Ruth Maria Graf, Afranio Bernardes, Andre Auerswald, and Lucia Noronha
Curitiba, Brazil
Abstract. The Ultrapulse CO2 laser (Coherent Inc., Palo Alto,CA, USA) was used in 239 patients, from March 1996 to July1998, for full-face laser resurfacing. In 106 (43%) of thesepatients rhytidectomy was performed in the same procedure.All patients submitted to laser resurfacing were prepared for 1to 2 months beforehand with retinoic acid and hydroquinone.The procedures were done under local anesthesia controlled byan anesthesiologist. A clear film dressing impregnated withsilicone gel (Silon TSR; Bio-Med Sciences, Bethlehem, PA,USA) was used for 6 to 7 days and complete healing wasobserved in 7 to 10 days. Complications were exclusively der-matologic, without relation to surgery. No necrosis of the cu-taneous flap was observed. Skin biopsies of 10 consecutivepatients undergoing the combined procedures revealed no vas-cular impairment to the dermis. The patients were able to re-sume their activities 2 weeks after the procedure.
Key words: Laser—Resurfacing—Facial rejuvenation
During the last several years a series of authors has beenstudying applications of the CO2 laser for skin resurfac-ing in an effort to achieve facial rejuvenation and thesestudies have led to increased interest in this technology[3,4,9,10,12,14]. As the evolution of this technology hasprogressed the “computer pattern generator scanner”(CPG) has made the treatment of large surface areasfaster and easier [1,2,11]. After successfully employingthe CO2 laser in association with minimal procedures infacial surgery such as superior blepharoplasty, inferiortransconjunctival blepharoplasty, and endoscopic brow-lift, we began using the CO2 laser in conjunction withcervical facelifting. In order to maintain optimal vascu-larity of the flap the undermining was carried out in deep
subcutaneous and sub-SMAS planes, while the residualthermal coagulation of the CO2 laser reached the papil-lary dermis, leaving the subdermal flap vascularizationtotally intact [8].
Patients and Methods
From March 1996 to September 1998, 260 laser resur-facing procedures were carried out using an UltrapulseCO2 laser (Coherent, Inc., Palo Alto, CA, USA). Twohundred thirty-six patients were female and 24 weremale. The age range was from 15 to 70 years, with thegreatest incidence among 40 to 49 and 50 to 59 years.The patients were prepared preoperatively, beginning 1month prior to surgery in patients with fairer skin types(Fitzpatrick I and II classifications) to 2 months prior inpatients with darker skin types (Fitzpatrick III and Vclassifications), with 0.025% retinoic acid, 2–4% hydro-quinone (according to skin type) and SPF-25 (solar pro-tection factor). Forty-eight hours before the proceduresall patients received acyclovir and antibiotics (cephalo-sporin) and were maintained on this regimen for 7 daysafter the laser procedure as recommended by other au-thors [6]. The patients who had full facial resurfacingwere given dexamethasone (Decadron), 4 mg intrave-nously during and after the operation, followed by oralDecadron for 2 days. The procedures were all done underlocal anesthesia and sedation with control by an anesthe-siologist. After preparation, all wrinkles and deep sulciwere marked with methylene blue. Anesthetic nerveblocks were performed (supra- and infraorbital, nasalciliary, mental, maxillary, and cutaneous branches of thecervical plexus) and were complemented with local an-esthesia subcutaneously. Lidocaine (2%) was used forthe nerve blocks and Marcaine with 1:400,000 epineph-rine was used subcutaneously. Tetracaine eyedrops wereused. During all resurfacing procedures around the eyethe globe was protected by an eye shield. Full-face laser
Correspondence to Ruth Graf, R. Solimo˜es 1184, Curitiba, Pa-rana, 80.810-070, Brazil
resurfacing was carried out in 134 patients alone or inassociation with surgical procedures such as superiorblepharoplasty, inferior transconjunctival blepharo-plasty, canthopexy, and facial lipoinjection. In 106 pa-tients, the laser was associated with full rhytidectomy atthe same time. In these cases, the rhytidectomy was car-ried with deep undermining at the SMAS-platysma levelafter a brief subcutaneous approach. Laser resurfacingwas applied over the cutaneous flap and neck with alower energy and only one pass. In 20 patients the laserwas regional, mainly perioral and periorbital. All surgi-cal procedures were carried out before resurfacing. Thelaser treatment was begun with the laser in the margins ofwrinkles previously marked (shoulders) with 500 mJ at10 W with the Ultrapulse and CPG off. The treated areaswere cleaned with saline to remove the vaporized epi-dermis, and following this two passes at 300 mJ and 60W with CPG 396 were made in the nasal and frontal area,lips, and cheeks, and two passes at 175 mJ and 30 W withCPG 366 in the eyelids. On the neck and the small un-dermined skin flap in the preauricular area, one pass at175 mJ and 30 W with CPG 396 was employed. All areaswere cleaned after each pass. All laser-treated areas weredressed with a clear film dressing impregnated with sili-cone gel (Silon TSR; Bio-Med Sciences, Bethlehem, PA,USA), changed when necessary, usually on the thirdpostoperative day, and used until the seventh or eighthpostoperative day. On exposed areas such as around themouth and the lower neck where Silon could not be used,Vaseline was used on a daily basis. After the occlusivedressings were removed, the patients were instructed inthe use of neutral hydrating creams, hydrocortisonecreams for itching and erythema, and a solar filter withsunlight protection. After the first month the skin wasmore sensitive and erythematous and was prone to hy-perpigmentation unless prevented or treated. For this rea-son, topical treatment was begun at the first postopera-tive month utilizing 8% glycolic acid and 2–4% hydro-quinone. The patients were advised to avoid sunexposure for 3 to 4 months.
Biopsies were carried out in 10 consecutive patientsfor histologic study. The area was the preauricular regionover the cutaneous flap, which had been treated with 175mJ, 30 W, and CPG 396 and only one pass. These sameparameters were used for all biopsies.
Results
Table 1 shows that among 260 patients, 134 (50.6%)were submitted to full-face laser resurfacing (FFLR) as-sociated with limited surgical procedures, 106 patients(42.7%) had a complete rhytidectomy with FFLR, and 20patients (6.7%) were submitted to a regional facial laser.
In all patients who had lower eyelid flaccidity (posi-tive Snap test), a canthopexy with Flowers’ technique [5]was performed. Personal satisfaction studies revealedthat in 148 patients (57%) the results were beyond ex-pectations 6 months after surgery, and in 86 patients(33%) good results were obtained, with complaints re-
garding some wrinkle reappearance, which were treatedpostoperatively with botulin toxin [7]. In 20 patients(8%) the results were considered average due to postop-erative complications, return of some wrinkles, long-lasting hyperpigmentation, and the reappearance of someacne scars. Five patients (2%) with severe acne scarsconsidered their results poor and additional laser therapywas considered.
Studies have been done to define the histological dam-age of the CO2 laser on the skin [13]. In order to definethe CO2 laser effect on the skin flap, biopsies of the flapat the preauricular area were carried out in 10 patientswith one pass of the CO2 laser at 175 mJ and 30 W withCPG 396. Coagulative necrosis of the epidermis throughthe papillary dermis was observed. No histological dam-age was seen on vessels of the superficial reticular der-mis. The vessels of the superficial and deep reticulardermis were maintained intact (Figs. 1 and 2).
Complications occurred in two cases with localizedbacterial infections, which were treated with topicaltherapy. One case of fungus infection treated with flu-conazole, 100 mg for 7 days, associated with topicaltherapy (Figs. 22 and 23) and eight cases of contactdermatitis during the first month postoperatively wererelated to hypersensitivity to the chemical agent or hyd-roquinone allergy solved by changing the active creamagents. The erythema disappeared in all cases in 3months or less and hyperpigmentation was treated withclarifying creams for 2 to 3 months. Figures 3 to 21 showthe typical normal evolution of six patients submitted tofull-face laser resurfacing and rhytidectomy at the sametime. There were no cases of intense hypopigmentationand clarifying creams were discontinued as soon as theskin reached a natural color, because prolonged utiliza-tion can lead to unrecoverable hypopigmentation. No pa-tients had necrosis of the cutaneous flap associated withlaser therapy. With the exception of those patients un-dergoing the above-mentioned dermatologic complica-tions, all patients were able to resume activities 2 weeksafter surgery, but utilizing makeup in order to minimizethe intensity of the erythema.
Our experience has shown that laser resurfacing is asignificant adjunct in facial rejuvenation and that full-face laser resurfacing can be carried out in patients un-dergoing full rhytidectomy if the surgical plane is keptdeep and the laser application in the more superficialsubcutaneous dissection is kept at a minimal level (175mJ, one pass). The management of patients undergoingfull-face laser resurfacing extends far beyond the imme-diate operative experience. Aggressive treatment of thesurface should be carried out for 2 months postopera-
tively and attention should be directed to observing thedevelopment of late dermatologic sequelae. Our histo-logical studies confirmed the safety of using the CO2laser, one pass at 175 mJ, over the cutaneous flap carriedout during rhytidectomy. The histologic aspects includedcoagulative necrosis of the epidermis through the papil-lary dermis. No histological damage was seen on vesselsof the superficial reticular dermis. In the deeper layers ofthe cutaneous flap (deep reticular dermis and hypoder-mis), the vessels also were intact. If the cutaneous flap inthe rhytidectomy is thick enough, the CO2 laser can be
Fig. 1. Histological study of the skinflap after one CO2 laser pass at 175 mJand CPG 396, showing epidermalvaporization, papillary dermiscoagulation, and intact vessels of thesuperficial reticular dermis.Fig. 2. Histological study of the sameskin flap as in Fig. 1, showing intactvessels of the deep dermis andhypodermis.
Fig. 3. Preoperative 62-year-old female patient, with facialflaccidity and wrinkles around the eyes, mouth, and frontalregion.Fig. 4.The 14th postoperative day: the patient was submitted to
rhytidectomy, full-face laser resurfacing, superior blepharo-plasty, inferior transconjunctival blepharoplasty, canthopexy,and lipoinjection of the nasolabial fold.Fig. 5. Same patient at the sixth postoperative month.
103R.M. Graf et al.
Fig. 6. 57-year-old female patient who needs facial rejuvena-tion surgery.Fig. 7. Seventh postoperative day after rhytidectomy combinedwith full-face laser resurfacing; erythema still present.
Fig. 8. Same patient at the sixth postoperative month.Figs. 9, 10, and 11.Same patient, another position: preopera-tive, seventh postoperative day, and sixth postoperative month.
Fig. 12. A 50-year-old female patient submitted to rhytidec-tomy and full-face laser resurfacing.
Fig. 13. Same patient at the 14th postoperative day.Fig. 14. Same patient 1 year after surgery.
104 Full-Face Laser Resurfacing
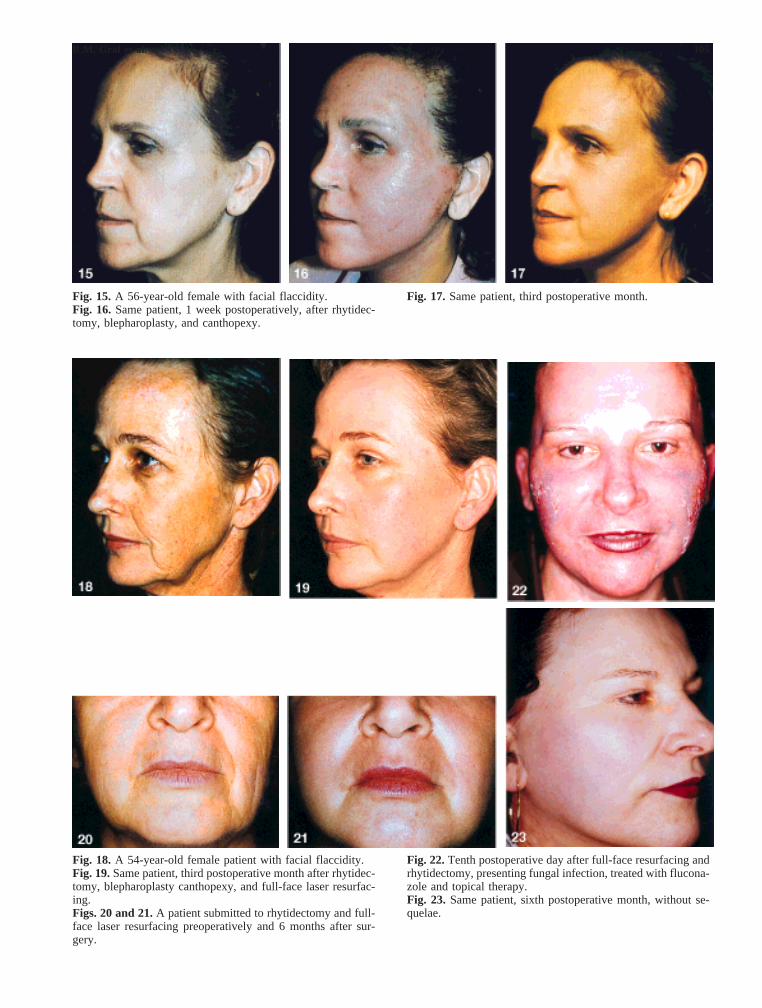
Fig. 15. A 56-year-old female with facial flaccidity.Fig. 16. Same patient, 1 week postoperatively, after rhytidec-tomy, blepharoplasty, and canthopexy.
Fig. 17. Same patient, third postoperative month.
Fig. 18. A 54-year-old female patient with facial flaccidity.Fig. 19.Same patient, third postoperative month after rhytidec-tomy, blepharoplasty canthopexy, and full-face laser resurfac-ing.Figs. 20 and 21.A patient submitted to rhytidectomy and full-face laser resurfacing preoperatively and 6 months after sur-gery.
Fig. 22.Tenth postoperative day after full-face resurfacing andrhytidectomy, presenting fungal infection, treated with flucona-zole and topical therapy.Fig. 23. Same patient, sixth postoperative month, without se-quelae.
105R.M. Graf et al.
used over the entire flap safely as observed in the histo-logic studies.
Prior to utilizing the CO2 laser for facial rejuvenationthe plastic surgeon should observe an experienced teamcarrying out this procedure. It would be advisable toundermine the cutaneous flap in a limited extension anduse the CO2 laser at a lower energy over the flap duringthe beginning of a surgeon’s experience and to conductcareful screening of the patient’s psychological capacityto deal with the possibility of prolonged erythema ordermatologic complications.
Acknowledgments.The authors are grateful to Dr. ThomasBiggs and Dr. Ricardo Baroudi for their continuous support,advice, and critical review of the manuscript.
References
1. Apfelberg DB: Ultrapulse carbon dioxide laser with CPGscanner for full-face resurfacing for rhytids, photoagingand acne scars. Plast Reconstr Surg99(7):1817, 1997
2. Alster TS: Treatment of facial rhytides with a high-energypulsed carbon dioxide laser. Plast Reconstr Surg98(5):791, 1996
3. Fitzpatrick RE, et al.: The depth of thermal necrosis usingthe CO2 laser. A comparison of the superpulsed mode andconventional mode. J Dermatol Surg Oncol17:340, 1991
4. Fitzpatrick RE: Depth of vaporization and residual thermal
damage using multiple passes of the ultrapulse CO2 laser.Lasers Surg Med21(9):31, 1997
5. Flowers RS: Canthopexy and aestheyic blepharoplasty.Presented to the Annual Meeting of the American Societyfor Aesthetic Plastic Surgeons, 1983
6. Hoefflin SM: Preoperative and postoperative care for laserresurfacing patients. Aesth Surg16(4):232, 1996
7. Matsudo PK: Botulinum toxin for correction of fronto-glabella wrinkles: Preliminary evaluation. Aesth Plast Surg20:439, 1996
8. Nathan M, Felder DS: CO2 laser resurfacing over facialflaps. Aesth Surg17(5):285, 1997
9. Roberts TL III, et al.: CO2 laser resurfacing: Recognizingand minimizing complications. Aesth Surg16(2):142,1996
10. Roberts TL III, Weinstein C, et al.: Aesthetic CO2 lasersurgery: Evaluation of 907 patients. Aesth Surg17(5):293,1997
11. Roncati C, Tundisi M: Resurfacing com o ultrapulse-laser;Nova arma no rejuvenescimento facial. Rev Bras SBCPEstet Reconstr11(2):69, 1996