Schlaganfallmobils (Regensburg Stadt und Landkreis)
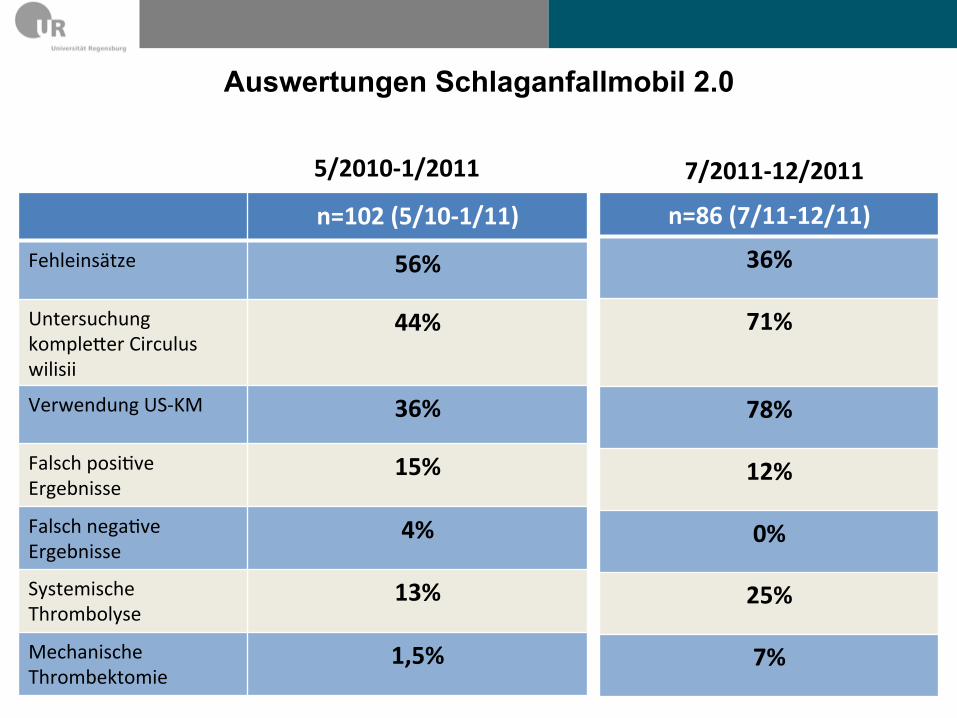
Auswertungen Schlaganfallmobil 2.0
n=102 (5/10-‐1/11)
Fehleinsätze 56%
Untersuchung kompleNer Circulus wilisii
44%
Verwendung US-‐KM 36%
Falsch posiPve Ergebnisse
15%
Falsch negaPve Ergebnisse
4%
Systemische Thrombolyse
13%
Mechanische Thrombektomie
1,5%
n=86 (7/11-‐12/11)
36%
71%
78%
12%
0%
25%
7%
5/2010-‐1/2011 7/2011-‐12/2011
Ø Was ist der legale Hintergrund? Ø Gibt es Daten bzgl. prähospitaler Ultraschall-gestützte
Schlaganfalltherapie? Ø Was sind die Vorrausetzungen für prähospitale Thrombolyse
gestützt durch diagnostischen Ultraschall?
Ø Was ist der Gold-Standard in der Prähospitaldiagnostik?
Ø Ist es die Mühe und das Risiko wert?
5 Fragen zu prähospitaler Ultraschalldiagnos?k/ Therapie
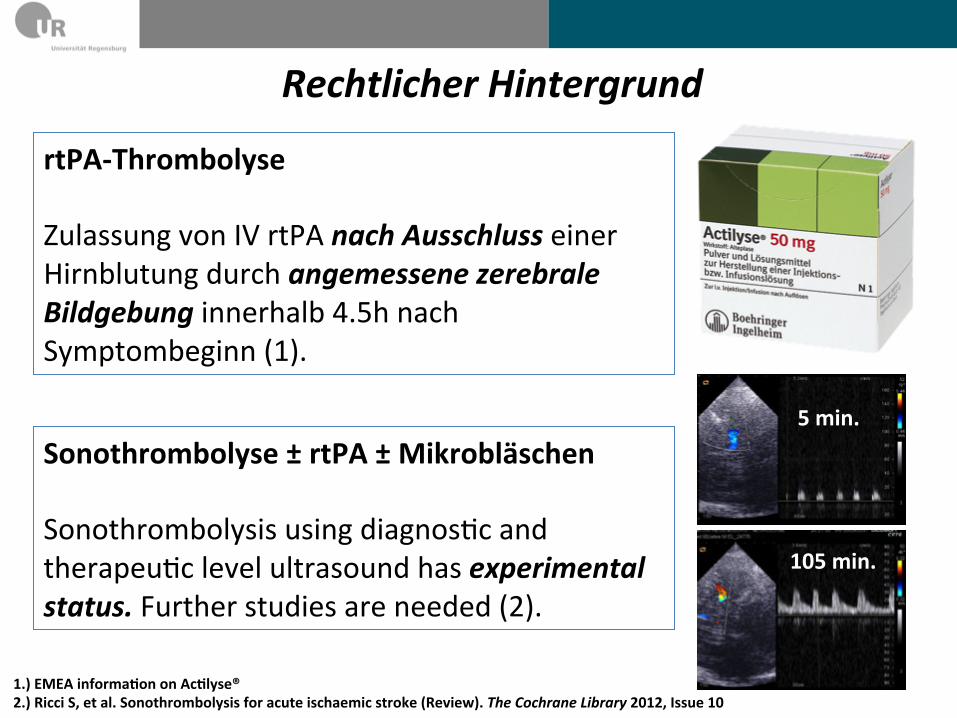
Rechtlicher Hintergrund rtPA-‐Thrombolyse Zulassung von IV rtPA nach Ausschluss einer Hirnblutung durch angemessene zerebrale Bildgebung innerhalb 4.5h nach Symptombeginn (1).
Sonothrombolyse ± rtPA ± Mikrobläschen Sonothrombolysis using diagnosPc and therapeuPc level ultrasound has experimental status. Further studies are needed (2).
5 min.
105 min.
1.) EMEA informaeon on Acelyse® 2.) Ricci S, et al. Sonothrombolysis for acute ischaemic stroke (Review). The Cochrane Library 2012, Issue 10

Bisherige Daten
Keine Studies über rtPA-‐Thrombolyse/ Sonothrombolyse ± rtPA ± Mikrobläschen (Stand Oktober 2014)
Fallbeispiel Gabe von Aspirin beim akuten Schlaganfall nach transkranieller Duplexsonographie (Finale Diagnose: kleiner embolischer thalamic ischaemia) Wilson MH, et al. Stroke at high alPtude diagnosed in the field using portable ultrasound. Wilderness Environ Med. 2011 Mar;22(1):54-‐7
5 min.
105 min.

Voraussetzungen für US-‐assis?erte Stroke-‐Therapie -‐ 1
Klinische Schlaganfalldiagnose mit hoher Sensievität / Spezifität (59 – 92% / 74 – 92%)
Sensievität Spezifität Klinische Parameter FAST 89 % n.n. Lähmung Gesicht u. Arm, Sprachstörung
LAPPS 59 % -‐ 68 % 85 % Lähmung Gesicht u. Arm, Händedruck, Ausschluss DD (Alter <45; bek. Epilepsie, PaPent kann nicht gehen, BZ <60 u. >400mg/dL)
CPSS 66 % -‐ 88 % 87 % -‐ 95 % Lähmung Gesicht u. Arm, Satz nachsprechen
3I-‐SS 67 % 92 % Grad des Bewusstseins, Kopf-‐ und Blickwendung, graduierte Hemiparese
ROSIER 92 % 86 % Asymmetrie im Gesicht, Arm, Bein, Sprachstörung, Gesichtsfeldausfall, Ausschluss Synkope/ Bewusstseinsverlust und Epilepsie
MASS 90 % 74 % Lähmung Gesicht u. Arm, Satz nachsprechen, Händedruck, BZ

Klinische Schlaganfalldiagnose mit hoher Sensievität / Spezifität (59 – 92% / 74 – 92%)
1.) Schlachetzki F, et al. 'Transcranial Ultrasound from Diagnosis to Early Stroke Treatment. Part II: Prehospital neurosonography in paeents with acute stroke – the Regensburg Stroke Mobile Project.' Cerebrovasc Dis 2012; 33(3): 262-‐271 2.) Herzberg M, et al. 'Prehospital stroke diagnosecs based on neurological examinaeon and transcranial ultrasound.' Cri?cal Ultrasound Journal 2014; 6: 3. Doi: 10.1186/2036-‐7902-‐6-‐3
264 classified as stroke mimics. In the field, 4 patients were265 given the misdiagnosis of a non-stroke event (4%), whereas266 15 patients (15%) received the misdiagnosis of stroke267 when their symptoms merely mimicked those of a268 stroke. In summary, the initial working diagnosis prior269 to patient admission to the hospital showed a sensitivity270 of 95% (95% CI 86 to 98) and a specificity of 48% (29 to 67)271 in the hospital workup (TablesT2 2,T3 3, andT4 4). Two examples272 of stroke mimics with interesting neurosonographic find-273 ings (normal flow but indications for subdural hematoma274 or midline shift) were found in a patient with a subdural275 hematoma (FigureF2 2) and a brain tumor (FigureF3 3). In 68%276 of the patients, stroke-like symptoms were caused by ische-277 mic stroke/TIA with suspected etiology of large artery ath-278 erosclerosis in 50% followed by cardioembolism and small279 vessel disease (TableT5 5). Only 5% of symptoms were caused280 by any intracranial hemorrhage. During the study period, 9281 of 50 patients (18%) received IV thrombolysis and 1 patient282 underwent mechanical thrombectomy.
283 Transcranial color-coded duplex sonography in the field284 Ultrasound contrast agents were administered in 41 pa-285 tients (40%), and no adverse event was noted. Despite286 the use of UCA, inferior temporal bone windows were287 found in 11 of the 102 patients (11%) (in 5 patients bilat-288 erally, in 6 patients unilaterally), and these were excluded289 from further analysis testing sensitivity and specificity of290 prehospital TCCS. An additional patient was excluded291 who presented with MCA occlusion with related hemipar-292 esis and spontaneous thrombolysis during transport. One293 patient with a non-stroke diagnosis (temporal arteritis)
294and three patients with unremarkable neuroimaging find-295ings yet stroke diagnosis at discharge were also excluded.296The flow diagram (Figure F44) shows the diagnostic path-297way and the neurovascular imaging reference methods298obtained as ‘gold standard in hospital’. In 4% of patients,299diagnosis of stroke was first detected by non-contrast300CT (cerebral computed tomography (CCT)). In 7% of301patients, CTA imaging first led to the final diagnosis.302Preclinical TCCS demonstrated 12 occlusions or high-303grade stenoses of major brain-supplying arteries (MCA and304ICA) including 10 M1-MCA occlusions. Internal carotid305artery (ICA) occlusions were diagnosed when reversed flow306(‘cross-filling’) occurred in the ipsilateral ACA; this finding307is indicative of >80% stenosis or total occlusion of the ICA308according to the ECST criteria [24]. Standard imaging309studies (CTA, MRA, and CCT) showed 14 major cerebral310artery occlusions: 10 involving the MCA and 4 involving311the ICA (Table T66). In the early days of the study, a PCA312was mistaken to be a patent MCA in one patient when the313UCA was incorrectly injected through a filter system,314resulting in the destruction of microbubbles and inferior315image quality. Also, TCCS resulted in the misdiagnosis of316distal MCA occlusion in one patient, according to the317Zanette index [22]. In this patient, an atypical parieto-318occipital intracerebral hemorrhage (ICH) caused disloca-319tion of the MCA, which led to a near-perpendicular angle320of insonation. In retrospect, considering the lack of resist-321ance in the low-flow profile and use of the UCA may have322helped avoid the misdiagnosis (an example of a correct323diagnosis of distal MCA occlusion is shown in Figure F55).324Two >80% stenoses or total occlusions of the ICA were325not detected; in those cases, the examiner investigated326both MCA arteries according to the study protocol but327did not examine the ACA and, therefore, missed a cross-328filling phenomenon (Figure F66). In summary, we found a329sensitivity of 90% and specificity of 98% (positive predict-330ive value 90%, negative predictive value 98%) in achieving331a correct diagnosis of MCA occlusion.
t2:1 Table 2 Initial working diagnostict2:2 Stroke (n = 102) Stroke mimics
t2:3 Proved right (n = 69) n = 3 exsiccosis
t2:4 n = 2 hypoglycemia
t2:5 n = 2 syncope
t2:6 n = 1 pneumonia
t2:7 n = 1 migraine
t2:8 n = 1 slipping
t2:9 n = 1 persisting atrial fibrillation
t2:10 n = 1 functional brachiofacial hemiparesis
t2:11 n = 1 hypertensive rise
t2:12 n = 1 epileptic seizure
t2:13 Proved wrong (n = 4) n = 5 epileptic seizure
t2:14 n = 4 tumor
t2:15 n = 2 subdural hematoma
t2:16 n = 1 exsiccosis
t2:17 n = 1 MI + brain concussion
t2:18 n = 1 metabolic encephalopathy
t2:19 n = 1 peripheral nerve compression (C7)t2:20
t3:1Table 3 Preclinical working and discharge diagnosticst3:2Discharge diagnostic
t3:3Stroke Stroke mimic Total
t3:4Preclinical workingt3:5diagnostic
Stroke 69 15 84
t3:6Stroke mimic 4 14 18
t3:7Total 73 29 102
t4:1Table 4 Sensitivity, specificity, positive predictive value,t4:2and negative predictive valuet4:3SE
(95% CI)Sp
(95% CI)PPW
(95% CI)NPW
(95% CI)
t4:4Stroke vs. mimic 94%(86 to 98)
48%(29 to 67)
82%(72 to 89)
77%(52 to 93)
t4:5SE, sensitivity; Sp, specificity; PPW, positive predictive value; NPW, negativet4:6predictive value.
Herzberg et al. Critical Ultrasound Journal 2014, 6:3 Page 5 of 13http://www.criticalultrasoundjournal.com/content/6/1/3
Transkranielle Farbduplexsonographie mit Sensievität / Spezifität (78 – 94% / 48 -‐ 98%) für Verschlüsse im vorderen Kreislauf:
Voraussetzungen für US-‐assis?erte Stroke-‐Therapie -‐ 2

Foerch C, et al. ‘Diagnosec accuracy for glial fibrillary acidic protein for differeneon of brain hemorrhage and cerebral ischemia in paeents with symptoms of acute stroke .’ Clinical chemistry 2012; 51: 237-‐245
Blut Serum Test zur Idenefikaeon intrazerebraler Blutungen mit hoher Sensievität /Spezifität: Cut off 0,28μg/ml: 84,2% / 96,3% Cut off 1,0μg/ml 60,5% / 100%
ischemic stroke, including stroke mimic [AUC 0.915(95% CI 0.847– 0.982), P ! 0.001]. Diagnostic accu-racy remained stable when we analyzd only those pa-tients who were admitted very early (i.e., !60 min, n "52, AUC 0.904) (Fig. 2B). Diagnostic accuracy wasslightly lower in patients with a less severe clinical def-icit (i.e., NIHSS score !14, n " 104, AUC 0.873) (Fig.2C) compared with those patients having a more severefunctional deficit (i.e., NIHSS score above the medianscore of 14, n " 97, AUC 0.944) (Fig. 2D).
When we applied the predefined cutoff of 0.29"g/L for discriminatory analysis, the diagnostic sensi-
tivity and specificity of plasma GFAP for the differen-tiation between ischemic stroke and ICH were 84.2%and 96.3%, respectively (positive and negative predic-tive value 84.2% and 96.3%, respectively). The diag-nostic specificity of the GFAP test increased to 98.8%when 0.5 "g/L was selected as the cutoff (diagnosticsensitivity 73.7%), and to 100% when 1.0 "g/L wasselected as the cutoff (diagnostic sensitivity 60.5%). Apost hoc analysis revealed that the optimal cutoff of0.28 "g/L for differentiating ICH from ischemic strokein our dataset was nearly identical with our predefinedcutoff.
In ICH patients, the median hematoma volume,calculated on the basis of first available brain imaging,was 39.8 mL (interquartile range 6.1–97.7 mL, mini-mum 2.4 mL, maximum 179.0 mL). Hematoma vol-ume was positively correlated with plasma GFAP val-ues (P " 0.046). The 2 ICH patients with the lowesthematoma volumes (2.4 and 2.7 mL) did not show anincrease in GFAP. However, all 5 ICH patients withhematoma volumes between 3 and 10 mL did showpositive GFAP signals (median 1.3 "g/L). A significantcorrelation was found between NIHSS values andGFAP plasma concentrations in ICH patients (P "0.022), whereas no relationship between these 2 pa-rameters was found in ischemic stroke patients (P "0.472) (Fig. 3A and 3B).
Based on the entire dataset including patients withICH, ischemic stroke, and stroke mimic, a binary logis-tic regression analysis did not reveal age, arterial hyper-tension, or diabetes mellitus to independently influ-ence GFAP plasma concentrations (Table 2).
Discussion
Our study was based on a plausible pathophysiologicalconcept. GFAP, a highly brain-specific astroglial pro-tein, is detectable in very low concentrations in the
Table 1. Baseline characteristics of the study population.
Ischemicstroke ICH
Strokemimic Alla
n (%) 163 (79.5) 39 (19.0) 3 (1.5) 205 (100.0)
Mean age, years (SD) 75.3 (13.4) 70.7 (17.4) 44.3 (23.5) 73.9 (14.8)
Men, n (%) 79 (48.5) 21 (55.3) 2 (66.7) 102 (50.0)
Patients with hypertension, n (%) 121 (74.2) 22 (57.9) 0 (0.0) 143 (70.1)
Patients with diabetes, n (%) 35 (21.5) 4 (10.5) 1 (33.3) 40 (19.6)
Median NIHSS, (interquartile range) 12 (8–18) 16 (13–20) 5 14 (8–18)
Mean time from symptom onset to hospitaladmission, min (SD)
122.7 (65.2) 134.0 (63.7) 140.0 (45.8) 125.0 (64.4)
a Because of a few missing values, sums do not always equal 100%.
Fig. 1. Box plots illustrating the distribution of GFAPplasma concentrations in patients with ischemicstroke, ICH, and stroke mimics.The boundaries of the box indicate the 25th and 75thpercentile, and the line within the box marks the median.Whiskers above and below the box indicate the 90th and10th percentiles. The y axis is log transformed.
240 Clinical Chemistry 58:1 (2012)
Voraussetzungen für US-‐assis?erte Stroke-‐Therapie -‐ 2 Klinische Schlaganfalldiagnose mit hoher Sensievität / Spezifität (59 – 92% / 74 – 92%)
Transkranielle Farbduplexsonographie mit Sensievität / Spezifität (78 – 94% / 48 -‐ 98%) für Verschlüsse im vorderen Kreislauf:
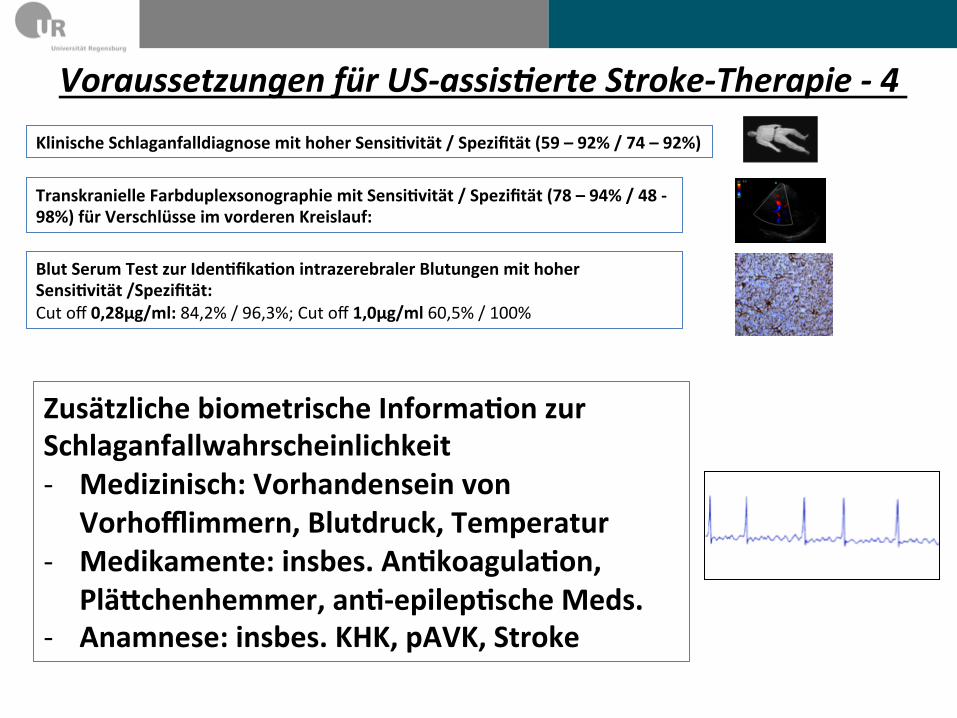
Zusätzliche biometrische Informaeon zur Schlaganfallwahrscheinlichkeit -‐ Medizinisch: Vorhandensein von
Vorhofflimmern, Blutdruck, Temperatur -‐ Medikamente: insbes. Anekoagulaeon,
PläJchenhemmer, ane-‐epilepesche Meds. -‐ Anamnese: insbes. KHK, pAVK, Stroke
Voraussetzungen für US-‐assis?erte Stroke-‐Therapie -‐ 4
Blut Serum Test zur Idenefikaeon intrazerebraler Blutungen mit hoher Sensievität /Spezifität: Cut off 0,28μg/ml: 84,2% / 96,3%; Cut off 1,0μg/ml 60,5% / 100%
Klinische Schlaganfalldiagnose mit hoher Sensievität / Spezifität (59 – 92% / 74 – 92%)
Transkranielle Farbduplexsonographie mit Sensievität / Spezifität (78 – 94% / 48 -‐ 98%) für Verschlüsse im vorderen Kreislauf:

Stroke Bayesian Network (SBN)
Stroke Bayes Network (SBN) – Schlaganfallwahrscheinlichkeit
S.Theiss, personal communicaPon
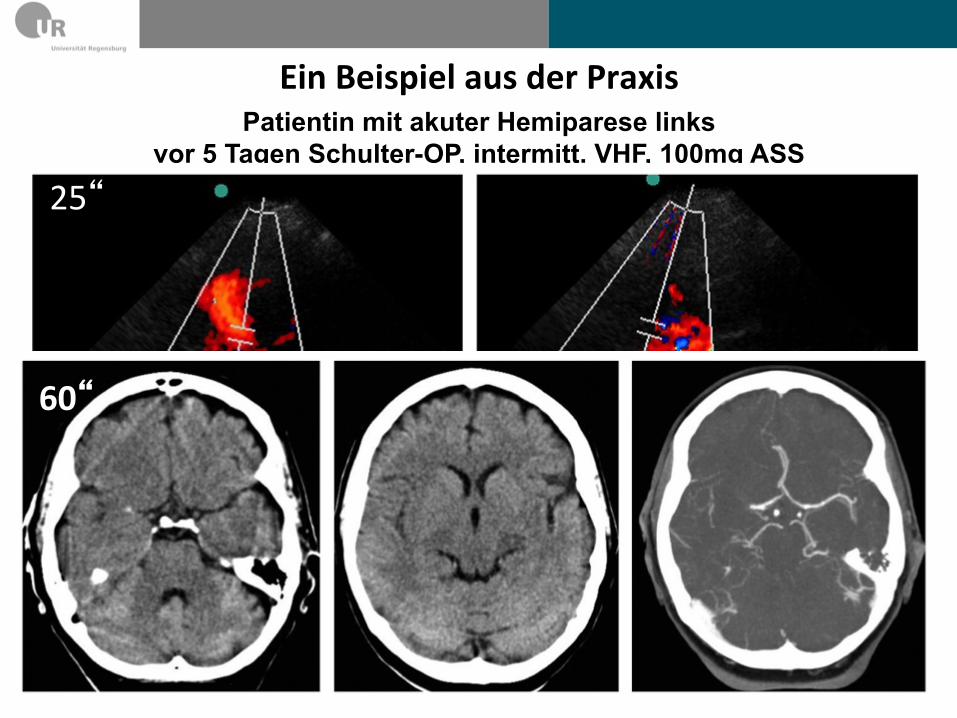
Patientin mit akuter Hemiparese links vor 5 Tagen Schulter-OP, intermitt. VHF, 100mg ASS
25“
60“
Ein Beispiel aus der Praxis
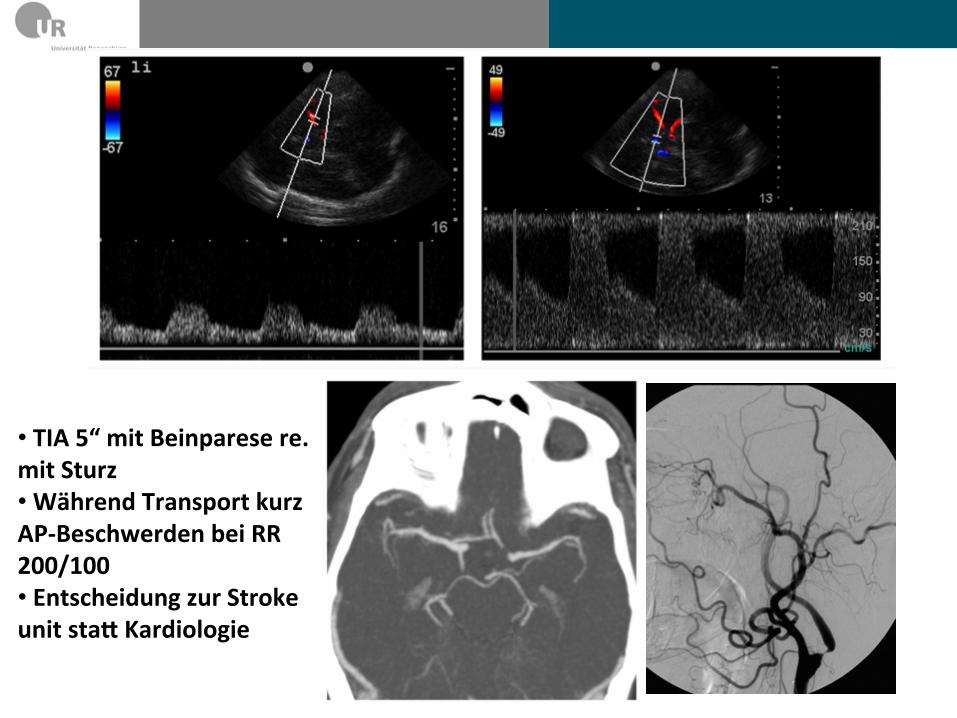
• TIA 5“ mit Beinparese re. mit Sturz • Während Transport kurz AP-‐Beschwerden bei RR 200/100 • Entscheidung zur Stroke unit staJ Kardiologie
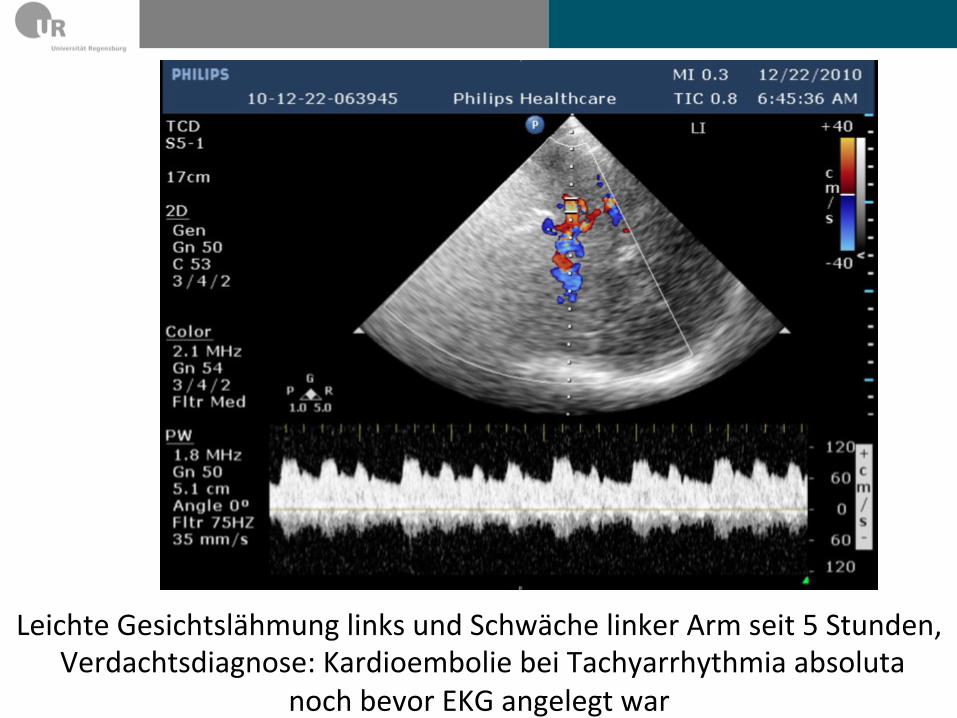
Leichte Gesichtslähmung links und Schwäche linker Arm seit 5 Stunden, Verdachtsdiagnose: Kardioembolie bei Tachyarrhythmia absoluta
noch bevor EKG angelegt war
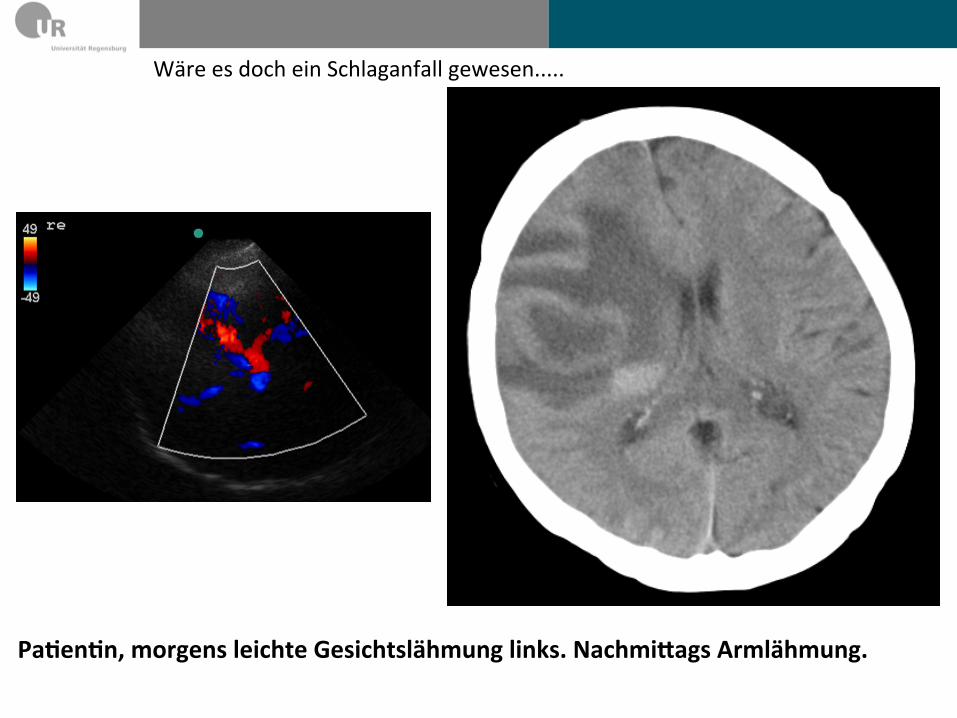
Wäre es doch ein Schlaganfall gewesen.....
Paeenen, morgens leichte Gesichtslähmung links. NachmiJags Armlähmung.
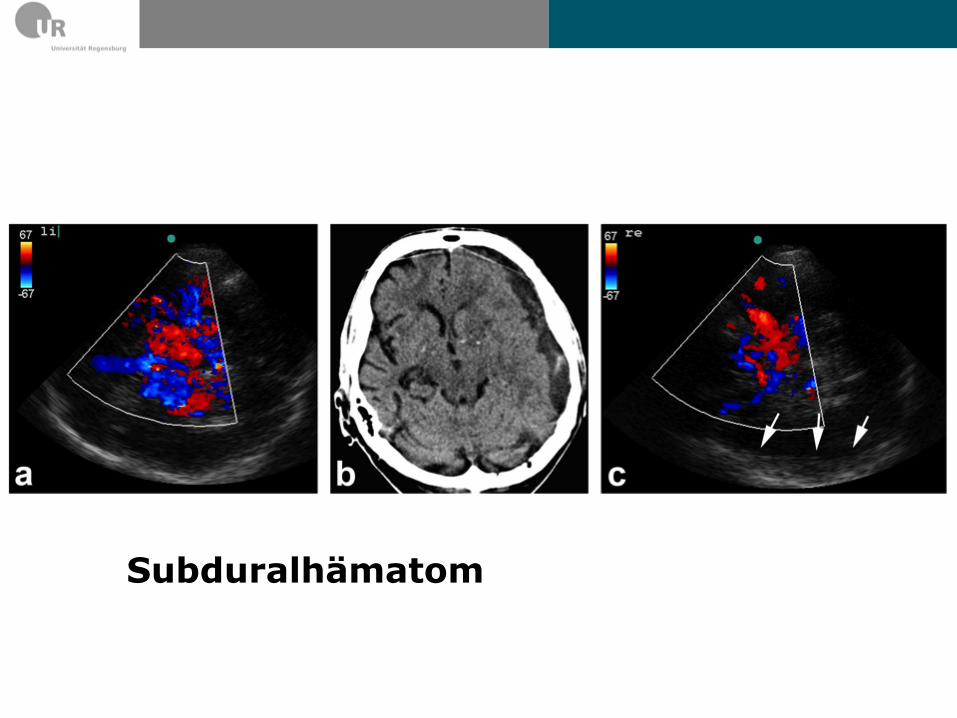
Subduralhämatom


Die Vision... Pat. mit akuter schwerer Halbseitensymptomatik
Neurosonographie-‐Diagnose: Mediaverschluss
GFAP-‐POC: Normal
Neurosonographie-‐Diagnose: Kein Verschluss
GFAP-‐POC: Pathologisch erhöht
-‐ Neurologie: cCT/ Thrombolysis -‐ ? Prähospitale Thrombolyse -‐ ? rtPA + Vorbereitung Embolektomie -‐ ? NeuroprotekPon
-‐ ? Aggressive Blutdrucksenkung -‐ ? NeuroprotekPon -‐ ? Neurochirurgie-‐Alarmierung
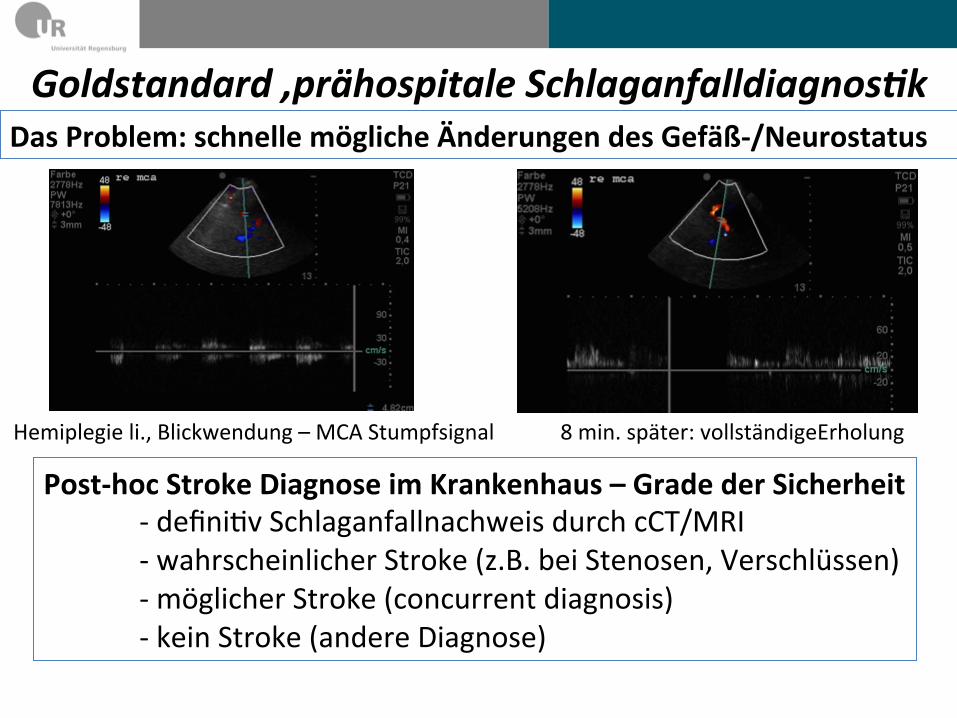
Goldstandard ‚prähospitale Schlaganfalldiagnos?k
Post-‐hoc Stroke Diagnose im Krankenhaus – Grade der Sicherheit -‐ definiPv Schlaganfallnachweis durch cCT/MRI -‐ wahrscheinlicher Stroke (z.B. bei Stenosen, Verschlüssen) -‐ möglicher Stroke (concurrent diagnosis) -‐ kein Stroke (andere Diagnose)
Hemiplegie li., Blickwendung – MCA Stumpfsignal 8 min. später: vollständigeErholung
Das Problem: schnelle mögliche Änderungen des Gefäß-‐/Neurostatus

newly designed ambulance, the so-called strokeemergency mobile unit (STEMO), which is de-ployed when patients suspected of having strokeare identified at the dispatch center with a spe-cialized stroke identification interview algo-rithm.16 We report the results of the pilotstudy of an ongoing project to show a relevantreduction in time from emergency call to treat-ment.17 This study was focused on feasibility andtechnical reliability but also assessed preliminarysafety and call-to-needle times in patients whoreceived tPA treatment in the prehospital setting.
METHODS Details of the PHANTOM-S study (NCT01382862)have been described previously.17 The pilot study of thePHANTOM-S was conducted in the emergency medical serv-ices system of the city of Berlin during the period from February8, 2011 to April 30, 2011.
Stroke emergency mobile unit. STEMO (see figure 1) isdesigned as a mobile intensive care unit additionally equipped witha CT scanner (CereTom® 8-slice mobile CT scanner; NeuroLogica®,Danvers, MA), a point-of-care laboratory (Micros 60, ABX Diag-nostics; CoaguChek XS Plus, Roche Diagnostics Germany;and i-STAT Portable Clinical Analyzer, American ScreeningCorporation, Shreveport, LA), and the telemedicine infrastructurefor remote imaging reading as well as video-conferencing support(MEYTEC GmbH, Seefeld, Germany) for evaluating patients withsuspected AIS. The CT scanner is locked in a resting position whenthe vehicle is moving and unlocked for scanning during examination.The CT scanner is run from a small lead-shielded compartment insidethe vehicle. Radiation shielding had been calculated beforehand, andtechnical procedures were tested during a 2-week simulation period
before starting patient examinations. STEMO is staffed by a teamconsisting of a physician with at least 4 years of training in clinicalneurology and additional qualification in emergency medicine(neurologist), a paramedic of the fire brigade (similar to Emer-gency Medical Technician–Paramedic),18 and a radiographer(radiology technician with at least 2.5 years of clinical experienceand specially trained in the use of the CereTom scanner) withadditional paramedic qualification (similar to Emergency MedicalTechnician–Intermediate).18 The radiographer and the physician(who both stay inside the protected compartment in the vehicleduring CT examination) were provided with a dosimeter to rec-ord the radiation exposure caused by the CT scanner. The STE-MO is based at a fire brigade station close to the center of Berlin.The operating range was defined by a previously calculated 75%probability to arrive at the scene within 16 minutes and coversmore than 1,000,000 inhabitants. In the pilot study, STEMOwas supposed to operate from 7:00 AM to 6:30 PM from Mondayto Friday every week (11.5 hours daily). The only exception wastime required for maintenance, technical upgrades, and severalofficial engagements and presentations.
Dispatcher. The dispatch center of the fire brigade used a pre-viously validated interview algorithm16 to identify patients with ahigh probability of stroke within 4 hours after symptom onset orwith unknown time of onset. In this case, STEMO was deployedif available. STEMO was assisted by a regular ambulance at alltimes to avoid delays in the treatment of patients in case a tech-nical problem associated with STEMO occurred.
Patients and procedures. Basic medical care including specificneurologic expertise was offered to all patients who were managedby the STEMO team. Exclusion criteria for STEMO-specific pro-cedures (CT scan and point-of-care laboratory) were age youngerthan 18 years and possible or known pregnancy. Prehospital diag-nostics were started on-site or in the STEMO ambulance. Strokediagnosis was made clinically by the neurologist. In case of a sus-pected acute stroke, a brain CT was conducted (with the STEMOin the parking position) after phone consultation with a radiolo-gist. CT was performed only if it was considered to be helpfulfor a therapeutic decision in the STEMO. After completion ofthe scan, image data were sent to the radiologist on call via a tele-radiology system using bundled 3G standard (universal mobile tel-ecommunications system bandwidth: high-speed packet access).Additional analyses of blood glucose concentration, blood count,international normalized ratio, and electrolytes were performedsimultaneously. The radiologist conveyed the CT results to theneurologist on board the STEMO by mobile phone. The finaldecision for tPA treatment was made by the STEMO physicianafter a short telephone consultation with the project’s senior neu-rologist. Decision about eligibility for tPA was made on the basis ofthe drug license except for exclusion of patients older than 80 years(for detailed information, see http://www.strokeforum.com). Incase of AIS, patients were admitted to the closest “appropriatehospital” equipped with a stroke unit.
Data collection including follow-up documentation andstatistics. Data were collected from prehospital sources (data-base of the dispatch center and STEMO operation protocols),from hospital sources (medical reports), as well as from a 3-monthfollow-up telephone survey including a structured interviewregarding the modified Rankin scale and living conditions. Datawere analyzed only when patients had given informed consent forthe use and publication of individual data.
If patients were unavailable at the 3-month follow-up, theregistration office was contacted to ascertain whether the patienthad survived. All data are presented in a descriptive manner and
Figure 1 The stroke emergency mobile unit with CT scanner on board
Note the CT scanner in the back of the cabin and the separated shielded workstation on theright behind the door.
164 Neurology 80 January 8, 2013
ª 2013 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Walter S, et al. ‚Diagnosis and treatment of paPents with stroke in a mobile stroke unit versus in hospital: a
randomised controlled trial.‘ Lancet Neurol 2012;11:397–404.
The ‚mobile stroke unit‘ Konzept
Ebinger JE, et al. ‚Effect of the Use of Ambulance-‐Based Thrombolysis on Time to Thrombolysis in Acute Ischemic Stroke. A Randomized Clinical Trial.‘ JAMA 2014; 311(16):1621-‐32 -‐ Mobiles CT -‐ ‚point-‐of-‐care‘ Labor -‐ Röntgen-‐MTA -‐ Neurologe mit Notarztausbildung -‐ Telemedizinische Unterstützung

5 Antworten Ø Was ist der legale Hintergrund?
EXPERIMENTELLE THERAPIE Ø Gibt es Daten bzgl. prähospitaler Ultraschall-gestützte
Schlaganfalltherapie? KEINE
Ø Was sind die Vorrausetzungen für prähospitale Thrombolyse gestützt durch diagnostischen Ultraschall?
Voraussetzung ist ein sensitive/-spezifische Diagnostik Wahrscheinlich nur bei großen Gefäßverschlüsen
Ø Was ist der Gold-Standard in der Prähospitaldiagnostik? Krankenhausdiagnose (retrospektiv)
Ø Ist es die Mühe und das Risiko wert? in verzweifelten Situationen, JA
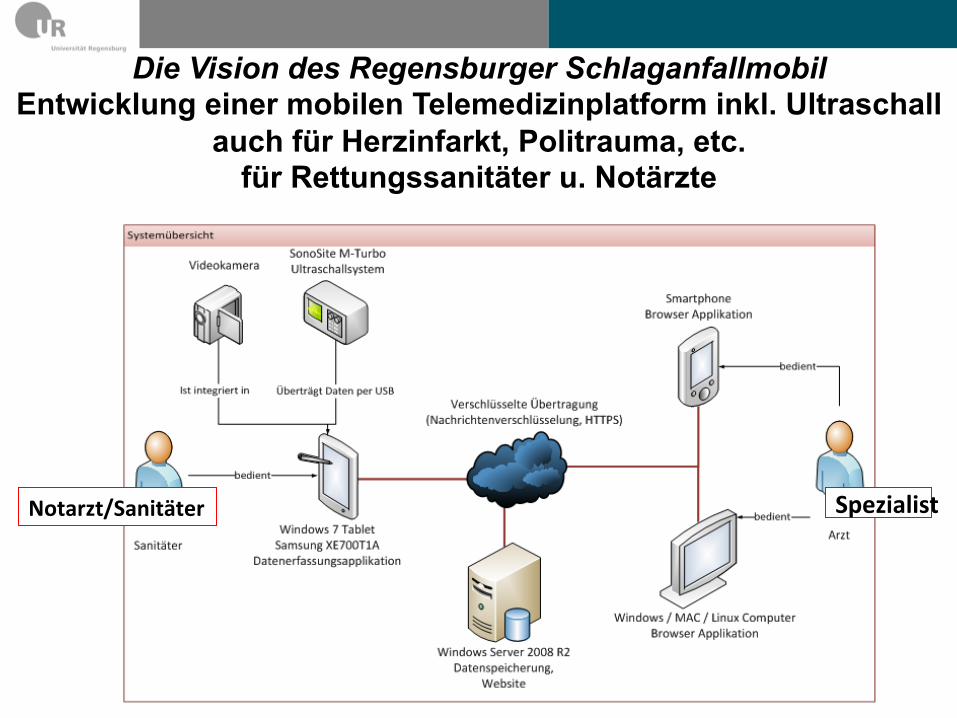
Notarzt/Sanitäter
Die Vision des Regensburger Schlaganfallmobil Entwicklung einer mobilen Telemedizinplatform inkl. Ultraschall
auch für Herzinfarkt, Politrauma, etc. für Rettungssanitäter u. Notärzte
Spezialist

Herzlichen Dank an alle Beteiligten!
Neurologie am Bezirksklinikikum Regensburg: S. Boy, F. Schlachetzki, M. Herzberg, S. Theiss, M. Ertl, A. Komenkho, D. Baldaranov, U. Bogdahn Interdisziplinäre Notaufnahme Universitätsklinikum Regensburg: M.Zimmermann Anästhesie Universitätsklinikum Regensburg: K.P. IJner University of California San Diego: T.Hölscher Neurologie KH Barmherzige Brüder Regensburg: H. Pels Integrierte ReJungsleitstelle Regensburg Hochschule für angewandte Wissenscha{en Regensburg: K. Pflug, M. Kucera, T. Waas, A. Leis Allen Notärzten und ReJungsdienstmitarbeitern in und um Regensburg

n = 14
„was alle angeht, können nur alle lösen“ Friedrich DürrenmaJ (1921-‐1990)
















