Functional MR Imaging of the Uterus Asako Nakai, MD, PhD*,Takashi Koyama, MD, PhD , Koji Fujimoto, MD , KaoriTogashi, MD, PhD MR imaging is an established method for the eval- uation of a variety of gynecologic conditions and diseases. It is established as a problem-solving modality when ultrasound evaluation is equivocal, because of its excellent tissue contrast reflecting pathology compared with CT. MR imaging has additional advantages because it is noninvasive and more importantly free from ionizing radiation, being especially beneficial to evaluate repro- ductive-aged women. The standard technique involves the acquisition of spin-echo T1- and T2- weighted sequences. On T2-weighted images, the uterus in reproductive-aged women demon- strates distinct anatomic zonal differentiation (Fig. 1). The combination of these two types of se- quences with different contrasts provides informa- tion on tissue contents so that a specific diagnosis is often reached. Recent developments in MR techniques have enabled the functional assessment of the uterus. Cine MR imaging using rapid T2 sequences is used to evaluate the kinematic function of the uterus by demonstrating temporal morphologic changes. Diffusion-weighted imaging (DWI) pro- vides tissue contrast based on molecular diffusion phenomenon. Finally, dynamic contrast-enhanced (DCE) MR imaging is a promising tool for evaluat- ing vascular dynamics. Although most of these techniques are still in the experimental stage, they may provide functional information when used in combination with standard imaging methods. UTERINE CONTRACTIONS ON CINE MR IMAGING Technique Recent developments in ultrafast MR imaging techniques have enabled the acquisition of serial images with few seconds between each acquisi- tion, although spatial and contrast resolutions are worse than those of conventional imaging. Under quiet respiration, 60 serial rapid T2-weighted images in the midsagittal plane of the uterus can be obtained repeatedly within 2 to 3 minutes. T2-weighted half-Fourier rapid acquisition with the relaxation enhancement technique provides sufficient contrast between three layers of the uterus with an acquisition time of less than a sec- ond. Of great importance is the display of images in the cine mode at a faster speed than real time to enhance slow and subtle movements of uterine peristalsis. Assessment of uterine peristalsis can be performed visually or semiautomatically by using software with an automated contour-tracing method. 1 Results In nongravid myometrium, at least two patterns of myometrial contractions are known. One involves sustained contraction and the other consists of uterine peristalsis. Sustained contraction is mainly characterized by focal and sporadic myometrial contractility, which frequently involves the entire layer of the myometrium; this type of contraction may be sustained for several minutes. 2,3 On static Department of Diagnostic Radiology, Kyoto University Hospital, 54 Kawahara-cho Shogoin Sakyo-ku, Kyoto 606-8507, Japan * Corresponding author. E-mail address: [email protected] (A. Nakai). KEYWORDS Uterus Function Cine MR imaging Diffusion-weighted MR imaging Dynamic contrast-enhanced MR imaging Magn Reson Imaging Clin N Am 16 (2008) 673–684 doi:10.1016/j.mric.2008.07.010 1064-9689/08/$ – see front matter ª 2008 Elsevier Inc. All rights reserved. mri.theclinics.com
KEYWORDS� Uterus � Function � Cine MR imaging� Diffusion-weighted MR imaging� Dynamic contrast-enhanced MR imaging
MR imaging is an established method for the eval-uation of a variety of gynecologic conditions anddiseases. It is established as a problem-solvingmodality when ultrasound evaluation is equivocal,because of its excellent tissue contrast reflectingpathology compared with CT. MR imaging hasadditional advantages because it is noninvasiveand more importantly free from ionizing radiation,being especially beneficial to evaluate repro-ductive-aged women. The standard techniqueinvolves the acquisition of spin-echo T1- and T2-weighted sequences. On T2-weighted images,the uterus in reproductive-aged women demon-strates distinct anatomic zonal differentiation(Fig. 1). The combination of these two types of se-quences with different contrasts provides informa-tion on tissue contents so that a specific diagnosisis often reached.
Recent developments in MR techniques haveenabled the functional assessment of the uterus.Cine MR imaging using rapid T2 sequences isused to evaluate the kinematic function of theuterus by demonstrating temporal morphologicchanges. Diffusion-weighted imaging (DWI) pro-vides tissue contrast based on molecular diffusionphenomenon. Finally, dynamic contrast-enhanced(DCE) MR imaging is a promising tool for evaluat-ing vascular dynamics. Although most of thesetechniques are still in the experimental stage,they may provide functional information whenused in combination with standard imagingmethods.
Department of Diagnostic Radiology, Kyoto University H606-8507, Japan* Corresponding author.E-mail address: [email protected] (A. Nakai).
Magn Reson Imaging Clin N Am 16 (2008) 673–684doi:10.1016/j.mric.2008.07.0101064-9689/08/$ – see front matter ª 2008 Elsevier Inc. All
UTERINE CONTRACTIONS ON CINEMR IMAGINGTechnique
Recent developments in ultrafast MR imagingtechniques have enabled the acquisition of serialimages with few seconds between each acquisi-tion, although spatial and contrast resolutions areworse than those of conventional imaging. Underquiet respiration, 60 serial rapid T2-weightedimages in the midsagittal plane of the uterus canbe obtained repeatedly within 2 to 3 minutes.T2-weighted half-Fourier rapid acquisition withthe relaxation enhancement technique providessufficient contrast between three layers of theuterus with an acquisition time of less than a sec-ond. Of great importance is the display of imagesin the cine mode at a faster speed than real timeto enhance slow and subtle movements of uterineperistalsis. Assessment of uterine peristalsis canbe performed visually or semiautomatically byusing software with an automated contour-tracingmethod.1
Results
In nongravid myometrium, at least two patterns ofmyometrial contractions are known. One involvessustained contraction and the other consists ofuterine peristalsis. Sustained contraction is mainlycharacterized by focal and sporadic myometrialcontractility, which frequently involves the entirelayer of the myometrium; this type of contractionmay be sustained for several minutes.2,3 On static
Fig.1. Normal uterus (asymptomatic28-year-oldwomanduring periovulatoryphase). Sagittal fast spin echo (FSE)T2-weighted image (TR/TE 5 3800/105). The endome-trium demonstrates high signal intensity (white arrow-head); the inner myometrium demonstrates low signalintensity also known as the ‘‘junctional zone’’ (blackarrowhead); and the myometrium shows relativelyhigh signal intensity (arrow).
Nakai et al674
T2-weighted images, sustained uterine contrac-tions are seen as transient focal masses of low sig-nal intensity, which bulge into the endometrium.2
These focal contractions are known as ‘‘pseudole-sions,’’ which can mimic disease processes, suchas leiomyomas and adenomyosis (Fig. 2).2,3
Uterine peristalsis is identifiable on ultrasound asrhythmic and subtle wave-like endometrial move-ments associated with contractions of the suben-dometrial myometrium.4–6 The frequency, height,and direction of the peristaltic waves have been
Fig. 2. Sustained contraction (asymptomatic 27-year-old wo120). Ill-defined focal area with low signal intensity in thescans 12 days later (B). This pseudolesion can mimic adeno
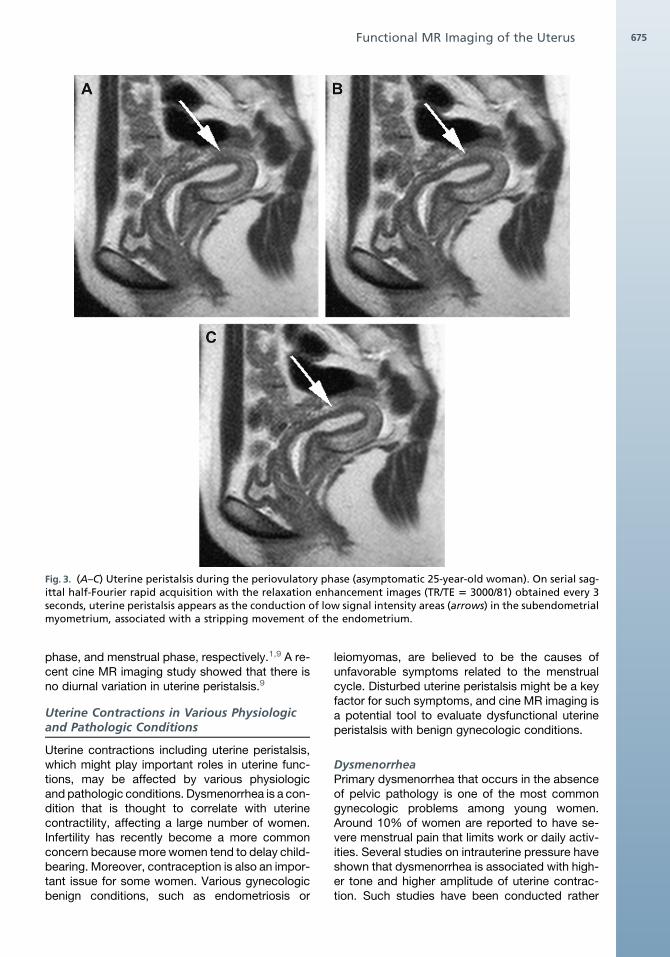
reported to vary throughout the phases of themenstrual cycle.4,5 It has been postulated that uter-ine peristalsis occurs for such activities as spermtransport, discharge of menstrual blood, andconservation of the gestational sac during the earlystages of pregnancy.4,5 Uterine peristalsis hasnot been identified on conventional T2-weightedimages, however, because of insufficient temporalresolution. On cine MR imaging, uterine peristalsiscan be depicted as the conduction of low-intensityareas in the subendometrial myometrium, usuallyassociated with a stripping movement of theendometrium (Fig. 3).7,8 The conduction of low-intensity areas seems directly to display subtleand rhythmic contractions of the subendometrialmyometrium.
Cine MR imaging allows the observation of bothsustained contractions and peristalsis, and is usedfor investigating the changes and impairment inuterine function in a variety of conditions andgynecologic disorders.
Uterine Peristalsis in HealthyNongravid Women
Cine MR imaging demonstrates drastic changes inuterine peristalsis through the phases of the men-strual cycle. Peristaltic waves predominantly travelin a cervicofundal direction during the proliferativeand periovulatory phases, and in a fundocervicaldirection during menstruation.1,7–9 On cine MR im-aging, it was observed that uterine peristalsis wasmost active during the periovulatory phase (91.7%positive) and most subdued during the lutealphase (27.1% positive). The average frequenciesof the conduction waves are 4.5, 0.9, and 1.3 per2 minutes for the periovulatory phase, luteal
man). Sagittal FSE T2-weighted images (TR/TE 5 4000/myometrium (arrow in A) disappears during repeatedmyosis.
Fig. 3. (A–C) Uterine peristalsis during the periovulatory phase (asymptomatic 25-year-old woman). On serial sag-ittal half-Fourier rapid acquisition with the relaxation enhancement images (TR/TE 5 3000/81) obtained every 3seconds, uterine peristalsis appears as the conduction of low signal intensity areas (arrows) in the subendometrialmyometrium, associated with a stripping movement of the endometrium.
Functional MR Imaging of the Uterus 675
phase, and menstrual phase, respectively.1,9 A re-cent cine MR imaging study showed that there isno diurnal variation in uterine peristalsis.9
Uterine Contractions in Various Physiologicand Pathologic Conditions
Uterine contractions including uterine peristalsis,which might play important roles in uterine func-tions, may be affected by various physiologicand pathologic conditions. Dysmenorrhea is a con-dition that is thought to correlate with uterinecontractility, affecting a large number of women.Infertility has recently become a more commonconcern because more women tend to delay child-bearing. Moreover, contraception is also an impor-tant issue for some women. Various gynecologicbenign conditions, such as endometriosis or
leiomyomas, are believed to be the causes ofunfavorable symptoms related to the menstrualcycle. Disturbed uterine peristalsis might be a keyfactor for such symptoms, and cine MR imaging isa potential tool to evaluate dysfunctional uterineperistalsis with benign gynecologic conditions.
DysmenorrheaPrimary dysmenorrhea that occurs in the absenceof pelvic pathology is one of the most commongynecologic problems among young women.Around 10% of women are reported to have se-vere menstrual pain that limits work or daily activ-ities. Several studies on intrauterine pressure haveshown that dysmenorrhea is associated with high-er tone and higher amplitude of uterine contrac-tion. Such studies have been conducted rather
Nakai et al676
invasively, however, and they might have causedartifactual contractility. Because of these limita-tions and the difficulty of assessing subjectivepain, the literature on dysmenorrhea is extremelylimited. The evaluation of uterine contraction onMR imaging may provide a potential tool objec-tively to evaluate dysmenorrhea. On MR imaging,the volume of the myometrium is smaller whenthe subjects have maximum pain compared withthose without pain.10 Remarkable changes werenoted on uterine cine MR imaging in early cyclewith severe pain and on a different cycle date with-out pain (Fig. 4).10 Increased pain is related toa thicker junctional zone, the presence of focalcontractions, or endometrial distortion, all of thesecharacteristics representing stronger uterinecontractility.10
Cine MR imaging is also useful for the evaluationof treatment effects. During menstruation, womentaking oral contraceptives (OC) for contraceptionor dysmenorrhea show less prominent endome-trial distortion and a thinner subendometrial low-intensity area11 compared with healthy women.There was a slight tendency for a larger myometrialarea in women taking OCs, indicating less myome-trial contractility, which might be one of the rea-sons for reduced menstrual pain.11
Effects of contraceptivesIntrauterine devices are very effective ways of con-traception worldwide. Two major mechanisms areconsidered to be involved in this method of contra-ception: the interrupted implantation of the fer-tilized ovum, and a spermicidal effect by theinhibition of sperm transport.12,13 The exact mech-anisms, however, remain controversial.12,13 Ina previous study using cine MR imaging, dominantfundocervical directed peristaltic waves weredemonstrated in as many as 4 of 11 intrauterine
Fig. 4. Dysmenorrhea during menstruation (30-year-old wodate 1 (A) and day 3 (B). The uterine myometrium on cyclsignal intensity (arrows in A) compared with that on cycle
device–bearing subjects during their periovulatoryphase, whereas cervicofundal-directed peristalsiswas dominant in healthy control women.14 Suchfundocervical waves spread through more thanhalf of the thickness of the myometrium, and mightserve for expelling intrauterine devices from theuterine cavity rather than supporting sperm trans-port. Furthermore, the peristaltic frequency in in-trauterine device users (five per 3 minutes) wasless than that of the control group (6.5 per 3 min-utes).14 Uncoordinated contractions on cine MRimaging and a significantly thick junctional zoneon static images were also observed, which mightbe closely related to each other (Fig. 5).14
OCs are the most widely used and effectivemethod of contraception, and are commonlyused to minimize dysmenorrhea. Preliminary datashow that uterine peristalsis was hardly discern-able even at the midcycle in OC users on cineMR imaging.15 Sporadic contractions were lessfrequent, and endometrial distortion was muchless identified in the OC group. On staticT2-weighted images, OC users showed a thinendometrium and junctional zone (Fig. 6).15 Theuterine myometrial area was larger in the OC group(19.8 cm2) than in the control group (16.4 cm2).15
All these observations suggest that uterine contra-ctility is suppressed in OC users. It is still unclear,however, how these facts affect the mechanismsof contraception and reduction of dysmenorrhea.
Infertility with endometriosis or leiomyomaInfertility is associated with a wide variety of patho-logic conditions, and much of the etiology of infertil-ity remains unresolved. Endometriosis representsone of the most important factors of infertility, and30% to 50% of women with endometriosis areinfertile.16 Preliminary results showed that uterineperistalsis was suppressed and identifiable in less
man). Sagittal RARE images (TR/TE 5 2000/81) on cyclee date 1 with severe pain is smaller and exhibits lower
date 3 without pain (B).
Fig. 5. Intrauterine device user during the periovula-tory phase (34-year-old woman). On a sagittal FSET2-weighted image (TR/TE 5 5470/122), a thick junc-tional zone more than half of the myometrium isnoted (arrow). This finding suggests the presence ofstrong myometrial contractility, which might servefor expelling the intrauterine device from the uterinecavity rather than supporting sperm transport. Intra-uterine device is seen as dotted low-intensity areaslined at the center of the endometrium.
Fig. 6. Oral contraceptive user during the periovula-tory phase (22-year-old woman). On a sagittal FSET2-weighted image (TR/TE 5470/122), both the endo-metrium (arrowheads) and the junctional zone(arrows) are thin. On cine MR imaging (not shown),uterine peristalsis is not observed in this thin junc-tional zone even in the periovulatory phase, whennormally frequent and strong uterine peristalsis isobserved, suggesting sperm transport is not sup-ported by the uterine motion.
Functional MR Imaging of the Uterus 677
than half of the patients with endometrioma even inthe periovulatory phase when nearly 100% ofhealthy women demonstrated uterine peristalsis.17
The frequency of peristalsis in the endometriosisgroup was also less than that in the control group.Decreased peristalsis in patients with endometri-osis could be a possible cause of infertility, byadversely affecting sperm transport. Sporadiccontractions were more frequently observed inthe endometriosis group than in healthy controls,although this observation was not statisticallysignificant.
Submucosal leiomyoma is a well-known uterinefactor for miscarriage or infertility.18 The role ofsubmucosal leiomyoma in miscarriage or infertilityhas not been elucidated, although the mechanicalprevention of sperm transportation and nidation,and hypercontractility, have been postulated aspossible causes. Preliminary investigations usingcine MR imaging demonstrated focal and irregularmyometrial contractions that were different fromperistalsis around submucosal leiomyomas in55% of patients with submucosal leiomyomas.19
The conduction of the peristaltic movementsbecame indistinct at the site of submucosal leio-myomas.19 These observations indicate that theobliteration of regular peristalsis or dysfunctionalmyometrial movements caused by submucosalleiomyomas may be one of the causative factorsin pregnancy loss or infertility.
DIFFUSION-WEIGHTED IMAGING
DWI is a recently introduced technique that allowsthe observation of differences in molecular diffu-sion caused by the random and microscopicmotion of molecules, also known as ‘‘brownianmotion.’’20 One of the attractive benefits of DWIis that it provides tissue contrast based on mo-lecular diffusion, which differs from conventionalT1- and T2-weighted images. The use of this tech-nique has been initially established in the centralnervous system, mainly for the diagnosis of acutestroke. This technique has now become availablefor the abdomen and pelvis. DWI can delineatemalignant lesions displaying hyperintense signalbecause water diffusion is restricted in tissues ofhigh cellularity.21,22 Recent developments in paral-lel imaging techniques have improved the qualityof abdominal DWI by reducing the acquisitiontime, and by minimizing the echoplanar imaging–related susceptibility artifacts. DWI also allowsthe quantitative measurement of the apparent dif-fusion coefficient (ADC) value. Decreased ADCvalues of malignant tumors compared with thoseof normal tissues or benign lesions have been pre-viously reported in various organs.
nard
iffusionim
agingof
thepe
lvisin
thesagittalplan
e
rslice
(mm)
Num
ber
ofSlices
Acquisitio
nMatrix
Band
width
(Hz/Pixe
l)
Paralle
lIm
aging
Factor
NEX
Total
Acquisitio
nTime(m
in:s)
bVa
lue
(s/m
m2)
19
128�
61
1446
25
1:3
40,
500,
1000
Nakai et al678
Technique
DWI measures the loss of signal after a series oftwo symmetric gradient pulses called ‘‘motion-probing gradient’’ pulses, which are added toboth sides of a 180 refocusing radiofrequencypulse to enhance the difference of molecular diffu-sion phenomena between tissues. Motion-probinggradient pulses are commonly applied in threedirections on a X-Y-Z axis. DWI with single-shotecho-planar imaging can provide excellent con-trast-to-noise ratio because the signals of mostorgans are very low, whereas the lesion signalsremain high.23,24 The intensity of motion-probinggradient pulses is represented by the b-value,which affects the signal intensity on DWI. On DWIwith an intermediate b-value (eg, 500 s/mm2), urineor ascites appear as comparatively high-signalintensity according to T2 contamination.25 ThisT2 contamination is successfully excluded by look-ing at ADC maps. On DWI with a higher b-value(eg, 800 or 1000 s/mm2), malignant tumors andlymph nodes are more conspicuous comparedwith images with lower b-value because most ofthe normal pelvic tissue is strongly suppressed,although anatomic detailed information is lost.
In body regions, short TI inversion recovery fatsuppression may provide more homogeneous fatsuppression compared with the chemical shift-selective method; the latter method has bettersignal-to-noise ratio.22
The authors’ standard protocols for pelvic DWIare performed with a 1.5-T magnet unit, a multi-channel body phased-array coil, and a single-shot echo-planar imaging sequence under freebreathing in the sagittal plane (Table 1).
Table1
Sugg
estedpa
rametersf
oracqu
isition
ofsing
leshot
echo
pla
TR(m
s)TE
(ms)
Fieldof
View
(mm)
Thickn
ess
(mm)
Inte
Gap
2300–2
600
75–7
9260–3
00
51.5
Diffusion-Weighted Imaging Assessment
There are two methods for assessment: visual as-sessment and quantitative assessment of ADCvalues. The latter gives more specific informationon molecular diffusion.
Visual assessmentA three-dimensional display of images acquired intwo dimension with a reversed grayscale can pro-duce positron emission tomography–like imagesbecause of a strong suppression of backgroundsignal. It may be difficult, however, to define theanatomic locations.22 Recently fusion software,which overlays DWI onto conventional MR images,has become available.26
Assessment of apparent diffusioncoefficient valuesThe ADC value describes microscopic water diffu-sivity, and decreases in the presence of factors
Functional MR Imaging of the Uterus 679
that restrict water diffusion, such as cell mem-branes and the viscosity of the fluid. The ADCvalue can be obtained on a voxel-by-voxel basis,and depicted on an ADC map, allowing the mea-surement of a target tissue ADC value using re-gions of interest. In solid tumors, the ADC valuesare considered to be influenced by changes inthe balance between extracellular and intracellularwater molecules, and changes in cytologic mor-phology including the nuclear-to-cytoplasm ratioand cellular density.
Clinical Application
In the female pelvis, the expected clinical applica-tions of DWI include tumor detection and differenti-ation between malignant and benign lesions.The latter role of DWI may be limited, however, be-causea varietyofbenign tumorscan show restricteddiffusion. Accordingly, it is important to refer to con-ventional MR images when interpreting DW images.
Endometrial cancerTo evaluate endometrial cancer, visual assessmentof DWI is not useful because both endometrial can-cerous tissues and the normal endometrium canappear hyperintense on diffusion images. Alongwith the calculation of the ADC values, however,DWI has the potential to demonstrate uterine endo-metrial cancer, and differentiate between normaland cancerous tissues of the endometrium. TheADC value of endometrial cancer is prominentlylower than that of the normal endometrium(Fig. 7).27 The ADC map image can be used for de-tecting endometrial cancer lesions. In addition, theADC values of endometrial cancers of higher gradetend to decrease compared with those of lowergrade, although there is considerable overlap.27
Cervical cancerDWI has been shown to be useful in cervical can-cer to detect tumor location and the extensions oftumor and the normal uterine cervical tissues,which have similar signal intensities on T2-weighted images. The ADC value of cervical can-cer lesions has been reported to be lower thanthat of normal cervical tissues, and the ADC in-crease after chemotherapy or irradiation.28
Uterine sarcoma and leiomyomaUterine myometrial lesions with high signal intensityon T2-weighted images raise concerns if they aremalignant. For such lesions, DWI is helpful in differ-entiating uterine sarcomas from leiomyomas, byshowing restricted diffusion in the former, whereasordinary leiomyomas (including degenerated leio-myomas, which demonstrate high intensity onT2-weighted images) do not display restricted
diffusion.29 Cellular leiomyoma, however, which isa specific subtype of leiomyoma characterized byhypercellularity, also exhibits restricted diffusion;it is difficult to differentiate uterine sarcomas fromcellular leiomyomas on DWI.29,30 ADC values ofsarcomas also overlap with those of cellularleiomyomas. Accordingly, conventional MR im-ages should be meticulously observed to differen-tiate uterine sarcomas better from leiomyomas,although currently differentiation is limited. DWIcannot tell the difference between cellular leiomyo-mas and sarcomas but ordinary leiomyomasincluding degenerated leiomyomas.
For uterine leiomyomas, DWI and ADC maps mayserve for assessing treatment response after uter-ine artery embolization by providing functional infor-mation at a cellular level. The ADC values ofleiomyomas have been reported to decrease signif-icantly after uterine artery embolization31 or focusedultrasound ablation.32 For the confirmation of thetherapeutic effect, contrast-enhanced MR imagingis the standard technique recommended becauseit adds direct information on the lesion’s vascularity.
DYNAMIC CONTRAST-ENHANCEDMR IMAGING
DCE MR imaging is becoming a promising tool forassessment of cancer, and for monitoring tumortreatment response.33,34 Malignant tumors tendto have increased vessel density and vascular per-meability, with subsequent increased enhance-ment in the early phase of DCE MR imagingcompared with normal tissues.35 DCE MR imagingcan quantify tumor perfusion and permeability, andpotentially could be used as a noninvasive markerof angiogenesis, by showing correlation with histo-pathologic markers of angiogenesis (eg, micro-vessel density), which are performed on tissuesamples and are not always easily available.Assessments of tumor perfusion and permeabilitywith DCE MR imaging can be used for monitoringtreatment response, for prediction of treatmentresponse, and to predict clinical outcome.35–37 Re-cent developments in anticancer drugs have beendirected from cytotoxic therapies to more selectivetherapies that target the oncogenic abnormalitiesunderlying the tumors. Novel therapies includingantiangiogenic drugs and vascular targeting drugsare expected to improve the efficacy and toleranceof anticancer treatments.36–38 In gauging the thera-peutic effects of these treatments, there is a grow-ing need to evaluate drug efficacy based on suchfactors as hypoxia and tumor blood supply.
Technique
DCE MR imaging is usually performed with the useof low-molecular-weight contrast media, such as
Fig. 7. Endometrial cancer, stage T1b, grade 2 (34-year-old woman). (A) On a sagittal T2-weighted image, endo-metrial cancer (asterisk) appears lower signal intensity compared with normal endometrium, which shows highintensity (arrowheads). (B) On single-shot echo-planar imaging diffusion-weighted image (using b 5 1000),both the endometrial cancer (asterisk) and the normal endometrium appear hyperintense. (C) On the apparentdiffusion coefficient map, however, the endometrial cancer (asterisk) displays lower apparent diffusion coeffi-cient compared with normal endometrium (arrowheads).
Nakai et al680
gadopentetate dimeglumine. DCE MR imagingcommonly uses T1-weighted gradient-echo pulsesequences. Standard gradient-echo sequencesinclude spoiled gradient-echo (eg, fast low-angleshot) and magnetization-prepared gradient-echo(eg, turbo fast low-angle shot). The latter may bea preferable sequence for assessing T1-weightedperfusion because of excellent temporal resolu-tion, although its decreased flip angle may result ina decreased contrast-to-noise ratio and impairedimage quality. Compared with standard gradient-echo sequences, three-dimensional gradient-echosequences have the potential to provide highersignal-to-noise ratio and contrast-to-noise ratio,and fewer partial-volume effects. The applicationof parallel imaging can improve the temporalresolution.
Assessment of Dynamic Enhancement
Tissue perfusion can be assessed in two ways:a semiquantitative method analyzing the changesin signal intensity, and a quantitative method usinga pharmacokinetic model.
Semiquantitative assessmentThe semiquantitative method analyzes thechanges in signal intensity. This method is simpleand commonly used in the clinical setting witha dynamic enhancement curve. Parameters in-clude the onset time of enhancement, initial andmean gradients of the enhancement curves, max-imum signal intensity, and washout gradient.Although this method has the advantage of rela-tively simplified calculations, it is difficult to
Fig. 8. Cervical cancer, stage T1b (38-year-old woman). (A) Sagittal FSE T2-weighted image. (B) Dynamic contrastsagittal T1-weighted images: precontrast and postcontrast 20 seconds after the intravenous injection of gado-pentetate dimeglumine. Tumor detection is difficult on the T2-weighted image because of poor tumor contrastagainst normal cervical stromal tissue. (C) On an early postcontrast image, cervical cancer is more conspicuousbecause of strong enhancement (arrows).
Functional MR Imaging of the Uterus 681
compare data among patients and systems be-cause the parameters provided by the signal inten-sity are relative values and are influenced by thecardiac output of the patients, sequence parame-ters, and machines used. Such a semiquantitativemethod still provides valuable information, how-ever, to clinical management.
Quantitative assessmentThe quantitative method uses pharmacokineticmodeling and provides details of several parame-ters including (1) the volume transfer constant Ktrans
(min�1), which expresses blood flow and perme-ability; (2) the volume of extravascular-extracellularspace per unit volume of tissue ve (0 < ve < 1); and (3)the flux rate constant between extravascular-extra-cellular space and plasma kep.39 These three pa-rameters are linked as follows: kep 5 Ktrans / ve.When a bolus of a paramagnetic contrast agentpasses through a capillary bed, the contrast agent
rapidly passes into the extravascular-extracellularspace at Ktrans. Recently, Ktrans has been chosenas the primary end point in antivascular clinicaltrials because it reflects contrast agent delivery(perfusion) and transport across the vascular endo-thelium (permeability).36 If the contrast-agentconcentration is properly measured, the pharma-cokinetic parameters can be readily comparedwith the data obtained at different times in a givenpatient, in different patients, or with different sys-tems. There are several limitations, however, withthis technique: difficulties in data acquisition,need of an arterial input function, postprocessing,and image display using software.39
Clinical Applications for Uterine Cancers
DCE MR imaging is a technique used for assessinguterine pathologic conditions. It is especially use-ful for tumor detection and staging in malignant
Nakai et al682
tumors by adding different contrast between theuterine layers (ie, strong contrast against normaluterine tissues). In addition, parametric assess-ment allows the quantitative evaluation of vascu-larity of tumor.
Cervical cancerAlthough DCE MR imaging does not significantlyimprove staging accuracy compared with stan-dard T2-weighted images, it may be additionallyapplied for detection of early stage cervical cancer(Fig. 8).40 Furthermore, the functional assessmentof the microcirculation using DCE MR imaging hasbeen suggested to predict therapy outcome incervical cancer, in addition to traditional factors,such as stage, extent of disease, histologic type,lymphatic spread, and vascular invasion. Oxygen-ation and perfusion (microcirculation) are believedto be important factors affecting the outcomes ofthe cytotoxic therapies.41 In a preradiation therapystudy, a favorable outcome was present in pa-tients with strong tumor enhancement, suggestinggood oxygenation. Tumors with baseline higherpermeability (Ktrans) tend to show a better re-sponse to radiotherapy.40,41 After radiotherapy,the onset time of tumor enhancement has beendelayed compared with that before therapy.42 Itis believed that local recurrence arises from radio-resistant hypoxic tumor regions represented bythe low-perfusion proportion of the pixel distribu-tion.41 A tendency of poorer prognosis has alsobeen reported, however, in tumors with a fast initialrate of enhancement or vascular permeability.43
Endometrial cancerWhen evaluating the local staging of endometrialcancers, early enhancement of the normal inner-most muscle layer on DCE MR imaging is the firstevident characteristic against the presence ofmyometrial invasion, and is considered to be rele-vant to the junctional zone on T2-weighted im-ages.44,45 This finding on DCE MR imaging forassessing myometrial invasion is valuable whenthe junctional zone on T2-weighted images isindistinct as in postmenopausal women.
LeiomyomaDCE MR imaging is also useful for assessing be-nign myometrial lesions to select effective therapy.The extent of enhancement and the degree ofhyaline degeneration seem to be related in leio-myomas.46 Increased vascularity may be helpfulin predicting the therapeutic effects of either uter-ine artery embolization or gonadotropin-releasinghormone analogue therapy.47,48
SUMMARY
Cine MR imaging is a useful tool for evaluatinguterine kinematic functions derived from myome-trial contractility, and for investigating the alter-ation of uterine contractility in a variety ofconditions and gynecologic disorders. DWI candemonstrate abnormal signal in pathologic focibased on differences in molecular diffusion, andcould provide useful information in evaluatingmalignant conditions. DCE MR imaging has thepotential to improve tumor detection and localstaging, and quantitative information may be use-ful for both monitoring therapeutic effects and pre-dicting outcome. The use of these state-of-the-artfunctional MR imaging techniques is beneficial forelucidating various uterine conditions when usedappropriately, and the findings provide the basisof future MR imaging investigations.
REFERENCES
1. Kido A, Nishiura M, Togashi K, et al. A semiauto-
mated technique for evaluation of uterine peristalsis.
J Magn Reson Imaging 2005;21:249–57.
2. Togashi K, Kawakami S, Kimura I, et al. Sustained
uterine contractions: a cause of hypointense myo-
metrial bulging. Radiology 1993;187:707–10.
3. Masui T, Katayama M, Kobayashi S, et al. Pseudole-
sions related to uterine contraction: characterization
with multiphase-multisection T2-weighted MR imag-
ing. Radiology 2003;227:345–52.
4. Lyons EA, Taylor PJ, Zheng XH, et al. Characteriza-
tion of subendometrial myometrial contractions
throughout the menstrual cycle in normal fertile
women. Fertil Steril 1991;55:771–4.
5. de Vries K, Lyons EA, Ballard G, et al. Contractions
of the inner third of the myometrium. Am J Obstet
Gynecol 1990;162:679–82.
6. Chalubinski K, Deutinger J, Bernaschek G. Vagino-
sonography for recording of cycle-related myome-
trial contractions. Fertil Steril 1993;59:225–8.
7. Nakai A, Togashi K, Yamaoka T, et al. Uterine peri-
stalsis shown on cine MR imaging using ultrafast
sequence. J Magn Reson Imaging 2003;18:726–33.
8. Nakai A, Togashi K, Kosaka K, et al. Uterine peristal-
sis: comparison of transvaginal ultrasound and two
different sequences of cine MR imaging. J Magn
Reson Imaging 2004;20:463–9.
9. Kido A, Togashi K, Nakai A, et al. Investigation of
uterine peristalsis diurnal variation. Magn Reson
Imaging 2006;24:1149–55.
10. Kataoka M, Togashi K, Kido A, et al. Dysmenorrhea:
evaluation with cine-mode-display MR imaging–
initial experience. Radiology 2005;235:124–31.
11. Kido A, Togashi K, Kataoka M, et al. The effect of
oral contraceptives on uterine contractility and
Functional MR Imaging of the Uterus 683
menstrual pain: an assessment with cine MR imag-
ing. Hum Reprod 2007;22:2066–71.
12. Stanford JB, Mikolajczyk RT. Mechanisms of action
of intrauterine devices: update and estimation of
postfertilization effects. Am J Obstet Gynecol
2002;187:1699–708.
13. Kadanali S, Varoglu E, Komec D, et al. Evaluation of
active and passive transport mechanisms in genital
tracts of IUD-bearing women with radionuclide hys-
terosalpingoscintigraphy. Contraception 2001;63:
41–5.
14. Kido A, Togashi K, Kataoka ML, et al. Intrauterine
devices and uterine peristalsis: evaluation with
MRI. Magn Reson Imaging 2008;26:54–8.
15. Kido A, Togashi K, Nakai A, et al. Oral contracep-
tives and uterine peristalsis: evaluation with MRI.